Embed Size (px)
Citation preview

Crit Care Nurs Clin N
Nutritional Assessment and Enteral Support of Critically
Ill Children
Erwin Ista, RNT, Koen Joosten, MD, PhD
Department of Pediatrics, Erasmus MC - Sophia Children’s Hospital, P.O. Box 2060, 3000 CB Rotterdam, The Netherlands
Critical illness has a major impact on the nutri-
tional status of children. Nutritional assessment is
required as an integral part of patient care; however,
during an intensive care stay, attention is focused
mostly on the primary medical problem and not on
the child’s nutritional status. When the child stays in
the ICU for longer than 5 to 7 days, the chance of
developing serious nutritional deficiencies increases
significantly [1]. As early as 1980, researchers dem-
onstrated protein-energy malnutrition in 15% to 20%
of children who were admitted to the ICU [2].
A recent study showed a high prevalence (24%) of
acute or chronic malnutrition in critically ill chil-
dren who were admitted to a pediatric ICU (PICU)
[3]. Therefore, nutritional support after initial nutri-
tional assessment should be an essential aspect of
the clinical management of patients in the PICU. The
diversity in clinical presentation and the various age
groups dictate a patient-tailored approach.
Several common hospital practices have been
identified that may cause the deterioration of nutri-
tional status in admitted patients (Box 1). In general,
the development of malnutrition during an ICU stay
can be related to the disease, incomplete nutritional
assessment or determination of the patient’s nutri-
tional needs, or lack of adequate nutritional support.
Widespread ignorance of the physiologic effects
of different feeding routes and the composition
of nutritional products results in the inappropriate
use of routes of administration of enteral and par-
0899-5885/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.ccell.2005.07.011
T Corresponding author.
E-mail address: [email protected] (E. Ista).
enteral feeds of uncertain composition or inade-
quate amounts.
Critical care nurses play an important role in the
feeding of critically ill children. Many procedures
and caregiving interventions, such as placement of
feeding tubes, registration of gastric retention, obser-
vation and care of the mouth, and administration of
nutrition (enteral or parenteral), are within the nurs-
ing domain. This article discusses nutritional as-
sessment techniques and enteral nutrition (EN) in
critically ill children.
Nutritional assessment
Definition
Nutritional assessment can be defined as the inter-
pretation of data concerning an individual’s intake
and use of nutrients to determine his or her health
status. Data must be obtained by different means,
and interpreted together to perform a comprehensive
nutritional assessment. These data includes:
� General evaluation (including dietary and medi-
cal history and physical signs)� Severity of illness assessment� Assessment of body composition� Laboratory studies (including the estimation of
energy requirements)
Nutritional assessment is necessary to: (1) identify
patients who have, or who are at risk for developing,
protein-energy malnutrition; (2) establish the degree
of malnutrition and the risk of developing malnu-
Am 17 (2005) 385 – 393
reserved.
ccnursing.theclinics.com

Box 1. Common hospital practices thatmay result in deterioration of nutritionalstatus
Diffusion of responsibility for the nutri-tional care of patients
Lack of interaction between medical,nursing, and dietetic staff
Little emphasis on nutrition educationin nursing and medical schools
Limited availability of methods toassess nutritional status
Failure to record patients’ heightand weight
Failure to observe and record patients’dietary intake
Frequent withholding of food becauseof diagnostic tests
Delay in commencing nutritional sup-port with prolonged use ofglucose administration
Adapted from Corish CA, Kennedy NP.Protein-energy undernutrition in hospitalin-patients. Br J Nutr 2000;83(6):575–91;with permission.
Box 2. Degree of stress
Pathology
Grade 1: mild stress factorDetection of health problemBronchiolitisGastroenteritisMinor surgeryOther minor infection
Grade 2: moderate stress factorCurrent surgeryChronic cardiopathyChronic enteropathySevere infectionCystic fibrosisSickle cell disease
Grade 3: severe stress factorCardiac surgeryDeterioration of chronic diseaseMajor visceral surgeryHemopathySevere depressionSevere sepsis
Adapted from Sermet-Gaudelus I, Poisson-Salomon AS, Colomb V, et al. Simple pe-diatric nutritional risk score to identifychildren at risk of malnutrition. Am J ClinNutr 2000;72(1):64–70;with permission.
ista & joosten386
trition related complications; and (3) evaluate the
effect of nutritional support [4]. Accurate assess-
ment of nutritional status in children is complex
because of ongoing growth, changing energy needs,
varying body composition, and disease [5]. In criti-
cally ill children this phenomenon is more complex
because of weight shifts that are caused by third
spacing of fluid; this can result in inaccurate anthro-
pometric measurements and inaccurate assumptions
of true weight [1].
Techniques
General evaluation
A full medical and dietary history is necessary for
an extensive nutritional assessment. When the criti-
cally ill child has a history of chronic disease, the
initial nutritional status at admission might be poor
and the child may need extra attention. Physical signs
of malnutrition usually do not appear until malnu-
trition had been prolonged and severe; however, the
first impression of the child and subjective assess-
ment of muscle and fat mass can help. Subjective
global assessment is a clinical technique that assesses
nutritional status based on features of the history and
physical examination [6]. On admission, a detailed
history concerning nutrition can be performed by the
nursing staff.
It also is important to be alert for the develop-
ment of malnutrition during admission. A study by
Sermet-Gaudelus and colleagues [7] showed that
79% of hospitalized children lost weight (>2%) dur-
ing admission. Using a pediatric nutritional risk
score, they found that the patients’ degree of stress
(Box 2), food intake, and pain were associated with
weight loss. They developed a pediatric nutritional
risk score that identifies three classes of risk (low,
moderate, and high) and recommendations for nu-
tritional interventions (Table 1).
Anthropometry
Classic anthropometry is a term that describes
the measurement of body weight, body length, and
head circumference. Additional anthropometric mea-

Table 1
Pediatric nutritional risk score and recommendations for nutritional intervention
Risk factors [coefficients]
Score Nutritonal risk Nutritional interventionPathology
Pain [1] Food
intake <50% [1]
Mild (grade 1) [0] None 0 Low None
Mild (grade 1) [0] One 1 Moderate Assess food intake and weight daily
Mild (grade 1) [0] Both 2 Moderate Refer to a dietitian
Moderate (grade 2) [1] None 1 Moderate Start oral nutritional support (NS)
Moderate (grade 2) [1] One 2 Moderate
Moderate (grade 2) [1] Both 3 High Measure ingested food precisely
Severe (grade 3) [3] None 3 High Refer to a nutrition team
Severe (grade 3) [3] One 4 High Consider enteral or parenteral NS
Severe (grade 3) [3] Both 5 High
Adapted from Sermet-Gaudelus I, Poisson-Salomon AS, Colomb V, et al. Simple pediatric nutritional risk score to identify
children at risk of malnutrition. Am J Clin Nutr 2000;72(1):64–70; with permission.
picu nutritional assessment and enteral support 387
surements concern circumferences (mid upper arm,
calf, abdominal), skin fold thickness, and lower leg
length (knemometry).
Weight
Weight is the most important parameter for nu-
tritional assessment of the critically ill child; there-
fore, it is a gold standard [1]. The assessment of
weight in this group is not easy and changes in weight
cannot be ascribed only to growth, because edema
plays an important role. In our practice we propose
assessing weight on admission and daily during the
PICU stay (except in chronically ill children) [3,8].
Length
Body length is difficult to measure and generally
is of limited value as a nutritional assessment tool on
the ICU, because changes in linear growth are hard
to point out over a short period of admission. For
newborn infants and children up to 24 months of
age, the lower leg length measure is a promising
method for measurement of short-term linear growth;
it consists of a heel-to-knee measurement (knemo-
metry) [9]. The tool is hand-held, can be used in-
side an incubator, and is less disruptive than making
length measurements.
Head circumference
Head circumference is another important aspect
of nutritional assessment in young children and
should be included in the initial assessment and
follow-up. In the PICU this parameter is used rarely;
however, on admission it could signal a history of
severe chronic malnutrition. Serial measurements
in neonates can aid in detecting the development
of malnutrition.
Body circumferences and skin fold thickness
Measurements of body circumferences (mid up-
per arm, calf, abdominal) and skin fold thickness
are anthropometric measurements that can provide
information on fat mass and fat-free mass. Mid upper
arm circumference (MUAC) is a measure of muscle,
fat, and bone. It has been used as an index of mal-
nutrition in rapid nutritional surveys when weight and
length measurements were not feasible. We advocate
measuring the MUAC in all children because it is
simple to perform on admission and follow-up and
it is an easy screening tool for malnutrition.
Feasibility of anthropometry. One has to take into
account that the feasibility to perform anthropomet-
ric measurements decreases with the severity of dis-
ease. The feasibility to perform anthropometric
measurements routinely was investigated. For weight,
35% of ventilated children were weighed on admis-
sion; 84% of all children who were in the PICU for
more than 48 hours were weighed [3,8]. This knowl-
edge underlines the need for a patient-tailored ap-
proach in which measurements can be performed in
the individual patient to detect malnutrition.
Indirect calorimetry
Measuring energy expenditure allows for a more
accurate monitoring of the child’s varying energy
needs in the course of critical illness. Clinically, the
measurement of energy expenditure by indirect calo-
rimetry (IC) is applicable in critical care, and is more
accurate than estimating individual energy expendi-
ture from standard prediction equations. IC provides
noninvasive, reliable, repeatable, and affordable mea-
surements of actual energy expenditure (resting
energy expenditure in nonventilated children and

ista & joosten388
total daily energy expenditure in ventilated children)
and the respiratory quotient (RQ).
RQ is a helpful parameter in nutritional assess-
ment because it has been considered important in
evaluating substrate use or nutritional support and in
determining overfeeding and underfeeding [10,11].
Table 2 shows the RQ values related to the feeding
status used in clinical practice. An RQ of greater
than 1 indicates overfeeding, which most of the time
is due to carbohydrate overfeeding; therefore, atten-
tion should be focused on the carbohydrate intake.
In the critically ill child, quantification of energy
expenditure also is important from the diagnostic
standpoint because it allows the detection of hyper- or
hypometabolic conditions that are related directly to
the individual prognosis. The greatest advantage of
using IC is to design a nutrition regimen that exactly
meets the patient’s energy requirements and avoids
the complications of overfeeding [12].
The IC in the ICU is valuable because not much
other information is available for approximating
the needs of the critically ill child [1]. IC to deter-
mine energy requirements is being used widely as a
research tool. In most ICUs, limited space at the
bedside, the cost of multiple metabolic carts, and the
availability of trained staff to operate them limit its
routine use.
For the practical use of IC in critically ill chil-
dren, accurate measurement requires the follow-
ing conditions:
� Fraction of inspired oxygen of less than 0.60� Tube leakage of less than 10%. Tube leakage
is determined by comparison of inspired and
expired tidal volumes measured by the ventila-
tor, assuming that there are no other leaks in the
patient–ventilator circuit.
In one investigation, the feasibility of routine use
of IC performed by the nursing staff was studied;
it was possible in 70% to 80% of the eligible
mechanically ventilated children [3,8].
Taken together, nutritional assessment is impor-
tant in providing optimal care to critically ill children.
A simple and integrated nutrition screening should
Table 2
Feeding status related to respiratory quotient
Feeding status Respiratory quotient
Underfeeding < 0.85
Adequate feeding 0.85–1.0
Overfeeding > 1.0
be part of the admission procedure in the ICU. It
has to be followed by an individual calculation of
macro- and micronutrient needs. In addition, nutri-
tional assessment should be repeated regularly to
monitor changes in nutritional status, diagnoses, or
conditions that might put the child at nutritional
risk, and to monitor the efficacy of nutritional sup-
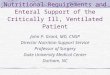
port. Fig. 1 shows a standard of nutritional assess-
ment for the PICU population.
Nutritional support
The most important element in nutritional sup-
port in the intensive care setting is to have a stan-
dard feeding protocol in which three issues should
be considered:
� When to feed: indications for nutritional support� What to feed: composition of nutritional for-
mula and enteral feeding� How to feed: how to administer EN
Application of such a protocol is the most im-
portant step in treating the malnourished patient in
the ICU. The working group on nutrition and metabo-
lism of the European Society of Intensive Care Medi-
cine published a practical approach in 1998 for EN
for adult patients in the ICU [13]. These recommen-
dations consisted of the supply of macronutrients,
micronutrients, and immunomodulating agents, and
recommendations for feeding and organ dysfunction,
feeding preparations, and conditioning and routes of
feeding. Such a practical approach has not been pub-
lished for critically ill children; however, the concept
of this working group should be translated for the
critically ill child.
When to feed: indications for nutritional support
For assessing the total nutritional status of a pa-
tient, several parameters have to be evaluated. Souba
[14] stated that identification of the malnourished
adult patient at risk is important because besides estab-
lished indications for the use of nutritional support,
there is a list of unproven indications that requires
further study. There are accepted guidelines for the
time to start additional nutritional support for the
adult patient who has a severe illness; these consist
of items, such as the duration of the catabolic state,
days without nutrition, and the presence of mal-
nutrition on admission [15].
Compared with adults, children have less physio-
logic reserves of fat and protein and increased energy

Initial nutritional screening in all children on admission
Term neonates and older children with poor nutritional statusat admission or at high risk*
Anthropometry
(evaluation of nutritional risk)
Weight (SDS)Length (SDS), if possibleHead circumference (SDS)Primary diagnosisIllness severity score (PRISM, PIM, CRIB)Presence of comorbiditiesSurgery neededExpected duration of mechanical ventilationExpected length of ICU-stay
Weight
Indirect calorimetry - ASAP after adm, 2x/ wk thereafter(to adjust intake)
Alternative: 0.5-1.0*RDA
Daily calculation of nutrient intake compared to prescribed intake (energy and protein)⇒interruptions?
Daily calculation of actual energy intake compared to estimated/measured EE ⇒ deficits?
Evaluation of RQ (2x/ wk): RQ > 1.0 ⇒ decrease carbohydrate or energy intake; RQ < 0.85 increase intake
Weekly calculation of cumulative energy and protein deficits in relation to growth/anthropometry
- twice a week†
- biweekly- adm, weekly- adm, weekly- adm, weekly
HC (< 1 y)MUAC/CCKHL (< 2 y)TSF
Energy requirements
LOS < 48 h LOS > 48 h
No furtherassessment
Adjustmentof intake
Fig. 1. Proposed standard of nutritional assessment in the pediatric ICU population. Adapted from Hulst JM. Nutritional
assessment of critically ill children: the search for practical tools [master’s thesis]. Rotterdam (The Netherlands): Erasmus
University; 2004; with permission.
Abbreviations: Adm, admission; ASAP, as soon as possible; CC, calf circumference; CRIB, Clinical Risk Index for Babies;
EE, energy expenditure; HC, head circumference; LFA, length for age; KHL, knee-heel length; LOS, length of stay; MUAC,
mild upper arm circumference; PIM, Pediatric Index of Mortality; PRISM, Pediatric Risk of Mortality; RQ, respiratory quotient;
SDS, standard deviation score; TSF, triceps skin fold; WFA, Weight for age; WFL, Weight for length.
* poor nutritional status: WFA-SDS or LFA-SDS or WFL-SDS <�2; risk groups: prolonged expected ICU-stay, prolonged
duration of mechanical ventilation, children undergoing surgery, children with underlying growth-affecting disease such as
children with major congenital malformations, cardiac anomalies, cystic fibrosis, Inflammatory bowel disease, HIV-infection.
y depending on age of child.
picu nutritional assessment and enteral support 389
expenditure; therefore, children are at increased risk
for malnutrition [16]. Furthermore, it seems appro-
priate to start nutritional support as soon as possible
because children are in a state of growth, develop-
ment, and organ maturation.
What to feed: composition of nutritional formulas
Current recommendations for nutritional support
in critically ill pediatric patients are not based on
randomized trials with feeding intervention studies.
Knowledge concerning substrate intake and substrate
use can be derived from adult studies and studies
concerning primarily surgically treated newborn
infants. Knowledge concerning energy expenditure
can be derived from a few studies of mechanically
ventilated children; however, some important con-
clusions can be drawn from these studies:
� There is a significant discrepancy between mea-
sured energy expenditure compared with calcu-
lated energy expenditure using predictive equations� The total daily energy requirements can be higher
or lower than values of resting energy expendi-

ista & joosten390
ture but in general the total daily energy re-
quirements of the critically ill child will be
lower than the total daily energy requirements
for healthy children� There is a considerable risk for overfeeding in
the critically ill child for carbohydrate, fat and
protein [11,17]� There might be an individual maximum of oxi-
dative capacity for carbohydrate, fat and protein� Carbohydrate overfeeding can be determined by
measuring the respiratory quotient; an RQ of
more than 1.0 indicates overfeeding.� Fat overfeeding can be determined by measur-
ing plasma triglycerides levels or comparing fat
intake with fat use.� Protein needs can be determined by measuring
urinary nitrogen excretion [11,18].� Protein retention can be increased by a balanced
glucose/fat solution [19].� There might be an optimal nonprotein calorie:
nitrogen ratio to enhance protein retention.
Energy requirements
The reference method to evaluate the energy need
is IC. Some factors (eg, fever, injury, dialysis) cause
an increase in energy expenditure, whereas other
factors (eg, sedation or relaxation, decreased work of
breathing, decreased loss of heat during mechanical
ventilation) cause a decrease of energy expenditure.
A pragmatic estimate of energy requirements is
given in Table 3, based on a percentage of the rec-
ommended daily allowances of healthy children.
For growth of the infant for each 1 gram growth,
4 kcal growth should be added. One should account
for 10% to 15% loss of energy when enteral feeding
is supplied.
Protein requirements
The method to evaluate the protein need is to
calculate urinary nitrogen excretion. Protein need can
Table 3
Nutrition schedule of early enteral feeding protocol
Age Type of feedinga
0–1 months Nutrilon / breast milk
1–12 months Infatrini / breast milk
1–6 years Nutrini multi fiber
7–12 years Tentrini multi fiber
>12 years Nutrison multi fiber
a Nutricia, Zoetermeer, The Netherlands.
range from 1 g/kg/d to 4 g/kg/d in the severely ill
child. A recommendation is to start with enteral or
parenteral protein of 1 g/kg/d, and to increase the
amount depending on the need and level of blood
urea. Proteins that are administered with fresh frozen
plasma should not be taken into account. Standard
enteral formulas can be administered because there
is no evidence to use protein diet formulas.
Glucose requirements
Enteral or parenteral glucose should be admin-
istered at 4 to 6 mg/kg/min, depending on the se-
verity of disease and the tolerance of the patient.
The method to evaluate carbohydrate overfeeding is
measuring a respiratory quotient with IC or to
determine serum hyperglycemia or glucosuria. Insu-
lin therapy is started for hyperglycemia, depending
on the duration and the diagnosis, according to the
current guidelines of intensive insulin therapy in
adults [20].
Fat requirements
In general, the parenteral fat intake is less than
the enteral fat intake because there is a maximum
capacity to hydrolyze the administered parenteral fat
emulsions. Furthermore, the absorption of enteral fat
is 80% to 90%. When parenteral feeding, a low
amount of fat—0.5 g/kg/d—is started in the acute
phase of illness because of the risk of fat overload-
ing. In general, a least 2% to 3% of calories should
be linoleic acid to prevent fatty acid deficiency. The
method to evaluate fat overload is to measure plasma
triglycerides; fat intake should be adjusted depend-
ing on this level. The fat intake can be increased
gradually to between 3 g/kg/d and 4 g/kg/d. When
enteral feeding is supplied, fat in the amount of
1 g/kg/d to 1.5 g/kg/d should be given initially.
This amount can be increased gradually to between
7 g/kg/d and 8 g/kg/d in small infants and to be-
tween 3 g/kg/d and 4 g/kg/d in older children.
Amount of feeding
Day 1 - half of
RDA (kcal/kg/d)
Day 2 - total
RDA (kcal/kg/d)
50 100
47–100 95–100
46 92
35–42 70–84
25–30 49–60

Table 4
Amount of ice water
Age child Ice water
0–6 months 5 ml
6–12 months 10 ml
> 1 year 1 ml/kg
picu nutritional assessment and enteral support 391
How to feed: administration of enteral nutrition
Although nutrition can be provided to critically ill
children enterally or parenterally, the enteral route
is preferred if there are no contraindications [21]. EN is
the preferred method of nutritional support for
pediatric patients when the gastrointestinal tract can
by used. Advantages of EN are convenience, safety,
and low cost. EN also is important in maintaining
gastrointestinal mucosal integrity and immunologic
function that may prevent bacterial translocation and
multisystem organ failure in critically ill children [22].
Gastric and duodenal/jejunal feedings are the primary
routes for EN administration in critically ill children.
Gastric tubes usually are placed easily by bedside
nurses with fewer complications. Nasoduodenal feeding
tubes are recommended to reduce the risk of aspira-
tion in the presence of delayed gastric emptying or re-
flux [22], and is a safe ‘‘way’’ when continuous enteral
feeding of mechanically ventilated children is given.
Many strategies have been developed to increase
the success rate for placement of feeding tubes in
the small bowel/duodenum. Spalding and colleagues
[23] tested the effectiveness of gastric insufflation as
an adjunct to the placement of feeding tubes in the
small bowel compared with the standard insertion
technique. The investigators assumed that gastric in-
sufflation is a technique for bedside insertion of a
transpyloric feeding tube. Determination of tube po-
sition was done by a radiographic method. Other
studies demonstrated that the transpyloric placement
of feeding tubes using pH sensing is successful, but
specialized equipment is required [24,25]. Chellis and
colleagues described their experience with bedside
placement method using metoclopramide (0.1 mg/kg,
intravenously). Transpyloric placement was con-
firmed by absence of blue dye in nasogastric secre-
tions as well as by an abdominal radiograph [26].
In the PICU at Sophia Children’s Hospital, Rotter-
dam, The Netherlands, enteral feeding is given by a
transpyloric route (duodenal feeding tube) in mechani-
cally ventilated critically ill children. Transpyloric
feeding was easy to establish within 24 hours after
admission in most (44/46 [95%]) of the mechani-
cally ventilated children of various ages and with
various diseases [8] using a standard protocol.
The protocol for inserting a transpyloric feeding
tube is as described:
A 6, 8, or 10 French enteral feeding tube of ap-
propriate size for each patient is used.
Before insertion, the length of tubing needed to
reach the stomach and the fourth part of the
duodenum is determined.
The tube is placed in the stomach and the position is
confirmed by injection of air with auscultation.
Children are positioned right side down.
Before the feeding tube is advanced to the pre-
determined length, ice water is inserted to stimu-
late pyloric opening. The amount of ice water is
related to the age of the patient (Table 4).
The position of a transpyloric feeding tube is
determined by the use of a pH stick; if the pH
is between 7.0 and 8.0 it can be concluded that
the feeding tube is located transpyloric.
If this method is not successful after two attempts
with ice water, erythromycin (10 mg/kg) is
administrated intravenously for 30 minutes.
Directly after infusion of erythromycin, a new
attempt is executed. The use of erythromycin
can be helpful in stimulating pyloric opening.
The bedside placement of pH-guided transpyloric
small bowel feeding tubes can be done by nurses. In
addition, it is a low cost method for determining the
location of the feeding tube tip. Both of these are
considered advantages of this particular method. If
it is not possible to feed transpyloricly, continuous
gastric feeding will be started and gastric motility
agents (eg, motilium) will be added; however, it is
not possible to give all patients EN. Gastric retention,
diarrhea, and abdominal distention can limit the use
of enteral feeding. If possible, the enteral route of
feeding should be used, even with small amounts,
unless it is absolutely contraindicated (eg, bowel ob-
struction, intractable diarrhea).
Early enteral nutrition
Zaloga and Roberts [27] reviewed the results of
early EN in animal and human adult studies. Animal
studies showed that early EN improved gut blood
flow and gut mass, diminished the invasiveness of gut
bacteria, protected the liver and prevented injury
during shock, improved protein synthesis and the rate
of wound healing, and increased survival after critical
illness. More importantly, prospective, randomized
trials in humans have indicated that early EN im-
proved outcome during critical illness.

ista & joosten392
Studies in premature and low birth-weight infants
found that the lack of enteral feeding may result in
an absence of the natural stimulus for growth of the
intestinal mucosa, as well as diminished production
of intestinal mucins, which acts as a barrier to bac-
terial translocation [28]. Further proof of the efficacy
and safety of early enteral feeds was given in the
form of case reports and case series of burn patients
[29,30]. Chellis and colleagues performed a study
in 42 critically ill children to evaluate the feasibility
and safety of early enteral feedings. All patients were
able to achieve caloric goals within 48 hours of
beginning enteral feedings, and there were no docu-
mented complications, such as aspiration or abdomi-
nal distention [31]. A more recent retrospective study
in 95 critically ill children showed that it was possi-
ble to start EN within 24 hours after admission in
most children [32]. A limitation of both of these
studies was the use of retrospective chart review for
data collection.
A recent prospective analysis examined the use
of an early enteral feeding protocol in critically ill
children who were hemodynamically stable and who
had not undergone abdominal surgery. The aim of
the enteral feeding protocol was to feed critically ill
children within 2 days after admission according to
the total recommended daily energy intake (RDA)
for healthy children. The type and amount of enteral
feeding were based on the age category and weight
of the child (see Table 3). On day 1 of admission,
enteral feeding is started at 50% of the total RDA
and increased to 100% of RDA on day 2. With
this protocol, on day 1 and day 2, 90% and 89%,
respectively, of the children received the type of
feeding according to the protocol. In 10% and 11%
of the cases, respectively, the caregivers deviated
from the standard because of nutrition intolerance
and logistical problems. Concerning the amount of
the enteral feeding, on day 1 and day 2, 84% and 78%
of the children, respectively, received the amount
according to the protocol [8].
Despite the enthusiasm about enteral feeding, it
is not possible to give all critically ill children the
maximum required amount of enteral feeding accord-
ing to RDA. Barriers for the adequacy of nutri-
tional support in critically ill children are restriction
of fluid intake, clinical interventions (extubation),
administration of medications, gastrointestinal intol-
erance, and mechanical complications with the
enteral feeding tube [32–34].
Enteral feeding in critically all children should be
started as soon as possible. If critically ill children
are hemodynamically stabilized—even if high doses
of inotropics are necessary—small amounts of en-
teral feeding can be started. Because critically ill
children suffer from gastric dysmotility and empty-
ing difficulties, transpyloric tube feeding is the pre-
ferred route.
Total parenteral feeding is indicated when the
gastric– intestinal tract is nonfunctional, when it is
impossible to obtain enteral access, or when EN alone
is not able to meet the child’s energy requirements.
References
[1] Huddleston KC, Ferraro-McDuffie A, Wolff-Small T.
Nutritional support of the critically ill child. Crit Care
Nurs Clin North Am 1993;5(1):65–78.
[2] Pollack MM, Ruttimann UE, Wiley JS. Nutritional
depletions in critically ill children: associations with
physiologic instability and increased quantity of care.
J Parenter Enteral Nutr 1985;9(3):309–13.
[3] Hulst JM. Nutritional assessment of critically ill chil-
dren: the search for practical tools [master’s thesis]. Rot-
terdam (The Netherlands)7 Erasmus University; 2004.
[4] Klein S, Kinney J, Jeejeebhoy K, et al. Nutrition sup-
port in clinical practice: review of published data and
recommendations for future research directions. Sum-
mary of a conference sponsored by the National Insti-
tutes of Health, American Society for Parenteral and
Enteral Nutrition, and American Society for Clinical
Nutrition. Am J Clin Nutr 1997;66(3):683–706.
[5] Khoshoo V. Nutritional assessment in children and
adolescents. Curr Opin Pediatr 1997;9(5):502–7.
[6] Detsky AS, McLaughlin JR, Baker JP, et al. What
is subjective global assessment of nutritional status?
J Parenter Enteral Nutr 1987;11(1):8–13.
[7] Sermet-Gaudelus I, Poisson-Salomon AS, Colomb V,
et al. Simple pediatric nutritional risk score to identify
children at risk of malnutrition. Am J Clin Nutr 2000;
72(1):64–70.
[8] Ista E, Joosten KFM. Successful early enteral feed-
ing of critically ill children [abstract]. 15th ESPNIC
Medical and Nursing Annual Congress; London;
2004. p. 103.
[9] Hermanussen M. Knemometry, a new tool for the in-
vestigation of growth. A review. Eur J Pediatr 1988;
147(4):350–5.
[10] McClave SA, Lowen CC, Kleber MJ, et al. Clinical
use of the respiratory quotient obtained from indirect
calorimetry. J Parenter Enteral Nutr 2003;27(1):21–6.
[11] Joosten KFM, Verhoeven JJ, Hazelzet JA. Energy ex-
penditure and substrate utilization in mechanically
ventilated children. Nutrition 1999;15(6):444–8.
[12] Brandi LS, Bertolini R, Calafa M. Indirect calorimetry
in critically ill patients: clinical applications and prac-
tical advice. Nutrition 1997;13(4):349–58.
[13] Van den Berghe G, de Zegher F, Bouillon R. Clinical
review 95: acute and prolonged critical illness as dif-
ferent neuroendocrine paradigms. J Clin Endocrinol
Metab 1998;83(6):1827–34.

picu nutritional assessment and enteral support 393
[14] Souba WW. Nutritional support. N Engl J Med 1997;
336(1):41–8.
[15] Revhaug A, Kjaeve J. Nutrition in the acute catabolic
state. In: Revhaug A, editor. Acute catabolic state.
Berlin7 Springer-Verlag; 1996. p. 257–67.
[16] Cunningham JJ. Body composition and nutrition
support in pediatrics: what to defend and how soon
to begin. Nutr Clin Pract 1995;10(5):177–82.
[17] Chwals WJ. Overfeeding the critically ill child: fact
or fantasy? New Horiz 1994;2(2):147–55.
[18] Mickell JJ. Urea nitrogen excretion in critically ill
children. Pediatrics 1982;70(6):949–55.
[19] Nose O, Tipton JR, Ament ME, Yabuuchi H. Effect of
the energy source on changes in energy expenditure,
respiratory quotient, and nitrogen balance during total
parenteral nutrition in children. Pediatr Res 1987;
21(6):538–41.
[20] Van den Berghe G, Wouters P, Weekers F, Verwaest C,
Bruyninckx F, Schetz M, et al. Intensive insulin
therapy in the critically ill patients. N Engl J Med
2001;345(19):1359–67.
[21] Curley MA, Castillo L. Nutrition and shock in pedi-
atric patients. New Horiz 1998;6(2):212–25.
[22] Marian M. Pediatric nutrition support. Nutr Clin Pract
1993;8(5):199–209.
[23] Spalding HK, Sullivan KJ, Soremi O, et al. Bedside
placement of transpyloric feeding tubes in the pediatric
intensive care unit using gastric insufflation. Crit Care
Med 2000;28(6):2041–4.
[24] Krafte-Jacobs B, Persinger M, Carver J, et al. Rapid
placement of transpyloric feeding tubes: a comparison
of pH-assisted and standard insertion techniques in
children. Pediatrics 1996;98(2 Pt 1):242–8.
[25] Dimand RJ, Veereman-Wauters G, Braner DA. Bed-
side placement of pH-guided transpyloric small bowel
feeding tubes in critically ill infants and small children.
J Parenter Enteral Nutr 1997;21(2):112–4.
[26] Chellis MJ, Sanders SV, Dean JM, et al. Bedside
transpyloric tube placement in the pediatric intensive
care unit. J Parenter Enteral Nutr 1996;20(1):88–90.
[27] Zaloga GP, Roberts PR. Early enteral feeding improves
outcome. In: Vincet JL, editor. Yearbook of intensive
care and emergency medicine. Berlin7 Springer-Verlag;
1997. p. 701–14.
[28] Wesley JR. Nutritional support in the pediatric intensive
care unit. Curr Opin Gastroenterol 1994;10:210–7.
[29] Trocki O, Michelini JA, Robbins ST, et al. Evaluation
of early enteral feeding in children less than 3 years
old with smaller burns (8–25 per cent TBSA). Burns
1995;21(1):17–23.
[30] Engelhardt VJ, Clark SM. Early enteral feeding of a
severely burned pediatric patient. J Burn Care Rehabil
1994;15(3):293–7.
[31] Chellis MJ, Sanders SV, Webster H, et al. Early enteral
feeding in the pediatric intensive care unit. J Parenter
Enteral Nutr 1996;20(1):71–3.
[32] Taylor RM, Preedy VR, Baker AJ, et al. Nutritional
support in critically ill children. Clin Nutr 2003;22(4):
365–9.
[33] Adam S, Batson S. A study of problems associated
with the delivery of enteral feed in critically ill patients
in five ICUs in the UK. Intensive Care Med 1997;
23(3):261–6.
[34] Rogers EJ, Gilbertson HR, Heine RG, et al. Barriers to
adequate nutrition in critically ill children. Nutrition
2003;19(10):865–8.