Embed Size (px)
Citation preview

Crit Care Clin 20 (2004) 135–157
Nutritional support of the critically ill and
injured patient
D. Sue Slone, MDTrauma Critical Care Section, Swedish Medical Center, 499 East Hamden Avenue, Suite 380,
Englewood, CO 80110, USA
Critically injured patients are characterized by hypermetabolism and accelerated
catabolism, leading to rapid malnutrition. The prevalence of malnutrition among
hospitalized patients is as high as 50% [1,2]. Inadequate nutrition is associated with
an increased risk of morbidity, mortality, and longer hospital stays [3]. Most trauma
patients are well nourished before injury. These patients are candidates for
nutritional support because of the hypercatabolic state associated with multiple
trauma. Adjuvant nutritional therapy has developed an expanding role in clinical
intensive care, as the medical community begins to understand the immune system,
sepsis, multiple organ dysfunction, and wound healing. With a better understand-
ing of the endogenous responses to injury, more can be learned about the mediators
of these responses. These mediators can be manipulated through improved insight
into nutritional support, its timing, complications, and its role in the full recupera-
tion of patients from the acute phase to rehabilitation.
Nutritional assessment
Assessment is used to identify patients who would benefit from nutritional
support and suggests a design for that therapy. No patient is more difficult to feed
than one with multiple injuries. As catecholamines, cytokines, and insulin levels
rise in response to these traumatic insults, energy expenditure and protein turnover
increase. Because of the heterogeneity of this patient population, it is difficult to
develop guidelines applicable to all critically injured patients. There is a great need
for clinical judgment. Many authors have provided exhaustive lists of possible
markers for nutritional assessment [4]. The focus of this discussion will define a
practical strategy, using readily available means of assessing nutritional status.
Conditions such as thermal injuries, severe CNS (central nervous system) insult,
0749-0704/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/S0749-0704(03)00093-9
E-mail address: [email protected]

D.S. Slone / Crit Care Clin 20 (2004) 135–157136
sepsis, and certain comorbid conditions (eg, cancer, COPD [chronic obstructive
pulmonary disease], alcoholism, and heart disease) produce added metabolic
challenges and complications. These conditions exacerbate energy expenditure
and protein catabolism brought on by severe injury. This evokes a variation even
among patients with the same disease process [5].
The assessment begins with a thorough history. This is not always practical
during a trauma resuscitation and evaluation. The added challenge of alcohol
intoxication, coma, pharmacologic management of the ventilator, and frequent
anesthesia adds to the inherent challenge. Once the history is attainable, it should
include alcoholic tendencies (associated with malnutrition), history of diabetes,
chronic pulmonary disease, renal failure, weight gains, and weight losses (asso-
ciated with increased morbidity) [6]. The underlying mechanism of injury is
relevant to the assessment. Body weight change in the intensive care unit (ICU)
patient is not a good measure of outcome, because it usually reflects fluid shifts.
Body weight is most useful as serial measurements of the hospitalized patient to
assess fluid status and response to therapy. The largest problemwith body weight is
that it relies on the comparison of a range of normal values that often is limited by
the diversity of the control population [7]. A more optimal nutritional indicator is
body mass index (BMI, body weight in kilograms divided by square of height in
meters). This index overcomes the limitations of changes in body weight and the
need to compare it with expected normal values (Fig. 1).
Clinicians should inspect for body habitus, obesity, muscle mass, pretemporal
wasting, and edema. Although anthropometrics measures, such as triceps, skinfold
thickness, and midarm muscle circumference are objective evaluations of these
energy pools, they add little to the overall clinical plan [8]. These measurements are
safe, simple, and inexpensive. They can be done at the bedside. Because the ratio of
subcutaneous to total body fat may vary from 20% to 70% in normal subjects [9], it
is notoriously inaccurate over a range of body sizes. It is most inaccurate in the
extreme patients. These measures will often overestimate body fat in malnourished
patients. They will underestimate body fat in obese patients. Acute changes are not
detected accurately with anthropometrics [10]. These findings often are very hard
to assess after aggressive fluid resuscitation.
Serum albumin
Albumin remains a useful tool in evaluating nutrition and predicting the
patient’s risk for morbidity [11]. Gibbs et al found this to be a significant predictor
for sepsis and major infections. This clinical trial involved over 54,000 patients,
and the preoperative albumin level was identified as a significant predictor of
mortality and morbidity for patients undergoing surgical procedures. There would
be no baseline albumin in trauma patients. It was a predictor of pneumonia and
wound infections [12], which would be applicable in the critically injured patients.
Clinicians are cautioned that serum albumin can be altered with excessive protein
losses, catabolism, and decreased hepatic protein synthesis. Dilutional effects

Fig. 1. Body mass index calculator.
D.S. Slone / Crit Care Clin 20 (2004) 135–157 137
following massive fluid resuscitation are a very big factor in the trauma care
setting. Transferrin, prealbumin, and other proteins have been studied for pos-
sible improvements over albumin. They did not increase the sensitivity of this
laboratory value. The difference in their usefulness is related to their reduced half-
life. Transferrin (8- to 10-day half-life) and prealbumin (2- to 3-day half-life) have
been accepted as sensitive indicators of acute protein and energy depletion, but
they have not been shown to make a significant difference in the prediction
of outcome [3]. Retinol binding protein has a 20-hour half-life, but it is limited
by the same multifactor concerns.

D.S. Slone / Crit Care Clin 20 (2004) 135–157138
Objective multi-parameter indices designed to predict clinical outcomes rely on
these values and thus are limited by the same concerns. For example, when tested
clinically, the prognostic nutrition index (PNI) grossly overestimates the risk of
complications and death [13].
Measures of immunocompetence
Immunity is suppressed by malnutrition. Cell-mediated immunity is more
affected than humoral. [3] The total lymphocyte count (TLC) and delayed
hypersensitivity skin testing (DHST) are the two tests most frequently used. A
TLC of less than 3000/mm3 reflects immunodeficiency. It is not useful in patients
who are critically ill, since sepsis, trauma, and disseminated intravascular coagul-
opathy also depress immune function, including TLC. There has been a strong
association between DHST results and morbidity. Mortality rates are higher in
patients with negative skin test reactions when compared with patients with normal
reactivity [14].
Caloric and nitrogen balance studies
Balance studies are used in the ICU to clarify nutritional requirements. They
do not furnish a dynamic picture of the adequacy of current nutritional status.
Balance studies fail to provide an assessment of past deficits and future improve-
ments. Nitrogen balance is an inexpensive, easy, and effective measurement. It is
calculated by subtracting the total excreted nitrogen from the total dietary
nitrogen intake (Box 1).
Box 1. Nitrogen output and balance equations
Nitrogen output
24-hour urine urea nitrogen(UUN)(g/d)=
UUN(mg/d)� urine output(mL/d) �1 g/1000 mg
�1 dL/100 mL
Total nitrogen loss(g/d)24-hour UUN(g/d)
+(0.20� 24-hour UUN g/d)+2 g/d
Nitrogen balance
24-hour intake protein (g)/6.25(g)� urinary nitrogen (g/d)=N/d

D.S. Slone / Crit Care Clin 20 (2004) 135–157 139
The seemingly simple determination of nitrogen balance is fraught with
difficulties. About 80% of nitrogen is eliminated through the urine. Other losses
(purines, ammonia, and others) are estimated at 2 g daily. Twenty percent of urea is
eliminated through feces and various other body fluids. A positive nitrogen
balance, in the range of 2 to 4 g of nitrogen per 24 hours (anabolic state) is very
difficult to achieve in the critically injured patient. This is simply not attainable
when severe hypermetabolism is present [15].
Metabolic requirements
The balance between energy intake and expenditure determines the daily energy
requirements (calories). If measured energy expenditure (MEE) is not readily
available, the estimated caloric requirement is 104.67 to 146.54 kJ/kg of ideal
body weight. Calorie balance can be measured using indirect calorimetry or
calculated by the Harris–Benedict equation (published nearly 85 years ago,
Box 2) [16]. This equation was developed using healthy volunteers and there-
fore dramatically underestimates the energy requirements of trauma patients.
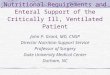
Stress factors evolved for the modification of this formulation and are highly
suspicious for overestimation of caloric requirements (Table 1) [17].
The most accurate measure of BEE is the indirect calorimetry using a metabolic
cart [18]. The basal metabolism can be determined by measuring oxygen con-
sumption (VO2) and carbon dioxide production (VCO2).
Energy expenditure ¼ cardiac output � VO2 þ ð1:11Þ ðVCO2Þ ½19�
The procedure to measure BEE is slightly more labor intensive and sometimes
difficult in the critical care setting. It also provides a respiratory quotient (RQ).
This ratio of the carbon dioxide production (VCO2) to oxygen consumption
(VO2) provides the composition of the oxidized substrate. It is unclear whether
Box 2. Harris–Benedict equation
Men:
basal metabolic expenditure (BEE)=
66+(13.7) (weight kg)+ (5) (height cm)� (6.8) (age years)
Women:
BEE=
655+(9.6) (weight kg)+(1.7) (height cm)� (4.7) (age years)
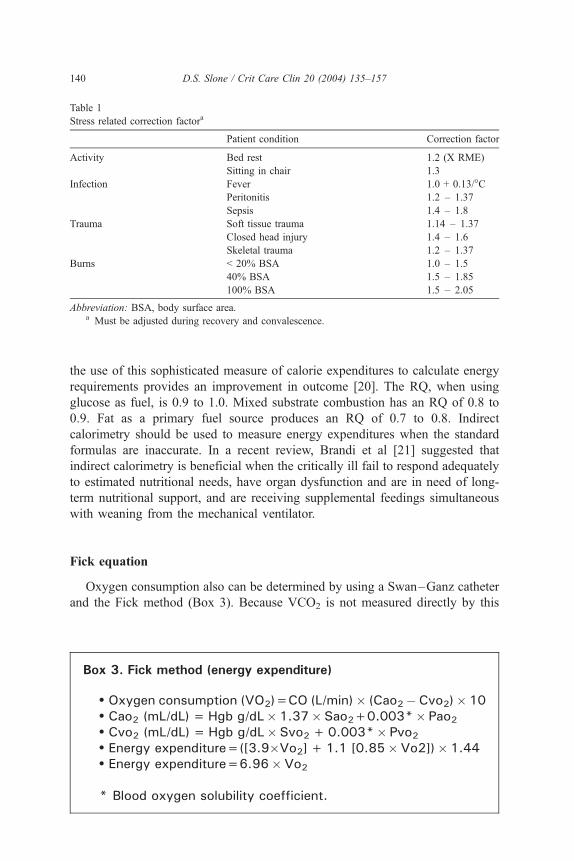
Table 1
Stress related correction factora
Patient condition Correction factor
Activity Bed rest 1.2 (X RME)
Sitting in chair 1.3
Infection Fever 1.0 + 0.13/�CPeritonitis 1.2 – 1.37
Sepsis 1.4 – 1.8
Trauma Soft tissue trauma 1.14 – 1.37
Closed head injury 1.4 – 1.6
Skeletal trauma 1.2 – 1.37
Burns < 20% BSA 1.0 – 1.5
40% BSA 1.5 – 1.85
100% BSA 1.5 – 2.05
Abbreviation: BSA, body surface area.a Must be adjusted during recovery and convalescence.
D.S. Slone / Crit Care Clin 20 (2004) 135–157140
the use of this sophisticated measure of calorie expenditures to calculate energy
requirements provides an improvement in outcome [20]. The RQ, when using
glucose as fuel, is 0.9 to 1.0. Mixed substrate combustion has an RQ of 0.8 to
0.9. Fat as a primary fuel source produces an RQ of 0.7 to 0.8. Indirect
calorimetry should be used to measure energy expenditures when the standard
formulas are inaccurate. In a recent review, Brandi et al [21] suggested that
indirect calorimetry is beneficial when the critically ill fail to respond adequately
to estimated nutritional needs, have organ dysfunction and are in need of long-
term nutritional support, and are receiving supplemental feedings simultaneous
with weaning from the mechanical ventilator.
Fick equation
Oxygen consumption also can be determined by using a Swan–Ganz catheter
and the Fick method (Box 3). Because VCO2 is not measured directly by this
Box 3. Fick method (energy expenditure)
Oxygen consumption (VO2)=CO (L/min)� (Cao2�Cvo2)� 10 Cao2 (mL/dL)=Hgb g/dL� 1.37� Sao2+0.003*� Pao2 Cvo2 (mL/dL)=Hgb g/dL� Svo2+0.003*� Pvo2 Energy expenditure=([3.9�Vo2]+1.1 [0.85�Vo2])� 1.44 Energy expenditure=6.96�Vo2
* Blood oxygen solubility coefficient.
D.S. Slone / Crit Care Clin 20 (2004) 135–157 141
method, a standard RQ of 0.85 is assumed. By using the Fick equation to compute
VO2, and using RQ to compute the VCO2, this equation seems to correlate well
with the indirect calorimetry and Harris–Benedict equation [22].
Patient selection
The patient who is a candidate for nutritional support is the healthy uninjured
patient who has been without nutrition for 5 to 7 days. The trauma patient with an
Injury Severity Score (ISS) of greater than 15, burn victim with a Body Surface
Area (BSA) burn of greater than 20%, the patient with severe peritonitis or
septicemia are all hypermetabolic and at risk for malnutrition. The only other
patient who benefits from nutritional support is the malnourished patient who has
by definition lost greater than 10% of the usual body weight. No other patient
groups have been shown to benefit from adjuvant nutritional therapy. This has been
studied carefully and reported by Buzby et al in 1991, among others. The
participants were 395 malnourished patients known as the Veterans Affairs Total
Parenteral Nutrition Cooperative Study Group [23]. The purpose of the study was
to examine the efficacy of perioperative total parenteral nutrition (TPN). In all
instances of poor patient selection, the risk of using TPNmay outweigh the benefits
[24]. The only applicability to the trauma patient population is the frequency with
which they can develop malnutrition. Patient selection may be one of the reasons
well-designed, reproducible nutritional studies with significant outcome differ-
ences are so difficult to develop. The major point of awareness is the importance of
patient selection in the nutritional support for the trauma patient population. It may
be better to wait 1 extra day for adjuvant enteral therapy than the start TPN on the
third or fourth day after injury. The risk of TPN may outweigh the significance of
the benefit and always must be considered in the trauma patient population.
Caloric/energy requirement
The goal of surgical nutrition in the critically injured patient is maintenance,
not repletion. Overfeeding results in lipogenesis and results in a large increase in
carbon dioxide production. It should be suspected when the clinically measured
RQ is 1.1 or greater. The increased CO2 production associated with overfeeding
requires an increase in minute ventilation or respiratory acidosis occurs. Both of
these complications are undesirable in the trauma patient. The clinician should
consider glucose intolerance if the provided nutrition is based on measured
energy expenditures (MEE), but the patient retains an elevated RQ, attendant
respiratory acidosis, or high minute ventilation. The glucose use rate (5 mg/kg per
minute) may have been exceeded. Some patients may have pulmonary physiol-
ogy that does not allow them to handle normal CO2 production. In this situation,
manipulation of the ratio of lipids to carbohydrates may prove to be beneficial.
Lipid calories should not exceed 60% of energy requirements. Dextrose mono-

D.S. Slone / Crit Care Clin 20 (2004) 135–157142
hydrate in TPN provides 14.24 kJ per gram. Ten percent lipid emulsion provides
5.02 kJ/mL. Twenty percent lipid emulsion provides 8.79 kJ/mL. Lipids are iso-
osmotic, calorie dense, and useful during glucose intolerance. Unfortunately, their
use has been associated with a higher risk of infection [25]. This risk is not huge,
but it is concerning. The minimum calorie requirement that should be delivered as
lipids to prevent fatty acid deficiency is 5% [26]. There has not been an evidence-
based answer concerning the maximal lipid intake or ideal lipid ratio. Serum
triglyceride levels must be maintained within a normal range while the patient
receives intralipids.
Protein requirements
In a healthy patient without protein intake, there is an obligatory loss of 20 to
30 g of protein per day. In hypermetabolic critical trauma patients, protein
degradation and synthesis typically increase in concert with a net loss. Patients
lose up to 1% of their body protein per day. For this reason, 1.5 to 2.0 g of protein
per kilogram of ideal body weight per day is recommended [27]. There is little
doubt that the new mode of postlaparotomy open abdominal wound, increasing
entercutaneous fistulae formation, systemic inflammatory response syndrome
(SIRS), and new modes of mechanical ventilation have an impact on the insensible
protein losses in critically injured patients. Studies of graded protein delivery
demonstrated no significant benefit when providing the trauma patient with more
than 1.5 g/kg ideal body weight [12]. There are no published data suggesting
improved survival for adults with protein supplements that exceed this rate.
Alexander [28], however, showed that children with severe burns had a significant
reduction inmortality when proteins were supplemented with more than 1.5 g/kg of
ideal body weight.
Amino acids
The need for certain amino acids during a stressful critical illness has been
demonstrated by several clinical studies [29]. Glutamine is the most abundant
amino acid in the body, but it shows deficits during episodes of severe stress
(therefore considered semiessential). Glutamine production is up-regulated signifi-
cantly during times of stress, trauma, and sepsis. It serves as a nitrogen donor for
ammonia synthesis in the kidney to increase the excretion of acid. It acts as a
primary fuel for enterocytes and immunologic cells. It is also important in glu-
tathione synthesis [30]. Arginine is another semiessential amino acid that contrib-
utes to the immune system and metabolic function. Branched-chain amino acids
(BCAA) are considered essential and the primary energy source for muscle [31].
There has not been any clinically proven benefit to supplementation with BCAA
[32]. One theoretical nutritional use for BCAA is the reduction of the level of false
transmitters that are caused by aromatic amino acids [33].

D.S. Slone / Crit Care Clin 20 (2004) 135–157 143
Glucose/insulin
The association between hyperglycemia and infectious complications is as-
suming greater importance in the critically ill. Hyperglycemia and insulin re-
sistance are common in critically ill patients, even if patients were not previously
diabetic. The normalization of blood glucose levels with intensive insulin therapy
improves the prognosis of such patients as seen in a large ICU study reported
by Van Den Berghe et al [34]. The use of insulin to maintain blood glucose at
a level that did not exceed 110 mg/dL substantially reduced mortality in this ICU.
The patient group included only 8% (n = 68) major trauma and burn patients.
The applicability of these data to trauma patients has not been determined.
Electrolyte requirements
Phosphorus is a ubiquitous mineral, and approximately 70% to 90% of adult
intake is absorbed [35]. The total stores are 500 to 800 g. It is located mostly
(80%) in bones and teeth. Muscle contains 9% of phosphorus. A small per-
centage is available for synthesis of intracellular energy compounds (ATP). It is
also useful in formation of 2,3 diphosphoglycerate (2,3 DPG) [36]. There are so
many phosphorus-dependent metabolic pathways that maintaining phosphorus
homeostasis is critical for normal body function. Hypophosphatemia can lead
to significant respiratory failure, as it is a major energy component for the
diaphragm. Excessive nutritional support can cause hypophosphatemia, com-
monly known as refeeding syndrome, which will be discussed later.
Trace elements
Copper has multiple effects on immune response, including both T and B cell
defects. Interactions with iron often occur, and low copper may be associated with
reduced nutritional intake. Both anemia and immune suppression are observed in
patients with copper deficiencies. Decreasing copper causes a significant reduc-
tion in proliferative response to reduced interleukin (IL)-2 receptor secretion [37].
The liver stores several vitamins and micronutrients. As liver failure progresses,
its ability to store nutrients is impaired. There is malabsorption of vitamins A,
E, and K because of steatorrhea. Vitamin D levels may be reduced in the blood,
in the presence of impaired renal function. Niacin, folate, and vitamin B12 also
may be deficient in a patient with a history of alcohol abuse. Iron deficiency
anemia may be found in patients with a history of gastrointestinal (GI) bleed.
Bombesin is a tetradecapeptide analogous to mammalian gastrin-releasing
peptide, which stimulates the release of several other GI tract hormones. It has
been shown to increase the levels of intestinal IgA. Bombesin given three times per
day has completely reversed the negative effect of TPN on respiratory tract
immunity and gut associated lymphoid tissue (GALT) [38].

D.S. Slone / Crit Care Clin 20 (2004) 135–157144
Metabolic responses
The metabolic responses to injury differ significantly from those of starvation.
During starvation, the body attempts to compensate by decreasing its metabolic
rate. Glycogen stores are depleted in the first 24 hours, and fat becomes the chief
energy source. Proteins are conserved until late in the process. In most trauma
patients, numerous metabolic processes join to produce a hypermetabolic state
characterized by a rapid and significant negative nitrogen balance. The net result of
protein tissue and muscle mass loss is two to three times that lost during starvation.
Lipolysis is functionally reduced to the progressive elevation in insulin levels and
relative glucose intolerance. This causes high levels of circulating glucose, which is
not useful energy for the traumatized patient. Substrate delivery in the trauma and
burn patient becomes key to preventing lipolysis and protein degradation. The
overprovision of calories can cause the following hazards: increased metabolic
rate, increased oxygen consumption, hyperglycemia, fluid imbalance and de-
hydration caused by hyperosmotic load, fatty infiltrated liver, fluid overload,
immunosuppression, prolonged ventilator dependence caused by increased CO2
production, and electrolyte imbalance. Using graded calorie infusions in patients
with burns, Burke [39] found the level of calorie input, which demonstrated
increased rates of CO2 production and hepatic fat deposition when exceeded. The
ideal level that he identified was 104.67 kJ/kg of ideal body weight per day.
Immunonutrition
The suppressive effect of nutrient imbalance on the immune system is seen
most readily in malnutrition [40]. Nutritional deficits produce significant atrophy
of lymphoid organs and impaired function leading to infections [41,42]. Addi-
tionally, studies suggest that overnutrition, particularly excessive fat intake, can
cause immunosuppression [43]. Because microbes have a direct effect on di-
gestion, these relationships are linked tightly in a mutually interactive fashion
through the function of the GI immune system. Advances in the field of im-
munology over the past 20 years have led to a better understanding of the role
nutrition plays in the immune status of injured patients. It has been apparent that
certain specific nutrients might exert pharmacologic immune-enhancing effects
upon individuals independent of routine nonenergy protein intake. These include
arginine, glutamine, nucleotides, and omega-3 fatty acids.
Arginine
Arginine promotes normal T-cell function and helper T-cell levels. It also
enhances delayed type hypersensitivity and lymphocyte blastogenesis. It has been
shown to stimulate macrophages and natural killer cell function [44]. It also plays a
significant role in wound healing [45]. Most studies have evaluated arginine in
conjunction with n–3 polyunsaturated fatty acids (PUFA) and dietary nucleotides.

Linoleic acid
Linoleic acid is a w–6 PUFA that is a major constituent of cell membranes and a
precursor of prostanoid and leukotriene synthesis. It is considered an essential
amino acid. Deficiency causes dermatitis. These deficiencies can be prevented by
the minimal free fatty acid (FFA) requirement, which is 5% of total calorie intake.
Its role in immune enhancement and as a substrate for the synthesis of prostanoids
and leukotrienes is gaining acceptance quickly. There are no parenteral forms of
linoleic acid available. Enteral immune-enhancing formulas containing w–3 PUFAare commercially available.
Glutamine
Glutamine is an oxidative fuel for rapidly replicating cells, including GI mu-
cosal cells, lymphocytes, and macrophages. It is also a nitrogen shuttle and
precursor of the antioxidant glutathione. During stressed states, the body requires
an exogenous source of glutamine to avoid catabolism and muscle glutamine
depletion [46,47].
Nucleotides
Nucleotides enhance the replication of rapidly growing cells to include im-
mune cells and GI mucosal cells [48], In addition, Good et al [49] were first to
recognize the association between micronutrient deficiencies of vitamins and
trace elements with a depressed immune response. Specifically, Good proposed
that a certain key elemental deficiency, zinc, might be the cause. Primary zinc
deficiency causes intractable and even fatal infections. Zinc is essential, as it
is required for the biologic activity of thymic hormone needed for the matu-
ration of T cells [50]. Copper has multiple effects on immunity, including T- and
B-cell function. Other trace elements included in some of the diets were sele-
nium and taurine, with known antioxidant properties [51]. Antioxidants have
been shown in vitro to modulate the activity of various immune cells such as the
T lymphocyte, endothelial cell, and monocyte/macrophage. Selenium deficiency
also reduces antibody responses.
There have been numerous studies of the clinical, immunologic, nutritional,
and biochemical effects of arginine, glutamine, w–3 FFA and nucleotides. There
are over 400 citations in the medical and biochemical literature. There were three
meta-analyses [52–54] that determined immune enhancement showed clinical
results such as decreased infection. There was no significant change in mortality
resulting from dietary immunomodulation. Moore et al [55] published the results
of a prospective randomized multi-center trial using isocaloric formulas on
primarily traumatically injured critical care patients. The patients were fed
immediately and received the diet for a week. There were increases in immuno-
logic responses in the study group, with significantly fewer intra-abdominal
abscesses and fewer multiple organ failures. This trial demonstrated similar
findings with most of the many other immunomodulation studies. It showed that
D.S. Slone / Crit Care Clin 20 (2004) 135–157 145

D.S. Slone / Crit Care Clin 20 (2004) 135–157146
there were some clinical improvements in outcome but no significant reductions in
mortality. It also can be noted that none of the centers studied any of the
components separately. A clinical trial was presented from Seattle, using a trauma
patient population that showed a significant increase in the development of adult
respiratory distress syndrome (ARDS) among those fed Impact (Novartis, Basel,
Switzerland; a commercially developed ‘‘immune-enhancing’’ formula) [56]. This
balance between improved immunity and heightened inflammation could make
the overall response to these enhancing diet harmful. It is potentially unpredictable
in different clinical settings. The danger of extrapolation between disparate groups
is prevalent. This was a very small study and was powered higher in the original
design. It raises interesting concerns about the routine use of immune-enhanced
formulas without further evaluation.
Twenty-two randomized trials (2419 patients) compared the use of various
immune-enhancing formulas. When the data are aggregated, there is no mortality
advantage, although many of the study patients had a reduction in infectious
complications. All studies looked at the additives in combination, making it hard to
evaluate any single component. Animal studies suggested that arginine was dose-
dependent and varied with the timing of administration [57]. Immunonutrition was
effective in elective surgical patients but had no affect on critical care patients in
general. These supplements showed no significant affect on infectious complica-
tions, length of ICU stay, or duration of mechanical ventilation. Immunonutrition
was associated only with a reduction in total hospital length of stay. There were
suggestions of methodologic weakness in some primary studies, sample size
problems, and even some evidence (in one small study) that immune-enhanced
diets may be associated with an increased mortality in critically injured patients.
One wonders about the merit of immunonutrition, it is known today. Further
research needs to define the underlying mechanism by which immunonutrition
may be harmful, to identify which ingredients have a clinical affect, and which
patients are associated with an outcome benefit. Once this study design is
developed, it needs to be applied to trauma patients to evaluate the effect of
immunonutrition on the critically injured patient.
Timing
It has not been established clearly when to initiate nutritional support. Extensive
data-based literature suggests that nutrition will attenuate the hypermetabolic
response to injury, reduce the rate of infectious complications, and maintain the
integrity of the intestinal mucosa along with its immunologic defenses [58,59].
Obviously, a healthy young well-nourished individual with no significant injury
can go several days without nutritional support. This will cause minimal effect on
the patient’s mortality or morbidity. Any variation, such as the infliction of a major
injury, advanced age, or the presence of comorbidities can alter the patient’s
requirement for nutritional support drastically. Although many authors have
defined the patient population requiring this support adequately, the optimal timing

D.S. Slone / Crit Care Clin 20 (2004) 135–157 147
has not been elucidated. The benefits of early feeding in hypermetabolic patients
have not been studied adequately. The heterogeneity of the hypermetabolic group
of patients makes the study designs problematic and flawed. The largest study
group of trauma patients reported by Moore and Jones [60] demonstrated a
decrease in septic complications in patients who received early jejunal feedings,
compared with a control group who received TPN. Because of the mixed route of
administration seen in this study group, one cannot be certain that the significant
difference in outcome was attributable to the early timing of the feeds, the enteral
route of nutrition, or some other unidentified factor. Moore et al were credited with
the first clinical studies that demonstrated a benefit with early enteral nutrition. A
subsequent clinical trial by the same authors showed a reduction in pneumonia and
intra-abdominal abscess formation [61]. A meta-analysis was published by Moore
to clarify the findings from multiple clinical trials [62]. Because of the paucity
of clinical trials to base practice guidelines, a summary report from a panel of
experts sponsored by the National Institutes of Health, The American Society for
Parenteral and Enteral Nutrition, and the American Society for Clinical Nutrition
reviewed all published literature concerning the benefits of perioperative nutrition
[59]. TPN was found to decrease complications in malnourished populations only.
A final statement was made that ‘‘nutritional support should be initiated in patients
who are not expected to resume oral feeding for 7 to 10 days.’’ The panel
also called for more prospective controlled trials with revised designs that would
allow the question of whether the timing of nutritional support affects outcome to
be explored.
One prudent practice is to withhold nutritional support until after achieving
hemodynamic stability even though hypermetabolic state may be present imme-
diately. Shock has been shown clinically to reduce mesenteric perfusion, and it is
presumed that early feeding during the shock state can contribute to mesenteric
ischemia, infarction, and perforation [63]. Furthermore, metabolic derangements
such as glucose intolerance resulting in hyperglycemia and osmotic diuresis can
complicate further an already compromised critically injured patient. Even without
evidence-based literature specific to the timing of nutritional support, most
clinicians agree that early feeding in the severely injured patient is favorable.
Route of administration
Before 1968 [64], the GI tract was the only route available for nutrition. Dudrick
et al revolutionized the management of patients dying from the inability to take
enteral nutrition with a description of TPN. This became the preferred route of
nutrition in the 1970s, because it was relatively safe, convenient, and widely
available in spite of the condition of the digestive tract. In the 1980s, it was
determined that there were compelling advantages to enteral nutrition, including
the improved usefulness of the nutrients with the first pass through the liver [65]. It
was advanced more slowly than TPN, but the nitrogen losses were found to be less.
GI feeding did not cause the glucose intolerance seen in TPN, was felt to be

D.S. Slone / Crit Care Clin 20 (2004) 135–157148
protective against significant gut atrophy, attenuated the stress response better,
maintained immunocompetence, and preserved the gut flora [66–68]. Thus, by the
end of the 1980s, there was renewed interest in enteral feeding. After being the first
to establish the importance of early feeding for trauma patients, Moore et al were
credited with the first randomized controlled trial in the trauma population
designed to evaluate the advantages offered by enteral nutrition compared with
TPN [62]. Kudsk et al confirmed these observations at Presley Memorial Trauma
Center in Memphis, Tennessee [69]. Investigators argue that enteral nutrition
maintains the integrity of the GI tract and has fewer associated infectious
complications compared with TPN. The problem with these two similar class I
studies was the size, which may have been suboptimal [70]. A meta-analysis done
by Moore and Feliciano [63] found support for early total enteral nutrition (TEN)
versus TPN in the trauma patient but did not find defined support in the nontrauma
population. Just as many trials showed no difference between TPN and enteral
nutrition. Most of these trials were not done on trauma patients, but Pacelli et al
demonstrated that enteral feeding following major abdominal surgery failed to
reduce postoperative complications and mortality when compared with parenteral
nutrition [71]. Was the design flaw, which provided patients in the enteral feeding
arm of the study with TPN during the periods of time when the patient would not
tolerate enteral feeds, the reason for the disparity between these results and the
findings that Moore published when evaluating the trauma patient population?
Many of the comparative trials were characterizedwith inadequate patient selection
(not restricted to patients who required nutritional support), small study size, and
insufficient definitions of complications. Lipman did a thorough review of the
literature as it concerned the route of delivery of nutrition [72]. He evaluated the
common arguments that enteral nutrition is better because it is cheaper, safer, more
physiologic, promotes better GI function, prevents bacterial translocation, and
improves outcome. This comparison of enteral nutrition and TPN on gut–barrier
function and other clinical outcomes did not demonstrate an advantage in patients
with abdominal trauma, except in the reduction of sepsis. This inconsistency
undoubtedly highlights the shortcomings of meta-analyses when used to assess
trials of different quality involving heterogeneous patient groups and diverse
endpoints. If the risks of enteral nutrition were equal to TPN, then enteral nutrition
is better because of its reduction of cost alone. To take a current look at the old
controversial issue of TPN versus TEN, a common theme should become apparent
when initiating support. TPN should be reserved for those patients whose GI tract
will remain unavailable for a prolonged period, resulting in eventual malnutrition.
There is some concern that most of the complications associated with TPN are
caused by the lipid component. Battistella et al suggest lipids be withheld from the
TPN of trauma patients able to tolerate at least 10% of their nutrition enterally. This
group received fewer calories, but no intravenous lipids. They had fewer infections,
shorter LOS, and fewer days on a ventilator [72]. Cerra found no difference in the
potential for multiple organ failure in patients receiving enteral feeds versus TPN
[73]. A logical resolution to the conflict of TPN and TEN is that if the gut is
functional, use it. One should not have a slavish commitment to enteral feeds in the
D.S. Slone / Crit Care Clin 20 (2004) 135–157 149
patient who does not tolerate it. It even has been suggested that the increase in
splanchnic blood flow induced by enteral feeds may be detrimental to the critically
injured patient. The time has come for the TEN versus TPN debate to be laid to rest.
Patients with questionable GI function should be fed using a combination of TEN
and TPN. The enteral feed should be increased or decreased according to tolerance,
with TPN adjusted accordingly. If the patient is going back and forth, with
procedures requiring intermittent deferment of enteral feeds, then TPN should be
used preferentially. Although TPN has infectious implications and is associated
with GI atrophy, it is immediately available and does not require much time and
tolerance to reach full support. Border et al found less sepsis in patients who
received at least 40% of their nutrition by enteral routes [74].
The debate about the route continues to raise controversy, but flawless trials
demonstrating consistent benefits to major outcomes have been rare. There is a
general lack of evidence-based guidelines involving the decisions related to
nutritional timing and route.
Feeding access
The benefits of enteral nutrition in trauma patients are recognized widely. The
optimal method of enteral access in severely injured patients is not established.
Feeding jejunostomy generally is considered to be a safe method of establishing
enteral access in elective surgical patients, but the safety in trauma patients is less
certain. Holmes et al [75] retrospectively evaluated the complication rate of the
jejunostomy feeding tube in trauma patients and found it to be 10%. Although the
value of enteral feeding has been investigated extensively, the safety of feeding
jejunostomy as an adjunct to trauma celiotomy has received less evaluative
investigation. Many centers have become quite discouraged with the use of this
type of access, although this may be premature. With appropriate patient se-
lection, judicious tube feeding regimens, and attention to technical details, the
jejunostomy related complications could be controlled. Alternative enteral ac-
cess techniques should be considered in this population, however. Other such
access can be provided with nasal jejunal feeding tubes and needle catheter
jejunostomy. Nasoduodenal (postpyloric) feeding tubes may be placed easily and
can provide a safer method than surgical jejunal access for feeding the severely
injured patient [76].
Complications
Overfeeding
Overfeeding critically ill patients can cause metabolic complications that are
serious and sometimes fatal. Patients who are very small, very large, or very old are
particularly vulnerable to overfeeding.

Azotemia
Azotemia occurs when the rate of urea production exceeds the excretion. The
rate of synthesis of urea in the liver depends on the protein intake and endogenous
catabolism. Inflammation and infection activate cytokines (eg, IL-1 and IL-6) that
accelerate muscle breakdown. Furthermore, adrenal hormones and catecholamines
such as glucagons, cortisol, and epinephrine, which are elevated after traumatic
injury, stimulate muscle catabolism. Accelerated proteolysis in critically ill and
injured patients, combined with overzealous protein delivery, sets the stage for
azotemia [77].
Fat overload syndrome
Life-threatening complications are rare but can occur because of excessive
amounts of soybean oil emulsions [78]. Respiratory distress, coagulopathies, and
abnormal liver function tests are the primary manifestations of fat overload. Less
commonly reported abnormalities are acute renal failure, fever, rash, depressed
platelet counts, low hemoglobin concentration, hypertension, and tachycardia [79].
Patients who have sustained injury have stimulated cytokine production and
depressed lipoprotein lipase activity [80]. Lipase activity probably further stimu-
lates the cytokine response.
Hypertriglyceridemia
Overfeeding carbohydrates may lead to hypertriglyceridemia within a matter of
days [81]. Infusing lipid in excess of 2 gm/kg per day has been associated with
hypertriglyceridemia in patients receiving propofol, a lipid-based drug used for
sedation [82]. It is not known whether propofol exerts an effect that is independent
of the effect of the lipid carrier. Propofol decreases tissue oxidation and carbon
dioxide production [83].
Hepatic steatosis
More than one mechanism may be responsible for the accumulation of hepatic
fat. Hepatic steatosis during overfeeding derives from exogenous lipid or redistri-
bution of fat from adipose tissue.
Hypercapnia
Carbon dioxide is formed when intracellular substrates are broken down to
produce ATP. With overfeeding, the ratio of carbohydrate to fat in substrate
oxidation continues to increase over time. When and how much fat oxidation is
displaced by carbohydrate oxidation may depend on the patient’s ability to store
glycogen. Eventually, overfeeding will lead to more carbon dioxide production
over time [84]. Plasma triglyceride is elevated in patients with infectious illness,
particularly gram-negative sepsis. This is primarily caused by the effect of tumor
necrosis factor, which decreases the activity of lipoprotein lipase [85].
D.S. Slone / Crit Care Clin 20 (2004) 135–157150

Table 2
Complications of central venous catheterization
Pneumothorax Catheter occlusion Hydrothorax/hydromediastinum
Air embolism Thoracic duct injury Catheter embolus
Improper location Hemomediastinum Brachial plexus injury
Venous thrombosis Arterial puncture Local hematoma/bleeding
Failure to cannulate Hemothorax Subcutaneous emphysema
Catheter sepsis Local infection Bacteremia
D.S. Slone / Crit Care Clin 20 (2004) 135–157 151
Metabolic acidosis
Metabolic acidosis has been reported recently with excessive protein intake
from an enteral formula [86].
Refeeding syndrome
Initiation of nutrition support to patients with severely depleted nutrient stores is
associated with clinically significant shifts in phosphorus, magnesium, and
potassium from extracellular to intracellular spaces [87]. In the fed state, ATP
production, glycogenesis, and protein anabolism place extra demands on the
supply of these important minerals, whose transport into cells is stimulated by
insulin [88]. Additionally, starvation causes a catabolic release of intracellular
phosphate, which is excreted in the urine. Total body stores of intracellular
electrolytes slowly are depleted, because these constituents of the body cell mass
are lost slowly during catabolism. Refeeding and the early stages of overfeeding are
both cardiovascular demands. Chronically malnourished patients whose cardiac
muscle is depleted are not prepared to deal with the circulatory demands caused by
the initiation of aggressive nutrition support [89]. Approaches for the prevention
and management of refeeding syndrome (also called nutritional recovery syn-
drome) include supplement with vitamins and minerals as soon as possible.
Consider thiamin, folate, B-6, and zinc [90] supplementation. Clinicians may have
to reach the nutritional goals slowly, with close monitoring of cardiac and mineral
status for acute changes. The refeeding syndrome is a complication of nutritional
support that potentially causes considerable morbidity and mortality associated
with sodium retention and expansion of the extracellular space, leading to weight
gain [91].
Central line complications
The complications seen in central venous catheterization associated with TPN
are found in Table 2.
Special problems
Head injuries
This patient profile can portray a significant hypermetabolic/catabolic response.
Sedation, paralytics, and muscle relaxants modulate this. Energy requirements in

D.S. Slone / Crit Care Clin 20 (2004) 135–157152
the paralyzed or comatose patient are quite difficult to estimate. Indirect calorime-
try or MEE calculations are useful in these patients. Early nutritional support can
be achieved, but special attention must be made to prevent hyperglycemia, which
has been shown to exacerbate ischemic brain injury.
Burn injury
Major burns are the most hypermetabolic/hypercatabolic injuries and can
double the MEE. The profound immunosuppression seen in these patients has
prompted a great deal of work on nutritional approaches to immune-enhancement.
Burn patients require the most calories, the most proteins, and vitamin C, and high
doses of vitamin E.
Obese trauma patients
Nutritional support in critically ill or injured obese patients can pose unique
problems for clinicians. Many of these patients have chronic diseases related to
their obesity such as diabetes, degenerative joint disease, hypertension, respiratory
abnormalities, hyperlipidemia, and hepatobiliary disease. They are more likely
than their nonobese counterparts to develop complications such as nosocomial
infections, wound dehiscence, and cardiorespiratory complications [92–94]. The
MEE of obese patients is widely variable, and their energy needs are difficult to
predict accurately [95]. As a result, nutritional intake very easily could be given in
excess, leading to the complications of overfeeding. This has become a recognized
problem, and alternative hypocaloric, high-protein feeding has been developed for
the critically ill obese patient [96,97]. Dickerson, et al [98] reported results of a
retrospective trial examining 40 obese trauma patients who received enteral tube
feedings. They examined the nutrition and clinical outcomes of critically ill obese
patients who received eucaloric or hypocaloric enteral feeds. Nitrogen balance and
protein responses were similar between groups. Clinical outcomes favored the
hypocaloric group, with a significantly lower number of ICU days, fewer days of
antibiotic therapy, and fewer days on the ventilator. A randomized double blind trial
is warranted to confirm the clinical outcome of the superiority of hypocaloric
enteral feeding over eucaloric enteral feeding in critically ill, obese patients.
Summary
The understanding of the importance of nutrition, particularly in the critically ill
patient, is based on the known physiologic consequences of malnutrition. It
includes respiratory muscle function, cardiac function, the coagulation cascade
balance, electrolyte and hormonal balance, and renal function. Nutrition affects
emotional and behavioral responses, functional recovery, and the overall cost of
health care. The need to identify and treat the malnourished or potentially

D.S. Slone / Crit Care Clin 20 (2004) 135–157 153
malnourished patient is a critical aspect of patient management. Much is known of
catabolic and hypermetabolic state caused by trauma and burns. The response to
injury needs to be mediated. There is much to learn about the intervention of that
response through adjuvant nutritional therapy.
References
[1] Bistrian BR, Blackburn GL, Hallowell E, Heddle R. Protein status of general surgical patients.
JAMA 1974;230(6):858–60.
[2] Hill GL, Blackett RL, Pickford I, Burkinshaw L, Young GA, Warren JV, et al. Malnutrition in
surgical patients: an unrecognised problem. Lancet 1977;1:689–92.
[3] Smith LC, Mullen JL. Nutritional assessment and indications for nutritional support. Surg Clin
North Am 1991;71:449–57.
[4] Abbasi A. Nutrition. In: Duthie EH, editor. Practice of geriatrics. 3rd edition. New York: WB
Saunders Company; 1998. p. 145–58.
[5] McClave SA, Snider HL. Understanding the metabolic response to critical illness: factors that
cause patients to deviate from the accepted pattern of hypermetabolism. New Horiz 1994;2:
139–46.
[6] Studley HO. Percentage of weight loss: a basic indicator of surgical risk. JAMA 1999;106:
2013–9.
[7] Master AM, Lasser RP, Beckman G. Tables of average weight and height of Americans aged
65–94. JAMA 1960;172:658–62.
[8] Baker JP, Detsky AS, Wesson DE. Nutritional assessment: a comparison of clinical judgment
and objective measurements. N Engl J Med 1982;306:969–72.
[9] Svendsen OL, Haarbo J, Heitmann BL, Gotfredsen A, Christiansen C. Measurement of body
fat in elderly subjects. Am J Clin Nutr 1991;53(5):1117–23.
[10] Lohman TG. Skinfolds and body density and their relation to body fatness. Hum Biol 1981;
53:181–225.
[11] Gibbs J, Cull W, Henderson W, Daley J, Hur K, Khuri SF. Preoperative serum albumin level as
a predictor of operative mortality and morbidity. Arch Surg 1999;134:36–42.
[12] Mullen JL, Buzby GP, Waldman MT. Prediction of operative morbidity by preoperative nutri-
tional assessment. Surg Forum 1979;30:80–2.
[13] Buzby GP, Mullen JP, Matthews DC, et al. Prognostic nutritional index in gastrointestinal
surgery. Am J Surg 1980;139:160–7.
[14] Twomey P, Ziegler D, Rombeau JL. Utilization of skin testing in nutritional assessment: a criti-
cal review. JPEN J Parenter Enteral Nutr 1982;6:50–7.
[15] Ishibashi N, Plank L, Sando K, Hill GL. Optimal protein requirements during the first 2 weeks
after the onset of critical illness. Crit Care Med 1998;26(9):1529–35.
[16] Harris JA, Benedict FG. Biometric Studies of Basal Metabolism in Man. Washington, DC:
Carnegie Institute; 1919.
[17] Daly JM, Heymsfield SB, Head CA, Harvey LP, Nixon DW, Katzeff H, et al. Human energy
requirements: Overestimation by widely used prediction equation. Am J Clin Nutr 1985;42(6):
1170–4.
[18] Makk LJ, McClave SA, Creech PW, Johnson DR, Short AF, Whitlow NL, et al. Clinical
application of the metabolic cart to the delivery of total parenteral nutrition. Crit Care Med
1990;18(12):1320–7.
[19] Weir JB. New methods for calculating metabolic rate with special reference to protein metabo-
lism. J Physiol 1949;109:1–9.
[20] Kinney J. Indirect calorimetry: the search for clinical relevance. Nutr Clin Pract 1992;7:203–6.
[21] Brandi LS, Bertolini R, Calafa M. Indirect calorimetry in critically ill patients: clinical applica-
tions and practical advice. Nutrition 1997;13:349.

D.S. Slone / Crit Care Clin 20 (2004) 135–157154
[22] Cobean RA, Gentilello LM, Parker A, Jurkovich GJ, Maier RV. Nutritional assessment using
a pulmonary artery catheter. J Trauma 1992;33(3):452–6.
[23] Veterans Affairs Total Parenteral Nutrition Cooperative Study Group. Perioperative total paren-
teral nutrition in surgical patients. N Engl J Med 1991;325:525–32.
[24] Buzby GP, Blouin G, Colling CL. Perioperative parenteral nutrition in surgical patients. N Engl
J Med 1991;325:525–31.
[25] Pomposelli JJ, Bistrian BR. Is total parenteral nutrition immunosuppressive? New Horiz 1994;
2:224–9.
[26] Goodgame JT, Lowry SF, Brennan MF. Essential fatty acid deficiency in total parenteral nu-
trition: time course of development and suggestions for therapy. Surgery 1978;84:271.
[27] Rombeau JL, Rolandelli RH, Wilmore DW. Nutritional support. In: Wilmore DW, Cheung LY,
Harken AJ, Holcroft JW, Meakins JL, editors. Scientific American surgery. New York: Scientific
American; 1999. p. 10–5.
[28] Alexander JW, MacMillan BG, Stinnett JD, Ogle CK, Bozian RC, Fischer JE, et al. Bene-
ficial effects of aggressive protein feeding in severely burned children. Ann Surg 1980;192:
505–17.
[29] Garlick PJ, Wernerman J. Protein metabolism in injury. In: Cooper GJ, Dudley HAF, Gann DS,
Little RA, Maynard RL, editors. Scientific foundation of trauma. Oxford (UK): Butterworth
Heineman; 1997. p. 690–728.
[30] Souba WW. Glutamine: a key substrate for the splanchnic bed. Annu Rev Nutr 1991;11:285.
[31] Freund HR, Hanani M. The metabolic role of branched-chain amino acids. Nutrition 2002;18:
287–8.
[32] Meyenfeld MF, Soeters PB, Vente JP. Effect of branched-chain amino acid enrichment of total
parenteral nutrition on nitrogen sparing and clinical outcome of sepsis and trauma. Br J Surg
1990;77:924–9.
[33] Naylor CD, O’Rourke K, Detsky AS, Baker JP. Parenteral nutrition with BCAA in hepatic
encephalopathy: a meta-analysis. Gastroenterology 1989;97:1033.
[34] Van Den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive
insulin therapy in critically ill patients. N Engl J Med 2001;345(19):1359–67.
[35] Peppers MP, Geheb M, Desai T. Hypophosphatemia and hyperphosphatemia. Crit Care Clin
1991;7(1):201–14.
[36] Knochel JP. The pathophysiology and clinical characteristics of severe hypophosphatemia. Arch
Intern Med 1977;137:203–20.
[37] Kelley DS, Daudu PA, Taylor PC, Mackey BE, Turnlund JR. Effects of low copper diets on
human immune response. Am J Clin Nutr 1995;62:412.
[38] Li J, Kudsk KA, Hamidian M, Gocinski BL. Bombesin affects mucosal immunity and gut-
associated lymphoid tissue in IV-fed mice. Arch Surg 1995;130:1164.
[39] Burke JF, Wolfe RR, Mullany CJ, Mathews DE, Bier DM. Glucose requirements following
burn injury. Ann Surg 1979;190:274–85.
[40] Smythe PM, Brereton-Stiles GG, Grace HJ, Mafoyane A, Schonland M, Coovadia HM, et al.
Thymolymolymphatic deficiency and depression of cell-mediated immunity in protein-calorie
malnutrition. Lancet 1971;2:939–43.
[41] Chandra RK. Nutrition and the immune system. Proc Nutr Soc 1993;52:77.
[42] Shronts EP. Basic concepts of immunology and its application to clinical nutrition. Nutr Clin
Pract 1993;8:177.
[43] Lorenz E, Good RA. Nutritional indications for cancer prevention-calorie restriction. In: Cun-
ninghan-Rundles S, editor. Nutrient modulation of the immune response. New York: Marcel
Dekker; 1993. p. 481.
[44] Barbul A, Lazarou SA, Efron DT, Wasserkrug HL, Efron G. Arginine enhances wound healing
and lymphocyte immune responses in humans. Surgery 1990;108:331.
[45] Barbul A, Sisto DA, Wasserkrug HL, Levenson SM, Efron G, Seifler E. Arginine stimulates
lymphocyte immune response in healthy human beings. Surgery 1981;90:244.
[46] Calder PC, Uaqoob P. Glutamine and the immune system. Amino Acids 1999;17:227.
D.S. Slone / Crit Care Clin 20 (2004) 135–157 155
[47] Saito H, Furukawa S, Matsuda T. Glutamine as an immunoenhancing nutrient. JPEN J Parenter
Enteral Nutr 1999;23:S59.
[48] Carver JD. Dietary nucleotides: cellular, immune, intestinal and hepatic system effects. J Nutr
1994;124:144.
[49] Good RA, Fernandes G, Cunningham–Rundles C. The relation of zinc deficiency to immunologic
function in animals and man. In: Seligman M, Hitzig WH, editors. Primary immunodeficiencies.
Amsterdam (Netherlands): Elsevier; 1980. p. 223.
[50] Dardenne M, Savino W, Borrih S, Bach JF. A zinc-dependent epitope of the molecule of thy-
mulin, a thymic hormone. Proc Natl Acad Sci U S A 1985;82:1202.
[51] Grimble RF. Nutritional antioxidants and the modulation of inflammation: theory and practice.
New Horiz 1994;2:412–20.
[52] Heys SD, Walker LG, Smith I, Eremin O. Enteral nutritional supplementation with key nu-
trients in patients with critical illness and cancer: a meta-analysis of randomized control clini-
cal trials. Ann Surg 1999;229:467–77.
[53] Beale RJ, Bryg DJ, Bihari DJ. Immunonutrition in the critically ill: a systematic review of
clinical outcome. Crit Care Med 1999;27:2799–805.
[54] Heyland DK, Novak F, Drover JW, Jain M, Su X, Suchner U. Should immunonutrition become
routine in critically ill patients? JAMA 2001;286(8):944–53.
[55] Moore FA, Moore EE, Kudsk KA. Clinical benefit of an immune-enhancing diet for early
postinjury enteral feeding. J Trauma 1994;37:607–15.
[56] Mendez C, Jurkovich GJ, Garcia I, Davis D, Parker A, Maier RV. Effects of an immune-
enhancing diet in critically injured patients. J Trauma 1997;42(5):933–41.
[57] Barbul A, Wasserkrug HL, Goldfine J. Enteral nutrition with supplemental arginine in normal
and injured rats. J Surg Res 1980;29:228–35.
[58] Braga M, Gianotti L, Cestari A, Bignali A, Pellegatta F, Dolei A, et al. Gut function, immune
and inflammatory responses in patients perioperatively fed with supplemented enteral formulas.
Arch Surg 1996;131:1257–65.
[59] Klein S, Kinney J, Jeejeebhoy K, Alpers D, Hellerstein M, Murray M, et al. Nutrition support
in clinical practice. JPEN J Parenter Enteral Nutr 1997;21(3):133–56.
[60] Moore EE, Jones TN. Benefits of immediate jejunal feeding after major abdominal trauma.
J Trauma 1986;26:874.
[61] Moore FA, Moore EE, Jones TN, McCroskey BL, Peterson VM. TEN versus TPN following
major abdominal trauma-reduced septic mortality. J Trauma 1989;29:916–23.
[62] Moore FA, Feliciano DV, Andrassy RJ, McArdle AH, Booth FV, Morgenstein–Wagner TB,
et al. Early enteral feeding, compared with parenteral reduces postoperative septic complications.
Ann Surg 1992;216(2):172–83.
[63] Boley SJ, Brandt LJ, Veith FJ, Kosches D, Sales C. A new provocative test for chronic mesen-
teric ischemia. Am J Gastroenterol 1991;86(7):888–91.
[64] Dudrick SJ, Wilmore DW, Vars HM, Rhoads JE. Long-term parenteral nutrition with growth
and development and positive nitrogen balance. Surgery 1968;64(1):134–42.
[65] Enrione EB, Gelfand MJ, Morgan D, Sperling M, Wagner SC, Popp MB. The effect of rate
and route of nutrient intake on protein metabolism. J Surg Res 1986;40(4):320–5.
[66] Meyer J. Nutrition. Surg Gynecol Obstet 1988;167:50.
[67] Lowry SF. The route of feeding influences injury responses. J Trauma 1990;33:S10–5.
[68] Alverdy J, Chi HS, Sheldon GF. The effect of parenteral nutrition on GI immunity. Ann Surg
1985;202(6):681–4.
[69] Kudsk KA, Croce MA, Fabian TC, Minard G, Tolley EA, Poret HA, et al. Enteral versus
parenteral feeding. Ann Surg 1992;215:503–11.
[70] Battistella FD, Widergren JT, Anderson JT, Siepler JK, Weber JC. A prospective, randomized
trial of intravenous fat emulsion administration in trauma victims requiring total parenteral
nutrition. J Trauma 1997;43:52–60.
[71] Pacelli F, Bossola M, Papa V, Malerba M, Modesti C, Sgadari A, et al. Enteral versus parenteral
nutrition after major abdominal surgery. Arch Surg 2001;136:933–5.
D.S. Slone / Crit Care Clin 20 (2004) 135–157156
[72] Lipman TO. Grains or veins: is enteral nutrition really better than parenteral nutrition? JPEN J
Parenter Enteral Nutr 1998;22:167.
[73] Cerra FB. Hypermetabolism, organ failure, and metabolic support. Surgery 1987;101:1.
[74] Border JR, Hassett J, LaDuca J, Seibel R, Steinberg S, Mills B, et al. The gut origin septic
states in blunt multiple trauma (ISS = 40) in the intensive care unit. Ann Surg 1987;206(4):
427–48.
[75] Holmes JH, Brundage SI, Pak-chuen Y, Hall RA, Maier RV, Jurkovich GJ. Complications of
surgical feeding jejunostomy in trauma patients. J Trauma 2003;47(6):1009–15.
[76] Myers JG, Page CP, Stewart RM, Schwesinger WH, Sirinek KR, Aust JB. Complications of
needle catheter jejunostomy in 2022 consecutive applications. Am J Surg 1995;170:547–51.
[77] Bessey PQ. Parenteral nutrition and trauma. In: Rombeau JL, Caldwell MD, editors. Clinical
nutrition: parenteral nutrition. 2nd edition. Philadelphia: WB Saunders; 1993. p. 538–65.
[78] Hansen LM, Hardie WR, Hidalgo J. Fat emulsion for intravenous administration: clinical expe-
rience with intralipid 10%. Ann Surg 1976;184:80–8.
[79] Belin RP, Bivins BA, Jona JZ, Young VL. Fat overload with a 10% soybean emulsion. Arch
Surg 1976;111:1391–3.
[80] Roth B, Nilsson–Ehle P, Eliasson I. Possible role of short-term nutrition with fat emulsions
for development of haemophagocytosis with multiple organ failure in a patient with traumatic
brain injury. Intensive Care Med 1993;19:111–4.
[81] Aarsland A, Chinkes D, Wolfe RR. Contributions of de novo synthesis of fatty acids to total
VLDL-triglyceride secretion during prolonged hyperglycemia/hyperinsulinemia in normal man.
J Clin Invest 1996;98:2008–17.
[82] Eddleston JM, Shelly MP. The effect on serum lipid concentrations of a prolonged infusion
of propofol-hypertriglyceridemia associated with propofol administration. Intensive Care Med
1991;17:424–6.
[83] Barr J. Propofol: a new drug for sedation in the intensive care unit. Int Anesthesiol Clin 1995;
33:131–54.
[84] Wolfe RR, O’Donnell Jr TF, Stone MD, Richmond DA, Burke JR. Investigation of factors de-
termining the optimal glucose infusion rate in total parenteral nutrition. Metabolism 1980;29:
892–900.
[85] Beisel WR. Nutrition and infection. In: Linder MC, editor. Nutritional biochemistry with clinical
applications. 2nd edition. New York: Elsevier Press; 1991. p. 507–52.
[86] Bauer B, Gardner L, Holdy K, Kalafer M. Case report: metabolic acidosis associated with
high protein enteral nutrition (EN). Presented at: Nutrition And Metabolic Support: Challenges
in the Age of Managed Care; 21st Clinical Congress of the American Society for Parenteral and
Enteral Nutrition. San Francisco, January 26–29, 1997.
[87] Brooks MJ, Melnik G. The refeeding syndrome: an approach to understanding its complica-
tions and preventing its occurrence. Pharmacotherapy 1995;15:713–26.
[88] Genuth SM. Whole body metabolism and the hormones of pancreatic islets. In: Berne RM, Levy
MN, editors. Physiology. 2nd edition. St. Louis (MO): Mosby; 1988. p. 864.
[89] Heymsfield SB, Bethel RA, Ansley JD, Gibbs DM, Felner JM, Nutter DO. Cardiac abnormali-
ties in cachectic patients before and during nutritional repletion. Am Heart J 1978;95:5884–94.
[90] Cravo ML, Gloria LM, Selhub J, Nadeau MR, Camilo ME, Resende MP, et al. Hyperhomocys-
teinemia in chronic alcoholism: correlation with folate, vitamin B-12, and vitamin B-6 status.
Am J Clin Nutr 1996;63:220–4.
[91] Weinsier RL, Krumdieck CL. Death resulting from overzealous total parenteral nutrition:
the refeeding syndrome revisited. Am J Clin Nutr 1981;34:393–9.
[92] Pasulka PS, Bistrian BR, Benotti PN, Blackburn GL. The risks of surgery in obese patients. Ann
Intern Med 1986;104:540–9.
[93] Choban PS, Heckler R, Burge JC, Flancbaum L. Increased incidence of nosocomial infections
in obese surgical patients. Am Surg 1995;61:1001.
[94] Printen KJ, Paulk SC, Mason EE. Acute postoperative wound complications after gastric sur-
gery for morbid obesity. Am Surg 1975;41:483–7.
D.S. Slone / Crit Care Clin 20 (2004) 135–157 157
[95] Feurer ID, Crosby LO, Buzby GP, Rosato EF, Mullen JL. Resting energy expenditure in mor-
bid obesity. Ann Surg 1983;197(1):17–21.
[96] Burge JC, Goon A, Choban PS, Glancbaum L. Efficacy of hypocaloric total parenteral nutri-
tion in hospitalized obese patients: a prospective, double-blind randomized trial. JPEN J Parenter
Enteral Nutr 1994;18:203.
[97] Dickerson RN, Rosato EF, Mullen JL. Net protein anabolism with hypocaloric parenteral nu-
trition in obese stressed patients. Am J Clin Nutr 1986;44:747.
[98] Dickerson RN, Boschert MA, Kudsk KA, Brown RO. Hypocaloric enteral tube feeding in
critically ill obese patients. Nutrition 2002;18:241–6.