Embed Size (px)
Citation preview

N
I
Msdcbscmp
aosvrspctocathTttTt1atdettnst
GASTROENTEROLOGY 2008;134:1729–1740
utrition in End-Stage Liver Disease: Principles and Practice
Alastair O’Brien Roger Williams
nstitute of Hepatology, Royal Free and University College Medical School, University College London, London, England
osc
mm(vaa
tmpas
dbatnNgbmtacc
Da
alnutrition is commonly seen in both alcoholicand nonalcoholic liver disease1–3 and has been
hown to adversely affect outcome (see Figure 1).4,5 Byefinition, it occurs when diet does not provide adequatealories and protein to maintain nutritional status or theody is unable to fully absorb or utilize food eatenecondary to liver disease. Despite the obvious relevance,linical research in this field is surprisingly limited andalnutrition is frequently underdiagnosed in clinical
ractice.6
The prevalence of malnutrition in cirrhosis is as highs 65%–90%.1–3 Evidence concerning the impact of etiol-gy (of cirrhosis) on malnutrition is conflicting. Sometudies have shown no difference in prevalence and se-erity of malnutrition in patients with viral- and alcohol-elated cirrhosis who were abstinent.2,7,8 Others havehown that alcoholic cirrhosis was associated with aoorer nutritional state compared with virus-associatedirrhosis.9 Active alcoholism is a major cause of malnu-rition per se and could contribute to the earlier devel-pment observed.10 Protein depletion and reduced mus-le function are common in cirrhosis, particularly in mennd patients with alcoholic liver disease.11 The reason forhe male preponderance is unknown and is not related toypermetabolism or reduced energy and protein intake.11
he reduced levels of testosterone observed in male pa-ients with cirrhosis12 may contribute to decreased pro-ein anabolism, but this requires further investigation.he largest studies on prevalence and severity have been
he Veterans Affairs Cooperative Studies in 1984 and993, which focused on alcoholic hepatitis.13,14 Thesend other studies showed that the severity of malnutri-ion correlated with that of the liver disease and theevelopment of serious complications such as hepaticncephalopathy, ascites, hepatorenal syndrome, post-ransplantation outcome, and mortality.15–18 Also, short-erm survival is reduced in parallel with severity of mal-utrition.19 The majority of patients in these pivotaltudies had advanced liver disease; however, more sophis-
icated methods of analysis (neutron activation analysisr intracellular/extracellular body water) have shown thatignificant losses of body cell mass may occur in Child Airrhosis.20
In this review, we examine the mechanisms underlyingalnutrition in chronic liver disease, the assessmentethods available, and the role of nutritional therapy
advice, supplementation, enteral or parenteral) in thearious stages of chronic liver disease. Acute liver failurend transplantation and the emerging data on probioticsre considered separately.
Mechanisms of Malnutrition inCirrhosisA variety of mechanisms are considered to con-
ribute to malnutrition in cirrhosis: poor dietary intake,alabsorption, increased intestinal protein losses, low
rotein synthesis, disturbances in substrate utilization,nd hypermetabolism. Many of these are not fully under-tood.
In advanced liver disease, patients often have poorietary intake. Recommended diets may be unpalatableecause of the sodium restriction needed for control ofscites and peripheral edema. A distortion or decrease inaste sensation (dysgeusia) associated with zinc or mag-esium deficiency is well described and may contribute.21
ausea and early satiety are well recognized, secondary toastroparesis, tense ascites, small bowel dysmotility, andacterial overgrowth.22,23 When admitted to the hospital,alnutrition is paradoxically further worsened as pa-
ients are often starved, for instance, for endoscopy. Inddition, as glucose storage is reduced in alcohol-inducedirrhosis,24 gluconeogenesis is active and can cause mus-le mass breakdown to provide amino acids for glucose
Abbreviations used in this paper: BCAA, branched-chain amino acid;EXA, dual-energy x-ray absorptiometry; PUFA, polyunsaturated fattycid; SAMe, S-adenosylmethionine.
© 2008 by the AGA Institute0016-5085/08/$34.00
doi:10.1053/j.gastro.2008.02.001

fmet6drsmcd
erdcpqnhssbpuee2iali
amMeemfde
mPcpPdctostafsKPItrtrlTtt
cpTdiitFtcrcdodct
Fcbam(nsA
1730 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
ormation.25 Patients need frequent meals to protectuscle mass, which are not always provided. However,
ven when inpatients receive specific attention to nutri-ion, as in the Veterans Affairs Cooperative Studies, only7% were found to consume the recommended 2500-kcaliet.13,14 In severe cholestasis, intraluminal bile salts areeduced with consequent malabsorption of fat and fat-oluble vitamins. This can be further worsened by neo-
ycin, which may blunt intestinal villi, and the use ofholestyramine for pruritus, which may induce bile salteficiency.26
The metabolic disturbances consequent to liver dis-ase, such as increased energy expenditure,27,28 insulinesistance,29 and low respiratory quotient (indicating re-uced glucose and increased lipid oxygenation),30 mayontribute to malnutrition even in the early stages. Hy-ermetabolic patients tend to weigh less, are more fre-uently malnourished, and have a higher mortality thanormometabolic patients.31 The estimated prevalence ofypermetabolism varies considerably, with the largesttudy of 473 cirrhotic patients reporting 34%.32 A smallertudy of 50 cirrhotic patients found only 2 hypermeta-olic patients,33 whereas a more recent study of 268atients found 15%.11 The cause of hypermetabolism isnclear, with one group finding no association with sex,tiology, severity of disease, protein depletion, and pres-nce of ascites or tumor.11 Indirect evidence suggests that5% of hypermetabolism in cirrhosis may be explained by
ncreased sympathetic nervous system activity, possiblys part of the commonly observed hyperdynamic circu-ation.34 Sepsis is common in liver disease and is likely to
igure 1. Malnutrition is predictive of survival in patients with liverirrhosis. Survival rates in patients with midarm muscle circumferenceselow the 5th (group 1), 10th (group 2), and 75th (group 3) percentilesnd above the 75th percentile (group 4). P � .001 at 6, 12, and 24onths between patients with severe and moderate malnutrition
groups 1 and 2, respectively) and those with normal and overnourishedutrition (groups 3 and 4, respectively). Patients with transplants werecreened at the time of transplantation. Reprinted with permission fromlberino et al.5
ncrease energy expenditure further. The use of �-block- S
de for variceal bleeding prophylaxis, which will reduceetabolic rate, is likely to be a confounding variable.easurement of energy expenditure by indirect calorim-
try is not straightforward or frequently available, andstimates such as the Harris–Benedict equation are com-only applied.35 It should be noted that significant dif-
erences have been shown between resting energy expen-iture values measured by indirect calorimetry and suchstimations.36
Polyunsaturated fatty acid (PUFA) deficiency is com-on in cirrhosis, especially alcoholic cirrhosis, because
UFA synthesis from essential fatty acid precursors oc-urs in the liver.37 PUFA deficiency has been found inlasma lipids, erythrocytes, platelets, and adipocytes.37
arenchymal cells are most likely deficient, although noata exist. The consequences of PUFA deficiency are un-lear, and supplementation is controversial.38 PUFA con-ributes to the fluidity of cell membranes and the releasef an array of secondary messengers (including eico-anoids), and PUFA deficiency is an independent predic-ive factor of mortality in alcoholic cirrhosis.37 However,ttempts to reverse deficiency have been disappointing;or example, parenteral nutrition containing Intralipid (aoybean oil, linoleic acid– based lipid emulsion; Freseniusabi, Uppsala, Sweden) failed to improve long-chainUFA deficiency in 9 malnourished alcoholic patients.39
ntriguingly, in alcohol-fed rats, a PUFA-enriched diet ledo more severe liver injury than a diet enriched in satu-ated fatty acids.40 Also, PUFA deficiency has been showno reverse alcohol-related mitochondrial dysfunction inodents via an increase in phospholipid arachidonic overinoleic ratio, which raises cytochrome oxidase activity.41
hus, PUFA deficiency may be an adaptive phenomenono counteract the decline in adenosine triphosphate syn-hesis flux.
Micronutrient Deficiencies in CirrhosisDeficiencies in water-soluble vitamins (vitamin B
omplex and C) are common in alcoholic cirrhosis inarticular but also occur in nonalcoholic liver disease.42
he risks of Wernicke’s encephalopathy and Korsakoff’sementia are well described in alcoholic patients deficient
n thiamine.43 Thiamine deficiency has also been shownn hepatitis C–related cirrhosis,44 and administration ofhiamine to all cirrhotic patients has been recommended.at-soluble vitamin deficiencies occur more commonly inhe cholestatic liver syndromes. Vitamin A (retinol) defi-iency has been described in cirrhosis and is considered aisk factor for development of cancer, including hepato-ellular carcinoma.45 Vitamin E, an antioxidant, is re-uced in cholestasis and alcoholic liver disease. Low levelsf trace elements such as selenium and zinc have beenescribed.46 Zinc deficiency in patients with chronic al-oholism is attributed to decreased intake and absorp-ion and diuretic-induced increased urinary excretion.47
upplementation with zinc has been shown to improve

gmdetsmMamctppdtto
twdmpTpicpHvcmscwxdmpete
clIiimeawh
ckpcf
cgnutbnlapotpgi
cdttc(mamsussmmpasChsbacidgitdwhm
May 2008 NUTRITION IN END-STAGE LIVER DISEASE 1731
lucose disposal in cirrhotic patients,48 and deficiencyay contribute to the impaired glucose tolerance and
iabetes commonly observed. Zinc deficiency is consid-red to precipitate hepatic encephalopathy49; however,rials of supplementation have shown conflicting re-ults.50,51 Zinc is also used in alcoholic patients for treat-
ent of night blindness not responsive to vitamin A.47
agnesium deficiency occurs in alcoholic liver disease,nd muscle magnesium is an independent predictor ofuscle strength.52 This is probably related to the reduced
ontent of sodium-potassium pumps in skeletal musclehat accompanies magnesium deficiency. However, sup-lementation did not restore muscle magnesium or im-rove muscle function in patients with alcoholic liverisease.53 Interestingly, patients treated with spironolac-one had higher contents of sodium-potassium pumps;he underlying mechanism is unclear and the subject ofngoing investigation.
Studies have shown that serum levels of 25-hydroxyvi-amin D are low in patients with liver disease54 and fallith disease progression.55 The likely causes include re-uced exposure to UV light, dietary insufficiency, andalabsorption. A high prevalence of osteoporosis is re-
orted in both cholestatic and noncholestatic cirrhosis.56
reatment with corticosteroids as part of immunosup-ressive regimens for autoimmune hepatitis and follow-
ng liver transplantation is a risk factor. Few randomizedontrolled trials have assessed the role of intervention inrevention of osteoporosis in chronic liver disease.57
owever, it is reasonable to recommend correction ofitamin D insufficiency with vitamin D3 and calcium inonditions where osteoporosis is likely. In addition, hor-one replacement therapy increases bone mineral den-
ity in primary biliary cirrhosis and should always beonsidered for postmenopausal women.58 All patientsith chronic liver disease should undergo a dual-energy-ray absorptiometry (DEXA) scan to assess bone mineralensity.57 Treatment with bisphosphonates is recom-ended in those with osteoporosis, as for noncirrhotic
atients. Oral alendronate (not risedronate) may causesophageal ulceration and should be avoided in view ofhe risk of precipitating variceal hemorrhage; cyclicaltidronate appears safe.
Diagnosis and AssessmentIt is not difficult to diagnose malnutrition in a
achectic patient with advanced liver disease, but in ear-ier stages of the disease diagnosis is more challenging.20
n addition, the cachexia of liver disease may developnsidiously and be masked by edema. Early diagnosis ismportant to allow appropriate intervention, because
alnutrition is predictive of complications of liver dis-ase and mortality.6 There is no gold standard for clinicalssessment. Body weight can be misleading in patientsith ascites and peripheral edema, although one study
as validated body mass index in cirrhotic patients with Eut-off values of 22 kg/m2 in nonascitic patients, 23g/m2 for patients with mild ascites, and 25 kg/m2 foratients with tense ascites.59 The creatinine height indexan be unreliable owing to frequent disturbances in renalunction in patients with liver disease.60
Protein catabolism is a hallmark of critical illness. Onean assess protein requirement by measuring the nitro-en balance, intake excretion, in which intake representsutritional nitrogen and excretion, the sum of measuredrinary nitrogen plus an estimate of cutaneous and gas-rointestinal losses.61 Achievement of a positive nitrogenalance is widely considered to be the primary goal ofutritional support, and several studies of nutrition in
iver disease have reported clinical improvements associ-ted with increases in nitrogen balance.62,63 Indeed, im-roved nitrogen balance calculations of improvementver time in response to nutrition is the single nutri-ional variable most consistently associated with im-roved outcome during critical illness.63 However, nitro-en balance is rarely measured outside clinical trials ands not routine practice at the authors’ hospital.
The 2 common bedside assessments, plasma proteinoncentration and anthropometry, both have significantrawbacks. Plasma protein concentration correlates bet-er with the severity of liver disease than with malnutri-ion.64 Anthropometric techniques such as midarm mus-le circumference assess body composition. Fat-free masslean body weight; water, protein, and mineral) and fat
ass are measured, and these techniques are referred tos 2-compartment systems. Anthropometric techniquesay be affected by edema65 and have been shown in one
tudy to classify up to 20%–30% of healthy controls asndernourished.66 However, several other studies havehown that anthropometric measurements and handgriptrength correlate well with more sophisticated assess-
ents such as DEXA in cirrhotic patients.67,68 Indeed,idarm muscle circumference was shown to be an inde-
endent predictor of mortality in advanced cirrhosis.69 Inn Italian multicenter study of more than 1000 patients,urvival was related to midarm muscle circumference forhild A and B but not C.70 Midarm muscle circumferenceas also been shown to be independently associated withurvival and improve prognostic accuracy when com-ined with the Child score.5 The measurement of phasengle by bioimpedance analysis as an indicator of bodyell mass has been shown to be of prognostic significancen cirrhosis71; however, most, but not all, investigatorseem it unreliable in patients with ascites.72-74 Subjectivelobal assessment uses clinical information obtained dur-ng history taking and examination to determine nutri-ional status without objective measurements and canetermine outcome in patients with cirrhosis.75 However,hen compared with nutritional prognostic index andandgrip strength, handgrip strength was the onlyethod that predicted a poorer clinical outcome.69 The
uropean Society for Clinical Nutrition and Metabolism
ggatamrcg
iioss
ob4dsDepatsapscita
m
t(isttphsdtr
m
Fmta gory
T
1
2
3
4
5
1732 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
uidelines state that bedside methods such as subjectivelobal assessment, anthropometry, or handgrip strengthre adequate for identification of undernutrition andhat composite scores do not add value. For quantitativenalysis, the determination of phase angle or body cellass using bioimpedance analysis is recommended
ather than anthropometry, despite limitations with as-ites.76 The authors’ current practice is to use subjectivelobal assessment or handgrip strength.
Although anthropometrical methods are useful fornitial assessment, they are of much less value for mon-toring treatment effects because of their high coefficientf variation and interobserver variability. Thus, moreophisticated methods are often used in research studies,uch as DEXA and in vivo neutron activation analysis.
The limitations of 2-compartment assessment meth-ds that distinguish fat mass from fat-free mass haveeen recently highlighted.77 This study compared a-component model (data obtained from densitometry,euterium dilution, and DEXA) with reference and bed-ide 2-component techniques, such as anthropometry,EXA, and bioimpedance analysis. Significant differ-
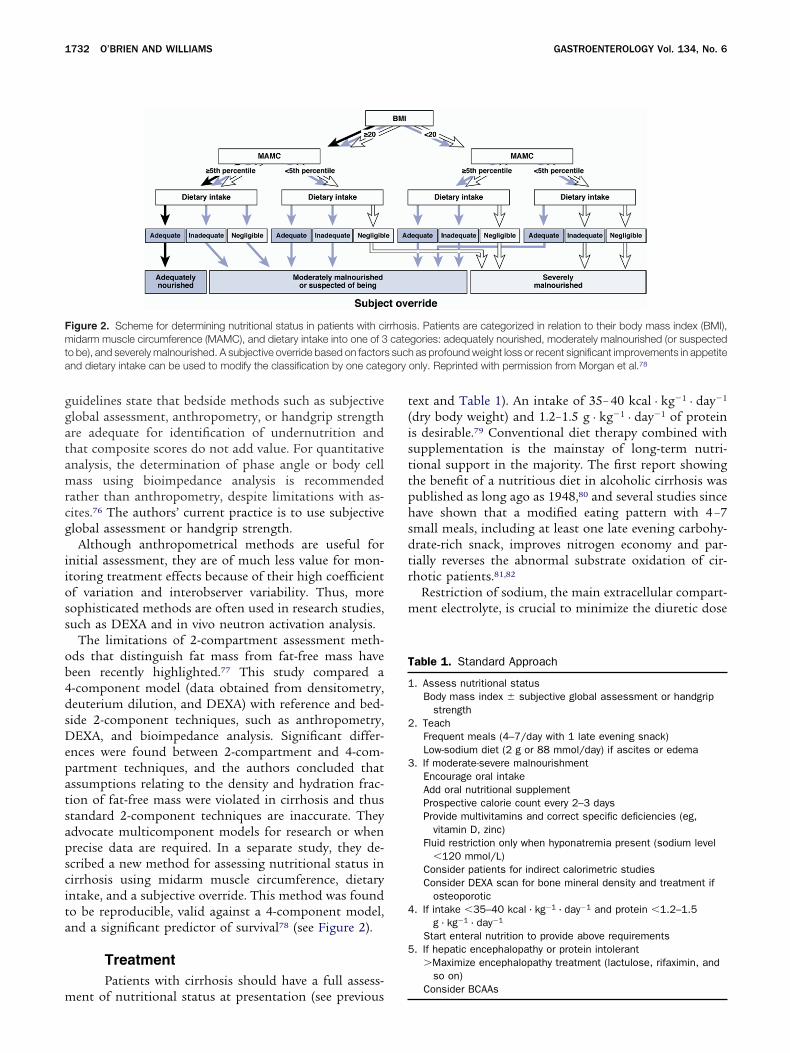
nces were found between 2-compartment and 4-com-artment techniques, and the authors concluded thatssumptions relating to the density and hydration frac-ion of fat-free mass were violated in cirrhosis and thustandard 2-component techniques are inaccurate. Theydvocate multicomponent models for research or whenrecise data are required. In a separate study, they de-cribed a new method for assessing nutritional status inirrhosis using midarm muscle circumference, dietaryntake, and a subjective override. This method was foundo be reproducible, valid against a 4-component model,nd a significant predictor of survival78 (see Figure 2).
TreatmentPatients with cirrhosis should have a full assess-
igure 2. Scheme for determining nutritional status in patients with ciidarm muscle circumference (MAMC), and dietary intake into one of 3
o be), and severely malnourished. A subjective override based on factornd dietary intake can be used to modify the classification by one cate
ent of nutritional status at presentation (see previous
ext and Table 1). An intake of 35– 40 kcal · kg�1 · day�1
dry body weight) and 1.2–1.5 g · kg�1 · day�1 of proteins desirable.79 Conventional diet therapy combined withupplementation is the mainstay of long-term nutri-ional support in the majority. The first report showinghe benefit of a nutritious diet in alcoholic cirrhosis wasublished as long ago as 1948,80 and several studies sinceave shown that a modified eating pattern with 4 –7mall meals, including at least one late evening carbohy-rate-rich snack, improves nitrogen economy and par-ially reverses the abnormal substrate oxidation of cir-hotic patients.81,82
Restriction of sodium, the main extracellular compart-ent electrolyte, is crucial to minimize the diuretic dose
is. Patients are categorized in relation to their body mass index (BMI),gories: adequately nourished, moderately malnourished (or suspectedas profound weight loss or recent significant improvements in appetite
only. Reprinted with permission from Morgan et al.78
able 1. Standard Approach
. Assess nutritional statusBody mass index � subjective global assessment or handgrip
strength. Teach
Frequent meals (4–7/day with 1 late evening snack)Low-sodium diet (2 g or 88 mmol/day) if ascites or edema
. If moderate-severe malnourishmentEncourage oral intakeAdd oral nutritional supplementProspective calorie count every 2–3 daysProvide multivitamins and correct specific deficiencies (eg,
vitamin D, zinc)Fluid restriction only when hyponatremia present (sodium level
�120 mmol/L)Consider patients for indirect calorimetric studiesConsider DEXA scan for bone mineral density and treatment if
osteoporotic. If intake �35–40 kcal · kg�1 · day�1 and protein �1.2–1.5
g · kg�1 · day�1
Start enteral nutrition to provide above requirements. If hepatic encephalopathy or protein intolerant
�Maximize encephalopathy treatment (lactulose, rifaximin, andso on)
rrhoscate
s such
Consider BCAAs

npdw
imom1csmcfasai
tcadbpcot
ktaacapbcdaimiztesdOvisbat
s2sdmf
fisthvheqltsnr“tmapbtbvwieRnlgibtpasmtocfpmaittv
May 2008 NUTRITION IN END-STAGE LIVER DISEASE 1733
ecessary to control ascites, peripheral edema, and he-atic hydrothorax. A 2-g (88 mmol/L) sodium-restrictediet is recommended rather than the previous 0.5 g,hich is very unpalatable.In severely malnourished patients with cirrhosis, feed-
ng approximately 40 kcal · kg�1 · day�1 orally over 1onth increases body fat mass, irrespective of the degree
f liver damage.83 When counseling is insufficient toaintain an intake of 35– 40 kcal · kg�1 · day�1 and 1.2–
.5 g · kg�1 · day�1 protein, as documented by calorieount, chemically defined nutritional oral supplementshould be added.79 A controlled trial with a daily supple-
ent of 1000 kcal and 34 g protein for 1 year in alcoholicirrhosis showed a reduction in hospitalization due toewer infective episodes and a trend to improved surviv-l.84 Additionally, 3 months of treatment with a dailyupplement containing 500 kcal, 32 g protein, 11 g fat,nd 70 g carbohydrate improved nutritional and biolog-cal parameters in malnourished cirrhotic patients.85
If nutritional supplementation is insufficient to main-ain desired intake, then artificial nutrition should beommenced, either via a nasogastric feeding tube (enter-lly) or intravenously (parenterally). A nasoenteric (naso-uodenal or nasojejunal) feeding tube is considered aetter option; however, insertion requires an endoscopicrocedure, and thus nasogastric tubes are used moreommonly. Although mostly used for inpatients becausef practical considerations, both forms of artificial nutri-ion may be tolerated at home, with appropriate support.
A whole protein formula providing 35– 40cal · kg�1 · day�1 energy and 1.2–1.5 g · kg�1 · day�1 pro-ein is recommended for enteral feeding.77 Standard prep-rations contain approximately 100 kcal energy, 4 g protein,nd 3.5 mmol of sodium and potassium per 100 mL. Con-entrated high energy (1.5 kcal/mL) and protein formulasre available in many countries and may be preferable inatients with hyponatremia and ascites to regulate fluidalance. This may also improve treatment adherence be-ause less volume needs to be consumed. For patients whoevelop steatorrhea, it is important to limit long-chain fattycids and increase short-chain and medium-chain fatty ac-ds in the formula. Pancreatic enzymes should be supple-
ented, especially in patients with alcohol-related cirrhosisn whom pancreatic insufficiency is common. As these en-ymes are inactivated by gastric acid, proton pump inhibi-ors are necessary. Four randomized trials concerning totalnteral nutrition in cirrhosis have been reported.86–89 Threehowed an increased dietary intake over conventional oraliet,87–89 and 2 showed improvements in liver function.88,89
ne showed lower hospital mortality compared with con-entional diet.87 The fourth was performed in well-nour-shed patients admitted with variceal bleeding and failed tohow benefit in nutritional status or disease-related mor-idity and mortality.89 However, most of these patients wereble to eat 2000 kcal/day from day 4. In hospitalized pa-
ients with an inadequate dietary intake, enteral nutrition chould be commenced as soon as possible, ideally within4–48 hours of admission.90 This is illustrated by a pro-pective study in 396 patients showing that a decrease inietary intake was an independent predictor of hospitalortality and corresponded with a deterioration of liver
unction.91
Two important considerations during nasogastriceeding are hepatic encephalopathy and variceal bleed-ng. Hepatic encephalopathy must be treated aggres-ively with lactulose or rifaximin and attention giveno possible precipitating causes (eg, electrolyte status,ypoxemia, sedative use, and presence of sepsis orariceal bleed). Traditionally, a restricted protein dietas been considered a mainstay of treatment92; how-ver, cirrhotic patients exhibit increased protein re-uirements to achieve balanced nitrogen metabo-
ism,93 and normal protein diets have been given safelyo patients with hepatic encephalopathy.94 Thus, re-triction is rarely required but, if necessary, usually foro more than 48 hours. It should be noted that theecommended protein supplementation is based ondry” body weight and may need alteration in edema-ous patients. Importantly, the risk of aspiration pneu-
onia in patients with advanced hepatic encephalop-thy during tube feeding must be weighed against theotential complications of parenteral nutrition (seeelow). The European Society for Parenteral and En-eral Nutrition guidelines support insertion of fine-ore nasogastric tubes in patients with esophagealarices.77 This has been addressed in only one study, inhich 22 patients with esophageal varices after bleed-
ng and endoscopic treatment were randomized toither nasogastric feeding or no oral diet for 3 days.89
ecurrent bleeding occurred in 3 patients from theasogastric tube group but none of the controls. In
ight of these findings, it has been suggested that theuidelines should state that tube feeding is dangerousn patients with esophageal varices that have bledefore and that in patients without former bleeding,here is a tendency for an adverse effect.95 The Euro-ean Society for Clinical Nutrition and Metabolismuthors responded that endoscopic therapies in thistudy were unbalanced between the 2 groups, which
ight have influenced outcome, with a higher propor-ion of injection sclerotherapy in the feeding group aspposed to a greater number of band ligations inontrols.96 They also referred to a small series of tube-ed cirrhotic patients in which fine-bore tubes did notrovoke variceal hemorrhage97 and a trial of low/nor-al protein diets via fine-bore tube in hepatic enceph-
lopathy in which gastrointestinal bleeding occurredn only one of 30 patients.83 They concluded “if pa-ients are unable to maintain adequate oral intake,ube feeding is recommended (even when esophagealarices are present).”96 They acknowledged that there is
oncern in the immediate days following a bleed. In-
dfi
aafpstwstfuphd(iptslworosrn
sctApodfHr2tppitbmd
tuo
cf
abanmtrhllactteihBpppec
hciasJpbptswm
acie
btFiasn
1734 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
eed, our current practice is to wait at least 24 hoursollowing endoscopic therapy for a bleed and thennsert a nasogastric tube and commence feeding.
Total parenteral nutrition (containing Intralipid,mino acids, dextrose, electrolytes, vitamins, and miner-ls) in severe alcoholic hepatitis has shown benefit in liverunction but not (short-term) survival.98,99 One study inatients with transjugular intrahepatic portosystemichunts concluded that small intestinal metabolism con-ributes to postfeeding (enteral) hyperammonemia,hich may worsen hepatic encephalopathy, and that, in
uch cases, parenteral nutrition may be superior to en-eral nutrition.100 Further supportive evidence comesrom a meta-analysis of studies performed in the 1980ssing parenteral nutrition in hepatic coma. This showedrobable improved survival, but the studies were veryeterogeneous and so firm conclusions are difficult toraw.101 However, the risks of mechanical complications
eg, pneumothorax) and catheter-related sepsis are highn malnourished cirrhotic patients; it is essential thatarenteral nutrition is administered via a dedicated lineo reduce the incidence of sepsis. Also, the osmotictrength of parenteral mixtures requires the infusion ofarge amounts of fluid that may be excessive for patientsith ascites. Thus, enteral feeding is the preferred modef artificial nutrition in liver disease, and the parenteraloute is reserved for intensive care patients with multi-rgan failure and subsequent paralytic ileus that preventsuccessful enteral feeding. It should be mentioned that aandomized trial comparing the two in liver disease hasever been performed.Severe alcoholic hepatitis, defined by a Maddrey
core �32, has a significant mortality rate. Althoughorticosteroids remain the mainstay of treatment,102
here have been several studies of nutritional support.multicenter, randomized, controlled trial that com-
ared 4 weeks of treatment with total enteral nutritionr corticosteroids showed no difference in mortalityuring treatment between the 2 groups.103 Deaths wereound to occur earlier in the enteral nutrition group.owever, 10 of the survivors treated with corticoste-
oids died in the first year of follow-up compared withof 24 who received enteral nutrition. The majority of
hese deaths were due to sepsis. The investigators hy-othesized that the increase in infection seen withrolonged immunosuppression could be reduced by
mproving gut barrier function and thus reducing bac-erial translocation. They went on to examine the com-ination of enteral nutrition with corticosteroid treat-ent in a pilot study in 13 patients and found no
eaths related to infection.104
Finally, insertion of a percutaneous feeding gastros-omy may be indicated in patients with an esophageal/pper gastrointestinal stricture, but ascites, impairment
f the coagulation system, and portosystemic collateral airculation due to portal hypertension are significant riskactors.105
Value of Branched-Chain Amino AcidsOver the years, the use of the branched-chain
mino acids (BCAAs) leucine, isoleucine, and valine haseen the subject of continued interest. These are essentialmino acids, meaning that they cannot be synthesized deovo, must be obtained from the diet, and are largelyetabolized by muscle rather than liver. In cirrhosis,
here is a likely reduced total body pool of BCAAs due toeduced lean muscle mass and defective use secondary toyperinsulinemia.106 Conversely, amino acids metabo-
ized by the liver are elevated in cirrhosis (eg, the circu-ating aromatic amino acids phenylalanine, tryptophan,nd tyrosine).106 BCAAs compete with the serotonin pre-ursor tryptophan for the same amino acid transporter inhe blood-brain barrier, and the imbalance between thewo in cirrhosis probably influences brain ammonia lev-ls directly or indirectly.107 This is considered to be anmportant mechanism underlying the development ofepatic encephalopathy, and so supplementation withCAAs may reduce brain uptake of tryptophan and im-rove encephalopathy.108 Additionally, both enteral andarenteral BCAA supplementation improved cerebralerfusion in cirrhotic patients, which again may improvencephalopathy; the underlying mechanism is un-lear.109,110
Oral BCAAs have been shown to benefit patients withepatic encephalopathy111,112; moreover, a large multi-enter study showed that oral BCAAs given for 1 yearmproved the Child score, reduced hospital admissions,nd prolonged event-free survival.113 A further large trialhowed improved event-free survival and quality of life inapanese patients treated with BCAAs for 2 years com-ared with controls.114 However, a Cochrane analysisased on 11 trials of oral supplementation and 556atients found no convincing evidence of benefit.115 Al-hough no toxicity was reported, many patients stopupplementation because of the taste and amount ofater required. Importantly, no benefit of BCAA supple-entation was observed in protein-tolerant patients.Parenteral administration of BCAAs to patients with
cute liver failure–related encephalopathy within intensiveare units has been advocated because these patients havencreased total amino acids but reduced BCAAs.116,117 How-ver, there have been no controlled studies.
The timing of BCAA supplementation was addressedy one crossover study of 12 cirrhotic patients.118 Day-ime administration improved nitrogen balance andischer’s ratio; however, both were further significantly
mproved with nocturnal administration. At 3 months,significant increase in serum albumin level was ob-
erved in patients administered nocturnal BCAAs butot daytime BCAAs. It is possible that daytime BCAAs
re used primarily as calories, whereas nocturnal
Bs
naEgretp
mgtmnipdcipeswatsmaLfo
aitissdgowhsimtm
mbThcmw
oyvcEpcli
oAfctpstr8rhpaMsubvpaapesscostsptmp
May 2008 NUTRITION IN END-STAGE LIVER DISEASE 1735
CAAs may be preferentially used for protein synthe-is.
The use of BCAAs remains controversial, and they areot widely available in many centers due to their expensend unpalatability.106 The authors currently follow theuropean Society for Parenteral and Enteral Nutritionuidelines,77 which recommend that enteral feed en-iched with BCAAs be reserved for patients who developncephalopathy with enteral feeding despite appropriatereatment. This represents a very small proportion ofatients.
Additional Nutritional SupplementsNutritional supplements containing S-adenosyl-
ethionine (SAMe), a coenzyme involved in methylroup transfers, are postulated to improve gut or sys-emic defenses to infection and injury.119 Experimental
odels have shown that SAMe protects against tumorecrosis factor hepatotoxicity.120 Patients with alcohol-
nduced liver disease have reduced SAMe levels that mayredispose to mitochondrial glutathione depletion andysfunction, and oral administration resulted in signifi-antly decreased liver transplantation and liver mortalityn patients with alcoholic liver disease compared withlacebo.121 Supplementation also reduced pruritus andlevated serum bilirubin levels in gestational cholesta-is.122 However, a Cochrane analysis concluded that thereas no evidence supporting or refuting the use of SAMend high-quality randomized trials were needed beforehey could be recommended.123 Another frequently takenupplement is polyenylphosphatidylcholine (lecithin), a
ixture of glycolipids, triglycerides, and phospholipidsnd an essential component of the plasma membrane.ecithin has been shown to prevent cirrhosis in alcohol-ed baboons,124 but in humans it did not improve clinicalutcome in heavy drinkers.125
Acute Liver FailureBecause there is usually no preceding illness in
cute liver failure, the patient is not generally malnour-shed at presentation. The aim of treatment is to main-ain a nutritional balance in the face of the markedlyncreased catabolic state that occurs both as a result ofevere hepatic impairment and frequently coexistent sep-is. Hypoglycemia is commonly seen in the initial stagesue to impaired gluconeogenesis, depletion of hepaticlycogen, and hyperinsulinism, and hence administrationf intravenous glucose at 1.5–2 g · kg�1 · day�1 has beenidely adopted. At a later stage, often secondary to sepsis,yperglycemia related to insulin resistance may be ob-erved. In general intensive care patients, 2 large random-zed trials have shown that intensive insulin therapy to
aintain normoglycemia produced an absolute reduc-ion in risk of hospital death of 3%– 4% and an improve-
ent in morbidity.126 Strict blood glucose control (�110 s
g/dL) is required to obtain the most clinical benefit,ut this inherently increases the risk of hypoglycemia.hese studies did include patients with hepatic disorders;owever, no study has formally addressed strict glycemicontrol in acute liver failure. Because hypoglycemia isore frequent in these patients, great care must be takenith insulin regimens.A recent European survey was answered by 33 hepatol-
gy units attending 2–170 cases of acute liver failure perear. All units used specific nutrition regimens, but thesearied considerably and mostly resembled those used inritically ill patients with near-normal liver function.127
ight units preferentially used enteral feeding and 25arenteral. Two thirds used standard parenteral regimensontaining amino acids, although plasma amino acidevels are already greatly elevated due to liver failure andncreased protein catabolic rate.128
Liver TransplantationSeveral studies have examined the impact of pre-
perative malnutrition on outcome posttransplantation.series of 100 patients 6 months posttransplantation
ound that muscle wasting was one of 6 variables asso-iated with reduced survival.129 Other studies have shownhat preoperative malnutrition impacts negatively onosttransplantation outcome.15,27,31 These include a pro-pective study of 150 patients who underwent transplan-ation for cirrhosis and who could be divided into high-isk and low-risk groups, with survival rates of 54% and8%, respectively, based on preoperative nutrition andesting energy expenditure.31 Other studies have shownigher rates of complications and mortality in cirrhoticatients with malnutrition compared with those withdequate nutrition who undergo transplantation.129,130
ore recently, however, this has been questioned. A pro-pective series of 53 patients from the Mayo Clinic whonderwent transplantation failed to show an associationetween any preoperative nutritional parameters and sur-ival or global resource utilization.131 In this series, theostoperative mortality was quite low after 1 year (7.5%),s was the frequency of preoperative malnutrition (9.4%),nd patients were offered preoperative nutritional sup-ort. Thus, this study could be interpreted as showingither that adverse outcome after transplantation is as-ociated with factors other than preoperative nutritionaltate, or that preoperative nutritional support can over-ome the adverse effect of malnutrition on outcome. Anlder study used a prognostic nutritional index based onerum albumin and transferrin levels, triceps skinfoldhickness, and delayed hypersensitivity responses to as-ess malnutrition and outcome posttransplantation. Allatients were found to be malnourished pretransplanta-ion, but there was no correlation between this index and
ortality or morbidity posttransplantation.132 A furtherrospective series of 61 candidates for transplantation
howed poor correlation between nutritional parameters
aepfadnt
tsttpcorssevbce
lsrspp(fd
tlsopattpw
lstliutt
tadmamo
teerptdtTabgpapfca
mmwitoPppr
stm1mcsp
tcrveT
1736 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
nd the Child score and Model of End-Stage Liver Dis-ase score.133 Interestingly, a retrospective study in 121atients examined risk factors for acute rejection andound that the only significant predictor on multivariatenalysis of a reduction in acute cellular rejection wasecreased midarm muscle circumference, that is, mal-ourished patients had a lower incidence of acute rejec-ion.134
To date, no controlled trial has shown that preopera-ive intervention improves clinically relevant outcomes. Atudy of 82 patients randomized to enteral supplemen-ation (750 kcal, 20 g protein, and 34 g fat) and conven-ional diet or conventional diet alone showed an im-rovement in handgrip strength and midarm muscleircumference but not outcome.135 The difference inverall survival at 6 months posttransplantation almosteached significance, and a larger sample size might havehown benefit. Two studies have examined nutritionalupport following transplantation. Early postoperativenteral nutrition, within 12 hours, reduced the rate ofiral infections and showed a trend toward a lower rate ofacterial infections.136 Postoperative parenteral nutritionompared with intravenous administration of fluid andlectrolytes reduced the length of intensive care stay.137
Obesity has a negative impact on outcome after non-iver surgery.138 However, the published reports on obe-ity in liver transplantation are inconclusive.139 –141 Mostecently, a case-control study from John Hopkins Univer-ity Hospital examined 121 patients undergoing trans-lantation. Although postoperative complications, hos-ital stay, and cost were higher in severely obese patients
body mass index �32.3 kg/m2 for women, �31.1 kg/m2
or men) compared with nonobese patients, there was noifference in overall survival rates.142
Immunonutrition, supplementation with nutrientshat have been shown to beneficially influence immuno-ogic or inflammatory parameters in clinical or laboratorytudies (eg, glutamine), has shown positive results inther gastrointestinal surgery.143 A pilot study of 15atients given an immunomodulatory diet containingrginine, n-3 fatty acids, and nucleotides (Impact; Novar-is Consumer Health, Nyon, Switzerland) before and af-er transplantation showed an increase in total bodyrotein and a trend to reduction in infections comparedith historical controls receiving standard nutrition.144
Use of Probiotics and SynbioticsAlthough not directly related to nutrition and
iver disease, the use of probiotics and synbiotics along-ide nutritional supplements merits consideration in thereatment of the frequent septic episodes that accompanyiver decompensation. Probiotics are living microorgan-sms, prebiotics are indigestible carbohydrates that stim-late the growth and activity of beneficial bacteria withinhe intestinal flora, and synbiotics are a combination of
he two.145 There is increasing evidence that bacterial eranslocation of intestinal flora combined with failure ofntibacterial defense mechanisms plays a key role in theevelopment of sepsis.146 Probiotic or prebiotic treat-ent aims to augment the intestinal content of lactic
cid–type bacteria at the expense of other species withore pathogenic potential and thus reduce the incidence
f sepsis.A randomized study compared postoperative infec-
ions in 95 liver transplant recipients treated with anarly supply of standard enteral feed supplemented withither a synbiotic regimen including Lactobacillus planta-um and fermentable fiber, a heat-inactivated Lactobacilluslantarum and fiber, or selective intestinal decontamina-ion.147 The patients who received the synbiotic regimeneveloped significantly fewer bacterial infections (13%)han those undergoing intestinal decontamination (48%).he mean duration of antibiotic therapy, hospital stay,nd intensive care unit stay was also shorter in the syn-iotic group but did not reach significance. The sameroup compared the postoperative use of a mixture of 4rebiotics versus the same mixture plus a probiotic prep-ration containing lactic acid bacteria (synbiotic) in 66atients.148 The incidence of postoperative bacterial in-ections was significantly reduced (48% given prebioticsompared with 3% given synbiotics), and the duration ofntibiotic therapy was significantly shorter in the latter.
There is also evidence that synbiotic/probiotic supple-entation improves hepatic function. Synbiotic treat-ent improved the Child score in 55 cirrhotic patientsith minimal hepatic encephalopathy, with significant
mprovements in bilirubin level, albumin level, and pro-hrombin time.149 Also, supplementation with the probi-tic VSL#3 (lactobacillus and bifidobacterium bacteria: VSLharmaceuticals, Inc, Fort Lauderdale, FL) improved he-atic function and serum alanine transferase level inatients with alcohol-related and hepatitis C–related cir-hosis.150
ConclusionsIn summary, malnutrition is common in end-
tage liver disease and adversely affects prognosis. Nutri-ional support improves outcome in patients unable to
aintain an intake of 35– 40 kcal · kg�1 · day�1 and 1.2–.5 g · kg�1 · day�1 protein. Simple methods of assess-ent such as subjective global assessment, midarm mus-
le circumference, and calorie counting are useful, andtandard enteral products may be used in the majority ofatients.However, considerable difficulties remain concerning
he treatment modalities. Enteral nutrition is usuallyonsidered first line, but the parenteral route may beequired if the patient is intolerant due to nausea andomiting or develops increasing encephalopathy. How-ver, there is a significant risk of catheter-related sepsis.he value of BCAAs remains uncertain despite a consid-
rable number of studies, and a more palatable form
wmcntbossuseaacws
May 2008 NUTRITION IN END-STAGE LIVER DISEASE 1737
ould help clarify their value. There is very little infor-ation concerning nutrition in acute liver failure and
onflicting data regarding the effect of preoperative mal-utrition and intervention on outcome in liver transplan-ation, although early postoperative nutrition seems toe of benefit. Synbiotics may provide additional benefitsver dietary supplementation in reducing infective epi-odes, which impact malnutrition. Future researchhould be aimed at answering these questions. In partic-lar, disease-specific nutritional therapy should be con-idered for acute liver failure, sepsis, transplantation, andncephalopathy. Further large-scale intervention studiesre required before treatment guidelines can be based on
formal meta-analysis. The implementation of theserucial studies will be extremely difficult, and researchersill need to collaborate on a national or international
cale.
References
1. Italian Multicentre Cooperative Project on nutrition in liver cir-rhosis. Nutritional status in cirrhosis. J Hepatol 1994;21:317–325.
2. Caregaro L, Alberino F, Amodio P, et al. Malnutrition in alcoholicand virus-related cirrhosis. Am J Clin Nutr 1996;63:602–609.
3. Campillo B, Richardet J-P, Scherman E, et al. Evaluation ofnutritional practice in hospitalized cirrhotic patients: results of aprospective study. Nutrition 2003;19:515–521.
4. Kalman DR, Saltzman JR. Nutrition status predicts survival incirrhosis. Nutr Rev 1992;54:217–219.
5. Alberino F, Gatta A, Amodio P, et al. Nutrition and survival inpatient with cirrhosis. Nutrition 2001;17:445–450.
6. Cabre E, Gassull MA. Nutrition in chronic liver disease and livertransplantation. Curr Opin Clin Nutr Metab Care 1998;1:423–430.
7. Thuluvath PJ, Triger DR. Evaluation of nutritional status by usinganthropometry in adults with alcoholic and non-alcoholic liverdisease. Am J Clin Nutr 1994;60:269–273.
8. Sarin SK, Dhingra N, Bansai A, et al. Dietary and nutritionalabnormalities in alcoholic liver disease: a comparison withchronic alcoholics without liver disease. Am J Gastroenterol1997;92:777–783.
9. Caly WR, Strauss E, Carriho, et al. Different degrees of malnu-trition and immunological alterations according to the etiology ofcirrhosis: a prospective and sequential study. Nutr J 2003;2:10.
10. Simko V, Connell AM, Banks B. Nutritional status in alcoholicswith and without liver disease. Am J Clin Nutr 1982;35:197–203.
11. Peng S, Plank L, McCall J, et al. Body composition, musclefunction, and energy expenditure in patients with liver cirrhosis:a comprehensive study. Am J Clin Nutr 2007;85:1257–1266.
12. Baker H, Burger H, de Kretser D, et al. A study of the endocrinemanifestations of hepatic cirrhosis. Q J Med 1976;45:145–178.
13. Mendenhall CL, Anderson S, Weesner RE, et al. Protein-caloriemalnutrition associated with alcoholic hepatitis. Am J Med1984;76:211–222.
14. Mendenhall CL, Moritz TE, Roselle GA, et al. A study of oralnutritional support with oxandrolone in malnourished patientswith alcoholic hepatitis: results of a Department of VeteransAffairs Cooperative Study. Hepatology 1993;17:564–576.
15. Pikul J, Sharpe MD, Lowndes R, et al. Degree of preoperative
malnutrition is predictive of postoperative morbidity and mortal-ity in liver transplant recipients. Transplantation 1994;57:469–472.
16. Harrison J, McKiernan J, Neuberger JM. A prospective study onthe effect of recipient nutritional status on outcome in livertransplantation. Transplant Int 1997;10:369–374.
17. Moller S, Bendtsen F, Christensen E, et al. Prognostic variablesin patients with cirrhosis and esophageal varices without priorbleeding. J Hepatol 1994;21:940–946.
18. Mendenhall C, Roselle G, Gartside P, et al. Relationship ofprotein calorie malnutrition to alcoholic liver disease: a re-ex-amination of data from two Veterans Administration CooperativeStudies. Alcohol Clin Exp Res 1995;19:635–641.
19. Mendenhall C, Tosch T, Weesner R, et al. VA cooperative studyon alcoholic hepatitis II: prognostic significance or protein-calo-rie malnutrition. Am J Clin Nutr 1986;43:213–218.
20. Prijatmoko D, Strauss BJG, Lambert JR, et al. Early detection ofprotein depletion in alcoholic cirrhosis: role of body compositionanalysis. Gastroenterology 1993;105:1839–1845.
21. Madden AM, Bradbury W, Morgan MY. Taste perception in cir-rhosis: its relationship to circulating micronutrients and foodpreferences. Hepatology 1997:26:40–48.
22. Thuluvath PJ, Triger DR. Autonomic neuropathy in chronic liverdisease. QIM 1989;72:737–747.
23. Quigley EMM. Gastrointestinal dysfunction in liver disease andportal hypertension. Gut-liver interaction revisited. Dig Dis Sci1996;41:557–561.
24. Muller MJ, Fenk A, Lautz HU, et al. Energy expenditure andsubstrate metabolism in ethanol-induced liver cirrhosis. Am JPhysiol 1991;260:E338–E344.
25. Marsano L, Martin A, Randall H. Current nutrition in liver dis-ease. Curr Opin Gastroenterol 2002;18:246–253.
26. Thompson GR. Actions of neomycin on the intraluminal phase oflipid absorption. J Clin Invest 1971;50:321–323.
27. Muller MJ, Lautz HU, Plogmann B, et al. Energy expenditure andsubstrate oxidation in patients with cirrhosis: the impact ofcause, clinical staging and nutritional state. Hepatology 1992;15:782–794.
28. Greco AV, Mingrone G, Benedetti G, et al. Energy and substratemetabolism in patients with cirrhosis. Hepatology 1998;27:346–350.
29. Petrides AS, DeFronzo RA. Glucose and insulin metabolism incirrhosis. J Hepatol 1989;8:107–114.
30. Owen OE, Trapp VE, Reichard GA, et al. Nature and quantity offuels consumed in patients with alcoholic cirrhosis. J Clin Invest1983;72:1821–1832.
31. Selberg O, Bottcher J, Tusch G, et al. Identification of high andlow risk patients before liver transplantation. A prospectivecohort of nutritional and metabolic parameters in 150 patients.Hepatology 1997;25:652–657.
32. Muller MJ, Bottcher J, Seelberg O, et al. Hypermetabolism inclinically stable patients with liver cirrhosis. Am J Clin Nutr1999;69:1194–1201.
33. Riggio O, Angeloni S, Ciuffa L, et al. Malnutrition is not relatedto alterations in energy balance in patients with stable livercirrhosis. Clin Nutr 2003;22:553–559.
34. Cabré E, Abad-Lacruz A, Nunez M, et al. The relationship ofplasma polyunsaturated fatty acids deficiency with survival inadvanced cirrhosis: multivariate analysis. Am J Gastroenterol1993;88:718–722.
35. Muller MJ, Bottcher J, Seelberg O, et al. Hypermetabolism inclinically stable patients with liver cirrhosis. Am J Clin Nutr1999;69:1194–1201.
36. Madden A, Morgan M. Resting energy expenditure should bemeasured in patients with cirrhosis, not predicted. Hepatology
1999;30:655–664.
1738 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
37. Cabré F, Gassul M. Polyunsaturated fatty acid deficiency in liverdiseases: pathophysiological and clinical significance. Nutrition1996;12:542–548.
38. Cabré E, Gassul M. Feeding long-chain PUFA to advanced cir-rhotics: is it worthwhile? Nutrition 1999;15:322–324.
39. Duerksen DR, Nehra V, Palombo JD, et al. Essential fatty aciddeficiencies in patients with chronic liver disease are not re-versed by short-term intravenous lipid supplementation. Dig DisSci 1999;44:1342–1348.
40. Nanji A, Mendenhall C, French S. Beef fat prevents alcoholicliver disease in the rat. Alcohol Clin Exp Res 1989;13:15–19.
41. Piquet M-A, Roulet M, Nogueira V, et al. Polyunsaturated fattyacid deficiency reverses effects of alcohol on mitochondrialenergy metabolism. J Hepatol 2004;41:721–729.
42. Cabre Â, Gassull M. Nutritional aspects of chronic liver disease.Clin Nutr 1993;12(Suppl):S52–S63.
43. Sechi G, Serra A. Wernicke’s encephalopathy: new clinical set-tings and recent advances in diagnosis and management. Lan-cet Neurol 2007;6:442–455.
44. Levy S, Herve C, Delacoux E, et al. Thiamine deficiency inhepatitis C virus and alcohol-related liver diseases. Dig Dis Sci2002;47:543–548.
45. Newsome PN, Beldon I, Moussa Y, et al. Low serum retinollevels are associated with hepatocellular carcinoma in patientswith chronic liver disease. Aliment Pharmacol Ther 2000;14:1295–1301.
46. McClain CJ, Marsano L, Burk RF, et al. Trace metals in liverdisease. Semin Liver Dis 1991;11:321–339.
47. Lieber CS. Alcohol: its metabolism and interaction with nutri-ents. Ann Rev Nutr 2000;20:395–430.
48. Marchesini G, Bugianesi E, Ronchi M, et al. Zinc supplementsimprove glucose disposal in patients with cirrhosis. Metabolism1998;47:792–798.
49. van der Rijt CCD, Schalm SW, Schat H, et al. Overt hepaticencephalopathy precipitated by zinc deficiency. Gastroenterol-ogy 1991;100:1114–1118.
50. Reding P, Duchateau J, Bataille C. Oral zinc supplementationimproves hepatic encephalopathy. Results of a randomized con-trolled trial. Lancet 1984;2:493–494.
51. Riggio O, Ariosto F, Merli M, et al. Short-term oral zinc supple-mentation does not improve chronic hepatic encephalopathy.Results of a double-blind crossover trial. Dig Dis Sci 1991;36:1204–1208.
52. Aagaard NK, Andersen H, Vilstrup H, et al. Muscle strength, Na,K-pumps, magnesium and potassium in patients with alcoholicliver cirrhosis—relation to spironolactone. J Intern Med 2002;252:56–63.
53. Aagaard NK, Andersen H, Vilstrup H, et al. Magnesium supple-mentation and muscle function in patients with alcoholic liverdisease: a randomized, placebo-controlled trial. Scand J Gastro-enterol 2005;40:972–979.
54. Mobarhan S, Russell R, Recker R, et al. Metabolic bone diseasein alcoholic cirrhosis: a comparison of the effect of vitamin D2,25-hydroxyvitamin D of supportive treatment. Hepatology 1984;4:266–273.
55. Masuda S, Okano T, Osawa K, et al. Concentrations of vitaminD-binding protein and vitamin D metabolites in plasma of pa-tients with liver cirrhosis. J Nutr Sci Vitaminol Tokyo 1989;35:225–234.
56. Jorge-Hernandez JA, Gonzalez-Reimers CE, Torres-Ramirez A, etal. Bone changes in alcoholic liver cirrhosis. A histomorpho-metrical analysis in 52 patients. Dig Dis Sci 1988;33:1089–1095.
57. Collier J, Ninkovic M, Compston J. Guidelines on the manage-ment of osteoporosis associated with chronic liver disease. Gut
2002;50:1–9.58. Ormarsdóttir S, Mallmin H, Naessén T, et al. An open, random-ized, controlled study of transdermal hormone replacement ther-apy on the rate of bone loss in primary biliary cirrhosis. J InternMed 2004;256:63–69.
59. Campillo B, Richardet J-P, Bories P-N. Validation of body massindex for the diagnosis of malnutrition in patients with livercirrhosis. Gastroenterol Clin Biol 2006;30:1137–1143.
60. Pirlich M, Seiberg O, Boker K, et al. The creatinine approach toestimate skeletal muscle mass in patients with cirrhosis. Hepa-tology 1996;24:1422–1427.
61. Manning EMC, Shenkin A. Nutritional assessment in the criti-cally ill. Crit Care Clin 1995;11:603–634.
62. Diehl AM, Boitnott JK, Herlong HF, et al. Effect of parenteralamino acid supplementation in alcoholic hepatitis. Hepatology1985;5:57–63.
63. McGhee A, Henderson JM, Millikan WJ, et al. Comparison of theeffects of hepatic-aid and casein modular diet on encephalop-athy, plasma amino acids, and nitrogen balance in cirrhoticpatients. Ann Surg 1983;197:288–293.
64. Merli M, Romiti A, Riggio O, et al. Optimal nutritional indexes inchronic liver disease. J Parenter Enteral Nutr 1987;11(Suppl):130–134.
65. Heymsfield SB, Casper K. Anthropometric assessment of theadult hospitalized patient. J Parenter Enteral Nutr 1987;11:36S–41S.
66. Thuluvath PJ, Triger DR. How valid are our reference standardsof nutrition? Nutrition 1995;11:731–733.
67. Fiore P, Merli M, Andreoli A, et al. A comparison of skinfoldanthropometry and dual-energy x-ray absorptiometry for the eval-uation of body fat in cirrhotic patients. Clin Nutr 1999;18:349–351.
68. Figueiredo FA, Dickson ER, Pasha TM, et al. Utility of standardnutritional parameters in detecting body cell mass depletion inpatients with end-stage liver disease. Liver Transpl 2000;6:575–581.
69. Alvares-da-Silva MR, Reverbel da Silveira T. Comparison be-tween handgrip strength, subjective global assessment andprognostic nutritional index in assessing malnutrition and pre-dicting outcome in cirrhotic outpatients. Nutrition 2005;21:113–117.
70. Merli M, Riggio O, Dally L, et al. Does malnutrition affect survivalin cirrhosis? Hepatology 1996;23:1041–1046.
71. Selberg O, Selberg D. Norms and correlates of bioimpedancephase angle in healthy human subjects, hospitalized patients,and patients with liver cirrhosis. Eur J Appl Physiol 2002;86:509–516.
72. Zillikens MC, Van den Berg JWO, Wilson JHP, et al. Whole-bodyand segmental bioelectrical impedance analysis in patients withcirrhosis of the liver: changes after treatment of ascites. Am JClin Nutr 1992;55:621–625.
73. Cabre E, De Leon R, Planas R, et al. [Reliability of bioelectricalimpedance analysis as a method for nutritional monitorization inliver cirrhosis with ascites]. Gastroenterol Hepatol 1995;18:359–365.
74. Pirlich M, Schultz T, Spachos T, et al. Bioelectrical impedanceanalysis is a useful bedside technique to assess malnutrition incirrhotic patients with and without ascites. Hepatology 2000;32:1208–1215.
75. Detsky AS, Baker JP, Mendelson RA, et al. Evaluating the accu-racy of nutritional assessment techniques applied to hospital-ized patients: methodology and comparisons. J Parenter EnteralNutr 1984;8:153–159.
76. Plauth M, Cabre E, Riggio O, et al. ESPEN guidelines on enteralnutrition: liver disease. Clin Nutr 2006;25:285–294.
77. Morgan M, Madden A, Jennings G, et al. Two-component modelsare of limited value for the assessment of body composition in
patients with cirrhosis. Am J Clin Nutr 2006;84:1151–1162.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
May 2008 NUTRITION IN END-STAGE LIVER DISEASE 1739
78. Morgan M, Madden A, Soulsby C, et al. Derivation and validationof a new global method for assessing nutritional status inpatients with cirrhosis. Hepatology 2006;44:823–835.
79. Nompleggi D, Bonkovsky H. Nutritional supplementation inchronic liver disease: an analytical review. Hepatology 1994;19:518–533.
80. Patek A, Post J, Ralnoff O, et al. Dietary treatment of cirrhosis ofthe liver. JAMA 1948;139:543–549.
81. Riordan SM, Williams R. Treatment of hepatic encephalopathy.N Engl J Med 1997;337:473–479.
82. Kondrup J, Mueller MJ. Energy and protein requirements ofpatients with chronic liver disease. J Hepatol 1997;27:239–247.
83. Campillo B, Bories P, Pornin B, et al. Influence of liver failure,ascites, and energy expenditure on the response to oral nutri-tion in alcoholic liver cirrhosis. Nutrition 1997;13:613–621.
84. Hirsch S, Bunout D, De la Maza P, et al. Controlled trial onnutrition supplementation in out-patients with symptomatic al-coholic cirrhosis. J Parenter Enteral Nutr 1993;17:119–124.
85. Cunha L, Happi Nono M, Guibert AL, et al. Effects of prolongedoral nutritional support in malnourished cirrhotic patients: re-sults of a pilot study. Gastroenterol Clin Biol 2004;28:36–39.
86. Mendenhall CL, Bongiovanni G, Goldberg SJ, et al. VA coopera-tive study on alcoholic hepatitis III: changes in protein-caloriemalnutrition associated with 30 days of hospitalization with andwithout enteral nutritional therapy. J Parenter Enteral Nutr1985;9:590–596.
87. Cabre E, Gonzelz-Huix F, Abad A, et al. Effect of total enteralnutrition on the short term outcome of severely malnourishedcirrhotics: a randomized controlled trial. Gastroenterology1990;98:715–720.
88. Kearns PJ, Young H, Garcia G, et al. Accelerated improvement ofalcoholic liver disease with enteral nutrition. Gastroenterology1992;102:200–205.
89. De Ledinghen V, Beau P, Mannant PR, et al. Early feeding orenteral nutrition in patients with cirrhosis after bleeding fromesophageal varices? A randomized controlled study. Dig Dis Sci1997;42:536–541.
90. Cabre E, Gassull MA. Nutrition in liver disease. Curr Opin NutrMetab Care 2005;8:545–551.
91. Campillo B, Richardet JP, Scherman E, et al. Evaluation ofnutritional practice in hospitalized cirrhotic patients: results of aprospective study. Nutrition 2003;19:515–521.
92. Verboeket-van de Venne W, Westerterp K, Van Hoek B, et al.Energy expenditure and substrate metabolism in patients withcirrhosis of the liver: effects of the pattern of food intake. Gut1995;36:110–116.
93. Chang W, Chao Y, Tang H, et al. Effects of extra-carbohydratesupplementation in the late evening on energy expenditure andsubstrate oxidation in patients with liver cirrhosis. J ParenterEnteral Nutr 1997;21:96–99.
94. Cordoba J, Lopez-Hellin J, Planas M, et al. Normal protein dietfor episodic hepatic encephalopathy: results of a randomizedstudy. J Hepatol 2004;41:38–43.
95. Andus T. ESPEN guidelines on enteral nutrition: liver disease -tube feeding (TF) in patients with esophageal varices is notproven to be safe. Clin Nutr 2007;26:272.
96. Plauth M, Cabre E, Riggio O, et al. ESPEN guidelines on enteralnutrition: liver disease - tube feeding (TF) in patients with esoph-ageal varices is not proven to be safe. Clin Nutr 2007;26:273–274.
97. Keohane P, Attrill G, Grimble R, et al. Enteral nutrition in mal-nourished patients with hepatic cirrhosis and acute hepaticencephalopathy. J Parenter Enteral Nutr 1983;7:346–350.
98. Nasrallah SM, Galambos JT. Amino acid therapy of alcoholic
hepatitis. Lancet 1980;2:1276–1277.99. Simon D, Galambos JT. A randomized controlled study of pe-ripheral parenteral nutrition in moderate and severe alcoholichepatitis. J Hepatol 1988;7:200–207.
00. Plauth M, Roske AE, Romaniuk P, et al. Post-feeding hyperam-moniaemia in patients with transjugular intrahepatic portosys-temic shunt and liver cirrhosis: role of small intestinal ammoniarelease and route of nutrient administration. Gut 2000;46:849–855.
01. Naylor CD, O’Rourke K, Detsky AS, et al. Parenteral nutritionwith branched-chain amino acids in hepatic encephalopathy. Ameta-analysis. Gastroenterology 1989;97:1033–1042.
02. McCullough AJ, O’Connor JFB. Alcoholic liver disease: proposedrecommendations for the American College of Gastroenterol-ogy. Am J Gastroenterol 1998;93:2022–2036.
03. Cabre E, Rodriquez-Iglesias P, Caballeria J, et al. Short and longterm outcome of severe alcohol-induced hepatitis treated withsteroids or enteral nutrition: a multicenter randomized trial.Hepatology 2000;32:36–42.
04. Alvarez MA, Cabre E, Lorenzo-Zuniga V, et al. Combining ste-roids with enteral nutrition: a better therapeutic strategy forsevere alcoholic hepatitis? Results of a pilot study. Eur J Gas-troenterol Hepatol 2004;16:1375–1380.
05. Loser C, Aschl G, Hébuterne X, et al. ESPEN guidelines onartificial enteral nutrition--percutaneous endoscopic gastros-tomy (PEG). Clin Nutr 2005;24:848–861.
06. Khanna S, Gopalan S. Role of branched-chain amino acids inliver disease: the evidence for and against. Curr Opin NutrMetab Care 2007;10:297–303.
07. Mardini HA, Douglass A, Record C. Amino acid challenge inpatients with cirrhosis and control subjects: ammonia, plasmaamino acid and EEG changes. Metab Brain Dis 2006;21:1–10.
08. Bianchi G, Marzocchi R, Agostini F, et al. Update on nutritionalsupplementation with branched-chain amino acids. Curr OpinClin Nutr Metab Care 2005;8:83–87.
09. Iwasa M, Matsumura K, Watanabe Y, et al. Improvement ofregional cerebral blood flow after treatment with branched-chainamino acid solutions in patients with cirrhosis. Eur J Gastroen-terol Hepatol 2003;15:733–737.
10. Yamamoto M, Iwasa M, Matsumura K, et al. Improvement ofregional cerebral blood flow after oral intake of branched-chainamino acids in patients with cirrhosis. World J Gastroenterol2005;11:6792–6799.
11. Marchesinin G, Dioguardi FS, Bianchi G, et al. Long-term oralbranched chain amino acid treatment in chronic encephalopa-thy: a randomized double-blind casein-controlled trial. J Hepatol1990;11:92–101.
12. Plauth M, Egberts EH, Hamster W, et al. Long-term treatment oflatent portosystemic encephalopathy with branched-chainamino acids. A double-blind placebo-controlled crossover study.J Hepatol 1993;17:308–314.
13. Marchesinin G, Bianchi G, Merli M, et al. Nutritional supplemen-tation with branched chain amino acids in advanced cirrhosis: adouble blind, randomized trial. Gastroenterology 2003; 124:1792–1801.
14. Muto Y, Sato S, Watanabe A, et al; Long-Term Survival StudyGroup. Effects of oral branched-chain amino acid granules onevent-free survival in patients with liver cirrhosis. Clin Gastro-enterol Hepatol 2005;3:705–713.
15. Als–Nielsen B, Koretz RL, Kjaergard LL, et al. Branched-chainamino acids for hepatic encephalopathy. Cochrane DatabaseSyst Rev 2003;2:CD001939.
16. Strauss G, Knusden G, Kondrup J, et al. Cerebral metabolism ofammonia and amino acids in patients with fulminant hepaticfailure. Gastroenterology 2001;121:1109–1119.
17. Clemmesen J, Kondrup J, Ott P. Splanchnic and leg exchange ofamino acids and ammonia in acute liver failure. Gastroenterol-
ogy 2000;118:1131–1139.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
ISW
1740 O’BRIEN AND WILLIAMS GASTROENTEROLOGY Vol. 134, No. 6
18. Fukushima H, Miwa Y, Ida E, et al. Nocturnal branched-chainamino acid administration improves protein metabolism in pa-tients with liver cirrhosis: comparison with daytime administra-tion. J Parenter Enteral Nutr 2003;27:315–322.
19. Grimble RF, Grimble GK. Immunonutrition: role of sulfur aminoacids, related amino acids, and polyamines. Nutrition 1998;14:605–610.
20. Chawla R, Watson W, Eastin C, et al. S-adenosylmethioninedeficiency and TNF-alpha in lipopolysaccharide-induced hepaticinjury. Am J Physiol 1998;275:G125–G129.
21. Mato JM, Camara J, de Paz F, et al. S-Adenosylmethionine inalcoholic liver cirrhosis: a randomized placebo-controlled, dou-ble blind, multicenter clinical trial. J Hepatol 1999;30:1081–1089.
22. Roncaglia N, Locatelli A, Arreghini A, et al. A randomised con-trolled trial of ursodeoxycholic acid and S-adenosyl-L-methioninein the treatment of gestational cholestasis. BJOG 2004;111:17–21.
23. Rambaldi A, Gluud C. S-adenosyl-L-methionine for alcoholic liverdiseases. Cochrane Database Syst Rev 2006;19(2):CD002235.
24. Lieber CS, Leo MA, Aleynik S, et al. Polyenyphosphatidylcholinedecreases in alcohol-induced oxidative stress in the baboon.Alcohol Clin Exp Res 1997;21:375–379.
25. Lieber CS, Weiss DG, Groszmann R, et al, for the VeteransAffairs Cooperative Study 391 Group. II. Veterans Affairs Coop-erative Study of polyenylphosphatidylcholine in alcoholic liverdisease. Alcohol Clin Exp Res 2003;27:1765–1772.
26. Vanhorebeek I, Langouche L, Van den Berghe G. Tight bloodglucose control: what is the evidence? Crit Care Med 2007;35(Suppl):S496–S502.
27. Schultz T, Bechstein WO, Neuhaus P, et al. Clinical practice ofnutrition in acute liver failure: a European survey. Clin Nutr2004;23:975–982.
28. Kondrup J. Nutrition in end stage liver disease. Best Pract ResClin Gastroenterol 2006;20:547–560.
29. Shaw B Jr, Wood R, Gordon R, et al. Influence of selectedpatient variables and operative blood loss on six-month survivalfollowing liver transplantation. Semin Liver Dis 1985;5:385–393.
30. Deschennes M, Villeneuve JP, Dagenis M, et al. Lack of rela-tionship between preoperative measures of the severity of cir-rhosis and short term survival after liver transplantation. LiverTranspl Surg 1997;3:532–537.
31. Figuieredo F, Dickson ER, Pasha T, et al. Impact of nutritionalstatus on outcomes after liver transplantation. Transplantation2000;70:1347–1352.
32. DiCecco S, Wieners E, Wisener R, et al. Assessment of nutri-tional status of patients with end-stage liver disease undergoingliver transplantation. Mayo Clin Proc 1989;64:95–102.
33. Shahid M, Johnson J, Nightingale P, et al. Nutritional markers inliver allograft recipients. Transplantation 2005;79:359–362.
34. Bathgate A, Hynd P, Sommerville D, et al. The prediction ofacute cellular rejection in orthotopic liver transplantation. LiverTranspl Surg 1999;5:475–479.
35. Le Cornu KA, McKiernan FJ, Kapadia SA, et al. A prospective
randomized study of preoperative nutritional supplementation 0in patients awaiting elective orthotopic liver transplantation.Transplantation 2000;69:1364–1369.
36. Hasse JM, Blue LS, Liepa GU, et al. Early enteral nutritionsupport in patients undergoing liver transplantation. J ParenterEnteral Nutr 1995;19:437–443.
37. Reilly J, Mehta R, Teperman L, et al. Nutritional support afterliver transplantation: a randomized prospective study. J Par-enter Enteral Nutr 1990;14:386–391.
38. Gendall KA, Raniga S, Kennedy R, et al. The impact of obesityon outcome after major colorectal surgery. Dis Colon Rectum2007;50:2223–2237.
39. Keefe EB, Gettys C, Esquivel CO. Liver transplantation in pa-tients with severe obesity. Transplantation 1994;57:309–311.
40. Braunfield MY, Chan S, Pregler J, et al. Liver transplantation inthe morbidly obese. J Clin Anesth 1996;8:585–590.
41. Sawyer RG, Pelletier SJ, Pruett TL. Increased early morbidity andmortality with acceptable long-term function in severely obesepatients undergoing liver transplantation. Clin Transplant 1999;13:126–130.
42. Nair S, Cohen DB, Cohen MP, et al. Postoperative morbidity,mortality, costs and long term survival in severely obese pa-tients undergoing orthotopic liver transplantation. Am J Gastro-enterol 2001;96:842–845.
43. Heyland DK, Novak F, Drover JW, et al. Should immunonutritionbecome routine in critically ill patients? A systematic review ofthe evidence. JAMA 2001;286:944–953.
44. Plank LD, McCall JL, Gane EJ, et al. Pre and post operativeimmunonutrition in patients undergoing liver transplantation: apilot study of safety and efficacy. Clin Nutr 2005;24:288–296.
45. Riordan SM, Williams R. The intestinal flora and bacterial infec-tion in cirrhosis. J Hepatol 2006;45:744–757.
46. Wiest R, Garcia-Tsao G. Bacterial translocation (BT) in cirrhosis.Hepatology 2005;41:422–433.
47. Rayes N, Seehofer D, Hansen S, et al. Early enteral supply oflactobacillus and fiber versus selective bowel decontamination:a controlled trial in liver transplant patients. Transplantation2002;74:123–128.
48. Rayes N, Seehofer D, Theruvath T, et al. Supply of pre- andprobiotics reduces bacterial infection rates after liver transplan-tation—a randomized double blind controlled trial. Am J Transpl2005;5:125–128.
49. Liu Q, Zhong PD, Ha DK, et al. Synbiotic modulation of gut flora:effect on minimal hepatic encephalopathy in patients with cir-rhosis. Hepatology 2004;39:1441–1449.
50. Loguercio C, Federico A, Tuccillo C, et al. Beneficial effects of aprobiotic VSL#3 on parameters of liver dysfunction in chronicliver disease. J Clin Gastroenterol 2005;540–543.
Received November 28, 2007. Accepted February 1, 2008.Address requests for reprints to: Alastair O’Brien, BSc, MBBS, PhD,
nstitute of Hepatology, Royal Free and University College Medicalchool, University College London, 69 - 75 Chenies Mews, LondonC1E 6HX, England. e-mail: a.o’[email protected]; fax: (44) 207 380
405.





























