Embed Size (px)
Citation preview

Nurse Educatta Today (1988) 8,26&272 0 Longman Group UK Ltd 1988
Nurses’ perceptions of their interpersonal skills: a descriptive study using Six Category Intervention Analysis
Philip Burnard and Paul Morrison
This study used Heron’s (1986) Six Category Intervention Analysis to investigate 93 nurse’s self-perceptions of their interpersonal skills. The nurses were asked to rank order six intervention categories in terms of their perceived level of skills. It was found that a majority described themselves as being more authoritative in their interpersonal style and less facilitative. Some notable exceptions were observed and these are also reported here. Reasons for the findings in this study are offered and limitations of it are considered. The study has implications for the training and evaluation of nurses in the field of interpersonal skills.
INTRODUCTION
Interpersonal skills training is becoming an important aspect of nurse education. There has been a trend towards using models and methods of skills development, based on a variety of psychological approaches (French 1982, Kagan 1985, Hussey 1981). Our interest was in attempt- ing to identify how nurses viewed their own interpersonal competing. If interpersonal skills training is to progress, it would seem vital that we first assess the levels of skills that nurses believe they have. It is one thing to prescribe skills and training methods and quite another to attempt to assess skill levels.
This paper identifies a framework (six cat- egory intervention analysis) for classifying inter-
Philip Burnard MSc RMN RGN DipN Cert Ed RNT, Paul Morrison BA (Hon.4 RMN RGN Lecturer in Nursing Studies, School of Nursing Studies, University of Wales College of Medicine, Heath Park, Cardiff (Reprint requests to PB) Manuscript accepted 27 May 1988
266
personal skills in a wide variety of clinical and other situations. An aim for the study is offered, followed by a description of the methodology and a discussion of the findings. The study may have implications for the further development of theory and practice in the domain of inter- personal skills training for nurses.
Six Category Intervention Analysis
The conceptual framework known as Six Cat- egory Intervention Analysis was developed by John Heron (1975, 1986), building on the work of Blake and Mouton (1976). It was offered as a conceptual model for understanding inter- personal relationships, and as an assessment tool for identifying a range of possible therapeutic interactions between two people.
The six categories in Heron’s analysis are: prescriptive (offering advice), informative (offering information). confronting (challeng- ing), cathartic (enabling the expression of pent- up emotions), catalytic (‘drawing out’) and

KURSE EDUCATIOfi ‘I‘ODAY 267
supportive (confirming or encouraging). The
word ‘intervention’ is used to describe any
statement that the practitioner may use. The
word ‘category’ is used to denote a range of related interventions (Table 1).
Heron (1986) calls the first three categories of intervention, (prescriptive, informative and con- fronting), ‘authoritative’ and suggests that in
using these categories the practitioner retains
control over the relationship. He calls the second
three categories of intervention (cathartic, cata-
lytic and supportive), ‘facilitative’ and suggests
that these enable the client to retain control over the relationship. In other words, the first three
are ‘practitioner-centred’ and the second three are ‘client-centred’. Heron further argues that
all six categories are of equal status and no one category is more important than any other. In
contradiction, however, he also argues that cata- lytic interventions should form the ‘bedrock’ type of intervention on which effective interper-
sonal communication could be developed.
On another occasion (Heron 1977) offers the
opinion that because we live in a ‘non-cathartic
society’, where the open expression of emotion is not highly valued, the cathartic category will
tend to be less skilfully used by many people. This is a debatable point and one worthy of considerable discussion though such discussion
is beyond the remit of this paper. Heron claims that his analysis should not be
used to classify people’s behaviours but should serve as a means of helping people to clarify their
inte?llions in a therapeutic situation. Thus the
present research aimed at asking people about their therapeutic intentions in clinical situations.
The question remains, of course, as to the degree
to which researchers can have access to people’s intentions, after the event. On the other hand, it is equally difficult to ask people to assess their own behauiour after the event.
Table 1 Authoritative and facilitative categories
Authoritative Facilitative Categories Categories
1. Prescriptive 4. Cathartic 2. Informative 5. Catalytic 3. Confronting 6. Supportive
Prior to the present research, lronbar (1983)
had discussed the value of the category analysis
and its applications to psychiatric nursing. Hammond (1983). in the context of psychiatric
nurse education noted that the category analysis could be used in two ways:
a) as a means of interpreting nurse/patient interventions
b) as an aid to the nurse during counselling sessions.
Goodwin and Bond (1978) had called for the development of catalytic and cathartic skills
development, .as per the category analysis, in
health visitors. Bond and Kilt): ( 1983) described
the application of the category analysis for use in peer support groups. The use of the category analysis in interpersonal skills training and
counselling skills development had been de-
scribed elsewhere (Burnard 1983; 1984; 1985).
Training in the use of the category analysis is
offered by the Human Potential Research Pro- ject at the University of Surrey and that training
is endorsed by the E.N.B. (Nicholas 8c Gooder- ham 1982). One of the present writers (PB) had
received training in the category analysis from John Heron at that institution.
It is important to note, however. that Heron’s category analysis does not appeal- to have been
generated out of empirical research but was
devised from ,a theoretical starting point. No evidence could be found of an)- other published
research that tested out Her-on’s categork analysis.
Aim of the study
The aim of the present study b-as to identify some trained nurses’ perceptions of their own interpersonal ability. The analytical framework
used for the study was the above six categor? analysis. The methodology of thr study is now described.
Design of the study
An accidental sample (Fink 8c Kosecoff 1985) was used. An accidental sample is one that is

268 NURSE EDUCATION TODAY
obtained through participants being readily available and willing to take part in the study. Data were collected at workshops on interper- sonal and counselling skills development run by one of the present authors (PB). These workshops were conducted across several health authorities for qualified nurses of diverse back- grounds. During the early stages of these workshops the six category framework was introduced and an accompanying handout pro- vided respondents with a synopsis of the six category scheme Table 2.
Table 2 Synopsis of the Six Category Intervention Analysis
Category
1. Prescriptive
2. Informative
3. Confronting
4. Cathartic
5. Catalytic
6. Supportive
Nature of intervention
To offer advice, make suggestions, etc
To give information, instruct, impart knowledge, etc
To challenge restrictive or compulsive verbal or non-verbal behaviour
To enable the release of emotion through tears, angry sounds, etc
To be reflective, to ‘draw out’ through the use of questions, reflections, etc
To offer support, be validating, confirming, etc
Following a period of introduction and fam- iliarisation with the category analysis, members of each workshop were invited to take part in the study by completing a short ranking exercise. Specifically, each respondent was asked to rank order the six category items to correspond with how skilled they perceived themselves to be while interacting with others. The ‘interacting’, here, refers to any interaction: with patients, friends, family and so forth. A rank position of 1 was equivalent to ‘most skilled’, whilst a rank position of 6 indicated ‘least skilled’. In this way each of the categories was considered in relation to the others. The order of the categories on the response sheet was randomised to avoid influencing the order in which respondents completed the task.
Background information about the sex of the individual, the speciality in which they currently
work and the number of years in nursing was also collected (Table 3). Participation was volun- tary and none refused to take part. All replies were treated confidentially but respondents were forewarned of our intention to publish the overall results.
It is acknowledged that the sampling pro- cedure did not allow for generalisation of the findings to all nurses. The results do, however, offer some interesting perspectives on some nurses self-perceptions of their interpersonal skills. As we have identified above, this is a crucial and developing area of nursing concern.
Table 3 Sample characteristics (n = 93)
Sex Nursing speciality Time in nursing
Male 18 General 63 <5years 17 Female 75 Psvchiatrv 28 5-10vears 29
Mental handicap 2 11-15 vears 23 > 15years 24
Totals 93 93 93
Analysis of data
The analysis procedure involved counting the frequency with which each of the six categories were ranked in position 1, position 2, position 3 and so on across the group as a whole. A total picture of how ‘skilled’ these nurses perceived themselves thus emerged. To date, none of the demographic variables have been considered. A future extension of the study with increased numbers should yield a more detailed analysis. However, the emergent pattern of responses mapped out below has presented a useful start- ing point. Trends evident from these data are notable, if not surprising.
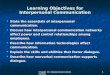
Figure 1 presents the results on a series of histograms. The top half of the figure represents the authoritative categories, while the lower section deals with the facilitative categories. Notable trends are evident.
Generally the nurses perceived themselves as more skilled in the authoritative categories and less skilled in the facilitative categories, 67 (72%) chose ranks 1, 2 and 3 and in the prescriptive

50
10
30
20
g 10 i= z Z z Y
z & > z
3 50
z
40
30
20
10
PRESCRIPTIVE INFORMATIVE CONFRONTING
32 30
27
123456
CATHARTIC CATALYTIC SUPPORTIVE
35
~
11 9 9
19
10
II 123156 1234 5 6 123156
RANKED POSITION (‘-61 1 -Most skilled 6 r Least skilled
Fig 1 Authoritative and facilitative categories
21
il f 1 2 3
category; 78 (84%) chose ranks 1, 2 and 3 in the informative category. In the confronting cat- egory, however, only 10 (11%) chose ranks 1, 2 and 3. Thus whilst a large proportion perceived themselves as being skilled in prescription and information giving, a considerably smaller pro- portion perceived themselves as skilled in con- frontation. It is notable, also, that 83 (89%) ranked this latter category in positions 4,5 and 6, thus identifying themselves as weak at confron- tation. Indeed, the confronting category was the one most frequently ranked in the sixth, (least
NURSE EDUCATIOK TODAY 269
46 P - c r
123456
skilled) position: 46 (49%,). A different picture emerged for the facilita-
tive categories. A majority of the sample, 82 (88%), placed catharsis in the 4, 5 and 6 rank positions, while 11 (12%) ranked it higher. A smaller majority, 64 (69%), ranked the catalytic category in positions 4, 5 and 6 but 29 (31%~), ranked it in positions 1,2 and 3. The supportive category, however, differed from the other two facilitative categories, in that 89 (95%) ranked it in positions 1, 2 and 3. Indeed the supportive category was the one most frequently ranked in
El

270 NURSE EDUCATION TODAY
the first (most skilled) position, 43 (46%). Figure 1 highlights, more graphically, the differences between the nurses’ perceptions of their ability to use authoritarian interventions versus their ability to use facilitative interventions.
DISCUSSION
In summary, then, it is noteworthy that this group of nurses, from a variety of backgrounds, generally saw themselves as being most skilled in being prescriptive, informative and supportive and least skilled in being cathartic and confront- ing. In the catalytic category, the results were less clear cut: the pattern of ranking was not so clearly distributed as was the case with the other categories. It is notable, too, that there were individual exceptions to these patterns. For example some nurses identified themselves as being most skilled in cathartic interventions and some identified themselves as being least skilled in being supportive. These exceptions need to be born in mind when considering the results of this study. Even though there are pointers that this group of nurses had certain skills and lacked others, individual idiosyncracies also need to be considered before planning interpersonal skills training courses.
In general, the results support Heron’s (1975) statement that a wide range of practitioners in our society show a much greater deficit in the skillful use of facilitative interventions than they do in the skilful use of authoritative ones. Whether or not this is viewed as an important fact depends upon ones’ view of therapeutic intervention. Clearly, Heron’s position is that nurses (alongside other practitioners) should
develop skills in being both facilitative and authoritative.
This view would be further supported by the literature on client-centred counselling (Rogers 1951, 1967), student-centred teaching (Rogers 1983; Postman and Weingartner 1971) and patient-centred nursing care (Little & Carvnevali 1976, Hunt & Marks-Moran 198 1, Yura 8c Walsh 1978). Indeed, if anything, these client-centred approaches would emphasise the facilitative approach. Cassee’s (1975) study of communica-
tion between patients and nurses also notes the importance of free expression of emotion and of patients being allowed to talk through their problems - further evidence of the need for nurses to develop facilitative skills. However, this present study indicates that this group of nurses do not describe themselves as being particularly facilitative. This study is a report of nurses’ perceptions rather than a study of nurses’ behav- iour. There may be considerable differences between how nurses’ perceive themselves and what they do in practice. Moreover, the authori- tative approach may be more effective, in certain circumstances, particularly in the field of information giving (Devine & Cook 1983).
It is worth speculating on some of the factors which may contribute to these nurses perceiving themselves as not particularly facilitative. First, comes the question of how we construe the consequences of our actions. For example, if we encourage someone to cry, can we cope with them when they do? If we encourage someone to talk through their problems, can we deal with any overt anger that they may express? This leads on to the issue of training. It is quite possible that many nurses do not receive training in:
a) using a range of therapeutic interventions b) coping with the expression of personal
problems and emotion.
Third, in clinical settings, the ‘organisational culture’ (Sathe 1983) may not encourage nurses to invite patients to talk about their problems, nor does such an organisational culture promote what Cassee (1975) called ‘open, two-way com- munication’. Again, in the clinical situation, the problem of time, work and perceived priority constraints may influence the degree to which nurses are prepared to be facilitative. This must be a short list of possible explanations that cannot claim to be exhaustive.
It is possible to identify problems arising out of the use of the six category intervention analysis framework. One readily identifiable difficulty may be Heron’s use of descriptors for the categories. Whilst the word ‘informative’, ‘con- fronting’ and ‘supportive’ may be familiar to many people in a variety of contexts, the words

NURSE EDUCATION TODAY ?i 1
‘prescriptive’, ‘cathartic’ and ‘catalytic’ may not.
It is possible, therefore, that the choice of words may have been influential when inviting people to identify their strengths and weaknesses within the range of categories. The category that fre- quently presented people in the sample with difficulty was the ‘catalytic’ category. Developing the above argument regarding understanding the meanings of words, there are at least three possible explanations for this. First, the word has a clear definition already established in the world of chemistry. Second, the word may not be a familiar one. Third, the types of interventions that Heron calls ‘catalytic’ are not so readily identifiable with that word as are, for example, the interventions associated with the word ‘supportive’ and ‘informative’. All of these factors and others, may affect the results of the research.
sorts of interpersonal skills are called for in
different sorts of situations. Lastly, there has been great emphasis placed
on information sgiving in nursing, in recent years (Hayward 1975; Boore 1978; Devine 8c Cook 1983; Engstrom 1984). It may be that nurses expect that an important part of their role is giving information to other people and thus this expectation may have influenced the outcome of the present study.
CONCLUSIONS
LIMITATIONS OF THE STUDY
Some limitations of the study may be noted. First, the sample may have biased results in the sense that people who perceive deficiencies in their own interpersonal performance may be highly motivated to attend counselling skills workshops. This study did not address the responses of those nurses who have not attended interpersonal skills workshops.
Second, we are assuming that practising nurses due interpersonal competence and aspire towards interpersonal expertise in clinical work settings. It is possible that some nurses do not give very much thought to the issue of whether or not they are interpersonally skilled or whether or not they need to be.
This paper has described a study into the per- ceptions of nurses with regard to their interper- sonal skills level. It has describecl the aim of the study, outlined the methodology and drawn tentative conclusions that indicate that some nurses perceive themselves as being more authoritative in terms of the six category analysis than facilitative. It has also offered some sug- gestions as to why those nurses may perceive themselves in that way. The research also answers the criticism made by Kasch (1984) that there has been a lack of clear theoretical guidelines as to how to investigate interpersonal competence in nurses. This offers a lirst step towards the self-assessment 01‘ interpersonal performance by nurses. A second stage of the research is now nearing completion: the explor- ation of student nurses’ views of their interper- sonal ability. This will be reported at a later date. If interpersonal skills training is to be appro- priate and effective, it would seem vital that we consider how the nurses, themselves, view their own skill level. This must be an important prerequisite to interpersonal skills training.
Third, problems arise over the use of a forced choice ranking exercise. When people are forced to choose one item in place of another, the activity may become rather artificial. It would be interesting to test nurses self perceptions using a more flexible rating format, at a later date.
Fourth, no acknowledgement was made of any differences that there may be in nurses’ interper- sonal performance in the clinical setting and in other sorts of settings. It may be that different
References
Blake R R, Mouton J S 1976 Consultation. Addison Wesley, New York
Bond M. Kitty J 1983 Practical methods of dealing with stress: Human Potential Research Project. I:niversity of Surrey, Guildford
Boore J 1978 A prescription for recovery. RCN. London
Burnard P 1983 Through experience and from experience. Nursing Mirror 156, 9: 29-34
Burnard P 1984 Counselling the counsellors. Nursing

272 NURSE EDUCATION TODAY
Mirror 159,40: 30-31 Burnard P 1985 Learning human skills: a guide for
nurses. Heinemann, London Burnard P 1987 Self and Deer assessment. Senior Nurse
1
6, 5: 16-17 Cassee E T 1975 Therapeutic behaviour, hospital
culture and communication. In C Cox and A Mead (eds). A Sociology of Medical Practice. Collier- Macmillan, London, 224-234
Devine E C, Cook T D 1983 A meta-analytical analysis of effects of psychoeducational interventions on length of postsurgical hospital stay. Nursing Research 32,5: 267-274
Engstrom B 1984 The patients need for information during hospital stay. International Journal of Nursing Studies 21: 113-130
Fink A, Kosecoff J 1985 How to conduct surveys. Sage, Beverly Hills, California
French P 1982 Social skills for nursing practice. Croom Helm, London
Goodwin S, Bond M 1987 Nursing humans. Self and Society: European Journal of Humanist Psychology 6, 11: 382-387
Hammond G H 1983 A clutch of concepts. Nursing Mirror May: 3435
Hayward J 1975 Information: a prescription against pain. RCN, London
Heron J 1975 Six category intervention analysis. Human Potential Research Project, University of Surrey, Guildford
Heron J 1977 Catharsis in human development. Human Potential Research Project, University of Surrey, Guildford
Heron J 1986 Six category intervention analysis. 2nd revised edition. Human Potential Research Project,
University of Surrey, Guildford Hunt J, Marks-Moran D J 1981 Nursing care plans: the
nursing process at work. HM and M, London Hussey A 1981 Interpersonal communication skills in
nursing. Unpublished MSc dissertation, Aston University, Birmingham
Ironbar 0 1983 Self instruction in psychiatric nursing. Balliere, Tindall, London
Kagan C (ed) 1985 Interpersonal skills in nursing: research and applications. Croom Helm, London
Kasch C R 1984 Interpersonal competence and communication in the delivery of nursing care. Advances in Nursing Science 6, 2: 71-88
Kilty I 1979 Self and peer assessment. Human Potential Research Project, University of Surrey, Guildford
Little D. Carnevali D 1976 Nurse care olannina. Harner and Row, New York
Nicholas B, Gooderham D 1982 Mental Nursing 1: Devising and implementing new syllabuses for mental and mental handicap nurse training. Nursing Times, March 17th, pages marked: Quest 2 and 3
Postman N, Weingartner C 1971 Teaching as a subversive activity. Penguin, Harmondsworth
Rogers C R 1951 Client-centre therapy. Constable, London
Rogers C R 1967 On becoming a person. Constable, London
Rogers C R 1983 Freedom to learn for the eighties. Merril, Ohio
Sathe V 1983 Implication of corporate culture: a manager’s guide to action. Organisational Dynamics 12,5-23
Yura H, Walsh M B 1978 Human needs and the nursing process: philosophy, theory, concept, process. Appleton-Century-Croft, New York.