Embed Size (px)
Citation preview

Review of Chapter Nine
Overview of the Micro and Macro Levels of the Four Brain Systems
• Phases of Step 3• Moving Inside & Outside of Four Brain Systems• Functional Behaviors Within the Four Brain Systems• Four Macro Uses of the Four Brain Systems• History Worksheet• History Worksheet Combined w/Needs Assessment• Four Stories Interviews (links w/History & Functional Capacities)• Cultural Awareness of Ourselves and the 4 Brain Systems
Supplemental Textbook Reading will now accompany these four Brain System Chapters. Each brain system in the textbook has two chapters to it. The first chapter will review the behaviors and functional capacities of each Brain System and the second chapter will review the assessment and intervention priorities. The Regulation System’s Chapters are Chaps four and five, which were recommended during Step One as well.
Chapter Ten, Regulation Brain System. Step #3, Intermediate Learning Phase
One of the primary strengths of Step Three is the capacity to orient to Triggers and to Toolkits, with learning the functional capacities within each brain system. In order to actually use the Trigger/Toolkit paradigm with confidence, and not in a rote way, choosing things off of a menu, the NRF has given you e functional capacities within each brain system. These range in number from two (sensory) up to six (regulation). They are designed to help you understand the functional behaviors that are associated with each brain system. As you know, the balance of flexibility with stability is a large theme defining “health” within the NRF. Thus, there always will be at least one functional capacity the represents flexibility and another one that represents stability, carrying our theme of health throughout.
It is important at this juncture to really understand the reason why learning these Functional Capacities is going to help you! Each brain system has a set of functional capacities that capture the meaning of the behaviors within each brain network. They are the underpinnings to understanding the origins of Triggers for the adaptive or toxic stress patterns and they highlight the Toolkits and strengths that can be used for building resilience. All of the “micro” levels to Step Three lead to the practitioner being more capable of identifying the multiple Triggers involved in a Stress Response Pattern and helping the family being able to address these.
The good news about the Regulation System is that by the time you get to this phase of your learning, you likely have covered each of these functional capacities – either in Step One’s stress and stress recovery voyage or in the “early story” interview process. The grid below connects you to how you likely already know the strengths and challenges of each of these from previous contact and observation with the child and caregivers. Much of the information you have already gathered will now be used to flush out the strengths and vulnerabilities of the Regulation System.
1

Six Functional Capacities of the Regulation System
1. Capacity for deep sleep cycling You know about the sleep cycle from the Step #1 interview. The NRF always begins with understanding the sleep cycle as the background to the awake cycle.
2. Capacity for the “green” zone Again, the amount of time spent in the “green” zone has been assessed in Step #1. This is always the first goal of everyone on the team - to expand that green zone in all contexts – from the school setting to the home.
3. Capacity for all three stress responses, either in an adaptive or toxic stress pattern
By spending time in Step #1, one should know whether there is a toxic pattern or not at play. There are 4 toxic patterns, otherwise known as “allostatic load.” These are when the stress response(s) (any of the 3 colors) occur:
1. Stress occurs too quickly and too frequently2. Stress lasts too long3. Stress challenge does not habituate over time4. There is no recovery to green and sleep may
be disrupted
4. Capacity for organized states with smooth transitions
When each state of arousal has clear markers and one can clearly tell the difference between each state of arousal, we refer to this as an “organized” state. In contrast, there may be infants, children, youth, and adults, where they have behavioral markers from all three stress zones and we would consider this a more “muddy” state.
With a well-organized nervous system, there are slow state shifts, wherein one moves up and down the daytime and nighttime arousal curve smoothly. In contract, if one shifts upwards instantly – such as from green to red, or shifts downward quickly – such as from red to asleep, these are fast transitions and usually connote a less organized nervous system.
5. Capacity to be connected to visceral cues This information has been suggested to be reviewed in the “early story” interview process. This pertains to the infant/child/youth/adult’s capacity to recognize
2

hunger, thirst, pain, temperature, wetness, fatigue, bowel, and bladder cues, communicating them clearly to his or her caregiver. As one matures, this relates to honoring his or her own cues and being able to attend to one’s self-regulation and self-care.
6. Capacity for efficient stress recovery This would be clear from Step #1. If there is a toxic stress pattern, there is not an efficient stress recovery system in place. If there is adaptive stress, there would be.
This slide highlights a distribution of how one will be able to get a “take” on each functional capacity as one works through Step #1 and Step #3. For further details on these functional capacities, please read Chapters 4 and 5 in the NRF Textbook.
Summary of Macro and Micro Sources:
The primary Triggers from this brain system have to do with vulnerabilities from the in utero experience, labor and delivery, the postpartum period of time, and one’s core visceral cues. Certainly feeding, sleeping, elimination, and pain triggers are high on the list.
3

Stability with Flexibility: Recall that the NRF’s definition of health across all of the brain systems comes from the core principle of Allostasis – flexibility with stability. Adaptive stress is healthy!
Stability Within the Regulation System: The stability of the regulation system is found in two of the six functional capacities – the capacity for deep sleep and the capacity for the green zone. These are states of arousal that support the infant/child/youth/adult showing they are experiencing conditions of safety. These are also signs of Resilience!
4

Flexibility Within the Regulation System: Flexibility is represented by being able to have all THREE stress responses. All three of these stress responses are inherently healthy! This is a neutral way to introduce Step One to all families. We all have stress that can be healthy and at times it can become unhealthy.
5

One can have a pretty good sense of now the stress patterns and what contributions come from the regulation system. There is now cumulative data that you have organized from multiple sources:
- the early story interview
- the strengths and risk Factors (prenatal, in utero, medical, etc.) on the History Worksheet from the Regulation System
- the strengths and risk factors from the Regulation’s Functional Capacities
To document the functional capacities, we return to the Early Phase Assessment Regulation form (pages 1 to 2 or 12 to 14 in the long form) to fill it out, with strengths and concerns listed here.
Go to the Early Phase Assessment Regulation Form, page 1 (or page 12 in the long version of the Early Phase Assessment Form). The top of page 1 is a space where you can list now all of the risk factors in a way that helps you visually see where they are weighted. We often take one dyad and look at their risk factors in relationship to each other as well. As mentioned in Chapter Nine, the cumulative score can be useful for looking at the “whole” of the big picture.
Go to the Graphical Display for History Worksheet, Strengths and Vulnerabilities Posted in Chapters 9 and 10. Enter in the exact number per person and per brain system, and they will shift to display the configuration you have inputted.
6

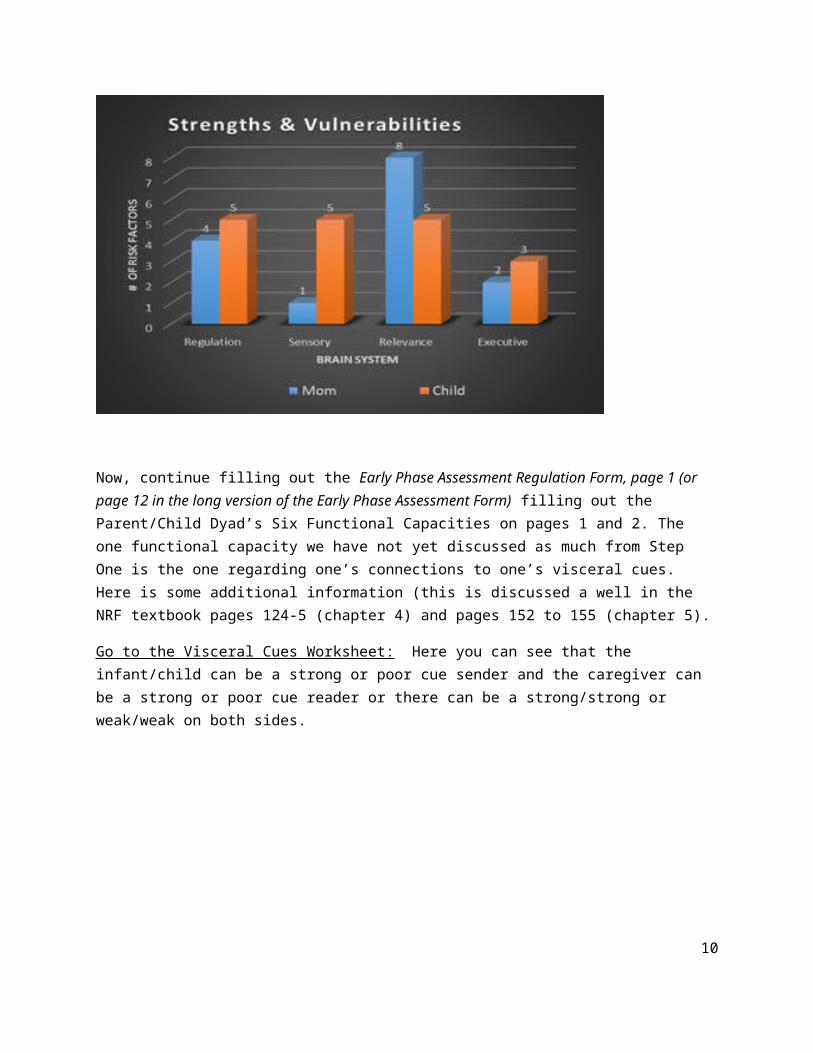
Based upon the count, there can be cases where one sees the strengths and vulnerabilities very clearly and other cases where all the systems are impacted.
For example, in this case history with the graphical display slide below, it is easy to see that the child has vulnerabilities across all networks. Whereas the mother has strengths in her sensory and executive system, there is a great deal of vulnerability in her Relevance System, in conjunction with her Regulation System. This gives you an idea of where the work may be weighted and if you might need additional supports from other disciplines for yourself.
Now, continue filling out the Early Phase Assessment Regulation Form, page 1 (or page 12 in the long version of the Early Phase Assessment Form) filling out the Parent/Child Dyad’s Six Functional Capacities on pages 1 and 2. The one functional capacity we have not yet discussed as much from Step One is the one regarding one’s connections to one’s visceral cues. Here is some additional information (this is discussed a well in the NRF textbook pages 124-5 (chapter 4) and pages 152 to 155 (chapter 5).
Go to the Visceral Cues Worksheet: Here you can see that the infant/child can be a strong or poor cue sender and the caregiver can be a strong or poor cue reader or there can be a strong/strong or weak/weak on both sides.
7

Are signals being sent that very weak and hard to read or really strong and very clear? For example, some babies do not cry nor show much interest in feeding and it’s hard to know if they are hungry. This might be understood as an “undershoot.” Others may cry loudly, yet they cry regularly and are inconsolable, where the cry is not readily distinguished from a tired, hungry, wet diaper cry, etc. This might be understood as an “overshoot” where there is a lot of communication yet the clarity is subtle or missing. With these types of cue senders, it is much more difficult to “read”, so even an empathic parent, typically a good cue reader, may have trouble discerning the meaning of the signals.
These early cue sending and reading experiences are often early ways in which the dyad experiences a “match or mismatch” or a “goodness of fit.” There are many different types of dyadic matches and mismatches that we will see. One of them is in relationship to these early sending/reading cues surrounding hunger, satiation, thirst, fatigue, drowsy, pain, bowel/bladder, and temperature.
8

Different cultures value certain approaches that may not necessarily match a western approach to cue reading. For example, an Ethiopian practitioner showed our IMH class I was teaching a video clip that looked like “over-feeding” to many of us. From her cultural perspective she explained that this way of feeding was normative and to do otherwise would be considered neglect. Another parent told me that her Chinese in-laws believed that young children could get ill from being cold, always commanding their grandson to wear a shirt, regardless of the climate temperature. Even though her son complained of being too hot and was indeed, heat sensitive, she was torn between honoring her husband’s parents (important to the culture) or honoring her son’s pleas to take his shirt off.
When the “visceral self” is missing in young children, youth, or adults, one may have this is an early treatment goal that may take some time to accomplish. Connecting to one’s internal cues can be a part of how one gains an awareness of one’s external stress responses at the same time. So, if parents are learning how to “read” externally driven behaviors, one might include becoming a scout for these more internal cues as well. When this is too much information for a parent to keep track of, the NRF therapist helps slow that down so that they are focusing their energy on what’s most important. If the child is suffering from constipation and red zone behaviors, both, while they may be exacerbating each other, one may have to decide where to place the emphasis. Sometimes, becoming more clued in to a child’s internal body world is seen as an empathic gift, helping him or her feel safe. Other times, it may be experienced as too intrusive, so these are clinical decisions that are made with the parent’s capacities in mind and the child’s experiences in mind, together.
Regulation Treatment Guidelines:
One of the first set of guidelines is for parents to place the oxygen mask on themselves, FIRST, before trying to help co-regulate his or her child. As mentioned, there are really three clients that one has – the parent, the child, and the relationship. This is challenging and whenever possible, helping the parent get
9
and stay green is critical to the long-term success. This means that parents have to be engaged in reading their own colors and looking for resources for stress recovery on a self or “other” (co-regulation) level. Not all parents are open to their being the focus at the front end! So, being flexible and prioritizing the child’s regulatory status often can be the “way-in”. As his or her child increases his or her green zone, parents often can begin to relax and can become more curious about their own needs as well. So sometimes the work begins with the child’s needs as front and center.
Of course, this principle of self-care applies to practitioners as well, and as part of the healing profession, we are often poor at this, ourselves! If you notice yourself in toxic stress, this becomes a priority. Without self-care we will experience vicarious trauma and burn out ourselves.
IDENTIFYING REGULATION STRESS TRIGGERS, MACRO AND MICRO
Whether its parent or child or ourselves, identifying our own triggers are key. This slide gives you suggestions, yet individualizing our own bodily needs and external stressors is paramount. These pictures are meant to convey basic needs for food, healthy nutrition, bodily and medical health, shelter, and fiscal climates are to be considered. For some, a recession becomes a huge stressor. For others who do not own a home or live at the poverty level, the middle class crunch may not affect them as much. The picture of the grandfather and baby signify the set of parents who are both raising their children and caring for an elderly parent.
10
The History Worksheet provides some clues as to what triggers may exist on a historical or macro level.
The Micro level triggers are often embedded or identified through the brain system’s Functional Capacities. Cycling back to these is always a good idea for catching stress triggers that may be present.
11
Being aware of where stress resides in one’s body is critical for self-care. For example, my stress happily locates itself in my shoulders and neck. For my self-care it is critical for me to regularly receive chiropractic adjustments to maintain my spinal and neck flexibility, for me to get weekly massages for me to unwind from the build-up of stress in my neck, and for me to nightly apply heat and massage to this area. I literally travel with a shoulder massager that applies mechanical massage and heat! I am able to very quickly relax with this help, aiding my cycling into sleep as well. While some may see getting a weekly massage a luxury, and it is, it is also a necessity for my personal health care.
IDENTIFYING STRESS RECOVERY TOOLKITS
12

Orientation to Triggers & Toolkits from the Regulation System: There can often be a rather simple 1:1 correlation with the regulation triggers. If there is fatigue, there needs to be more rest. If one is hungry, one needs to eat.
However, sometimes what looks like a simple solution is not so simple. For example, these visceral cues can be either difficult to “find” in one’s body, either due to poor interoceptive links within one’s body or due to years of a poor cue reading and responsive environment or both. Other times there are additional vulnerabilities that make something “simple” is very hard to do. For example, a premature infant that had a feeding tube down his or her throat may now be averse to eating due to the historical trauma and procedural memory of a gag reflex that occurs when one swallows. This may lead to years of difficulty with chewing and swallowing food once the tube is no longer present. All of these individual differences need to be sorted through.
For whatever the reason, when there is a lack of visceral connections to one’s bodily cues, a personal and family goal might be to get more connected. The following chart provides suggestions as to how one can connect to bodily cues that may have been disconnected or dissociated from for long periods of time. Building bodily awareness to one’s visceral self allows one to be able to begin to notice one’s stress responses! Without knowing one is having a stress response, its challenging to broach a family member working on stress recovery toolkits.
The following Table offers suggestions that rather organically allow one to begin to notice one’s internal bodily cues. However, if one has been cut off from his or her bodily cues for long periods of time, this has occurred for a reason. When there is a trauma history of abuse, neglect, or both, getting connected to one’s body can trigger procedural body memories of danger and threat, stimulating an even more activated state. While these exercises may seem innocuous, they are to be done with caution and under supervision of you are unlicensed or not certified in your professional degree. Please read and follow carefully the notes provided for you below this table to use as a guide.
Body Message ActivationHeart Beating - work to have him or her feel his or her resting heart rate. To get the “rhythm” of this, one may try rocking or bobbing.
Next, when ready, one can activate his or her heart rate, by running, jumping, etc.….take time to notice what this feels like when ones heart rate is activated.
Have him/her hold his/her hand over his/her heart to “feel” the heartbeat come back to baseline.
13

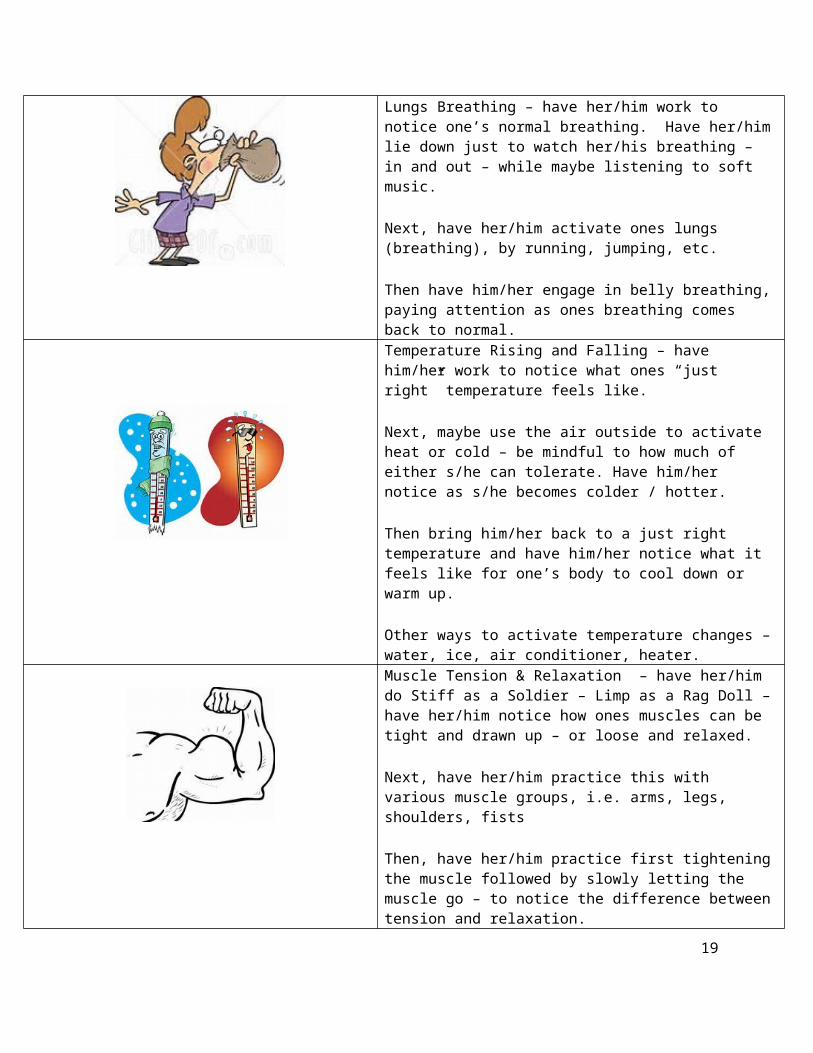
Lungs Breathing – have her/him work to notice one’s normal breathing. Have her/him lie down just to watch her/his breathing – in and out – while maybe listening to soft music.
Next, have her/him activate ones lungs (breathing), by running, jumping, etc.
Then have him/her engage in belly breathing, paying attention as ones breathing comes back to normal.
Temperature Rising and Falling – have him/her work to notice what ones “just right” temperature feels like.
Next, maybe use the air outside to activate heat or cold – be mindful to how much of either s/he can tolerate. Have him/her notice as s/he becomes colder / hotter.
Then bring him/her back to a just right temperature and have him/her notice what it feels like for one’s body to cool down or warm up.
Other ways to activate temperature changes – water, ice, air conditioner, heater.Muscle Tension & Relaxation – have her/him do Stiff as a Soldier – Limp as a Rag Doll – have her/him notice how ones muscles can be tight and drawn up – or loose and relaxed.
Next, have her/him practice this with various muscle groups, i.e. arms, legs, shoulders, fists
Then, have her/him practice first tightening the muscle followed by slowly letting the muscle go – to notice the difference between tension and relaxation.
This table was done with Jennifer Hixson, PsyD, BCBA
Guidelines for connecting to visceral cues: In general, disconnetion from bodily cues links up with long periods of time spent in the deep blue zone of dissociation. With this in mind, our goal is to promote safety and to do no harm. The following points are safety guidelines for working to restore bodily connections that have been ignored or severed.
1. Before starting any of these exercises, grounding techniques are practiced with the person when s/he is in the green zone. The purpose of grounding techiques is to help someone either stay in the present or to “come back” to being in the present, in their body, in the room. There are multiple stratgies for this purpose. The following strategies, as suggestions, have been organized according to bottom-up and top-down strategies. Another use of the term, bottom-up, if you will recall refers to using sensorimotor
14

strategies. These are considered bottom-up because they rely on the use of the senses and doing rather than thinking and talking (top-down).
Bottom-up.
Name 5 things you can see in the room right now Name 4 things you can feel in the room right now (e.g., head against head rest or back of chair;
back against chair; legs against couch; important -pressing his or her feet into the floor) Name 3 things you can hear right now (e.g., if in a very quiet room, may need to add some
sounds like tapping) Name 2 things you can smell or love to smell (having essential oils that are soothing is useful to
have such as lavendar and rose) Name one good thing about yourself
Source: http://www.ibiblio.org/rcip/copingskills.html
As mentioned above, any type of proprioceptive input is good for grounding one’s body into a present state, such as pressing one’s feet against the floor listed above. Here are a few other suggestions.
Claping hands together, slowly squeeze them together, increasing and then decreasing the pressure. Breathe in when clasping hands while increasing the pressure; breathe out when releasing the pressure
Wrap arms around ones shoulders; breathe in, hug, and squeeze; hold tightly, release, and exhale
Taking right index finger, starting at the base of one’s left thumb, follow the outline of one’s open hand, moving up and down, in and out of each finger until one is at the opposite end of one’s palm. Repeat with the opposite hand.
Top-down.
Choose a person you know well, feel safe with, and like/love. o Describe 5 things that characterize his or her physical appearanceo Describe 4 things activities/memories of things you have done togethero Name 3 adjectives that describe this person o Name 2 things this person does that makes you laugho Name 1 thing you like/love about this person
Visualize your favorate place that you have been to that gives you a safe and comforting feeling
o Describe 5 things about this physical locationo Decrbie 4 things you have done in this placeo Name 3 adjectives that describe why this is a safe placeo Name 2 things that are calming features of this locationo Name 1 one thing you love about this location
One could mix and match these up in that the same qustions about what does one see, hear, feel, and smell in the room can be applied to a favorite location or fantasy location one has created
15

2. Before starting any of these exercises, please take the heart rate, breathing rate, and temperature of the person when in the green zone. Knowing resting state numbers allow you to know how much physiological activation you have going on when you exercise as well as helps you know when you’ve returned back to “baseline” health. Incorporating natural rhthyms and patterns into getting to know one’s baseline, resting state is optimally done when there are sensorimotor activities that accompany this learning. Calming, green zone preferences might include coloring, swinging, listening to rhythmic music, playing with Moon Sand. Linking one’s sensory preference/activity with actually listening to one’s heart beat with a stethescope is optimal. Once one has been able to “hear and feel” one’s heart beat, one can take time to represent one’s own rhythm through tapping, rocking, colorng, or drumming to his or her own rhythm.
Dr. Bruce Perry’s six R’s orient us to to the importance of starting off with rhythmic activities that facilitate this discovery.
Relational – done with a safe caregiver Relevant – developmentally matched to the individual Repetitive – sensorimotor activities that are patterened Rewarding – pleaurable to the person Rhythmic – resonant with sequence and pattern Respectful – of the child/families values and culture
http://attachmentdisorderhealing.com/developmental-trauma-3/
http://www.youth4change.org/BrucePerry/NMT_Article_08.pdf
3. Short Duration, low Intensity, and slow Rhythms (DIR).
A safety rule when workiing to connect to bodily signals includes always starting with shorter durations, lower intensity, and slower rhythms. This way, keeping the input short, low, and slow is not likely to effect the nervous system adversly. We are always observing the child/parent’s state of arousal. The response of the state of arousal is what becomes our guide. This becomes tricky because these exercises have a rhthym to them of moving into faster heart rate/breathing rate/hotter temperature/tense body state and then oscillationg to a slower heart rate/breathing rate/cooler temperature/relaxed body state.
Again, using repetitive, patterned, and rhythmic acitivities can be the forum for increaing heart rate/breathing rate/ temperature, etc. Some of these might be playing or bouncing a basketball, playing dodge ball, playing “ga-ga ball”, or dancing together. The natural ebb and flow of shifting to higher and lower physiology, is done in moderation with the titration principle in mind. That might mean that as soon as ones heart rate goes up to 100, we pay attention to it and allow to go back down to a resting state. As soon as ones breathing rate goes up to 20, we pay attention and allow it to be back down, etc. The term “titration” refers to giving the just-right dose of challenge to any one nervous system. This is why gathering physiological data when in the green zone is so important to know, because you can check in, and know how far away you are from those resting state numbers. As one successfully reaches
16

100 heart beats with recovery, one can titrate up to 110 or 120 heart beats with recovery. Finding the right rhythm and increments for each individual allows there to be an expereince of connecting to one’s body with safety, knowing what to expect, and practicing how to recover.
We are carefully watching for anyone getting blue, staying blue, getting activated (combo/red), or staying activated (combo/red). What is the intensity level (also referred to as the Subjective Units of Distress Scale - SUDS levels, http://at-ease.dva.gov.au/professionals/files/2012/12/SUDS.pdf)? The SUDS uses a 0 to 10 scale. Others use a 1 to 5 scale. The importance of either scale is having some subjective measure the person can use to communicate getting into high intensity levels. If emotional distress is showing up with higher intensity levels of a stress zone, we know to shift out of the body exercise to a grounding technique. Each person should know what that switching point is for them. By keenly observing and listening, we find our way, safely. Please note: some practitioners associate DIR with the clinical model of Developmental, Individual, Relationship based treatment. I’m hopeful that if you already have this acronym in mind, that you will be able to easily adapt it to include these dimetional properties of intervention.
4. The rotation of these activities between heart rate, breathing rate, temperature, and muscle tension/relaxation, are likley best titrated to each individual. Some children/youth/adults are very temperature sensitive, and may be averse to even think about getting warm or cold. For those children/youth/adults using guided imagery to imagine a warm beach or the cold snow may be just the place to start - again, low intensity, slow rhytyhm and short duration, before one ever gets close to a heater, blow dryer, or ice cube. Others may be curious about listening to one’s internal rhythm but not want to feel tension in one’s muscles. Usually, whatever activity is going to increase one’s heart rate, is going to increase one’s respiratory rate. So, often, these can be paired together, one time listening or seeing (if you have a heart rate monitor) to one’s heart rate going up and down, the next time noticing one’s breathing rate going up and down.
Eventually, recognizing that one can tolerate one’s body accelertaing and decelerting across different modalities is useful for feeling safe within oneself. With the practitioner representing safety first, then guiding the client through these different types of activation and recovery activities that include rhthmic, repetitive, patterened, sequenced, and pleasurable activities that are predictable, the client can begin to connect in new ways with oneself that “own” one’s body. This furthers ones capacity to trust oneself and to know him or herself under modulated stress activities that represent pairing up conditions of safety with stress in contrast to conditons of danger with stress.
17

Here we see from the Macro point of view, that a medical home, access to fiscal and concrete help in time of need, and respite care are some of the larger items that may need guidance. Food, shelter, and clothing are always items that require being held as a priority. If one is not savvy with community services, now is a time to make a professional acquaintance with a Social Worker who is!
On a Micro level, again, linking up the need/trigger with the specific toolkit is essential. As in my previous example, knowing where the stress accumulates in my body is critical for not only minimizing stress but maximizing sleep. These two are interrelated, as often body stressors are.
18
The Sensory System is one’s “go-to” for arousal regulation to get to sleep, to get to green, to stay green and to recover back to green! We immediately begin to track both sensory triggers and toolkits for the regulating our colors. While there is more to come in the Sensory System, there are many types of devises now that aide in stress recovery which older youth/children can use on their own or parents can guide them in. One of my favorites, that I also use nightly, along with the massager with heat, is the sound of the ocean. One of my all-time sensory preferences is the sound of the ocean, and this lulls me to sleep along with the release of my shoulder/neck tension. This happens to be a free app that has a variety of visual scenes that are accompanied with specific sounds that match the scene. This particular app has a breathing exercise linked to it, along with many different types of guided meditations that can be used during the day or night with varying lengths of time, from 2 to 20 minutes.
19

Now, many young children cannot calm themselves without assistance, and, as we shall see in the Relevance System, the ability to do so comes with maturation. So, body-oriented exercises are often used and here are a few of them.
The Turtle: refers to squeezing one’s body by curling up into a fetal position or moving ones knees up onto a chair and hugging oneself. The hugs can be squeezing one’s arms or wrapping one’s arms around one’s knees and squeezing tightly. This is a way to get “proprioceptive” input into one’s joints and muscles that can be done on one’s own!
The Balloon: refers to breathing in and as one inhales, ones hands move up from resting on top of one’s head to slowly moving above one’s head. As one exhales, ones hands move down towards the top of one’s head. Accompanied by this is the sound of popping during exhaling. The puh-puh-puh-puh sound can be made as one slowly let’s out one’s air, as in letting out the air from a balloon.
The Drain: refers to spreading out one’s arms as if two large faucets. Both fists are clenched. As one exhales, the fists open up to pour out the water and the sound of the exhale now has a steady, shushing sound to it.
The Star: refers to the idea that even if one does not feel like smiling, if one smiles, one actually feels better just by moving one’s smiling muscles. So, this requires one to smile while inhaling, even if it’s a forced smile, and then one holds up a finger and blows out the candle while exhaling.
The Pretzel: refers to one twisting ones legs and one’s arms, then turning one’s hands inside out and pulling them up. One can squeeze one’s whole body while breathing in, and release the body tension while breathing out, also unwinding one’s “pretzel” body in the process.
The Weighted Blanket: refers to making or purchasing a blanket with sand or some type of material sown into it, which adds weight to it. They can be bought on-line with varying sizes and weights to them. This added weight brings on that proprioceptive input that can be comforting.
20

As mentioned during the section on visceral cues, accurately identifying the difference in the meaning of a baby’s cry or an adult’s mood is critical. Whenever possible “reading” one’s own cues and other’s means a lot to the success of working to reduce stress responses.
As these Triggers and Toolkits become more nuanced and understood, the hope is to begin to “catch things at the front end” which can mean circumventing a stress response before it hits or just as it’s on the rise. When one begins to be able to “know” that one’s baby or toddler is hungry and can meet that need quickly and efficiently, there is much less stress response duration and intensity. This begins to give hope to parents who feel like they are always “chasing” the stress responses. The goal is not to eliminate stress responses. The goal is to shift from a toxic pattern to an adaptive one. Thus, these toolkits are also used for stress recovery and we refer to these as “catching the stress response at the back-end”. Whether at the front end or back end, one usually begins to see a difference in the intensity, duration, and frequency of the stress responses. As soon as one of these parameters being to change, hope is on the way.
21

With this amount of information, we are now ready to cycle to the Triggers and Toolkits MENU for any additional Micro level support as to the Individual Differences that are contributing to the toxic stress patterns. For Macro level support we can use the Purple Wheel (simple) and cycle back to the NRF History and Needs Assessment (complex) to look for your community resource partners.
Next, go to the Body Trigger & Toolkit Menu for Child and Parent, Practitioner Version. This menu is also placed on the NRF phone App. [Show picture]
Here, on the left hand column you can see a detailed list of triggers that emanate from the regulation system. On the right hand column you see an almost 1:1 corresponding toolkit suggestion. Notice that this Trigger and Toolkit Menu is for the Practitioner. We offer suggestions as a way to “jumpstart” your clinical thinking and to have things you can suggest to try with the families you work with. Recall that you are forming a collaborative relationship with the parents so that they can engage in the hard work of trial and error with your guidance.
Almost immediately, whatever one has found during the interview process that is a tool, and as one “finds” the right tools that assist the child to get to sleep, to get green, and to stabilize, the following Worksheets are useful.
Go to the Body Trigger & Toolkit Menu for Child and Parent, Family Version.
The real work comes with individualizing the Trigger menu so that the exact triggers are identified for each parent/child and there are specific Toolkits that are entered in when one has enough trial and error experience to know what is working to up-regulate, down-regulate or do both for each individual. That is why the Toolkit side for the family’s menu is blank on your Menu for the parent/child dyad. The NRF
22

Practitioner fills this in over time. The power within the NRF is the individualization and organization the four brain systems give to understanding what helps each nervous system be at his or her best.
Go to the Brain Systems Trigger and Toolkit Worksheet.
As mentioned, as soon as any Triggers and Toolkits are identified, the NRF Practitioner can hand this sheet of paper to the parents, and together, both practitioner and parent(s) begin to fill it out and use it during the collateral and private parent sessions. With older youth, they can have their own sheet they are working on with you.
The goal for each Trigger list is to become individualized and for the Toolkits to be identified and filled in within the first few weeks and months of working together with a NRF therapist. As the NRF protocol for working with cases becomes more solidified, we have a vision for collecting this type of data from our cases across all NRF communities. From previous experience, we suspect that there will be some cases, where the parents’ relevance and executive systems are stronger with less vulnerabilities, then progress will be quickly made. When there are more pervasive vulnerabilities that the parents have, we expect to see slower change, which may have ups and downs. When there are complex cases for both parents and children/youth alike, we expect that much more co-regulation, support, and therapeutic services with the parents will be in order as well, in order for their regulatory capacities to improve.
Notice that this last Trigger and Toolkit Worksheet has two columns under it, one for self-regulation and one for co-regulation. Keeping Vygotsky’s principle in mind, what capacities does this baby/child/youth/parent have to self-regulate and can they make use of scaffolded support with co-regulation? Of course, the co-regulation has to be a match with the other’s needs, yet they still have to be able to accept support, guidance, and help from another.
Challenges with Co-regulation. So, the most challenging cases are when there is a tendency to disconnect when help is present. For example, in working with the NRF court teams, I often say, “yes,
23

our first goal is to support reunification and we offer all the support necessary for this repair to occur; however, the parent still has to take responsibility for what they need to do (e.g., maintain sobriety, find a job) and the parent has to be willing to make use of the support offered (e.g., show up at mutually agreed upon meeting times, participate in the dyadic treatment, etc.).” The “heart” alone is not enough. There have to be boundaries, there are time limits, and there are community structures in place with legal guidelines that have to be followed (the “hand” part of this work). Not everyone is ready to make use of others nor the help that exists in our community settings. Sometimes this is a maturity issue, where the person is not ready, and other times it’s a blend with a mismatch of what the community offers. There can be boundaries that are limiting and oppressive (few resources for undocumented immigrants) or resources can trigger trauma flashbacks. One of our NRF court team cases refused to go into inpatient rehab treatment for her substance use needs. What she could identify at the time, was that she had a trauma trigger about being inpatient; it reminded of her being locked up in Juvenile Hall, where she had experienced trauma. A few years later, when she was sober, she also related to not being “ready” or mature enough to make a good decision at that juncture in her life to approach sobriety as a way of life.
With a designated case that you are following, please take time to fill in the Provider Trigger/Toolkit menu. One can either use a highlight color to mark off triggers and toolkits or one can check the box that matches. Take what you already “know” and begin to fill it in with whichever Worksheet you think will be a good match with this particular family to share with them. This will get richer as we continue to walk through the rest of the brain systems remaining.
For now, to finish up this segment on the Regulation System, one can Go to the Macro level History and Needs Assessment Worksheet. On one hand, this is a very detailed list of risk factors, so one would say this is very micro oriented as we have mentioned! On the other hand, the community resource partners within this and each brain system begin to orient you to the types of community links you may need to have warm handoff relationships with. Often, one does not build those connections until one is in desperate need of them, and so we are then motivated to go searching. Knowing practitioners who are well versed in community links can be invaluable when one’s family goes into crisis. Finding an inpatient substance use rehabilitation center for an undocumented immigrant took time and effort. When our NRF court team case, just referred to, refused the services, we understood her trauma trigger and yet had worked so hard to find a venue that we were doubly disappointed that she was unable to make use of this resource. It had been like the saying, “finding a needle in a haystack.”
A few years later, there was another crisis and we were unprepared. Now, much older, with this same case, she was sober yet living with a boyfriend who had a history of beating her. She had left him many times before, yet this time she followed through with calling the police, filing charges, having him placed in jail, and getting a restraining order. Bottom line, she was now homeless. Would she be willing to go to a shelter? I wondered if this would be another institutional barrier like inpatient rehab had been for her. Would she tolerate being in an institutional setting this time? And a couple additional complications, she was pregnant with a one-year-old baby! Several of the shelters we contacted would not take her because she was pregnant and had a young child to care for as well. How this can happen in
24

our culture, where women with children have trouble accessing shelters is another commentary on our institutional culture and care. The good news is that she had enough maturity to recognize that she would have to put up with things she did not want to, and in her words “suffer” some, in order to stabilize her safety and to reach permanent housing. We scrambled to help her find the right setting, again, not easy with being undocumented, even in a community that’s supposedly rich in resources. We contacted several folks who are community linkage resources for us. One of these folks was my son, the twin with the regulatory disorder as a child, who now works in community development, specializing in working with the homeless, with an eye towards social justice concerns. He reminded me of a home type setting that not only provides a shelter but works to help women find work and attain permanent housing. It’s not a shelter for a few days, it’s a life changer. I had forgotten about this resource. I then realized I actually knew the executive director of this program! We had gone to graduate school together and there had been some collaborative overlap at one point where this director and I had consulted, with her bringing in dyadic coaching to her program where the levels of engagement were used to ensure the birth dyads were starting off with a good connection. When I called this director the next day I was thrilled to find that her program looks for this exact type of referral - a woman who realizes she needs to make serious life changes, is homeless, undocumented, pregnant, and has a child. The director had grown this program so that now there were alumni mothers who volunteered time to support new mothers entering the program. This was another “needle in the haystack” find! This young woman was so grateful that we found a setting for her. And, this being a home setting, rather than an institutional one, she began to thrive. She was “ready” this time. And now, we are “ready” the next time we have a need for an undocumented homeless pregnant woman with a child, fleeing a DV relationship, to find shelter and subsequently, permanent housing.
Nonlinear aspects to 4 brain systems.
Next step: as mentioned, the brain systems both develop in a linear and nonlinear fashion. The linear progression would be to go to Chapter 12 and follow the Sensory System guidelines in that chapter, which focuses on “bottom-up” sensorimotor principles for working with toxic stress patterns. So, why is the next chapter the Relevance System? As already mentioned, the Regulation and Relevance Systems have a lot of overlap to them. They both link up with the Internal Milieu, directly connecting with our bodies, and communicating directly with our brainstem (regulation-survival) and limbic areas (relevance-emotional centers). You’ve seen this picture a few times, so this may be a refresh for you on this point.
25

The functional capacities in the Relevance System have a lot of overlap with our Regulation System’s capacities. In this way, it makes sense to link these two up so that you can hold the integration of the Regulation and Relevance system’s properties tightly. Then, we will cycle back to the Sensory System, with an emphasis on looking at the bottom-up aspects of how to work with both the Regulation and Relevance System’s needs. Lastly, then, we will go to the Executive System, with an emphasis on top-down aspects of intervention.
Distributed nature of bottom-up and top-down aspects of brain networks.
Last but not least, let’s go one step deeper into our understanding of bottom-up and top-down processes. The general gist of bottom-up means that a process is occurring automatically without conscious awareness and most often involves non-verbal communication. The general gist of top-down means that a process is occurring with conscious intent and most often involves the use of language - verbal communication. We’ve focused upon regulation (arousal) and sensory (sensations) as our two primary bottom-up systems. They are. LeDoux and Porges’ work focus on how sensations are automatically “read” at all times, determining whether there is safety or threat. I add to that to this binary organization, the dimension of “challenge”. This allows there to be more of a continuum to danger, with a range that exists with degrees of challenge to threat. LeDoux refers to this automatic system as the “low road” of sensory processing (xxx) and the conscious capacity to process safety and threat as the “high road”. These are akin to the use of the NRF’s terms of bottom-up to refer to automatic habit and top-down as conscious awareness or control.
26

Porges refers to this automatic system as “neuroception” (2004). Porges’ life’s work has focused upon the 10th cranial nerve that is the vagus nerve. This very expansive vagal nerve is the parasympathetic side of our ANS. When we are born with good “vagal tone” we have a good vagal brake that helps us get into and maintain the green zone. This vagal system is actually the ANS’s contribution to our ability to stay modulated within the green zone. If one has a poor vagal brake, often linked with the prematurity and state of arousal dysregulation that runs across many diagnostic categories (Autism, Mood Disorders, Reactive Attachment Disorder, Schizophrenia, PTSD, and more - 2004), the challenge of inhibiting may have definite contributions coming from this arena.
From Porges and Greenspan’s work, the NRF really expands upon is that this continuum of safety, challenge, and threat occur on a sensory level that is at a relational level as well. All of the non-verbal cues that make up our states of arousal are sensory cues to the other that organize our experiences and perceptions of safety, challenge, and threat.
However, an advanced concept is that all of our brain networks have both bottom-up and top-down aspects to them. Even more recently, it is known that this dual tiered process is very integrated and much more intertwined than the way this slide is organized, which can look rather linear. Once one has more capacity to inhibit, with maturity of all of the brain networks including our executive system, one can use conscious control to inhibit our arousal states. This is why when we are in public, we can stop ourselves from using a curse word or from yelling out when something offensive happens or we get physically hurt, whereas at home, we might let it rip. We are consciously putting the brakes on and
27

putting a lid on our red zone behavior. As we go through the rest of the brain systems, the top-down and bottom-up aspects within each network will be pointed out.
The linear order of the four brain systems progresses from regulation into the sensory system, then the relevance and executive systems. Most often, when we have a toxic stress pattern at play, we indeed go to the sensory system to look for “bottom-up” sensory-motor ideas to reduce the toxic stress pattern. At the same time, there is a lot of overlap between the regulation system’s energy flow and the emotional valences of the relevance system. The functional capacities of the relevance system really evolve nicely from the regulation system. So if you learn better through complementary ideas, you can read the relevance system next, Chapter 11. If you are desperate for bottom-up sensory principles, then move into Chapter 12 to read about the sensory system.
At this juncture, you can proceed in a linear order of the brain systems by going to Chapter 12 to follow the Sensory System or you can proceed in a linear order of the Chapters by going to Chapter 11.
28





























