Embed Size (px)
Citation preview

INTRODUCTION
Fixed orthodontic appliances tend to accumulate dental plaque biofilms adjacent to brackets and tubes, which complicates the patients’ oral hygiene processes1-3). Greater accumulation of biofilms could increase the Streptococcus mutans (S. mutans) and Lactobacillus casei (L. casei), which are the two primary cariogenic pathogens related to decalcification and caries4,5). S. mutans is cariogenic because it produces lactic acid and leads to local acidic pH2). Enamel surfaces around brackets and tubes can be dissolved by lactic acid, which leads to the development of white spot leisions6-9). Furthermore, it could take only four weeks for white spot lesions to deteriorate into cavitated caries lesions10). Orthodontic patients usually spend 2.5 years wearing brackets, which is long enough to cause serious lesions. As a result, patients with fixed orthodontic appliances are vulnerable to white spot lesions and caries, especially those with poor oral hygiene6). Recent studies showed that 50–70% of patients had white spot lesions after fixed orthodontic treatment11-13). White spot lesions were considered as the main undesired adverse effect of fixed orthodontic treatment6,8,11,13,14).
For orthodontists seeking effective preventive approaches, it is essential to be able to streamline the
methods. Generally, it involves three aspects to prevent white spot lesions for patients with fixed orthodontic appliances: proper oral hygiene, dietary control, and fluoride therapy6,8,15). However, these approaches are unreliable because they rely on patient compliance11,13). Therefore, other promising strategies, such as novel antibacterial orthodontic cements, need to be developed to prevent white spot lesions and caries.
Orthodontic cement plays an important role because it is in direct contact with both enamel surface and dental plaque biofilms. However, most currently available orthodontic cements lack antibacterial capability. To inhibit caries and obtain clinical benefits, several studies incorporated various antibacterial agents into dental resins, including chlorhexidine16), nanosilver17), 12- methacryloyloxydodecylpyridinium bromide (MDPB)18,19), methacryloxylethyl cetyl dimethyl ammonium chloride (DMAE-CB)20), dimethylaminododecyl methacrylate (DMADDM)10) and other antibacterial agents21-23).
Quaternary ammonium monomers (QAMs) can cause bacteria lysis by disrupting the bacterial membranes and therefore effectively inhibit biofilm growth24). The methacrylate radical of QAMs can be immobilized in the resin matrix by copolymerizing with other dental monomers to endow a durable antibacterial property to dental adhesives and composites23,25). Long-chained QAMs possess double-killing effects including positive charges and physical insertion into the bacterial membrane26,27).
Novel orthodontic cement containing dimethylaminohexadecyl methacrylate with strong antibacterial capabilityXiaodong FENG1,2, Ning ZHANG2, Hockin H. K. XU3,4,5, Michael D. WEIR3, Mary Anne S. MELO3, Yuxing BAI2 and Ke ZHANG2
1 Division of Dentistry, Beijing Tongren Hospital, Capital Medical University, Beijing, China2 Department of Orthodontics, School of Stomatology, Capital Medical University, Beijing, China3 Biomaterials & Tissue Engineering Division, Department of Endodontics, Periodontics and Prosthodontics, University of Maryland School of
Dentistry, Baltimore, MD 21201, USA4 Center for Stem Cell Biology & Regenerative Medicine, University of Maryland School of Medicine, Baltimore, MD 21201, USA5 Department of Mechanical Engineering, University of Maryland, Baltimore County, MD 21250, USACorresponding authors, Yuxing BAI; E-mail: [email protected], Ke ZHANG; E-mail: [email protected]
Orthodontic treatments increase the incidence of white spot lesions. The objectives of this study were to develop an antibacterial orthodontic cement to inhibit demineralization, and to evaluate its enamel shear bond strength and anti-biofilm properties. Novel antibacterial monomer dimethylaminohexadecyl methacrylate (DMAHDM) was synthesized and incorporated into Transbond XT at 0, 1.5 and 3% by mass. Anti-biofilm activity was assessed using a human dental plaque microcosm biofilm model. Shear bond strength and adhesive remnant index were also tested. Biofilm activity precipitously dropped when contacting orthodontic cement with DMAHDM. Orthodontic cement containing 3% DMAHDM significantly reduced biofilm metabolic activity and lactic acid production (p<0.05), and decreased biofilm colony-forming unit (CFU) by two log. Water-aging for 90 days had no adverse influence on enamel shear bond strength (p>0.1). By incorporating DMAHDM into Transbond XT for the first time, the modified orthodontic cement obtained a strong antibacterial capability without compromising the enamel bond strength.
Keywords: Orthodontic cement, Oral biofilm, White spot lesions
Color figures can be viewed in the online issue, which is avail-able at J-STAGE.Received Nov 15, 2016: Accepted Jan 19, 2017doi:10.4012/dmj.2016-370 JOI JST.JSTAGE/dmj/2016-370
Dental Materials Journal 2017; 36(5): 669–676

Dimethylaminohexadecyl methacrylate (DMAHDM), with alkyl chain length (CL) of 16, was recently synthesized and showed the strongest antibacterial activity among a series of QAMs27). However, to date, no study has been reported with DMAHDM as the antibacterial agent in orthodontic adhesive systems.
The aims of this study were to develop a novel antibacterial orthodontic cement and to investigate the influence of adding DMAHDM on enamel bond strength and dental plaque microcosm biofilm properties for the first time. Two hypotheses were tested: (1) Strongly antibacterial orthodontic cement with DMAHDM could be developed without sacrificing the enamel bond strength; (2) DMAHDM-containing orthodontic adhesive would substantially reduce dental plaque microcosm biofilm growth, metabolic activity, and lactic acid production, compared to the commercial control orthodontic cement.
MATERIALS AND METHODS
Synthesis of DMAHDMDMAHDM was synthesized using a modified Menschutkin reaction method in which a tertiary amine was reacted with an organo-halide23,28,29). The advantage of this method is that the reaction products are generated at virtually quantitative amounts and require no further purification23). To form DMAHDM, 10 mmol of 2-(dimethylamino) ethyl methacrylate (DMAEMA), 10 mmol of 1-bromohexadecane (BHD) (TCI America, Portland, OR, USA), and 3 g of ethanol were added and reacted in a 20 mL scintillation vial. DMAEMA provided the tertiary amine and ethanol was the solvent. The vial was capped and stirred at 70°C for 24 h for the reaction to complete27). After the ethanol was evaporated completely, DMAHDM was obtained as a viscous liquid. The reaction and products were verified via Fourier transform infrared spectroscopy in previous studies28,29).
Fabrication of antibacterial orthodontic cementTransbond XT (3M Unitek, Monrovia, CA, USA) was used as the parent system to develop a DMAHDM-containing orthodontic cement with anti-biofilm properties. According to the manufacturer, Transbond XT consisted of silane-treated quartz (70–80% by weight), bisphenol-A-diglycidyl ether dimethacrylate (10–20%), bisphenol-A-bis (2-hydroxyethyl) dimethacrylate (5–10%), silane-treated silica (<2%) and diphenyliodonium hexafluorophosphate (<0.2%). DMAHDM was mixed with Transbond XT at DMAHDM/(DMAHDM+Transbond) mass fractions of 0, 1.5, and 3%. These mass fractions were selected on the basis of a previous study10). DMAHDM mass fractions>3% were not tested because of a decreased enamel bond strength10).
For bacterial tests, disk specimens were fabricated using polyethylene molds (inner diameter=9 mm, thickness=2 mm). The orthodontic cement disks were photo-polymerized (Triad 2000, Dentsply, York, PA, USA) for 1 min on each open side, following a previous
study30). The cured disks were immersed and agitated in sterile water for 1 h to remove any uncured monomers, then submitted to ethylene oxide sterilization (Anprolene AN 74i, Andersen, Haw River, NC, USA)30). Three groups were tested for enamel shear bond strength and anti-biofilm properties:
1. Transbond XT control with 0% DMAHDM (termed “TB control”).
2. Transbond XT+1.5% DMAHDM (termed “TB+1.5DMAHDM”).
3. Transbond XT+3% DMAHDM (termed “TB+3DMAHDM”).
Enamel shear bond test and adhesive remnant index (ARI)Ninety human maxillary first premolars without any caries or crackers were extracted and randomly allocated into three groups, with 30 teeth in each group. Each tooth was embedded vertically in a self-curing acrylic resin (Lang Dental, Wheeling, IL, USA), and their labial surface were paralleled with the force direction during shear bond testing. Enamel was etched for 20 s (typically between 15–30 s according to the manufacturer’s recommendation) with 37% phosphoric acid (Scotchbond, 3M ESPE, St. Paul, MN, USA) and then rinsed thoroughly with water for 10 s. The tooth was dried with a stream of oil-free compressed air. Transbond XT Primer was applied to the bonding surface and adhesive was placed to cover the bracket pad with a thin coat. Premolar metal orthodontic brackets (Ormco Series 2000, Sybron Dental, Orange, CA, USA) with a mean base surface area of 9.63 mm2 were bonded to the teeth using each orthodontic adhesive group31). Flash was removed from all sides of the bracket with a micro brush. The adhesive was cured from mesial and distal sides for 10 s each, using a light-curing unit (Optilux VCL 401, Demetron Kerr, Danbury, CT, USA)10). The 30 bonded specimens of each group were divided into three subgroups of 10 specimens each, and were stored in distilled water at 37 °C for 15 min, 24 h, and 90 days, respectively, before the shear bond testing.
Shear bond strength was tested with a computer-controlled universal testing machine (MTS, Eden Prairie, MN, USA) using a chisel at a crosshead speed of 0.5 mm per min. The applied load was recorded until the bond failed. To prevent deformation of the bracket, a stainless steel wire (with cross-section of 0.019×0.025 inch) was ligated into each bracket slot during testing. The shear bond strength was calculated as the debonding force divided by the bracket surface area.
The residual adhesive on the tooth surface was examined and scored with a stereoscopic microscope (Leica Zoom 2000, Leica Microsystems, Wetzlar, Germany) using the ARI3,32). The following scores were used: 0=no cement remaining on enamel; 1=less than half of the cement remaining on enamel; 2=more than half of cement remaining on enamel; 3=all the cement remaining on enamel, with a distinct impression of the bracket base.
670 Dent Mater J 2017; 36(5): 669–676

Dental plaque microcosm biofilm modelWhole human saliva was used as an inoculum, in order to provide multi-species biofilms consisting of organisms found in the oral cavity. To maintain the diversity of bacterial populations, mixed saliva was collected from 10 healthy donors, who had natural dentitions without active caries or periodontitis, and did not take antibiotics within the last 3 months33,34). The donor did not brush teeth for 24 h and abstained from food/drink intake for at least 2 h before donating saliva28). An equal volume from each of the subjects was pooled and mixed with sterile glycerol to a final 70% saliva concentration, and then stored at −80ºC for subsequent use33,34). The use of human saliva microcosm model in this study was approved by Capital Medical University.
Live/dead biofilm stainingThe saliva-glycerol stock was added, with 1:50 final dilution, to a growth medium as inoculum. The growth medium contained mucin (type II, porcine, gastric) at a concentration of 2.5 g/L; bacteriological peptone, 2.0 g/L; tryptone, 2.0 g/L; yeast extract, 1.0 g/L; NaCl, 0.35 g/L, KCl, 0.2 g/L; CaCl2, 0.2 g/L; cysteine hydrochloride, 0.1 g/L; haemin, 0.001 g/L; vitamin K1, 0.0002 g/L, at pH 735). Every disc sample was placed into a 24-well plate with 1.5 mL medium and incubated in 5% CO2 at 37ºC for 8 h. Each sample was transferred into a new 24-well plate with 1.5 mL fresh medium and then incubated for 16 h. Then, transfer each sample into a new 24-well plate with 1.5 mL fresh medium, and incubated for 24 h36).
The 2-day biofilms on samples were gently rinsed with phosphate-buffered saline (PBS), live/dead stained with a bacterial viability kit (Molecular Probes, Eugene, OR, USA) and then examined with an epifluorescence microscope (TE2000-S, Nikon, Melville, NY, USA). Live bacteria were stained with Syto 9 to show a green fluorescence, and bacteria with damaged membranes were stained with propidium iodide to show a red fluorescence. Four representative images were taken for each sample, with three specimens yielding 12 images for each group10).
MTT assay of metabolic activity and lactic acid productionSix separate cement disks were used for the MT assay for each group. Cement disks with 2-day biofilms were transferred to a new 24-well plate for the MTT (3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide) assay. The MTT is a colorimetric assay that measures the enzymatic reduction of MTT, a yellow tetrazole, into purple formazan23,37). One milliliter of MTT dye (0.5 mg/mL MTT in PBS) was added to each well and incubated at 37°C in 5% CO2 in the dark for 1 h. During this process, specific bacteria metabolized the yellow MTT and reduced it to purple formazan inside the living cells. After 1 h, the samples were transferred to a new 24-well plate, 1 mL of dimethyl sulfoxide (DMSO) was added to solubilize the formazan crystals, and the plate was incubated for 20 min with
gentle mixing at room temperature in the dark28). After brief mixing via pipetting, 200 μL of the DMSO solution from each well was transferred to a 96-well plate, and the absorbance at 540 nm (OD540) was measured via the microplate reader (SpectraMax M5, Molecular Devices, Sunnyvale, CA, USA). A higher absorbance reflects a higher formazan concentration, which in turn reflects more metabolic activity in the biofilm on the surface of orthodontic cement10).
Six separate cement disks were used for lactic acid production for each group. Cement disks inoculated and cultured for 2 days were rinsed with cysteine peptone water (CPW) to remove loosely-attached bacteria, and then transferred to 24-well plates containing 1.5 mL of buffered-peptone water (BPW) plus 0.2% sucrose. The samples were incubated for 3 h to allow the biofilms to produce acid. BPW solutions were stored and lactate concentrations were measured using an enzymatic method36). The 340 nm absorbance (OD340) of BPW was determined with a microplate reader (SpectraMax, Molecular Devices). Standard curves were prepared using a standard lactic acid (Supelco Analytical, Bellefonte, PA, USA).
Biofilm colony-forming unit (CFU) countsDisks inoculated and cultured for 2 days were transferred into tubes with 2 mL CPW. Biofilm on each disk was harvested by sonication/vortexing (Fisher, Pittsburgh, PA, USA), according to a previous study24). Three types of agar plates were used to evaluate the microorganism viability after serially dilution in CPW. Tryptic soy agar (TSA) with sheep blood plates were aimed at determing total microorganisms24,28). Mitis salivarius agar (MSA) culture plates containing 15% sucrose were used to determine total streptococci, since MSA inhibited many species of bacteria but streptococci24,28). MSA agar plates with 0.2 units of bacitracin per mL were for determining the mutans streptococci, because bacitracin is a selective antibiotic which has no influence on cariogenic mutans streptococci24,28).
Statistical analysisOne-way and two-way analyses-of-variance (ANOVA) were performed to detect the significant effects of the variables. Tukey’s multiple comparison test was used to compare the data at p=0.05.
RESULTS
The enamel shear bond strengths of the orthodontic cements are plotted in Fig. 1 (mean±SD; n=10). Control group at 15 min had the lowest shear bond strength, while the strengths of the other groups were not significantly different from each other (p>0.1). Therefore, incorporating DMAHDM up to 3% into orthodontic cement did not significantly decrease the bracket-enamel bond strength. In addition, there was no significant strength loss for all groups in water-aging from 1 day to 90 days (p>0.1).
671Dent Mater J 2017; 36(5): 669–676
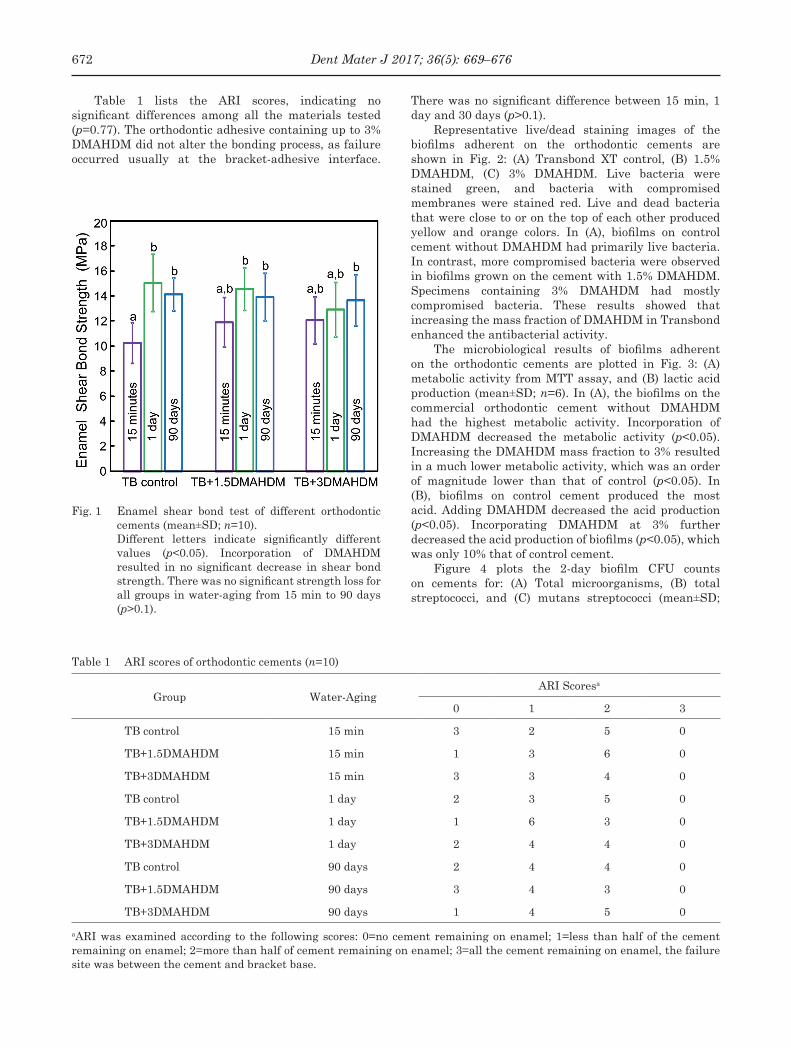
Fig. 1 Enamel shear bond test of different orthodontic cements (mean±SD; n=10).
Different letters indicate significantly different values (p<0.05). Incorporation of DMAHDM resulted in no significant decrease in shear bond strength. There was no significant strength loss for all groups in water-aging from 15 min to 90 days (p>0.1).
Table 1 ARI scores of orthodontic cements (n=10)
Group Water-AgingARI Scoresa
0 1 2 3
TB control 15 min 3 2 5 0
TB+1.5DMAHDM 15 min 1 3 6 0
TB+3DMAHDM 15 min 3 3 4 0
TB control 1 day 2 3 5 0
TB+1.5DMAHDM 1 day 1 6 3 0
TB+3DMAHDM 1 day 2 4 4 0
TB control 90 days 2 4 4 0
TB+1.5DMAHDM 90 days 3 4 3 0
TB+3DMAHDM 90 days 1 4 5 0
aARI was examined according to the following scores: 0=no cement remaining on enamel; 1=less than half of the cement remaining on enamel; 2=more than half of cement remaining on enamel; 3=all the cement remaining on enamel, the failure site was between the cement and bracket base.
Table 1 lists the ARI scores, indicating no significant differences among all the materials tested (p=0.77). The orthodontic adhesive containing up to 3% DMAHDM did not alter the bonding process, as failure occurred usually at the bracket-adhesive interface.
There was no significant difference between 15 min, 1 day and 30 days (p>0.1).
Representative live/dead staining images of the biofilms adherent on the orthodontic cements are shown in Fig. 2: (A) Transbond XT control, (B) 1.5% DMAHDM, (C) 3% DMAHDM. Live bacteria were stained green, and bacteria with compromised membranes were stained red. Live and dead bacteria that were close to or on the top of each other produced yellow and orange colors. In (A), biofilms on control cement without DMAHDM had primarily live bacteria. In contrast, more compromised bacteria were observed in biofilms grown on the cement with 1.5% DMAHDM. Specimens containing 3% DMAHDM had mostly compromised bacteria. These results showed that increasing the mass fraction of DMAHDM in Transbond enhanced the antibacterial activity.
The microbiological results of biofilms adherent on the orthodontic cements are plotted in Fig. 3: (A) metabolic activity from MTT assay, and (B) lactic acid production (mean±SD; n=6). In (A), the biofilms on the commercial orthodontic cement without DMAHDM had the highest metabolic activity. Incorporation of DMAHDM decreased the metabolic activity (p<0.05). Increasing the DMAHDM mass fraction to 3% resulted in a much lower metabolic activity, which was an order of magnitude lower than that of control (p<0.05). In (B), biofilms on control cement produced the most acid. Adding DMAHDM decreased the acid production (p<0.05). Incorporating DMAHDM at 3% further decreased the acid production of biofilms (p<0.05), which was only 10% that of control cement.
Figure 4 plots the 2-day biofilm CFU counts on cements for: (A) Total microorganisms, (B) total streptococci, and (C) mutans streptococci (mean±SD;
672 Dent Mater J 2017; 36(5): 669–676
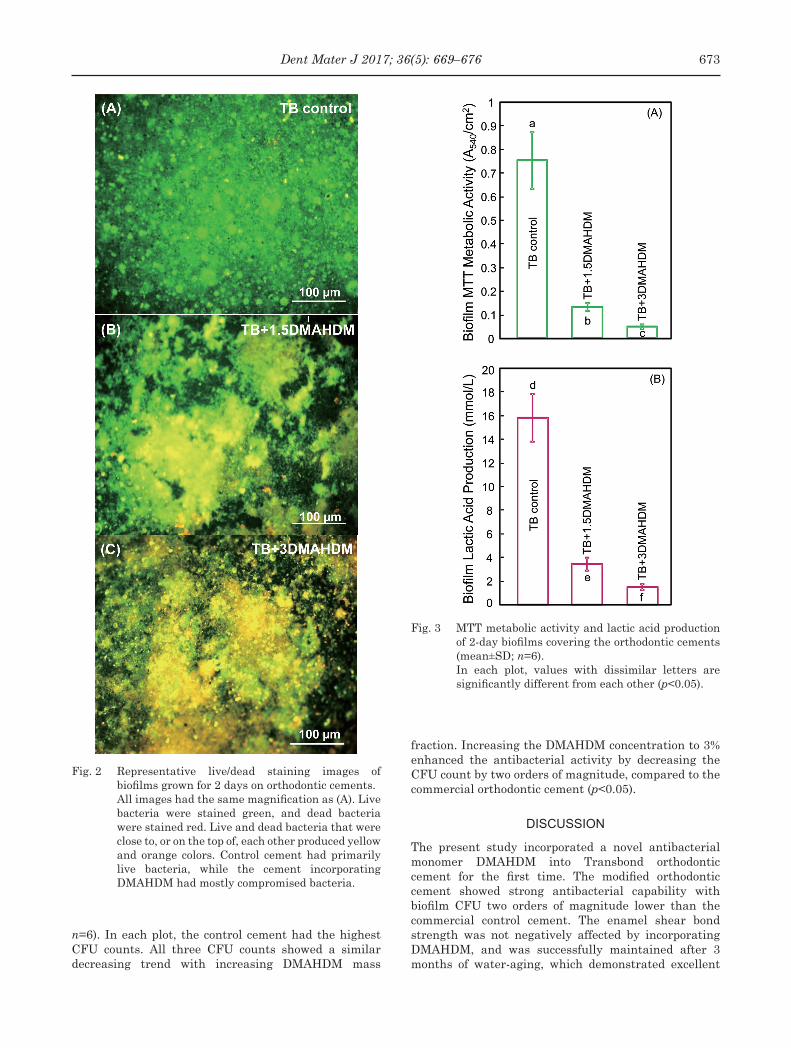
Fig. 2 Representative live/dead staining images of biofilms grown for 2 days on orthodontic cements.
All images had the same magnification as (A). Live bacteria were stained green, and dead bacteria were stained red. Live and dead bacteria that were close to, or on the top of, each other produced yellow and orange colors. Control cement had primarily live bacteria, while the cement incorporating DMAHDM had mostly compromised bacteria.
Fig. 3 MTT metabolic activity and lactic acid production of 2-day biofilms covering the orthodontic cements (mean±SD; n=6).
In each plot, values with dissimilar letters are significantly different from each other (p<0.05).
n=6). In each plot, the control cement had the highest CFU counts. All three CFU counts showed a similar decreasing trend with increasing DMAHDM mass
fraction. Increasing the DMAHDM concentration to 3% enhanced the antibacterial activity by decreasing the CFU count by two orders of magnitude, compared to the commercial orthodontic cement (p<0.05).
DISCUSSION
The present study incorporated a novel antibacterial monomer DMAHDM into Transbond orthodontic cement for the first time. The modified orthodontic cement showed strong antibacterial capability with biofilm CFU two orders of magnitude lower than the commercial control cement. The enamel shear bond strength was not negatively affected by incorporating DMAHDM, and was successfully maintained after 3 months of water-aging, which demonstrated excellent
673Dent Mater J 2017; 36(5): 669–676
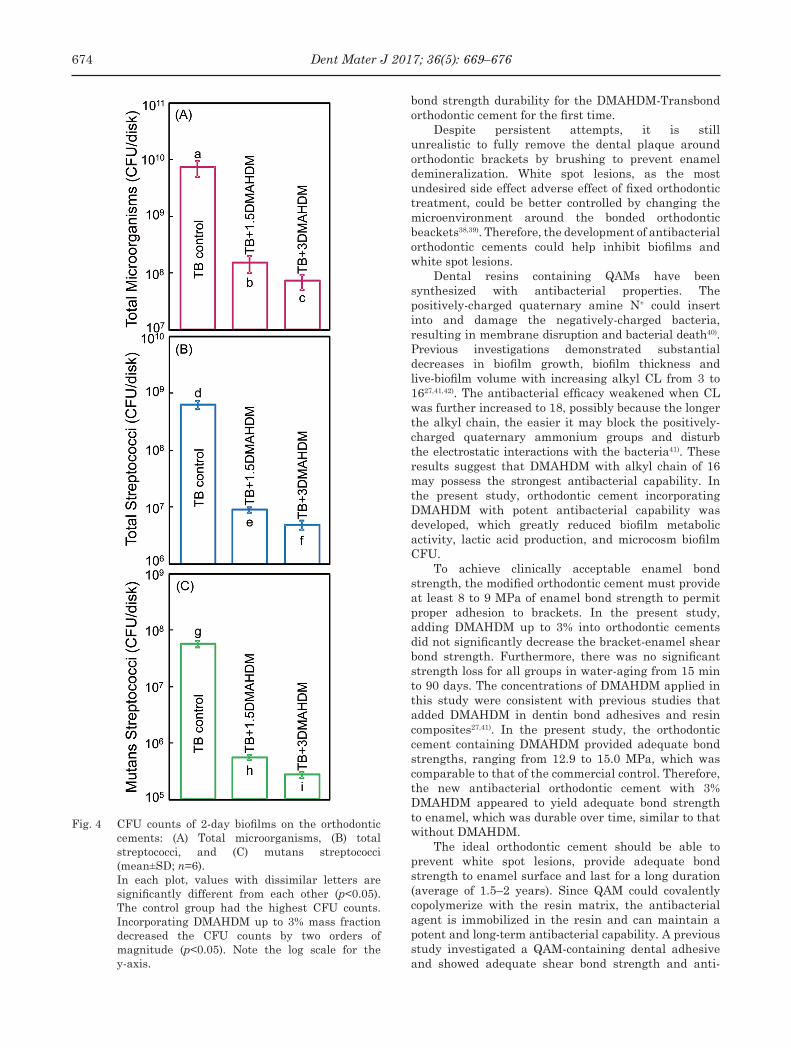
Fig. 4 CFU counts of 2-day biofilms on the orthodontic cements: (A) Total microorganisms, (B) total streptococci, and (C) mutans streptococci (mean±SD; n=6).
In each plot, values with dissimilar letters are significantly different from each other (p<0.05). The control group had the highest CFU counts. Incorporating DMAHDM up to 3% mass fraction decreased the CFU counts by two orders of magnitude (p<0.05). Note the log scale for the y-axis.
bond strength durability for the DMAHDM-Transbond orthodontic cement for the first time.
Despite persistent attempts, it is still unrealistic to fully remove the dental plaque around orthodontic brackets by brushing to prevent enamel demineralization. White spot lesions, as the most undesired side effect adverse effect of fixed orthodontic treatment, could be better controlled by changing the microenvironment around the bonded orthodontic beackets38,39). Therefore, the development of antibacterial orthodontic cements could help inhibit biofilms and white spot lesions.
Dental resins containing QAMs have been synthesized with antibacterial properties. The positively-charged quaternary amine N+ could insert into and damage the negatively-charged bacteria, resulting in membrane disruption and bacterial death40). Previous investigations demonstrated substantial decreases in biofilm growth, biofilm thickness and live-biofilm volume with increasing alkyl CL from 3 to 1627,41,42). The antibacterial efficacy weakened when CL was further increased to 18, possibly because the longer the alkyl chain, the easier it may block the positively-charged quaternary ammonium groups and disturb the electrostatic interactions with the bacteria41). These results suggest that DMAHDM with alkyl chain of 16 may possess the strongest antibacterial capability. In the present study, orthodontic cement incorporating DMAHDM with potent antibacterial capability was developed, which greatly reduced biofilm metabolic activity, lactic acid production, and microcosm biofilm CFU.
To achieve clinically acceptable enamel bond strength, the modified orthodontic cement must provide at least 8 to 9 MPa of enamel bond strength to permit proper adhesion to brackets. In the present study, adding DMAHDM up to 3% into orthodontic cements did not significantly decrease the bracket-enamel shear bond strength. Furthermore, there was no significant strength loss for all groups in water-aging from 15 min to 90 days. The concentrations of DMAHDM applied in this study were consistent with previous studies that added DMAHDM in dentin bond adhesives and resin composites27,41). In the present study, the orthodontic cement containing DMAHDM provided adequate bond strengths, ranging from 12.9 to 15.0 MPa, which was comparable to that of the commercial control. Therefore, the new antibacterial orthodontic cement with 3% DMAHDM appeared to yield adequate bond strength to enamel, which was durable over time, similar to that without DMAHDM.
The ideal orthodontic cement should be able to prevent white spot lesions, provide adequate bond strength to enamel surface and last for a long duration (average of 1.5–2 years). Since QAM could covalently copolymerize with the resin matrix, the antibacterial agent is immobilized in the resin and can maintain a potent and long-term antibacterial capability. A previous study investigated a QAM-containing dental adhesive and showed adequate shear bond strength and anti-
674 Dent Mater J 2017; 36(5): 669–676

biofilm capability that did not decrease after 6 months of water-ageing, compared to that at 1 day30). The present study showed for the first time that the shear bond strength of DMAHDM-Transbond lasted over 90 days of water-aging. However, enamel bond strength under in-vitro conditions cannot completely predict clinical efficiency, and further study is needed to evaluate the long-term mechanical strength of the orthodontic cement containing DMAHDM during immersion in saliva intraorally. Further study is also needed to investigate the effects of DMAHDM incorporation into Transbond on enamel white spot lesion reduction in vivo in a clinically relevant manner.
Further study is also needed to investigate any side-effects in applying QAMs to orthodontic cement. One issue is that QAMs are not tasteless, and tooth paste containing QAMs showed bitter and unpleasant taste in some family of QAMs. This issue may be minimized because the orthodontic cement is cured and the QAM is polymerized and immobilized in the resin. Another issue is potential irritation of QAMs to mucosal tissues. A recent study on in vitro cytotoxicity against fibroblasts and odontoblastic cells showed that the new antibacterial monomers had cytotoxicity matching HEMA and TEGDMA, with less cytotoxicity than Bis-GMA27). Further in vivo studies using animal models are needed to investigate the biocompatibility of orthodontic cement containing QAMs.
CONCLUSION
White spot lesions due to enamel demineralization are the most undesired adverse effect of fixed orthodontic treatments. In this study, a novel antibacterial monomer DMAHDM was incorporated into Transbond orthodontic cement for the first time. The orthodontic bracket cement incorporating 3% of DMAHDM possessed strong antibacterial effects, greatly reducing the biofilm metabolic activity and lactic acid production, and decreasing the biofilm CFU by two orders of magnitude, compared to commercial control. The modified orthodontic cement caused no loss in enamel shear bond strength, even after 90 days of water-aging. Hence, the DMAHDM-Transbond orthodontic cement is highly promising for durable enamel bonding to inhibit or eliminate white spot lesions for orthodontic patients.
ACKNOWLEDGMENTS
This work was supported by National Natural Science Foundation of China [81400540 to KZ]; Beijing Municipal Administration of Hospitals’ Youth Program [QML20151401 to KZ]; Capital Medical University Basic-Clinical Research Cooperation Fund [14JL78 to KZ]; Beijing Municipal Administration of Hospitals’ Ascent Plan [DFL20151401 to YB]; National Institutes of Health [R01 DE17974 to HX], and a Seed Grant (HX) from the University of Maryland School of Dentistry.
REFERENCES
1) Ahn SJ, Lim BS, Lee SJ. Surface characteristics of orthodontic adhesives and effects on streptococcal adhesion. Am J Orthod Dentofacial Orthop 2010; 137: 489-495.
2) Santamaria M Jr, Petermann KD, Vedovello SA, Degan V, Lucato A, Franzini CM. Antimicrobial effect of Melaleuca alternifolia dental gel in orthodontic patients. Am J Orthod Dentofacial Orthop 2014; 145: 198-202.
3) Uysal T, Amasyali M, Ozcan S, Koyuturk AE, Sagdic D. Effect of antibacterial monomer-containing adhesive on enamel demineralization around orthodontic brackets: an in-vivo study. Am J Orthod Dentofacial Orthop 2011; 139: 650-656.
4) Lim BS, Lee SJ, Lee JW, Ahn SJ. Quantitative analysis of adhesion of cariogenic streptococci to orthodontic raw materials. Am J Orthod Dentofacial Orthop 2008; 133: 882-888.
5) Papaioannou W, Gizani S, Nassika M, Kontou E, Nakou M. Adhesion of Streptococcus mutans to different types of brackets. Angle Orthod 2007; 77: 1090-1095.
6) Enaia M, Bock N, Ruf S. White-spot lesions during multibracket appliance treatment: A challenge for clinical excellence. Am J Orthod Dentofacial Orthop 2011; 140: e17-24.
7) Kronenberg O, Lussi A, Ruf S. Preventive effect of ozone on the development of white spot lesions during multibracket appliance therapy. Angle Orthod 2009; 79: 64-69.
8) Guzman-Armstrong S, Chalmers J, Warren JJ. Ask us. White spot lesions: prevention and treatment. Am J Orthod Dentofacial Orthop 2010; 138: 690-696.
9) Millett DT, Nunn JH, Welbury RR, Gordon PH. Decalcification in relation to brackets bonded with glass ionomer cement or a resin adhesive. Angle Orthod 1999; 69: 65-70.
10) Melo MA, Wu J, Weir MD, Xu HH. Novel antibacterial orthodontic cement containing quaternary ammonium monomer dimethylaminododecyl methacrylate. J Dent 2014; 42: 1193-1201.
11) Chapman JA, Roberts WE, Eckert GJ, Kula KS, Gonzalez-Cabezas C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 2010; 138: 188-194.
12) Lucchese A, Gherlone E. Prevalence of white-spot lesions before and during orthodontic treatment with fixed appliances. Eur J Orthod 2013; 35: 664-668.
13) Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod 2011; 81: 206-210.
14) Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013; 83: 641-647.
15) Derks A, Kuijpers-Jagtman AM, Frencken JE, Van’t Hof MA, Katsaros C. Caries preventive measures used in orthodontic practices: an evidence-based decision? Am J Orthod Dentofacial Orthop 2007; 132: 165-170.
16) Singh C, Dua V, Vyas M, Verma S. Evaluation of the antimicrobial and physical properties of an orthodontic photo-activated adhesive modified with an antiplaque agent: an in vitro study. Indian J Dent Res 2013; 24: 694-700.
17) Ahn SJ, Lee SJ, Kook JK, Lim BS. Experimental antimicrobial orthodontic adhesives using nanofillers and silver nanoparticles. Dent Mater 2009; 25: 206-213.
18) Imazato S, Kinomoto Y, Tarumi H, Ebisu S, Tay FR. Antibacterial activity and bonding characteristics of an adhesive resin containing antibacterial monomer MDPB. Dent Mater 2003; 19: 313-319.
19) Zhang K, Cheng L, Imazato S, Antonucci JM, Lin NJ, Lin-Gibson S, Bai Y, Xu HH. Effects of dual antibacterial agents MDPB and nano-silver in primer on microcosm biofilm, cytotoxicity and dentine bond properties. J Dent 2013; 41:
675Dent Mater J 2017; 36(5): 669–676
464-474.20) Li F, Chai ZG, Sun MN, Wang F, Ma S, Zhang L, Fang M,
Chen JH. Anti-biofilm effect of dental adhesive with cationic monomer. J Dent Res 2009; 88: 372-376.
21) Poosti M, Ramazanzadeh B, Zebarjad M, Javadzadeh P, Naderinasab M, Shakeri MT. Shear bond strength and antibacterial effects of orthodontic composite containing TiO2 nanoparticles. Eur J Orthod 2013; 35: 676-679.
22) Xie D, Weng Y, Guo X, Zhao J, Gregory RL, Zheng C. Preparation and evaluation of a novel glass-ionomer cement with antibacterial functions. Dent Mater 2011; 27: 487-496.
23) Antonucci JM, Zeiger DN, Tang K, Lin-Gibson S, Fowler BO, Lin NJ. Synthesis and characterization of dimethacrylates containing quaternary ammonium functionalities for dental applications. Dent Mater 2012; 28: 219-228.
24) Zhang K, Melo MA, Cheng L, Weir MD, Bai Y, Xu HH. Effect of quaternary ammonium and silver nanoparticle-containing adhesives on dentin bond strength and dental plaque microcosm biofilms. Dent Mater 2012; 28: 842-852.
25) Imazato S, Ma S, Chen JH, Xu HH. Therapeutic polymers for dental adhesives: loading resins with bio-active components. Dent Mater 2014; 30: 97-104.
26) Simoncic B, Tomsic B. Structures of novel antimicrobial agents for textiles-a review. Text Res J 2010; 80: 1721-1737.
27) Li F, Weir MD, Xu HH. Effects of quaternary ammonium chain length on antibacterial bonding agents. J Dent Res 2013; 92: 932-938.
28) Cheng L, Zhang K, Melo MA, Weir MD, Zhou X, Xu HH. Anti-biofilm dentin primer with quaternary ammonium and silver nanoparticles. J Dent Res 2012; 91: 598-604.
29) Zhou C, Weir MD, Zhang K, Deng D, Cheng L, Xu HH. Synthesis of new antibacterial quaternary ammonium monomer for incorporation into CaP nanocomposite. Dent Mater 2013; 29: 859-870.
30) Zhang K, Cheng L, Wu EJ, Weir MD, Bai Y, Xu HH. Effect of water-ageing on dentine bond strength and anti-biofilm activity of bonding agent containing new monomer dimethylaminododecyl methacrylate. J Dent 2013; 41: 504-513.
31) Zhang N, Zhang K, Melo MA, Chen C, Fouad AF, Bai Y, Xu HHK. Novel protein-repellent and biofilm-repellent orthodontic cement containing 2-methacryloyloxyethyl phosphorylcholine. J Biomed Mater Res B Appl Biomater
2016; 104: 949-959.32) Tuncer C, Tuncer BB, Ulusoy C. Effect of fluoride-releasing
light-cured resin on shear bond strength of orthodontic brackets. Am J Orthod Dentofacial Orthop 2009; 135: 14 e1-6.
33) Pratten J, Wilson M, Spratt DA. Characterization of in vitro oral bacterial biofilms by traditional and molecular methods. Oral Microbiol Immunol 2003; 18: 45-49.
34) Badawi H, Evans RD, Wilson M, Ready D, Noar JH, Pratten J. The effect of orthodontic bonding materials on dental plaque accumulation and composition in vitro. Biomaterials 2003; 24: 3345-3350.
35) McBain AJ, Sissons C, Ledder RG, Sreenivasan PK, De Vizio W, Gilbert P. Development and characterization of a simple perfused oral microcosm. J Appl Microbiol 2005; 98: 624-634.
36) Cheng L, Exterkate RA, Zhou X, Li J, ten Cate JM. Effect of Galla chinensis on growth and metabolism of microcosm biofilms. Caries Res 2011; 45: 87-92.
37) Cheng L, Weir MD, Xu HH, Antonucci JM, Kraigsley AM, Lin NJ, Lin-Gibson S, Zhou X. Antibacterial amorphous calcium phosphate nanocomposites with a quaternary ammonium dimethacrylate and silver nanoparticles. Dent Mater 2012; 28: 561-572.
38) Skold-Larsson K, Borgstrom MK, Twetman S. Effect of an antibacterial varnish on lactic acid production in plaque adjacent to fixed orthodontic appliances. Clin Oral Investig 2001; 5: 118-121.
39) Madlena M, Vitalyos G, Marton S, Nagy G. Effect of chlorhexidine varnish on bacterial levels in plaque and saliva during orthodontic treatment. J Clin Dent 2000; 11: 42-46.
40) Beyth N, Yudovin-Farber I, Bahir R, Domb AJ, Weiss EI. Antibacterial activity of dental composites containing quaternary ammonium polyethylenimine nanoparticles against Streptococcus mutans. Biomaterials 2006; 27: 3995-4002.
41) Zhang K, Cheng L, Weir MD, Bai YX, Xu HH. Effects of quaternary ammonium chain length on the antibacterial and remineralizing effects of a calcium phosphate nanocomposite. Int J Oral Sci 2016; 8: 45-53.
42) Zhou H, Weir MD, Antonucci JM, Schumacher GE, Zhou XD, Xu HH. Evaluation of three-dimensional biofilms on antibacterial bonding agents containing novel quaternary ammonium methacrylates. Int J Oral Sci 2014; 6: 77-86.
676 Dent Mater J 2017; 36(5): 669–676





























