-
Novel H1N1 (Swine) Epidemiology & Control
Ahmed MandilProf of EpidemiologyDept of Family & Community
MedicineCollege of Medicine, King Saud University
Avian Flu
-
Influenza VirusDefinitionsIntroductionSpread/Transmission
Timeline/FactsResponse Case-DefinitionsTreatmentOther Protective
MeasuresConclusion & Recommendations
HEADLINES
-
Credit: L. Stammard, 1995Virus
-
Epidemic a located cluster of casesPandemic worldwide
epidemicAntigenic driftChanges in proteins by genetic point
mutation & selection Ongoing and basis for change in vaccine
each yearAntigenic shift Changes in proteins through genetic
reassortmentProduces different viruses not covered by annual
vaccineDefinitions General
-
Lessons Learned formPast PandemicsFirst outbreaks March 1918 in
Europe, USAHighly contagious, but not deadlyVirus traveled between
Europe/USA on troop shipsLand, sea travel to Africa, AsiaWarning
signal was missedAugust, 1918 simultaneous explosive outbreaks in
in France, Sierra Leone, USA10-fold increase in death rateHighest
death rate ages 15-35 yearsCytokine Storm?Deaths from primary viral
pneumonia, secondary bacterial pneumoniaDeaths within 48 hours of
illnessCoincident severe disease in pigs20-40 million killed in
less than 1 yearWorld War I 8.3 million military deaths over 4
years25-35% of the world infected
-
Pandemics are unpredictableMortality, severity of illness,
pattern of spreadA sudden, sharp increase in the need for medical
care will always occurCapacity to cause severe disease in
nontraditional groups is a major determinant of pandemic
impactEpidemiology reveals waves of infectionAges/areas not
initially infected likely vulnerable in future wavesSubsequent
waves may be more severe1918- virus mutated into more virulent
form1957 schoolchildren spread initial wave, elderly died in second
wavePublic health interventions delay, but do not stop pandemic
spreadQuarantine, travel restriction show little effectDoes not
change population susceptibilityDelay spread in Australia later
milder strain causes infection thereTemporary banning of public
gatherings, closing schools potentially effective in case of severe
disease and high mortality Delaying spread is desirableFewer people
ill at one time improve capacity to cope with sharp increase in
need for medical care
Lessons Learned formPast Pandemics
-
Swine Influenza A(H1N1) IntroductionSwine Influenza (swine flu)
is a respiratory disease of pigs caused by type A influenza that
regularly cause outbreaks of influenza among pigs
Most commonly, human cases of swine flu happen in people who are
around pigs
Swine flu viruses do not normally infect humans, however, human
infections with swine flu do occur, and cases of human-to-human
spread of swine flu viruses have been documented
-
Swine Influenza A(H1N1) Transmission to HumansThrough contact
with infected pigs or environments contaminated with swine flu
viruses
Through contact with a person with swine flu
Human-to-human spread of swine flu has been documented also and
is thought to occur in the same way as seasonal flu, through
coughing or sneezing of infected people
-
Swine Influenza A(H1N1) Transmission Through Species
Reassortment in Pigs
-
Swine Influenza A(H1N1) FactsVirus described as a new subtype of
A/H1N1 not previously detected in swine or humans
CDC determines that this virus is contagious and is spreading
from human to human
The virus contains gene segments from 4 different influenza
types: North American swineNorth American avianNorth American human
and Eurasian swine
-
Swine Influenza A(H1N1) Global ResponseThe WHO raises the alert
level to Phase 6WHOs alert system was revised after Avian influenza
began to spread in 2004 Alert Level raised to Phase 3In Late April
2009 WHO announced the emergence of a novel influenza A virus April
27, 2009: Alert Level raised to Phase 4April 29, 2009: Alert Level
raised to Phase 5June 11, 2008:Alert Level raised to Phase 6
Source: WHO
-
GLOBALLY: March 1-December 23 At least 11,516 Deaths Africa
Region (AFRO): 109Americas Region (AMRO): 6,670 Eastern
Mediterranean Region (EMRO): 663Europe Region (EURO)
:2,045South-East Asia Region (SEARO): 990 Western Pacific Region
(WPRO) :1,039
Source: WHOSwine Influenza A(H1N1) Status UpdateECDC reported a
total of 12,776 deaths December 28, 2009
-
Swine Influenza A(H1N1) CDC Estimates from April-November 14,
2009, By Age GroupSource: CDC.
http://www.cdc.gov/h1niflu/surveillanceqa.htm
2009 H1N1Mid-Level Range*Estimated Range *Cases0-17 years~16
million~12 million to ~23 million18-64 years~27 million~19 million
to ~38 million65 years and older~4 million~3 million to ~6
millionCases Total~47 million~34 million to ~67
millionHospitalizations0-17 years~71,000~51,000 to ~101,00018-64
years~121,000~87,000 to ~172,00065 years and older~21,000~15,000 to
~29,000Hospitalizations Total~213,000~154,000 to ~303,000Deaths0-17
years~1,090~790 to ~1,55018-64 years~7,450~5,360 to ~10,57065 years
and older~1,280~920 to ~1,810Deaths Total~9,820~7,070 to
~13,930
-
Pandemic (H1N1) 2009 in the EMR as of 6 November, 200922/22
countries affectedRegular reports from 17 countries: 26,400
confirmed cases and 150 deaths.Localized to moderate geographical
distribution.Increasing trend in most of the countriesLow to
moderate intensity Low to moderate impact on the health system
CountryCumulative number of confirmed casesCumulative number of
deathsTrendKuwait6,
64017IncreasingUAE790NABahrain7936NALebanon7612NAEgypt1,
5925IncreasingSaudi Arabia4, 11928NAPalestine
7771IncreasingMorocco4840IncreasingJordan2, 0503Increasing
Qatar231NAYemen62917IncreasingOman3, 32925IncreasingIran1,
63822IncreasingTunisia1, 2850IncreasingIraq1,
0807IncreasingLibya210UnchangedSyria1606IncreasingAfghanistan77210IncreasingSudan70Unchanged
Pakistan50UnchangedDjibouti90UnchangedSomalia20UnchangedTotal26,400150
-
Pandemic H1N1 2009 in the EMR as of 6 November, 2009
Avian Flu
-
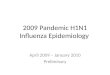
The Epidemic CurveSingle-wave profile showing proportion of new
clinical cases, consultations, hospitalisations or deaths by week.
Based on London, second wave 1918.
0%5%10%15%20%123456789101112WeekProportion of total cases,
consultations, hospitalisations or deaths
InitiationAccelerationPeakDecline
-
Aims of community reduction of influenza transmission
mitigationDelay and flatten epidemic peak.Reduce peak burden on
healthcare system and threat.Somewhat reduce total number of cases.
Buy a little time.DailycasesDays since first caseNo
intervention
-
Swine Influenza A(H1N1) Mediterranean & Middle East
Confirmed Deathsn=1,246Source: ECDCAs of December 28, 2009
-
Global Distribution of Reported Laboratory Confirmed Cases &
Deaths of Swine Influenza A(H1N1), December 23, 2009 Source:
WHO
-
Geographic Spread of Influenza ActivityBased Upon Country
Reporting, Week 50, 2009 (07-23 December)Source: WHO
-
Impact on Healthcare Services Based Upon Degree of Disruption,
As a Result of Acute Respiratory DiseasesWeek 50, 2009 (07-13
December)Source: WHO
-
Number of Specimens Positive for Influenza Sub-TypeSource:
CDC
-
Laboratory-Confirmed Cases & Deaths of New Influenza A(H1N1)
by WHO Regions, September 20, 2009 *Given that countries are no
longer required to test and report individual cases, the number of
cases reported actually understates the real number of cases. At
least 318,925 Cases & Over 3917 DeathsOverall Case-Fatality
Rate (CFR) in Confirmed ~ 1.2%Source: WHOCFR = 0.5%CFR = 2.5%CFR =
0.6%CFR = 1.1%CFR = 0.3%CFR = 0.4%
-
Swine Influenza A(H1N1) Guidelines for General
PopulationCovering nose and mouth with a tissue when coughing or
sneezingDispose the tissue in the trash after use. Handwashing with
soap and waterEspecially after coughing or sneezing. Cleaning hands
with alcohol-based hand cleaners Avoiding close contact with sick
peopleAvoiding touching eyes, nose or mouth with unwashed handsIf
sick with influenza, staying home from work or school and limit
contact with others to keep from infecting them
-
Comparison of Available Influenza Diagnostic Tests1 Source:
CDC
Influenza Diagnostic TestsMethodAvailabilityTypicalProcessing
Time2Sensitivity3 for2009 H1N1influenzaDistinguishes 2009 H1N1
influenza from other influenza A viruses?Rapid influenza diagnostic
tests (RIDT)4Antigen detectionWide0.5 hour10 70%NoDirect and
indirectImmunofluorescenceassays (DFA and IFA)5Antigen
detectionWide2 4 hours4793%NoViral isolation in tissue
cellcultureVirus isolationLimited2 -10 days-Yes 6Nucleic acid
amplification tests (including rRT-PCR) 7RNA detectionLimited848 96
hours [6-8 hours toperform test]86 100%Yes
Avian Flu
-
There are two flu antiviral drugs recommendedOseltamivir or
Zanamivir Use of anti-virals can make illness milder and recovery
faster
They may also prevent serious flu complications
For treatment, antiviral drugs work best if started soon after
getting sick (within 2 days of symptoms)
Warning! Do NOT give aspirin (acetylsalicylic acid) or
aspirin-containing products (e.g. bismuth subsalicylate Pepto
Bismol) to children or teenagers (up to 18 years old) who are
confirmed or suspected ill case of swine influenza A (H1N1) virus
infection; this can cause a rare but serious illness called Reyes
syndrome. For relief of fever, other anti-pyretic medications are
recommended such as acetaminophen or non steroidal
anti-inflammatory drugs.
Treatment is recommended for: All hospitalized patients with
confirmed, probable or suspected novel influenza (H1N1). Patients
who are at higher risk for seasonal influenza complicationsIf
patient is not in a high-risk group or is not hospitalized,
healthcare providers should use clinical judgment to guide
treatment decisions
Swine Influenza A(H1N1) Antiviral ProtectionSource: CDC
-
Antiviral Chemoprophylaxis for Treatment: Post-exposure:
Duration chemoprophylaxis is 10 days after the last known exposure
to novel (H1N1) influenza and may be considered in the following:
Close contacts of cases (confirmed, probable, or suspected)Health
care personnel, public health workers, or first responders who have
had a recognized, unprotected close contact exposure to a person
(confirmed, probable, or suspected) during that persons infectious
period.
Pre-exposure: Antivirals should only be used in limited
circumstances, and in consultation with local medical or public
health authorities.
Antiviral Use for Control of Novel H1N1 Influenza OutbreaksA
cornerstone for the control of seasonal influenza outbreaks in
nursing homes and other long term care facilities. If outbreaks
were to occur, it is recommended that ill patients be treated with
oseltamivir or zanamivir and that chemoprophylaxis with either
oseltamivir or zanamivir be started as early as possible to reduce
the spread of the virus as is recommended for seasonal influenza
outbreaks in such settings.
Children Under 1 Year of AgeOseltamivir is not licensed for use
in children less than 1 year of age. Because infants experience
high rates of morbidity and mortality from influenza, infants with
novel (H1N1) influenza virus infections may benefit from treatment
using oseltamivir.
Swine Influenza A(H1N1) Antiviral ProtectionSource: CDC
- Source: CDCDosing recommendations for antiviral treatment of
children younger than 1 year using oseltamivir. Recommended
treatment dose for 5 days.
-
Novel H1N1 vaccine available for since Mid-September
Seventh Harvard Pandemic Survey 38% of Children in the US
immunized50% Adults do not intend to be immunized35% of parents do
not intend to get their children immunized
Novel H1N1 vaccine is not intended to replace the seasonal flu
vaccine it is intended to be used along-side seasonal flu
vaccine
Vaccines:Inactivated influenza virus vaccinesCSL Ltd. of
Australia Novartis Vaccines of Switzerland Sanofi Pasteur of France
800,000 pre-filled syringes were recalled are for young children,
ages 6 months to 3 years in the USGlaxoSmithKline (GSK) of
UKSinovac Biotech of ChinaLive-attenuated virus vaccineMedImmune
LLC of US (nasal-spray)4.5 million doses recalled due to decreased
potency in the USSwine Influenza A(H1N1) Vaccine Protection
-
CDCs Advisory Committee on Immunization Practices (ACIP)
recommends the following groups to receive the novel H1N1 influenza
vaccine:
Pregnant women because they are at higher risk of complications
and can potentially provide protection to infants who cannot be
vaccinated;
Household contacts and caregivers for children younger than 6
months of age because younger infants are at higher risk of
influenza-related complications and cannot be vaccinated.
Vaccination of those in close contact with infants less than 6
months old might help protect infants by cocooning them from the
virus;
Healthcare and emergency medical services personnel because
infections among healthcare workers have been reported and this can
be a potential source of infection for vulnerable patients. Also,
increased absenteeism in this population could reduce healthcare
system capacity;
All people from 6 months through 24 years of age
Children from 6 months through 18 years of age because we have
seen many cases of novel H1N1 influenza in children and they are in
close contact with each other in school and day care settings,
which increases the likelihood of disease spread, and
Young adults 19 through 24 years of age because we have seen
many cases of novel H1N1 influenza in these healthy young adults
and they often live, work, and study in close proximity, and they
are a frequently mobile population; and,
Persons aged 25 through 64 years who have health conditions
associated with higher risk of medical complications from
influenza.
Swine Influenza A(H1N1) Vaccine ProtectionSource: CDC
-
Swine Influenza A(H1N1): Face Mask and Respirator
ProtectionSource: CDC
SettingPersons not at increased risk of severe illness from
influenza(Non-high risk persons)Persons at increased risk of severe
illness from influenza (High-Risk Persons)CommunityNo 2009 H1N1 in
communityFacemask/respirator not recommendedFacemask/respirator not
recommended2009 H1N1 in community: not crowded
settingFacemask/respirator not recommendedFacemask/respirator not
recommended2009 H1N1 in community: crowded
settingFacemask/respirator not recommendedAvoid setting. If
unavoidable, consider facemask or respiratorHomeCaregiver to person
with influenza-like illnessFacemask/respirator not recommendedAvoid
being caregiver. If unavoidable, use facemask or respiratorOther
household members in homeFacemask/respirator not
recommendedFacemask/respirator not recommendedOccupational
(non-health care)No 2009 H1N1 in communityFacemask/respirator not
recommendedFacemask/respirator not recommended2009 H1N1 in
communityFacemask/respirator not recommended but could be
considered under certain circumstancesFacemask/respirator not
recommended but could be considered under certain
circumstancesOccupational (health care)Caring for persons with
known, probable or suspected 2009 H1N1 or influenza-like illness
RespiratorConsider temporary reassignment. Respirator
Avian Flu
-
Swine Influenza A(H1N1) Other Protective MeasuresDefining
Quarantine vs. Isolation vs. Social-Distancing Isolation: Refers
only to the sequestration of symptomatic patents either in the home
or hospital so that they will not infect others
Quarantine: Defined as the separation from circulation in the
community of asymptomatic persons that may have been exposed to
infection
Social-Distancing: Has been used to refer to a range of
non-quarantine measures that might serve to reduce contact between
persons, such as, closing of schools or prohibiting large
gatheringsSource: CDC
-
Swine Influenza A(H1N1) Other Protective MeasuresPersonnel
Engaged in Aerosol Generating Activities CDC Interim
recommendations:Personnel engaged in aerosol generating activities
(e.g., collection of clinical specimens, endotracheal intubation,
nebulizer treatment, bronchoscopy, and resuscitation involving
emergency intubation or cardiac pulmonary resuscitation) for
suspected or confirmed swine influenza A (H1N1) cases should wear a
fit-tested disposable N95 respirator
Pending clarification of transmission patterns for this virus,
personnel providing direct patient care for suspected or confirmed
swine influenza A (H1N1) cases should wear a fit-tested disposable
N95 respirator when entering the patient room
Respirator use should be in the context of a complete
respiratory protection program in accordance with Occupational
Safety and Health Administration (OSHA) regulations. Source:
CDC
-
Infection Control of Ill Persons in a Healthcare Setting
Patients with suspected or confirmed case-status should be
placed in a single-patient room with the door kept closed. If
available, an airborne infection isolation room (AIIR) with
negative pressure air handling with 6 to 12 air changes per hour
can be used. Air can be exhausted directly outside or be
recirculated after filtration by a high efficiency particulate air
(HEPA) filter. For suctioning, bronchoscopy, or intubation, use a
procedure room with negative pressure air handling.
The ill person should wear a surgical mask when outside of the
patient room, and should be encouraged to wash hands frequently and
follow respiratory hygiene practices. Cups and other utensils used
by the ill person should be washed with soap and water before use
by other persons. Routine cleaning and disinfection strategies used
during influenza seasons can be applied to the environmental
management of swine influenza. Swine Influenza A(H1N1) Other
Protective MeasuresSource: CDC
-
Infection Control of Ill Persons in a Healthcare Setting
Standard, Droplet and Contact precautions should be used for all
patient care activities, and maintained for 7 days after illness
onset or until symptoms have resolved. Maintain adherence to hand
hygiene by washing with soap and water or using hand sanitizer
immediately after removing gloves and other equipment and after any
contact with respiratory secretions.
Personnel providing care to or collecting clinical specimens
from suspected or confirmed cases should wear disposable
non-sterile gloves, gowns, and eye protection (e.g., goggles) to
prevent conjunctival exposure.Swine Influenza A(H1N1) Other
Protective MeasuresSource: CDC
-
SummaryWHO raised the alert level to Phase 6 on June 11, 2009As
of December 28, 2009, worldwide more than 208 countries and
overseas territories or communities have reported laboratory
confirmed cases of pandemic influenza H1N1 2009, including at least
13,000 deaths Northern Hemisphere: Overall disease activity has
recently peaked.Central and Eastern Europe, and in parts of West,
Central, and South Asia: Continued increases in influenza activity
United States and Canada: Influenza activity continues to be
geographically widespread but overall levels of
influenza-like-illness has declined substantially Approximately 53%
of hospitalized cases in Canada had an underlying medical
conditionEurope: Widespread and active transmission continued to be
observed throughout the continentOverall pandemic influenza
activity appears to have recently peaked across a majority of
countriesWestern and Central Asia: Virus circulation remains active
throughout the region, however disease trends remain variableEast
Asia: Influenza transmission remains active but appears to be
declining overallCentral and South America and the Caribbean:
influenza transmission remains geographically widespread but
overall disease activity has been declining or remains unchanged in
most parts, except for in Barbados and Ecuador, were recent
increases in respiratory diseases activity have been
reportedSouthern Hemisphere: Sporadic cases of pandemic influenza
continued to be reported without evidence of sustained community
transmission.
-
SummaryIn the US Highest incidence of lab-confirmed cases
reported among 5-24 years oldHighest hospitalization rate among 0-4
years oldUnderlying health conditions confers high risk of
complications and deathsIn MexicoMajority of the cases reported in
health young adults70% of the deaths were reported in healthy young
adults, 20-54 years Individuals 60+ seem to be protected as the
number of cases and have a lower case-fatality compared to the rest
of the populationIn EUMajority of the cases reported in health
young adults (20-29 years)GloballyNumber of deaths being reported
is risingVaccine Total Adverse Events: 5.4% (0.3% fatal)Sanofi
Pasteur & MedImmune vaccine recalled due to potency
issuesAnti-virals (oseltamivir and zanamivir)Oseltamivir resistance
reported recently in immunocompromised patents
-
Conclusion/RecommendationsPast experience with pandemics have
taught us that the second wave is worse than the first causing more
deaths due to:Primary viral pneumonia, Acute Respiratory Distress
Syndrome (ARDS), & Secondary bacterial infections, particularly
pneumoniaFortunately compared to the past now we have vaccines,
anti-virals and antibiotics (to treat secondary bacterial
infections) & rT-PCR based rapid diagnostic devicesThis
pandemic is milder than previously predicted with a case-fatality
less than 1%
At present most of the deaths due to the novel H1N1 strain has
been reported from the Americas. Disease seems to be affecting the
healthy strata of the population based upon epidemiological
dataAnecdotal data suggests that the number of deaths among the
pediatric population has risen recently due to infection with the
novel H1N1Most of these deaths however have been reported in cases
with underlying medical conditions60 years and above age group
seems to show some protection against this strain suggesting past
exposure and some immunity
-
Conclusion/RecommendationsEach locality/jurisdiction needs to
Have enhanced disease and virological surveillance
capabilitiesDevelop a plan to house large number of severely sick
and provide care if needed to deal with mildly sick at home
(voluntary quarantine) Healthcare facilities/hospitals need to
focus on increasing surge capacity and stringent infection
prevention/controlGeneral population needs to follow basic
precautions
In the Northern Hemisphere influenza viral transmission
traditionally stops by the beginning of May but in pandemic years
(1957) sporadic outbreaks occurred during summer among young
adultsThis novel H1N1 strain has survived high humidity or
temperature and continued to spread during the summer months and
will continue to spread and cause infection
-
Conclusion/RecommendationsSchool Closures:Preemptive school
closures merely delay the spread of disease Once schools reopen the
disease transmits and spreads Puts unbearable pressure on
single-working parents and would be devastating to the economy
Closure after identification of a large cluster would be
appropriate as absenteeism rate among students and teachers would
be high enough to justify this action
Burden of Disease & MortalityActual burden of the disease
will be higher than the regular seasonal flu despite the
availability of vaccine, antivirals and excellent public knowledge
With the variation in reporting it is very difficult to appreciate
the total number of deaths
It is imperative to appreciate that times-have-changed Though
this strain has spread very quickly across the globe and seems to
be highly infectious, today we are much better prepared than 1918
There is better surveillance, communication, understanding of
infection control, vaccines, anti-virals, antibiotics and
advancement in science and resources to produce countermeasures
quickly
-
References World Health Organization
(WHO):http://www.who.int/csr/disease/avian_influenza/en/ World
Organization for Animal Health (OIE):
http://www.oie.int/wahid-prod/public.php? Centers for Disease
Control & Prevention (CDC):
http://www.cdc.gov/flu/avian/index.htmChotani R. Just-in-time, H1N1
Influenza. Epidemiology Supercourse. December 2009.El-Bushra H.
Global and Regional Update on Human Pandemic Influenza A H1N1 2009.
Cairo: WHO/EMRO, 2009
**This lecture provides basic information on Swine Flu. The
lecture is updated to include the latest information and data.*The
internal antigens (M1 and NP proteins) are the type-specific
proteins (type-specific antigens) used to determine if a particular
virus is A, B or C. The M1 proteins of all members of each type
show cross reactivity. The NP proteins of all members of each type
also show cross reactivity.The external antigens (HA and NA) show
more variation and are the subtype and strain-specific antigens.
These are used to determine the particular strain of influenza A
responsible for an outbreakFlu strains are named after their types
of hemagglutinin and neuraminidase surface proteins, so they will
be called, for example, H3N2 for type-3 hemagglutinin and type-2
neuraminidase. If two different strains of influenza infect the
same cell simultaneously, their protein capsids and lipid envelopes
are removed, exposing their RNA, which is then transcribed to mRNA.
The host cell then forms new viruses that combine antigens; for
example, H3N2 and H5N1 can form H5N2 this way. Because the human
immune system has difficulty recognizing the new influenza strain,
it may be highly dangerous.
*A cytokine storm is the systemic expression of a healthy and
vigorous immune system resulting in the release of more than 150
inflammatory mediators (cytokines, oxygen free radicals, and
coagulation factors). Both pro-inflammatory cytokines (such as
Tumor Necrosis Factor-alpha, InterLeukin-1, and InterLeukin-6) and
anti-inflammatory cytokines (such as interleukin 10, and
interleukin 1 receptor antagonist) are elevated in the serum, and
the fierce and often lethal interplay of these cytokines is
referred to as a "Cytokine Storm". The primary contributors to the
cytokine storm are TNF-a (Tumor Necrosis Factor-alpha) and IL-6
(Interleukin-6). The cytokine storm is an inappropriate
(exaggerated) immune response that is caused by rapidly
proliferating and highly activated T-cells or natural killer (NK)
cells. These cells are themselves activated by infected
macrophages. The cytokine storm must be treated and suppressed or
lethality can result. *Reassortment, or Viral Subunit Reassortment,
is the exchange of DNA between viruses inside a host cell. Two or
more viruses of different strains (but usually the same species)
infect a single cell and pool their genetic material creating
numerous genetically diverse progeny viruses. It is a type of
genetic recombination.Reassortment can lead to a viral shifts under
some conditions.
*WHO Definition of Phases Phase 4 is characterized by verified
human-to-human transmission of an animal or human-animal influenza
reassortant virus able to cause community-level outbreaks. The
ability to cause sustained disease outbreaks in a community marks a
significant upwards shift in the risk for a pandemic. Any country
that suspects or has verified such an event should urgently consult
with WHO so that the situation can be jointly assessed and a
decision made by the affected country if implementation of a rapid
pandemic containment operation is warranted. Phase 4 indicates a
significant increase in risk of a pandemic but does not necessarily
mean that a pandemic is a forgone conclusion. Phase 5 is
characterized by human-to-human spread of the virus into at least
two countries in one WHO region. While most countries will not be
affected at this stage, the declaration of Phase 5 is a strong
signal that a pandemic is imminent and that the time to finalize
the organization, communication, and implementation of the planned
mitigation measures is short. Phase 6, the pandemic phase, is
characterized by community level outbreaks in at least one other
country in a different WHO region in addition to the criteria
defined in Phase 5. Designation of this phase will indicate that a
global pandemic is under way.During the post-peak period, pandemic
disease levels in most countries with adequate surveillance will
have dropped below peak observed levels. The post-peak period
signifies that pandemic activity appears to be decreasing; however,
it is uncertain if additional waves will occur and countries will
need to be prepared for a second wave. Previous pandemics have been
characterized by waves of activity spread over months. Once the
level of disease activity drops, a critical communications task
will be to balance this information with the possibility of another
wave. Pandemic waves can be separated by months and an immediate
at-ease signal may be premature. In the post-pandemic period,
influenza disease activity will have returned to levels normally
seen for seasonal influenza. It is expected that the pandemic virus
will behave as a seasonal influenza A virus. At this stage, it is
important to maintain surveillance and update pandemic preparedness
and response plans accordingly. An intensive phase of recovery and
evaluation may be required.
*World Health Organization**World Health Organization**For
planning purposes there are these four components of a pandemic
wave Initiation, Acceleration, Peak and Decline. The percentage on
the vertical axis represents the proportion of all those infected
in the first wave that are infected in the different phases After
the decline there may be a second and even a third wave before
influenza settles back down to its seasonal pattern again. The
seasonal flu is usually worse than the years before the pandemic
because the seasonal flu is invigorated with new genetic material.
The same four phases actually apply to epidemics as well. This
particular wave has been given an erratic Initiation Phase
representing what is happening in Europe in the summer and perhaps
early Autumn when there are small outbreaks and it is not clear
when each country will enter their Acceleration Phase. However, no
pandemic has ever behaved in quite so neat a way as shown here.
Pandemics dont follow set patterns and each is different. It is
also important that this is a national curve. The local curves are
more narrow and with a higher central peak, i.e. local pandemic
spread is shorter and sharper but also highly variable.This slide
the original of which was developed by the United States CDC
illustrates the theoretical aims of community mitigation by public
health measures, mass use of antivirals etc. However it needs to be
appreciated that the effectiveness of PHM is by no means certain. A
further discussion of this can be found through the ECDC PHM Menu
http://ecdc.europa.eu/en/Health_Topics/Pandemic_Influenza/phm.aspx
1 - Serologic testing on paired acute- (within 1 week of illness
onset) and convalescent-phase (collected 2-3 weeks later) sera is
limited to epidemiological and research studies, is not routinely
available through clinical laboratories, and should not inform
clinical decisions. 2 - The amount of time needed from specimen
collection until results are available. 3 - Compared with rRT-PCR
tests; rRT-PCR tests are compared to other testing modalities
including other rRT-PCR assays. 4 - Rapid Influenza Diagnostic
Tests include tests that are CLIA waived (can be performed in an
outpatient setting) and tests that are moderately complex (can be
performed only in a laboratory). Clinical specimens approved for
RIDTs vary by test, and may not include all respiratory specimens.
5 - Performance of these assays relies heavily on laboratory
expertise and requires a fluorescent microscope 6 - Requires
additional testing on the viral isolate 7 - The performance of
rRT-PCR assays specific for 2009 H1N1 influenza have not been
established for bronchoalveolar lavage and tracheal aspirates. If
testing these specimens for 2009 H1N1 influenza consider testing in
parallel with a nasopharyngeal, nasal, or oropharyngeal swabs or a
nasal aspirate. 8 - See discussion on available rRT-PCR assays at
http://www.cdc.gov/h1n1flu/guidance/diagnostic_tests.htmPregnant
WomenOseltamivir and zanamivir are "Pregnancy Category C"
medications, indicating that no clinical studies have been
conducted to assess the safety of these medications for pregnant
women. Because of the unknown effects of influenza antiviral drugs
on pregnant women and their fetuses, oseltamivir or zanamivir
should be used during pregnancy only if the potential benefit
justifies the potential risk to the embryo or fetus; the
manufacturers' package inserts should be consulted. However, no
adverse effects have been reported among women who received
oseltamivir or zanamivir during pregnancy or among infants born to
women who have received oseltamivir or zanamivir. Pregnancy should
not be considered a contraindication to oseltamivir or zanamivir
use. Because of its systemic activity, oseltamivir is preferred for
treatment of pregnant women. The drug of choice for prophylaxis is
less clear. Zanamivir may be preferable because of its limited
systemic absorption; however, respiratory complications that may be
associated with zanamivir because of its inhaled route of
administration need to be considered, especially in women at risk
for respiratory problems.Adverse Events:
http://www.cdc.gov/flu/professionals/antivirals/side-effects.htmStaff
should be medically cleared, fit-tested, and trained for respirator
use, including: proper fit-testing and use of respirators, safe
removal and disposal, and medical contraindications to respirator
use. Information on respiratory protection programs and fit test
procedures can be accessed at
www.osha.gov/SLTC/etools/respiratory
More information can be found at
http://www.cdc.gov/ncidod/dhqp/gl_environinfection.html
Please send questions or comments to Dr. Chotani at
[email protected] send questions or comments to Dr. Chotani
at [email protected]