Embed Size (px)
Citation preview
11/29/2016
1
Taking the Leap –Radical System Transformation to Advanced Team Based Care
Presented byBellin HealthJames Jerzak, MDKathy Kerscher, BACynthia Lasecki, MDBrad Wozney, MD
M-22This presenter has
nothing to disclose
12/5/20168:30 – 4:00
#IHIFORUM
Session ObjectivesP2
#IHIFORUM
• To develop a practical framework for implementing an advanced team based care model of patient care that produces 3 Wins – a win for the patient, a win for the care team and a win for they system.
• To develop a plan to build the necessary infrastructure for a sustainable model of team base care across your organization.
• To develop the cultural changes necessary to transform your system and to support radical system redesign to team based care.
• To understand the barriers to implementing team based care, and to develop strategies for overcoming these barriers.
11/29/2016
2
Agenda
8:30 Introductions/About Bellin Health 8:45 Huddle 1 – Setting the Stage 9:00 Bellin Health’s Journey 9:30 The Foundation of System Transformation
10:00 Break -15 min10:15 9 step framework – Primary Care 11:15 Questions and Answers 11:30 Huddle 2- Getting to Work11:45 Lunch
1:00 Infrastructure Training/Financials
2:30 Break 2:45 Barriers 3:30 General Lessons Learned3:45 Open Discussion4:00 Huddle 3 -Plan for Home
Kathy Kerscher
Team Based Care – Change Leader
11/29/2016
3
Introductions
Bellin Health – Planning Team Members, Team Based
Care Transformation
James Jerzak M.D.
Kathy Kerscher
Cynthia Lasecki M.D.
Brad Wozney M.D.
Bellin Health OverviewServing a Market of 636,682 People Bellin Hospital, a 244-bed community hospital with proven
excellence in heart and vascular care; orthopedics and sports
medicine; family programs and services; cancer care; and
minimally invasive procedures including robotic surgery
Bellin Health Oconto Hospital, a 10-bed critical-access
hospital in Oconto
Bellin Medical Group , a 121-member primary care group
with 27 clinic sites and proven excellence in disease
management and wellness care
Employer Clinics, 125 clinics located within employer
facilities
FastCare Retail Clinics, 4 convenient care clinics in
discount retail stores
Bellin Health Partners incorporates all of Bellin Health
System, their employed providers and approximately 116
independent providers
Bellin Psychiatric Center, a dominant provider of in- and
outpatient behavioral health services, staffed by 10
psychiatrists, 4 psychologists, and 35 licensed mental health
& addiction therapists
Unity Hospice, providing hospice and palliative care
services

11/29/2016
4
7
Mission / VisionMission:
Bellin Health is a community-owned not-for-profit organization responsible for
improving the health and wellbeing of people living in Northeast Wisconsin and
the Upper Peninsula of Michigan, and all others we serve.
We carry out this responsibility through individualized care excellence,
community health improvement, and equitable healthcare financing plans –all
designed to positively impact health and wellbeing. We are steadfast in our
commitment to providing compassionate, safe, and coordinated care that is
accessible and affordable for everyone.
We build trusted relationships and advance true collaboration, fueling our desire
to constantly improve and innovate.
Vision:
The people in our region will be the healthiest in the nation, resulting in improved economic vitality in the communities we serve.
8
Strategic Objectives
Patient, Family and Customer-Driven Organization
Bellin Health provides a individualized and equitable experience for every patient, family and customer by creating trusted relationships that allow us to know them, care for them, and ease their way. We embrace them as partners on their journey toward optimal health and wellbeing.

11/29/2016
5
9
Strategic ObjectivesTeam Culture
Bellin Health creates and engages teams of healthcare professionals, patients, board members, volunteers and community members, empowering them to achieve our vision. We will maintain a positive culture rooted in relationships and our core values:• People are the foundation of Bellin Health. As individuals, team
members, and members of various communities, our actions and attitudes must demonstrate respect, commitment, accountability, competence, and integrity.
• Service Excellence is provided in every interaction.• Continuous Improvement ensures customer and staff safety and
achieves superior outcomes.• Learning & Development enables personal and organizational
excellence through the advancement of our knowledge and skill in support of our Mission and Vision.
• Innovative Thinking fosters an environment to attain breakthrough results.
10
Population Health Improvement
By building trusted relationships and advancing true
collaboration we improve the health and wellbeing of the
populations and communities we serve while providing an
exceptional experience and reducing costs.
Strategic Objectives
11/29/2016
6
11
Growth and Sustainability
Bellin Health will continue to be a financially strong and
sustainable organization by increasing the number of people
aligned with us and striving to provide the lowest cost of care
in the nation.
Strategic Objectives
TEAM HUDDLE - 1
Setting the StageKathy Kerscher
11/29/2016
7
Advanced Team Based Care;
Bellin Health’s Journey
James Jerzak, MD
Cynthia Lasecki, MD
11/29/2016
8
Disclosure
No relevant conflicts of
interest to disclose
11/29/2016
9
Agenda
Setting the Stage : Advanced Team Based Care:
• Why Now?
• What is It?
• How did we get there?
Why Now?
• Clinician and staff burnout
• More complex patient needs, coupled with higher copays
and deductibles, leads to a higher intensity of the office visit.
• Impending change to value based reimbursement will
require a new focus and even greater emphasis on
achieving quality goals
• At Bellin Health, our vision is to have the healthiest people
in the country
11/29/2016
10
”The current practice model in Primary Care is unsustainable.”
C. Sinsky, M.D. et. al.
Bellin Health’s View – Fundamental
Causes of Burnout
• EHR demands on the provider during the
office visit.
• Inefficient workflow of the in basket work
with most work directed to provider.
• Challenge for individual clinicians to provide
comprehensive care to increasingly complex
patients.
11/29/2016
11
”Physician Burnout is a Public Health Crisis”
Art Caplin PhD.Division of
Medical Ethics NYU
Bellin Health’s View of the Solution:
FIX THE PROBLEM !!
11/29/2016
12
Bellin Health’s Journey
Achieving Population Health
Through Team Based Care
11/29/2016
13
Evolution of Transformation - 1
“Primary Care Redesign”
Timeline to Transformation
March 2014
SWOT analysis
Future of Primary Care meeting,
Administration and physicians
11/29/2016
14
Timeline to Transformation
May 2014
Visit to Stanford - Coordinated
Care of Complex patients, Dr Alan
Glasaroff, Dr Ann Lindsley
Evolution of Transformation - 2
”Patient Care
Redesign”

11/29/2016
15
Timeline to Transformation
June 30,2014
First weekly meeting of planning
team
Beginning of true collaboration
Timeline to Transformation
June 30, 2014 –
Planning Team• Composed of 4 physicians, 2 advanced practice
clinicians, and administrative support including
executive sponsor, change lead, IT
representative, change engineer, project
manager, and others as needed
• Meeting 4 hours weekly since then
11/29/2016
16
Planning Team Work, mid 2014:
Development of Problem, Aim, and Vision statements
Problem Statement
Problem: An imbalanced workload with
misaligned incentives has led to
unattained Patient care goals
11/29/2016
17
Aim Statement
Aim: Build a prototype for team based
care that is scalable throughout the
medical and specialty group
Vision Statement
Vision: A healthier patient who is
empowered to better manage his/her own
personal health with the support of the
Bellin Health medical team
11/29/2016
18
Timeline to Transformation
November 3 2014
Prototype Launch
One MD and one NP
11/29/2016
19
Transformation Timeline
May 18,2015
Spread of prototype to other
planning team members
”Good beginning, half done”
Fortune cookie
11/29/2016
20
Transformation Timeline
11/29/2016
21
WHAT IS IT?
Our Definition: Advanced Team Based Care
“A comprehensive approach to health care delivery transformation including office visit redesign, in-basket management redesign, and use of extended care team members and system resources to deliver effective population health management”
11/29/2016
22
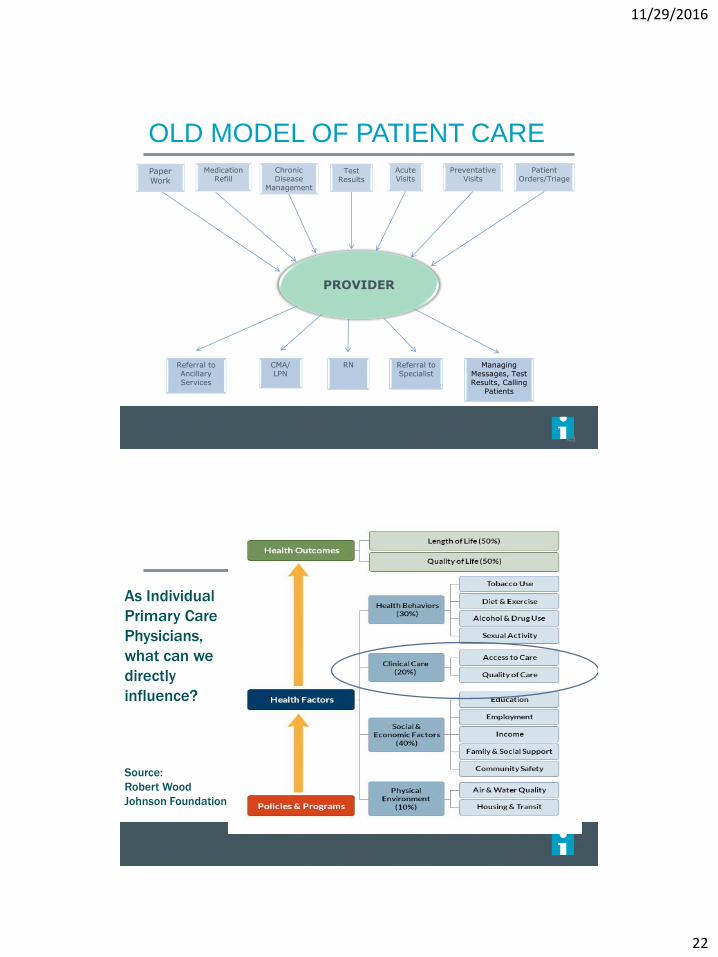
MedicationRefill
Chronic Disease
Management
PROVIDER
Test Results
AcuteVisits
PreventativeVisits
Patient Orders/Triage
RNCMA/LPN
Referral to Specialist
Referral to Ancillary Services
Managing Messages, Test Results, Calling
Patients
Paper Work
OLD MODEL OF PATIENT CARE
43
As Individual
Primary Care
Physicians,
what can we
directly
influence?
Source:
Robert Wood
Johnson Foundation
• .
11/29/2016
23
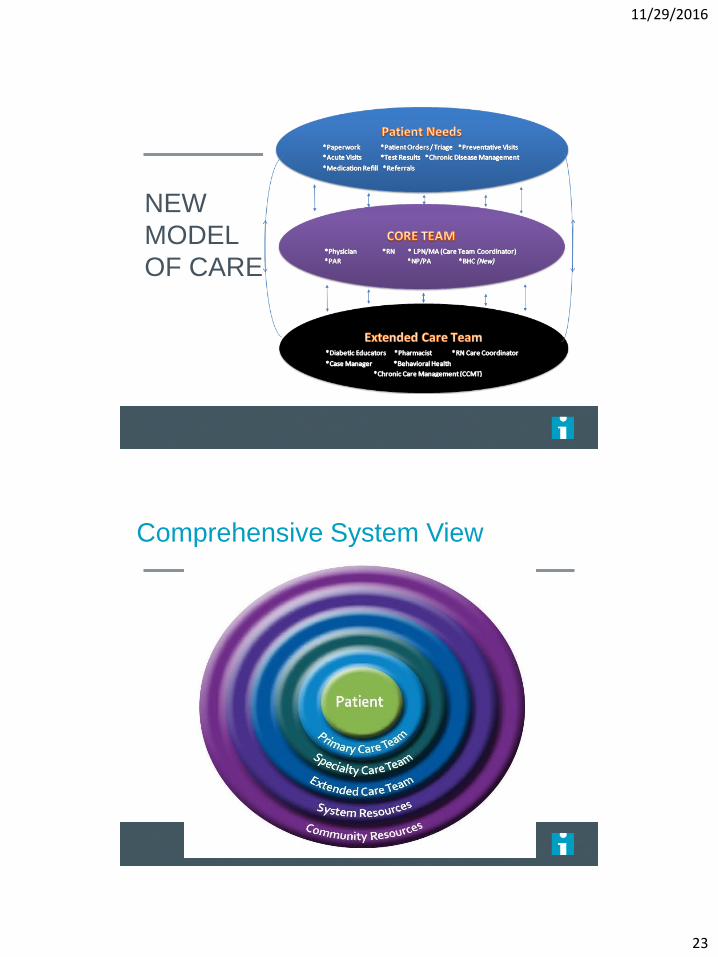
NEW
MODEL
OF CARE
Comprehensive System View
11/29/2016
24
Evolution of Transformation - 3
”Achieving Population
Health through Team
Based Care”
The Three Wins (details later)
Win for the Patient
Win for the Care Team
Win for the System
11/29/2016
25
Current Status: November 2016
22 MD/DOs live on full team based care
11 NP/PAs live on full team based care
Finalizing criteria and expectations for team
based care for clinicians
Finalizing spread plan for rest of Bellin Medical
Group and Bellin Health
Refining approach to specialty, condition, and
hospital work
11/29/2016
26
“Joy in practice implies a fundamental redesign of the medical encounter to restore the healing relationship of patients with their physicians and health care systems.”
C. Sinsky, M.D. et. al.
“Do you want to be part of the future, or
do you want to resist the future?”
Garret Camp
Founder of Uber
11/29/2016
27
11/29/2016
28
The Foundation of System
TransformationA Population Health Framework
Bradley Wozney, MD
Disclosure
No relevant conflicts of
interest to disclose

11/29/2016
29
Agenda
1. Population Health vs Population Management
vs Population Health Management
2. Our 9 step model
3. Our populations
4. Putting it all together
57
Population Health – Bellin Health definition
An opportunity for health care delivery systems, public health agencies, community-based organizations, and many other entities to work together to improve health outcomes in the communities they serve.
It’s Bellin Health’s vision:
The people in our region will be the healthiest in the nation,
resulting in improved economic vitality in the communities we
serve.
58
11/29/2016
30
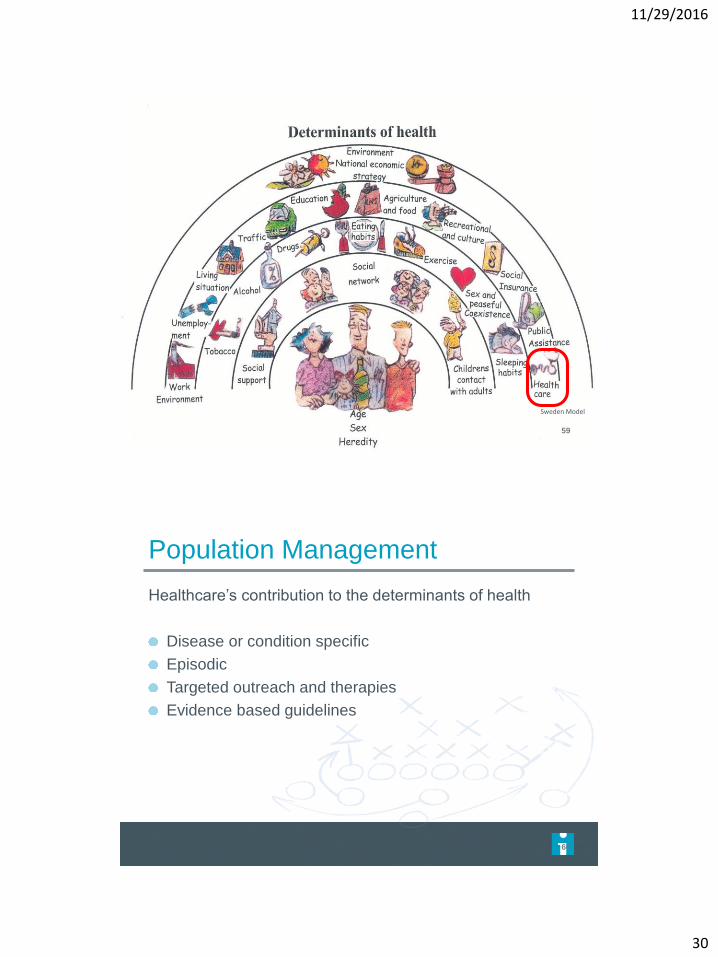
59
Sweden Model
Population Management
Healthcare’s contribution to the determinants of health
Disease or condition specific
Episodic
Targeted outreach and therapies
Evidence based guidelines
60
11/29/2016
31
So, what is Population Health Management?
61
62
11/29/2016
32
Bellin’s 9 Step Model
1. Knowledge of the population
Understand the needs of the population
Allows for risk stratification
Clinical and nonclinical data
2. Define goals
Triple Aim focused
3. High level design
Demand/capacity matching
Resource allocation
63
4. Activate the care team
Clearly defined work flows
Training
Team building
5. Engage the individual
Patient activation level
Goal setting
6. Measure outcomes
Defined in step 2
64
11/29/2016
33
7. Provide feedback
Specific to the role
8. 30 day action plans
9. Celebrate and recalibrate goals
65
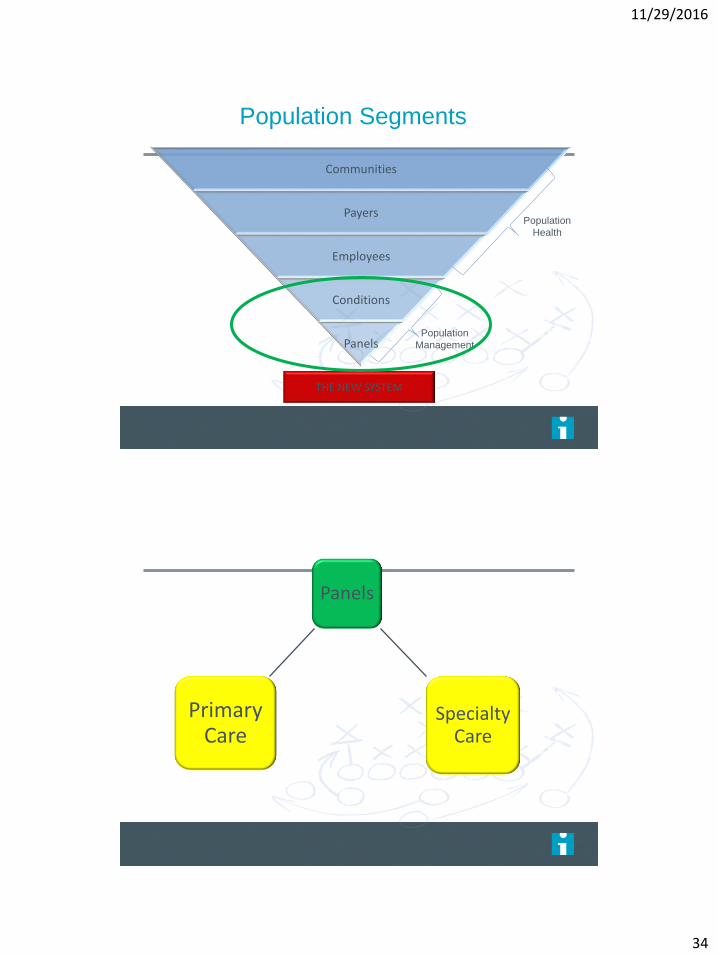
Population Segments
Communities
Payers
Employees
Conditions
Panels
THE NEW SYSTEM
Population
Management
Population
Health
11/29/2016
34
Population Segments
Communities
Payers
Employees
Conditions
Panels
THE NEW SYSTEM
Population
Management
Population
Health
Panels
Primary Care
Specialty Care
11/29/2016
35
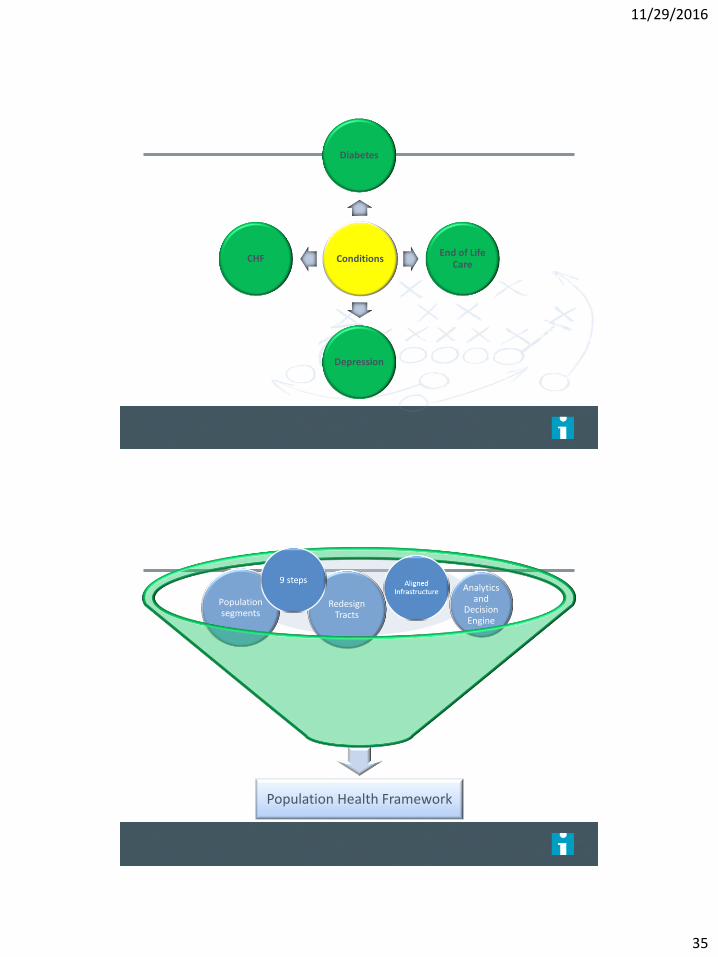
Conditions
Diabetes
End of Life Care
Depression
CHF
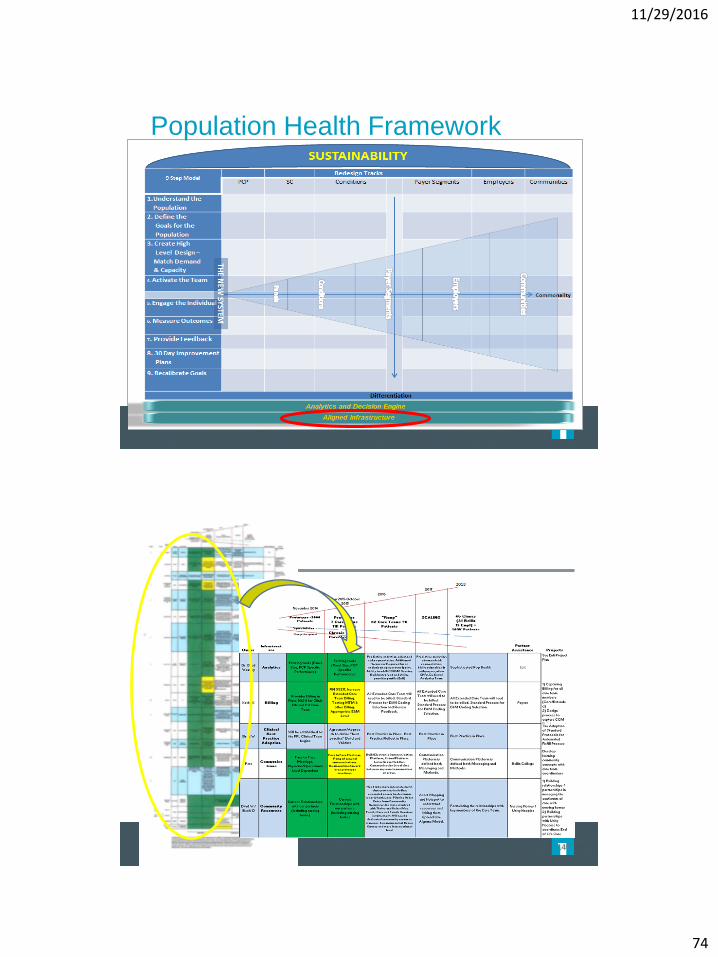
Population Health Framework
Redesign Tracts
Population segments
Analytics and
Decision Engine
11/29/2016
36
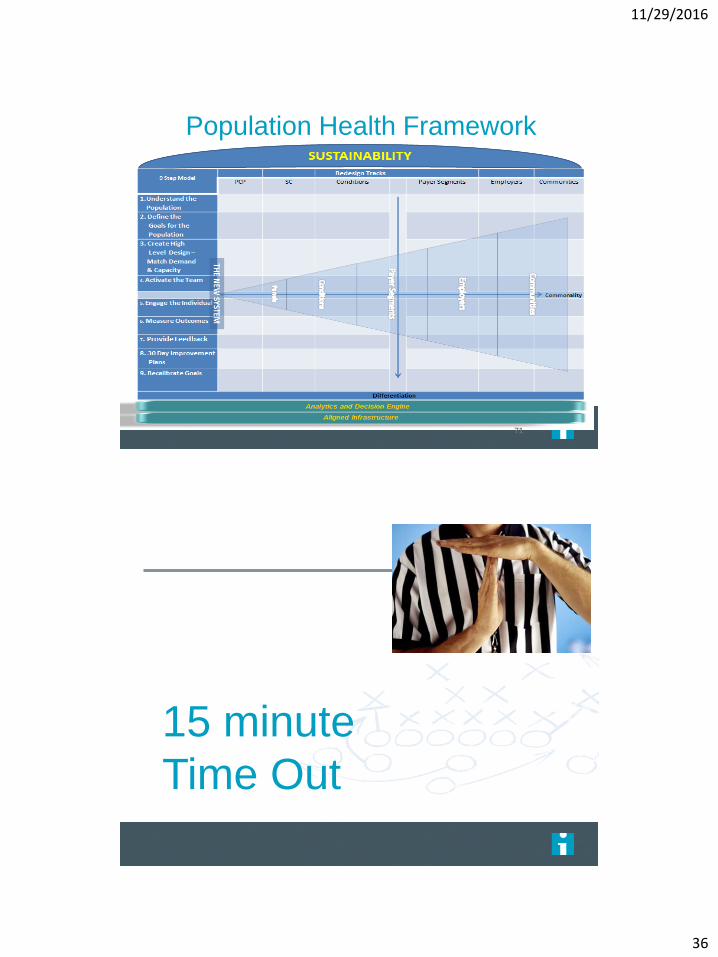
Population Health Framework
71
15 minute
Time Out
11/29/2016
37
Implementing
Team Based Care
Using the 9 Step Framework
James Jerzak, MD
Cynthia Lasecki, MD
11/29/2016
38
9 Steps Recap
1. Knowledge of Population
2. Define Goals
3. Create High Level Design – Demand and Capacity
4. Activate the Team
5. Engage the Individual
6. Measure Outcomes
7. Provide Feedback
8. 30 Day Action Plans
9. Recalibrate and Celebrate
Meet Julie
11/29/2016
39
DIAGNOSES: October 30, 2014
• COPD, severe dyspnea
• Tobacco Use Disorder – 2 PPD
• Type 2 Diabetes
• Depression
• Congestive Heart Failure
• Morbid Obesity
• Hypertension
• Hyperlipidemia
• Sleep Apnea
October 30,2014 visit
We had a long talk with her and were quite frank in
talking about this. this literally cannot go on. She's had
multiple admissions a regular basis. She is feeling
absolutely terrible on a constant basis. She
continues to smoke despite breathing difficulties. She
needs help.
To that end we talked about the new team care
approach of healthcare that we are starting next week.
And I talked to her about this, that it is literally her last
chance to get these things under control.
11/29/2016
40
Step 1 - Knowledge of the Population
Total Population – 141,561<20 – 35,250
20-39 – 28,101
40-49 – 17,469
50-64 – 33,081
65+ - 27,660
Financial Class57% Commercial
6% Self-pay
21% Medicare
15% Medicaid
ACO’s – Medicare or commercial – 44,160 or 31%Medicare - Next Generation, UHC MA, Humana MA
Commercial - Anthem, UHC
Step 1 - Knowledge of the Population
Health and Well-Being
33.4% Obese
17% Diabetes
5% > 9 A1c
6.5% Blood Pressure out of control
1527 patients >15 medications
813 patients >10 problems on problem list
11/29/2016
41
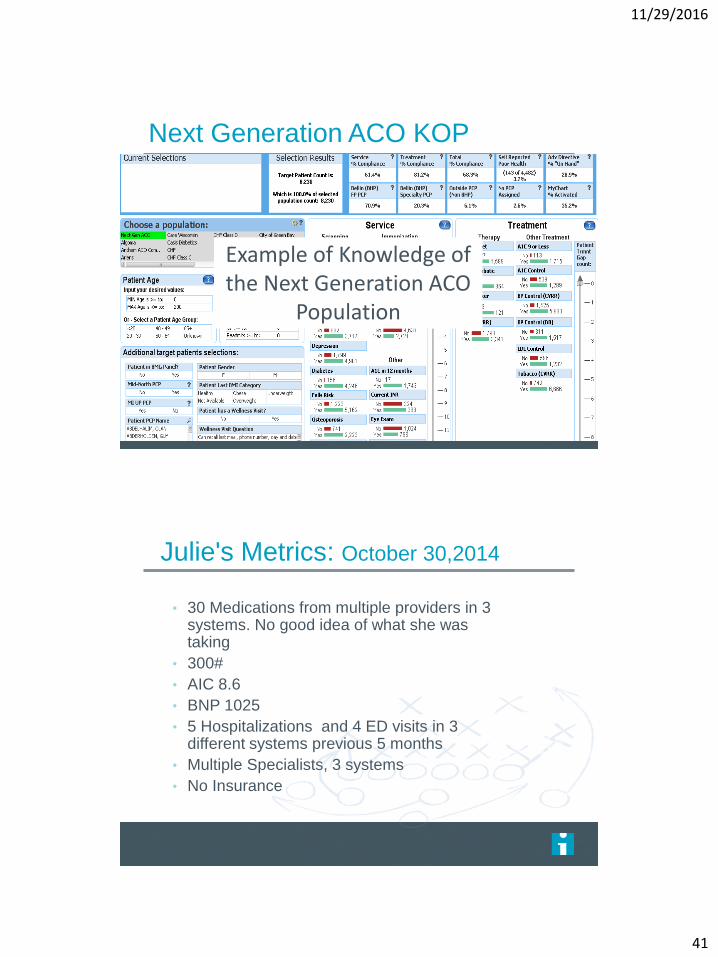
Next Generation ACO KOP
Screen shot
Example of Knowledge of the Next Generation ACO
Population
Julie's Metrics: October 30,2014
• 30 Medications from multiple providers in 3 systems. No good idea of what she was taking
• 300#
• AIC 8.6
• BNP 1025
• 5 Hospitalizations and 4 ED visits in 3 different systems previous 5 months
• Multiple Specialists, 3 systems
• No Insurance
11/29/2016
42
Step 2: Goals
Enhance Experience
Patient Satisfaction Survey (Win for
Patient)
Staff Satisfaction Survey (Win for
care team)
Likelihood to Recommend (Win for
the System)
Access to patient visits (Win for
Patient)
Step 2: Goals
Manage Total Cost of Care
PMPM targets for ACO (Win for the Patient,
Win for the system)
Maximize Quality Care
Cancer Screenings (Win for the Patient)
Diabetic Screenings (Win for the Patient)
11/29/2016
43
Step 2: Goals
Ensure Sustainability
HCC score (Win for System)
Increase in visits/day (Win for the System)
Increase in E/M coding (Win for the System)
Increase in Patient Panel Size (Win for the System)
Retention of Staff (Win for the System)
Our Goals for Julie October 30 2014
Get her insurance coverage
Figure out her meds
Get AIC in control
Stop smoking
11/29/2016
44
Step 3: Care Team Design
Core team: Physician, RN, MA/LPN(care team
coordinator), Patient account rep(scheduler) Behavioral
health consultant (pilot)
Extended care team: Case Manager, RN Care
Coordinator, Diabetic Educator, Clinical Pharmacist
Team Based Care Processes
Office Visit – Before Provider
Care Team Coordinator (MA/LPN)
• Follows standard rooming procedures
• Populates visit diagnoses from problem list
• Sets up 1 year refills
• Identifies visit agenda
• Identifies and addresses care gaps
• Pulls up appropriate template
• Starts documentation
11/29/2016
45
Team Based Care Processes
Office Visit – with Provider
Care Team Coordinator
• Presents patient to provider
• Continues team documentation
• Enters orders for consults, new meds, and tests
• Acts as patient advocated
Provider
• Focuses on the patient, the examination, and decision
making
11/29/2016
46
Team Based Care ProcessOffice Visit – After Provider
Care Team Coordinator:
• Reviews ordered tests or consults
• Pends future orders
• Schedules future appointments
• Reviews AVS with patient (and basic health coaching)
• Engages other team members as appropriate
Provider
• Responsible for editing and finalizing team documentation and
signing pended orders
11/29/2016
47
Team Based Care Processes
In-Basket Management
• RN/CTCs assist with in basket management
• Increased verbal communication with co-location
decreases electronic messaging
• Intercept unnecessary messages to Provider
• Test results managed by team per protocols
• Panel management by core team in conjunction with
Central Care Management team
• Expanded role of office RN in direct patient care
RN Role Reimagined: Co-Located,
Resource for CTCs, and Patient visits
11/29/2016
48
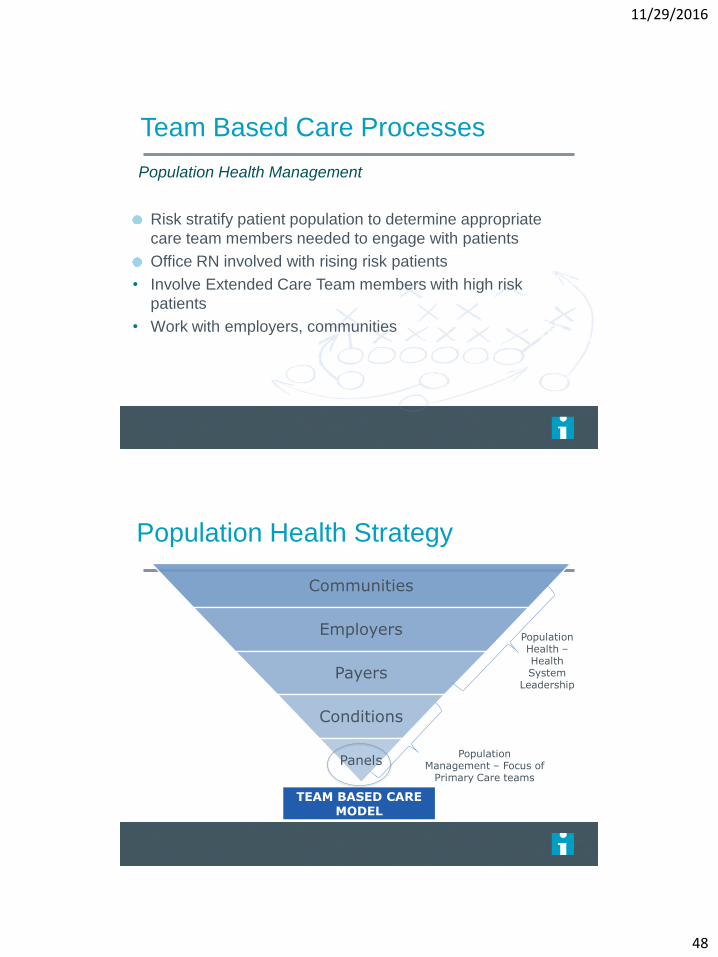
Team Based Care Processes
Population Health Management
Risk stratify patient population to determine appropriate
care team members needed to engage with patients
Office RN involved with rising risk patients
• Involve Extended Care Team members with high risk
patients
• Work with employers, communities
Population Health Strategy
Communities
Employers
Payers
Conditions
Panels
TEAM BASED CARE MODEL
PopulationManagement – Focus of
Primary Care teams
Population Health –Health System
Leadership
11/29/2016
49
Step Three: Design Workflows
Step 3: Design – Co Location Area
11/29/2016
50
11/29/2016
51
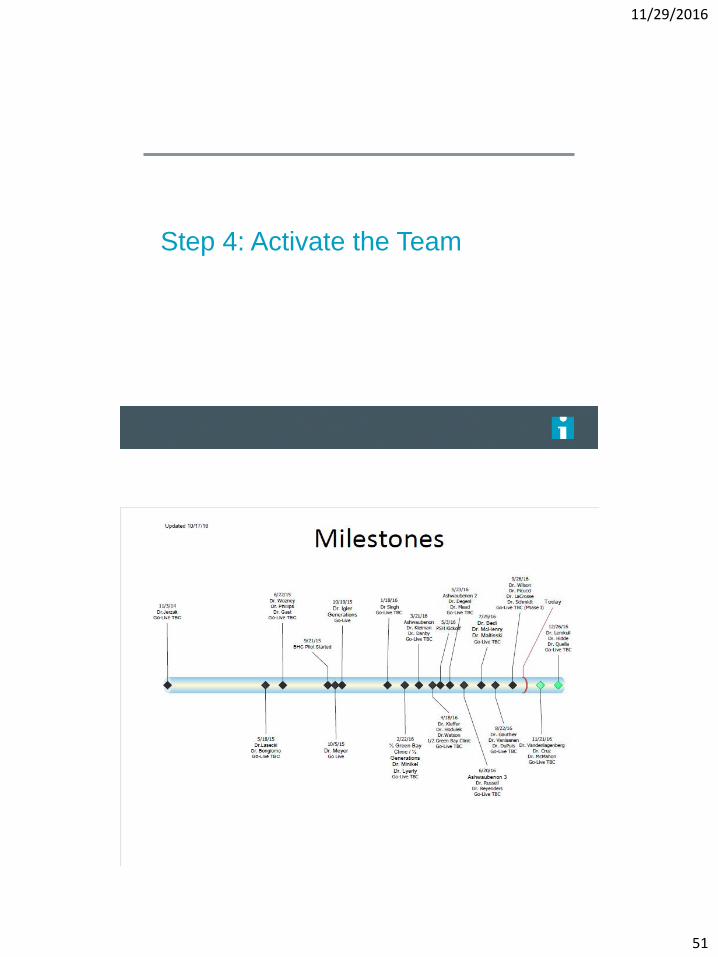
Step 4: Activate the Team
Milestones for Team Based Care
11/29/2016
52
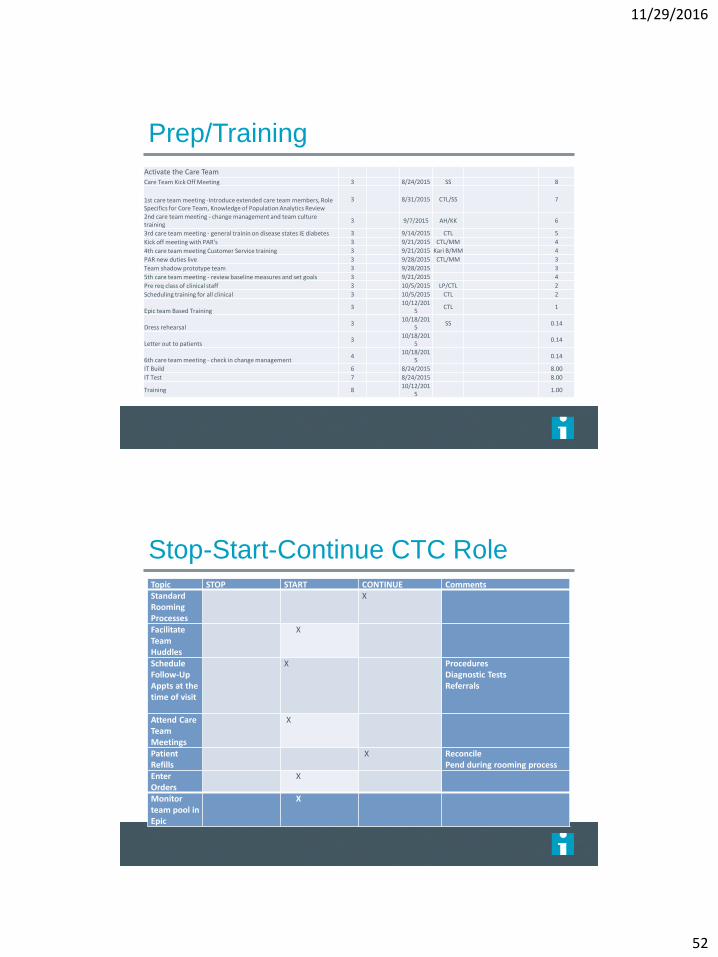
Prep/Training
Activate the Care TeamCare Team Kick Off Meeting 3 8/24/2015 SS 8
1st care team meeting -Introduce extended care team members, Role Specifics for Core Team, Knowledge of Population Analytics Review
3 8/31/2015 CTL/SS 7
2nd care team meeting - change management and team culture training
3 9/7/2015 AH/KK 6
3rd care team meeting - general trainin on disease states IE diabetes 3 9/14/2015 CTL 5
Kick off meeting with PAR's 3 9/21/2015 CTL/MM 4
4th care team meeting Customer Service training 3 9/21/2015 Kari B/MM 4
PAR new duties live 3 9/28/2015 CTL/MM 3
Team shadow prototype team 3 9/28/2015 3
5th care team meeting - review baseline measures and set goals 3 9/21/2015 4
Pre req class of clinical staff 3 10/5/2015 LP/CTL 2
Scheduling training for all clinical 3 10/5/2015 CTL 2
Epic team Based Training3
10/12/2015
CTL 1
Dress rehearsal 3
10/18/2015
SS 0.14
Letter out to patients3
10/18/2015
0.14
6th care team meeting - check in change management 4
10/18/2015
0.14
IT Build 6 8/24/2015 8.00
IT Test 7 8/24/2015 8.00
Training 810/12/201
51.00
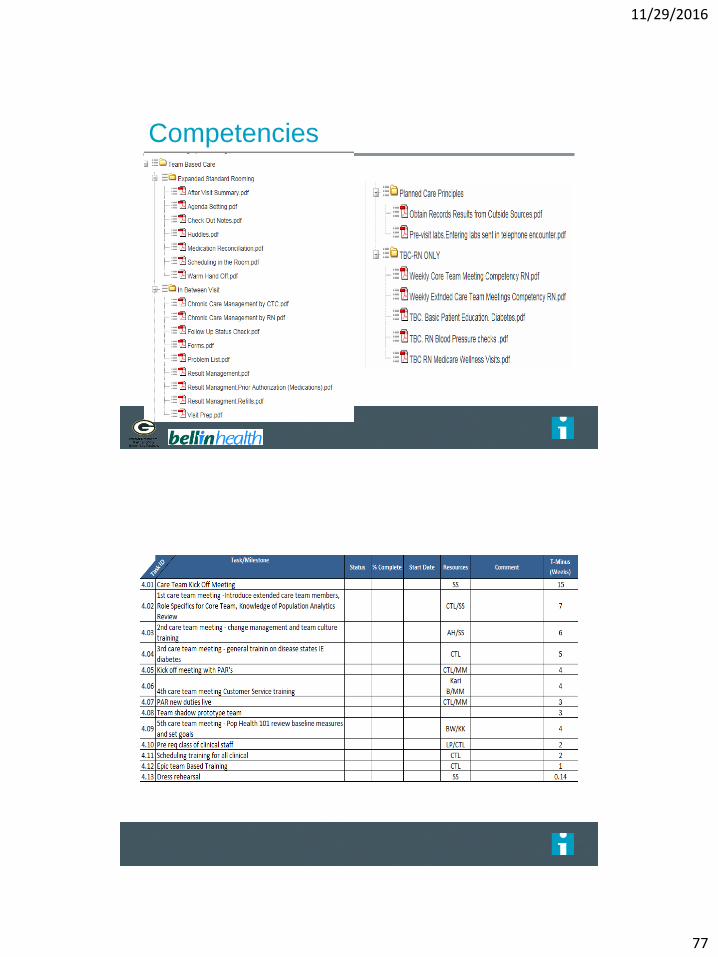
Stop-Start-Continue CTC RoleTopic STOP START CONTINUE CommentsStandard Rooming Processes
X
Facilitate Team Huddles
X
Schedule Follow-Up Appts at the time of visit
X ProceduresDiagnostic TestsReferrals
Attend Care Team Meetings
X
Patient Refills
X ReconcilePend during rooming process
Enter Orders
X
Monitor team pool in Epic
X
11/29/2016
53
Competencies
Step 5: Engaging the Individual
Relationship with core team
Relationship with extended care team
Processes like the Chronic Care Management program
Outreach from Central Care Management team
11/29/2016
54
Step 5: Engaging the Individual
Example: PDSA for Diabetic Engagement
137 diabetics A1C 7.1-8.9
Warm hand off to Clinic RN for diabetic education and
support
Approach is to get to know the individual and what is
important to them. Set goal based on this information.
Result - 80% of the patients who met with the RN
lowered their A1C by 1% or went below 7% after 6
months.
Engaging with Julie
Patient centered goals
Getting to know what's important for her
Staying connected
11/29/2016
55
Core TeamEngagement and bonding with MA/LPN
Behavioral Health: Ongoing counseling regarding
depression and life stressors; support for smoking cessation
11/29/2016
56
Case Manager: Obtain and backdate insurance;
provide ongoing support
Diabetic Educator: Reviewed and adjusted
diabetic meds, reinforced lifestyle changes
11/29/2016
57
Clinical Pharmacist: Reviewed meds, cut number
by over half, enhanced Julie’s understanding of her meds
RN Care Coordinator: Home visits, and
beginning of intensive involvement to coordinate care
and guide Julie to better health on an ongoing basis
11/29/2016
58
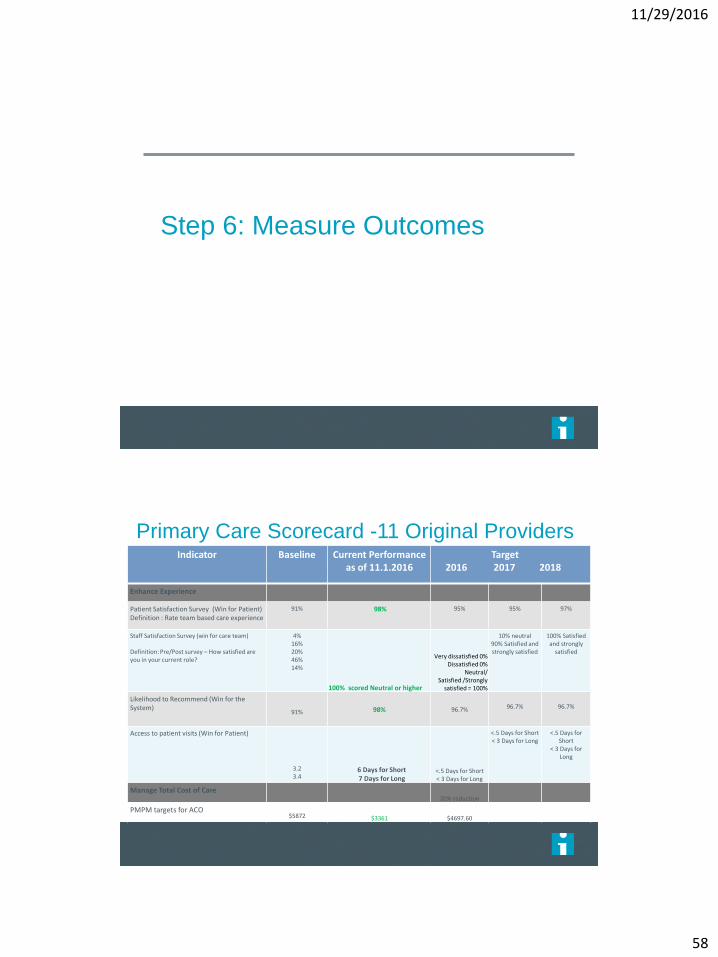
Step 6: Measure Outcomes
Indicator Baseline Current Performance as of 11.1.2016
Target2016 2017 2018
Enhance Experience
Patient Satisfaction Survey (Win for Patient) Definition : Rate team based care experience
91% 98% 95% 95% 97%
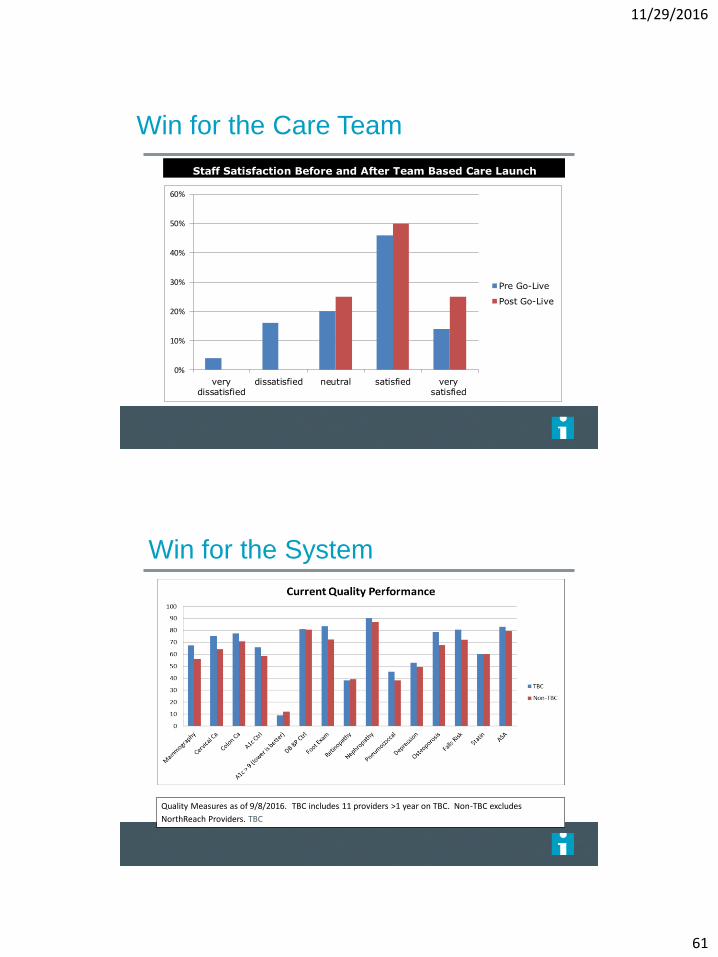
Staff Satisfaction Survey (win for care team)
Definition: Pre/Post survey – How satisfied are you in your current role?
4%16%20%46%14%
100% scored Neutral or higher
Very dissatisfied 0%Dissatisfied 0%
Neutral/Satisfied /Strongly
satisfied = 100%
10% neutral90% Satisfied and strongly satisfied
100% Satisfied and strongly
satisfied
Likelihood to Recommend (Win for the System)
91% 98% 96.7% 96.7% 96.7%
Access to patient visits (Win for Patient)
3.23.4
6 Days for Short7 Days for Long
<.5 Days for Short< 3 Days for Long
<.5 Days for Short< 3 Days for Long
<.5 Days for Short
< 3 Days for Long
Manage Total Cost of Care20% reduction
PMPM targets for ACO$5872 $3361 $4697.60
Primary Care Scorecard -11 Original Providers
11/29/2016
59
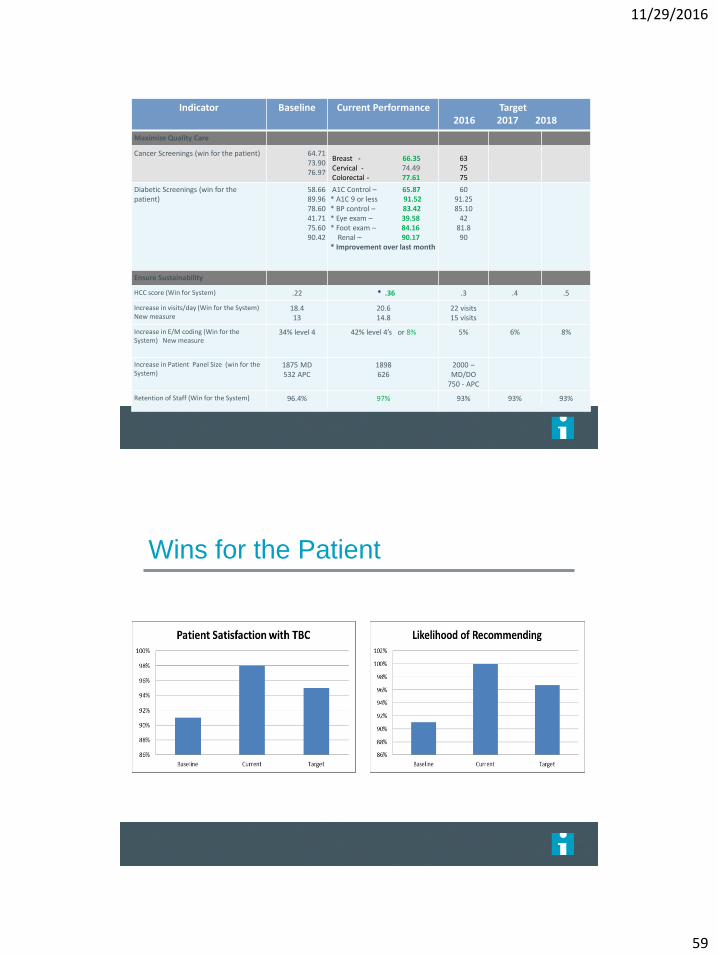
Indicator Baseline Current Performance Target2016 2017 2018
Maximize Quality Care
Cancer Screenings (win for the patient) 64.7173.9076.97
Breast - 66.35Cervical - 74.49Colorectal - 77.61
637575
Diabetic Screenings (win for the patient)
58.6689.9678.6041.7175.6090.42
A1C Control – 65.87* A1C 9 or less 91.52* BP control – 83.42* Eye exam – 39.58* Foot exam – 84.16
Renal – 90.17* Improvement over last month
6091.2585.10
4281.890
Ensure Sustainability
HCC score (Win for System) .22 * .36 .3 .4 .5
Increase in visits/day (Win for the System) New measure
18.413
20.614.8
22 visits15 visits
Increase in E/M coding (Win for the System) New measure
34% level 4 42% level 4’s or 8% 5% 6% 8%
Increase in Patient Panel Size (win for the System)
1875 MD532 APC
1898626
2000 –MD/DO
750 - APC
Retention of Staff (Win for the System) 96.4% 97% 93% 93% 93%
Wins for the Patient
11/29/2016
60
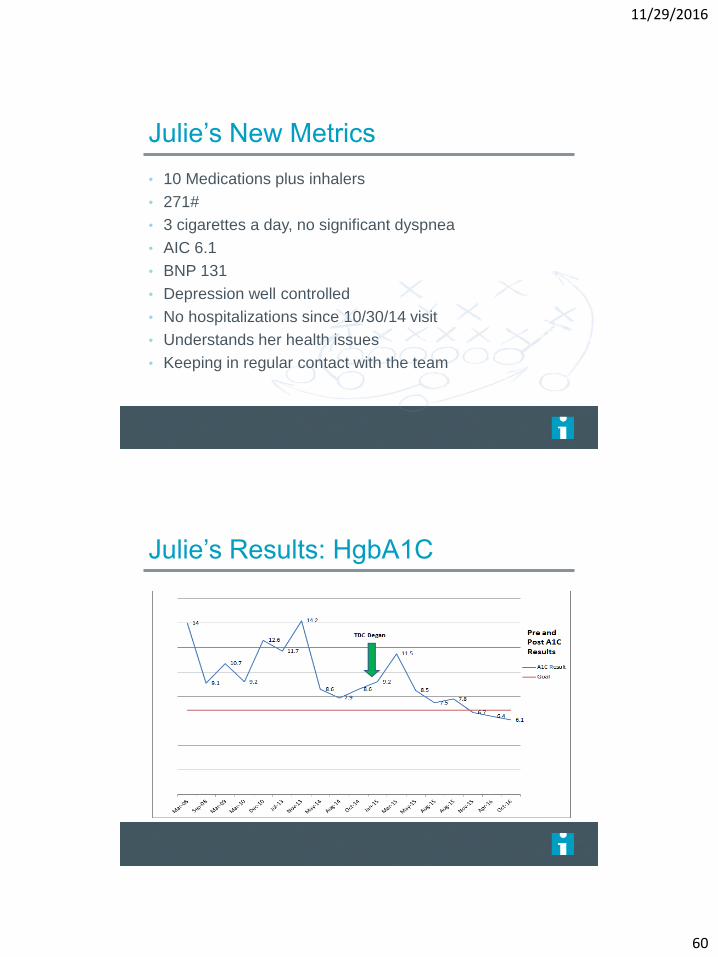
Julie’s New Metrics
• 10 Medications plus inhalers
• 271#
• 3 cigarettes a day, no significant dyspnea
• AIC 6.1
• BNP 131
• Depression well controlled
• No hospitalizations since 10/30/14 visit
• Understands her health issues
• Keeping in regular contact with the team
Julie’s Results: HgbA1C
11/29/2016
61
Win for the Care Team
Staff Satisfaction Before and After Team Based Care Launch
0%
10%
20%
30%
40%
50%
60%
verydissatisfied
dissatisfied neutral satisfied verysatisfied
Pre Go-Live
Post Go-Live
Quality Measures as of 9/8/2016. TBC includes 11 providers >1 year on TBC. Non-TBC excludes
NorthReach Providers. TBC
Win for the System
11/29/2016
62
Step 7: Provide Feedback
11/29/2016
63
Patient Comments
• “Love the team-based approach!”
• “Excellent people! The program has been so helpful. Thanks!”
• “It is much nicer that the nurse is in the room so the doctor doesn't
have to look at the computer. It helps me because I understand what is
happening better than before.”
• “Absolutely awesome. Treated like a person, not just a number. :)”
• “I like this new team approach.”
“My visit today seemed a lot more efficient and beneficial than
many others I have had in the past. The whole team/staff also
seems to be happier! Keep up the great work!”
Provider and Staff Comments
• “I never want to go back to the old way.”
• “I feel empowered”
• “I am finally part of a team with the focus on patient
care.”
• “Work-Life balance is great. I can spend time with my
family.”
• “I have enjoyed the time it has given me to build
quality relationships with our patients. I feel I can
support them better”
11/29/2016
64
Julie’s Comments
“Everyone needs someone that shows they care,
that they are here to help you, that doesn’t judge you, and
wants to get to know you. The team knows me better, and
my experience is much more positive.”
Step 8: 30 Day Actions
Model for ImprovementPDSA Planning Worksheet
Team Name:
Cycle Start Date: Cycle End Date:
PLAN:Describe the change you are testing and state the question you want this test to answer:
What do you predict the result will be?
What measure will you use to learn if this test is successful or has promise?
Plan for change or test: who, what, when, where:
Plan for what data/evaluation is needed: who, what, when, where:
DO: Report what happened after you carried out the test. Describe observations, findings, problems encountered, special circumstances:
STUDY: Compare results from this completed test to your predictions. What did you learn? Any surprises?
ACT: Modifications or refinements for the next cycle, what will you do next?
11/29/2016
65
Step 9: Recalibrate goals and
Celebrate
Original goals for sustainability included:RAF
Number of Value Based contracts
Retention rate of staff
New goals for sustainability includes:HCC
Increased 99214/99213 ratio
Increase number of visits
Appropriate staffing ratios, CTC:Provider
Ownership of measures by team, not just clinician – especially the CTCs
Team culture – once developed, invaluable
11/29/2016
66
11/29/2016
67
Lessons Learned
• There needs to be a strong partnership and shared
vision between administration and physicians
• Team based care is the key driver of effective
population health management
• Empowering staff to take on new roles leads to
better patient care and engagement, and higher
staff satisfaction
• The importance of training for expanded roles, as
well as for team culture, cannot be underestimated
Lessons Learned
• Scale and spread take time, effort, and resources. Be prepared!
• Be sure to set appropriate expectations for physicians and APC’s
• Having team support for EHR work, including documentation, is a key in eliminating clinician burnout
• BUT - Team Based Care is not just extra support for providers, it’s a system wide transformation that allows your system to provide the best care for your patients
11/29/2016
68
Question/Answers
11/29/2016
69
TEAM HUDDLE - 2
Getting to Work
Kathy Kerscher
1 Hour
LUNCH - Time
Out
12 to 1 pm
11/29/2016
70
Building the System:
Spread, Scale and
Sustainability
Kathy Kerscher

11/29/2016
71
Disclosure
No relevant conflicts of
interest to disclose
Innovation Cycle Spread
143
PrototypePhaseSpread
Phase 2Spread
Phase 3Spread
FullSpread
P
DS
ATest DesignHypothesis
P
DS
A P
DS
A P
DS
A
11/29/2016
72
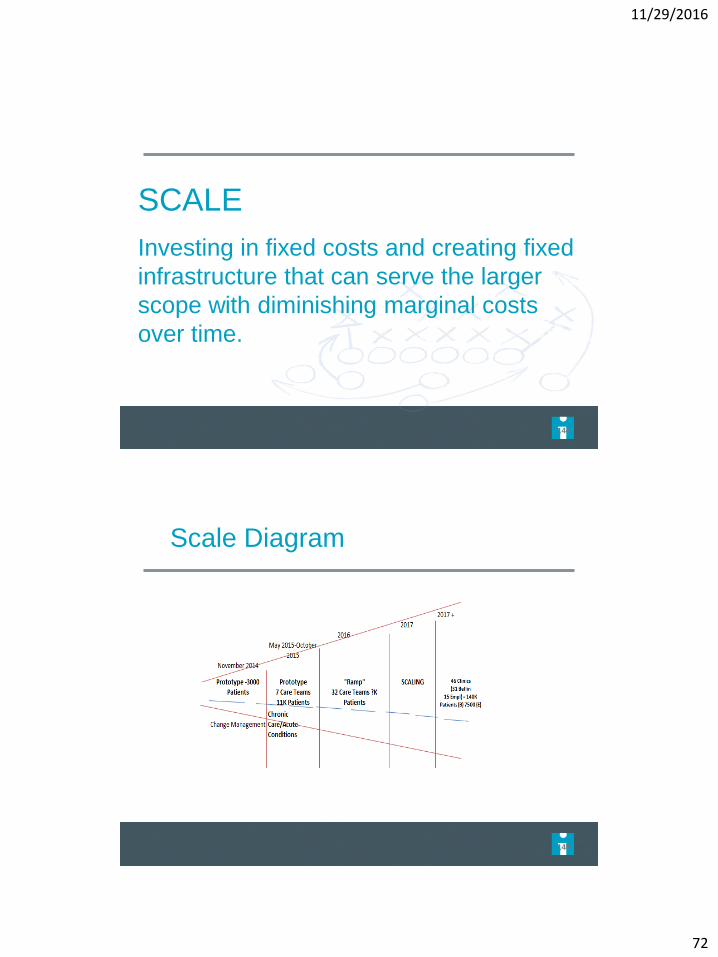
SCALE
Investing in fixed costs and creating fixed
infrastructure that can serve the larger
scope with diminishing marginal costs
over time.
144
145
Scale Diagram
11/29/2016
73
Infrastructure
Brad Wozney, MD
Kathy Kerscher
11/29/2016
74
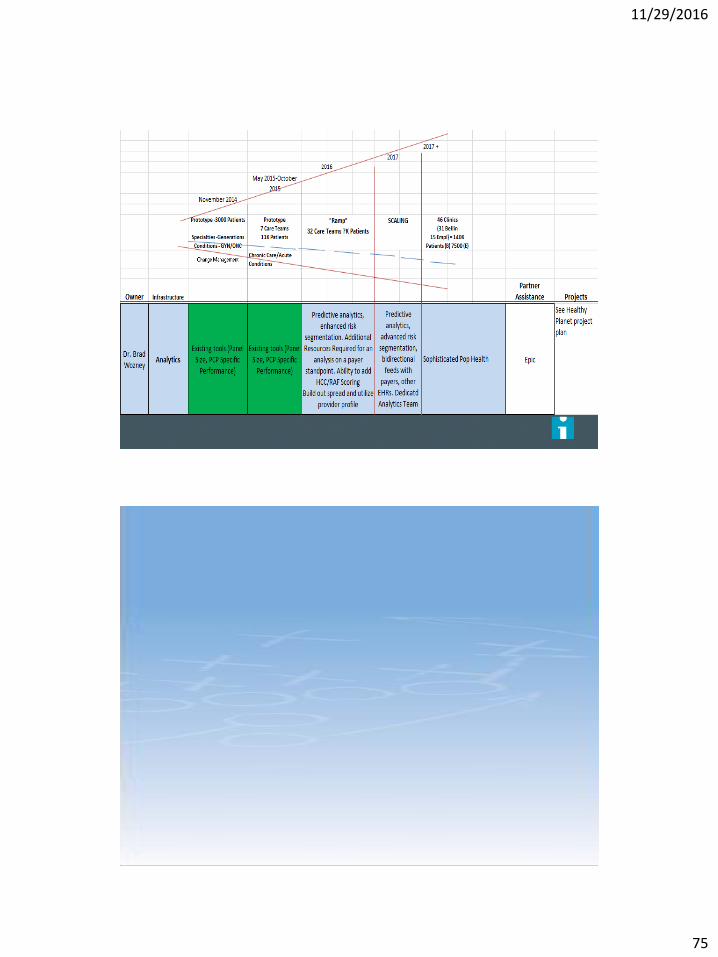
Population Health Framework
149
Epic
11/29/2016
75
11/29/2016
76
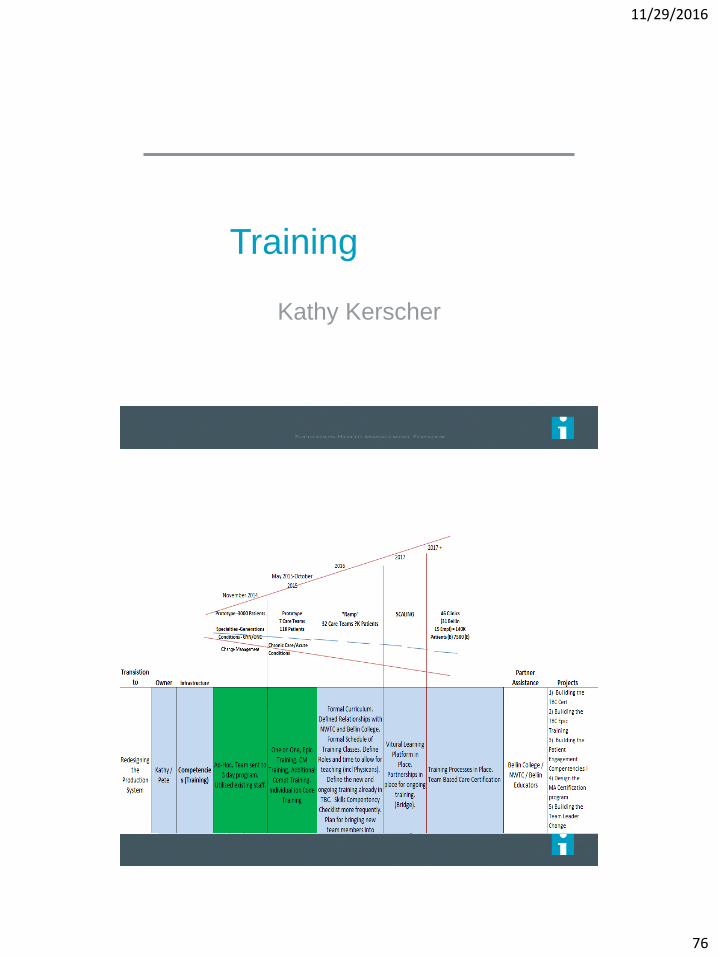
Training
Kathy Kerscher
11/29/2016
77
Competencies
11/29/2016
78
“Do not under estimate the time
and resources to properly train!”
Tom Bodenheimer, MD
11/29/2016
79
Sustainability
Kathy Kerscher
Why is Sustainability Important?
Managing the change
Workflows upheld
Skills and competencies proficient
3 wins upheld
Adjust if needed
11/29/2016
80
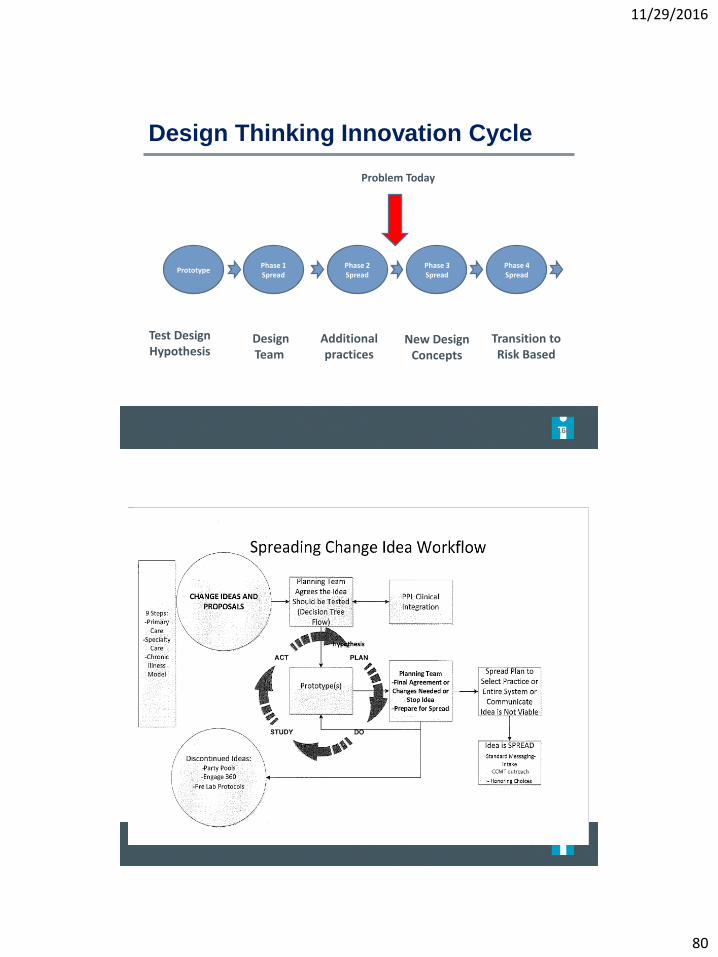
Design Thinking Innovation Cycle
160
PrototypePhase 1 Spread
Phase 2Spread
Phase 3Spread
Phase 4 Spread
Test DesignHypothesis
DesignTeam
Additional practices
New Design Concepts
Transition to Risk Based
Problem Today
11/29/2016
81
How To Achieve Sustainability?
Learning center modules by role
Review what was trained
What is actually happening
Spread of best practice
Check in’s with providers bi-annually
Dyad - Change and Physician Leaders
Ongoing Communication
120 day cycle report out to everyone in the organization
especially senior leadership
Provider lead meeting – quarterly
Website for all employees to get the latest updates
11/29/2016
82
Financial Modeling
Kathy Kerscher
Overview
Transition from Insuring Health to Managing Health Risk Based Revenues
Financial Sustainability Considerations
Primary Care
Our journey in Primary Care
Specialty
Condition Management
Financial Lessons Learned
Questions
11/29/2016
83
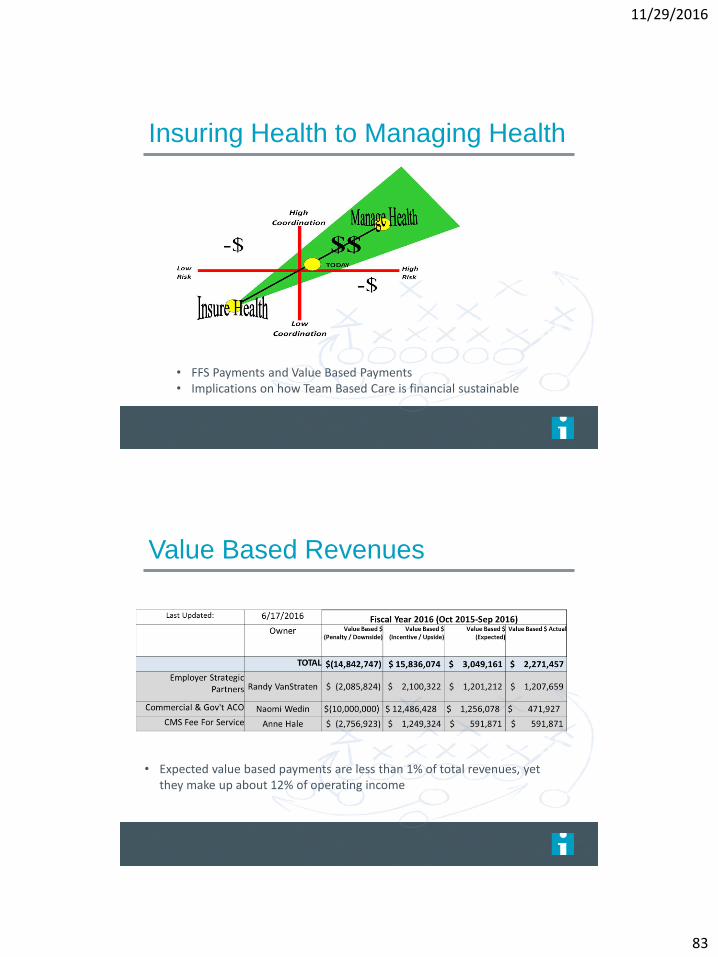
Insuring Health to Managing Health
• FFS Payments and Value Based Payments• Implications on how Team Based Care is financial sustainable
Value Based Revenues
• Expected value based payments are less than 1% of total revenues, yet they make up about 12% of operating income
11/29/2016
84
Primary Care
Significant investment in staffing resources
Managing health payment environment:
Allow providers to manage more patients while improving quality,
satisfaction, and total cost of care
Get paid for value
Insuring Health payment environment:
Increase FFS payments… (not our goal)
We are in the middle
Our Journey in Primary Care
Investment in TBC
Our Investment for “full resources”
Annual expenses
Core Team - $10.1 million ($6.8 million for CTC & RN)
Extended Care Team - $3.5 million
One-time expenses
Facility and IT - $2 million
Go-lives - $1.5 million
If only considering FFS payments, every primary care
provider would have to add about 5 visits per day to pay
for this investment
Unlikely to happen…
11/29/2016
85
Our Journey in Primary Care Bellin
Health’s Internal Financial Measures
Further complicated by internal financial measures
Internal financial sustainability measuresWorked hours per unit of service (visits)
Total expense per unit of service (visits)
Targets set based largely on prior year performance
TBC was not looking favorable through these measures
Needed to explain further…
Our Journey in Primary Care
Considering Value Based Revenues
Had to demonstrate value in managing health environment
Considering value based payments introduced difficulties• Conceptually made sense... Difficult to directly attribute
“Were successes due to TBC or something else?”
Measured improvements in patient value• Improved satisfaction, quality, and total cost of care
Early data is showing improvements in cost of care
Need to continue to analyze cost data
Attributed half of value based payments to pay for TBC Investment
11/29/2016
86
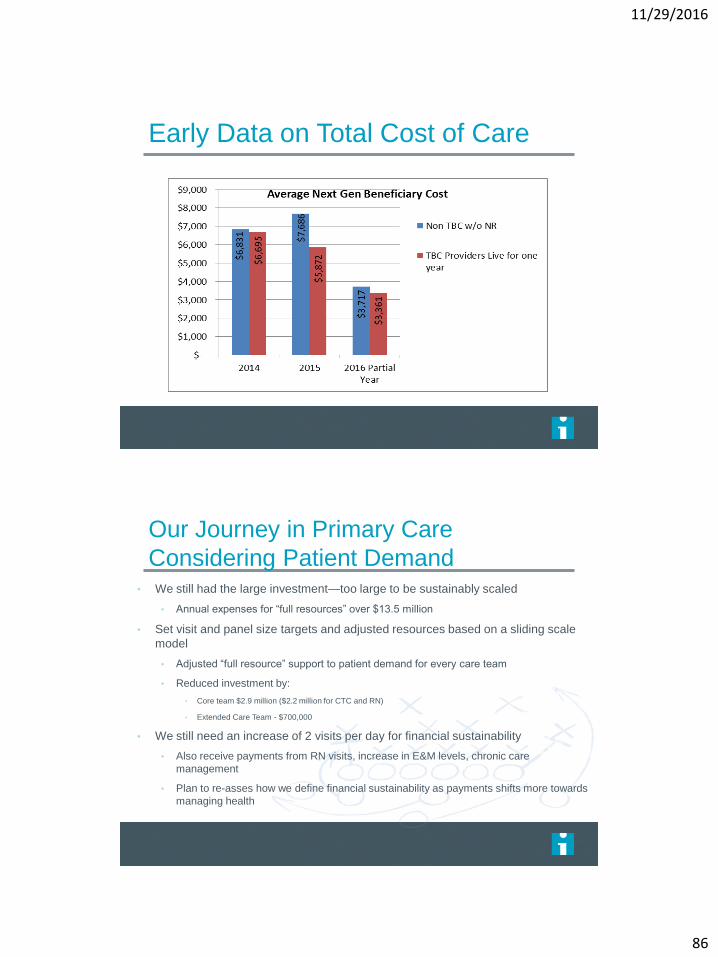
Early Data on Total Cost of Care
Our Journey in Primary Care
Considering Patient Demand• We still had the large investment—too large to be sustainably scaled
• Annual expenses for “full resources” over $13.5 million
• Set visit and panel size targets and adjusted resources based on a sliding scale
model
• Adjusted “full resource” support to patient demand for every care team
• Reduced investment by:
• Core team $2.9 million ($2.2 million for CTC and RN)
• Extended Care Team - $700,000
• We still need an increase of 2 visits per day for financial sustainability
• Also receive payments from RN visits, increase in E&M levels, chronic care
management
• Plan to re-asses how we define financial sustainability as payments shifts more towards
managing health
11/29/2016
87
Our Journey in Primary Care-Next Steps
• Enhance analytics on claims data to refine
measurement of cost of care
• Factor in patient risk
• Redesign provider compensation
• Currently, large focus on wRVU production
• Align compensation with patient value
• Get paid for value—enter more risk based arraignments
• Consider different internal financial metrics
• Aligned lives
Specialty Practice
• Each provider functioning at the top of their license
• Current design has providers at far below full capacity
• For physicians
• Increasing capacity for consults and surgeries
• Advanced Practice Clinicians
• Follow-up, prevention, coordination with primary care for care
management
• Modeling for OB practice shows we need to create
physician capacity for 3 additional procedures per week
to pay for additional resources
11/29/2016
88
Condition Management
• Prototype model with CHF population
• Investment of $475,000 to better manage population
and reduce re-admissions
• Targeted to reduce cost of care to population
• Next Gen shared savings target from CHF population
$472,000
• Need to be paid for improving total cost of care
15 minute
Time Out
11/29/2016
89
Barriers to Team Based
Care Panel Discussion
James Jerzak, MD
Cindy Lasecki, MD
Brad Wozney, MD
Facilitator – Kathy Kerscher
11/29/2016
90
Disclosure
No relevant conflicts of
interest to disclose
The Patient
“I don’t want to see all these new people. I
want to see my doctor.”
11/29/2016
91
Medical Assistant/LPN
“Can I do what is now expected of me,
especially helping with documentation?”
Registered Nurse
“I am comfortable in my triage role, I am
hesitant to be involved directly in patient
care.”
11/29/2016
92
Physicians
“These are my patients, I don’t want to
pass off responsibility for care to other
people.”
Risk Managers
“Doctors are the only ones permitted to do
this work per guidelines.”
11/29/2016
93
Finance
“We can’t justify the added cost of hiring
additional personnel.”
Executive Leadership
“This is not a strategic priority at this
time.”

11/29/2016
94
Final Thoughts
James Jerzak, MD
Kathy Kerscher
Cynthia Lasecki, MD
Brad Wozney, MD
11/29/2016
95
Lessons Learned
Joint collaboration and vision between clinicians and
administration is essential
Keep adjusting your model as more data is obtained
Set clear expectations to clinicians
Sustainability needs ongoing attention
Don’t assume workflows and core concepts are being
followed
• Stay true to the 9 step framework
Guiding Principles
• Put the Patient first
• Build Team Culture
• Empower Staff
• Encourage Critical thinking
• Know your Population
11/29/2016
96
Core Concepts
• Planned Care Principles
• Enhanced rooming process
• Co - Location
• Daily Huddles
• Regular Care Team Meetings
• Maximize Use of Warm Handoffs
• Effective Use of Extended Care Team Members
• Standard Documentation and Communication
• Team Approach to In-Between Visit Work
• Start On Time
Open Discussion
11/29/2016
97
TEAM HUDDLE - 3
Starting the Plan for Home
Kathy Kerscher
Thank you





























