Embed Size (px)
Citation preview

Review
Nocardiosis: a review
Marcel0 E. Corti@) and Maria F. Villafafie Fioti@)
Background: Nocardiosis is a localized or disseminated infection caused by an aerobic actinomycete that usually affects immunocompromised patients. Nocardiosis has been described in patients receiving immunosuppressive therapy, organ transplant recipients, subjects with chronic pulmonary diseases, and patients infected with the human immunodeficiency virus (HIV).
Data review: Nocardial infection shows a broad and variable geographic distribution. The clinical forms include pulmonary involvement, skin or soft tissue infection, and disseminated forms with brain and pulmonary lesions. Primary nocardial infection includes pulmonary or cutaneous and/or subcutaneous lesions. Disseminated disease is defined by the identification of nocardial infection in two or more organs. The lung is the most commonly involved organ, followed by the skin and the brain. HIV-related nocardiosis usually appears in patients with advanced immunodepression and CD4 counts less than 50 cells/ml. Sulfonamides are the standard therapy for nocardiosis and are effective in the majority of cases. Several other drugs, such as imipenem, amikacin, minocycline, amoxicillin clavulanic acid and third-generation cephalosporins, have also been used in these patients. Surgery is usually reserved for the drainage of abscesses.
Conclusions: Nocardiosis is an important cause of opportunistic infection in immunosuppressed patients. Early recognition and prompt treatment usually results in complete cure, except for patients with nocardial brain abscesses, in whom the mortality remains at approximately 50%.
Int J Infect Dis 2003; 7: 243-250
Infections caused by Nocardia species are infrequent but challenging to clinicians. They cause a wide variety of diseases in both normal and immunocompromised patients. In recent years, the number of case reports has been increasing, and this can be attributed to the improvements in diagnostic capabilities and the higher clinical index of suspicion accompanying the increased prevalence of immunosuppressed patients. The treat- ment of nocardiosis also requires expertise. This report reviews the epidemiology, physiopathology, clinical manifestations, diagnosis and treatment of this aerobic bacterial disease.
INTRODUCTION
Nocavdia is a genus of aerobic Actinomycetes respon- sible for localized or disseminated infections in animals and humans. The genus is named after Edward Nocard,
(Wnit 10, Infectious Diseases, E J. Mufiiz Hospital, Buenos Aires, Argentina.
Address correspondence to: Marcel0 Corti, Pub 381 2”, cCQG 1406, Buenos Aires, Argentina.
E-mail: [email protected]
Corresponding Editor: Michael Ellis, Al Ain, UAE
who in 1888 described the isolation of an aerobic Actinomycete from cattle with bovine farcy. Eppinger reported the first human case of nocardiosis in 1890.The incidence of human disease has increased substantially in the last two decades in association with an increasing population of immunocompromised hosts and improved methods for detection and identification of Nocardia spp. in the clinical laboratory. Hematogenous dissemi- nation from the lung can contribute to the development of subcutaneous or cerebral abscesses. In humans, infect- ion can also take place by penetration through the skin.
The agents of these infections are aerobic fila- mentous Gram-positive, weakly acid-fast bacteria that live as soil saprophytes. The species that can infect humans are Nocardia asteroides and N. brasiliensis. The first of these, in most cases, shows pulmonary and systemic involvement; the second one is associated with cutaneous lesions and 1ymphadenitis.l
The incidence in patients with acquired immuno- deficiency syndrome (AIDS) is between 0.1% and 0.3 %. These infections affect patients in advanced stages of HIV disease and with CD4’ T-cell counts below 50 cell/yL.2
EPIDEMIOLOGY
Nocardiosis has a universal distribution, and affects people between 20 and 60 years of age. Cross and

244 International Journal of Infectious Diseases I Volume 7, Number 4,2003
Bindford noticed the high frequency with which nocardiosis complicates other pathologic conditions that act as predisposing causes, such as lymphoprolifer- ative syndromes, solid neoplasias, AIDS, liver cirrhosis, organ transplant and immunodepression treatments such as cytotoxics and corticosteroids.3
There is a tendency to think that Nocardia infection affects only immunocompromised patients, but this is only partially true. In 1980, Curry4 reviewed 455 cases of nocardiosis; 39% of them did not receive immuno- suppressive therapy. Dominguez and Anthony5 found that 58% of cases of Nocardia infection occurred in immunocompetent hosts. Finally, Menendez et al6 reported 10 cases with pulmonary nocardiosis; four of them were receiving corticosteroids, and two had concomitant HIV-l infection. Intravenous drug abuse also seems to be a risk factor. Palacios et al7 found an incidence of 82% in intravenous drug abusers. The use of systemic corticosteroids remains an important independent risk factor for nocardial infections.
Recently, episodes of nocardiosis in AIDS patients and in recipients of solid organ and bone marrow transplants have been reported.8-12 Risk factors for the development of nocardiosis in these patients include early rejection of graft and intensive immunosuppressive therapy.13 Finally, there is a third group of illnesses that increase the risk for the development of nocardiosis; these are the chronic granulomatous diseases and hema- tologic malignancies. In these cases, the species that is found most frequently is N. @~inica.r~J~
The incidence of nocardiosis in AIDS patients shows geographic variations; it occurs mainly in rural regions rather than in urban areas. In general, AIDS patients with CD4’ T-cell counts less than 100 cell/yL are more likely to develop pulmonary and extra- pulmonary disease. The frequency of Nocavdia infections in HIV-l patients increased from 0.3% in 1985 to 1.8% in 1989. This incidence is still low, and one of the reasons for this, although not the only one, may be the extensive use of cotrimoxazole for Pneumocystis carinii pneu- monia prophylaxis. The clinical presentation requires a differential diagnosis with other pulmonary diseases such as tuberculosis.r6
ETIOLOGY
The Nocardia genus includes a variety of species that are important pathogens in humans. N. asteroides complex includes a heterogeneous group of microorganisms with similar biochemistry, structure and antimicrobial resistance. This complex includes the subgroup N. asteroides sensu stricto, N. farcinica and N. nova. With regard to resistance, N. farcinica is resistant to tobramycin and third-generation cephalosporins. N. brasiliensis is resistant to minocycline and produces lymphocutaneous disease (sporotrichoid form), whereas N. transvalensis and N. otitidiscaviarum cause mostly noncutaneous disease.
PATHOGENESIS
Although the exact mechanism is unknown, the main route of acquisition of pulmonary nocardiosis is pro- bably through direct inhalation of contaminated particles. Most of the cases start as minor respiratory syndromes that self-limit spontaneously. In some patients, the in- fection spreads, starting from the lung, with a particular predilection for the brain, skin and subcutaneous tissues. Infection with Nocardia may also occur by direct inoculation through the skin, producing cellulitis, lymphangitis or both.
Intravenous drug abuse may provide another route of entry, i.e. direct inoculation through the skin, leading to abscesses, especially in recent venopuncture sites.r7Jg Surgical wound infections due to N. furcinica have also been described.r9 Rarely, gastrointestinal colonization has been reported, resulting from inhalation of spores or sputum swallowing. There is no definitive evidence of person-to-person transmission of Nocardia infections.
Host resistance to nocardial infection depends on sufficient numbers, and the phagocytic and lytic capabilities, of polymorphonuclear cells, and cell- mediated immunity. The last of these fails in AIDS patients and predisposes to the development of severe forms of the disease. However, the low frequency of this complication in patients with advanced HIV-l disease can be attributed to sulfonamide therapy and the leading role of neutrophils in the immune response to Nocardia.
CLINICAL MANIFESTATIONS
Pulmonary nocardiosis
This is an acute, subacute or chronic suppurative infection with a pronounced tendency for remissions and exacerbations. The clinical manifestations are acute or subacute pneumonia with abscess or cavity formation (Figure 1). Generally, the initial diagnoses are pneu- monia, tuberculosis, and carcinoma or lung abscesses
Figure 1. Chest radiograph showing acute pneumonia with abscess and cavity, due to N. asteroides.

Nocardiosis: a review I Corti and Fioti 245
of other etiologies. The most common symptoms are productive cough, high fever, chills, sweats and weight 10~s.~~ Twenty-five percent of cases present with pleural involvement, including pleural effusions and empyema. Nothing in the radiographic presentation is sufficiently distinctive to allow a diagnosis. The chest X-ray may show fluffy infiltrates, upper-lobe processes with cavitation (mimicking pulmonary tuberculosis), lobar consolidation, irregular nodules or masses, often cavitated, or single and multiple abscesses, and even simple alveolar or interstitial reticular or reticulonodular infiltrates.20 Also, miliary lesions and hiliar adenopathy have been described, as has presentation as an adult respiratory distress syndrome. 21 Rarely, Nocardia species can invade preexisting lung cavities, producing a ‘fungus ball’ appearance. Computed tomography (CT) reveals the presence of nodules or masses in more than 80% of patients.
Pulmonary lesions show tissue necrosis with poly- morphonuclear leukocyte, macrophage and lymphocyte infiltrates, but usually not the hallmark epithelioid cells seen in tuberculosis. Sometimes, tissue sections may reveal a granulomatous response with central necrosis that may mimic tuberculosis or histoplasmosis. Pro- gressive fibrosis occurs in inadequately treated patients, with a chronic course similar to that of tuberculosis. Immunocompromised patients, including AIDS patients, with nocardial pulmonary involvement can be difficult to diagnose because of the possible coexistence of other opportunistic pathogens.
Cutaneous and subcutaneous nocardiosis
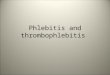
Primary cutaneous and subcutaneous nocardiosis represent 25% of cases, and can follow any puncture or other traumatic introduction of Nocardia with other microorganisms. Generally, this form is underdiagnosed, because culture incubation is not routinely done.22,23 In addition to the classic mycetoma, cutaneous infection also leads to cellulitis (Figures 2 and 3), pustules, pyoderma, paronychia, or localized abscesses that mimic infections due to pyogenic bacteria. It can also produce lymphangitis with subcutaneous nodules mimicking sporotrichosis, and for this reason is called the sporotrichoid form.24
While any pathogenic Nocardia species may cause primary cutaneous or subcutaneous lesions, N brasiliensis is the most frequently isolated in cases of disseminated disease. Palasi et a125 described a retromammary abscess caused by N asteroides in an HIV-positive patient. Rarely, Nocardia species can be inoculated into the bloodstream in intravenous drug abusers, producing septic thrombophlebitis.20
Mycetoma is a chronic cutaneous and subcutaneous disease that evolves progressively and causes a destructive infection of the skin, subcutaneous tissues, fascia, muscles and bones following local trauma to the hand, foot, leg or arm.24,26,27 It produces an area of localized
swelling containing suppurative granulomas and multiple sinus tracts with macroscopic white-yellow granules. Mycetoma is the only clinical form of nocardiosis associated with the presence of such granules.27 At least half of the cases of mycetoma are caused by Nocardia species, whereas members of the genus Actinomadura are frequently recorded only in certain geographic areas.
Systemic nocardiosis
Primary nocardial infection, either respiratory or cutaneous, may spread hematogenously and lead to an extrapulmonary form of this disease. The presence of lesions in two or more organs of the body defines systemic or disseminated disease. The most common sites for dissemination include the central nervous system (CNS), skin and subcutaneous tissues, kidneys, joints, bones, heart and eyes.20,22,28
In the early stages of systemic infection, Nocardia species behave as pyogenic bacteria, whereas the host cell response is dominated by neutrophils.24 Subse-
Figure 2. Subcutaneous nocardiosis due to N. brasiliensis in an intravenous drug abuser, HIV seropositive.
Figure 3. The same patient as in Figure 2 after antibiotic treatment.

246 International Journal of Infectious Diseases I Volume 7, Number 4,2003
quently, the illness evolves into a chronic phase, with macrophage and lymphocyte responses. Tissue abscesses result from the progressive tissue invasion with nocardial filaments. Generally, pulmonary and dissemi- nated forms progress unless treatment is started. That is to say, the infection is not self-limited, although it may evolve slowly over a period of many months or even years.29,30 Less frequent clinical presentations include peritonitis, epididymo-orchitis, iliopsoas and perirectal abscesses, pericarditis, endocarditis, septic arthritis, osteomyelitis and peritonitis in cases of chronic peritoneal dialysis. 24 Ramanathan and Rahirni31 reported a case of Nocardia pericarditis with pericardial effusion as an initial manifestation of HIV-l infection; N. asteroides was isolated from pericardial fluid. River0 et a132 described a case of cardiac tamponade caused by N. asteroides in an HIV-infected patient.
Eye involvement includes retinitis and endoph- thalmitis, but also surface lesions, as keratoconjunctivitis has been described as a consequence of traumatic inoculation.22
In AIDS patients, the incidence of nocardiosis has increased since 1990.24 Beaman and Beaman reviewed 71 cases of nocardiosis in AIDS patients from 1984 to 1992. The most common sites of disease were the lung (51.3%) and the brain (11.7%).
Central nervous system infection
CNS infection occurs in more than 40% of cases of systemic nocardiosis. 24,30 More than 25% of reported cases, other than mycetomas, affected the CNS, and, in half of them, this was the only parenchyma involved.‘3”5 The clinical manifestations are insidious, and, for this reason, diagnosis is difficult.13,24 The clinical symptoms result from the mass effect of brain abscesses and, less frequently, abscesses of the spinal cord and meninges.13 CNS infection is generally diagnosed after the develop- ment of focal neurologic deficits and diagnostic aspiration of CNS lesions. There are reports of patients undergoing surgical excision for a presumed brain tumor whose postoperative cultures grew Nocardia.
Sometimes, psychiatric disorders herald the infection.24x29,30 Patients with minimal neurologic symptoms can be treated with antibiotics only; however, in most cases, surgical excision is needed because of the natural tendency of nocardial abscesses to be multi- loculated. The abscesses can involve parietal, frontal or occipital cortex, basal ganglia and cerebellum. The majority of reported cases of Nocardia brain abscesses involve N. astevoides, although other species have been reported.
Mamelak et a13’j reported 11 cases of nocardial abscesses treated between 1971 and 1993, and reviewed 120 cases reported since 1950. The clinical findings included focal deficits in 42%, nonfocal findings in 27 %, and seizures in 30%. In this report, the abscesses were single in 54% and multiple in 38%; 34% of 131 patients
were immunocompromised, and 15% of them had HIV- 1 infection. In 66% of the cases, the authors verified extraneural localization, pulmonary in 38% and cutaneous and subcutaneous in 20%. The mortality rate was 33% in patients with single abscesses and 66% in those with multiple abscesses. In 22% of the cases, diagnosis was made by autopsy. Although the mortality rate for nocardial abscesses has dropped by almost 50% since the advent of CT, this percentage has not changed in immunocompromised patients, and is three times higher than for other bacterial brain abscesses (30% versus 10%). For this reason, stereotactic biopsy is needed for the isolation of the microorganisms. Finally, CNS infection can manifest with extrapyramidalism or acute meningoencephalitis.24
Needle aspiration or biopsy may not be necessary to confirm the diagnosis for most patients with pulmonary nocardiosis; nevertheless, in AIDS patients, the possibility of infections with multiple organisms, or infection plus tumor (especially lymphomas), means that the diagnostic procedure must be modified. Beaman and Beaman noted that CNS infections tended to be destructive and more rapidly progressive in immuno- compromised hosts than in patients with normal host defenses, whose infections are insidious and slowly progressive.
DIAGNOSIS
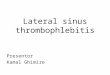
The most common specimens from which Nocardia species are isolated are respiratory secretions, skin biopsies, aspiration from deep collections, cerebrospinal fluid (CSF) and biopsy smears. Gram staining and modified Kinyoun staining are the techniques for the identification of Nocardia. Direct smears typically show Gram-positive, beaded, branching filaments that are usually acid fast (Figure 4). In general, the colonies have a chalky white or cotton ball appearance because of the presence of abundant aerial filaments.
Figure 4. Micrograph of a sputum smear stained with modified Kinyoun stain, showing the characteristic structure of Nocardia species.

Nocardiosis: a review I Corti and Fioti 247
Nocardia species will grow on most non-selective media used routinely for the culture of bacteria, fungi and mycobacteria. However, in specimens containing mixed flora, nocardial colonies are easily obscured by those of more rapidly growing bacteria, and the yield is increased by the use of selective media such as Thayer-Martin agar with antibiotics. Growth of Nocardia species may take from 48 h to several weeks, but typical colonies are usually seen after 3-5 days.37 Once the microorganism is isolated, multiple laboratory tests can be used to differentiate the different species, especially from mycobacteria that can present a similar structural pattern. Exceptionally, Nocardia can be isolated from blood.
When brain infection is present, the CSF shows protein elevation, hypoglycorrachia and neutrophilic pleocytosis. N. asteroides can be isolated rarely from CSE3*
HISTOPATHOLOGIC DIAGNOSIS
The lesions of nocardiosis cause intense suppuration, and the macroscopic aspects are similar to those of lesions caused by pyogenic bacteria. Different kinds of abscess can be seen, miliary or large and multiloculated. The absence of fibrosis, the small number of fistula and the lack of granules can differentiate these lesions from those of actinomycosis. There is not much of a tendency for the process to be limited.The histopathology of brain biopsy shows the existence of suppurative granuloma with central necrosis and fibrosis.
TREATMENT
Antibiotic treatment
Clinical experience has shown that successful therapy requires the use of antimicrobial drugs in combination with appropriate surgical drainage. The optimal anti- microbial therapy depends on the severity and localiza- tion of the infection, the species of Nocardia, host immune status, potential drug interactions and toxicity associated with antibiotic use. In some circumstances, and especially in cases of relapse after therapy, antimicrobial susceptibility testing is recommended, and it is appropriate for a reference laboratory to confirm test results. Indications for testing include isolation of Nocardia species from areas of deep-seated or disseminated infection, lack of response to initial therapy, contraindications to the use of sulfonamides, and infections that are caused by resistant strains such as N. farcinica and N. otitidiscaviarum.33,3g42 On the other hand, a recent study showed an unexplained discrepancy with respect to the susceptibility of N. asteroides to sulfonamides between European patients and US patients. 41,42 Although different kinds of antibiotics have been shown to be active against Nocardia strains, sulfonamides have represented the treatment of choice since their introduction in the 1940s. They are active
against N. brasiliensis, N. asteroides complex and N. transvaZensis,13,43~44 but are less effective in vitro against N. otitidiscaviarum.41,42 Some authors suggest the utility of the combination of trimethoprim (TMP) and sulfamethoxazole (SMX), based on their efficacy in this combination in comparison to sulfadiazine, in spite of the increased myelotoxicity, especially in patients receiving myelosuppressive therapy.43
Pleuropulmonary infections caused by strains of N. asteroides complex respond favorably to sulfonamides in 90% of cases.13 In adults with normal renal function and localized disease, the recommended dose of TMP is 5-10 mg/kg per day, and that of SMX is 25 mglkg per day, divided into three or four doses. In patients with primary cutaneous infection including sporotrichoid nocardiosis, TMP-SMX at 5 mg/kg per day (TMP component) is sufficient in combination with surgical debridement.
Higher initial doses (15 mg/kg TMP and 75 mg/kg SMX intravenously) are frequently used in patients with cerebral abscesses, extensive and disseminated infection, or AIDS.44-46 After 3-6 weeks, doses can be reduced and given orally. In severely ill or immunosuppressed patients, two or more drugs in combination can be necessary, including sulfonamides. Sulfadiazine and sulfisoxazole show equal efficacy in the treatment of nocardiosis. The recommended dose of sulfadiazine is lo-12 g/day and that of sulfisoxazole is 6-12 g/day, in four to six oral doses with a high fluid intake and oral sodium bicarbonate, because it can induce oliguria, azotemia and crystalluria. I3 Lower doses can be used in cases of pulmonary involvement.35 In AIDS patients, higher doses are needed. 47 In cases of disseminated forms and CNS involvement, the minimal course of treatment is 6 weeks, although the optimal duration may be up to 3 months. 48 Alternative antimicrobial agents should be considered in patients with allergy, gastro- intestinal intolerance or myelotoxicity. In these cases, amikacin is probably the most active agent in vitro against Nocardia species, except for N. transvalensis. l3 Amikacin shows synergistic activity when used with other antimicrobials, especially imipenem, third-genera- tion cephalosporins and TMP-SMX. The major dis- advantages of amikacin are the necessity for parenteral administration and the potential for renal toxicity and ototoxicity with prolonged administration.
Imipenem is also very active in vitro, although N. furcinica and N. brasiliensis are highly resistant to it.13 Imipenem is most active when used with amikacin. This combination is the optimal parenteral therapy for initial treatment. Meropenem is an alternative to imipenem in patients with cerebral nocardiosis, because it has a similar pharmacokinetic profile, good CSF penetration and a lower incidence of seizures.49
Minocycline may be effective (only N. transvalensis shows resistance) when it is used alone or in combination with other drugs or in sequential therapy.4,45 The usual doses are between 100 and 600 mg/day.50

248 International Journal of Infectious Diseases I Volume 7, Number 4,2003
Amoxicillin-clavulanate has been shown to be effective against N. asteroides, N. farcinica and N. brasiliensis, and may be especially useful in the treat- ment of cutaneous infections, especially those caused by B-lactamase-producing strains.51%52
Third-generation cephalosporins are active against Nocardia species, with the exception of N. farcinica, N. transvalensis and N. otitidiscaviarum. Ceftriaxone, cefotaxime and cefuroxime are useful, especially in cases of cerebral nocardiosis, because they have excellent CSF penetration and low toxicity.
Linezolid, a member of a new class of antibiotics called the oxazolidinones, has been shown to have in vitro activity against 56 strains of Nocardia species, including N. farcinica and N. transvalensis.53
Surgical treatment
The place of surgery in the management of nocardiosis depends on the site and extent of the infection. In extraneural disease, indications for aspiration, drainage or excision of abscesses are similar to those for other chronic bacterial infections. Therapeutic aspiration is generally inadequate in patients with thick-walled multiloculated abscesses, which contain free-flowing pus, including patients with mycetomas.36 In patients with brain abscesses, surgery should be performed when the abscesses are accessible and relatively large, the patient’s condition deteriorates or lesions progress within 2 weeks of therapy, or no reduction in abscess size is seen within a month of therapy.36 Decompression of lesions can be accomplished by stereotactic aspiration, although cure in many cases is achieved only after craniotomy and total excision.36%54 Mamelak et a13(j reported a significant reduction in mortality rate in patients with craniotomy (24%) in comparison to those who had undergone aspiration or drainage (50%). On the assumption that Nocardia brain abscesses are often multiple, surgery is extended, and the mortality rate is 66%, compared to 33% for those with single abscesses. In contrast, in cases of bacterial abscesses, the mortality rate is less than 10%.55,56
The mortality rate for nocardial brain abscesses has dropped by almost 50% since the introduction of CT. However, the reduction of the global mortality rate between 1975 and 1990 was not significant (39% versus 31%). In this same period, mortality rates were significantly higher among immunocompromised patients.36
DURATION OF THERAPY AND PROGNOSIS
Clinical improvement is evident within 7-10 days after the initiation of therapy. Parenteral therapy can be changed to an oral regimen, and high doses of TMP- SMX may be reduced after 3-6 weeks. Patients with extensive nocardiosis, subjects with lesions not accessible to surgery or those who respond slowly may benefit
from prolongation of parenteral and oral treatment. Lack of response to initial therapy may be due to primary drug resistance, inadequate penetration of drugs into sites of infection, especially in abscesses, and immuno- compromised status, including AIDS.13
The duration of therapy is variable, and depends on the localization of the lesions and the immune status. Cutaneous forms are cured after l-3 months of treat- ment; but prolonged therapy is required in cases of mycetoma.35,43 Pulmonary and systemic nocardiosis, excluding CNS involvement, should be treated for at least 6 months. In non-HIV-infected54 immunocom- promised patients, therapy should be continued for 12 months or longer; depending on concurrent increases in immunosuppression, treatment with low doses of TMP-SMX may be needed.44 In AIDS patients, secondary treatment is maintained with low doses of TMP-SMX. Primary treatment is generally not needed in patients who are immunocompromised, because of the low incidence of nocardiosis.57 However, the extended use of TMP-SMX for the treatment of other opportunistic infections probably has a beneficial effect against nocardiosis.js Palacios et al7 reported 17 cases of nocardiosis in AIDS patients; only four of them were receiving treatment with TMP-SMX at the moment of diagnosis.7
The clinical outcome of therapy depends on the site and extent of diseases and underlying host factors; cure rates of almost 100% are found in patients with skin and soft tissue involvement, as compared with 90% in pleuropulmonary disease, 60% in disseminated forms and 50% in brain abscesses. 44 Mortality is higher among immunocompromised patients and those with multiple brain abscesses.
In summary, most of the patients have favorable outcomes and show good response to treatment, in almost all cases of immunosuppression, when early treatment is given.57,59 Delay in diagnosis and early suspension of treatment, especially in AIDS patients, is associated with relapse and failure of treatment.47
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Kwon-Chung KJ, Bennett JE. Medical mycology. Philadelphia: Lea & Febiger, 1992. Negroni R. Mitosis en pacientes con sida. Rev Arg Micol 1990; 13:3-14. Cross RM, Bindford ChH. Is Nocardia asteroides an opportunistic pathogen. Lab Invest 1962; 11:1103. Curry WA. Human nocardiosis. A clinical review with selected case reports. Arch Intern Med 1980; 140:818-826. Dominguez DC, Anthony SJ. Actinomyces and Nocardia infections in immunocompromised and nonimmunocom- promised patients. J Nat1 Med Assoc 1999; 91:35-39. Menendez R, Corder0 PJ, Santos M, Gobernado M, Marco V. Pulmonary infection with Nocardia species: a report of 10 cases and review. Eur Respir J 1997; 10:X42- 1546. Palacios R, Santos J, Garcia-Ordkez JM, et al. Nocardiosis in patients with HIV infection [Abstract P309]. In: 8th

Nocardiosis: a review I Corti and Fioti 249
European Conference on Clinical Aspects and Treatment of HIV Infection, Athens, Greece. Athens: Provoli Publicity, 2001:192.
8. Uttamchandani RB, Daikos GL, Reyes RR, Fischl MA, Dickinson GM, Yamaguchi E. Nocardiosis in 30 patients with advanced human immunodeficiency virus infection: clinical features and outcome. Clin Infect Dis 1994; l&348-353.
9. Machado CM, Macedo MC, Castelli JB, Ostronoff M, Silva AC, Zambon E. Clinical features and successful recovery from disseminated nocardiosis after BMT. Bone Marrow Transplant 1997; 19:81-82.
10. Bhave AA, Thirunavukkarasu K, Gottlieb DJ, Bradstock K. Disseminated nocardiosis in a bone marrow transplant recipient with chronic GVHD. Bone Marrow Transplant 1999; 23:519-521.
11. Palmer SM, Kanj SS, Davis RD, Tapson VF. A case of disseminated infection with Nocardia braziliensis in a lung transplant recipient. Transplantation 1997; 63:1189-1190.
12. Mufioz P, Palomo J, Guembe P, Rodriguez-Creixems M, Gijon P, Bouza E. Lung nodular lesions in heart transplantation recipients. J Heart Lung Transplant 2000; 19:660667.
13. Lerner PI. Nocardiosis. Clin Infect Dis 1996; 22:891-905. 14. Fijen CA, Schrama J, Kuijper EJ, Boiron P, Gerritsen
W, Speelman I? Infection due to Nocardia farcinica in a woman with chronic granulomatous disease. Clin Infect Dis 1998; 26:222-224.
15. Mok CC, Yuen KY, Lau CS. Nocardiosis in systemic lupus erythematosus. Semin Arthritis Rheum 1997; 26:675-683.
16. Mgrquez-Diaz F, Soto-Ramfrez LE, Sifuentes Osornio J. Nocardiosis in patients with HIV infection. AIDS Patient Care STDs 1998; 12(11):825-832.
17. Arranz JA, Bueno C, Daza R, Moya MS. Nocardiosis cutanea primaria y Sindrome de Inmunodeficiencia Adquirida. Rev Clin Esp 1990; 187:207.
18. Boixeda de Miguel P Espafia A, Hermida JM, Buzon L. Nocardiosis cutanea y sida. Rev Clin Esp 1991; 189:395-396.
19. Blumel J, Blumel E, Yassin AF, Schmidt-Rotte H, Schaal KP Typing of Nocardia farcinica by pulsed-field gel electrophoresis and randomly amplified polymorphic DNA PCR. J Clin Microbial 1998; 36:118-122.
20. Lerner PI. Nocardia species. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and practice of infectious diseases, 4th edn. New York: Churchill Livingstone, 1995:2273-2280.
21. Scott WW, Kuhlman JE. Focal pulmonary lesions in patients with AIDS: percutaneous transthoracic needle biopsy. Radiology 1991; 180:419-421.
22. McNeil MM, Brown JM. The medically important anaerobic Actinomycetes: epidemiology and microbiology. Clin Microbial Rev 1994; 7:357-417.
23. Sahathevan M, Harvey FAH, Forbes G, et al. Epidemiology, bacteriology and control of an outbreak of Nocardia asteroides infection on a liver unit. J Hosp Infect 1991; lS(supp1 A):473480.
24. Beaman BL, Beaman L. Nocardia species: host-parasite relationships. Clin Microbial Rev 1994; 7:213-264.
25. Palasi P Lopez J, Valls JM, et al. Absceso retromamario por Nocardia asteroides en un paciente HIV positivo. Enferm Infec Microbial Clin 1998; 16:201-202.
26. Stevens DA, Pier AC, Beaman BL, Morozumi PA, Lovett IS, Houang ET. Laboratory evaluation of an outbreak of nocardiosis in immunocompromised hosts. Am J Med 1981; 71:928-934.
27. Mahgoub ES. Agents of mycetoma. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and practice of infect-
ious diseases, 4th edn. New York: Churchill Livingstone, 1995:2327-2330.
28. Matthay RA, Greene WH. Infecciones pulmonares en pacientes con deficiencia inmune. Clin Med Nor 1980; 3:531-554.
29. Beaman BL, Boiron P Beaman L, Brownell GH, Schaal K, Gombert ME. Nocardia and nocardiosis. J Med Vet Mycol 1992; 3O(suppl 1):317-331.
30. Beaman BL, Beaman L, Kjelstrom JA, Ogata SA. Bacteria and neurodegeneration. In: Calne D, ed. Neurodegenerative diseases. Orlando, Florida: WB Saunders, 1994:319-338.
31. Ramanathan P, Rahimi AR. Nocardia asteroides pericarditis in association with HIV Aids Patient Care STDs 2000; 14(12):621-625.
32. River0 A, Estevez A, Santos J, Marquez M. Cardiac tamponade caused by Nocardia asteroides in an HIV- infected patient. J Infect 2000; 40:206-207.
33. Boiron P, Provost F, Chevrier G, DuPont B. Review of nocardial infections in France 1987 to 1990. Eur J Clin Microbial Infect Dis 1992; 11:709-714.
34. Schaal KP, Lee HJ. Actinomycete infections in humans-a review. Gene 1992; 115:201-211.
35. Georghiou PR, Blacklock ZM. Infection with Nocardia species in Queensland: a review of 102 clinical isolates. Med J Aust 1992; 156:692-697.
36. Mamelak AN, Obana WG, Flaherty JF, Rosenblum ML. Nocardial brain abscess: treatment strategies and factors influencing outcome. Neurosurgery 1994; 35:622-631.
37. Ashdown LR. Improved screening technique for isolation of Nocardia species from sputum specimens. Pathology 1990; 22:157-161.
38. Shawar RM, Moore DG, LaRocco MT. Cultivations of Nocardia spp. on chemically defined media for selective recovery of isolates from clinical specimens. J Clin Microbial 1990; 28:508-512.
39. Saboulle MA. In vitro susceptibility testing of clinical isolates of Nocardia. Clin Microbial Newslett 1993; 15: 169-172.
40. McNeil MM, Brown JM, Hutwagner LC. Evaluation for therapy for Nocardia asteroides complex infections. Infect Dis Clin Pratt 1995; 4:287-292.
41. Berkey P Moore D, Rolston K. In vitro susceptibilities of Nocardia species to newer antimicrobial agents. Antimicrob Agents Chemother 1998; 32:1078-1079.
42. Boiron P Provost F. In-vitro susceptibility testing of Nocardia spp. and its taxonomic implication. J Antimicrob Chemother 1988; 22:623-629.
43. Wallace RJ Jr, Septimus EJ, Williams TW Jr, et al. Use of trimethoprim-sulfamethozaxole for treatments of infections due to Nocardia. Rev Infect Dis 1982; 4:315-325.
44. Smego RA, Gallis HA. The clinical spectrum of Nocardia braziliensis infection in the United States. Rev Infect Dis 1984; 6:164-180.
45. Lucas SB, Hounnou A, Peacock C, Beaumel A, Kadio A, De Cock KM. Nocardiosis in HIV-positive patients: an autopsy study in West Africa. Tuber Lung Dis 1994; 75: 301-307.
46. Smego RA, Moeller MB, Gallis HA. Trimethoprim- sulfamethoxazole therapy for Nocardia infections. Arch Intern Med 1983; 143:711-7X
47. Gallant JE, Ko AH. Cavitary pulmonary lesions in patients infected with human immunodeficiency virus. Clin Infect Dis 1996; 22:671-682.
48. Negroni R. Mitosis de1 sistema nervioso. In: Negroni R, ed. Lecciones de clinica micologica, 1st edn. Buenos Aires: La Agenda, 1997:61-72.

250 International Journal of Infectious Diseases I Volume 7, Number 4,2003
49. Wilson RW, Steingrube VA, Brown BA, et al. Recognition of a Nocardia transvalensis complex by resistance to aminoglycosides, including amikacin, and PCR restriction fragment length polymorphism analysis. J Clin Microbial 1997; 35:2235-2242.
50. Leitersdof I, Silver J, Naparstek E, Raveh D. Tetracycline derivatives, alternative treatment for nocardiosis in transplanted patients. Clin Nephrol 1997; 48:48-51.
51. Wortman PD. Treatment of a Nocardia brasiliensis mycetoma with sulfamethoxazole and trimethoprim, amikacin and amoxicillin and clavulanate. Arch Dermatol 1993; 129:564-567.
52. Wallace RJ, Nash DR, Johnson WK, Steele LC, Steingrube VA. l3-Lactam resistance in Nocardia braziliensis is mediated by B-lactamase and reversed in the presence of clavulanic acid. J Infect Dis 1987; 156:959-966.
53. Brown BA, Ward SC, Mann L. In vitro activity of linezolid against multiple species of Nocardia: a new drug of choice for a difficult disease [Abstract POO-01841. In: Proceedings of the 100th General Meeting of the American Society for
Microbiology, Los Angeles, CA, 2000. Washington, DC: ASM.
54. Byrne E, Brophy BP, Perrett LV. Nocardial cerebral abscess: new concepts in diagnosis, management, and prog- nosis. J Neurol Neurosurg Psychiatry 1979; 42:1038-1045.
55. Mamelak AN, Mampalam TJ, Rosemblum ML. Brain abscesses: diagnosis and management. Hosp Med 1992; 28:22-38.
56. Mampalam TJ, Rosemblum ML. Trends in the manage- ment of bacterial brain abscesses: a review of 102 cases over 17 years. Neurosurgery 1988; 23:451-4X
57. Arduino RC, Johnson PC, Miranda AG. Nocardiosis in renal transplant recipients undergoing immunosuppres- sion with cyclosporine. Clin Infect Dis 1993; 16:505- 512.
58. Kim J, Minamoto GY, Grieco MH. Nocardial infection as a complication of AIDS: report of six cases and review. Rev Infect Dis 1991; 13:624-629.
59. Van Burik JA, Hackman RC, Nadeem SQ. Nocardiosis after bone marrow transplantation: a retrospective study. Clin Infect Dis 1997; 24:1154-1160.