Embed Size (px)
Citation preview

New Horizons in Multiple Myeloma
2013
James R. Berenson, MD
Medical & Scientific Director
Institute for Myeloma & Bone Cancer Research
Los Angeles, CA

Treatment Choices for
Myeloma Patients
• The number of choices is growing rapidly! – More new combinations involving already approved
drugs
– Clinical trials of drugs recently and not yet approved
• Thus, it is becoming more difficult to come up with a clearcut paradigm – i.e. it’s becoming much more complicated
• Patient wants the longest life possible with therapy and a disease that has the least impact on their life!
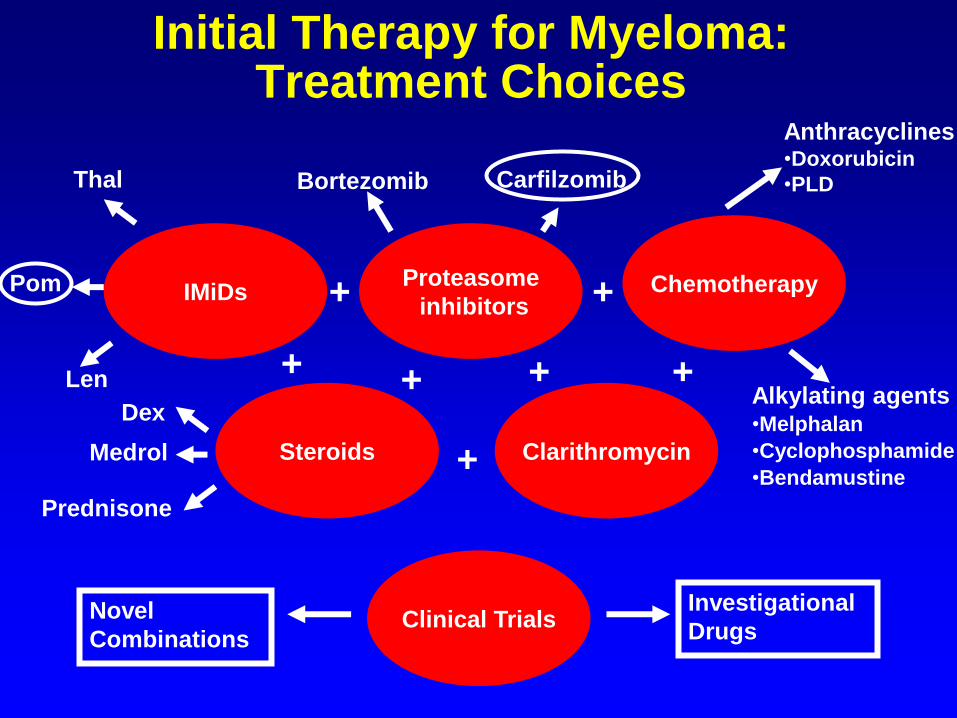
Initial Therapy for Myeloma: Treatment Choices
IMiDs Proteasome
inhibitors Chemotherapy
Steroids Clarithromycin
Clinical Trials
+
+ +
+
+
+
Investigational
Drugs Novel
Combinations
Thal
Len
Dex
Medrol
Prednisone
Alkylating agents •Melphalan
•Cyclophosphamide
•Bendamustine
Anthracyclines •Doxorubicin
•PLD
+
Bortezomib Carfilzomib
Pom
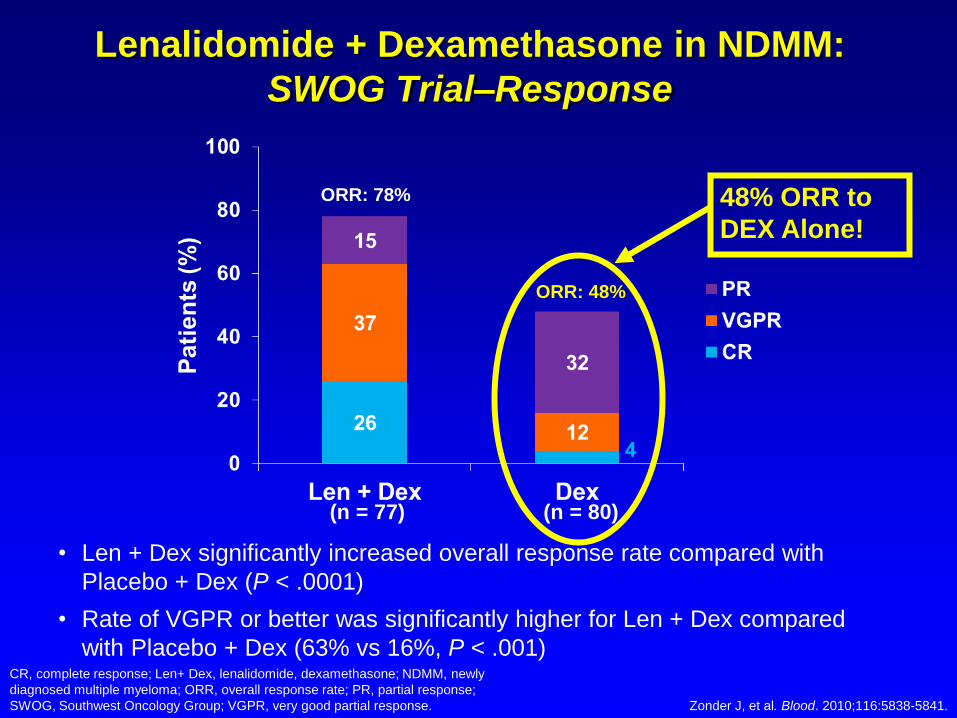
• Len + Dex significantly increased overall response rate compared with
Placebo + Dex (P < .0001)
• Rate of VGPR or better was significantly higher for Len + Dex compared
with Placebo + Dex (63% vs 16%, P < .001)
Lenalidomide + Dexamethasone in NDMM:
SWOG Trial–Response
CR, complete response; Len+ Dex, lenalidomide, dexamethasone; NDMM, newly
diagnosed multiple myeloma; ORR, overall response rate; PR, partial response;
SWOG, Southwest Oncology Group; VGPR, very good partial response. Zonder J, et al. Blood. 2010;116:5838-5841.
ORR: 78%
ORR: 48%
(n = 77) (n = 80)
48% ORR to
DEX Alone!

Newly Diagnosed Multiple Myeloma: Lenalidomide 25 mg d1-21 (28 days per cycle)
48%

Lenalidomide + Dexamethasone in NDMM: ECOG E4A03 Trial–Overall Survival
Months
6 12 24 30 36 42 18
1.0
0.2
0.4
0.6
0.8
Ove
rall
Su
rviv
al
Rd
• One-year OS was significantly better for Rd compared with RD regardless of age
– < 65 years of age: 98% vs 91%; P = .01
– ≥ 65 years of age: 94% vs 83%; P = .004
a P = .0002 vs RD.
ECOG, Eastern Cooperative Oncology Group; NDMM, newly diagnosed multiple
myeloma; OS, overall survival; Rd, lenalidomide, low-dose dexamethasone; RD,
lenalidomide, high-dose dexamethasone.
RD
0
0
Rajkumar SV, et al. Lancet Oncol. 2010;11:29-37.
1-y OS 2-y OS
87% 75%
96%a 87%
Len 25 mg + Dex 40 mg d1-4, 9-12, 17-20
Len 25 mg + Dex 40 mg d1, 8, 15, & 22
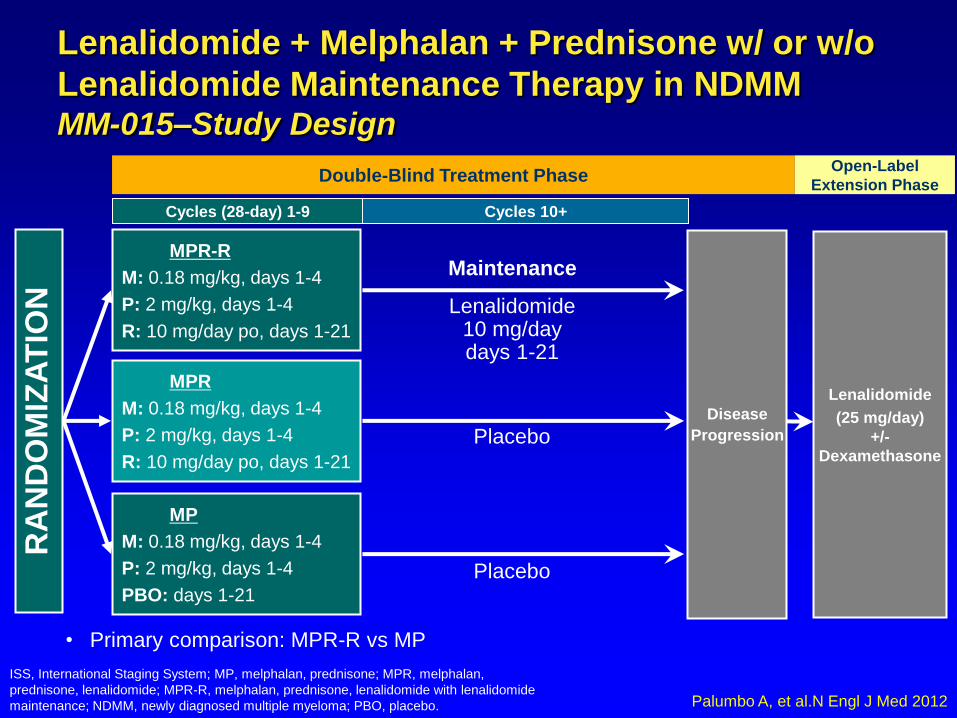
MP
M: 0.18 mg/kg, days 1-4
P: 2 mg/kg, days 1-4
PBO: days 1-21
MPR
M: 0.18 mg/kg, days 1-4
P: 2 mg/kg, days 1-4
R: 10 mg/day po, days 1-21
Placebo
Placebo
MPR-R
M: 0.18 mg/kg, days 1-4
P: 2 mg/kg, days 1-4
R: 10 mg/day po, days 1-21
RA
ND
OM
IZA
TIO
N
Double-Blind Treatment Phase
Disease
Progression
Maintenance
Lenalidomide
(25 mg/day)
+/-
Dexamethasone
Open-Label
Extension Phase
Lenalidomide 10 mg/day days 1-21
Cycles (28-day) 1-9 Cycles 10+
ISS, International Staging System; MP, melphalan, prednisone; MPR, melphalan,
prednisone, lenalidomide; MPR-R, melphalan, prednisone, lenalidomide with lenalidomide
maintenance; NDMM, newly diagnosed multiple myeloma; PBO, placebo.
• Primary comparison: MPR-R vs MP
Lenalidomide + Melphalan + Prednisone w/ or w/o
Lenalidomide Maintenance Therapy in NDMM MM-015–Study Design
Palumbo A, et al.N Engl J Med 2012

0
HR, hazard ratio; MP, melphalan, prednisone; MPR, melphalan, prednisone, lenalidomide; MPR-R, melphalan, prednisone,
lenalidomide with lenalidomide maintenance; OS, overall survival; PFS, progression-free survival; TTP, time to progression.
ProgressionProgression--Free and Overall SurvivalFree and Overall SurvivalAll PatientsAll Patients
• TTP HR advantages were similar: MPR-R vs MP = 0.337; MPR vs MP = 0.826
Time (Months)
Pati
en
ts (
%)
HR 0.395 P < .001
HR 0.796P = .135
0 10 20 30 400
25
50
75
100
Median PFS
MPR-R 31 months
MPR 14 months
MP 13 months
Median PFS
MPR-R 31 months
MPR 14 months
MP 13 months
0 20 30 40 50 60
4-year OS
MPR-R 59%
MPR 58%
MP 58%
4-year OS
MPR-R 59%
MPR 58%
MP 58%
Pati
en
ts (
%)
25
50
75
10
100
HR 0.898 P = .579
HR 1.089P = .648
Time (Months)
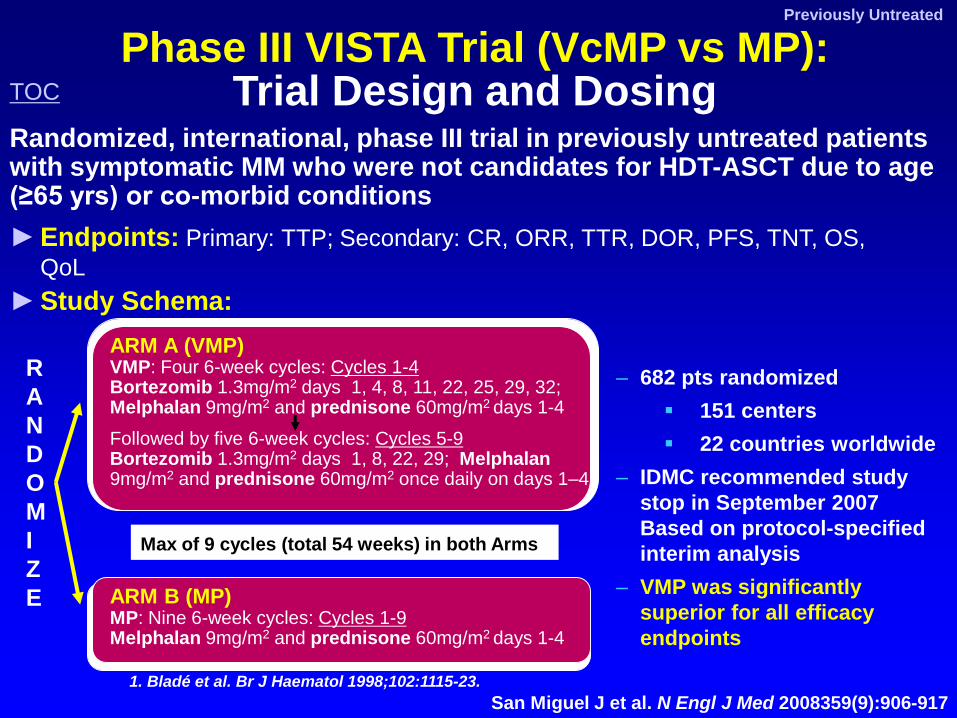
Phase III VISTA Trial (VcMP vs MP): Trial Design and Dosing
► Endpoints: Primary: TTP; Secondary: CR, ORR, TTR, DOR, PFS, TNT, OS,
QoL
Previously Untreated
San Miguel J et al. N Engl J Med 2008359(9):906-917
Randomized, international, phase III trial in previously untreated patients with symptomatic MM who were not candidates for HDT-ASCT due to age (≥65 yrs) or co-morbid conditions
1. Bladé et al. Br J Haematol 1998;102:1115-23.
ARM A (VMP) VMP: Four 6-week cycles: Cycles 1-4 Bortezomib 1.3mg/m2 days 1, 4, 8, 11, 22, 25, 29, 32; Melphalan 9mg/m2 and prednisone 60mg/m2 days 1-4 Followed by five 6-week cycles: Cycles 5-9 Bortezomib 1.3mg/m2 days 1, 8, 22, 29; Melphalan 9mg/m2 and prednisone 60mg/m2 once daily on days 1–4
ARM B (MP) MP: Nine 6-week cycles: Cycles 1-9 Melphalan 9mg/m2 and prednisone 60mg/m2 days 1-4
Max of 9 cycles (total 54 weeks) in both Arms
R
A
N
D
O
M
I
Z
E
► Study Schema:
– 682 pts randomized
151 centers
22 countries worldwide
– IDMC recommended study
stop in September 2007
Based on protocol-specified
interim analysis
– VMP was significantly
superior for all efficacy
endpoints
TOC
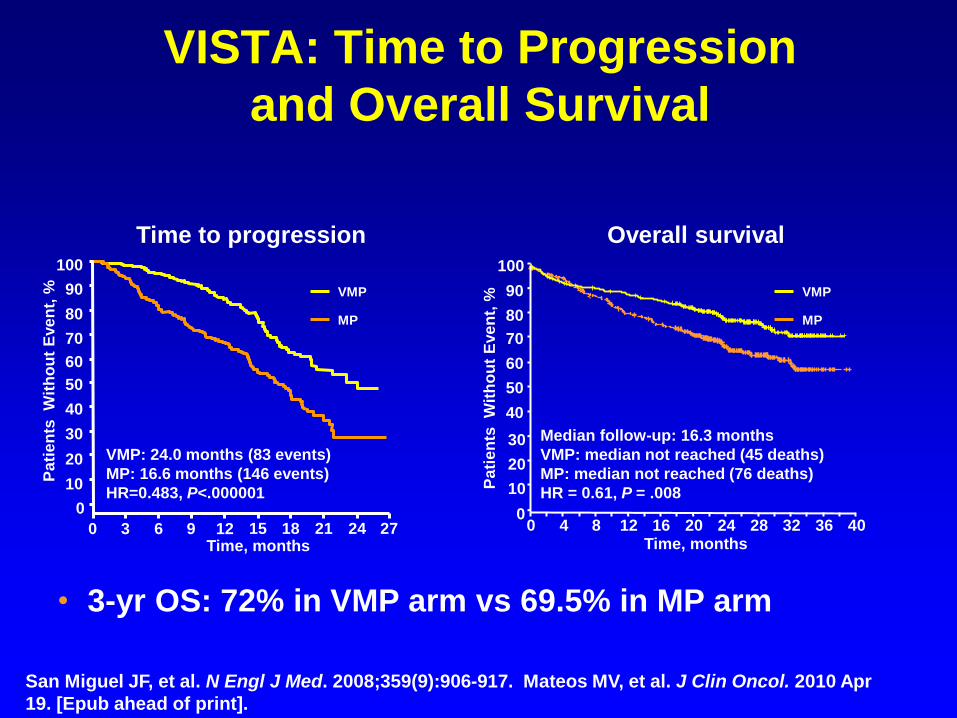
VISTA: Time to Progression
and Overall Survival
San Miguel JF, et al. N Engl J Med. 2008;359(9):906-917. Mateos MV, et al. J Clin Oncol. 2010 Apr
19. [Epub ahead of print].
VMP: 24.0 months (83 events)
MP: 16.6 months (146 events)
HR=0.483, P<.000001
Median follow-up: 16.3 months
VMP: median not reached (45 deaths)
MP: median not reached (76 deaths)
HR = 0.61, P = .008
Time, months
Pa
tie
nts
W
ith
ou
t E
ve
nt,
%
0 4 8 12 16 20 24 28 32 36 40 0
10
20
30
40
50
60
70
80
90
100
Time, months 0 3 6 9 12 15 18 21 24 27
0
10
20
30
40
50
60
70
80
90
100
Pa
tie
nts
W
ith
ou
t E
ve
nt,
%
VMP
MP
VMP
MP
Time to progression Overall survival
• 3-yr OS: 72% in VMP arm vs 69.5% in MP arm


Bortezomib + Pegylated Liposomal
Doxorubicin (Doxil) + Dexamethasone for
Patients with Previously Untreated Myeloma: A Phase II Trial
Days 1 2 3 4 5 6 7 8 9 10 11 29
Cycle repeats Bortezomib: 1.0 mg/m2 IV
Doxil: 5 mg/m2 IV infusion
Dexamethasone 40 mg IV
Berenson et al. Brit J Haematol, 2011

Response Type Number of Patients
(N = 35)
Complete Response (CR) (no serum M-protein)
7 (20%)
Very Good Partial Response (VGPR) (≥ 90% decrease in serum M-protein)
3 (8.6%)
Partial Response (PR) (50-74% decrease in serum M-protein)
15 (42.9%)
Minor Response (MR) (25-49% decrease in serum M-protein)
5 (14.3%)
Objective Response (CR+VGPR+PR+MR) 30 (85.8%)
Stable Disease (SD) (no serum M-protein)
3 (8.6%)
Disease Control (CR+VGPR +PR+MR+SD) 33 (94.4%)
Progressive Disease (PD) (>25% increase in serum M-protein)
2 (5.7%)
DVD: Response Rates
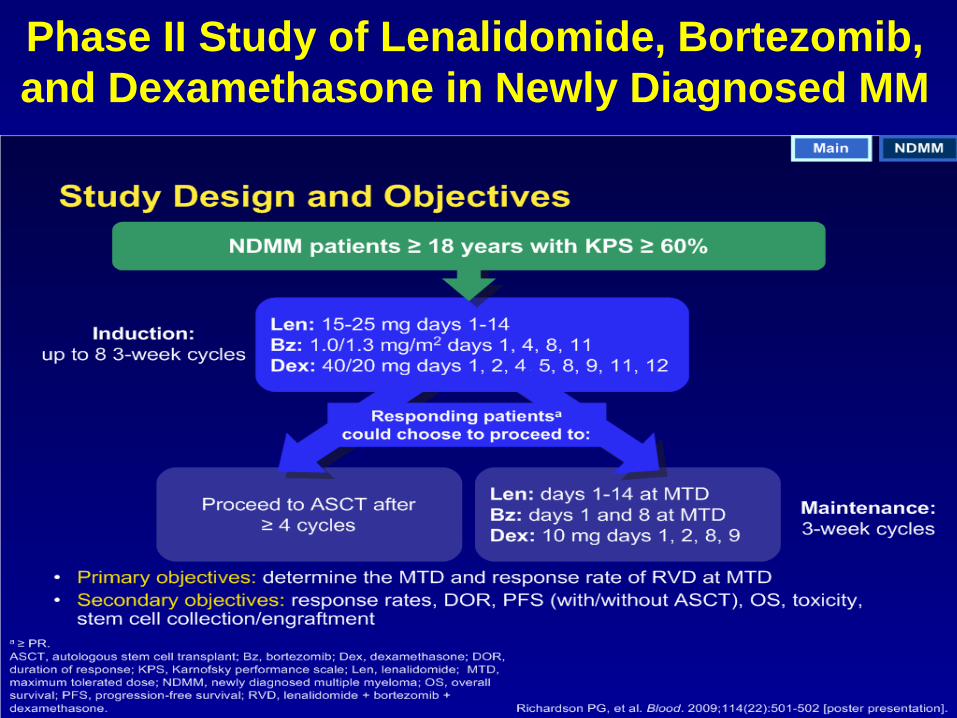
Phase II Study of Lenalidomide, Bortezomib,
and Dexamethasone in Newly Diagnosed MM
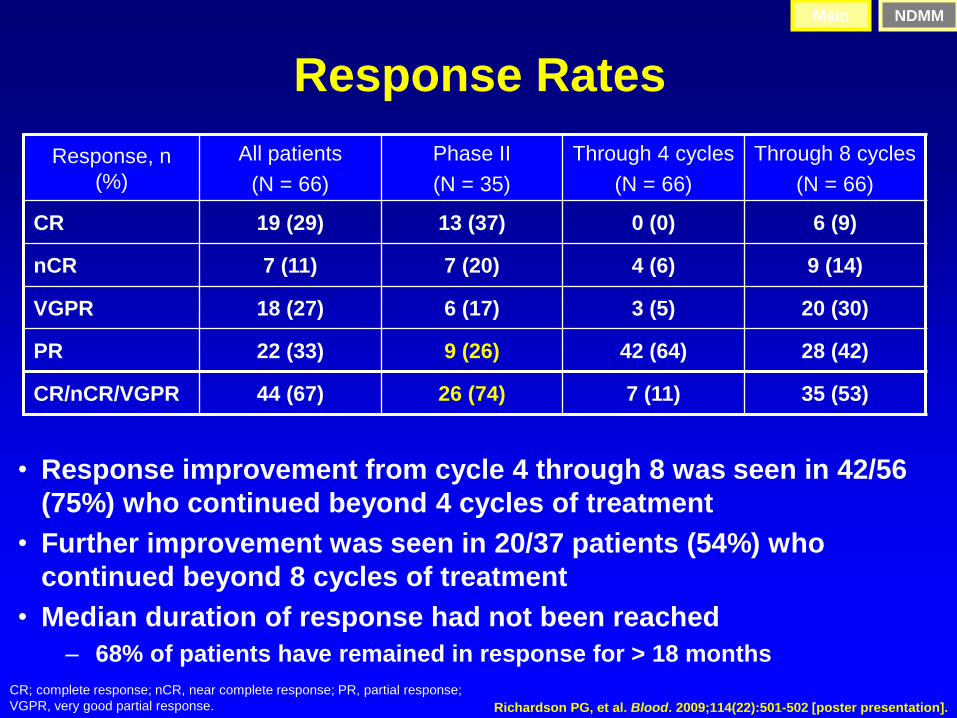
Response Rates
Response, n
(%)
All patients
(N = 66)
Phase II
(N = 35)
Through 4 cycles
(N = 66)
Through 8 cycles
(N = 66)
CR 19 (29) 13 (37) 0 (0) 6 (9)
nCR 7 (11) 7 (20) 4 (6) 9 (14)
VGPR 18 (27) 6 (17) 3 (5) 20 (30)
PR 22 (33) 9 (26) 42 (64) 28 (42)
CR/nCR/VGPR 44 (67) 26 (74) 7 (11) 35 (53)
• Response improvement from cycle 4 through 8 was seen in 42/56
(75%) who continued beyond 4 cycles of treatment
• Further improvement was seen in 20/37 patients (54%) who
continued beyond 8 cycles of treatment
• Median duration of response had not been reached
– 68% of patients have remained in response for > 18 months
CR; complete response; nCR, near complete response; PR, partial response;
VGPR, very good partial response.
Main NDMM
Richardson PG, et al. Blood. 2009;114(22):501-502 [poster presentation].
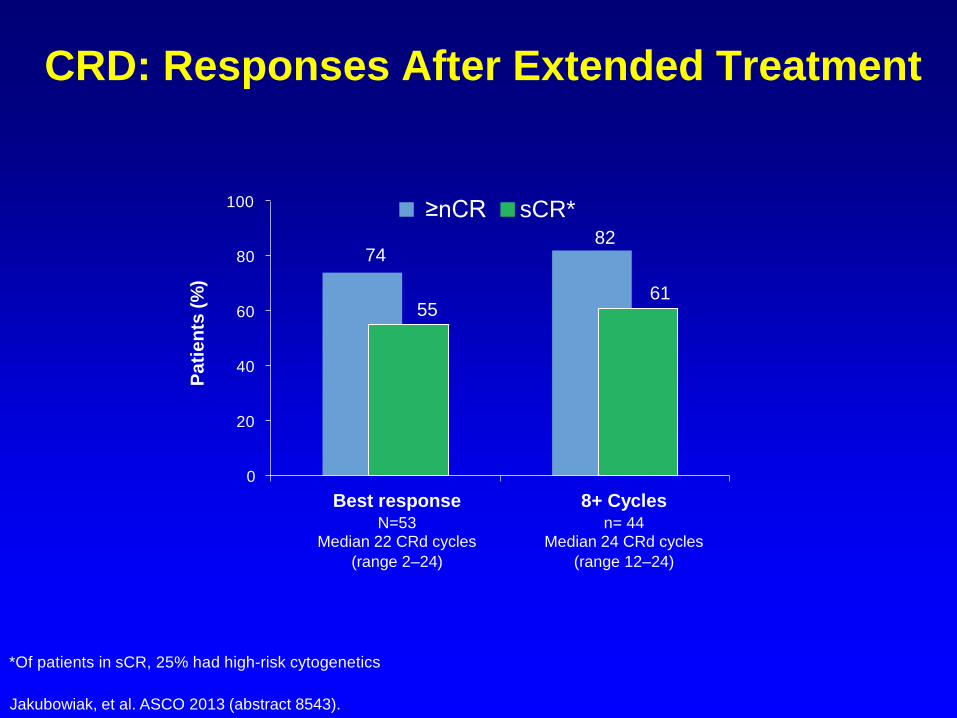
CRD: Responses After Extended Treatment
74 82
55 61
0
20
40
60
80
100 ≥nCR sCR*
Best response N=53
Median 22 CRd cycles
(range 2–24)
8+ Cycles n= 44
Median 24 CRd cycles
(range 12–24)
Pa
tie
nts
(%
)
*Of patients in sCR, 25% had high-risk cytogenetics
Jakubowiak, et al. ASCO 2013 (abstract 8543).

CRD: Progression-Free Survival
*For patients in sCR, estimated 24-month PFS was 97%
Jakubowiak, et al. ASCO 2013 (abstract 8543).
N=53
Median follow-up 25 months (range 5–37)
24-month rate 94%*
0 5 10 15 20 25 30 35 40
1.0
0.8
0.6
0.4
0.2
0.0
PF
S P
robabili
ty
Months




Principles of Treating
Relapsed/Refractory Multiple Myeloma
• Be sure a patient has really progressed before changing therapy – REPEAT MYELOMA LABS!
• Try to use drugs patient has not seen before • HOWEVER,
– progression on one drug in combination does not mean that drug will not be effective w/ another agent
• e.g., pts progressing from bortezomib w/ melphalan often respond to bortezomib w/ PLD
• Even different drugs in the same class may be active so that – bortezomib+melphalan failures may respond to other alkylating
agents- cyclophosphamide or bendamustine – LEN failures may respond to THAL and vice versa
– pts progressing from a drug at one dose may respond to the same drug at a higher dose- e.g., LEN
– the same combination may be effective again if the patient has not seen the combination in a long time
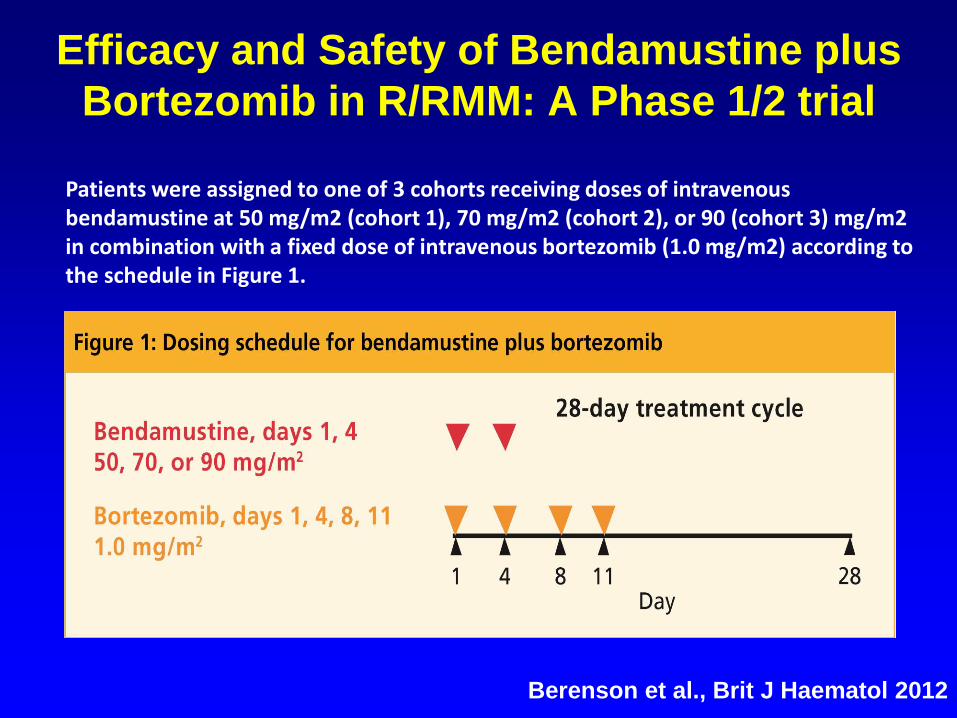
Efficacy and Safety of Bendamustine plus
Bortezomib in R/RMM: A Phase 1/2 trial
Patients were assigned to one of 3 cohorts receiving doses of intravenous bendamustine at 50 mg/m2 (cohort 1), 70 mg/m2 (cohort 2), or 90 (cohort 3) mg/m2 in combination with a fixed dose of intravenous bortezomib (1.0 mg/m2) according to the schedule in Figure 1.
Berenson et al., Brit J Haematol 2012

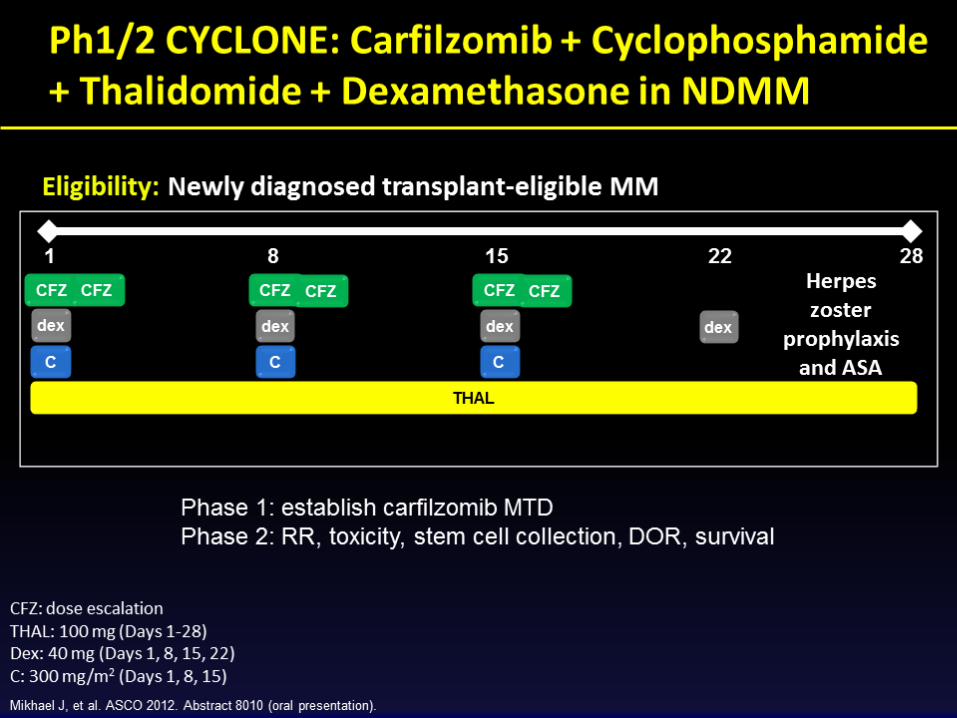
No DLT was observed at any dose level. 50 mg/m2 (n = 5) 70 mg/m2 (n = 4) 90 mg/m2 (n = 5)
The maximum dose of bendamustine (90 mg/m2) was well tolerated in combination with bortezomib 1.0 mg/m2 and was designated as the MTD Overall response rate
Overall 48% (1 CR, 2 VGPR, 9 PR, & 7 MR) At MTD (90 mg/m2) 52% Bortezomib-exposed (n=31) 42% Alkylator-exposed (n=28) 46%
Bendamustine & Bortezomib: Results

IFM 2009-01: Phase II study of bendamustine
+ bortezomib + Dex in elderly pts with
relapsed/refractory MM
• Objectives: Primary: response rate; Secondary:
time to best response, PFS, OS, toxicity
• Patients: 73 pts in first relapse or refractory to first-
line therapy; median age 76 yrs (66–86); no prior
bortezomib or bendamustine; Dose and schedule:
28-day cycles: bortezomib 1.3 mg/m2 IV and Dex 20
mg days 1, 8, 15, 22; bendamustine 70 mg/m2 days
1, 8; regimen given in 3 phases: – Induction: 4 consecutive cycles. Pts achieving ≥PR proceed to:
– Consolidation: 2 consecutive cycles; pts maintaining response
proceed to:
– Maintenance: 6 cycles, 1 cycle given every 2 mos
Rodon P, et al. ASH 2012, abstract #4044 Relapsed/Refractory MM

IFM 2009-01: Phase II study of bendamustine
+ bortezomib + Dex in elderly pts with
relapsed/refractory MM
• Results: Analysis restricted to first 6 cycles
• Adverse prognostic factors for response
(ORR) – Prior IMiD: yes, 61%; no, 100% (p=0.006)
– Del 17p: present, 20%; absent, 72% (p=0.036)
• 6-mo PFS: 67%; 6-mo OS: 81%
Rodon P, et al. ASH 2012, abstract #4044
Response (N=73)
ORR
(≥PR)
CR VGPR PR MR
67% 12% 17% 38% 8%
Relapsed/Refractory MM

Bendamustine (B) w/ Lenalidomide (L)
and Dexamethasone (D): Phase 1/2 Trial
• R/R MM patients
• N=29
• Regimen (28-day cycles) – B 75-100 mg/m2 d1 & 2
– L 5-10 mg qd d1-21
– Dex 40 mg PO weekly
• MTD: B 75/ L 10/ D 40
• Results (only 25 considered evaluable for response) – ORR (> PR): 52% w/ 24% VGPR
– MR 24%
– PFS: 6.1 mo Lentzsch et al. Blood 2012
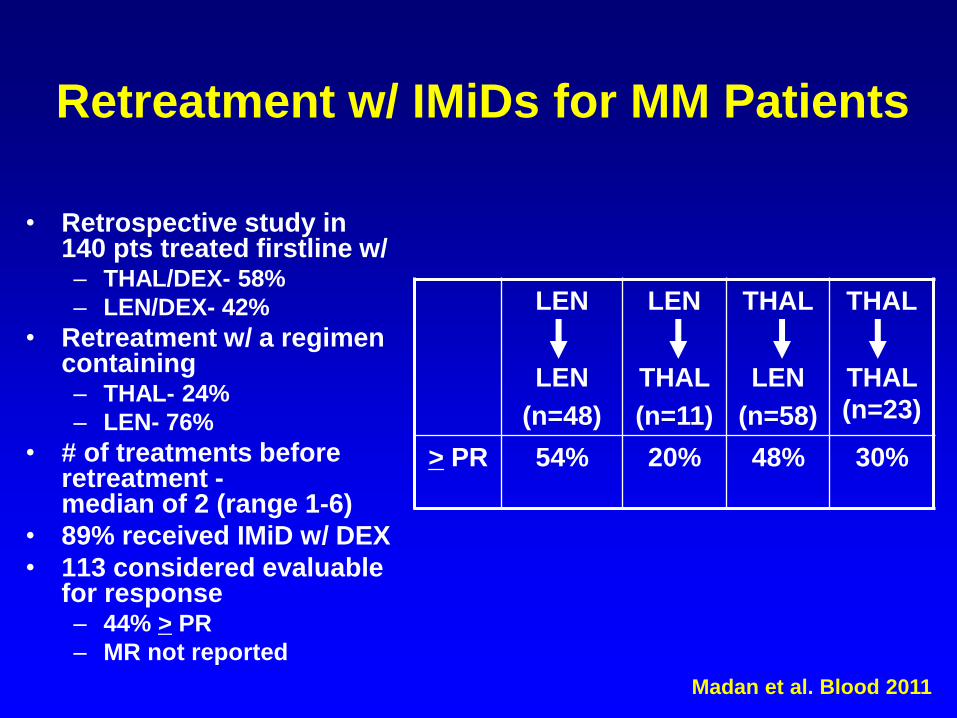
Retreatment w/ IMiDs for MM Patients
• Retrospective study in 140 pts treated firstline w/ – THAL/DEX- 58%
– LEN/DEX- 42%
• Retreatment w/ a regimen containing – THAL- 24%
– LEN- 76%
• # of treatments before retreatment - median of 2 (range 1-6)
• 89% received IMiD w/ DEX
• 113 considered evaluable for response – 44% > PR
– MR not reported
Madan et al. Blood 2011
LEN
LEN
(n=48)
LEN
THAL
(n=11)
THAL
LEN
(n=58)
THAL
THAL
(n=23)
> PR 54% 20% 48% 30%
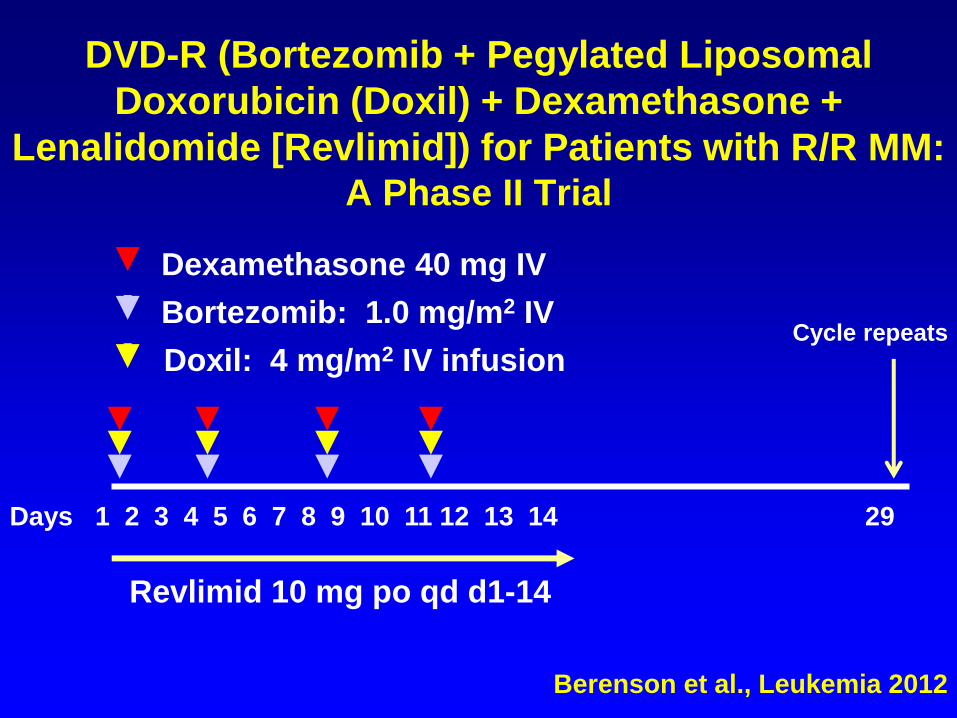
DVD-R (Bortezomib + Pegylated Liposomal
Doxorubicin (Doxil) + Dexamethasone +
Lenalidomide [Revlimid]) for Patients with R/R MM: A Phase II Trial
Days 1 2 3 4 5 6 7 8 9 10 11 12 13 14 29
Cycle repeats Bortezomib: 1.0 mg/m2 IV
Doxil: 4 mg/m2 IV infusion
Dexamethasone 40 mg IV
Berenson et al., Leukemia 2012
Revlimid 10 mg po qd d1-14

DVD-R: Response Rate N=39
Perc
en
t w
/o P
rog
ressio
n
Complete Response (CR) 8* (21%)
(no serum M-protein)
Very Good Partial Responses (VGPR) 4 (10%)
(> 90% decrease in serum M-protein)
Partial Response (PR) 7 (18%)
(50-74% decrease in serum M-protein)
Minor Response (MR) 14 (36%)
(25-49% decrease in serum M-protein)
Objective Response (CR+VGPR+PR+MR) 30 (85%)
Stable Disease (SD) 4 (10%)
(change in M-protein + 25%)
Disease Control (CR+VGPR+PR+MR+SD) 37 (95%)
Progressive Disease (PD) 2 (5%)
(>25% increase in M-protein)
*Based on the modified Blade’ criteria
*Based on the modified Blade’ criteria *Based on the modified Blade’ criteria
*Based on the modified Blade’ criteria
1. Chanan-Khan AA, et al. J Clin Oncol. 2008;26:1544-1552.
2. Richardson P, et al. Blood. 2010;116:377-378.[abstract 864].
3. Lacy MQ, et al. J Clin Oncol. 2009;27:5008-5014.
4. Lacy MQ, et al. Leukemia. 2010;24:1934-1939.
5. Lacy M, et al. J Clin Oncol. 2010;28:573s.[abstract 8002].
6. Lacy M, et al. Blood. 2010;116:377.[abstract 863].
7. Leleu X, et al. Blood. 2010;116:375.[abstract 859].
Pomalidomide: Background
• Pomalidomide (CC-4047) is a distinct IMiD®
immunomodulatory compound with anti-
angiogenic and potent anti-proliferative and pro-
apoptotic activities1
– Combines structures of lenalidomide and thalidomide
• Pomalidomide is now FDA-approved for the
treatment of patients with multiple myeloma who
have been treated with bortezomib and an IMiD
and are currently progressing while on therapy2-7
N H 2
N
N H
O O
O
O
RRMM, relapsed/refractory multiple myeloma.
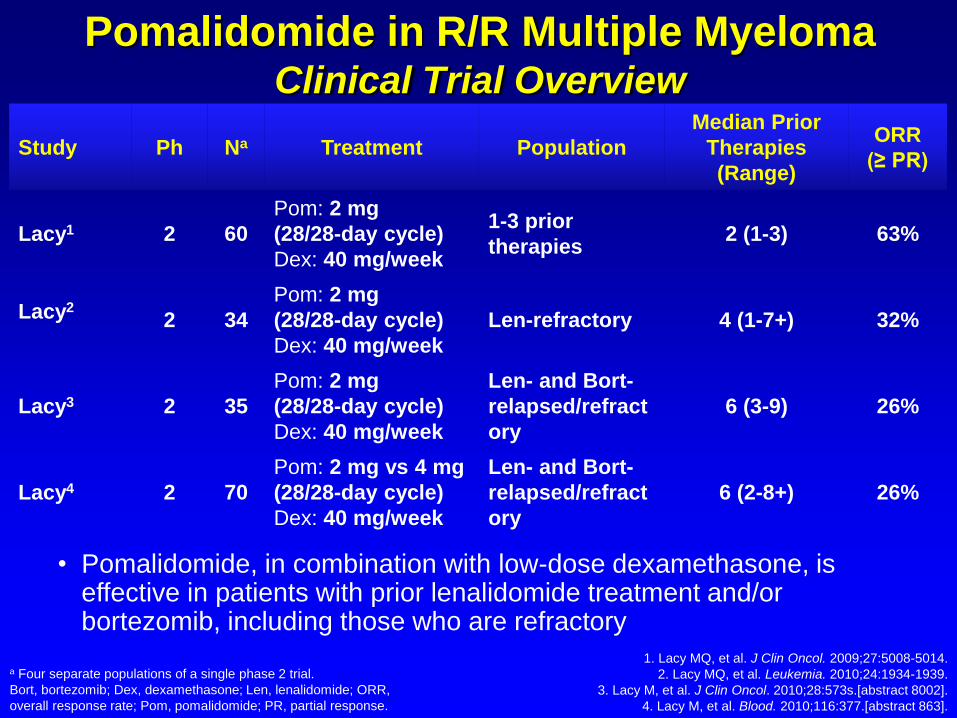
Study Ph Na Treatment Population
Median Prior
Therapies
(Range)
ORR
(≥ PR)
Lacy1 2 60
Pom: 2 mg
(28/28-day cycle)
Dex: 40 mg/week
1-3 prior
therapies 2 (1-3) 63%
Lacy2
2 34
Pom: 2 mg
(28/28-day cycle)
Dex: 40 mg/week
Len-refractory 4 (1-7+) 32%
Lacy3 2 35
Pom: 2 mg
(28/28-day cycle)
Dex: 40 mg/week
Len- and Bort-
relapsed/refract
ory
6 (3-9) 26%
Lacy4 2 70
Pom: 2 mg vs 4 mg
(28/28-day cycle)
Dex: 40 mg/week
Len- and Bort-
relapsed/refract
ory
6 (2-8+) 26%
1. Lacy MQ, et al. J Clin Oncol. 2009;27:5008-5014.
2. Lacy MQ, et al. Leukemia. 2010;24:1934-1939.
3. Lacy M, et al. J Clin Oncol. 2010;28:573s.[abstract 8002].
4. Lacy M, et al. Blood. 2010;116:377.[abstract 863].
Pomalidomide in R/R Multiple Myeloma Clinical Trial Overview
a Four separate populations of a single phase 2 trial.
Bort, bortezomib; Dex, dexamethasone; Len, lenalidomide; ORR,
overall response rate; Pom, pomalidomide; PR, partial response.
• Pomalidomide, in combination with low-dose dexamethasone, is effective in patients with prior lenalidomide treatment and/or bortezomib, including those who are refractory

MM-003: Pomalidomide +
LoDEX vs Single-Agent HiDEX • Patients with relapsed/refractory myeloma have
few therapeutic options, except high-dose
dexamethasone as a salvage therapy
• Patients stratified by number of
previoustherapies, refractory and
relapsed/refractory disease – Refractory to both lenalidomide and bortezomib: 73% in POM
+ LoDEX and 71% in HiDEX arms Dimopoulos MA, et al. ASH 2012. Abstract LBA-6.
POM + LoDEX Pomalidomide 4 mg on Days 1-21 +
Dexamethasone 40 mg (≤ 75) or 20 mg (> 75 yrs) on Days 1, 8, 15, 22
(n = 302)
HiDEX Dexamethasone 40 mg (≤ 75) or 20 mg
(> 75 yrs) on Days 1-4, 9-12, 17-20 (n = 153)
Patients with relased/
refractory MM
(N = 455)
Until PD or intolerable AE
Until PD
Follow-up for OS and SPM until 5 yrs
postenrollment
Companion trial MM-003C
Pomalidomide 21/28 days
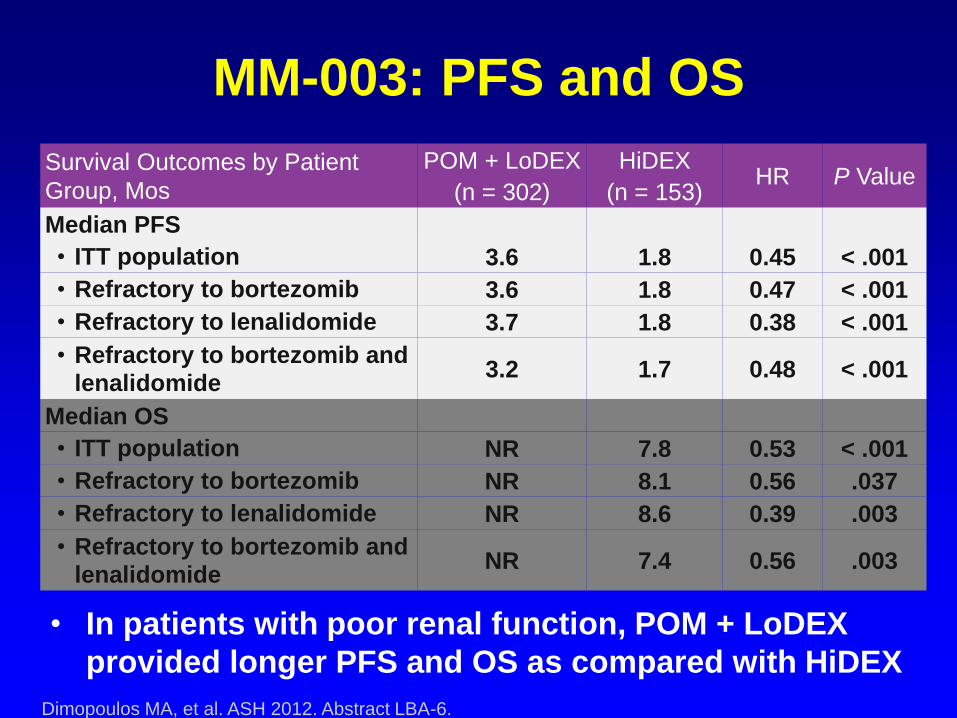
MM-003: PFS and OS
• In patients with poor renal function, POM + LoDEX
provided longer PFS and OS as compared with HiDEX
Dimopoulos MA, et al. ASH 2012. Abstract LBA-6.
Survival Outcomes by Patient
Group, Mos
POM + LoDEX
(n = 302)
HiDEX
(n = 153) HR P Value
Median PFS
• ITT population 3.6 1.8 0.45 < .001
• Refractory to bortezomib 3.6 1.8 0.47 < .001
• Refractory to lenalidomide 3.7 1.8 0.38 < .001
• Refractory to bortezomib and
lenalidomide 3.2 1.7 0.48 < .001
Median OS
• ITT population NR 7.8 0.53 < .001
• Refractory to bortezomib NR 8.1 0.56 .037
• Refractory to lenalidomide NR 8.6 0.39 .003
• Refractory to bortezomib and
lenalidomide NR 7.4 0.56 .003
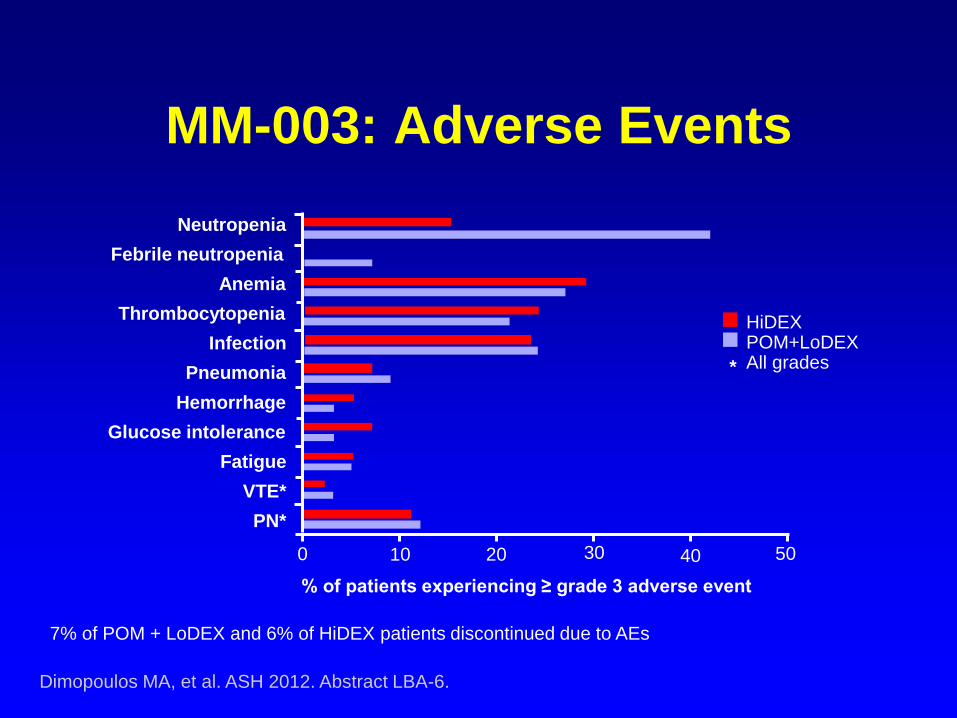
MM-003: Adverse Events
7% of POM + LoDEX and 6% of HiDEX patients discontinued due to AEs
Dimopoulos MA, et al. ASH 2012. Abstract LBA-6.
HiDEX POM+LoDEX All grades
% of patients experiencing ≥ grade 3 adverse event
Neutropenia
Febrile neutropenia
Anemia
Thrombocytopenia
Infection
Pneumonia
Hemorrhage
Glucose intolerance
Fatigue
VTE*
PN*
*
0 10 20 30 40 50

MM-005: A Phase I trial of Pom + Bortezomib +
Low-Dose Dexamethasone (PVD) in RR MM
• Objectives: Primary: MTD; Secondary: Safety,
response, OS, TTR, DOR
• Patients: 22 patients with RR MM; median age 57 yrs
(36-75); median 2 lines prior therapy (1-4); lenalidomide-
refractory; not refractory to bortezomib; no Gr ≥2 PN
• Dose and Schedule: 21-day cycles of bortezomib IV 1-1.3
mg/m2 days 1, 4, 8, and 11 (days 1 and 8 for cycles 9+),
pomalidomide (POM) 1-4 mg/day days 1-14, and low-
dose Dex 20 mg day of and after bortezomib (10 mg for
pts >75 yrs); thromboprophylaxis (aspirin or LMWH)
and antiviral prophylaxis required
Richardson PG et al. ASCO 2013., abstract # 8584
Relapsed/Refractory MM
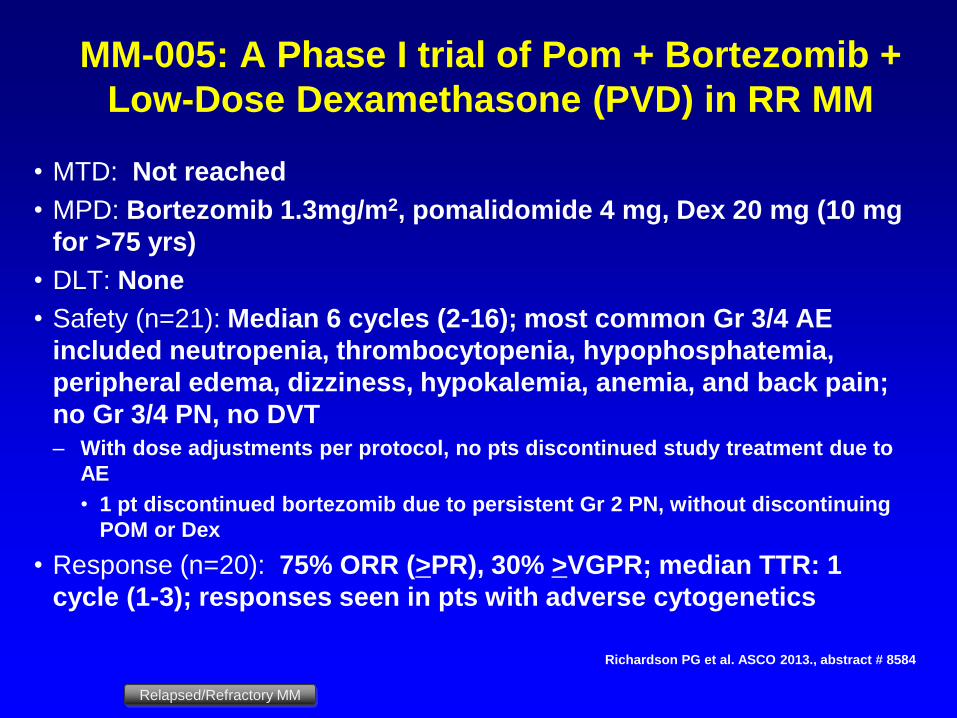
MM-005: A Phase I trial of Pom + Bortezomib +
Low-Dose Dexamethasone (PVD) in RR MM
• MTD: Not reached
• MPD: Bortezomib 1.3mg/m2, pomalidomide 4 mg, Dex 20 mg (10 mg
for >75 yrs)
• DLT: None
• Safety (n=21): Median 6 cycles (2-16); most common Gr 3/4 AE
included neutropenia, thrombocytopenia, hypophosphatemia,
peripheral edema, dizziness, hypokalemia, anemia, and back pain;
no Gr 3/4 PN, no DVT
– With dose adjustments per protocol, no pts discontinued study treatment due to
AE
• 1 pt discontinued bortezomib due to persistent Gr 2 PN, without discontinuing
POM or Dex
• Response (n=20): 75% ORR (>PR), 30% >VGPR; median TTR: 1
cycle (1-3); responses seen in pts with adverse cytogenetics
Richardson PG et al. ASCO 2013., abstract # 8584
Relapsed/Refractory MM
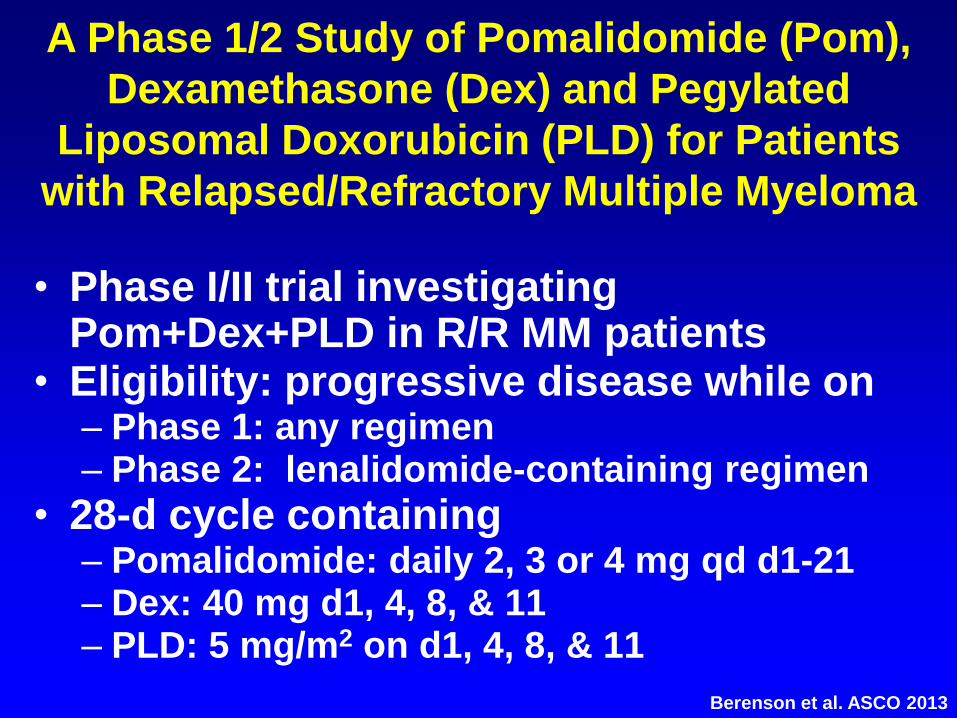
• Phase I/II trial investigating Pom+Dex+PLD in R/R MM patients
• Eligibility: progressive disease while on – Phase 1: any regimen – Phase 2: lenalidomide-containing regimen
• 28-d cycle containing – Pomalidomide: daily 2, 3 or 4 mg qd d1-21 – Dex: 40 mg d1, 4, 8, & 11 – PLD: 5 mg/m2 on d1, 4, 8, & 11
A Phase 1/2 Study of Pomalidomide (Pom),
Dexamethasone (Dex) and Pegylated
Liposomal Doxorubicin (PLD) for Patients
with Relapsed/Refractory Multiple Myeloma
Berenson et al. ASCO 2013
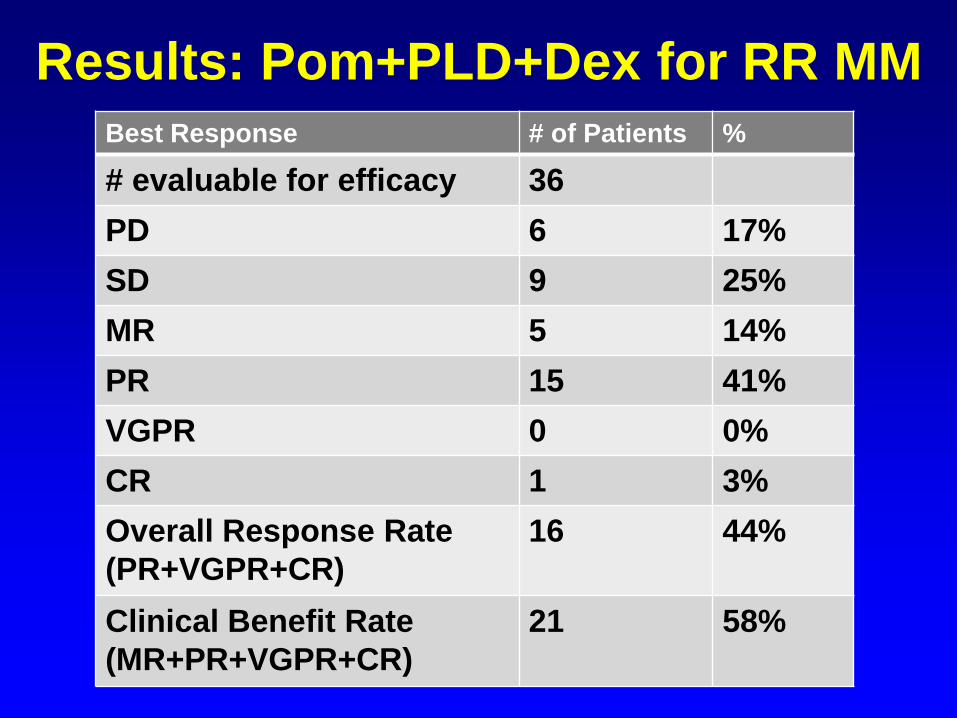
Best Response # of Patients %
# evaluable for efficacy 36
PD 6 17%
SD 9 25%
MR 5 14%
PR 15 41%
VGPR 0 0%
CR 1 3%
Overall Response Rate
(PR+VGPR+CR)
16 44%
Clinical Benefit Rate
(MR+PR+VGPR+CR)
21 58%
Results: Pom+PLD+Dex for RR MM
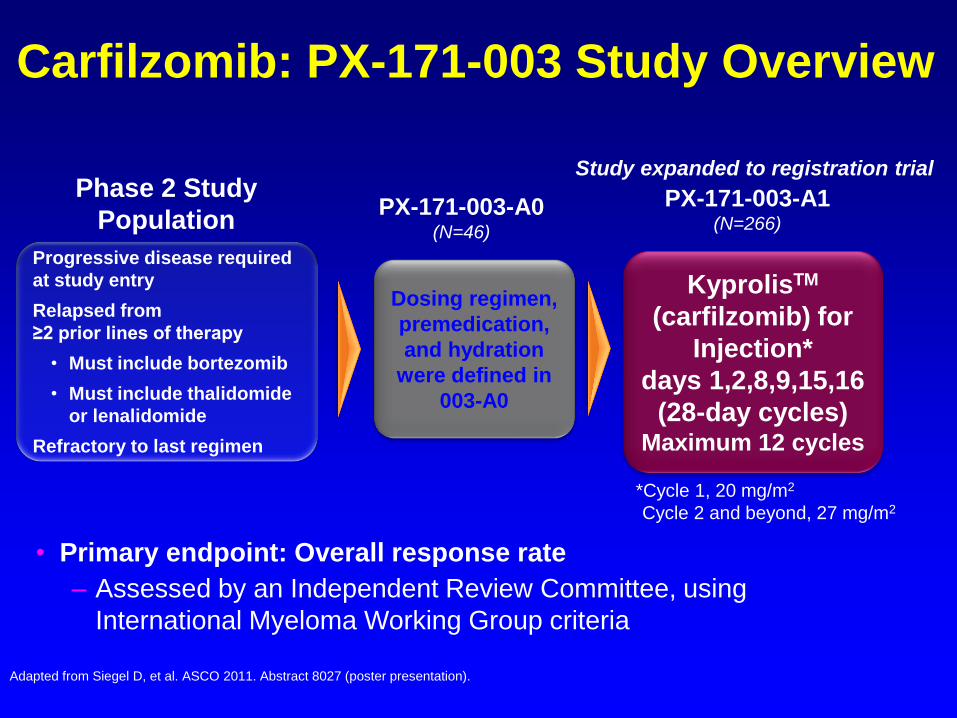
PX-171-003-A0 (N=46)
PX-171-003-A1 (N=266)
Phase 2 Study
Population
Dosing regimen,
premedication,
and hydration
were defined in
003-A0
KyprolisTM
(carfilzomib) for
Injection*
days 1,2,8,9,15,16
(28-day cycles) Maximum 12 cycles
Progressive disease required
at study entry
Relapsed from
≥2 prior lines of therapy
• Must include bortezomib
• Must include thalidomide
or lenalidomide
Refractory to last regimen
Carfilzomib: PX-171-003 Study Overview
Study expanded to registration trial
• Primary endpoint: Overall response rate
– Assessed by an Independent Review Committee, using
International Myeloma Working Group criteria
*Cycle 1, 20 mg/m2
Cycle 2 and beyond, 27 mg/m2
Adapted from Siegel D, et al. ASCO 2011. Abstract 8027 (poster presentation).

PX-171-003-A1: Response
N=266
Response rates*
Overall response rate (ORR)
Complete response
Very good partial response
Partial response
61 (22.9%)
1 (0.4%)
13 (4.9%)
47 (17.7%)
Median duration of response
(95% CI)
7.8 months
(5.6-9.2)
*As assessed by the Independent Response Review Committee

Carfilzomib Monotherapy MM Patients With 1-3 Prior Therapies
Bortezomib-Treated Cohort 1 (20 mg/m2 Carfilzomib)
n = 34
ORR 21%
CBR (> MR) 33%
Median TTP 8.1 months
Median DOR (> PR) 11.5 months
Stewart K, et al. Hematologica. 2010;95(S2). Abstract 1099. Vij R, et al. ASH Annual Meeting Abstracts.
2011;118(21):813.
Bortezomib-naïve
Cohort 1 (20 mg/m2)
n = 59
Cohort 2 (20→27 mg/m2)
n = 70
ORR 42% 52%
CBR 59% 64%
CR 3% 2%
VGPR 14% 27%
Median TTP 8.3 mo Not reached
Median DOR 13.1 mo Not reached
Median PFS 8.2 mo Not reached
• Nontraditional intrapatient Phase I/II trial • Eligibility: Progressive disease while on
bortezomib or relapsed within 12 wks of the last dose of bortezomib in a combination regimen
• Carfilzomib replaces bortezomib in combination with: – Alkylating agent – Anthracycline – Glucocorticosteroid – IMiD
A Phase I/II Study of Carfilzomib as a Replacement
for Bortezomib for Multiple Myeloma Patients Failing
Bortezomib-Containing Regimens

Study Design (cont’d)
• Study treatment – Carfilzomib
• starting at 20 mg/m2 for the 1st cycle
• increased to 27, 36 and 45 mg/m2 during cycles 2, 3 and 4, respectively if no DLT is observed
– DLT considered > Grade 2
• administered on days 1, 2, 8, 9, 15, and 16 of each 28-day cycle
– Cycle length, schedule(s) and dose(s) of other drugs identical to that of the previous bortezomib-containing regimen
• A patient must complete a minimum of a full cycle without DLT before continuing onto a subsequent cycle (cycles 1-4 only)
• Maximum # of cycles- 8

Results
Demographics
Enrolled (N) 38
Efficacy (N) 37
Age (median) 67
Sex (M:F) 25:13
Prior Regimens
Number of prior
regimens-
median (range)
6 (1-23)
Number of prior
bortezomib-
containing
regimens-
median (range)
2 (1-13)
Regimen Details
Cycle
length
8 pts- 21-day
24 pts- 28-day
Cycles
completed,
median
(range)
3
(range 0-12)
Follow-up
median
(range)
5.9 mo
(0.4-14.4 mo)
Number of
DLTs
8 (25%)
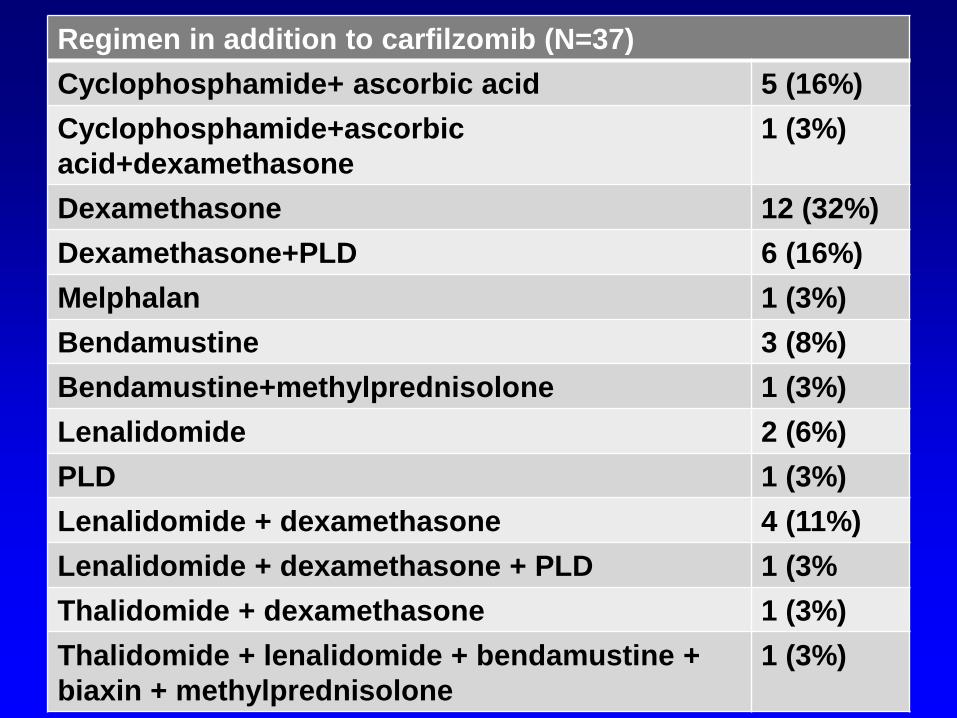
Regimen in addition to carfilzomib (N=37)
Cyclophosphamide+ ascorbic acid 5 (16%)
Cyclophosphamide+ascorbic
acid+dexamethasone
1 (3%)
Dexamethasone 12 (32%)
Dexamethasone+PLD 6 (16%)
Melphalan 1 (3%)
Bendamustine 3 (8%)
Bendamustine+methylprednisolone 1 (3%)
Lenalidomide 2 (6%)
PLD 1 (3%)
Lenalidomide + dexamethasone 4 (11%)
Lenalidomide + dexamethasone + PLD 1 (3%
Thalidomide + dexamethasone 1 (3%)
Thalidomide + lenalidomide + bendamustine +
biaxin + methylprednisolone
1 (3%)
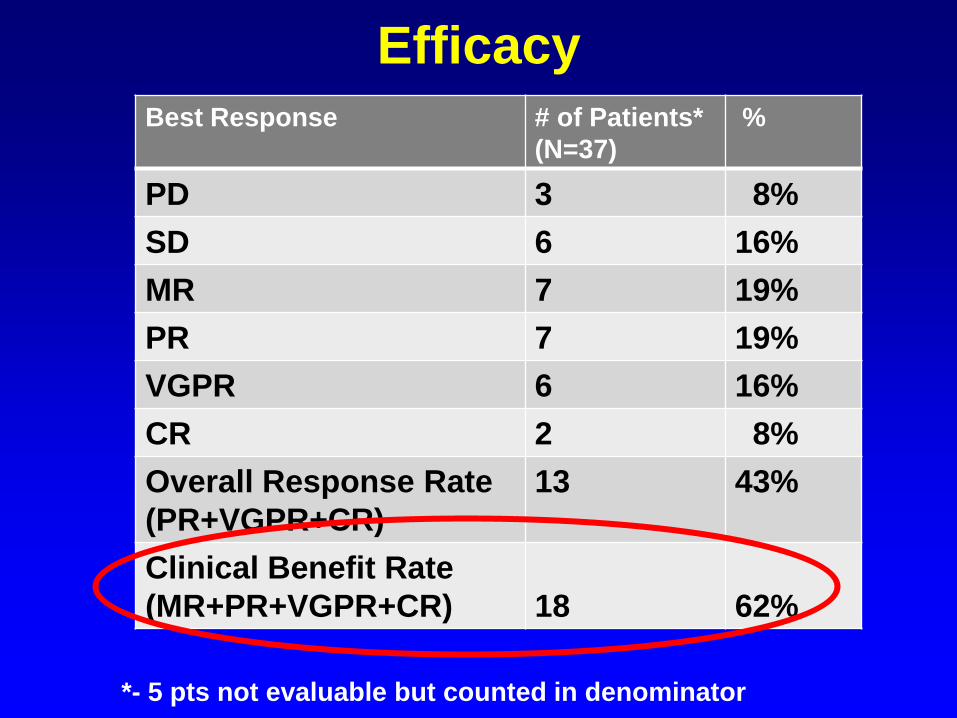
Best Response # of Patients*
(N=37)
%
PD 3 8%
SD 6 16%
MR 7 19%
PR 7 19%
VGPR 6 16%
CR 2 8%
Overall Response Rate
(PR+VGPR+CR)
13 43%
Clinical Benefit Rate
(MR+PR+VGPR+CR)
18
62%
Efficacy
*- 5 pts not evaluable but counted in denominator
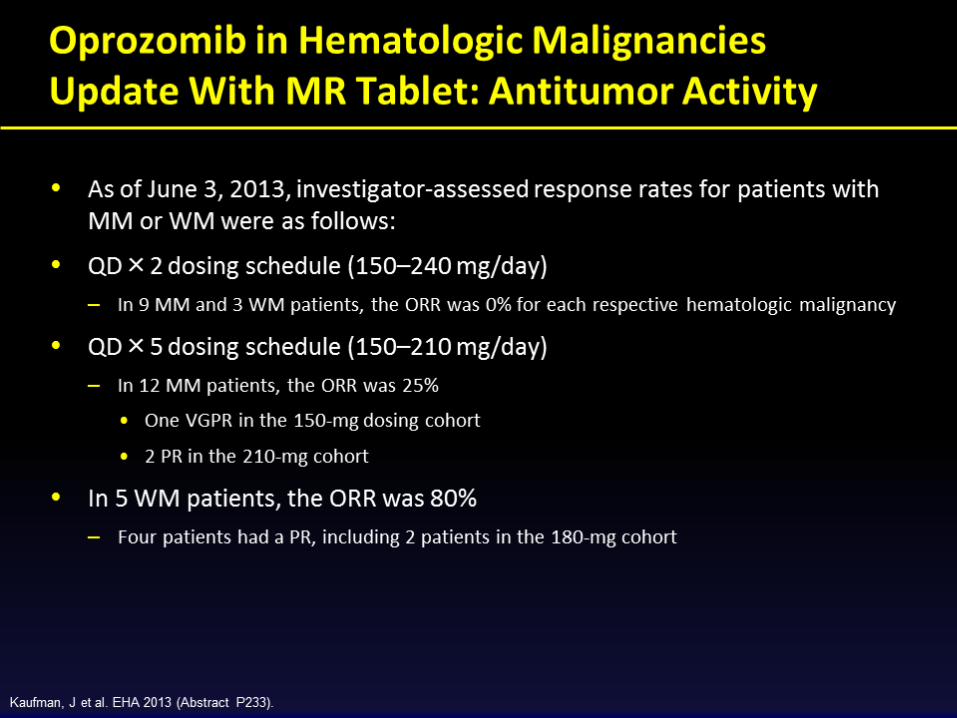
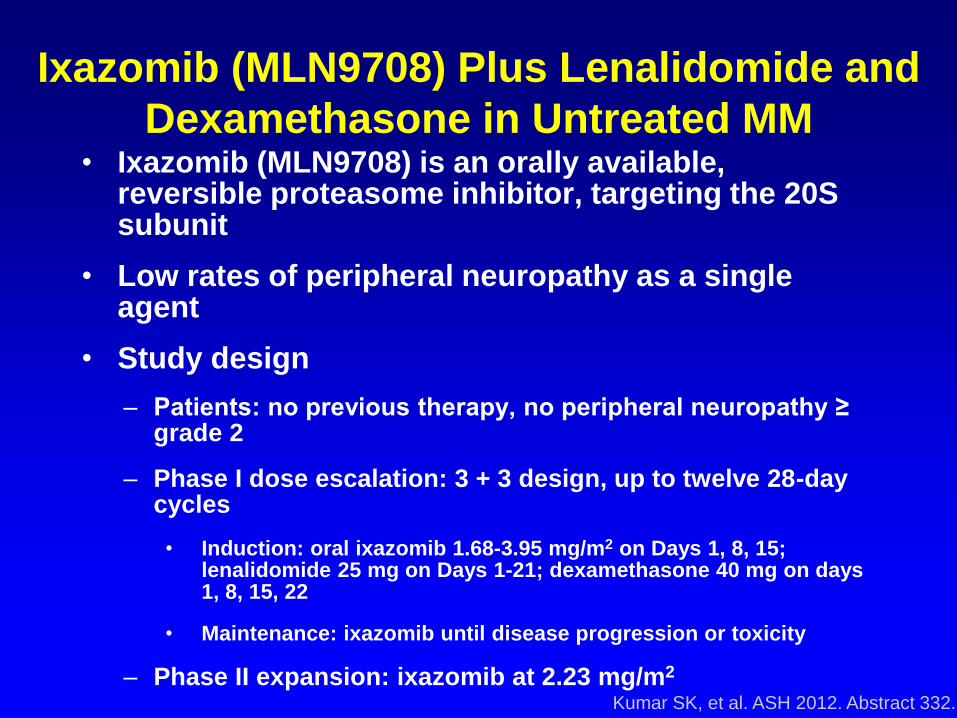
Ixazomib (MLN9708) Plus Lenalidomide and
Dexamethasone in Untreated MM • Ixazomib (MLN9708) is an orally available,
reversible proteasome inhibitor, targeting the 20S subunit
• Low rates of peripheral neuropathy as a single agent
• Study design
– Patients: no previous therapy, no peripheral neuropathy ≥ grade 2
– Phase I dose escalation: 3 + 3 design, up to twelve 28-day cycles
• Induction: oral ixazomib 1.68-3.95 mg/m2 on Days 1, 8, 15; lenalidomide 25 mg on Days 1-21; dexamethasone 40 mg on days 1, 8, 15, 22
• Maintenance: ixazomib until disease progression or toxicity
– Phase II expansion: ixazomib at 2.23 mg/m2
Kumar SK, et al. ASH 2012. Abstract 332.

Ixazomib + Lenalidomide/Dexamethasone
Responses and Efficacy
Kumar SK, et al. ASH 2012. Abstract 332.
Ixazomib at 2.23 mg/m2
Pati
en
ts (
%)
≥ VGPR 58%
≥ VGPR 49% ≥ VGPR
58%
ORR 94% ORR 95% ORR 90%
Estimated probability of survival at 1 yr: 93%
CR
VGPR
PR
100
90
80
70
60
50
40
30
20
10
0 After 4 Cycles
(n = 47) After 8 Cycles
(n = 19)
Overall (n = 52)
45
30
19
37
26
32
32
35
23
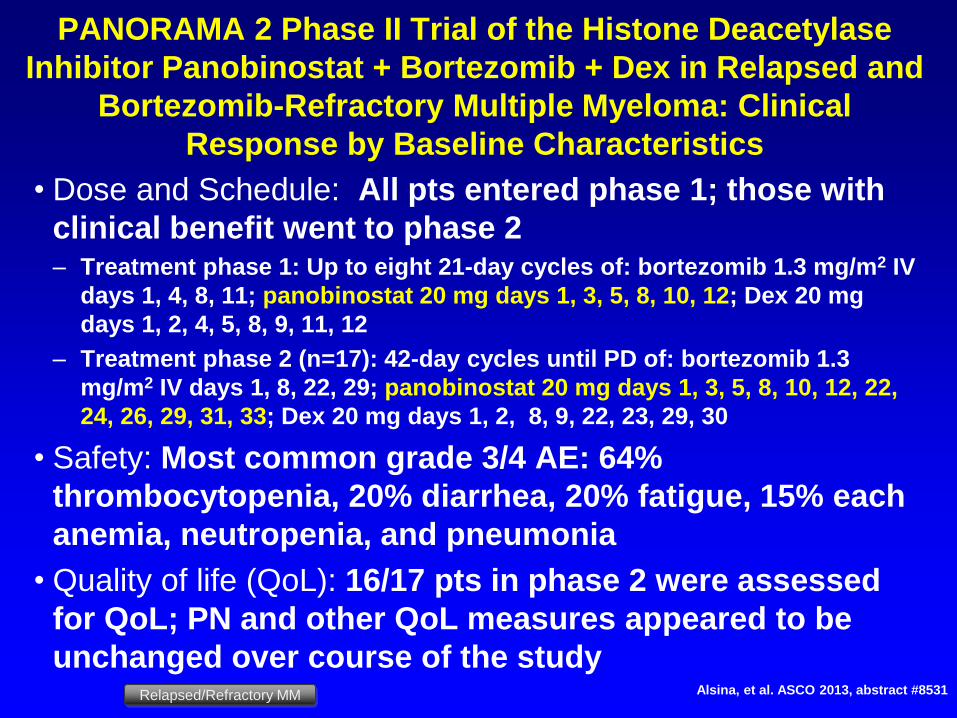
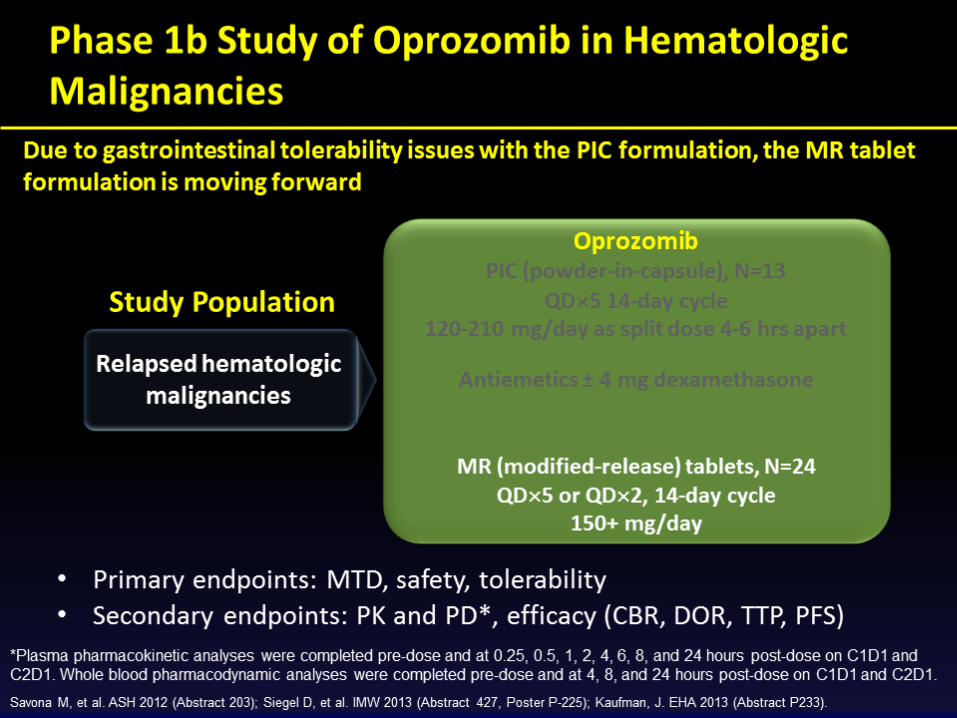
PANORAMA 2 Phase II Trial of the Histone Deacetylase
Inhibitor Panobinostat + Bortezomib + Dex in Relapsed and
Bortezomib-Refractory Multiple Myeloma: Clinical
Response by Baseline Characteristics
• Dose and Schedule: All pts entered phase 1; those with
clinical benefit went to phase 2 – Treatment phase 1: Up to eight 21-day cycles of: bortezomib 1.3 mg/m2 IV
days 1, 4, 8, 11; panobinostat 20 mg days 1, 3, 5, 8, 10, 12; Dex 20 mg
days 1, 2, 4, 5, 8, 9, 11, 12
– Treatment phase 2 (n=17): 42-day cycles until PD of: bortezomib 1.3
mg/m2 IV days 1, 8, 22, 29; panobinostat 20 mg days 1, 3, 5, 8, 10, 12, 22,
24, 26, 29, 31, 33; Dex 20 mg days 1, 2, 8, 9, 22, 23, 29, 30
• Safety: Most common grade 3/4 AE: 64%
thrombocytopenia, 20% diarrhea, 20% fatigue, 15% each
anemia, neutropenia, and pneumonia
• Quality of life (QoL): 16/17 pts in phase 2 were assessed
for QoL; PN and other QoL measures appeared to be
unchanged over course of the study Alsina, et al. ASCO 2013, abstract #8531 Relapsed/Refractory MM
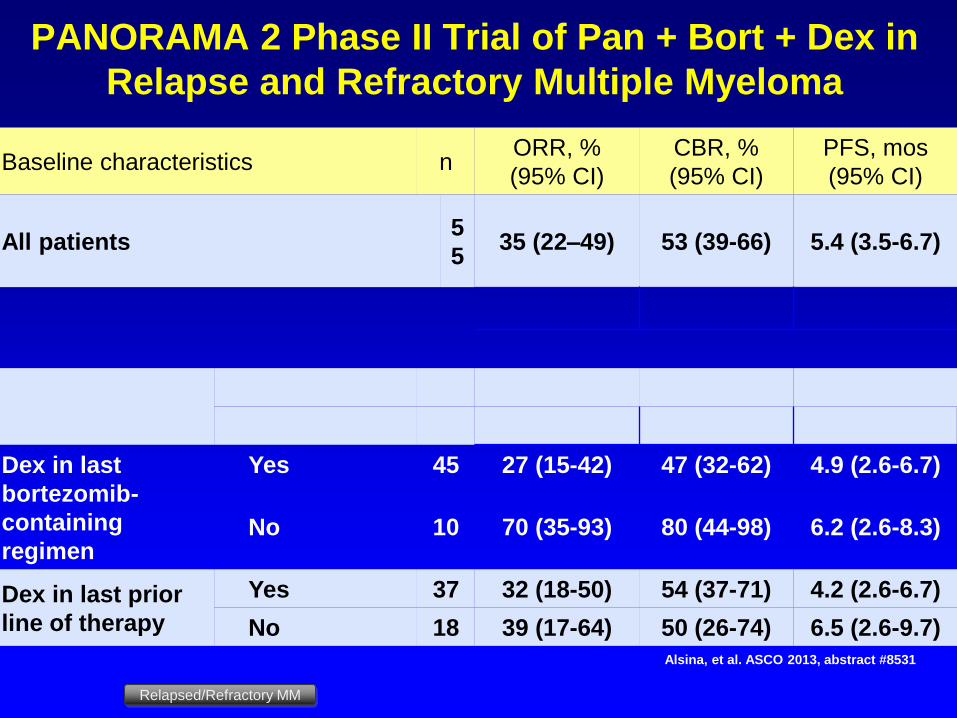
PANORAMA 2 Phase II Trial of Pan + Bort + Dex in
Relapse and Refractory Multiple Myeloma
Alsina, et al. ASCO 2013, abstract #8531
Relapsed/Refractory MM
Baseline characteristics n ORR, %
(95% CI)
CBR, %
(95% CI)
PFS, mos
(95% CI)
All patients 5
5 35 (22–49) 53 (39-66) 5.4 (3.5-6.7)
Dex in last
bortezomib-
containing
regimen
Yes 45 27 (15-42) 47 (32-62) 4.9 (2.6-6.7)
No 10 70 (35-93) 80 (44-98) 6.2 (2.6-8.3)
Dex in last prior
line of therapy
Yes 37 32 (18-50) 54 (37-71) 4.2 (2.6-6.7)
No 18 39 (17-64) 50 (26-74) 6.5 (2.6-9.7)
Anti-CS-1 Antibody Elotuzumab and Bortezomib for R/R MM: A Phase I Trial
Jakubowiak AJ et al. ASH 2010, abs #3023
•Objectives: Primary: MTD; Secondary: safety, efficacy, elotuzumab PK/PD
•Patients: 28 pts; median age 63 (41–77); median 2 (1–3) prior therapies; 39% prior bortezomib; 43% refractory to last treatment, 14% refractory to bortezomib
•Dose: 21-day cycles of bortezomib 1.3 mg/m2 on days 1, 4, 8, and 11; elotuzumab 2.5, 5, 10, or 20 mg/kg on days 1 and 11; premed w/ methylprednisolone 50 mg, diphenhydramine and acetaminophen; pts with ≥SD after 4 cycles continued therapy until progression; Dex 20 mg on days 1, 2, 4, 5, 8, 9, 11, and 12 added at cycle 3 in 2 pts
Jakubowiak AJ et al. J Clin Oncol 2012
Elotuzumab and Bortezomib for R/R MM: Results
•MTD: Not reached at doses up to elotuzumab at 20 mg/kg with bortezomib 1.3 mg/m2 d1, 4, 8, & 11 on a 21-day cycle
DLT: None observed
•ORR (> PR): 48%* (7% CR; 41% PR)
•MR: 15%
•CBR: 63%
•Median TTP: 9.5 mo
Jakubowiak AJ et al. J Clin Oncol 2012
*however, only 39% previously exposed to
bortezomib and only 11% refractory to bortezomib

Elotuzumab (E), Lenalidomide (L) & Dexamethasone (D) for R/R MM: A Phase I Trial
Jakubowiak AJ et al. ASH 2010, abs #3023
Objectives: Primary: MTD; Secondary: safety, efficacy, immunogenicity, pharmacokinetics, & pharmacodynamics
•Patients: 29 pts; median age 60 (40–83); median 3 (1–10) prior therapies: L 21%, bortezomib 69%, thalidomide 59%; 41% refractory to last treatment, ? refractory to L
•Dose: 28-day cycles of E at 5, 10, or 20 mg/kg on days 1, 8, 15, & 22 during cycles 1 & 2 and days 1 & 15 subsequently (steroids & diphenhydramine allowed); L 25 mg qd d1-21; D 40 mg qwk
Lonial et al. J Clin Oncol 2012

Elotuzumab (E), Lenalidomide (L) &
Dexamethasone (D) for R/R MM: Results
•MTD: Not reached at doses up to E at 20 mg/kg with L 25 mg, and D 40 mg
•DLT: None observed
•89% infusion reactions
•ORR (> PR): 82% (32% > VGPR; 50% PR)
• 95% ORR among lenalidomide-naïve pts
• However, only 33% ORR among lenalidomide-exposed pts
•Median TTP: Not reported
Jakubowiak AJ et al. J Clin Oncol 2012

Novel Combinations and New Drugs Greatly Expand
the Therapeutic Options for R/R Myeloma Patients!
• Approved drugs – Novel combinations
– Modifications of dose and schedule
• Improve efficacy
• Better tolerability
• Many new drugs in development – Similar targets
• Proteasome inhibitors- carfilzomib- FDA-approved
• IMiDs- pomalidomide- FDA-approved
– New classes of agents
• Monoclonal antibodies
– Anti-CS-1- elotuzumab
– Anti-CD40- dacetuzumab
• MTOR inhibitors- temsirolimus
• PI3K inhibitors- perifosine
• HDAC inhibitors- vorinostat, panobinostat
• Antibody-based conjugates