Embed Size (px)
Citation preview

New breast cancer classification: traditional pathology and
molecular subtypes
Dr. PN Mainwaring
Centre for Personalised
NanoMedicine
AIBN@UQ

Disclosures
Lectures, Honoraria, Advisory Boards
- Astellas–, BMS, Gelgene, Ipsen, Janssen, Medivation, Merck, Novartis, Pfizer, Roche/Genentech

Outline
• Traditional Pathology• Haematoxylin & Eosin• Descriptors; Scarff Bloom Richardson• Proliferation & Apoptosis• Protein IHC classification• Immune context
• Molecular Subtypes• DNA classification• Epigenetic classification• RNA classification
• Integration
Aim
Classification
Prognosis
Prediction
Monitoring
?Screening/Early detection

Baselga and Norton, 2002 updated
Evolution in Breast Cancer Classification
Classical Diagnosis
Ductal infiltrating carcinoma of breast with
high grade of nuclear atypia
Protein Expression
ErbB2 over expressing breast tumour
Gene Expression Profiling
Partial two dimensional cluster analysis of17 breast tumours
MorphologicalDiagnosis
Immunohistochemicalassessment
DNA microarrayanalysis
CIRCOS Plot
Integrated Analysis
Chromosome, SNV,LSV, indel, amplification
miRNA, RNA

AJCC 8th Edition: 1st January 2018
• Combining T/N/M with biology grade,proliferation, ER/PgR/HER2/GEP• NB GEP only apply to LN negative disease; T1a-bN0M0
• OncotypeDx, Mammaprint, EndoPredict, PAM50, Breast Cancer Index
Giuliano Breast Feb 2018

Histology - T

H&E
Neoadjuvant Biopsy Surgical Specimen

Nucleoli reflect chromatincondensation

Differentiation
Well-differentiated Poorly-differentiated

Lymphovascular invasion
Anti-vascular antibodyCD34

Proliferation & Apoptosis
• MIB-1
• Antibody to Ki67• Protein expressed variably through
cell cycle not G0
• Apoptosis
• One form of cell death
International Ki67 in Breast Cancer Working Group

Immune Context
Angiogenesis; CD34 Tumour-infiltrating lymphocytes; PD-1
Salgado Adv Anat Pathol. 2017
Intra-tumourStromal
ImmuneInfiltrateSub-typing

Special subtypes
Tubular Metaplastic

Biology – Standard Immunohistochemistry & RPPA

ER; cutoff <1% vs <10%ER-negative ER-negative; positive GATA3ER-positive
Lobular
E-cadherin

PR
• Cytoplasmic
Carroll NRC 2016

HER2
HER2
0 1 2 3
FISH
Normal Amplified

Basal
Cytokeratin 5/6 (CK 5/6) EGFR
R
Histology - N

Nodal Metastasis
Micrometastasis
Extracapsular spread
Isolated Tumour Cells

One-step CK19 mRNA Amplification
Osako BJC 2017

Molecular Classification

TCGAIGCG
Weinstein Nat Gen 2013
Now 5 years onFrom the initialpublications

Technologies
IlluminaSeq by Synth
LifeSeq by Synth
NanostringDigital PCR
BGIRolling Circle
PacBioSMART

DNA ClassificationTri NA Breast
Age 60%APOBEC 14%BRCA1/2 10%
?
APOBEC 2%
Point mutation SNV/SNA vs SNP; indel (30bp); amplif’n; LSV
Nik-Zainal Nature 2016

TCGA: Molecular characteristics of TNBC provides fuel for future therapeutics
Basal-like Breast Cancer
p53 mut 84% RB1 mut/loss 20%
PIK3CA mut 7% MYC focal gain 40%
PTEN loss 35% Global Hypomethylation
INPP4B loss 30% Aneuploidy and genomic instability
TCGA Nature 2012

Post-translationalHistones & tails
within the 25 genes most significantly altered among all tumour types, seven (28%) code for chromatin-modifying enzymes—KMT2C/MLL3, KMT2D/MLL2, ARID1A, PBRM1, SETD2, CREBBPand SMARCA4/BRG1 it is estimated that approximately 20% of all solid malignancies harbor mutations in at least one SWI/SNF componentincl ~20% breast cancer
Morel Annals 2017
CpG island

Slinky
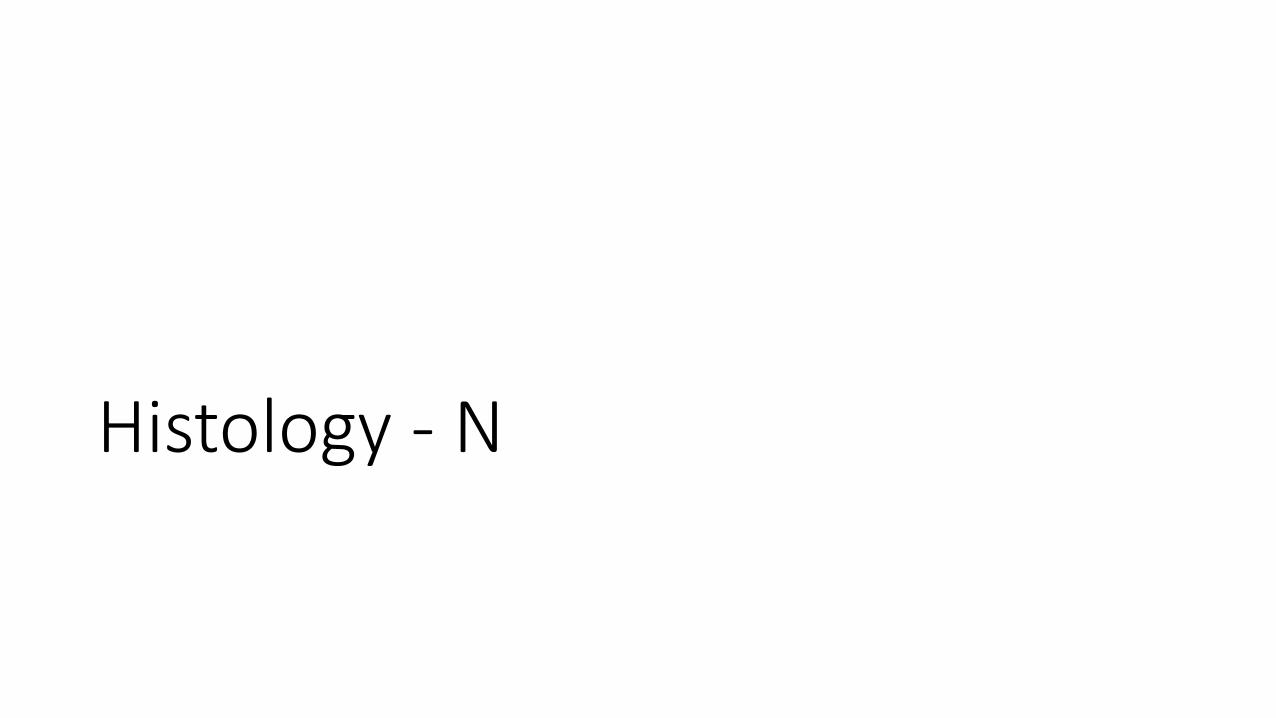
ER-pos enhancer regions methylation
Stone Nat Comm 2015

TNBC; Differential methylation
Stirzaker Nat Comm 2015
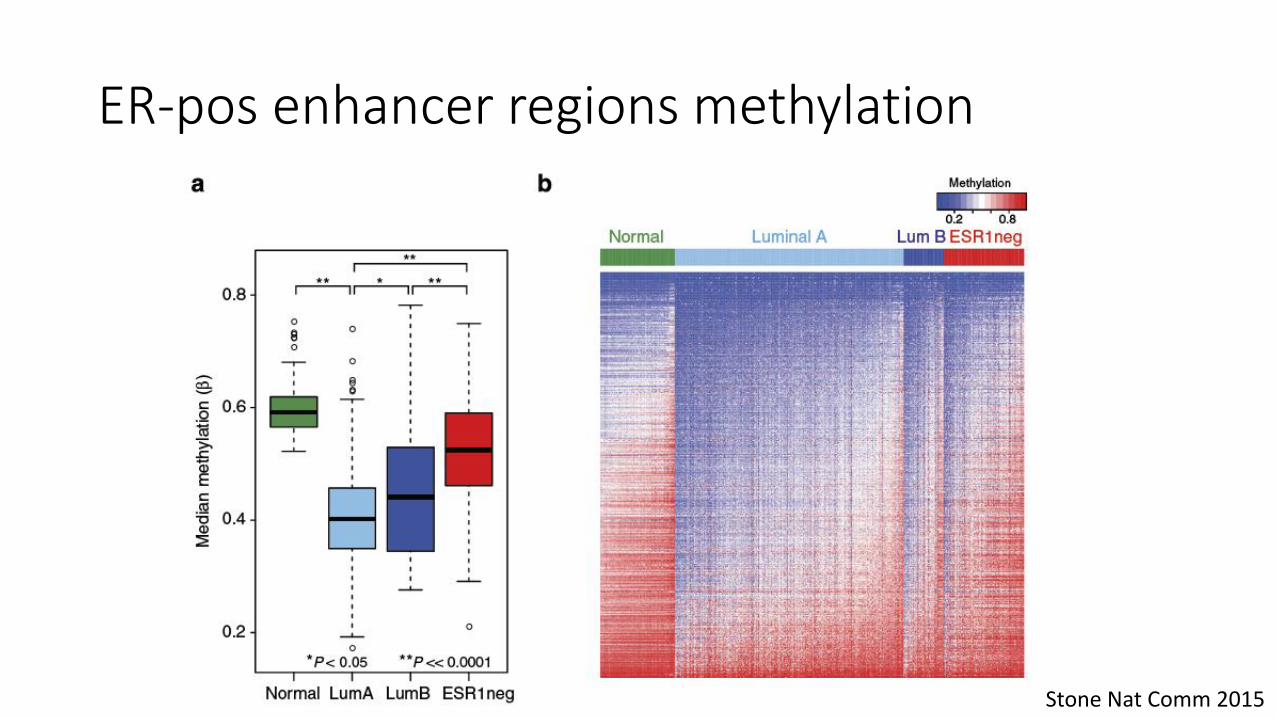
Epigenetic Classification
• miRNA
• lncRNA
• Others, sno/circ
• miRNA signatures
• lncRNA signatures• Prognostic
• Predictive
• Need large scale

RNA Editing
• Transcription
• Enhancers/Super-enhancers
• Splice Variants
• Fusion Genes

Perou Nature 200
Sørlie et al PNAS 2003
ER+
ER+
Original Microarray analyses
A vs BHeterogeneity
in Outcome

Increasing Complexity
Ali Genome Biol 2014
METABRIC

RNA Classification
Prat Mol Oncol 2015

Stratification of TNBC
TNBC
Luminal/AR Basal
Luminal A+B HER2-enriched Claudin-low/mesenchymal Basal-like
AR expressionLow – Immune – High
Gene expression or TILs
Chemo sensitivity
Lapatinib sensitivity
Chemo sensitivity
Proliferation
20–30% 70–80%
Perou SABCS 2016.

PI3K/Akt/mTOR inhibitors
Targeted RTK inhibitors
DNA-repair targeting agents
Cell cycle/mitotic spindle inhibitors
RAF/MEK inhibitors
Clinically targetable pathways in TNBC
~90% of all patients had an aberration in at least one of
these pathways
IMMUNOTHERAPEUTICSN
um
be
r o
f sa
mp
les
wit
h a
be
rrat
ion
s
PI3K/Akt/mTOR DNA repair Ras/MAPK Cell cycle GFRs0
10
20
30
40TSC1
PIK3CA
PTEN
PIK3R1
RICTORRAPTORAKT1AKT2
AKT3
BRCA1
BRCA2ATM
RB1
AURKA
CDNK2A
CCNE1
CCND3
CCND2
CCND1
CDK6CDK4
NF1CRAFBRAF
KRAS EGFR
MET
IGF1RKITFGFR1
FGFR2
FGFR4
Balko Cancer Discov 2014.

Protein
• Ultimate effector• capture the functional
state and dynamic properties of a cell
• Kinome• Phospho, other PTMs
• Membrane
• Cytoplasm
• Golgi etc
• Nuclear

TNBC – IHC; 133 biomarkers
• Stratify TNBC patients into high risk groups that showed over 5, 6, 7 and 8 times higher risk of developing metastasis to the bone, liver, lung and brain, respectively, than low-risk subgroups
KlimovBJC 2017


Metabolome
• Metabolic reprogramming inER-positive breast cancer
• Super-SILAC mix to quantifyover 10,000 proteins with high accuracy
Pozniak Cell 2016
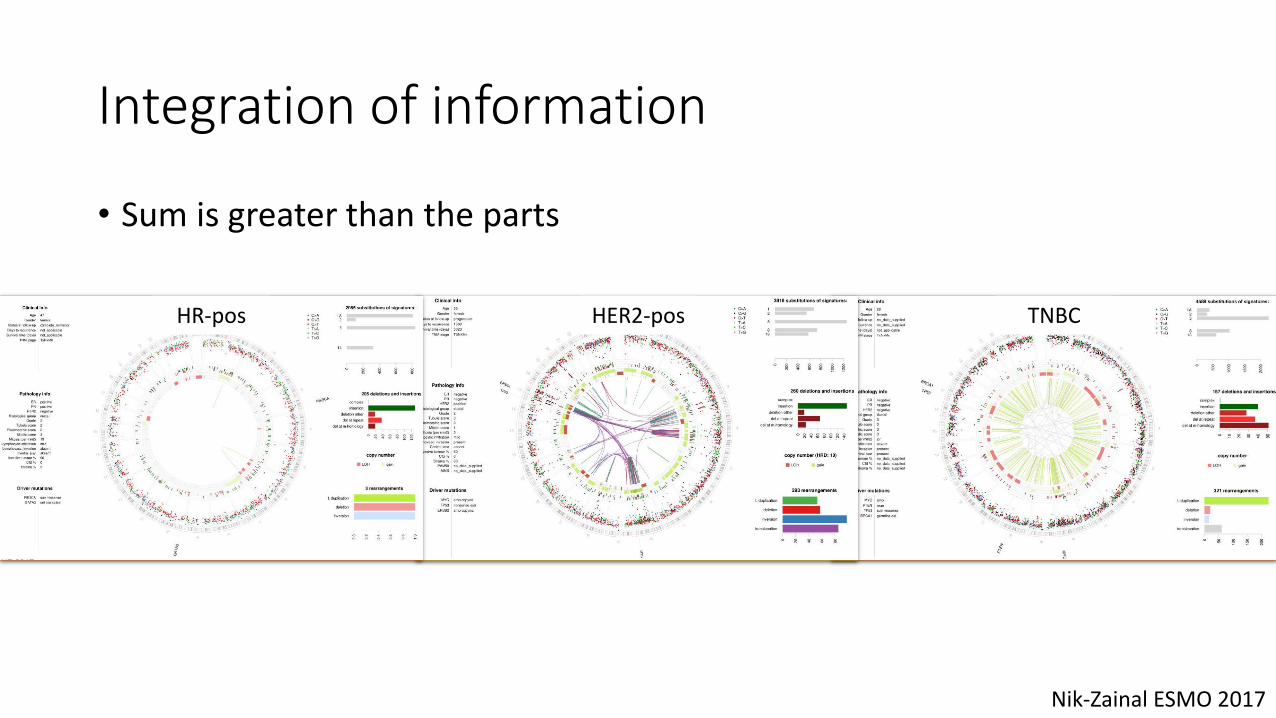
Integration of information
• Sum is greater than the parts
HR-pos HER2-pos TNBC
Nik-Zainal ESMO 2017

Triple Negative
Basal
Gluz et al, Ann Oncol 2009; Carey et al, Nat Rev Clin Oncol 2010;Young et al, BMC Cancer 2009; Schneider et al, CCR 2008; Shah et al, Nature 2012
~75% of TNBC have basal gene expression
• ~5% of breast cancers• ~75-80% of BRCA1 mutation-associated BC are TN• 50% BRCA1 carriers are basal-like
• Basal but not TN (15-40%)
• Definition by gene expression
• Express basal cytokeratins
• Includes most BRCA1 mutated tumours
• Triple negative but not basal (20-30%)
• Definition by IHC
• Includes non-IDC histologies
• 10-30% can also include “claudin-low”,a subtype notable for high expression of stem cell markers
• 90% of TNBC do not have BRCA mutations
BRCA1/2mutated
TNBC; integrating clinical & molecular

Immune-Context

Immune gene signature
Nagalla Genome Biol 2013

Mol.Subtype
PD-L1/PD-1 IHC expression; meta-analysis
• Grade, Tumour, Lymph Nodes, ER, PgR, HER2
Kim BMC 2017

Crosstalk between DDR and Immune System: TMB & Neoepitopes
Zehir A et al. Nat Med 2017.

Future is now; ? ESMO ?
• Multi-omic analysis
• Integration into biological pathways
• Application of systems biology to decide1. Major pathway drivers
2. Major nodal points
3. Druggable nodal points
4. Integrated systemic therapy
• Monitor ‘response’• cfDNA, CTC, exosomes, proteins
“N-of-One” vs Many;