Embed Size (px)
Citation preview
November-2017
Bret Bostwick, M.D.
“New Approaches to the Genetic Evaluation of Developmental Delay”
The following individuals have reported financial relationships with commercial interests (drug/device companies):
Bret Bostwick, M.D. receives funding support from BioMarin Pharmaceuticals Inc.
Bret Bostwick, M.D. is a consultant for Baylor Genetics
Bret Bostwick, M.D. is employed by the Department of Molecular and Human Genetics at Baylor College of Medicine, which derives revenue from Baylor Genetics

Introduction• Children with developmental delay are those who
present with delays in the attainment of developmental milestones at the expected age.
• Global developmental delay (GDD) is a subset of developmental disabilities defined as significant delay in two or more of the following developmental domains: – gross/fine motor– speech/language– cognition– social/personal– activities of daily living
Terminology• The term "developmental delay" is usually reserved for younger
children (typically younger than 5 years), and the term “intellectual disability" is usually applied to older children when IQ testing is valid and reliable
• Severity = functional age / chronological age.– Mild: 67-80 %ile– Moderate: 34-66 %ile; – Severe: 0-33 %ile
• “Significant” delay is defined as performance two standard deviations or more below the mean on age-appropriate, standardized norm-referenced testing.
• Person-first language: “child with developmental delay” instead of “delayed child”.
Prevalence
• Global developmental delay is estimated as 1% to 3%of children younger than 5.– Similar to prevalence of ID in the adult population.
• Approximately 40,000 to 120,000 children born each year in the United States and Canada will manifest developmental delays.
• Developmental disabilities, taken together, affect 5% to 10% of all children
"Developmental Surveillance and Screening of Infants and Young Children” AAP Committee on Children With Disabilities
• Early identification and referral of infants with DD by the primary care pediatrician
• The pediatrician's responsibility to "determine the cause of delays or refer to appropriate consultant for determination.”
• Developmental screening or surveillance identifies those who may need further evaluation and referral for services.
• Parent report instruments (Parents' Evaluation ofDevelopmental Status) or direct examination of the child's skills (Denver-II screening test, Bayley Infant Neurodevelopmental Screener)
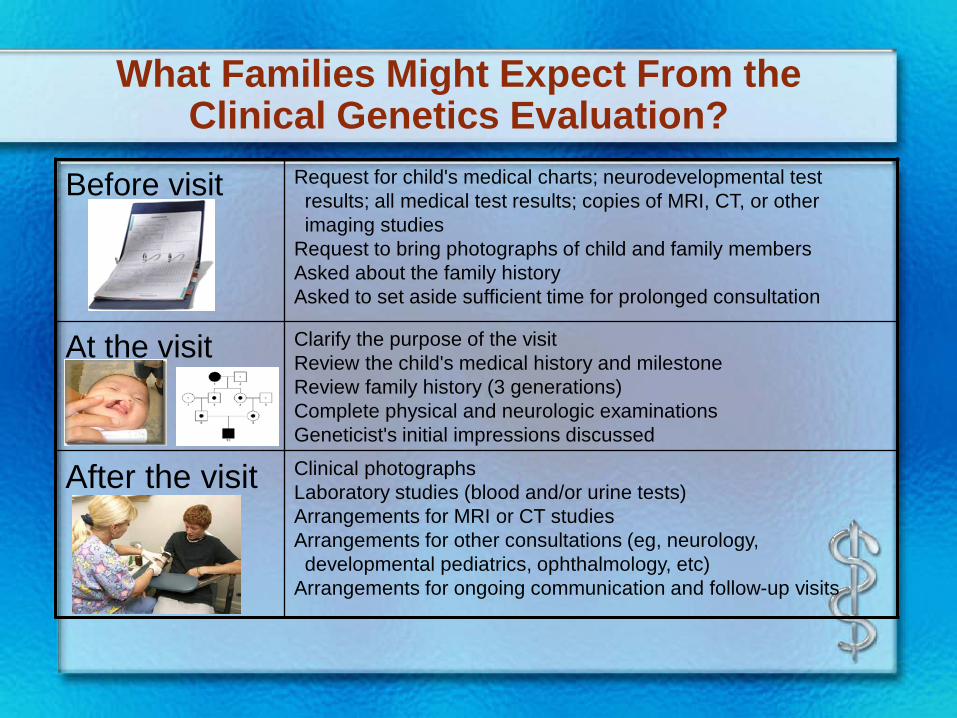
What Families Might Expect From the Clinical Genetics Evaluation?
Before visit Request for child's medical charts; neurodevelopmental test results; all medical test results; copies of MRI, CT, or other imaging studies
Request to bring photographs of child and family membersAsked about the family historyAsked to set aside sufficient time for prolonged consultation
At the visit Clarify the purpose of the visitReview the child's medical history and milestone Review family history (3 generations)Complete physical and neurologic examinationsGeneticist's initial impressions discussed
After the visit Clinical photographsLaboratory studies (blood and/or urine tests)Arrangements for MRI or CT studiesArrangements for other consultations (eg, neurology, developmental pediatrics, ophthalmology, etc)
Arrangements for ongoing communication and follow-up visits
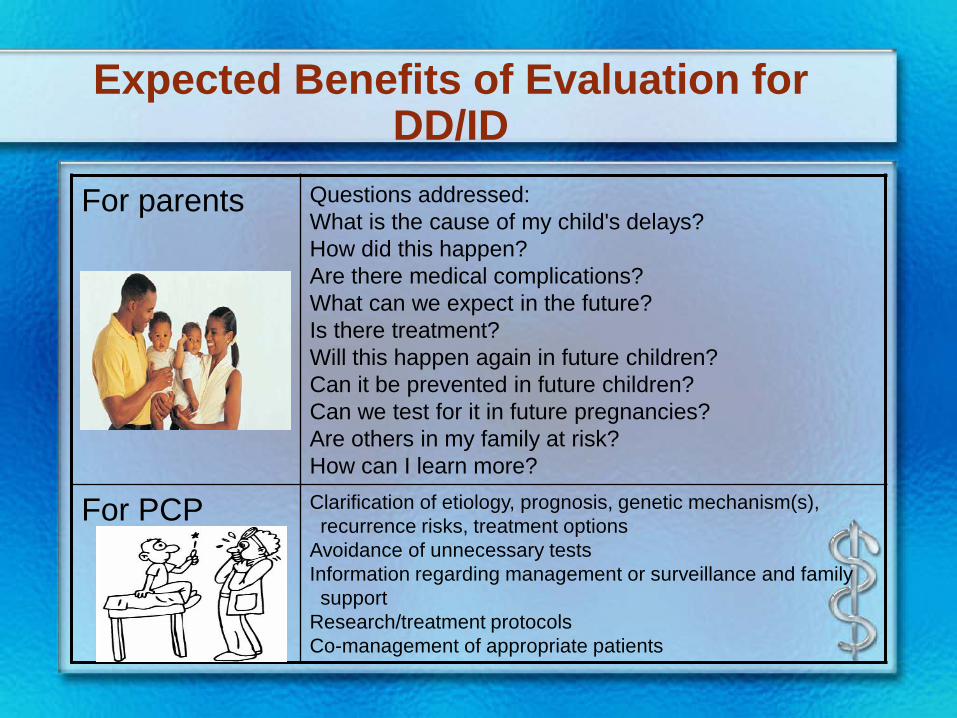
Expected Benefits of Evaluation for DD/ID
For parents Questions addressed:What is the cause of my child's delays? How did this happen? Are there medical complications? What can we expect in the future? Is there treatment? Will this happen again in future children? Can it be prevented in future children?Can we test for it in future pregnancies?Are others in my family at risk?How can I learn more?
For PCP Clarification of etiology, prognosis, genetic mechanism(s), recurrence risks, treatment options
Avoidance of unnecessary testsInformation regarding management or surveillance and family support
Research/treatment protocolsCo-management of appropriate patients
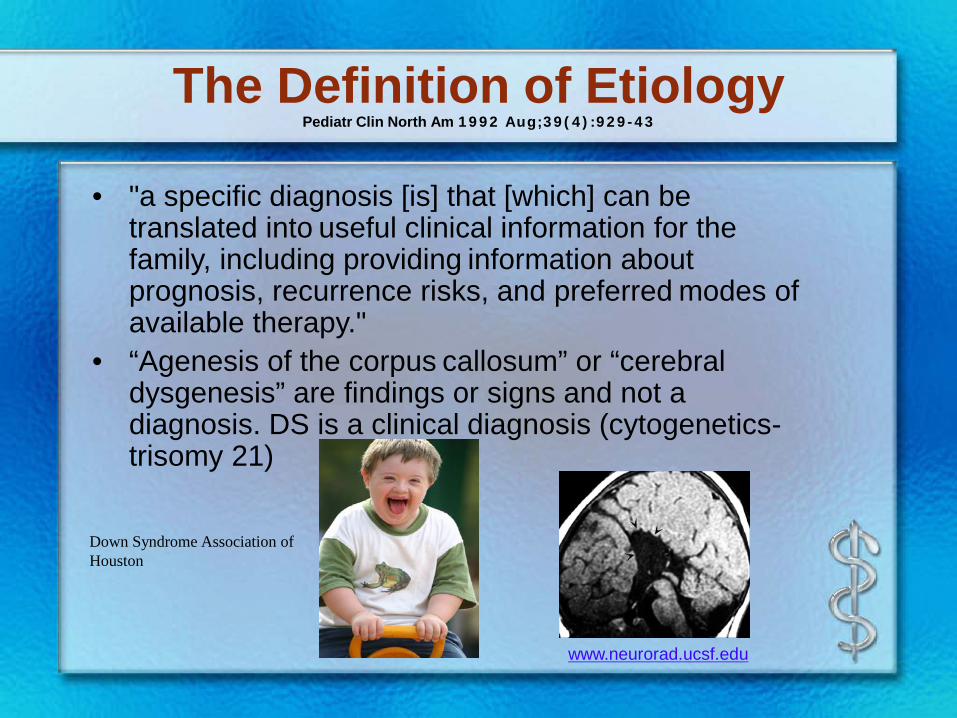
The Definition of EtiologyPediatr Clin North Am 1992 Aug;39(4):929-43
• "a specific diagnosis [is] that [which] can be translated into useful clinical information for the family, including providing information about prognosis, recurrence risks, and preferred modes of available therapy."
• “Agenesis of the corpus callosum” or “cerebral dysgenesis” are findings or signs and not a diagnosis. DS is a clinical diagnosis (cytogenetics-trisomy 21)
Down Syndrome Association of Houston
www.neurorad.ucsf.edu
The Yield of Etiologic Evaluation
• Vary widely (10% to 81%).
• 18% to 47% have detectable genetic causes
• Factors: study population differences, extent of evaluation, era during which the study was completed, and improving diagnostic technologic advances over time.
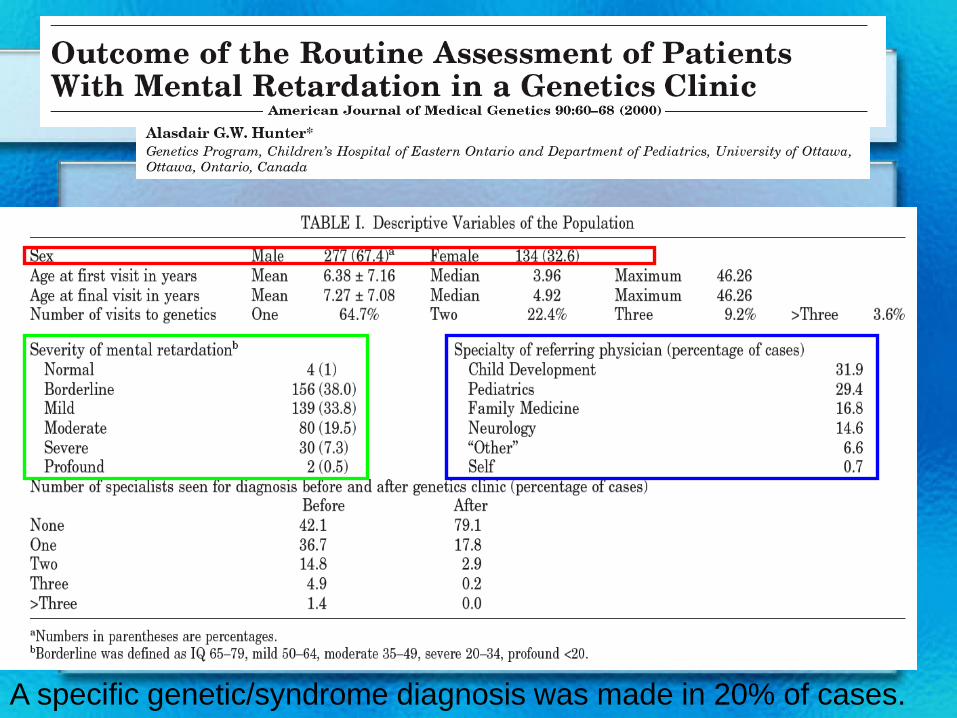
A specific genetic/syndrome diagnosis was made in 20% of cases.
European Journal of Human Genetics(2006) 14, 1082-1089.
Dysmorphology exam by an experienced clinical geneticist remains a key element of the diagnostic evaluation.
The Dysmorphology Examination
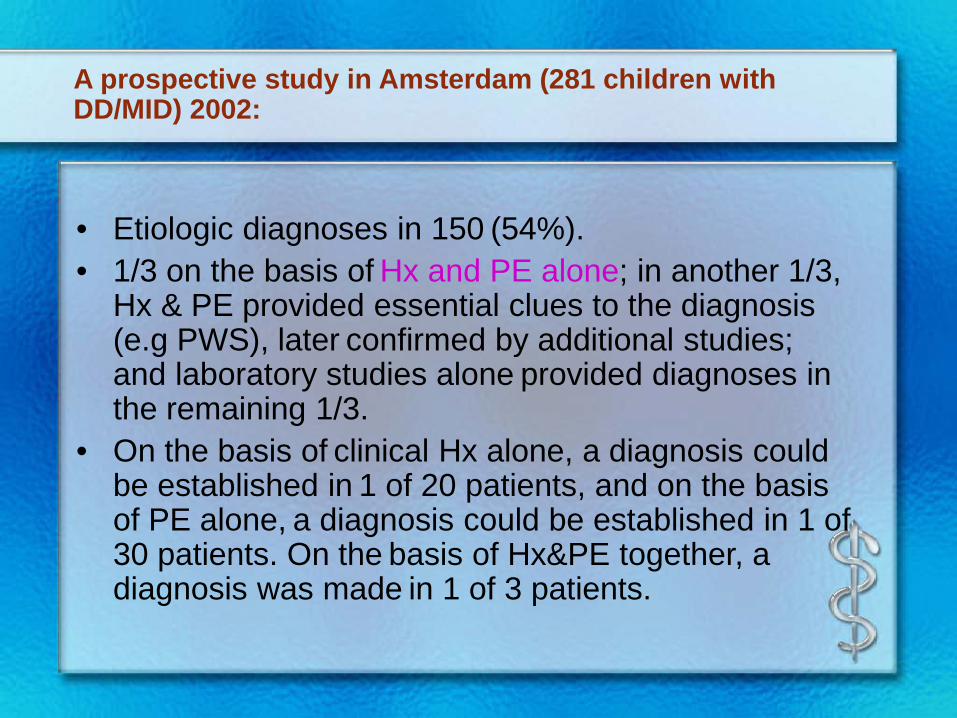
A prospective study in Amsterdam (281 children with DD/MID) 2002:
• Etiologic diagnoses in 150 (54%). • 1/3 on the basis of Hx and PE alone; in another 1/3,
Hx & PE provided essential clues to the diagnosis (e.g PWS), later confirmed by additional studies; and laboratory studies alone provided diagnoses in the remaining 1/3.
• On the basis of clinical Hx alone, a diagnosis could be established in 1 of 20 patients, and on the basis of PE alone, a diagnosis could be established in 1 of 30 patients. On the basis of Hx&PE together, a diagnosis was made in 1 of 3 patients.
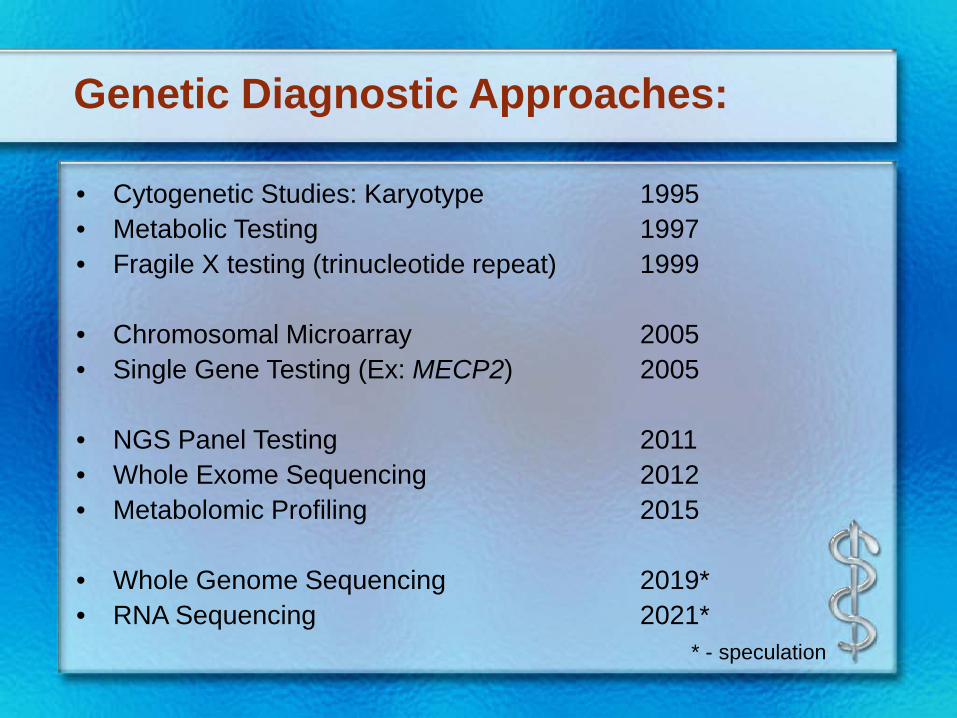
Genetic Diagnostic Approaches:
• Cytogenetic Studies: Karyotype 1995• Metabolic Testing 1997• Fragile X testing (trinucleotide repeat) 1999
• Chromosomal Microarray 2005• Single Gene Testing (Ex: MECP2) 2005
• NGS Panel Testing 2011• Whole Exome Sequencing 2012• Metabolomic Profiling 2015
• Whole Genome Sequencing 2019*• RNA Sequencing 2021*
* - speculation
Genetic Diagnostic Approaches:
• Cytogenetic Studies: Karyotype 1995• Metabolic Testing 1997• Fragile X testing (trinucleotide repeat) 1999
• Chromosomal Microarray 2005• Single Gene Testing (Ex: MECP2) 2005
• NGS Panel Testing 2011• Whole Exome Sequencing 2012• Metabolomic Profiling 2015
• Whole Genome Sequencing 2019*• RNA Sequencing 2021*
* - speculation
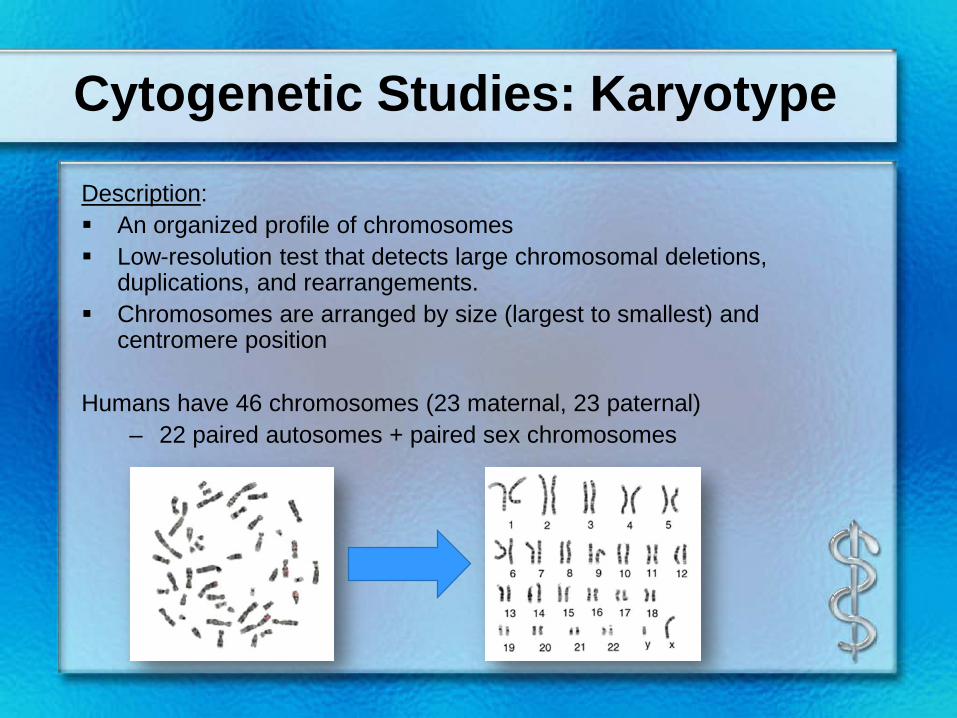
Cytogenetic Studies: Karyotype
Description: An organized profile of chromosomes Low-resolution test that detects large chromosomal deletions,
duplications, and rearrangements. Chromosomes are arranged by size (largest to smallest) and
centromere position
Humans have 46 chromosomes (23 maternal, 23 paternal)– 22 paired autosomes + paired sex chromosomes
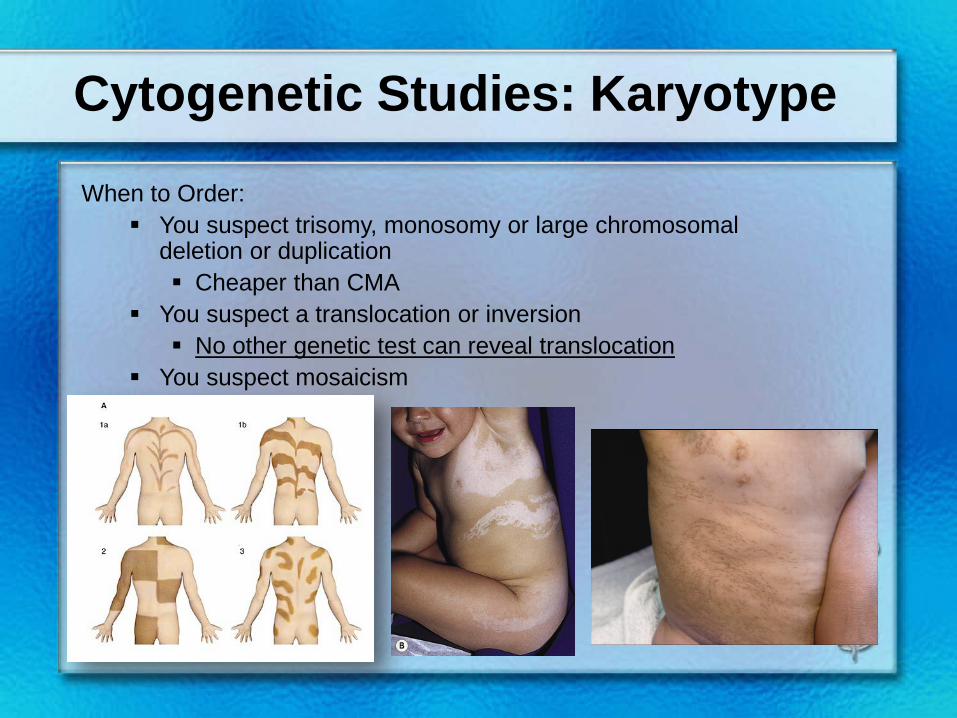
Cytogenetic Studies: Karyotype
When to Order: You suspect trisomy, monosomy or large chromosomal
deletion or duplication Cheaper than CMA
You suspect a translocation or inversion No other genetic test can reveal translocation
You suspect mosaicism
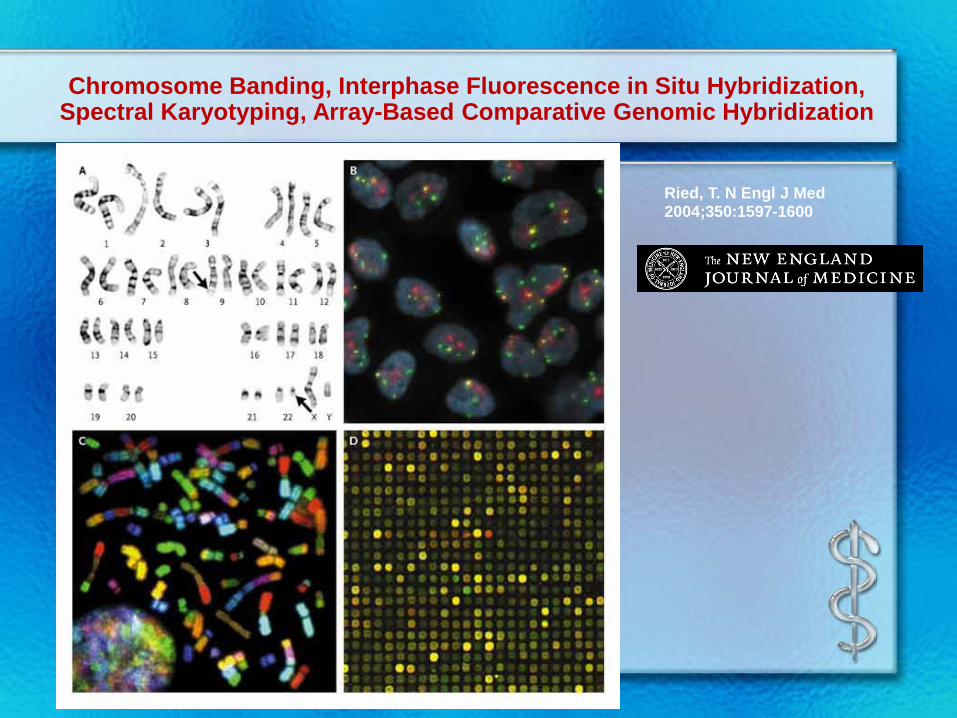
Chromosome Banding, Interphase Fluorescence in Situ Hybridization, Spectral Karyotyping, Array-Based Comparative Genomic Hybridization
Ried, T. N Engl J Med 2004;350:1597-1600
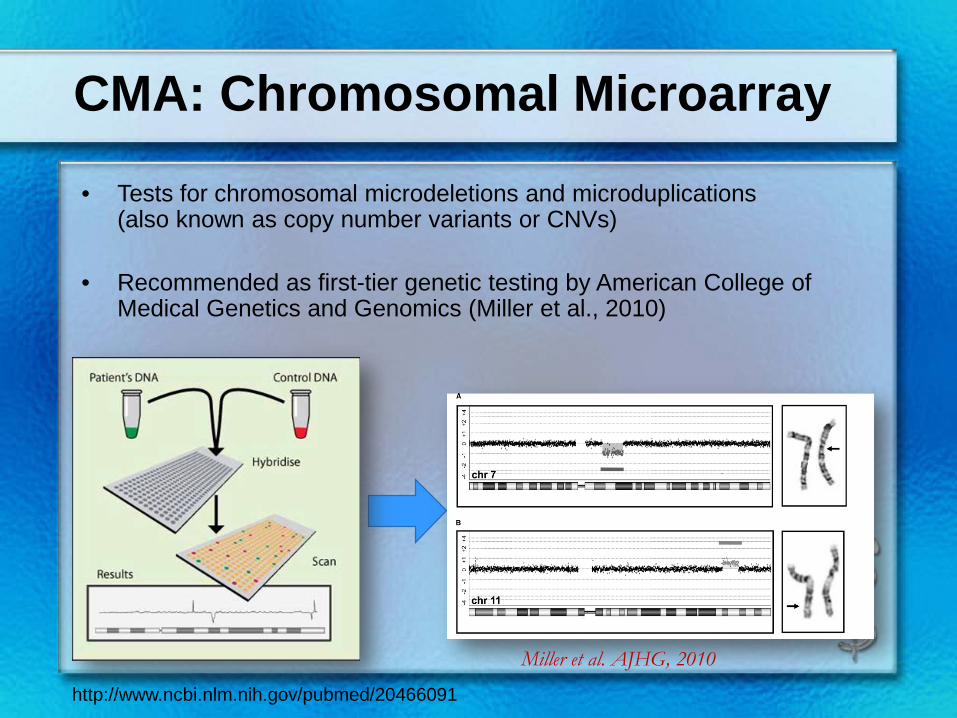
CMA: Chromosomal Microarray
• Tests for chromosomal microdeletions and microduplications(also known as copy number variants or CNVs)
• Recommended as first-tier genetic testing by American College of Medical Genetics and Genomics (Miller et al., 2010)
http://www.ncbi.nlm.nih.gov/pubmed/20466091
Miller et al. AJHG, 2010
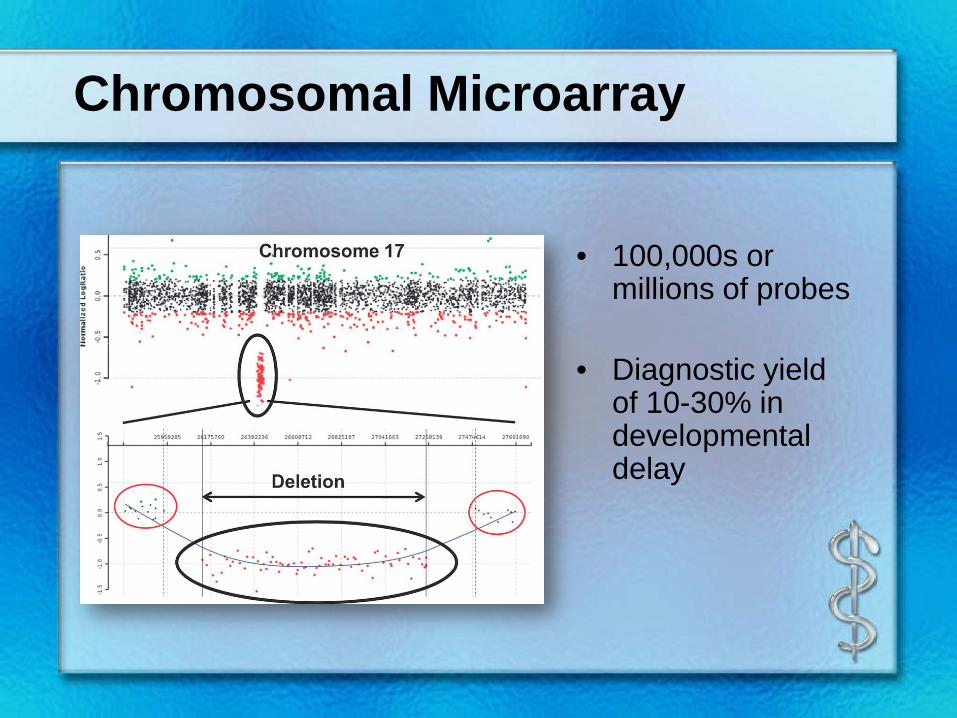
Chromosomal Microarray
• 100,000s or millions of probes
• Diagnostic yield of 10-30% in developmental delay
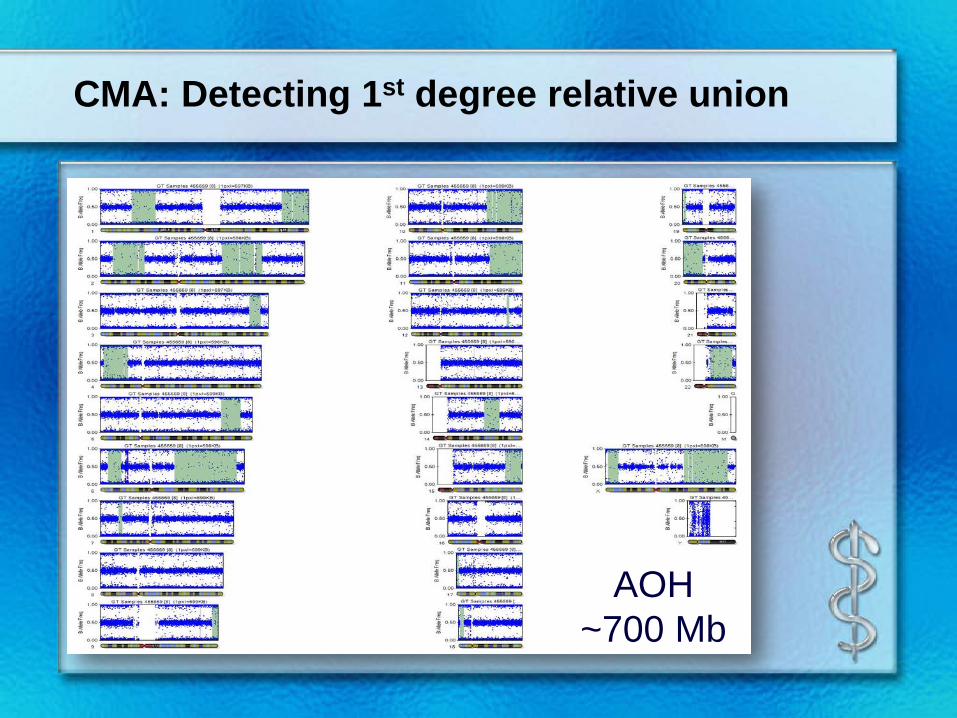
CMA: Detecting 1st degree relative union
AOH ~700 Mb
Advantages
Higher resolution than karyotype (3-10Mb vs. 100-200kb)
Higher diagnostic rate (10-20% higher than karyotype)
Disadvantages
Does not evaluate for translocations or low mosaicism
0.16% of chromosomal abnormalities were missed by using CMA as first-line test (Bi et al., 2013)
Due to low-level mosaicism or balanced translocation
Chromosomal Microarray
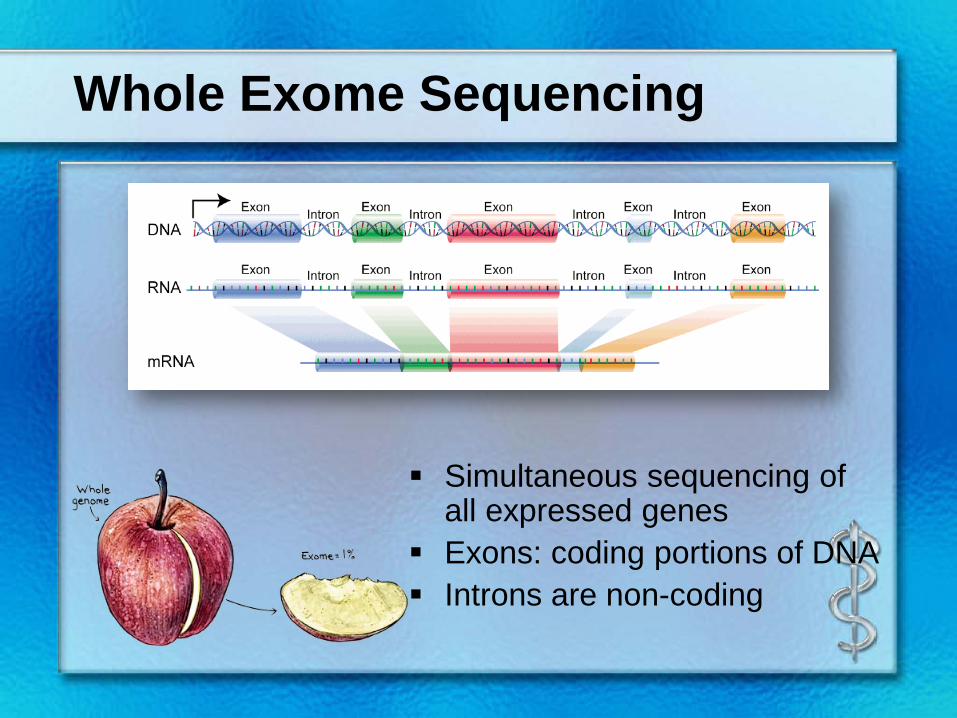
Whole Exome Sequencing
Simultaneous sequencing of all expressed genes
Exons: coding portions of DNA Introns are non-coding
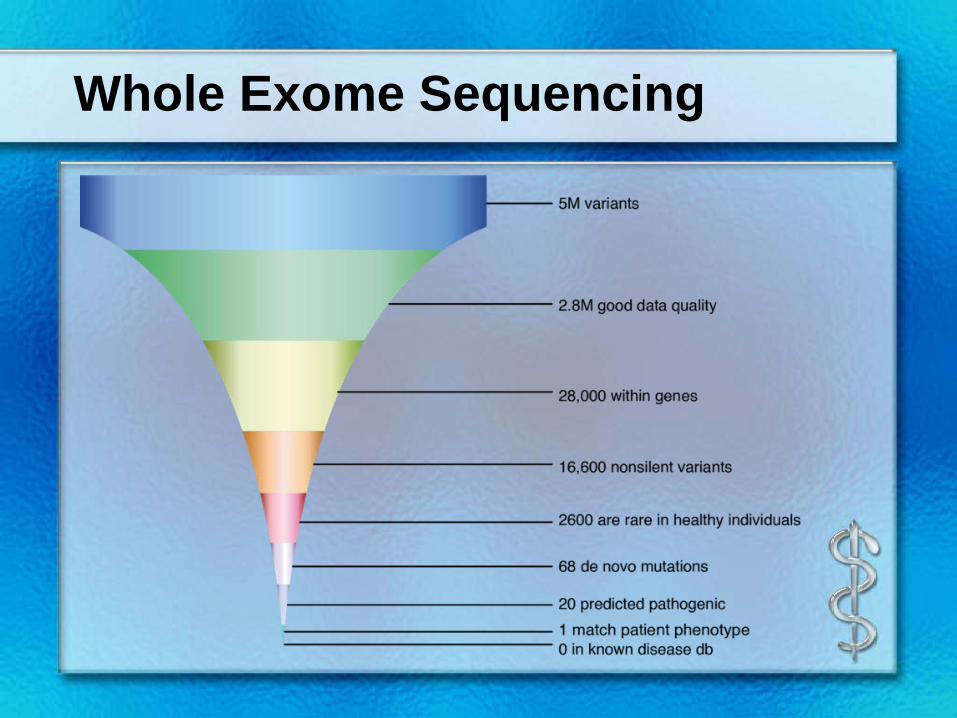
Whole Exome Sequencing

Whole Exome Sequencing
Each variant is categorized according to its predicted clinical significance
When to Order WES??
Phenotype suggests genetic etiology:
GDD + Seizures GDD + Neuroregression GDD + Dysmorphisms GDD + Malformations
Previous testing (CMA) has been normal Minor and major malformations present Numerous possible syndromes could fit the
phenotype
WES Possible Outcomes
1. Pathogenic mutation in genes related to clinical phenotype (~35-50%, depending on indication)
2. Variants of unknown significance in genes related to clinical phenotype
3. Medically actionable mutations in genes unrelated to clinical phenotype
4. Carrier status for recessive Mendelian disorders
5. Pharmacogenetic variants
Whole Exome Sequencing:
Advantages Sequencing of many genes simultaneously Incidental findings (medically actionable can be helpful) Provides a molecular approach to diagnosing a difficult
phenotype
Disadvantages Cost and turn around time …improving Exome only, limited by current literature Does not detect large deletions or duplications Does not detect trinucleotide repeat expansions Does not detect methylation Incidental findings
Genetic Testing – TIPS!
• Cytogenetic Studies: Karyotype 1995– Only technique that can detect translocations or inversions
• Fragile X testing (trinucleotide repeat) 1999– Only test that can detect Fragile X Syndrome
• Chromosomal Microarray 2005– Best first-line test for developmental delay today!
• Whole Exome Sequencing 2012– Generally ordered AFTER a CMA when a genetic diagnosis is suspected.
• Metabolomic Profiling 2015• Whole Genome Sequencing 2019*• RNA Sequencing 2021*
* - speculation
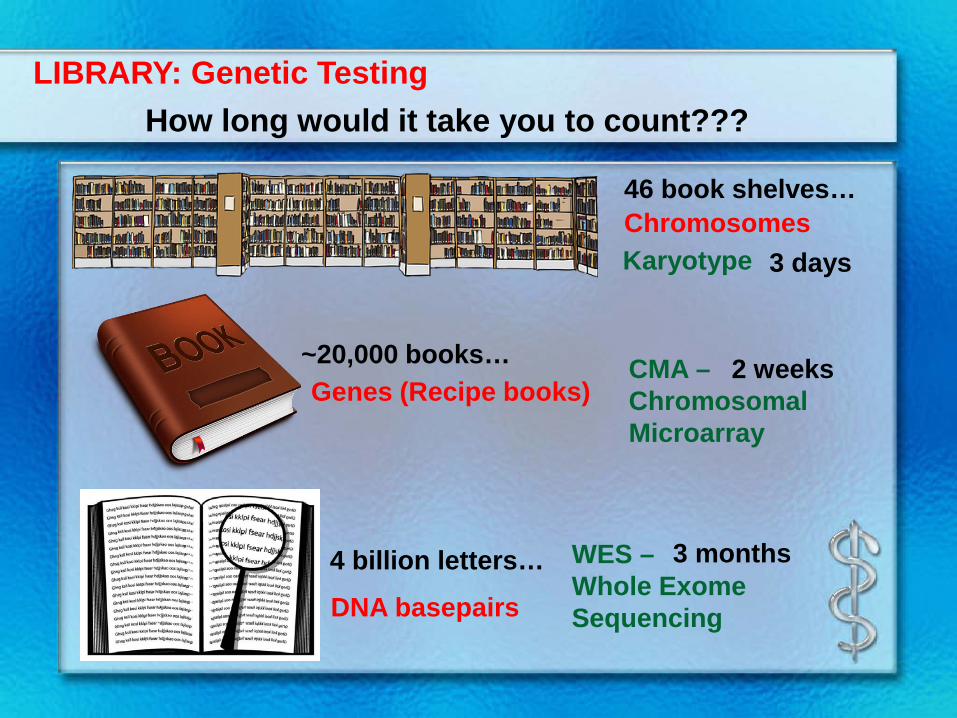
THIS IS A LIBRARY!!!
How to discuss with parents?
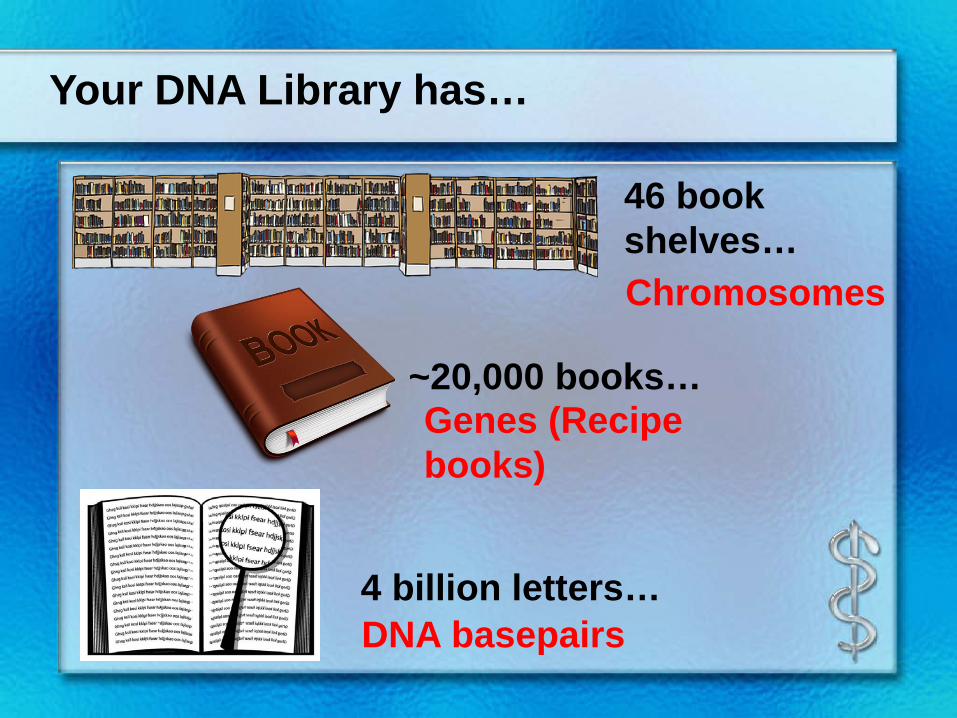
46 book shelves…
~20,000 books…
Your DNA Library has…
4 billion letters…
Chromosomes
Genes (Recipe books)
DNA basepairs
46 book shelves…
~20,000 books…
4 billion letters…
Genes (Recipe books)
DNA basepairs
How long would it take you to count???LIBRARY: Genetic Testing
Karyotype 3 days
WES –Whole Exome Sequencing
3 months
CMA –Chromosomal Microarray
2 weeks
Chromosomes
Questions???
Cited References• McDonald & et.al.Investigation of global developmental delay.Arch Dis Child. 2006
Aug;91(8):701-5.
• Moeschler JB, Shevell M; American Academy of Pediatrics Committee on Genetics. Clinical genetic of the child with mental retardation or developmental delays.Pediatrics. 2006 Jun;117(6):2304-16.
• Shaffer, Lisa G. PhD; on behalf of the American College of Medical Genetics (ACMG) Professional Practice and Guidelines Committee. American College of Medical Genetics guideline on the cytogenetic evaluation of the individual with developmental delay or mental retardation. Genet Med, 2005 Nov-Dec;7(9):650-4
• van Karnebeek CD.Diagnostic investigations in individuals with mental retardation: a systematic literature review of their usefulness.Eur J Hum Genet. 2005 Jan;13(1):6-25.
• Shevell M et. al. Practice parameter: evaluation of the child with global developmental delay: report of the Quality Standards Subcommittee of the American Academy of Neurology and The Practice Committee of the Child Neurology Society.Neurology. 2003 Feb 11;60(3):367-80.
• Curry CJ. et al. Evaluation of mental retardation: recommendations of a Consensus Conference: American College of Medical Genetics.AJMG 1997 Nov 12;72(4):468-77.





























