-
8/3/2019 Neuromuscular dis .
1/47
MUSCLES DISEASES
Dr.Rashad A. ghani
-
8/3/2019 Neuromuscular dis .
2/47
Introduction: structure and functionWe possess more than 150
voluntary (skeletal) muscles.
Complex voluntary movements of the body are achievedby
integrated activity of different skeletal muscle groups.
-
8/3/2019 Neuromuscular dis .
3/47
Each muscle fibre has a membrane (thesarcolemma), it contains
cytoplasm (thesarcoplasm), and it has an endoplasmic reticulum
(the sarcoplasmic reticulum) as well as othersubcellular
organelles such as mitochondria.Typically the nuclei are positioned
at the edges ofthe muscle fibre.
-
8/3/2019 Neuromuscular dis .
4/47
A chain of important structural proteins maintain the integrity
of thesarcolemma by linking intracellular muscle fibre cytoskeletal
proteinsto the extracellular matrix. These structural proteins
includedystrophin (located in a subsarcolemmal distribution), the
dystrophin-
associated glycoprotein complex (a trans-sarcolemmal
proteincomplex), and laminin (located extracellularly). These
importantproteins may be dysfunctional in certain forms of genetic
musclediseases.
-
8/3/2019 Neuromuscular dis .
5/47
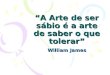
After staining, muscle fibres are seen
to have regular cross-striations ,
dividing it up into sarcomeres. Thelight I band is divided by
the dark Z
line and the dark A band has the
lighter H zone in its centre. The
region between two adjacent Z
lines is called a sarcomere. The
cross-striations are due to the
presence of the principal contracile
filamentous proteins, actin and
myosin, in the sacroplasm. These
filamentous proteins are arranged in
rod-like structures known asmyofibrils. A single myofibril
contains many protein filaments.
-
8/3/2019 Neuromuscular dis .
6/47
The thick filaments are
lined up to form the A
bands, whereas the array
of thin filaments formsthe less dense I bands.
The lighter H bands in
the centre of the A bands
are the regions where,when the muscle is
relaxed, the thin
filaments do not overlap
the thick filaments. The
Z lines transect the
myofibrils and connect
to the thin filaments
-
8/3/2019 Neuromuscular dis .
7/47
-
8/3/2019 Neuromuscular dis .
8/47
-
8/3/2019 Neuromuscular dis .
9/47
-
8/3/2019 Neuromuscular dis .
10/47
Neuromuscular disorders
Myopathies are disorders in which there is a
primary functional or structural impairment of
skeletal muscle. Myopathies usually cause
proximal symmetric weakness, with or without
other symptoms.
-
8/3/2019 Neuromuscular dis .
11/47
Causes of myopathies
Inherited
Muscular dystrophies
Myotonic dystrophy
Congenital myopathies
ChannelopathiesPrimary metabolic disorder
Congenital myasthenic syndromes
AcquiredDrug and toxin inducedEndocrine
Secondary metabolic
Inflammatory
Paraneoplastic
Myasthenia gravis
Lambert-Eaton myasthenic
syndrome
-
8/3/2019 Neuromuscular dis .
12/47
Muscular dystrophiesThe muscular dystrophies are a group of
inheriteddisorders characterised by progressive muscle
wasting and weakness.
The classification of muscular dystrophy is based onboth
clinical and genetic characteristics.
-
8/3/2019 Neuromuscular dis .
13/47
Progressive muscular dystrophies result from
diverse defects in muscle proteins
-
8/3/2019 Neuromuscular dis .
14/47
Disease Gene Inheritance Protein
X-linked dystrophiesDuchenne/BeckerEmery-Dreifuss
Xq 21Xq 28 XRXR DystrophinEmerin
Limb-girdle muscular dystrophiesLGMD 1 to CALGMD 2A to HA
2, 4, 513,17 ADAR CalveolinSarcoglycans,Calpain
Congenital muscular dystrophies(With CNS involvement)Fukuyama
CMDWalker - Warburg CMDMuscle - Eye-Brain CMD(Without CNS
involvement)Merosin-deficient classic typeMerosin-positive classic
type
9q 316q2Lama2ARARARARAR
Fukutin??Merosin?
Distal dystrophies 2,79 AR/AD
DysferlinFacioscapulohumeraleOculopharyngealMyotonic dystrophy
4q 351419ADADAD Repeat expansion
-
8/3/2019 Neuromuscular dis .
15/47
Type Onset Clinical features Other organsystem involedDuchenne
Before 5years Progressive weakness ofgirdle muscle,
calfhypertrophy.
Wheelchair bound: after12 years.KyphoscoliosisRespiratory
failure (death)in the 2nd or 3rd decade
Cardiomyopathy
Becker Earlychildhoodto adultProgressive weakness ofgirdle
musclesAble to walk after age 15Respiratory failure maydevelop by
4th decade
Cardiomyopathy
Emery- drefuss Childhood to adult Elbow contractures,humeral and
peronealweaknessDeath by the 4th decadeunless treated
bypacemaker
CardiomyopathyHeart block
-
8/3/2019 Neuromuscular dis .
16/47
Limb-girdle Earlychildhoodto earlyadult
Slow progressiveweakness of girdlemusclesCardiomyopathy
Facioscapulo-humeral Beforeage 20 Slowly progressiveweakness of
face,shoulder girdle, and footdorsiflexionSurvival
generallyunaffected
Deafness
Oculopharyngeal 5th to 6thdecade Slowly progressiveweakness of
extraocular,pharyngeal and limbmuscles
------
Congenital At birth orwithin 1stfewmonths
Hypotonia, contractures,delayed milestones,progression to
respiratoryfailure in some, staticcourse in others
CNSabnormalities(hypomyelination,malformation)Eye
abnormalities
-
8/3/2019 Neuromuscular dis .
17/47
Congenital
myopathy
early life or
infancy
Hypotonia,
Relatively
nonprogressiveweakness.
Unique
morphological
features onmuscle biopsy
dysmorphic
features
-
8/3/2019 Neuromuscular dis .
18/47
Epidemiology
Incidence:Duchenne / Becker muscular dystrophy 56%
Limb-girdle muscular dystrophy 19%
Congenital muscular dystrophy 18%
Facioscapulohumeral muscular dystrophy 4%
Emery-Dreifuss muscular dystrophy 1%
Others 2%
-
8/3/2019 Neuromuscular dis .
19/47
Investigated Approach In Suspected MDCreatinine
Phosphokinase
The serum levels of CPK are significantly elevated (in
thousands) in DMD/BMD patients.
Electromyography shows decreased amplitude and
duration of motor unit potential.
Muscle biopsy
variation in size
centralization of nuclei
rounded atrophic fibers
endomysial fibrosis
-
8/3/2019 Neuromuscular dis .
20/47
Immunohistochemistry:
Immunohistochemistry utilizing anti-dystrophin,
anti-sarcoglycan, and anti-laminin-alpha2 antibodiesNormal
Deficient Absent
Genetic testing:DNA studies are available for Duchenne,
becker,facioscapulohumeral, myotonic dystrophy and about half of
thelimb girdle MD.
-
8/3/2019 Neuromuscular dis .
21/47
Duchennes muscular dystrophy
This is the commonest form of muscular
dystrophy. It is virtually confined to males. The
genetic defect in Duchennes muscular dystrophy
affects the dystrophin gene, located in the X
chromosome. The dystrophin protein is absent invirtually all
cases ofDuchennes and is abnormal
in patients with Beckers muscular dystrophies.
-
8/3/2019 Neuromuscular dis .
22/47
Clinical features
Onset in the 1st decade (3-6 years). Waddling gait
is the first symptom. Walking difficulties appear,followed by
difficulty in climbing stairs and in
rising from the floor. Pseudohypertrophy,
particularly of the calf muscles, is almostinevitable. Gowers
sign is characteristic
manoeuvre . By about the age of 10, the patient is
unable to walk; the majority of cases die by the
age of 20. Cardiomyopathy is almost always
present and some patients develop cardiac failure.
-
8/3/2019 Neuromuscular dis .
23/47
-
8/3/2019 Neuromuscular dis .
24/47
The myotoniasMyotonia is the phenomena of impaired
relaxation of muscle after forceful voluntary
contraction. Myotonia can be triggered either by a
voluntary contraction or percussion.
-
8/3/2019 Neuromuscular dis .
25/47
Paramyotonia congenita
With paramyotonia congenita, exposure to coldtriggers attacks of
muscle contraction followed
by flaccid weakness. The condition is inherited
as an autosomal dominant.
-
8/3/2019 Neuromuscular dis .
26/47
Myotonic dystrophy (Dystrophia myotonica)
The gene responsible for myotonic dystrophy islocated on the
long arm of chromosome 19. The
genetic defect is an expansion of CTG trinucleotide
repeats.
Cli i l f t
-
8/3/2019 Neuromuscular dis .
27/47
Clinical features
The clinical features (onset &severity) are extremely
variable. The condition may be asymptomatic. The
muscle weakness is predominantly distal in both
upper and lower limbs.
Characteristic facies
Cataract is common and may be
the presenting feature. Other
findings include Cardiacconduction defects , testicular
atrophy, pituitary abnormalities
and diabetes.
-
8/3/2019 Neuromuscular dis .
28/47
Investigations
EMG studies reveal myotonic discharges (dive-
bomber sounds ) and a myopathic pattern. Musclebiopsy
demonstrates selective atrophy of Type 1
fibres associated with an increased proportion of
central nuclei
-
8/3/2019 Neuromuscular dis .
29/47
The Inflammatory Myopathies
Inflammatory disease of muscle (myositis) is
either idiopathic or infective in origin.Polymyositis and
dermatomyositis are the
commonest.
Diagnostic criteria include:A clinical picture ofproximal muscle
weakness,
often with pain
Histological evidence of muscle fibre necrosiswith cellular
infiltration,
An elevated serum CKactivity
and acharacteristic EMG pattern.
-
8/3/2019 Neuromuscular dis .
30/47
Polymyositis and dermatomyositis share the same
clinical characteristics in terms of muscle
involvement but with additional skin changes in thelatter.
There is predominant proximal
muscle weakness often accompaniedby pain and muscle tenderness.
Neck
weakness is common. Dysphagia
secondary to involvement of thepharyngeal muscles also
occur.
-
8/3/2019 Neuromuscular dis .
31/47
The dermatomyositis is associated with
malignancy in 40% of cases.
Polymyositis is associated with conective tissuedisorder in 20%
of cases.
Investigation
Serum CK activity is particularly high in the acuteforms. EMG
changes include spontaneous
activity, with fibrillation potentials, and volitional
units of small amplitude and duration associatedwith
polyphasia.
-
8/3/2019 Neuromuscular dis .
32/47
Muscle biopsy
Polymyositis: segmental necrosis withlymphocytic
infiltration
Dermatomyositis: perifascicular
atrophy and prominent perivascular
infiltrates.
http://www.emedicine.com/cgi-bin/foxweb.exe/makezoom@/em/makezoom?picture=/websites/emedicine/neuro/images/Large/576picture_51.jpg&template=izoom2http://www.emedicine.com/cgi-bin/foxweb.exe/makezoom@/em/makezoom?picture=/websites/emedicine/neuro/images/Large/11061099573picture_48.jpg&template=izoom2
-
8/3/2019 Neuromuscular dis .
33/47
Treatment:
Of all the treatments that are available,
prednisolone remains the drug of choice. Iftreatment with
steroids is not successful, other
lines of treatment are considered, such as
intravenous immunoglobulins (IVIG),immunosuppressive therapy;
and antineoplastic
agents.
-
8/3/2019 Neuromuscular dis .
34/47
Disorders of neuromuscular junctionMyasthenia Gravis
Myasthenia gravis (MG) is an acquired autoimmune
disorder characterized clinically by muscles
weakness and fatigability.
-
8/3/2019 Neuromuscular dis .
35/47
Pathophysiology:
The antibodies in MG are directed toward the
acetylcholine receptor (AChR) at the neuromuscularjunction (NMJ)
of skeletal muscles. Anti-AChR
antibody is found in approximately 80-90% of
patients with generalized MG and 50% for those withocular
myasthenia. The thymus is the central organ in
T cellmediated immunity, and thymic abnormalities
such as thymic hyperplasia (50%) or thymoma (15%)
are well recognized in myasthenic patients.
-
8/3/2019 Neuromuscular dis .
36/47
Epidemiology:
Estimated annual incidence is 2 per 1,000,000.The prevalence
rate is 14 per 100,000.
Age: MG presents at any age. Female incidence
peaks in the third decade of life, whereas maleincidence peaks
in the sixth or seventh decade.
Sex: The female-to-male ratio is said classically
to be 6:4.
-
8/3/2019 Neuromuscular dis .
37/47
Clinical features
MG is characterized by fluctuating weakness
increased by exertion. Weakness increases duringthe day and
improves with rest. Extraocular muscle
(EOM) weakness or ptosis is present initially in 50%
of patients and occurs during the course of illness in90%.
Bulbar muscle weakness is also common,
along with weakness of head extension and flexion.
Weakness may involve limb musculature with
myopathic-like proximal weakness greater than
distal muscle weakness.
-
8/3/2019 Neuromuscular dis .
38/47
Muscle fatiguability can be confirmed by a variety
of bedside tests (counting test).
Characteristic triple
forrowed tongue
-
8/3/2019 Neuromuscular dis .
39/47
Edrophonium test (a trial dose of 2mg, followed after
about 30s by 8mg) is a valuable means of confirming
the diagnosis
-
8/3/2019 Neuromuscular dis .
40/47
Investigations:Anti-acetylcholine receptor antibody: Results
are
positive in about 80% of patients with generalized
myasthenia and in 50% of those with pure ocular
myasthenia. CT scanning detects all thymomas, and
may reveal abnormalities in some patients with
thymic hyperplasia.
-
8/3/2019 Neuromuscular dis .
41/47
RNS produced decremental response & SFEMG showsabnormal
jitter
http://www.emedicine.com/cgi-bin/foxweb.exe/makezoom@/em/makezoom?picture=/websites/emedicine/neuro/images/Large/163rns.jpg&template=izoom2
-
8/3/2019 Neuromuscular dis .
42/47
TreatmentAChE inhibitors (Pyridostigmine, neostigmine)
and immunomodulating therapies are the
mainstays of treatment. Plasmapheresis and
thymectomy are important modalities for treating
MG. Plasma exchange (PE) is an effectivetreatment for MG,
especially in preparation for
surgery or as short-term management of an
exacerbation. Thymectomy may induce remissionin young patients
with a short duration of disease,
hyperplastic thymus, and high antibody titer.
-
8/3/2019 Neuromuscular dis .
43/47
Myasthenic crisis: is an acute exacerbation of MG
with severe weakness and/or acute respiratory
failure. This is a true neuromuscular emergency,
and immediate intubation may be necessary.
-
8/3/2019 Neuromuscular dis .
44/47
Symptomatic myastheniaCauses
Polymyositis or dermatomyositis.
Penicillamine
Antibiotics and with exposure to botulinum toxin
and organophosphate pesticides
-
8/3/2019 Neuromuscular dis .
45/47
Lambert-Eaton syndrome
A myasthenic syndrome is recognized to occur in
association with various autoimmune diseases andis associated
with malignancy in 40% of cases,
particularly small cell carcinoma of the bronchus.
It mainly affects women.
Clinically, the condition often mimics a proximal
myopathy with muscle pain. Fatiguability is
seldom conspicuous.
-
8/3/2019 Neuromuscular dis .
46/47
There are certain very characteristic EMG findings.
-
8/3/2019 Neuromuscular dis .
47/47