-
8/18/2019 Nephrology 02
1/5
13 : 2
ABSTRACT:
The term “Cardiorenal syndrome” has gained wide attentionof
physicians in recent times specially due to the
increasingpresentations of patients with dual organ dysfunction
resulting froma web of pathophysiological causation , the proper
understandingof which might have important bearings on management
andoutcome of these patients. This web of causation, though
poorlyunderstood has been termed the cardio-renal connection
and
in nutshell includes the Renin- Angiotensin- Aldosterone
System(RAAS), Sympathetic Nervous system (SNS), Nitric Oxide
,inflammatory cytokines etc1.Recently in the World Congress
ofNephrology the bi-directional nature of the Cardiorenal
syndromewas emphasized and a classification based on
pathophysiology wasproposed. Till now the management of the
syndrome has metwith little success and no specific treatment
strategy has beenestablished definitively. Diuretics, inotropes,
vasodilators, renalreplacement therapy and others have all been
tried with variable
success. More research and definitive clinical trials are
requiredto further understand the pathophysiology and devise
effectivemanagement strategies for the syndrome.
Key Words: Cardiorenal syndrome, RAAS, heart failure
Concomitant cardiac and renal dysfunction is the most
simplisticview of cardio-renal syndrome. However the definition
isambiguous as it lacks a direction of pathogenesis of the
diseaseprocess. In fact the general view holds that renal injury
occurssecondary to a diseased heart and in the presence of a
normalcardiac function the same kidneys would perform normally
(c.fHepato-renal syndrome) 2. However it is a known fact that
primarydisorder of one of these two organs often causes
secondarydysfunction of the other.3Hence a more comprehensive
definitionthat encompasses the complete patho-physiology linking
the twoorgans is required.
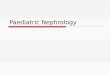
CARDIO-RENAL SYNDROME: DEFINITION
The cardio-renal syndrome includes a variety of acute or
chronicdisorders where the primary failing organ can be either the
heartor the kidney leading to the secondary dysfunction of the
other. 4 (Fig.1)Thus according to the chronology of events the
cardio-renal syndrome can be subdivided into 5 sub-types,
namely4:
1. CRS type 1:Acute cardio-renal syndrome
2. CRS type 2:Chronic cardio-renal syndrome
3. CRS type 3: Acute reno-cardiac syndrome
4. CRS type 4: Chronic reno-cardiac syndrome
5. CRS type 5: Secondary cardio-renal syndrome
CRS type 1: Acute cardio-renal syndrome is defined as
acutecardiac failure leading to worsening of renal function. Within
this isa spectrum of disorders involving the heart and the blood
vesselsleading to acute heart failure which further causes Acute
kidneyinjury through multiple mechanisms5. These mechanisms
include:
1. Acute hypo perfusion leading to decreased G.F.R
2. Decreased Oxygen delivery
Khan SA, Gupta V, Haque SF, Aligarh
CARDIO-RENAL SYNDROME
Fig. 1 : Cardiorenal syndrome Pathophysiology
KIDNEY
INJURY
CARDIAC
FAILURE
RAAS, SNS,
NO-ROS,
Inflammatory
Mediators
C ARDI O-RE NAL S Y NDR OM
E
-
8/18/2019 Nephrology 02
2/5
Medicine Update 2010 Vol. 20
686
3. Resistance to ANP/BNP
4. Cell Necrosis/ apoptosis
In fact AKI tends to be more severe in patients with
impairedLeft Ventricular ejection fraction, being >70% in
patients withcardiogenic shock 6.
Early diagnosis of kidney injury in CRS 1 and also CRS 3
(discussedlater) is important , but still remains difficult as
serum creatininerises when the AKI is already established.
Recently, novelbiomarkers which rise within first few hours of
onset of AKIhave been discovered. Of these Neutrophil Gelatinase
AssociatedLipocalin (NGAL) is one of the earliest and highly
sensitive markerof ischemic/nephrotoxic kidney injury detected in
the blood/urine. Similarly Kidney Injury Molecule is a highly
specific markerfor ischemic AKI. Table 1 lists important biomarkers
for the earlydetection of AKI.
Thus by using a combination of assay of these biomarkers Type
1CRS can be diagnosed early with timely intervention to
preventongoing renal damage.
Management: While diuretics, both loop and thiazides have
beenuseful in volume overloaded non-hypotensive patients,
thereoverzealous use is associated with worsening of renal
function7.Also diuretic therapy exacerbates neurohormonal activity,
activatesthe RAAS, increases systemic vascular resistance and
worsensleft ventricular function8 9. Besides, inotropes
like dobutamine,dopamine, milrinone may be judiciously used in
patients withimpaired cardiac output although their role is still
controversialas they have been associated with increased mortality
and cardiac
events
10
.Vasodilators like Nesiritide have been used favourably
inthe treatment of Acute Decompensated Heart Failure where anon
hypotensive, low cardiac output state is combined with
coldextremities and increased peripheral vascular resistance due
toexcessive vasoconstriction. In fact Nesiritide has been shown
toreduce both systemic and pulmonary pressures and increase
thecardiac and stroke volume indices11. However in the context
ofcardiorenal dysfunction Wang and colleagues found that
nesiritidehad no effect on GFR, renal plasma flow, urine output, or
sodium
excretion12.
Patients who have diuretic resistant volume overload may
stillrespond to ultrafiltration13.
Newer promisimg approaches in the management include theArginine
Vassopressin Receptor antagonists like Tolvaptan(EVEREST trial)
14 15and Adenosine A
1 receptor antagonists.
CRS type 2: Chronic cardio-renal syndrome involves
ChronicCongestive cardiac failure causing progressive kidney
dysfunctionset on a background of chronically reduced renal
perfusionand chronic renal venous congestion. The prevalence of
renaldysfunction in chronic HF has been reported to be
approximately25% 16. In fact the pathophysiology of renal
dysfunction in thissyndrome is poorly understood. The ESCAPE study
found nolink between pulmonary artery catheter measured
hemodynamicvariables and serum creatinine17.The different putative
mechanismsinclude low cardiac output causing activation of RAAS
andsympathetic nervous system, subclinical inflammation,
endothelialdysfunction, increased renal vascular resistance and
acceleratedatherosclerosis. Recently it has been found that these
patientshave relative/absolute erythropoietin deficiency causing
moresevere anaemia than can be accounted for by renal failure
alone18.In fact erythropoietin receptor activation in the heart may
reducethe risk of apoptosis, inflammation and
fibrosis19 20.
Management: Although diuretics are helpful in managing avolume
expanded state, the key drugs in treating left ventricularsystolic
dysfunction are the Angiotensin-Converting EnzymeInhibitors and
Angiotensin Receptor Blockers. They by blockingthe RAAS not only
affect cardiac remodeling and cause regressionof LVH but also
retard proteinuria and progression of CKD.Due to the presence of
excessive vasoconstrictor mediators inchronic heart failure,
vasodilators might be of use in reducing the
congestion and improving renal perfusion.CRS type 3: Acute
renocardiac syndrome is Acute Kidneyinjury leading to acute cardiac
dysfunction through differentpathophysiological mechanisms
involving three main systems: theRAAS, Nitric Oxide-Reactive oxygen
species and the sympatheticnervous system. Fluid overload and
accelerated hypertensioncan lead to acute pulmonary edema.
Hyperkalemia can lead tolife threatening cardiac arrhythmias and
sudden cardiac arrest.Metabolic acidosis can affect cardiac
inotropy21 and causepulmonary vaso-constriction leading to
right sided heart failure22.Acute uremia may cause depression of
myocardial contractilitywhile uremic pericarditis may act as a
mechanical hindrancefor the same. Myocardial ischemia frequently
complicates AKI
which is due to a reduced coronary reserve which fails to
meetincreases in myocardial oxygen demand. Renal ischemia
alsoinduces a Systemic inflammatory response syndrome producinga
number of pro-inflammatory cytokines leading to a
delayedcardiodepressant response23.
A variety of markers of cardiac dysfunction/injury
includingCardiac Troponins, NT-Pro BNP, cytokines like TNF α, IL-6
andmyeloperoxidase may be utilized for early detection of this
Table 1 : Lists important biomarkers for the early de-
tection of AKI.
Biomarker Associated Injury
Cystatin C Proximal tubule injury
KIM-1 Ischemia and nephrotoxins
NGAL Ischemia and nephrotoxins
NHE3 Ischemia, pre-renal, post-renal AKI
α-GST Proximal Tubular injury, Acute rejection
π-GST Distal Tubular injury, Acute rejection
L-FABP Ischemia and nephrotoxins
Cyr61 Ischemic ATN
Netrin-1 Ischemia and nephrotoxins,sepsis
GST = glutathione S-transferase; IL = interleukin; KIM = kidney
in-
jury molecule; L-FABP = L-type fatty acid binding protein;
NGAL =
neutrophil gelatinase-associated lipocalin; NHE =
sodium-hydrogen
exchanger;Cyr61=Cysteine rich protein 61.
-
8/18/2019 Nephrology 02
3/5
Cardio-Renal Syndrome
687
syndrome.
Management: Adequate treatment of accelerated
hypertension,hyperkalemia and metabolic acidosis reduces the risk
of cardiacinjury. At the same time hemodialysis can be used in
removingthe uremic toxins as well as treating the pericarditis
effectively.In patients with hemodynamic instability Continuous
renalreplacement therapies may offer better outcomes.
CRS type 4: Chronic Renocardiac syndrome is characterized
byprimary chronic kidney disease contributing to the developmentof
cardiac dysfunction resulting in increased cardiovascularmorbidity
and mortality. While microalbuminuria is known to
increase the Cardiovascular risk 2-4 times, declining GFR per
seis associated with increasing CV risk as shown in Table 2 24.
Besides the traditional risk factors, uremia and related novel
riskfactors are responsible for the development of
cardiovasculardisease, especially in CKD stages IV and V.25These
include (1)Anemia (2) Hypervolemia and hypertension (3) Abnormal
Calciumand phosphate metabolism (4) Oxidative stress and
inflammation(5) Endothelial dysfunction (6) ADMA (7)
Hyperhomocystenemia(8) Proteinuria
1. Anemia: For every 1g/dl decrease in mean haemoglobin therisk
of cardiac failure increases by 25% 26 .Anemia furthercauses
reduced viscosity, increased venous return and ag-gravation of
sympathetic activity leading to Left ventricularhypertrophy.
2. Hypervolemia and hypertension: Fluid overload as well
ashypertension increases the risk of cardiac failure. It is
fur-ther associated with Left Ventricular hypertrophy, develop-ment
of Ischemic Heart Disease and cardiomyopathy.
3. Abnormal Calcium and phosphate metabolism: CKD pa-tients have
increased disturbances of calcium and phosphatemetabolism as early
as stage 3 and are associated with ac-celerated calcifying
atherosclerosis and arteriosclerosis. InESRD patients , extensive
vascular, in particular coronaryartery calcication can be observed
in young age group
and they are strong predictors of Cardiovascular Disease
and all cause mortality27. The secondary hyperparathyroid-ism
along with hyperphosphatemia and increased Calcium –Phosphate
ionic product are independent risk factors forCardiovascular
disease28.
4. Oxidative stress and inammation: CKD is a state of chron-ic
inammation and increased oxidative stress. Various en-zymes
involved in production of reactive oxygen species :NADPH Oxidase,
Superoxide Dismutase, Nitric Oxide Syn-
Table 2 : Chronic Kidney Disease and CV Risk
Stage CKD GFR(ml/min) CV Risk (OR)
1 >90 ??(proteinuria)
2 60-89 1.5
3 30-59 2-4
4 15-29 4-10
5 20
thase, Myeloperoxidase are capable of oxidizing LDL Be-sides
there are increased levels of inammatory biomarkers
like CRP,IL-6, brinogen which along with Oxidised LDL are
proatherogenic and also lead to endothelial dysfunction.The
situation is further worsened by coexisting hypoalbu-minemia which
is a scavenger for these oxidants29.Oxidativestress also increases
the production of Advanced Glycation
End Products –Pentosidine and N CarboxyMethyl Lysinewhich may
contribute to accelerated atherosclerosis.
5. Endothelial Dysfunction: In CKD various factors
includinginammation ,ADMA , oxidative stress, hypertension
result
in endothelial dysfunction leading to accelerated
athero-sclerosis and increased cardiovascular mortality30
6. Proteinuria: Urinary ACR is independently associated withthe
presence and severity of cardiovascular disease in non-diabetic
population.
7. Hyperhomocysteinemia: The prevalence of hyperhomo-cysteinemia
in ESRD patients exceeds 90%.However theirexact relationship with
Cardiovascular disease is still notclear31.
8. ADMA: A competitive inhibitor of NO synthase, causes
de-creased NO bioavailability. ADMA is degraded by dimethylarginine
aminohydrolase –an enzyme found in renal tissue.With advancing CKD,
ADMA accumulates and leads to en-dothelial dysfunction and is
strongly associated with CVmortality32.
Management: The primary prevention of CRS type 4 consistsof
cessation of smoking, adequate control of Diabetes
andhypertension,.
• Correction of anemia using iron supplements and Erythro-
poietin to maintain a Haemoglobin between 11-12g% and apacked
cell volume >36%33.
• Control of volume overload and hypertension by using loop
diuretics as well as blocking the overactive RAAS by usingACE
inhibitors and ARB’s. ACE inhibitors and ARB’s shouldbe used even
if the patient is not hypertensive because theyare antiproteinuric
and retard the progression of kidneydisease34.Since CKD is a state
of sympathetic overactivityβ blockers as well as central
sympatholytics are useful notonly in controlling the blood pressure
but also reducing thesympathetic drive.
• Hyperphosphatemia and secondary hyperparathyroidism
have to be controlled and the Calcium * Phosphate ionicproduct
should be kept below 50mg2/m2 by dietary phos-phate
restriction and use of phosphate binders. Moreovernewer non-calcium
containing phosphate binders likeSevelamer are known to reduce the
progression of coro-nary and aortic calcication better than the
calcium con-taining phosphate binders35.
• CKD patients are high risk cardiovascular individuals,
hence
-
8/18/2019 Nephrology 02
4/5
Medicine Update 2010 Vol. 20
688
Statins should be used to achieve a LDL cholesterol levelof less
than 100 mg/dl (K/DOQI guidelines).Besides Statinsalso have modest
antiproteinuric effect36.However thereuse should be judicious in
view of recent reports that theymay favour development of renal
brosis37
• Antioxidants like Vitamin E and acetylcysteine have been
shown to have a benecial effect on cardiovascular eventsin
recent small studies and require further authentication.
CRS type 5: It is characterized by cardiac and renal
dysfunctiondue to acute or chronic systemic cause. While in the
acute settingsepsis is the most important cause, chronic conditions
consist ofdiabetes, amyloidosis, SLE etc. The acute or chronic
inflammatorystates acting through various cytokines like TNF
α,IL-1β,IL-6 etc.may affect the functioning of both these
organs38 39.Thereafterthe pathophysiological mechanisms of
both Type 1 and Type 3CRS apply in sepsis while those of Type 2 and
Type 4 CRS forchronic conditions.
Management: Treatment is directed at the prompt
identificationand treatment of the underlying cause while
supporting organfunction , both cardiac and renal by judicious use
of vasopressors, inotropes and diuretics. In septic patients,
preliminary studiessuggest that intensive renal replacement therapy
may have a rolein improving myocardial performance while providing
optimalsmall solute clearance 40.
Conclusion: Thus the concept of Cardiorenal syndrome is
stillin its preliminary stages of development with further
researchneeded to clarify its pathophysiology and adequate
methodsof management. Till then individualization of each patient
with judicious use of drugs is the best line of
management.
REFERENCES
1 Mahapatra H S, Lalmalsawma Robert, Singh N P, Kumar M, Tiwari
S CCardiorenal syndrome. Iranian Journal of Kidney Diseases 2009
Vol-ume 3 Number 2
2 Bongartz L.G., Cramer M.J., Doevendans P.A., Joles J.A. ,
Braam B., Thesevere cardiorenal syndrome: ‘guyton revisited.’, Eur
Heart J 26 (2005),pp. 11–17.
3 Schrier R.W., Cardiorenal versus renocardiac syndrome: is
there a dif-ference?, Nat Clin Pract Nephrol 3 (2007), p.
637
4 Ronco C, Haapio M, House AA, Anavekar N, Bellomo R.
Cardiorenalsyndrome. J Am Coll Cardiol. 2008;52:1527-39.
5 Liang K.V., Williams A.W., Greene E.L. and Redeld M.M., Acute
decom-pensated heart failure and the cardiorenal syndrome, Crit
Care Med36 (2008), pp. S75–S88
6 Jose P., Skali H. , Anavekar N. et al., Increase in creatinine
and cardiovas-cular risk in patients with systolic dysfunction
after myocardial infarc-
tion, J Am Soc Nephrol 17 (2006), pp. 2886–28917 Weinfeld
MS, Chertow GM, Stevenson LW. Aggravated renal dysfunc-
tion during intensive therapy for advanced chronic heart
failure. AmHeart J. 1999;138:285–90
8 Bayliss J, Norell M, Canepa-Anson R, Sutton G,Poole-Wilson P.
Un-treated heart failure: clinical and neuroendocrine effects of
introducingdiuretics. Br Heart J. 1987; 57:17-22.
9 Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB,
Cohn JN.Acute vasoconstrictor response to intravenous furosemide in
patients
with chronic congestive heart failure. Activation of the
neurohumoralaxis. Ann Intern Med. 1985;103:1-6.
10 Felker GM, O’Connor CM. Inotropic therapy for heart failure:
an evi-dence-based approach. Am Heart J.2001;142:393 401.
11 [No authors listed]. Intravenous nesiritide vs nitroglycerin
for treat-ment of decompensated congestive heart failure: a
randomized con-trolled trial. JAMA. 2002;287:1531-40
12 Wang DJ, Dowling TC, Meadows D, et al. Nesirit ide does not
improve
renal function in patients with chronic heart failure and
worsening se-rum creatinine. Circulation. 2004;110:1620-5.
13 Jaski BE, Miller D. Ultraltration in decompensated heart
failure. CurrHeart Fail Rep. 2005;2:148–54
14 Gheorghiade M, Konstam MA, Burnett JC, Jr, et al. Short-term
clini-cal effects of tolvaptan, an oral vasopressin antagonist, in
patients hos-pitalized for heart failure: The EVEREST Clinical
Status Trials. JAMA.2007;297:1332–43
15 Konstam MA, Gheorghiade M, Burnett JC, Jr, et al. Effects of
oral tolvap-tan in patients hospitalized for worsening heart
failure: The EVERESTOutcome Trial. JAMA. 2007;297:1319–31
16 Hillege H.L., Nitsch D. ,Pfeffer M.A et al., Renal
function as a predictorof outcome in a broad spectrum of patients
with heart failure, Circula-tion 113 (2006), pp. 671–678.
17 Nohria A., Hasselblad V. ,Stebbins A. et al., Cardiorenal
interactions—
insights form the ESCAPE trial, J Am Coll Cardiol
51 (2007), pp. 1268– 1274.
18 Jie K.E, Verhaar M.C. and Cramer M.J. et al., Erythropoietin
and thecardiorenal syndrome: Cellular mechanisms on the cardiorenal
con-nectors, Am J Physiol Renal Physiol 291 (2006), pp.
F932–F944
19 Fu P. ,Arcasoy M.O., Erythropoietin protects cardiac myocytes
againstanthracycline -induced apoptosis, Biochem Biophys Res Commun
354 (2007), pp. 372–378
20 Riksen N.P., Hausenloy D.J., Yellon D.M., Erythropoietin:
ready forprime-time cardioprotection, Trends Pharmacol Sci
29 (2008), pp. 258– 267.
21 Brady J.P. and Hasbargen J.A., A review of the effects of
correction ofacidosis on nutrition in dialysis patients, Semin Dial
13 (2000), pp. 252– 255
22 Figueras J., Stein L., Diez V., Weil M.H. , Shubin H.,
Relationship between
pulmonary hemodynamics and arterial pH and carbon dioxide
tensionin critically ill patients
23 Prabhu SD Cytokine mediated modulation of cardiac function.
Circ.res.2004;95;1140-45
24 Schiffrin E.L et al. Chronic Kidney Disease: Effects on the
Cardiovascu-lar System Circ 2007;116:85
25 Muntner PHJ, Astor BC, Folsom AR, Coresh J:Traditional and
non-tra-ditional risk factors predict coronary heart disease in
chronic kidneydisease:Results from the atherosclerosis risk in
communities study. JAm.soc. Nephrol 2005;16:529-538
26 Levin A et al Left ventricular mass index increasing in early
renal dis-ease and impact of decline in hemoglobinAJKD
1999;34(1):1225-34
27 Blacher J,Guerin JP, Pannier B et al Arterial calcications,
artrerial stiff -ness, and cardiovascular risk in end – stage
renal disease. Hypertension2001:38:938-942
28 Block GA, Hulbert Shearon TE, Levin NW, Port FK: Association
of se-rum phosphorus and calcium * phosphate product with mortality
riskin chronic haemodialysis patients: Am j Kidney disease
1998;31:607-617
29 Himmelfarb J , Stenvinkel P, Ikizler TA, Hakim RM :The
elephant ofuremia:Oxidative stress as a unifying concept of
cardiovascular diseasein uremia. Kidnay Int 2002;62:1524-1538
30 Stam F, van GC, Becker A, et al. Endothelial
dysfunction contrib-utes to renal function-associated
cardiovascular mortality in a popula-
-
8/18/2019 Nephrology 02
5/5
Cardio-Renal Syndrome
689
tion with mild renal insufciency: the Hoorn study. J Am Soc
Nephrol(2006) 17:537–545
31 Suliman M , Barany P,Kalanther Zadeh K,et al Homocysteine in
uremia:A puzzling and conicting story. Nephrol Dial transplant
2005;20:16-21
32 Fliser D. Asymmetric Dimethyl arginine : A cardiovascular
risk factor inrenal disease ? Kidney Int2002:62
(Suppl.82):S12-22
33 Locatell i F, Aljama P,Barany P, et al: Revised European best
practice
guidelines for the management of anemia in patients with chronic
renalfailure. Nephrol Dial Transplant 2004;19 (Suppl 2):ii 1-47
34 Wilmer WA, Rovin BH,Hebert CJ, et al :Management of
glomerularproteinuria: A commentary. J Am Soc Nephrol
2003;14:3217-3232
35 Chertow GM, Burke SK, Raggi P :Sevalamer attenuates the
progressionthe progression of coronary and aortic calcication in
hemodialysispatients.Kidney Int.2002:62:245- 252
36 Strippoli GF, Navaneethan SD, Johnson DW, et al. Effects of
statins in
patients with chronic kidney disease: meta-analysis and
meta-regres-sion of randomised controlled trials BMJ
2008;336:645-651
37 Theodoros I. Kassimatis, Panagiotis A. Konstantinopoulos
Statins inPatients With Chronic Kidney Disease: A Double-Edged
Sword? J AmColl Cardiol, 2008; 52:1679
38 Cunningham P.N., Dyanov H.M., Park P., Wang J., Newell K.A.
and QuiggR.J., Acute renal failure in endotoxemia is caused by TNF
acting directlyon TNF receptor-1 in kidney, J Immunol
168 (2002), pp. 5817–5823
39 Kumar A, Paladugu B, Mensing J, Kumar A. , Parrillo J.E.,
Nitric oxide-de-pendent and independent mechanisms are involved in
TNF-α induceddepression of cardiac myocyte contractility, Am J
Physiol Regul IntegrComp Physiol 292(2007), R1900–R1906
40 Honore P.M., Jamez J. , M. Wauthier et al., Prospective
evaluation ofshort-term, high-volume isovolemic hemoltration on the
hemody-namic course and outcome in patients with intractable
circulatoryfailure resulting from septic shock. Crit Care Med
28 (2000), pp. 3581– 3587