Embed Size (px)
Citation preview
e220 Copyright © SLACK Incorporated
FEATURE ARTICLE
Neonatal Intestinal Obstruction SyndromeManuel Gil Vargas, MD; Mariana L. Miguel-Sardaneta, MD; Michelle Rosas-Téllez, MD; Dayana Pereira-Reyes, MD; and Jaime M. Justo-Janeiro, MD
ABSTRACTNeonatal intestinal obstruction is caused by an anatomical abnormality that produces
bowel movement failure. Intestinal obstruction presents with three classic clinical signs:
vomiting, abdominal distention, and failure to pass meconium. Intestinal obstruction is one
of the most common causes for admitting a pediatric patient to the pediatric surgery unit
in his or her first weeks of postnatal life. Congenital obstruction of the digestive tract in
neonates is a common problem, with the most frequent cause being anorectal malforma-
tions (41%), followed by esophageal obstruction (24%), and duodenal obstruction (20%).
[Pediatr Ann. 2018;47(5):e220-e225.]
Neonatal intestinal obstruc-tion is caused by an anatomi-cal abnormality that leads to
bowel movement failure. Intestinal obstruction usually presents with three clinical signs: vomiting, ab-dominal distention, and failure to pass meconium.1
The word “obstruction” comes from the Latin “obstruyer,” which means to plug, pointing to a mechanical impedi-ment.2 Congenital obstruction of the digestive tract in neonates is a common problem, with the most common causes being anorectal malformations (41%),
esophageal obstruction (24%), and duo-denal obstruction (20%).3
Obstructive syndrome is character-ized by interference with the flow of gases, liquids, and solids, and is mani-fested by vomiting, abdominal disten-tion, and absence of bowel movements. It can be classified in three ways. The first is mechanical, which is either in-trinsic (atresia, stenosis, membrane) or extrinsic (malrotation or Ladd’s bands). The second is functional, such as Hirschsprung’s disease, meconium ile-us, or necrotizing enterocolitis. The third is according to the level of obstruction,
which can be high, medium or low (ie, above the angle of Treitz,, between the angle of Treitz and the ileocecal valve, or below it, respectively).4
Neonatal intestinal obstruction usual-ly manifests with signs such as maternal polyhydramnios, vomiting, abdominal distension, and failure to pass meconi-um within 24 hours after birth.1 Changes that occur in the course of an intestinal obstruction as a result of the existing ob-stacle will cause an accumulation of liq-uids, gases, and alterations of the secre-tion and absorption above the occlusive lesion, giving rise to a whole cascade of events.5
SIGNS AND SYMPTOMS ARE THE BASIS OF DIAGNOSIS Polyhydramnios
Polyhydramnios is defined as the presence of an amniotic fluid index greater than 25 cm in obstetric ultra-sound using Phelan’s method.6 This method adds together the deepest pocket measured vertically in each of the four quadrants in which the uterus is divided, through two perpendicular lines (a vertical one from the symphysis of the pubis to the fundus of the uterus, and a horizontal one passing through the umbilicus).6 It occurs due to an im-balance between the inflow and outflow of amniotic fluid. Approximately 30% of cases with polyhydramnios are as-sociated with fetal anomaly,7 with gas-trointestinal abnormalities being the
Manuel Gil Vargas, MD, is the Head, Surgery Division, General Hospital of Puebla. Mariana L. Miguel-
Sardaneta, MD, is a Pediatrician, Health Services of the State of Puebla. Michelle Rosas-Téllez, MD,
is a Social Services Medical Intern, Autonomous University of the State of Puebla. Dayana Pereira-
Reyes, MD, is a Social Services Medical Intern, Autonomous University of the State of Puebla. Jaime
M. Justo-Janeiro, MD, is an Investigator and a Professor of Surgery, School of Medicine, Autonomous
University of the State of Puebla.Address correspondence to Manuel Gil Vargas, MD, Calle 5 sur No. 5305 interior 201. CP 72400,
Mexico; email: [email protected]: The authors have no relevant financial relationships to disclose.doi:10.3928/19382359-20180425-02

PEDIATRIC ANNALS • Vol. 47, No. 5, 2018 e221
FEATURE ARTICLE
most frequent malformations. The risk of developing a fetal anomaly increases significantly as the amount of amniotic fluid increases.7 Ultrasonographic ab-normalities of small bowel atresia are manifested by dilatation of bowel loops distal to the duodenum in the third tri-mester of pregnancy.8
Jejunum atresia is associated with polyhydramnios in 24% of cases.9 The use of obstetrical ultrasound allows the provision of neonatal care in the event of a congenital malformation diagnosis and the timely transfer to specialized centers. The development of innovative surgical techniques allows for the improvement of survival and future quality of life in children who suffer from this disease.8
Vomiting The occurrence of vomiting is more
frequent when the obstruction level is high. When at the duodenum, vomiting will depend on whether the obstruction is above the duodenal papilla or not. If it is above, then vomiting will be similar to pyloric stenosis, with absence of bile and pancreatic juice. If it is below the duodenum, then there will be loss of bile and pancreatic juice, which increases the loss of bicarbonate.2
The classic teaching in pediatric sur-gery is that vomiting of biliary contents in newborns should be attributed to in-testinal obstruction until proven other-wise. Because bile enters the intestine in the second part of the duodenum, obstruction below this level can result in vomiting bile. In newborns, this may be associated with surgical conditions, including intestinal atresia, malrotation, meconium ileus, necrotizing enterocoli-tis, and Hirschsprung’s disease.10
General symptoms depend on dehy-dration and hypovolemia; in cases of strangulation, there may be fever, leuko-cytosis, and increased tenderness of the abdomen or hernial sac.2
Abdominal Distension Small bowel obstruction produces
accumulation of liquids and gases in the portion next to the obstruction, causing distension of the intestine, which is initi-ated by gas, ingested fluid, and digestive secretions. Gas is derived from swallow-ing and bacterial fermentation in the in-testine. Fluid comes from swallowing as well as salivary, gastric, biliopancreatic, and intestinal secretions. With dehydra-tion, there is loss of water and electro-lytic alteration. Finally, there may be edema and venous stasis, which can lead to perforation and sepsis.11
Absence of Bowel Movements Meconium, the first deposition of
the newborn, is expelled between 12 and 48 hours after birth; its texture is viscous, sticky, and blackish green. It is composed of water, lipids, proteins, cholesterol precursors, free fatty acids, products of amniotic fluid, epithelial cells, bile, and intestinal secretions.12 Failure to pass meconium, when asso-ciated with other clinical data, indicates neonatal bowel obstruction. There is a lack of propulsion of intestinal con-tents, either partial or total. The cause may be mechanical or may be due to alterations in intestinal motility.13
In partial obstructions, there may be a reduced elimination of intestinal con-tents and gases. In colonic and partial obstructions, especially on the left, there may be what is called “pseudodiarrhea,” in which there are aqueous losses caused by hypersecretion above the obstacle. In total obstructions, there may be an elimination of preexisting content in the colon at the onset.2
FREQUENT PATHOLOGIES OF INTESTINAL OBSTRUCTION Intestinal Atresia
Intestinal atresia is the most common cause of neonatal intestinal obstruction.
The most common sites are the ileum (43.2%), jejunum (31%), duodenum (20.9%), and colon (4.72%).5 Mortality from atresia of the ileum is higher than that of the duodenum and has a higher incidence of early perforation. Duodenal atresia results from congenital failure of recanalization, which usually occurs at 9 to 11 weeks of gestation.5
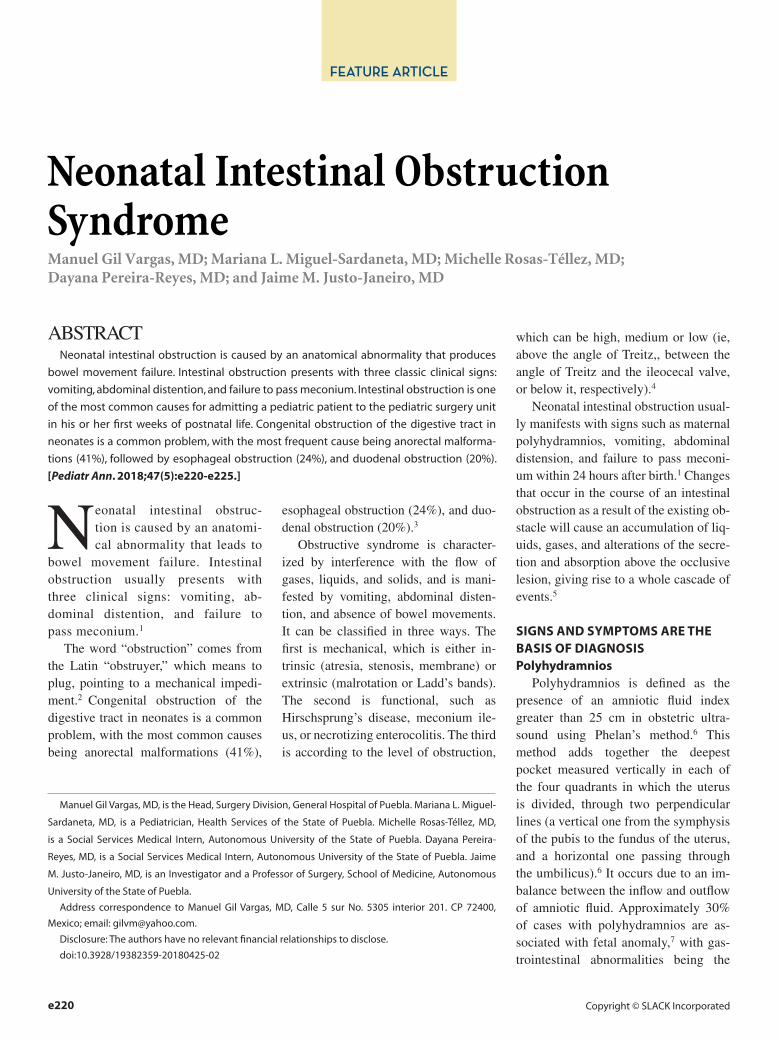
Prenatal diagnosis can be detected by the presence of polyhydramnios. Clini-cally, all patients with atresia present with bilious vomiting, except for those patients with obstructions found above the ampulla5 (Figure 1).
Hirschsprung’s Disease Hirschsprung’s disease is defined
as the congenital absence of neuronal ganglion in the intrinsic intestinal nerve plexus that results in overcontraction of the affected segment.14 Although rare (1 in 5,000 live births), it is one of the leading causes of intestinal obstruction and abdominal surgery in the newborn.14 The clinical presentation is delayed due to variability at onset of symptoms and lack of specificity.9 Pathogenic bases and genetic aspects of the disease have been established, including 13 genes involved in morphogenesis and differen-tiation of the enteric nervous system.15
The initial diagnosis is based on the clinical picture, which includes intermit-tent constipation, abdominal distension, and vomiting. If constipation does not have a mechanical cause (intestinal atre-sia, meconium ileus, malrotation, or im-perforate anus), Hirschsprung’s disease should be considered.
Histological study is the gold stan-dard for diagnosis.15 Before performing corrective surgery, diagnostic certainty should be established. A diagnosis is only confirmed with a biopsy of the rectal wall, which has a sensitivity and specificity close to 100%, according to the quality of samples and the experi-
e222 Copyright © SLACK Incorporated
FEATURE ARTICLE
ence of the pathologist who is perform-ing the evaluation.14 An adequate rectal biopsy (3 cm above the dentate line and
with an adequate amount of mucosa) is required, and appropriate histologi-cal sample processing. De la Torre and
Santos15 emphasize the use of intestinal biomarkers, mainly calretinin, which is absent from nerve fibers in the colon of patients with Hirschsprung’s disease but present in healthy patients.
Intestinal Malrotation Intestinal malrotation is the third
most common cause of neonatal intes-tinal obstruction, accounting for 11.7% of cases.9 Rotational abnormalities of the midgut include a wide spectrum of incomplete malrotation situations during fetal development. It may develop in iso-lation, but in some sufficiently extensive series, approximately 46% were associ-ated with congenital abnormalities.16 It may be paucisymptomatic or even as-ymptomatic, and can remain throughout the patient’s life. The first manifestation is usually bilious vomiting, because the obstruction is distal to the ampulla of Vater. Less common symptoms would be meteorism (tympanites), constipa-tion, and gastrointestinal hemorrhage.16
Meconium Ileus Meconium ileus is the accumulation
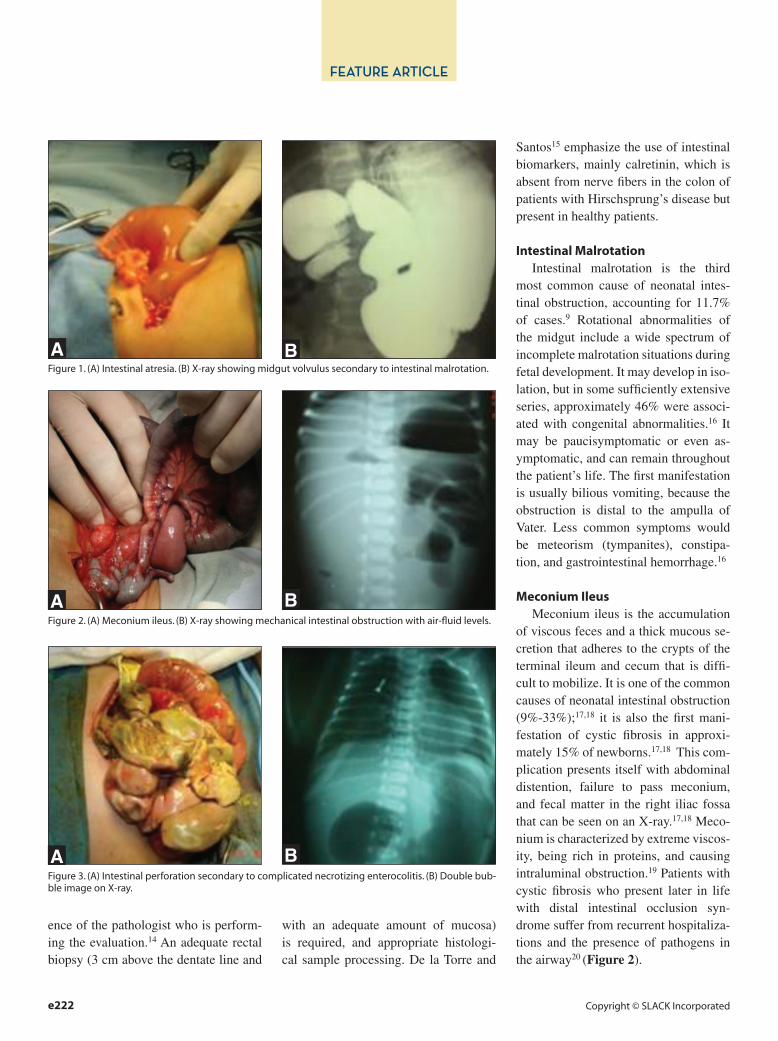
of viscous feces and a thick mucous se-cretion that adheres to the crypts of the terminal ileum and cecum that is diffi-cult to mobilize. It is one of the common causes of neonatal intestinal obstruction (9%-33%);17,18 it is also the first mani-festation of cystic fibrosis in approxi-mately 15% of newborns.17,18 This com-plication presents itself with abdominal distention, failure to pass meconium, and fecal matter in the right iliac fossa that can be seen on an X-ray.17,18 Meco-nium is characterized by extreme viscos-ity, being rich in proteins, and causing intraluminal obstruction.19 Patients with cystic fibrosis who present later in life with distal intestinal occlusion syn-drome suffer from recurrent hospitaliza-tions and the presence of pathogens in the airway20 (Figure 2).
Figure 1. (A) Intestinal atresia. (B) X-ray showing midgut volvulus secondary to intestinal malrotation.
A B
Figure 2. (A) Meconium ileus. (B) X-ray showing mechanical intestinal obstruction with air-fluid levels.
A B
Figure 3. (A) Intestinal perforation secondary to complicated necrotizing enterocolitis. (B) Double bub-ble image on X-ray.
A B
PEDIATRIC ANNALS • Vol. 47, No. 5, 2018 e223
FEATURE ARTICLE
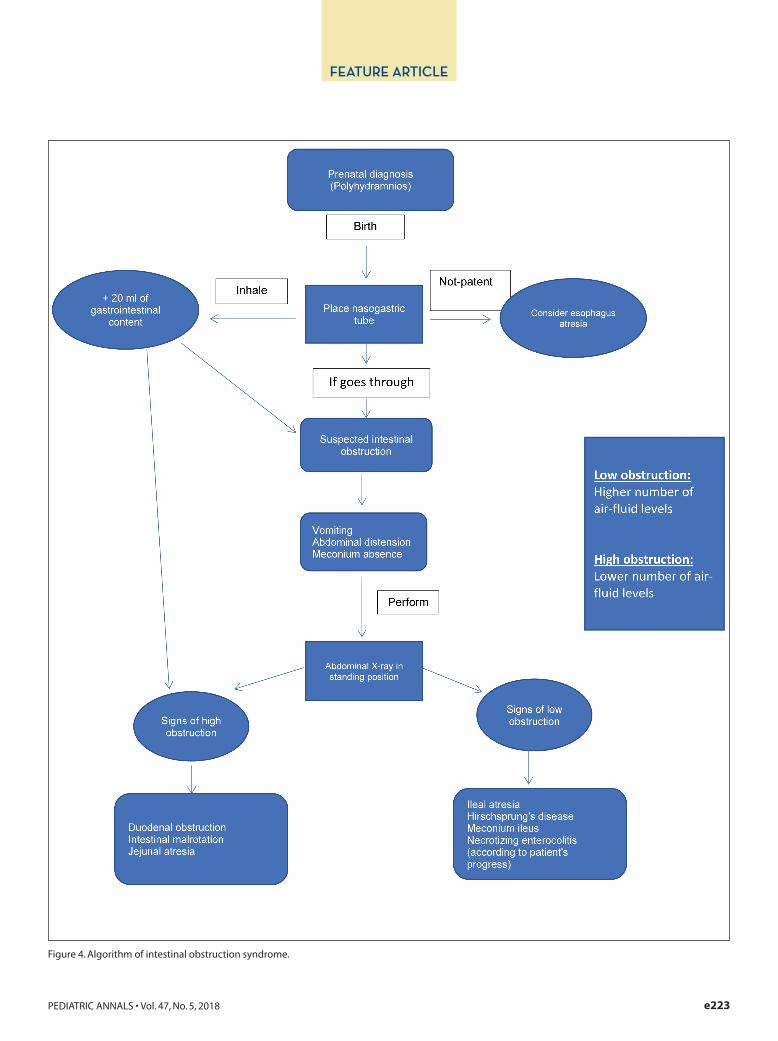
Figure 4. Algorithm of intestinal obstruction syndrome.

e224 Copyright © SLACK Incorporated
FEATURE ARTICLE
Necrotizing Enterocolitis Necrotizing enterocolitis is the
most frequent cause of acquired gas-trointestinal disease and surgical emergency in the neonate. It predomi-nantly affects premature infants with low birth weight, with a reported in-cidence of 5% to 15%.21 The patho-genesis is multifactorial and has not yet been clearly defined. Mortality remains high and varies from 20% to 50% depending on the severity of nec-rotizing enterocolitis and gestational age of the neonate.21
In the early stages, necrotizing en-terocolitis is difficult to diagnose be-cause the symptoms are nonspecific, insidiously progressing for several days to a fulminating onset with dif-ferent gastrointestinal signs, and fi-nally to multiorgan dysfunction and shock. The signs may present as ab-dominal distention, bilious vomiting, and visible or hidden blood in feces. A small number of infants has a pal-pable abdominal mass and/or persis-tence of intestinal obstruction data21 (Figure 3).
DISCUSSIONFigure 4 provides a diagnostic
algorithm for neonatal intestinal ob-struction syndrome. Radiological signs characteristic of each disease can be observed, and they are divided into high and low intestinal obstruc-tions. High intestinal obstruction is the most frequent surgical emergency in the unborn. This includes the gas-tric obstructions that cause the “sin-gle bubble sign”; duodenal obstruc-tion will result in the “double bubble sign,” which occurs with the existence of a duodenal obstruction with dila-tation of the gastric chamber and the duodenal bulb.
Intestinal obstruction is manifested radiologically according to the num-
ber of air-fluid levels (ie, the greater the number of air-fluid levels, the low-er the obstruction; whereas the lower the number of levels, the higher the obstruction). In Hirschsprung’s dis-ease, signs of low intestinal obstruc-tion are observed, so one should per-form an opaque enema, in which the transition from a normal or slightly reduced (aganglionic) intestine cali-ber to a distended one (ganglionic) is observed. In meconium ileus, signs of low intestine obstruction and images of “bubbles” or “breadcrumbs” are observed in the right iliac fossa due to the mixture of air and meconium.22
CONCLUSIONNeonatal intestinal obstruction
syndrome continues to be a diagnostic challenge; however, by using obstetri-cal ultrasound a timely diagnosis can be obtained. In this literature review, it was shown that intestinal atresia is the most common cause of neonatal intestinal obstruction. Worth noting is the importance of joint collaboration between the obstetrician at the time of prenatal diagnosis, the pediatrician accepting the newborn in the delivery room, and the pediatric surgeon, who will determine the treatment accord-ing to the etiology.
REFERENCES 1. Chen H, Jiang H, Kan A, et al. Intestinal ob-
struction due to dual gastrointestinal atresia in infants: diagnosis and management of 3 cases. BMC Gastroenterol. 2014;14:108. doi:10.1186/1471-230X-14-108.
2. Galindo F. Síndromes obstructivos y seu-doobstructivos del tubo digestivo. Enciclope-dia de Cirugía Digestiva. 2011;I-127:1-23.
3. Cano Muñoz I, Montoya Mendoza N. Ob-strucción duodenal en pacientes pediátricos. Anales de Radiología México. 2011;4:258-273.
4. Chi Argüelles D, Cobos Estrada G. Este-nosis congénita de íleon en un lactante de 5 meses de edad con síndrome de obstruc-ción intestinal. Bol Med Hosp Infant Mex. 2011;68(5):380-384.
5. Romea I, Moreno Mirallas M, Garrido Calvo A. Obstrucción intestinal. Medicina Integral. 2001;38(2):52-56.
6. Góngora Rodríguez J, Manzanares Galán S. Polihidramnios: diagnóstico y conducta obstétrica. http://www.hvn.es/servicios_asis-tenciales/ginecologia_y_obstetricia/ficheros/actividad_docente_e_investigadora/clases_residentes/2013/clase2013_polihidramnios_diagnostico_y_manejo_obstetrico.pdf. Ac-cessed May 3, 2018.
7. Tato S, Cabezas N, Gómez JA, Martínez JA. Diagnóstico prenatal de atresia ileal asociada a peritonitis meconial. Prog Obstet Ginecol. 2016;59(1):21-23.
8. Sepúlveda AC, Buena EP, Partida I, Cam-pos I. Abordaje quirúrgico para cirugía por obstrucción intestinal en neonatos. Rev Med Inst Mex Seguro Soc. 2015;53(6):698-703.
9. Verma A, Nain Rattan K, Yadav R. Neona-tal intestinal obstruction: a 15 year experi-ence in a tertiary care hospital. J Clin Diagn Res. 2016;10(2):SC10-SC13. doi:10.7860/JCDR/2016/17204.7268.
10. Walker G, Neilson A, Young D, Raine PA. Colour of bile vomiting in intestinal obstruc-tion in the newborn: questionnaire study. BMJ. 2006;332(7554):1363. doi:10.1136/bmj.38859.614352.55.
11. Ruíz F. Síndrome de obstrucción intestinal. Revista del Hospital General “La Quebra-da.” 2003;2(1):36-43.
12. Manrique López S, Puentes García S, Or-juela Velasco M. Meconio: vehículo de bio-marcadores de exposición a sustancias psi-coactivas en gestantes. http://unicolmayor.edu.co/publicaciones/index.php/nova/article/view/86/171. Accessed April 25, 2018.
13. Peñaranda Ávila R, Aguilar Liendo A. Carac-terísticas de las deposiciones de recién naci-dos alimentados con leche materna exclusiva. Rev Soc Bol Ped. 1996;35(1):11-15.
14. Menchaca-Cervantes C, Rodríguez-Velasco A, Ramón-García G, Rendón-Macías M. En-fermedad de Hirschsprung La inmunohisto-química como apoyo para el diagnóstico. Rev Med Inst Mex Seguro Soc. 2013;51(6):610-613.
15. De la Torre L, Santos K. Hirschsprung dis-ease. Evaluation of calretinin and S-100 as ancillary methods for the diagnosis of agan-glionosis in rectal biopsies. Acta Pediatr Mex. 2012;33(5):246-251.
16. Guerrero Vázquez J. Malrotación intestinal. http://www.webpediatrica.com/casosped/pdf/117_malrotacion_intestinal.pdf. Ac-cessed April 25, 2018.
17. Fernández-Ibieta M, Ayuso-González L, Fernández-Córdoba M, Argumosa-Salazar Y, González-Piñera J. Opciones de trata-miento del síndrome de obstrucción intesti-nal distal: ¿y si los enemas fallan? An Pedi-

PEDIATRIC ANNALS • Vol. 47, No. 5, 2018 e225
FEATURE ARTICLE
atr (Barc). 2016;84(1):54-55. doi:10.1016/j. anpedi.2015.05.009.
18. Henderson LB, Doshi VK, Blackman SM, et al. Variation in MSRA modifies risk of neonatal intestinal obstruction in cystic fi-brosis. PLoS Genet. 2012;8(3):e1002580. doi:10.1371/journal.pgen.1002580.
19. Caty MG, Escobar MA. Meconium disease.
In: Holcomb GW, Murphy JP, eds. Ashcraft’s Pediatric Surgery. 5th ed. Philadelphia, PA: Saunders Elsevier; 2010:433.
20. Lavie M, Manovitz T, Vilozni D, et al. Long-term follow-up of distal intestinal obstruction syndrome in cystic fibrosis. World J Gastro-enterol. 2015;21(1):318-325. doi:10.3748/wjg.v21.i1.318.
21. Gasque-Góngora J. Revisión y actualización de enterocolitis necrosante. Rev Mex Pediatr. 2015;82(5):175-185.
22. Raposo Rodríguez L, Anes González G, Pereira Menéndez C. Patología intestinal en el neonato. Sociedad Española de Ra-diología Médica. 2012;1-30. doi:10.1594/seram2012/S-0612.





























