Embed Size (px)
Citation preview

Neonatal Intensive Care for LowBirthweight Infants: Costs and Effectiveness
December 1987
NTIS order #PB88-158902

Recommended Citation:U.S. Congress, Office of Technology Assessment, Neonatal Intensive Care for Low Birth-weight Infants: Costs and Effectiveness (Health Technology Case Study 38), OTA-HCS-38(Washington, DC: U.S. Congress, Office of Technology Assessment, December 1987). Thiscase study was performed as part of OTA’s assessment of Healthy Children: Investing inthe Future.
Library of Congress Catalog Card Number 87-619883
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402-9325
(order form can be found in the back of this case study)

Preface
Neonatal Intensive Care for Low Birth weightInfants: Costs and Effectiveness is Case Study 38in OTA’s Health Technology Case Study Series.This case study has been prepared in connectionwith OTA’s assessment, Healthy Children: Invest-ing in the Future, which was requested by theHouse Energy and Commerce Committee and theSenate Labor and Human Resources Committee.
OTA case studies are designed to fulfill twofunctions. The primary purpose is to provideOTA with specific information that can be usedin forming general conclusions regarding broaderpolicy issues. The first 19 cases in the Health Tech-nology Case Study Series, for example, were con-ducted in conjunction with OTA’s overall projecton The Implications of Cost-Effectiveness Anal-ysis of Medical Technology. By examining the 19cases as a group and looking for common prob-lems or strengths in the techniques of cost-effec-tiveness or cost-benefit analysis, OTA was ableto better analyze the potential contribution thatthose techniques might make to the managementof medical technology and health care costs andquality.
The second function of the case studies is toprovide useful information on the specific tech-nologies covered. The design and the funding lev-els of most of the case studies are such that theyshould be read primarily in the context of the as-sociated overall OTA projects. Nevertheless, inmany instances, the case studies do represent ex-tensive reviews of the literature on the efficacy,safety, and costs of the specific technologies andas such can stand on their own as a useful contri-bution to the field.
Case studies are prepared in some instances be-cause they have been specifically requested bycongressional committees and in others becausethey have been selected through an extensive re-view process involving OTA staff and consulta-tions with the congressional staffs, advisory panelto the associated overall project, the Health Pro-gram Advisory Committee, and other experts invarious fields. Selection criteria were developedto ensure that case studies provide the following:
. examples of types of technologies by func-tion (preventive, diagnostic, therapeutic, andrehabilitative);
●
●
●
●
●
●
●
examples of types of technologies by physi-cal nature (drugs, devices, and procedures);examples of technologies in different stagesof development and diffusion (new, emerg-ing, and established);examples from different areas of medicine(e.g., general medical practice, pediatrics, ra-diology, and surgery);examples addressing medical problems thatare important because of their high frequency
or significant impacts (e. g., cost);examples of technologies with associated highcosts either because of high volume (for low-cost technologies) or high individual costs;examples that could provide information ma-terial relating to the broader policy and meth-odological issues being examined in the par-ticular overall project; andexamples with sufficient scientific literature.
Case studies are either prepared by OTA staff,commissioned by OTA and performed under con-tract by experts (generally in academia), or writ-ten by OTA staff on the basis of contractors’papers.
OTA subjects each case study to an extensivereview process. Initial drafts of cases are reviewedby OTA staff and by members of the advisory
panel to the associated project. For commissionedcases, comments are provided to authors, alongwith OTA’s suggestions for revisions. Subsequentdrafts are sent by OTA to numerous experts forreview and comment. Each case is seen by at least30 reviewers, and sometimes by 80 or more out-side reviewers. These individuals may be fromrelevant Government agencies, professional so-cieties, consumer and public interest groups, med-ical practice, and academic medicine. Academi-cians such as economists, sociologists, decisionanalysts, biologists, and so forth, as appropriate,also review the cases.
Although cases are not statements of officialOTA position, the review process is designed tosatisfy OTA’s concern with each case study’sscientific quality and objectivity. During the vari-ous stages of the review and revision process,therefore, OTA encourages, and to the extent pos-sible requires, authors to present balanced infor-mation and recognize divergent points of view.

-
Health Technology Case Study Seriesa
Case Study Case study title; author(s); Case Study Case study title; author(s);Series No. OTA publication numberb Series No. OTA publication numberb
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
Formal Analysis, Policy Formulation, and End-Stage RenalDisease;
Richard A. Rettig (OTA-BP-H-9 (1))C
The Feasibility of Economic Evaluation of Diagnostic Pro-cedures: The Case of CT Scanning;
Judith L. Wagner (OTA-BP-H-9(2))Screening for Colon Cancer: A Technology Assessment;
David M. Eddy (OTA-BP-H-9(3))Cost Effectiveness of Automated Multichannel ChemistryAnalyzers;
Milton C. Weinstein and Laurie A. Pearlman(OTA-BP-H-9(4))
Periodontal Disease: Assessing the Effectiveness and Costs ofthe Keyes Technique;
Richard M. Scheffler and Sheldon Rovin(OTA-BP-H-9(5))
The Cost Effectiveness of Bone Marrow Transplant Therapyand Its Policy Implications;
Stuart O. Schweitzer and C. C. Scalzi (OTA-BP-H-9(6))Allocating Costs and Benefits in Disease Prevention Programs:An Application to Cervical Cancer Screening;
Bryan R. Luce (Office of Technology Assessment)(OTA-BP-H-9(7))
The Cost Effectiveness of Upper Gastrointestinal Endoscopy;Jonathan A. Showstack and Steven A. Schroeder(OTA-BP-H-9(8))
The Artificial Heart: Cost, Risks, and Benefits;Deborah P. Lubeck and John P. Bunker(OTA-BP-H-9(9))
The Costs and Effectiveness of Neonatal Intensive Care;Peter Budetti, Peggy McManus, Nancy Barrand, andLu Ann Heinen (OTA-BP-H-9 (1 O))
Benefit and Cost Analysis of Medical Interventions: The Caseof Cimetidine and Peptic Ulcer Disease;
Harvey V. Fineberg and Laurie A. Pearlman(OTA-BP-H-9(11))
Assessing Selected Respiratory Therapy Modalities: Trends andRelative Costs in the Washington, D.C. Area;
Richard M. Scheffler and Morgan Delaney(OTA-BP-H-9(121)
Cardiac Radionuclide Imaging and Cost Effectiveness;
William B. Stason and Eric Fortess (OTA-BP-H-9(13))Cost Benefit Cost Effectiveness of Medical Technologies: ACase Study of Orthopedic Joint Implants;
Judith D. Bentkover and Philip G. Drew (OTA-BP-H-0 (14))Elective Hysterectomy: Costs, Risks, and Benefits;
Carol Korenbrot, Ann B. Flood, Michael Higgins,Noralou Roos, and John P. Bunker (OTA-BP-H-9(15)}
The Costs and Effectiveness of Nurse Practitioners;Lauren LeRoy and Sharon Solkowitz (OTA-BP-H-9(16))
Surgery for Breast Cancer;Karen Schachter Weingrod and Duncan Neuhauser(OTA-BP-H-9(17))
The Efficacy and Cost Effectiveness of Psychotherapy;Leonard Saxe (Office of Technology Assessment)(OTA-BP-H-9 (18))d
Assessment of Four Common X-Ray Procedures;Judith L. Wagner (OTA-BP-H-9 (19))e
‘Available tor sale by the Superintendent of Documents, U. S GovernmentPrlntlng office, Washington, DC, 20402, and by the National TechnicalInformation Serv]ce, 5285 Port Royal Rd., Springfield, VA, 22161. CallOTA’S Publlshlng Office (224-8996) f(or availability and ordering ]ntor-mation.
borlglna] publication numbers appear in parentheses.cThe first 17 cases in the series were 17 separately issued cases In &c/+~r[)undPaper #2 Case Studies of Lfedical Technologiesr prepared In conlunctlonw’]th OTA s August 1980 report The Implicatmns of Cmt-Eflect/veness .,in.;l}rSIS Of )lfedIcJ/ Technology},
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
Mandatory Passive Restraint Systems in Automobiles: Issuesand Evidence;
Kenneth E. Warner (OTA-BP-H-15 (20))f
Selected Telecommunications Devices for Hearing-ImpairedPersons;
Virginia W. Stern and Martha Ross Redden(OTA-BP-H-16(21))g
The Effectiveness and Costs of Alcoholism Treatment;Leonard Saxe, Denise Dougherty, Katharine Esty,and Michelle Fine (OTA-HCS-22)
The Safety, Efficacy, and Cost Effectiveness of TherapeuticApheresis;
John C. Langenbrunner (Office of Technology Assessment)(OTA-HCS-23)
Variation in Length of Hospital Stay: Their Relationship toHealth Outcomes;
Mark R. Chassin (OTA-HCS-24)Technology and Learning Disabilities;
Candis Cousins and Leonard Duhl (OTA-HCS-25)
Assistive Devices for Severe Speech Impairments;Judith Randal (Office of Technology Assessment)(OTA-HCS-26)
Nuclear Magnetic Resonance Imaging Technology: A Clinical,Industrial, and Policy Analysis;
Earl P. Steinberg and Alan Cohen (OTA-HCS-27)Intensive Care Units (ICUs): Clinical Outcomes, Costs, andDecisionmaking;
Robert A. Berenson (OTA-HCS-28)The Boston Elbow;
Sandra J. Tanenbaum (OTA-HCS-29)The Market for Wheelchairs: Innovations and Federal Policy;
Donald S. Shepard and Sarita L. Karen (OTA-HCS-30)The Contact Lens Industry: Structure, Competition, and PublicPolicy;
Leonard G. Schifrin and William J. Rich (OTA-HCS-31 )The Hemodialysis Equipment and Disposable Industry;
Anthony A. Romeo (OTA-HCS-32)Technologies for Managing Urinary Incontinence;
Joseph Ouslander, Robert Kane, Shira Vollmer, and MelvynMenezes (OTA-HCS-33)
The Cost Effectiveness of Digital Subtraction Angiography inthe Diagnosis of Cerebrovascular Disease;
Matthew Menken, Gordon H. DeFriese, Thomas R. Oliver,and Irwin Litt (OTA-HCS-34)
The Effectiveness and Costs of Continuous AmbulatoryPeritoneal Dialysis (CAPD)
William B. Stason and Benjamin A. Barnes (OTA-HCS-35)Effects of Federal Policies on Extracorporeal Shock WaveLithotripsy
Elaine J. Power (Office of Technology Assessment)(OTA-HCS-36)
Nurse Practitioners, Physician Assistants, and Certified Nurse-Midwives: A Policy Analysis;
(OTA-HCS-37)Neonatal Intensive Care for Low Birthweight Infants: Costsand Effectiveness
(OTA-HCS-38)
dBachground paper #3 t. The ]mpllcatlc)ns Of Co5t-Effectj L~enes5 Anal~rs)s (It
,tled)cal Technology.‘Background Paper #5 to The lmplicat]orts of Cost-Effect] ventw And/>rws (dLfedlcal Technology
~Backgrc)und Paper t] to OTA’S Nlay 1982 report Techno/og}’ ami Hand-
icapped People.g~ackground [’aPer gz to Techno/og} .]nd Handicapped Peep/e
iv

OTA Project Staff—Neonatal Intensive Care forLow Birthweight Infants: Costs and Effectiveness
Roger C. Herdman, Assistant Director, OTAHealth and Life Sciences Division
Clyde J. Behney, Health Program Manager
Judith L. Wagner, Project Director
Pony M. Ehrenhaft, Study Director
Other Contributing Staff
David W. Alberts, Research Analyst
Sarah M. Dry, Research Assistant
Maria Hewitt, Analyst
Kerry Britten Kemp, Division Editor
Virginia Cwalina, Administrative Assistant
Carol Ann Guntow, P.C. Specialist
Karen T. Davis, Secretary/Word Processor Specialist
Carolyn Martin, Clerical Assistant

Advisory Panel on Technology and Children’s Health
Harvey Fineberg, ChairmanHarvard School of Public Health
Boston,
LuAnne AdayCenter for Hospital Administration StudiesUniversity of ChicagoChicago, IL
Julianne BeckettChild Health Specialty ClinicUniversity of IowaIowa City, Iowa
Donald BerwickQuality of Care MeasurementsHarvard Community Health PlanBoston, MA
Alexander CapronMedicine and Public PolicyUniversity of Southern CaliforniaLos Angeles, CA
Norman FostProgram on Medical EthicsDepartment of PediatricsUniversity of Wisconsin HospitalMadison, WI
Robert GoldenbergDepartment of Obstetrics and GynecologyUniversity of AlabamaBirmington, AL
tMichael GrossmanHealth Economics ResearchNational Bureau of Economic ResearchNew York, NY
Robert HaggertyW.T. Grant FoundationNew York, NY
Patricia KingGeorgetown Law CenterWashington, DC
MA
Phyllis LeppertDirector of Perinatal ResearchSt. Lukes/Roosevelt Hospital CenterColumbia UniversityNew York, NY
Harvey LevyIEM-PKU Program, Children’s HospitalBoston, MA
Edward LisDivision of Services for Crippled ChildrenUniversity of IllinoisChicago, IL
Joanne MaconHolman Health RegionChicago Department of HealthChicago, IL
John MacQueenChild Health Specialty ClinicUniversity of IowaIowa City, IA
Janet ReisSchool of Nursing/SUNY BuffaloBuffalo, NY
Sarah RosenbaumChildren’s Defense FundWashington, DC
Barbara StarfieldDivision of Health PolicyJohns Hopkins UniversitySchool of Hygiene and Public HealthBaltimore, MD
NOTE: OTA gratefully acknowledges the members of this advisory panel for their valuable assistance andthoughtful advice. The panel does not, however, necessarily approve, disapprove, or endorse this report.OTA assumes full responsibility for the report and the accuracy of its contents.
vi

CONTENTS
CHAPTER 1: SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Scope of the Case Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Organization of the Case Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Summary . . . . . . . . . . . . . . . . . . . . . . . ..., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Supply, Use, and Costs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Mortality and Morbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Financing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cost-Effectiveness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 2: SUPPLY, USE, AND COST OF NEONATAL INTENSIVE CARE . . . . . . . . . . . .Introduction .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .supply . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Utilization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .cost... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 3: EFFECTIVENESS OF NEONATAL INTENSIVE CARE . . . . . . . . . . . . . . . . . . . . . .Introduction ..., ..., ., ..., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Mortality Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Handicap Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .,Neonatal Conditions That Cause Major Mortality and Morbidity . . . . . . . . . . . . . . . . . . . . . . . .
Respiratory Distress Syndrome. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Intraventricular Hemorrhage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Retinopathy of Prematurity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 4: FINANCING NEONATAL INTENSIVE CARE . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Reimbursement Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Medicaid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Expenditures for Neonatal Intensive Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 5: ACCESS TO NEONATAL INTENSIVE CARE . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Level 11 Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Concentration of Births in Level III Hospitals . . . . . . . . . . . . . . . . . .Barriers to Maternal and Neonatal Transport . . . . . . . . . . . . . . . . . .The Tiniest Babies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 6: ECONOMIC ANALYSIS OF NEONATAL INTENSIntroduction . . . . . . ..., . . . . . . . . . . . . . . . . . ..., ..., . . . . .Cost-Effectiveness and Cost-Benefit Studies . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
VE CARE . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . .
Conclusions and Policy Implications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
APPENDIX A: GLOSSARY OF ACRONYMS AND TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .APPENDIX B: ACKNOWLEDGMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33344445677
1111111214
2121212531313537
414142434343
474749505253
57575759
6365
69
(Continued on next page)
vii

CONTENTS—continued
BoxB o x Page
A. How To Interpret the Data in Tables 3, 4, and 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
FiguresFigure No. Page
1. Hospital Cost by Birthweight Group, 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162. Outcomes for Very Low Birthweight Infants ( < 1500 grams) Born in Level III Hospitals,
1960-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303. Outcomes for Extremely Low Birthweight Infants (=1000 grams) Born in Level III
Hospitals, 1960-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
TablesTable No. Page
1.2.3.4.5.6.7.
8.
9.
10.11.12.13.
14.15,
16.
17.
Supply of NICUs and Beds in the United States, 1983 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12NICU Days of Care and Occupancy in the United States, 1983 . . . . . . . . . . . . . . . . . . . . . . . . 13Length of Stay by Birthweight Group, 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Hospital Cost by Birthweight Group, 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Hospital Cost and Length of Stay Per Very Low Birthweight Survivor, 1984 . . . . . . . . . . . . 16Hospital Cost and Length of Stay for Newborns Requiring Assisted Ventilation, 1984 . . . . 17Comparative Neonatal Mortality for Very Low Birthweight Infants Born in Level IIIHospitals, 1975-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Comparative Neonatal Mortality in NICUs for Very Low Birthweight Infants,1975-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Inborn Neonatal Mortality Rates for Very Low Birthweight Infants,Pooled Institutional Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Handicap Rates in Infants With Birthweights Under 800 Grams, 1975-85 . . . . . . . . . . . . . . . . 27Handicap Rates in Infants With Birthweights Between 750 and 1000 Grams, 1975-85 . . . . . 28Handicap Rates in Infants With Birthweights Between 1000 and 1500 Grams, 1975-85 . . . . 29Medicaid Recipients in Neonatal Intensive Care Units, and Medicaid Expenditures,Selected States, 1983-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Regional Neonatal Mortality Rates for Very Low Birthweight Infants, 1976-81 . . . . . . . . . 47Concentration of Births of Infants Weighing Less Than 1500 Gramsin Level 111 Hospitals . . . . . . . . . . . . . . 51Measures of Economic Evaluation of Neonatal Intensive Care for Very LowBirthweight Infants (5 Percent Discount Rate), 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58Cost of Neonatal Intensive Care Per Additional Survivor, 1984 . . . . . . . . . . . . . . . . . . . . . . 59

Chapter 1
Summary and Conclusions

Chapter 1
Summary and Conclusions
INTRODUCTION
Neonatal intensive care is defined by the Amer-ican Academy of Pediatrics as the constant andcontinuous care of the critically ill newborn (2).Although modern, high-technology neonatal in-tensive care units (NICUs) are a relatively recentinnovation, their widespread application has al-ready played a major and definitive role in theimproved survival of low birthweight and prema-ture infants (25). Despite this success, ethical andeconomic concerns remain about this technology.Because of intensive care, some infants, who pre-viously would have died, survive but with seri-ous and permanent handicaps. The double-edgedsword of technology, at ever-increasing costs,both saves and disables babies. This case studyreviews the evidence on the effectiveness of ne-onatal intensive care and addresses a number ofthese related issues:
●
●
●
●
●
●
What are the chances of serious handicapamong surviving very low birthweight in-fants as mortality declines?What changes in technology and medicalpractices are and will affect the chances forsurvival and good developmental outcome?How are decisions made about treatment forextremely premature infants who are at theedge of viability?How much does neonatal intensive care cost?Who pays for treatment, and are there prob-lems with reimbursement?Is there unequal access to neonatal intensivecare? What are the barriers that may prevententry for some babies?What are the long-term economic conse-quences of providing neonatal intensive care?
Scope of the Case Study
Up to half of all patients in neonatal intensivecare are normal birthweight infants with congen-ital anomalies, pneumonia, or other problems.However, this case study limits discussion to lowbirthweight infants ( <2500 grams) for several rea-sons. First, low birthweight infants, particularly
Photo credit: March of Dimes Birth Defects Foundation
those with birthweights below 1500 grams, are atthe greatest risk for high mortality and morbidity.Moreover, outcomes are changing most rapidlyfor these infants, and new technologies currentlyunder investigation hold promise for continuingimprovements in the future. Second, there appearsto be a shift in the patient population in neonatalintensive care, with increasing numbers of bedsoccupied by extremely low birthweight infants.Difficult ethical, social, and economic judgmentsare involved in the decision to treat these infants.Finally, because low birthweight and low socio-economic status are associated, it is likely thatpublic payment programs pay a substantial por-tion of the expense for neonatal intensive care.
Throughout this case study, the term “lowbirthweight infant” is used to refer to infants whoweigh less than 2500 grams at birth.1 “Very lowbirthweight infant” refers to infants with birth-weights of less than 1500 grams, and “extremelylow birthweight infant” describes infants who areborn weighing less than 1000 grams. Gestationalage is likely more important than birthweight indetermining outcome, but the two are highly cor-related. Birthweight is easier and more reliable to
‘For ease of reference, 2500 grams is approximately 5 lb 5 OZ; 1500grams is about 3 lb 3 OZ; and 1000 grams is about 2 lb 2 oz.
3

4
measure, and most of the medical literature andavailable data focus on birthweight alone. Thatbias is reflected in this review.
Under the regionalization concept first intro-duced in the mid-1970s, the most sophisticated ne-onatal intensive care is provided in so-called Level111 hospitals. Level II hospitals also provide in-tensive care services but lack some of the com-ponents and expertise of Level III units, whileLevel I hospitals provide only normal newborncare. The extent to which high-risk mothers andinfants are referred to and treated at the appro-priate level of care is addressed in this study.
Organization of the Case Study
Findings and conclusions about the costs andeffectiveness of neonatal intensive care are sum-marized in the remainder of chapter 1. Chapter
SUMMARY
Supply, Use, and Costs
Between 150,000 and 200,000 infants (4 to 6percent of all newborns) are treated annually inNICUs, and at least one-half of them are lowbirthweight infants. Confusion over which hos-pitals deliver the most intensive v. less special-ized care complicates estimates of the supply ofneonatal intensive care. Of a total of 534 com-bined Level II and Level 111 neonatal intensive careunits in the country, about 420 of them offer verysophisticated Level III services. While many in-dividual neonatal intensive care units are filled toovercapacity, there does not appear to be a short-age of NICUs or intensive care beds nationwide.In 1983, the occupancy rate for NICUs was 73 per-cent, comparable to the national occupancy ratefor all hospital beds.
Neonatal intensive care for very low birth-weight infants ranks among the most costly of allhospital admissions. Although the average hos-pital cost for low birthweight infants ranges fromonly $12,000 to $39,000, the distribution of costsamong patients in the neonatal nursery is highlyskewed. A few infants incur truly extraordinary
2 inventories the national supply of neonatal in-tensive care units and describes recent trends inuse and costs. Chapter 3 reviews mortality andhandicap rate: over time and discusses the out-look for the three clinical problems that accountfor a majority of the deaths and poor outcomesamong very low birthweight infants (respiratorydistress syndrome, intraventricular hemorrhage,and retinopathy of prematurity). Problems infinancing neonatal intensive care, with special em-phasis on Medicaid policies and expenditures, arereviewed in chapter 4. Then, findings of unequalmortality risks in different types of hospitals arereviewed, and possible inequities in access to ne-onatal intensive care are considered (ch. 5). Com-petitive and financial constraints on hospitals andphysicians, as well as ethical considerations, areexplored. Finally, chapter 6 analyzes the lifetimeeconomic implications of neonatal intensive carefor very low birthweight infants and for society.
costs. About half of the variation in costs is ex-plained by four risk factors: birthweight, survivalto hospital discharge, use of assisted ventilation,and surgical intervention. A primary predictor ofcost is birthweight; costs increase as birthweightfalls. The average cost for a very low birthweightsurvivor is from $31,000 to $71,000. The tiniestinfants who survive, those with birthweights un-der 750 grams, have the longest average hospitalstays, about 98 days, and the highest costs, aver-aging $62,000 to $150,000. Hospitals report in-creasing numbers of these tiniest babies in theirNICUs. (About 8,500 infants weighing less than750 grams are born each year in the UnitedStates. )
Mortality and Morbidity
Neonatal intensive care, along with improvedobstetrical practices, is in large part responsiblefor the remarkable decline in birthweight-specificneonatal mortality rates over the past 25 years.Neonatal mortality for infants with birthweightsof 1000 to 1500 grams has fallen from more than50 percent to only 10 percent. And whereas morethan 90 percent of all infants weighing under 1000

5
grams died in 1960, the neonatal mortality ratefor this group now is about 50 percent. Thisachievement reflects improvements primarily inthe 750- to 1000-gram birthweight group (morethan two-thirds survive today), because mortal-ity in the smallest and most premature infants,those under 750 grams, is still very high.
Even among the most sophisticated neonatal in-tensive care centers, the risk of mortality for verylow birthweight infants varies substantially. In themid-1980s for example, the mortality rates re-ported for the most vulnerable group, infants withbirthweights under 750 grams, varied from 28 per-cent in one university-affiliated center, to 53 per-cent in another, and 74 percent in a third center.The success of some centers indicates that the tech-nology of neonatal intensive care is changing veryrapidly.
The rate of serious long-term disability increaseswith decreasing birthweight, but within eachbirthweight group, the proportion of NICU surviv-ors who have serious handicaps has not changedsignificantly since the introduction of neonatal in-tensive care. Because many very sick newbornswho previously would have died are now surviv-ing, an increasing rate of handicap might havebeen expected. OTA concludes that neonatal in-tensive care has contributed to improved long-term developmental outcomes for premature in-fants. The great decline in mortality among allsubgroups of very low birthweight infants overthe last 10 years, however, means there are nowlarger absolute numbers of both seriously handi-capped and normal survivors. For every 100 verylow birthweight infants treated in today’s NICUs,about 27 will die before hospital discharge, 16 willbe seriously or moderately disabled, and 57 willbe normal children, though some will developmild learning disabilities.
The majority of deaths in the extremely lowbirthweight group are attributable to respiratorydistress syndrome (RDS) or intraventricular hem-orrhage. The incidence of both these clinical prob-lems, -as well as the incidence of retinal disease,increases with progressively lower birthweights.About half of all very low birthweight infantshave RDS, and one-third have brain hemorrhages.Infants with severe hemorrhage have both high
mortality and, for those who survive, a high rateof later neurodevelopmental disability. Retinaldisease, which is almost entirely restricted to verylow birthweight infants, causes blindness in about1 percent of infants with birthweights between1000 and 1500 grams and in about 5 to 11 per-cent of infants with birthweights below 1000grams.
RDS is the most common problem in the neo-natal nursery, and assisted mechanical ventilationis usually essential to help babies in respiratorydistress breathe. But the use of assisted ventila-tion is correlated with both intraventricularhemorrhage and the development of chronic lungdisease. One-third of very low birthweight sur-vivors have chronic lung disease at 1 month ofage. A recent study showed that the way in whichventilator support is medically managed may beassociated with outcome; some neonatal intensivecare centers have significantly lower rates ofchronic lung disease than others. Changing andrefining existing medical practices in NICUs couldfurther decrease the mortality and poor outcomesassociated with RDS and assisted ventilation.
Moreover, it is possible that several technol-ogies could substantially prevent RDS in the fu-ture. Steroid treatment, administered to womenin preterm labor in order to accelerate fetal lungmaturation, has been available for 16 years. De-spite numerous studies confirming its efficacy,however, many obstetricians have concerns aboutspecific indications for use, and steroid treatmenthas not been widely integrated into obstetricalpractices. The other technology, administering ex-ogenous pulmonary surfactant into the lungs ofthe newborn, is new, and the medical communityis hopeful about its potential for treating lung defi-ciency. Controlled clinical trials conducted to datehave demonstrated lowered risk of death and res-piratory disease. It will be several more years be-fore surfactant therapy is generally available forpremature infants.
Financing
A study in children’s hospitals (some of themost sophisticated Level III centers) found thatneonatal intensive care is the most costly categoryof service to provide, and that these hospitals suf-

6
fer their greatest financial losses from neonatalcases. In those hospitals studied, neonates repre-sented only 8 percent of admissions but 21 per-cent of all patient days and 25 percent of the hos-pitals’ costs.
As third-party payers, including Medicaid, in-creasingly move to prospective payment methods,concerns have been raised that diagnosis-relatedgroups (DRGs) as currently constituted underMedicare do not adequately reimburse hospitals’costs in providing neonatal intensive care. Asmany as half of the admissions to NICUs are clas-sified as outliers (cases with statistically unusuallengths of stay) under the current Medicare sys-tem. Reform of the DRG system to reflect moreaccurately the true resource use of very low birth-weight infants will help hospitals’ finances, buthospitals may continue to experience revenueshortfalls for neonatal intensive care because oftheir inability in the future to shift costs as theproportion of charge-paying patients declines.
Medicaid is generally considered a poor payerby hospitals. The method of reimbursement andthe level of payment for neonatal intensive carevaries by State. Likewise, the proportion of Med-icaid admissions, and therefore Medicaid’s impor-tance as a payer, varies widely across institutions;overall, Medicaid recipients account for about aquarter of all NICU admissions. From the perspec-tive of the Medicaid program, about 6 percent ofall newborns whose deliveries are subsidized byMedicaid require neonatal intensive care, but thiscare is so expensive that it represents about 30 per-cent of all Medicaid expenditures for maternitycare. Through recent legislative changes, any new-born whose mother met income requirements forMedicaid prior to delivery is assured of at least60 days automatic Medicaid coverage. Financialcoverage for other infants in the NICU who arenot eligible for Medicaid is sometimes availablethrough a variety of State and county paymentprograms for the indigent.
Access
The statistics on survival and outcome that arecited in this case study refer to infants who aretreated in the regional perinatal centers (Level IIIhospitals). A number of studies document better
survival rates for very low birthweight infantsborn in Level III hospitals than for those born else-where in the same geographic area. Moreover,several studies go further and indicate that sur-vival rates for very low birthweight infants bornin Level III hospitals are significantly higher thanfor those infants born in either Level I or LevelII hospitals, despite transfer of sick infants afterbirth. Because deaths within a short time of birthcannot be influenced by infant transport, it maybe that very low birthweight infants are not ade-quately resuscitated and stabilized at birth in LevelI hospitals. Poorer survival rates in Level II hos-pitals were reported in only a few studies. TheLevel II hospitals with poorer survival rates rarelyreferred their very low birthweight patients to re-gional centers, and the researchers concluded thatthe intermediate units could not expertly managethe complications of low birthweight, such as res-piratory failure.
Because little is known about whether high-riskmothers and infants are actually redistributed tothe appropriate level of care, the observed gra-dient in mortality risk across hospital level couldindicate possible inequities in the provision of neo-natal intensive care. Although the contributionof infant transport cannot be assessed, one indi-cation of access to intensive care is the extent towhich high-risk deliveries are concentrated inLevel III centers. All published reports indicatethat although high-risk deliveries have increas-ingly been moved to Level III centers over time,there is still wide variation among geographicareas. Rural populations, as expected, clearly haveless access to perinatal centers than urban popu-lations, and one study showed better access to spe-cialized care for black infants than for whiteinfants.
Although the extent of a possible access prob-lem cannot be determined from existing datasources, hospitals may have financial incentivesnot to serve high-risk mothers and infants. Hos-pitals have no legal obligation to admit these pa-tients even if they are perinatal centers, and somehospitals suffer their greatest financial losses fromneonatal cases. Medicaid coverage for very lowbirthweight infants does not guarantee admission,because Medicaid is generally considered a poorpayer by hospitals. The same financial incentivesoperate for physicians with regard to nonpaying

7
or partial-pay patients. Obstetricians lag behindother specialties in the extent to which they ac-cept Medicaid patients.
A more important barrier to treatment, how-ever, is the unwillingness of many obstetriciansto refer high-risk maternity cases to perinatalcenters prior to delivery. The perceptions of ob-stetricians, many of whom substantially under-estimate the potential survival of extremely lowbirthweight infants, influence the management ofhigh-risk pregnancies and premature labors,which, in turn, actually affects the survival ofnewborns. On the other hand, once a low birth-weight infant, no matter how tiny and premature,is admitted to an NICU, aggressive treatment isalmost always assured. Neonatologists, in part inreaction to legal liability concerns raised by “BabyDoe” rules, are increasingly treating even the ti-niest infants born at the threshold of viability. Theprobability of handicap cannot be determined atbirth, and the normal outcome for a few of theseinfants encourages neonatologists to push for theunprecedented treatment of the lowest birthweightinfants.
CONCLUSIONS
This OTA case study corroborates earlierreports concluding that neonatal intensive care isan effective technology for the improved survivaland long-term developmental outcome of verylow birthweight infants. In the 1980s, continuedimprovements in outcomes are shown in everyvery low birthweight subgroup, with the great-est statistical improvement, recently, in the 750-to 1000-gram birthweight group.
The success of neonatal intensive care doescarry a burden of increasing numbers of seriouslyhandicapped children, As mortality rates decline,there are larger absolute numbers of both handi-capped and normal survivors. If today’s neonatalintensive care were provided for all very lowbirthweight infants, over 15,000 normal childrenwho would have died in 1975 would be added tothe Nation’s population. Likewise, families andsociety would face an increase of about 2,200 seri-
Cost-Effectiveness
The incremental cost of neonatal intensive careto produce a survivor in 1984 was $86,000 for in-fants with birthweights between 1000 and 1500grams and $118,000 for infants with birthweightsbelow 1000 grams. The long-term economic con-sequences of providing neonatal intensive care tovery low birthweight infants were evaluated ina cost-effectiveness study performed by Canadianresearchers. Projected over a lifetime, the intro-duction of neonatal intensive care costs $4,460 perquality-adjusted life-year gained for infants withbirthweights between 1000 and 1500 grams and$31,240 per quality-adjusted life-year gained forinfants with birthweights under 1000 grams. Thus,neonatal intensive care results in both increasedsurvival and increased costs. Moreover, neonatalintensive care becomes more expensive as it is em-ployed in increasingly marginal cases. The worthof a life saved, however, is ultimately a valuejudgment involving ethical and social considera-tions. The results from cost-effectiveness studiesalone cannot guide decisions regarding whoshould receive care.
ously handicapped infants who would not havesurvived a decade ago, These individuals requireoutside resources and help throughout theirlifetimes.
Neonatal intensive care is costly. While theaverage hospital cost for low birthweight infantsis about $620 per day in the hospital, a few in-fants incur truly extraordinary costs. The cost tosociety increases as neonatal intensive care is pro-vided to the very lowest birthweight infants, butit would be unethical and illegal categorically todeny treatment. So far, technology cannot deter-mine at birth which infants are doomed to se-verely handicapped lives. Physicians, in conjunc-tion with parents, have traditionally grappledwith decisions about treatment for premature andsick newborns—and they must continue to dothis.

8
The disturbing fact is that an extremely prema-ture baby’s chances for survival and normal de-velopment are in large part determined by wherethe baby is born. While moderately sized lowbirthweight infants do well in Level II units, thereis a gradient in mortality risk across hospital levelfor very low birthweight infants. Although thebirth of a premature infant cannot always be an-ticipated, there is ample evidence that a pregnantwoman at high risk should be transferred to aLevel III center prior to delivery. Very low birth-weight infants should be transported to Level IIIhospitals as soon as they are stabilized.
The extent of a possible problem in access toneonatal intensive care is unknown. Regionalorganization may have proceeded further in ne-onatal care services than in any other aspect ofmedicine in this country. This regionalization hasbeen accomplished, in almost all States, throughthe voluntary cooperation of hospitals, physi-cians, and maternal and child health officials.Moreover, the optimum concentration of high-risk births in Level III centers is unknown becauseof unavoidable hurdles to admission (e.g., accessto services in rural areas will always lag behindavailability in urban areas).
It does appear, however, that some high-riskmothers and infants are not transferred to LevelIII hospitals for financial reasons. It also appearsthat some Level II hospitals are not appropriatelytransferring high-risk women and newborns be-cause of a desire to offer competitively a full ar-ray of services even when those services do notmeet the needs of the patients. And most impor-tantly, surveys show that many obstetricians andpediatricians do not have a good understandingof the prognosis for extremely low birthweight in-fants; they substantially underestimate the poten-tial for survival and normal outcome. Their man-agement of high-risk pregnancies and birthsreflects these misunderstandings.
These problems point to a need to continue topush for further regionalization of perinatal serv-ices in the 1980s. Stronger guidance from profes-sional associations and State health authoritiesmay be necessary in two areas. One is the for-mulation of clear recommendations on treatmentand transfer policies for infants with particularproblems and/or birthweights by level of care.Second is the exercise of leadership in informingobstetricians and pediatricians about current prac-tices and outcomes in neonatal intensive care.
Even among Level III hospitals, there are sub-stantial differences in mortality risk for very lowbirthweight infants. At present, there is only sug-gestive evidence that variations in medical prac-tices within institutions may lead to these differ-ences. Differences in the organization of NICUs,the methods of applying existing technologies, andthe use or disuse of certain technologies may allplay a part in the success of some centers. Clearly,the technology of neonatal intensive care is chang-ing very rapidly. The rate of diffusion of the latestand most effective techniques and knowledge—even among the 420 most sophisticated NICUsoffering Level III services—may not be proceed-ing apace with developments.
The problem of disseminating information tomedical professionals and institutions is notunique to neonatal intensive care. The need toshare information among professionals is ongo-ing in all arenas of medicine. Moreover, skepti-cism about new ideas and techniques is healthyin that the diffusion of technologies which are notefficacious is at least slowed. Further research inNICUs is definitely necessary to evaluate whichmedical practices are effectively helping very lowbirthweight infants. Nevertheless, the speed oftechnology diffusion in neonatal intensive care iscritical because the lives and well-being of oursmallest babies may hang in the balance.

Chapter 2
Supply, Use, and Cost ofNeonatal Intensive Care

Chapter 2
Supply, Use, and Cost ofNeonatal Intensive Care
INTRODUCTION
With the evolution of perinatal medicine andthe development of associated medical technol-ogy in the 1960s, many hospitals introduced ne-onatal intensive care units (NICUs). Intensive careunits for adults had already been established inmost hospitals, and the similar needs of newbornsfor sophisticated, intensive treatment becameapparent (15). In the United States, the primarygrowth in special units for neonatal intensive care,combining high technology and highly trainedstaff, occurred in the 1970s. By 1976 the Com-mittee on Perinatal Health] had proposed guide-lines for the regionalization of maternal andperinatal health services that included a three-tiered system of hospital care (34). Level III hos-pitals serve as regional centers and provide themost intensive neonatal care. Level II facilitieshave many but not all components of newbornintensive care services, and Level I hospitals pro-vide normal newborn care with no special units
‘The Committee on Perinatal Health was a joint effort by theAmerican Medical Association, the American College of Obstetri-cians and Gynecologists, the American Academy of Family Physi-cians, and the American Academy of Pediatrics.
SUPPLY
The confusion over which hospitals deliver in-tensive v. less specialized newborn care complicatesdata collection and analysis. As a definitional min-imum, Level III NICUs have the capability to pro-vide ongoing respiratory support and are staffedby a full-time neonatologist. But today manyLevel II units also have these capabilities. The truedistinction between the two levels of care may liewith the kinds of patients treated, rather than inequipment and staffing capabilities. Level II hos-pitals are more likely to provide short-term res-piratory support, stabilize very sick or very pre-term patients, and then refer more complicated
for the care of seriously ill infants. The conceptof regionalization is that high-risk mothers andinfants are screened and referred or transportedto the appropriate level of care. Success dependson the coordinated relationship among hospitalsin the system.
Despite these guidelines, recommendations pub-lished by the American Academy of Pediatrics in1977 (2), and guidelines jointly issued by theAmerican Academy of Pediatrics and the Amer-ican College of Obstetricians and Gynecologistsin 1983 (4) outlining the responsibilities and re-quirements of the three hospital levels, there isno standard national application of what consti-tutes Level II or Level III care (25). Some Statesevaluate each hospital’s perinatal services and as-sign levels. In other States, the regional systemis informal, and each hospital classifies its ownservices. An earlier study by OTA on neonatalintensive care identified only four States in 1978that forced adherence to specific standardsthrough licensure or certificate-of-need authorities(25),
cases, especial111 units (144)
y those requiring surgery, to Level
Because of these ambiguities, most inventoriesgroup Level II and Level III hospitals together. Ta-ble 1 presents the most recent estimate of the com-bined number of Level II and Level III units iden-tified by the National Perinatal InformationCenter in a survey of hospitals offering perinataland neonatal special care. The reported 1983 to-tals of 534 NICUs and 7,684 NICU beds repre-sent a nationwide increase of 3 percent in avail-able neonatal intensive care beds and a decrease
11

12
Photo credit: Children's Hospital National Medical Center, Washington, DC
Level Ill hospitals provide the most sophisticatedintensive care for newborns.
of 13 percent in the number of NICUs since anearlier OTA assessment estimated the number ofunits and beds in 1978 (25). To illustrate the con-fusion over definitions, Ross Laboratories, whichinitially surveyed hospitals in 1978 and then in-formally updated its inventory, lists more thantwice as many Level II and Level III hospitals(1,137) on its 1986 roster (138). In part, this differ-ence is accounted for by the inclusion in the Ross
UTILIZATION
Table I.—Supply of Neonatal Intensive Care Units(NICUs) and Beds in the United States, 1983
Number of Number ofRegion hospitals NICU beds
Northeast . . . . . . . . . . . . . . . 100 1,622South Atlantic . . . . . . . . . . . 81 1,003North Central . . . . . . . . . . . . 135 2,391South Central . . . . . . . . . . . . 92 1,218West . . . . . . . . . . . . . . . . . . . 122 1,413Other . . . . . . . . . . . . . . . . . . . 4 37
Total . . . . . . . . . . . . . . . . . 534 7,684SOURCE: National Perinatal Information Center, unpublished data from the
American Hospital Association’s 1983 Annual Survey of Hospitals,Providence, Rl, December 1986.
Laboratories’ inventory of military hospitals andall special care units for newborns. It is also likelythat the National Perinatal Information Centerunderestimates the number of Level II units, butthe magnitude of the difference is still unexplained.
The actual number of Level 111 units, fullystaffed by neonatologists and capable of provid-ing the most sophisticated prolonged life support,is probably close to 420. About 485 hospitals re-ported that they had NICUs in 1983 on the Amer-ican Hospital Association’s Annual Survey ofHospitals, but further investigation by the Na-tional Perinatal Information Center refined thatfigure to about 420 (144). Through interviewswith maternal and child health officials and otherexperts in the field, some hospitals were droppedfrom the list while others were added.
Even Level III hospitals have varying capabil-ities. Forty children’s hospitals have NICUs. Thesechildren’s hospitals, along with many universityhospitals, tend to provide the most sophisticatedneonatal intensive care, often in conjunction withspecialized pediatric surgery, Neonatologistssometimes refer to these centers as Level IV hos-pitals.
Again reflecting data from Level II and Level cupancy by geographic area, with the North Cen-111 units combined, table 2 shows that infants tral region reporting only a 65-percent occupancyspent over 2 million days in NICUs in 1983, main- rate and the Northeast and the Western regionstaining an average NICU occupancy rate of 73 each reporting an 80-percent occupancy rate. Aspercent. There was considerable variation in oc- the national occupancy rate for all hospital beds

13
Table 2.—Neonatal Intensive Care Unit Days of Careand Occupancy in the United States, 1983
OccupancyRegion Patient days (percent)
Northeast . . . . . . . . . . . . . . 471,395 80South Alantic . . . . . . . . . . . . 277,582 76North Central ., . . . . . . . . . . 569,545 65South Central . . . . . . . . . . . . 300,771 68West . . . . . . . . . . . . . . . . . . . 411,961 80Other . . . . . . . . . . . . . . . . . . . 8,468 63
Total . . . . . . . . . . . . . . . . . 2,039,722 73SOURCE National Perinatal Information Center, unpublished data from the
American Hospital Association’s 1983 Annual Survey of Hospitals,Providence, RI December 1986
was 76 percent in 1983, the widely expressed con-cern that NICU beds are filled to overcapacity wasnot substantiated by these data (5). Of course, theexperience of individual neonatal intensive careunits varies widely, and some NICUs do reportregular over-utilization (47,143).
The number of admissions to NICUs, and there-fore the average length of stay, is not availablefrom national databases. Based on total patientdays and average lengths of stay reported by sev-eral groups of Level III centers (see table 3), OTAestimates that between 150,000 and 200,000 in-fants are admitted annually to neonatal intensivecare units, or between 4 to 6 percent of allnewborns.
Between 50 and 80 percent of all admissions toNICUs are low birthweight infants; there is con-
siderable variation across centers (110,130,186).While the proportion of infants born weighing be-tween 1500 and 2500 grams has decreased some-what relative to total births over the last 10 years(currently 5.5 percent of all births), the propor-tion of very low birthweight infants has increasedslightly (170). About 39,000 very low weight in-fants are born annually (a little more than 1 per-cent of all births), and virtually all of them requireneonatal intensive care. In 1984, almost 17,000of the very low birthweight infants weighed lessthan 1000 grams at birth.
Individual Level III centers report a trendtoward increasing admissions of infants weigh-ing under 1000 grams. Whereas these extremelylow birthweight infants may have constituted 5or 6 percent of admissions in the 1970s, in the1980s they represented 10 to 12 percent and even29 percent of all admissions to the NICU (48,87,126,129,186). At least one report also documentsa shift in the distribution of birthweights withinthe under 1000-gram birthweight group. From1974 to 1983 at the University of Alabama in Bir-mingham, the proportion of admissions in the501- to 700-gram category nearly doubled whilethe proportion of admissions in the 901- to 1000-gram group decreased (57).
Information on length of stay by birthweightcategory is shown in table 3. The average lengthof stay in 1984 for all sick newborns in those
Table 3.–Length of Stay by Birthweight Group, 1984
Average length of stay (days)
Maryland Children’s San FranciscoBirthweight (grams) Level Ill hospitals hospitals Level Ill hospitals
< 750 . . . . . . . . . . . . . . . . 39.2 57.7 40.8751-1000 . . . . . . . . . . . . . . . . . . . . . . . 65.3 59.1 56.31001-1500 . . . . . . . . . . . . . . . . . . . . . . . 46,4 45.4 41.21501-2000 . . . . . . . . . . . . . . . . . . . . . . 21.1 25.0 17.92001-2500 . . . . . . . . . . . . . . . . . . . . . . . 7,8 16.6 10.0>2500 . . . . . . . . . . . . . . . . . . . . . 4,4 11.3 8.4
Total < 1500 . . . . . . . . . . . . . . . . . . . . . 49.1 50.4 44.9Total < 2500 . . . . . . . . . . . . . . . . . . . . . 23,8 31.6 29.5
Total all infants . . . . . . . . . . . . . . . . 10.3 17.1 18.8aln Maryland’s Seven hospitals with Level III Neonatal Intensive Care Units (N ICUS), includes all newborns who fall into themajor dlagnosttc category (M DC) for neonates, MDC 15, excluding normal newborns.
bln a sample of IQ children’s hospitals. Includes all neonates admitted under age 28 days, except normal newborns and In.fants who died or were transferred within 24 hours of birth The latter are tncluded in the total for all Infants
Cln two San Francisco hospitals with Level Ill NICUS tncludes all Infants adm!tted to the NICUS
SOURCES Information Service Center, Inc Baltimore, MD, unpublished data, prepared under contract with the Of ftce of Tech.nology Assessment Ju Iy 1986, N at!onal ASSOCI atlon of Children Hospttals and Related Institutions, Inc , Alexan.drla VA, unpublished data, August 1986 and C S Phlbbs, Untvers!ty of Call fornla, San Diego, unpublished data,March 1987

14
centers reporting data ranged from 10 to 19 dayswhile the average length of stay for very lowbirthweight infants ranged from 45 to 50 days.As expected, the length of hospital stay increasesas birthweight decreases. For extremely low birth-weight
COST
infants under 1000 grams who survive to
Neonatal intensive care is expensive, rankingamong the most costly of all hospital care.2 Aver-age hospital costs for low birthweight babies in1984 ranged from $11,670 to $39,420 (see table4).3 Among 10 diagnoses studied by Showstack
‘The costs for physicians’ services in NICUs are not reflected inthis section because data on physician charges were unavailable.Estimates vary, but physicians’ charges probably raise overall med-ical care charges by about 15 percent (79,128). Typically, neona-tologists charge a daily visit fee for each patient in the NICU andadditionally bill all procedures, such as catheterization, separately.Other consulting physicians also charge for their services. With theextremely long hospital stays of most very low birthweight infants,physicians’ charges can become a substantial liability for patients’families.
‘The three data sources in tables 4 and 5 show such a wide rangein hospital costs in part because they report on different popula-tions. The data from the Maryland and children’s hospitals includeall newborns who are hospitalized (except normal newborns), whilethe data from the San Francisco hospitals include only NICU ad-missions. Because the majority of the larger low birthweight infants
hospital discharge, it takes at least 70 to 90 daysin the hospital to reach the necessary size andmaturity so that continuous professional nursingcare is no long required (see table 5). The impli-cations of other risk factors for length of stay arediscussed n the following section on costs.
and his colleagues, infants with respiratory dis-tress syndrome (a major problem among prema-ture, low weight babies) had substantially higherhospital charges than any other group, includingpatients with acute myocardial infarction or kid-ney transplantation (154). The costs for the sick-est and tiniest infants in neonatal intensive carerank with the most expensive medical proceduresthat are performed today, like cardiac or bonemarrow transplantation (96,145).
The distribution of costs among patients in theneonatal care nursery is highly skewed. A signif-icant portion of the variation among infants in
(those with birthweights between 1500 grams and 2500 grams) donot require intensive care, the cost data for these birthweight cate-gories, although reflecting average hospital costs, underestimateNICU costs. Box A provides a full explanation of the databases andtheir limitations.
Table 4.—Hospital Cost by Birthweight Group, 1984
Average hospital costsMaryland San Francisco
Birthweight (grams) Level Ill hospitals Children’s hospitals Level Ill hospitals
< 750 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $25,069 $48,773 $58,053751-1000 . . . . . . . . . . . . . . . . . . . . . . . . . . . 38,750 47,068 76,3871001-1500 . . . . . . . . . . . . . . . . . . . . . . . . . . 22,266 32,530 53,6631501-2000 . . . . . . . . . . . . . . . . . . . . . . . . . . 8,594 16,370 20,8452001-2500 . . . . . . . . . . . . . . . . . . . . . . . . . . 2,898 13,794 16,751>2500 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,202 9,358 14,601
Total < 1500 . . . . . . . . . . . . . . . . . . . . . . 26,737 38,171 60,015Total < 2500 ... , . . . . . . . . . . . . . . . . . . 11,666 23,639 39,421
Total all infants . . . . . . . . . . . . . . . . . 4,411 13,416 26,946aln Ma~yla”d,~ ~even hospitais with Level III Neonatal Intensive Care Units (N ICUS), includes all newborns who fall into the major diagnostic cate90W (MW for neo-
nates, MDC 15, excluding normal newborns. Charges are converted to costs through a weighted cost-to-charge ratio derived from the Maryland Health Services CostReview Commission’s ratios for individual hospitals and their relative contribution to total births.
bin a sample of 13 children’s hospitals, includes all neonates admitted under age 28 days, except normal newborns and iflfantS who died or were transferred within
24 hours of birth (The latter are included in the total for all infants.) Costs are derived from a cost finding methodology employed by National Association of Children’sHospitals and Related Institutions and adjusted for labor differentials.
Cln two San Francisco hospitals with Level III Nlcus, includes all infants admitted to the NICIJS, Charges are adjusted to costs using Medicaid’s cost-to-charge MiO.
SOURCES: Information Service Center, Inc., Baltimore, MD, unpublished data, prepared under contract with the Office of Technology Assessment, July 1988; NationalAssociation of Children’s Hospitals and Related Institutions, Inc., Alexandria, VA, unpublished data, August 1988; and C.S. Phibbs, University of California,San Diego, unpublished data, March 1987.

15
Box A.—How To Interpret the Data in Tables 3, 4, and 5
Tables 4 and 5 show such a wide range of costs because the three data sources that are cited reporton somewhat different populations. The seven Level III hospitals in Maryland have the lowest costs. Thesedata include all infants born in the hospitals who are assigned to the diagnosis-related groups (DRGs) forneonates (excluding normal newborns). Because of inconsistencies in coding, these data may include someinfants older than 28 days who return to the hospital for routine surgical corrections of congenital anoma-lies and may exclude some seriously ill newborns who are assigned to non-neonate DRGs that describethe organ system involved with their problems (109). Any newborn weighing less than 2500 grams is in-cluded in this classification because of his low birthweight, regardless of the extent of medical problems.Thus especially in the heavier low birthweight groups, the Maryland data underestimate NICU costs be-cause many of the babies, though hospitalized, are not sick enough to warrant intensive care.
Conversely, the other 2 data sources, 13 children’s hospitals and 2 university-affiliated San Franciscohospitals, tend to overestimate average NICU costs. Most children’s hospitals do not have obstetrical serv-ices, and they typically serve as super-referral centers for the most difficult and complicated cases, oftenthose requiring complex surgery. They, along with many university hospitals, are sometimes referred toas Level IV facilities because their caseloads require such intensive care. These data sources reflect averagecosts for the sickest infants.
There are several additional caveats about these data. The data from the children’s hospitals includeall admissions of infants under 28 days of age, but like the Maryland data, it is not known which infantsactually received care in the intensive care unit. For example, very complicated surgical patients with con-genital problems often are placed in pediatric intensive care units instead of NICUs even if they are new-borns. And because children’s hospitals are almost exclusively referral centers, many of the babies returnto their original hospitals after surgery or to complete recuperation. Such transfer policies underestimatetrue lengths of stay and concomitant costs for these newborns.
The two San Francisco hospitals constitute the only data source that reports only on infants admittedto the NICU. Thus it is the best source of information on the cost experience of the heavier birthweightinfants (over 1500 grams) in NICUs. However because one of these hospitals is also a surgical center forinfants with congenital anomalies, these data may overestimate typical NICU costs for the larger infants.Moreover, the same hospital has an aggressive program for back-referring infants to their originating hos-pitals which explains, in part, the generally shorter lengths of stay reported by the San Francisco hospitalscompared with the children’s and Maryland hospitals. Finally this database is limited by the size of thepopulation. The San Francisco hospitals had a total caseload of 580 infants while the Maryland hospitalsand the children’s hospitals each report on over 5,000 infants. There were 290 low birthweight infants inthe San Francisco hospitals. The Maryland hospitals had 1,540 infants and the children’s hospitals had 2,240infants in their low birthweight populations.
cost and length of stay is explained by four meas- these factors plus two others: multiple births andures of risk: birthweight, survival to hospital dis-charge, assisted ventilation, and surgical interven-tion (109,13 o). A study on costs in 13 children’shospitals conducted by the National Associationof Children’s Hospitals and Related Institutionsin 1984 found that these factors explained 45 per-cent of the variation in costs among neonatal caseswhen the extreme outliers were removed from thecalculation (111). A different study of admissionsto six Level 111 NICUs in California found 42 per-cent of the variation in costs was explained by
discharge to another hospital (130).
Birthweight has the greatest explanatory power.Costs increase as birthweight falls. The averagehospital costs for very low birthweight babiesrange from $26,740 to $60,015. (See table 4.) In-fants in the 750- to 1000-gram birthweight group,which uses resources very intensively, have aver-age costs between $38,750 and $76,390. The aver-age hospital costs for infants with birthweightsbelow 750 grams are lower than the average costs

16
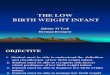
for those infants in the 750- to 1000-gram groupbecause so many of the tiniest babies die withina short time of birth, thus incurring fewer expenses(figure 1).
If only survivors are counted, costs increaseacross birthweight groups. (See table 5.) Becauseof the high mortality experienced at the lowestbirthweights, survival to discharge is the most im-portant factor in explaining variations in costs forinfants with birthweights under 1500 grams. Alarge percentage of these premature newborns diewithin a very short time after birth and consumeminimal resources. Another substantial portionof the infants live past the first critical 24 to 72hours and consume considerable resources, buteventually die. The children’s hospital data indi-cate that even if only this latter group, infants whouse resources intensively but ultimately die, is con-sidered, on average survivors are still more ex-pensive (109). As expected, the tiniest infants whosurvive, those with birthweights from 500 to 750grams, have the highest costs and hospital stays,from $61,700 to $149,180 and from 87 to 109 daysrespectively.
Table 6 shows costs and lengths of stay for new-borns who require assisted ventilation for morethan 72 hours. Unfortunately, virtually all infantsborn weighing under 750 grams and most infantsin the 750- to 1000-gram birthweight group do re-quire prolonged respiratory assistance. Only 15percent of the under 1000 gram survivors shownin table 6 did not require assisted ventilation. Theaverage costs of these nonventilated extremely low
Figure 1.— Hospital Cost by Birthweight Group, 1984
$80,000 r 76,387
$70000 I
$10,000
n t
54705353,063
< 750 751.1000 1001-1500Grams
Hospitals
SOURCE: Office of Technology Assessment (see table 4), 1987.
birthweight survivors are only a third of the$63,750 required to care for the infants on assistedventilation. For all low birthweight babies, aver-age hospital costs increase almost fourfold, from$11,470 to $40,550, if assisted ventilation is re-quired. The use of assisted ventilation over 72hours explains between 20 and 36 percent of thevariation in costs among infants who weigh lessthan 1500 grams (109). For the heavier low birth-weight babies, those in the 1500- to 2500-gramgroup, the most important explanatory factor iswhether surgery is required. About 12 percent ofthe variation in costs among cases is explained bysurgical intervention (109).
Table 5.—Hospital Cost and Length of Stay Per Very Low Birthweight Survivor, 1984
Maryland Level Ill San Francisco children’shospitals hospitals Level Ill hospitals
Birthweight (grams) ALOS d Mean $ ALOS d Mean $ ALOS d Mean $
> 750 . . . . . . . . . . . . . . . . 97.9 $61,706 87.4 $67,892 108.5 $149,184751-1000 . . . . . . . . . . . . . . 86.2 48,290 71.4 54,805 66.4 88,0281001 -1500 . . . . . . . . . . . . . 48.5 21,848 47.3 32,168 44.8 56,276
Total . . . . . . . . . . . . . . . 61.5 31,426 56.3 40,514 55.1 71,417aln Maryland,s seven ho~~ita[s ~lth Level III Nlcus, in~l”des all newborns Who fall into the major diagnostic catego~ (MDC) for neonates, MDC 15, excluding normal
newbornsbln a sample of 13 children’s hospitals includes all neonates admitted under a9e 28 days, excePt normal newborns.cln two San Francisco hospitals with Level Ill NICUS, includes all infants admitted to the NICUS.dALOS denotes average length of stay (days).
SOURCES Information Service Center, Inc., Baltimore, MD, unpublished data, prepared under contract with the Office of Technology Assessment, July 1986; NationalAssociation of Children’s Hospitals and Related Institutions, Inc., Alexandria, VA, unpublished data, August 1986, and C.S. Phibbs, University of California,San Diego, unpublished data, March 1987

17—
Table 6.—Hospital Cost and Length of Stay for Newbornsa
Requiring Assisted Ventilation, 1984
Assisted ventilation No assisted ventilation
Birthweight (grams) Mean $ ALOSC Mean $ ALOSC
< 1000 . . . . . . . . . . . . . . , .1001-1500 . . . . . . . . . . . . . . .1501-2000 . . . . . . . . . . . . . . .2001-2500 . . . . . . . . . . . . . . .>2500 . . . . . . . . . . . . . . . . . .
Total < 1500 . . . . . . . . . . . . .Total < 2500 . . . . . . . . . . . . .
Total all infants . . . . . . . .
$63,75340,05547,95123,23329,112
49,29540,54835,322
79,253.949.623.227.7
63.849.439.5
$22,69417,73211,3648,7095,383
18,55911,474
6.555
50.535.223.113.08.0
37.820.410.4
aDataex~lude~ normal newborns, Infants transferred to anotherhospltal within 4daysof birth, and all mfantswhodled before
dischargeblnfants required mechanlca[ venttlatlon forover3 daysCA LOS denotes average length of stay (days)
SOURCE National Association of Children’s Hospitals and Related Institutions, Inc., Alexandra. VA, unpublished data, Au-gust 1986
More of the increase in the costs of neonatalintensive care over time is due to a sicker case mixthan to the use of more services or general infla-tion. In comparing admissions to the NICU at theUniversity of California, San Francisco between1976-78 and 1983-84, Phibbs and his colleaguesfound that mean charges increased from $6,230to $25,230. The cost to treat similar types of casesincreased 30 percent, and this change was at-tributed to technology and higher prices. Infla-tion accounted for another 23 percent, and theremaining 47-percent increase in overall chargeswas attributed to a change in the kinds and sever-ity of cases (94). The caseload in this Level IIInursery became much more concentrated with ex-tremely low birthweight infants and with infantswho required complex surgery than in earlier
years. The researchers hypothesized that the sickercase mix was caused by increased regionalizationand greater availability of Level II beds (94).
Other researchers in the same institution fol-lowed the hospital course of infants with respi-ratory distress syndrome as part of a larger studyof costs and changes in clinical practice. Theyfound that between 1972 and 1982 resource useincreased more for infants with respiratory dis-tress syndrome than for any of the other nine diag-noses studied. They concluded that these new-borns received increasing quantities of servicesover the decade and that the most difficult coststo contain are those for such critically ill patients(154).

Chapter 3
Effectiveness of NeonatalIntensive Care

Chapter 3
Effectiveness of Neonatal Intensive Care
INTRODUCTION
The remarkable decline in infant and neonatalmortality in this country since 1960 is chronicledin the OTA assessment, Healthy Children: Invest-ing in the Future (170). Neonatal mortality rates(deaths during the first 28 days of life per 1000live births) are affected by both birthweight dis-tribution and birthweight-specific mortality rates.Assuming that better neonatal and obstetrical careimply improved outcomes for infants at a givenbirthweight while shifts in birthweight distribu-tion toward heavier babies can be attributed toimproved prenatal care and maternal health andnutrition, the concern in this case study is thedirection of the birthweight-specific mortalityrates.
Improvements in the birthweight-specific mor-tality rates accounted for 91 percent of the over-all decline in neonatal mortality between 1960 and1980 (27). Moreover, two-thirds of the decline inbirthweight-specific neonatal mortality resultedfrom improved survival of low birthweight in-fants. Decreases in the mortality rates of infantsweighing between 1500 and 2500 grams contrib-uted more than any other weight group, includ-ing the very low birthweight group, because ofboth greater proportional decreases and higherabsolute declines in mortality (184). In reviewingperinatal mortality rates by birthweight between1960 and 1977 in California, Williams and Chenconcluded that much of the decline could be at-
MORTALITY RATES
Birthweight-specific death rates on a nationalbasis are not available for trend analysis becausenot all States routinely link birth certificates(where birthweight is noted) with death certifi-cates. However, many individual Level III centersreport their experiences in the medical literature.Because the mortality rates for infants born in theLevel III hospitals are lower than the mortality
tributed to the advent of neonatal intensive care(as well as the increased rate of cesarean section)(184).
The effectiveness of neonatal intensive caremust be measured not only by whether more livesare being saved but also by whether the long-termhealth outcome for the babies and their familiesis good. The health status of survivors, specifi-cally the rate of serious disability or handicap,has been the subject of intense interest. For thelarger low birthweight infants, those with birth-weights between 1500 and 2500 grams, neonatalintensive care has been accepted as a mature andeffective technology (25,166). But because the riskof handicap increases with decreasing birthweight,debate continues about providing universal carefor all very low birthweight infants (151,25).
This chapter focuses on changes in mortalityand morbidity over the past 25 years for such verylow birthweight infants. Following discussions ofmortality and handicap rates, the three leadingcauses of mortality and morbidity in the neonatalintensive care unit (NICU) are examined in detail:respiratory distress syndrome, intraventricularhemorrhage, and retinopathy of prematurity.These clinical problems not only account for themajority of deaths among very low birthweightinfants, but they can also lead to substantial long-term disabilities. The outlook for technologicaladvances in these areas is also discussed.
rates for infants who do not have immediate accessto care in the intensive care units (see ch. 5), theseinstitutional reports may be the best indicator ofthe impact of NICUs on mortality outcomes.
There are problems, however, in comparingmortality results from one hospital to another be-cause of differences in the demographic charac-
2 1

22
teristics of the populations served, in the stand-ards of care, in the proportions of high-riskpregnancies, and in the selective application orwithdrawal of intensive treatment measures (83).Displaying the data by birthweight group does notcompletely control for these differences. For ex-ample, the distribution of gestational age withina given birthweight group is probably the mostimportant indicator of survival. Moreover, indi-vidual nurseries typically report on only smallnumbers of infants, and mortality rates may fluc-tuate from year to year. Bearing in mind thesecaveats, OTA reports and combines institutionaldata to permit generalization about mortality ratesover time.
Table 7 summarizes reports on mortality forvery low birthweight infants born in Level IIIhospitals (inborn) during the past 10 years. Table8 is a similar compilation, but it lists studies thatreport on admissions to NICUs (inborns andtransfers). The two kinds of denominator popu-lations are reported separately for several reasons.On the one hand, inborn populations would beexpected to have higher mortality rates becauseof the high proportion of infants who die almostimmediately in the delivery room and are neveradmitted to the NICU. On the other hand, whilethe infants admitted to the NICU have survivedthrough the first critical minutes or hours of life,the infants born in other hospitals (transfers) maybe selectively sicker because of the period of timethat they were denied intensive care before andduring transport. A study in New York City onthe effect of place of birth on mortality in fact sup-ports both these conclusions which are further dis-cussed in chapter 5 of this case study (119). InOTA’s literature review, inborn populations hadsignificantly lower pooled mortality rates (for1980 to 1985) than NICU populations in the 750-to 1000-gram and the 1001- to 1500-gram birth-weight groups. The differences between the twokinds of nursery populations were not statisticallysignificant in the smallest babies born weighingunder 750 grams.
With one exception, there has been steady andstatistically significant improvement in mortalityrates among very low birthweight infants through-out the last 10 years. In 1985, a baby born witha birthweight between 1001 and 1500 grams has
a 90 percent chance of surviving. The most sub-stantial improvement of the 1980s over the late1970s, in neonatal mortality rates is in the 751-to 1000-gram birthweight group where today’s in-fants have about a 70 percent chance of surviv-ing if they are admitted to an NICU.
The exception to the mortality decline over thepast decade is among the tiniest inborn babies,those in the under 750 gram group, where someextremely promising, but mostly variable, resultsare reported on babies born in the 1980s.1 For thisbirthweight group, Columbia University reportsonly 28 percent of their inborn infants died in 1986and the University of Missouri-Kansas CitySchool of Medicine shows only a 53 percent neo-natal mortality rate in 1983 and 1984 (46,80).However, other institutions which report their ex-periences in the 1980s show much worse mortal-ity rates. The 1980-85 pooled results for bothdenominator populations show that about two-thirds of this birthweight group dies. Such widevariation among centers may mean that the tech-nology of neonatal intensive care is continuing tochange rapidly.
Table 9 shows the great progress that medicinehas made over the past several decades in reduc-ing birthweight-specific mortality rates amongvery low birthweight infants.2 The pooled institu-tional results on mortality from 1961 through 1975are taken from an earlier OTA literature review(25). Mortality for infants with birthweights of1001 to 1500 grams has fallen from more than 50percent in 1961 to only 10 percent today. Andwhereas more than 90 percent of all infants weigh-ing under 1000 grams died in 1961, the inborn ne-
I Even for this birthweight subgroup (under 750 grams), the pooledmortality rates calculated for NICU populations decreased signifi-cantly from 1975-80 to 1980-85.
‘It should be noted that improvements in the birthweight-specificmortality rates may also be attributable to factors other than solelyneonatal intensive care. For example, healthier cohorts of low birth-weight infants may be delivered through selective abortion, betterobstetrical techniques, improved maternal care and nutrition, andso forth (18). It is not possible to sort through each factor’s relativecontribution, but clearly neonatal intensive care is very important.

Table 7.—Comparative Neonatal Mortality for Very Low Birthweight Infants Born in Level Ill Hospitals, 1975-85
Birthweight (grams)
501-750a 751 -1000a < 1000 1001-1 500a
Referenceb Year of birth Deaths/births Percent Deaths/births Percent Deaths/births Percent Deaths/births Percent
Knobloch (83) . . . . . . . . . . . . . . 1975-79 — — 50/74 68 ”/0KOOPS (85) . . . . . . . . . . . . . . . . . 1974-80 60/82 73 ”/0 49/108 45 ”/0Phibbs (129)C . . . . . . . . . . . . . . . 1976-78 — — —Kitchen (82)C . . . . . . . . . . . . . . . 1977-78 47/62d 760/o 30/65 d –460/oNelson (1 13). . . . . . . . . . . . . . . . 1977-78 — . —Buckwald (24)C. . . . . . . . . . . . . . 1977-81 50/90 d —560/o — —Hoskins (71). . . . . . . . . . . . . . . . 1979-80 20/39 51 “/0 14167 21 “/0
Pooled subtotal . . . . . . . . . . . 1975-80 1771273 65% 143/31 4 460/o
Brans (22) . . . . . . . . . . . . . . . . . . 1978-82 68177 880/0 49/105 480/oAvery (6)C . . . . . . . . . . . . . . . . . . 1983 31/50d 62% 71/46d 15“/0Kilbride (80) . . . . . . . . . . . . . . . . 1983-84 46/87 d 53 ”/0 —Horbar (69)e . . . . . . . . . . . . . . . . 1983-84 — 88/357 d —250/oHack (61)C. . . . . . . . . . . . . . . . . . 1982-85 57/77 –74% 24173 33 ”/0Driscoll (46)C . . . . . . . . . . . . . . . 1986 5/18d 280/o 2/21d 10 ”/0
Pooled subtotal . . . . . . . . . . . 1980-85 2071309 670/o 1701602 280/oasorne studies reported birthweight categories as 500 to 749, TSO to 999, and 1000 to Idgg 9bsee references in the back of this case study for full citations.cDeaths reported to hospital discharge.dlncludes blrthwelght categories 501 to 800 g and 801 to 10009e Re p o r t on multiple neonatal intensive care c e n t e r s.
SOURCE: Off Ice of Technology Assessment, 1987
— 61/21 1109/1 90 57 ”/0 58/348
18/35 51 “/0 10/82771127 61 0/0 33/250
220/360 61% 1221720— — —
34/106 320/o —
458/818 560/o 284/1,611
117/182 640/o 41123638/96 40 ”/0 13/109
— — —— — 101/1,243
81/150 54 ”/0 30/2167/39 180/0 1/75
2431467 520/o 186/1 ,879
290/o17“/012“/013“/017“/0
——
180/0
17“/012 ”/0
—80/0
14 ”/01%
10%

24
I
II
.
I
I
.0
“ -

Table 9.—inborn
25
Neonatal Mortality Rates for Very Low Birthweight Infants,Pooled Institutional Data
Birthweight (grams)< 1000 1001-1500
Year of birth Deaths/births Ratea Deaths/births Rate a
1961-65 . . . . . . . . . . . . . . . . . 1851197 939 1421274 518 -
1966-70 . . . . . . . . . . . . . . . . 381/443 860b 2121567 374b
1971-75 . . . . . . . . . . . . . . . . . 209/274 763b 541253 213b1976-80 ., . . . . . . . . . . . . . . . 4581818 560b 284/1,611 1761981-85 . . . . . . . . . . . . . . . . . 2431467 520 186/1,879 99b
aRate deaths /1 ,000 Ilve birthsbsrgnlflcantly d! fferent from preceding 5-year rate (P <0 01)
SOURCES For years 1976.85, Off Ice of Technology Assessment (see table 7) For years 1961.75, P Budetti, P McManus NBarrand et al , The Costs and Effectiveness of Neonatal Intensive Care (Health Technology Case Study #10), pre-pared for the Off Ice of Technology Assessment, U S Congress, OTA. BP-H-9 (Springfield, VA: National TechnicalInformation Services, August 1981)
onatal mortality rate now is about 52 percent.3 ily in the 750- to 1000-gram birthweight groupThis achievement reflects improvements primar- since mortality is still very high in the smallest
‘The true neonatal mortality rate today for newborns weighing and most premature infants, those under 750under 1000 grams who have access to neonatal intensive care is prob- grams. Neonatologists are justifiably proud ofably closer to 47 percent, the rate shown in table 8 for NICU popu- break ing the 1000 gram barr ie r , and they looklations. OTA used the 52 percent rate (from table 7 for inborn pop-
now to infants weighing under 800 grams as theirulations with birthweights under 1000 grams) in table 9 to beconsistent across time and denominator populations. Several of the great challenge.studies in table 7 showing the best survival rates for inborn popu-lations did not report on all infants with birthweights between 500and 1000 grams. The results of these studies could not be includedin the pooled total for infants with birthweights under 1000 grams,and thus the 52 percent rate probably overestimates mortality,
HANDICAP RATES
When neonatal intensive care was introduced,concern was expressed that many sick and prema-ture infants, who otherwise would have died,would be saved and result in a large number ofhandicapped children. Early, well-publicizedstudies of very low birthweight babies born in the1940s and early 1950s, long before the era of neo-natal intensive care, fueled this concern becausethey showed very high rates (30 to 40 percent)of cerebral palsy and other forms of impairmentin survivors (45,95). Two groups, Budetti and hiscolleagues in their earlier OTA assessment of neo-natal intensive care and a team of British research-ers, independently attempted to resolve this ques-tion by reviewing published reports from hospitalnurseries that described outcomes for very lowbirthweight infants who were born after 1945.Both review articles found that the handicap ratefrom the very early period dropped sharply by
the mid-1960s (possibly before neonatal intensivecare was widely introduced). Furthermore, fromthe mid-1960s through about 1977, the propor-tion of very low birthweight survivors with seri-ous handicaps remained stable and relatively low(about 14 percent of survivors or from 6 to 8 per-cent of live births) (25,162).
These reviews were reassuring in that the in-troduction of neonatal intensive care apparentlyhad not increased the proportion of survivors whoare seriously handicapped. However, the two re-views covered mortality outcomes only for infantsborn before 1977. At that time, no published datawere available on outcomes for infants with birth-weights below 800 grams, perhaps because so fewsuch infants survived. Moreover, mortality rateshave continued to drop significantly over the last10 years for all birthweight groups under 1500

26
grams, and the possibility exists that infants, whopreviously would have succumbed because oftheir problems, are now rescued through newtechnology and contribute to the incidence of sur-vivors with neurological damage. To determinewhether handicap rates have changed during thelate 1970s and the 1980s, OTA reviewed the liter-ature for reports on morbidity outcomes for in-fants born between 1975 and 1985. The results areshown in tables 10 through 12 by birthweightgroup.
Like birthweight-specific mortality data,birthweight-specific morbidity data are not col-lected on a routine basis in the United States. Thusreports from individual nurseries are the onlyavailable data source that reflects the long-termmorbidity of very low birthweight infants. All ofthe shortcomings discussed previously for the in-stitutional data on mortality hold as well in usingand pooling morbidity data from individual nurs-eries. Differences in the character and experiencesof the study populations yield different results.Moreover, comparisons of morbidity are furthercomplicated by the different ways in which out-come is measured and reported. There are differ-ences in the definitions of abnormalities, in thedetails with which diagnostic categories are speci-fied, in the ages at which followup examinationsare done, and in the measures used in the neuro-developmental evaluations (78,83).
The interrelationship of mortality and morbid-ity is especially difficult to interpret. It is likelythat neonatologists’ attitudes and decisions con-cerning termination of life support for very lowbirthweight infants who manifest severe neuro-logical dysfunction are a major factor in deter-mining the rate of serious morbidity among sur-vivors. Thus, a comparatively high neonatalmortality rate might be expected to be associatedwith a relatively low rate of handicap. Althoughseveral reports on the under 800-gram populationfit this hypothesis (13,60,61), just as many studiesreported relatively high survival and low handi-cap rates (68, 79,80, 161). Overall OTA found noconsistent relationship between mortality and therate of serious morbidity in its literature review,
Determinations of long-term morbidity and dis-ability cannot be made at hospital discharge. The
extent to which researchers were able to followNICU survivors through the first few years of lifeand classify their disabilities varied from studyto study. In general, followup rates were highestin the studies reporting on the smallest birthweightinfants. This is because the tiniest babies are lessnumerous and tend to have problems that encour-age their families to seek ongoing medical care.Conversely, a larger percentage of the NICU sur-vivors with birthweights between 1000 and 1500grams were lost to followup, but many of theseinfants are normal. In all three birthweight groupsexamined by OTA, a substantial portion of theinfants lost to followup died during the post-neonatal period. Although many of the deathswere directly related to complications of prematu-rity and intensive care treatment, sudden infantdeath syndrome (SIDS) was also a major causeof death after hospital discharge. The high post-neonatal mortality rate experienced by very lowbirthweight infants, perhaps 10 to 15 times thatfound among normal birthweight infants, is notwell understood by medical researchers (170,188).
OTA adopted the definitions of handicap usedby the reviewers in the earlier OTA assessmentin order to categorize disparate reports. “Serioushandicaps” are defined as: severe mental retarda-tion (IQ or developmental quotient below 70); ce-rebral palsy of significant degree (spastic diple-gia, paraplegia, tetraplegia, hemiplegia); majorseizure disorders; blindness; and severe hearingdefects (25). “Moderate handicaps” are narrowlydefined to include all infants with a developmen-tal quotient or IQ between 70 and 80. No attemptwas made in this review to capture the “mild” im-pairments that many very low birthweight infantsdevelop later in early childhood or even at schoolage because most published reports follow NICUsurvivors only to 2 or 3 years of age (68). It shouldbe noted that there is a higher incidence of suchrelatively mild handicaps, which include be-havioral, learning, and language disorders, in verylow birthweight infants than in normal birth-weight children (116).
The incidence of serious handicap increases sig-nificantly with decreasing birthweight (tables 10to 12). For infants born between 1975 and 1985,OTA found that 26 percent of surviving infantswith birthweights below 800 grams, 17 percent

27——.
“ -
. .. .. .. .. .. .. .. .. .. .. .. .. .. .

Table 11 .—Handicap Rates in Infants With Birthweights Between 750 and 1000 Grams, 1975-85
Survivors followed after hospital dischargeInfants surviving to Children with Children with serioushospital discharge Total serious handicaps or moderate handicaps
Reference c Year of birth Number Percent Number Percent d Number Percent e Number Percent e
Saigal (139) . . . . . . . . . . . . . . . . 1973-78 32f (49%) 31 (97°/0) 4 (13%) 10 (32%)Knobloch (83) . . . . . . . . . . . . . . 1975-78 — 9 5 (55%) 6 (67%)Marlow (99) . . . . . . . . . . . . . . . . 1976-80 43 (37%) 40 (93%) 10 (250/o) NAOrgill (118) . . . . . . . . . . . . . . . . . 1977-80 48 (59%)
—48 (100%) 7 (15°/0) 10 (21 %)
Cohen (32) . . . . . . . . . . . . . . . . . 1977-80 84 (720/o) 72 (86°/0) 4 (6°/0) 18 (25%)Saigal (140)g. . . . . . . . . . . . . . . . 1977-80 76f (67%) 72 (95°/0) 13 (18°/0) 35 (49%)Walker (180)g . . . . . . . . . . . . . . . 1977-81 58 (50%r) 48 (83°/0) 5 (10%) 10 (21%)Kraybill (87)g . . . . . . . . . . . . . . . 1980 26 (670/o) 25 (96°/0) 3 (12%) 7 (28%)Stewart (161) . . . . . . . . . . . . . . . 1979-83 73h (54%) 54 (74%) 7 (13%) NAPollara (132) . . . . . . . . . . . . . . . . 1983-84 44 (690/o)
—35 (80°/0) 17 (49%) NA —
Pooled total . . . . . . . . . . . . . . 1975-84 434 75 (17%) 96 (31%)f
aseriOu~ ha~di~aP~ are defined as the following: severe mental retardation (IQ Or develop~e~ta{ quotient below 70); cerebral palsy of significant degree, major Seizure disorders, Or blindnessbserious or moderate handicaps Includes all those handicaps defined above as serious PIUS a developmental CIUOtlent Or IQ between 70 and so.csee references In the back of thts case study fOr fUll Cltatl OnSdof those infants surviwng to hospital dischargeeof survivors followed after hospital discharge.fsuwival calculated on regional population of bitihs.glncludes infants with bifthweights between 500 and 800 gramshsuwived to end of first year.I Denominator population is 305 infants.
SOURCE Office of Technology Assessment, 1987

Table 12.— Handicap Rates in Infants With Birthweights Between 1000 and 1500 Grams, 1975-85
Survivors followed after hospital discharge
Infants surviving to Children with Children with ser ious
hospital discharge Total serious handicaps or moderate handicaps
Reference c Year of birth Number Percent Number Percent d Number Percente Number Percent e
Hack (62) . . . . . . . . . . . . . . . . . . 1975-76 153 (76%) 128 (84%) 20 (16°/0) NA —Saigal (139) . . . . . . . . . . . . . . . . 1973-78 147f (83%) 131 (89%) 6 (5%) 26 (20%)Knobloch (83) . . . . . . . . . . . . . . 1975-78 — 79 15 (19%) 28 (35%)Sherman (152) . . . . . . . . . . . . . . 1976-77 34 (81%) 26 (76%) NA 3 (12%)Marlow (99) . . . . . . . . . . . . . . . . 1976-80 226 (65%) 210 (93%) 27 (13%) NAPowell (133) . . . . . . . . . . . . . . . . 1979-81 285f (73%) 276 (97%) NA 31 (11%)Stewart (161) . . . . . . . . . . . . . . . 1979-83 227g (82%) 168 (74%) 9 (5%) NACrombie (36) . . . . . . . . . . . . . . . 1979-83 108 (82%) 77 (71%) 3 (4%) 5 (6%)Pollara (132) . . . . . . . . . . . . . . . . 1983-84 165 (85%) 120 (73%) 20 (17°/0) NA —
Pooled total . . . . . . . . . . . . . . 1975-85 1,215 100 (11%)h 93 (16%) j
lseriOu~ handlCaP~ are d~fi”ed as ~he fOll OWin Q: ~evere ~~”tal ~~ta~dat,~” (IQ ~~ de”~l~~nle”tal quotient below 70), cerebral palsy of slgnlflcant degree, ITlaJOr S(?IZUR disorders; Or bll ndnessbserlou~ or moderate handicaps in~l”des all those handiCapS defined above as serious plUS a development} quotient or IQ be tween 70 and 80Csee references in the back of this case study fOr fUll citations.dof those Infants survlvlng to hospital dischargeeof suwlvors followed after hospital dlschar9efsuwival calculated on regional population of birthsgSuwlved to end of first year.h D e n o m i n a t o r p o p u l a t i o n I S 913 i n f a n t s .
‘Denominator population IS 589 infants.
SOURCE Off Ice of Technology Assessment, 1987

30
of survivors with birthweights between 750 and1000 grams, and 11 percent of survivors withbirthweights between 1000 and 1500 grams havemajor disabilities at 1 or 2 years of age. Of thesurviving infants with birthweights under 800grams, 41 percent have either a moderate or se-vere handicap, while only 16 percent of the sur-vivors with birthweights between 1000 and 1500grams are so handicapped.
These results corroborate the conclusions ofBudetti and his coworkers (25). Within each birth-weight group, the proportion of survivors withserious handicaps has not changed significantlysince the mid-1960s. The earlier review did notreport on infants with birthweights under 800grams, so comparisons over time cannot be madefor this birthweight group. The group of infantsthat was labeled in the earlier review as weigh-ing less than 1000 grams almost exclusively in-cluded infants with birthweights between 750 and1000 grams; the pooled rate of serious handicapfor this birthweight category has not changed sig-nificantly from 1965-75 to 1975-85 (16 to 17 per-cent). Today, however, many more infants withbirthweights below 800 grams are living and con-tributing both relatively more normal and hand-icapped children to the pool of survivors withbirthweights under 1000 grams.
The conclusion that, within birthweight group,the rate of serious handicap among survivors hasnot changed significantly over time masks the con-tribution that neonatal intensive care probably hasmade to improved morbidity, as well as improvedmortality, outcomes. Since many very sick ba-bies who previously would have died are now sur-viving, increasing handicap levels among sur-vivors should be expected. The finding of constantlevels of handicap therefore points to the increas-ing effectiveness of neonatal intensive care forthe long-term developmental outcomes for thesechildren.
Figures 2 and 3 demonstrate graphically the ef-fects of declining mortality on the relative propor-tions of normal and abnormal survivors.4 The
4Figures 2 and 3 reflect mortality and morbidity outcomes for verylow birthweight infants who are born in Level 111 hospitals and haveaccess to neonatal intensive care. Neonatal mortality rates for thegeneral population of very low birthweight infants are significantlyhigher, and morbidity outcomes are unknown. Postneonatal mor-tality is not reflected in the figures, although such deaths probablyhave a substantial impact on overall outcome rates.
Figure 2.—Outcomes for Very Low Birthweight Infants(< 1500 gram) Born in Level III Hospitals, 1980-85
1,000
900
800
700
800
500
400
300
200
100
0
I
1 9 8 0 1971-75
Years
Normal Moderatehandicap
m Serious Neonatalhandicap death
568
59
1980-85
SOURCES: For years 1980-85, Office of Technology Assessment (see tables 7.10, 11, and 12). For years 1980 and 1971-75, P. Budetti, P. McManus,N. Barrand, et al., The Costs and Effectiveness of Neonatal IntensiveCare (Health Technology Case Study #l O), prepared for the Office ofTechnology Assessment, U.S. Congress, PB 82-101411 (Springfield,VA: National Technical Information Service, August 1981).
absolute numbers of both normal and seriouslyhandicapped children increase. Infants with birth-weights between 1000 and 1500 grams make upabout 54 percent of all very low-weight births inthe United States each year. Because of their rela-tive numerical strength, the comparatively lowerhandicap rates of this “larger” infant group mod-erate the overall rates of disability among all verylow birthweight infants. For example, with birthrates at the 1984 level, if today’s neonatal inten-sive care was provided for all very low birth-weight infants, about 2,200 seriously handicappedchildren would survive who would have died in1975. This figure must be balanced against the15,200 net increase in normal infants who wouldalso survive under current conditions. The over-whelming majority of survivors in both the un-der 1500-gram and the under 1000-gram birth-weight groups are normal.

3 1
Figure 3.—Outcomes for Extremely Low BirthweightInfants (< 1000 grams) Born in
1,000
900
700
600
500
400
300
200
100
(
Hospitals, 1960-85
- . u135
Level Ill
32
28
1960 “ 1971-75 ‘
Years
—
75
u Normal u Moderatehandicap
Serious Neonatalhandicap death
SOURCES For years 1980.85, Off Ice of Technology Assessment (see tables 7,10, 11, and 12) For years 1960 and 1971-75, P Budetti, P McManusN Barrand, et al , The Costs and Effectiveness of Neonatal IntensiveCare (Health Technology Case Study #10, prepared for the Off Ice ofTechnology Assessment, U S Congress, PB 82-101411 (Springfield,VA National Technical Information Service, August 1981)
NEONATAL CONDITIONS THAT CAUSE MAJORMORTALITY AND MORBIDITY
Deaths among very low birthweight infants in Respiratoryintensive care are caused primarily by two con-ditions, respiratory distress syndrome and in-traventricular hemorrhage. These conditions, Respiratoryalong with retinopathy of prematurity, are alsoresponsible for most of the long-term disabilitiesthat plague NICU survivors. The sophisticatedtechnology used in neonatal intensive care saveslives but also can exacerbate or even, in somecases, precipitate these problems. The applicationor withholding of such technologies presents anongoing ethical dilemma for neonatologists.
Distress Syndrome
distress syndrome (RDS) is themost common problem in the neonatal nurseryand the primary cause of mortality. It accountedfor 18 percent of all neonatal deaths in 1978 (122).For babies weighing under 1000 grams, over 60percent of the deaths have been attributed to RDSor to intraventricular hemorrhage, and for babiesin the 1000- to 1500-gram category, 25 percentof the deaths are blamed on these causes (11).

32
Photo credit: Strong Memorial Hospital, Rochester, NY
Premature infants with severe respiratory distresssyndrome usually require assisted ventilation.
Very premature infants experience respiratorydistress because they lack an essential substancein the lung (or pulmonary surfactant) that reducesthe surface tension along the alveoli and preventsthe collapse of the pulmonary air spaces. The im-mense strain of having to force the alveoli openwith each breath makes it increasingly difficultfor these tiny babies to breathe independently.The pulmonary surfactant does not begin to coatthe fetus’s alveoli until between the 24th and 28thweeks of gestation, and it is not produced in ma-jor amounts until the 33rd week.
RDS occurs in 14 to 60 percent of prematuredeliveries at gestational ages between 28 and 35weeks (174). Individual clinical centers report aneven higher incidence of RDS among the ex-tremely low birthweight babies. Kitchen and hisassociates reported an overall RDS incidence of
55 percent among the under 150&gram popula-tion (82). In the under 1000-gram group, Vohr andHack found that 82 percent and Saigal and col-leagues found that 74 percent of neonatal sur-vivors had RDS (140,176).
Infants with RDS stay in the hospital on aver-age twice as long as those without RDS (174). In1984 at the University of California at San Fran-cisco perinatal center, babies with RDS stayed inthe NICU almost four times longer than babieswithout RDS and had hospital costs more thanthree times higher (126).
RDS may take mild, moderate, or severe form.Its clinical course is marked by increasing oxy-gen need and often by the need for assisted me-chanical ventilation (breathing machines) to main-tain adequate oxygenation and to remove carbondioxide. The primary problem for RDS babies isthe collapse of the alveoli which makes the workof breathing increase to physiologically intolera-ble levels. Two respiratory therapy techniques,developed over the past 15 years, prevent alveo-lar collapse by keeping up positive pressure onthe lungs between breaths. Continuous positiveairway pressure (CPAP) is used by itself to fa-cilitate breathing, and positive end expiatorypressure (PEEP) is used in conjunction with posi-tive-pressure ventilation. These innovations in res-piratory therapies, as well as improvements inventilator techniques such as the now wide-spread use of continuous flow pressure regulatedventilators, have contributed to diminished sever-ity of RDS (167). Deaths associated with RDShave been decreasing since 1974, though it re-mains the leading cause of neonatal death (122).
Bronchopulmonary Dysplasia
Mechanical ventilation is essential for the sur-vival of babies with severe RDS, but it disruptsthe babies’ normal cardiopulmonary physiology.Its prolonged use leads to a chronic lung diseasecalled bronchopulmonary dysplasia (BPD). (Otherconditions besides RDS can lead to ventilation ofnewborns and thus to BPD; these include pneu-monia, meconium aspiration, patent ductus arteri-osus, and apnea of prematurity (52). ) BPD wasfirst recognized and described in the 1960s (168).By definition, all infants who require mechani-

33
cal ventilation during the first week of life, whoremain dependent on supplemental oxygen formore than 28 days, and who have a characteris-tic chest radiograph have BPD (52).
BPD has become one of the most common se-quelae of neonatal intensive care. A recent reviewarticle concluded that one-third of infants givenmechanical ventilation and weighing less than1500 grams at birth develop chronic lung disease(167). Two multicenter studies of 700- to 1500-gram babies in 1983 and 1984 also reported thatoverall about one-third of the survivors hadchronic lung disease (8,10,69). These studies foundthat female and black babies had significantlylower rates of chronic lung disease than their maleand white counterparts in similar birthweightgroups (10,69). Birthweight was the most signifi-cant predictor of lung damage. While only 19 per-cent of survivors with birthweights between 1000and 1500 grams had chronic lung disease, 51 per-cent of survivors with birthweights between 700to 1000 grams had BPD (69).
Reports from individual clinical centers conflicton the incidence of BPD among extremely smallinfants. Among the tiniest babies (under 800grams), Buckwald and associates found that 75percent of the survivors were still on a ventilatorat 1 month, and Hack and Fanaroff reported that70 percent of the survivors in their hospital de-veloped BPD (24,61). On the other hand, Ben-nett and colleagues, also reporting on babies withbirthweights under 800 grams, found only a quar-ter of the survivors developed BPD (13). Simi-larly, three reports on infants weighing less than1000 grams found 62, 30, and 13 percent, respec-tively, of survivors developed BPD (140,48,71).
Significant mortality and long-term morbidityare associated with BPD during the postneonatalperiod (86). Like RDS, bronchopulmonary dys-plasia can take mild, moderate, or severe forms.About 1 out of 40 infants discharged from the hos-pital with BPD is so severely affected that respi-ratory support continues to be required at home(41,147). Rehospitalization and chronic respira-tory problems are associated with BPD patients.Even after controlling for other risk factors likeintraventricular hemorrhage, prolonged mechan-ical ventilation has been found to be associated
with poor developmental progress during the first18 months of life in very low birthweight infants(21). When low birthweight infants with BPDwere compared to a control group without the dis-ease, the BPD infants had more respiratory dis-eases at 4 and 12 months and more severe neuro-developmental sequelae at 2 years (177). Anotherstudy that followed BPD patients prospectivelyfor 2 years post-term found that 85 percent of thechildren had lower respiratory tract infections and50 percent of the infants required rehospitaliza-tion during their first year (98). Finally, a recentstudy of infants with BPD who were born between1981 and 1983 confirmed the increased incidenceof hospitalization and respiratory problems dur-ing the first year of life, but found that, for sur-vivors, differences with the control group in neu-rodevelopment evident at 1 year had disappearedby 2 years of age (136).
Medical Practices
The detrimental effects of positive pressure ven-tilation have been known since 1965 (28). Thereis now some evidence that the way in which ven-tilatory support is medically managed may be as-sociated with outcome. When Avery and her col-leagues surveyed eight tertiary clinical care centersin 1983 and 1984 for their experience with BPDin infants weighing 700 to 1500 grams, they foundthat some institutions did significantly better thanothers (10). Even after adjustments were made forweight distribution, sex, and race (but not forgestational age), differences among centers per-sisted. Among those centers studied, the intensivecare unit at Columbia University had the best out-comes. At Columbia, the policies for respiratorymanagement are dictated by a single physician,and the policies are followed at all times and forall babies. Instead of resorting to mechanical ven-tilation immediately, nasal CPAP is used to treatRDS early in the course of the disease and dur-ing the weaning from assisted ventilation. At-tempts are made to minimize physical trauma; en-dotracheal tubes are used infrequently and foronly short periods of time and muscle relaxantsare never employed.
Medical practices and the use of technologyvary widely among perinatal centers, and thereare no clearly accepted norms for practice. Fur-

34
Photo credit: Strong Memorial Hospital, Rochester, NY
Coordinated management in the NICU and use ofnon intrusive therapies have been suggested as majorfactors leading to improved outcomes for very low
birthweight infants.
ther systematic research is needed so that relia-ble comparisons among centers can be made andepidemiological methods used to evaluate ventila-tory techniques (167).
Technological Advances
Improvements in existing ventilator techniquesmay hold promise for reducing the incidence ofBPD in the future. In recent years, for example,there has been considerable research on severalventilator techniques, known collectively ashigh-frequency ventilation (HFV), that use rapidventilator rates that may interfere less with nor-mal cardiopulmonary physiology. Thus far, how-ever, HFV has not been proven superior to con-ventional ventilation for treating neonates inrespiratory failure (20).
Another new technology is extracorporealmembrane oxygenation (ECMO) which entirelybypasses the lungs using a process that closelyduplicates the gas exchange function performedin utero by the placenta. ECMO can be used foras long as 2 weeks, allowing time for lung recov-ery by minimizing the harmful influences associ-ated with high-pressure mechanical ventilation.ECMO has been used on more than 300 infantsin 18 centers since 1975, but with very poor out-comes for premature, small infants. The incidenceof intracranial hemorrhage is exceedingly high inthese infants, and the bleeding may be aggravated
by the heparin administered during ECMO. Un-less further research can make ECMO availablefor infants who weigh less than 2000 grams, onlysmall numbers of patients are likely to be treatedby this technology. ECMO is currently indicatedand may be lifesaving for term infants with meco-nium aspiration syndrome, persistent pulmonaryhypertension, or diaphragmatic hernia (189).
The better solution for the problems posed bymechanical ventilation is to avoid the need for itsuse altogether. Two technologies are under devel-opment and testing that could substantially pre-vent RDS in the future. The first is the prenataladministration of glucocorticoids (steroids) tomothers in preterm labor in order to acceleratefetal lung maturation. The other technology,still experimental, is the introduction of exoge-nous pulmonary surfactant into the lungs of thenewborn.
Steroid treatment of women in preterm laborhas been used and studied for 16 years (7). Al-though all the studies support the efficacy of thesteroids in reducing the incidence of RDS in thebabies subsequently born, concerns remain aboutindications for use in specific situations, the in-fluence of the steroids on infection during labor,and the effect of the steroids on the long-term de-velopment of the babies (43). Because of theseconcerns (particularly for patients with prematurerupture of the membranes), some obstetricians usethe steroids either selectively or not at all (29).
A multicenter, 7-year collaborative study onantenatal steroid therapy attempted to resolvethese concerns. Reporting its results in 1985, thestudy confirmed the efficacy of steroids in reduc-ing the incidence of RDS and in decreasing theseverity of the disease in those affected. Further-more, it found no evidence that the risk of infec-tion is increased in the neonate or in the mother.And there is no effect of the steroid on either neu-rological maturation or function or developmentaloutcome during the first 3 years of life. However,the researchers also reported no effect on mor-tality and suggested that the effectiveness ofsteroid therapy is significant only for female off-spring and only when the membranes are intact(174).

35
The collaborative study excluded infants under28 weeks gestational age. A recent, retrospectivestudy in Australia, designed to include a largenumber of very low birthweight infants at highrisk of death, contradicted the findings of the col-laborative study. It found survival is substantiallyimproved by antenatal steroid therapy and thatsurvival improves in both girls and boys (44).
Although the efficacy of steroid treatment is notresolved, the therapy clearly has several limita-tions. It does not work for all babies; at best, itlowers incidence and severity of RDS. And inaddition, because steroid therapy must be initi-ated at least 24 hours before delivery in order tobe effective, for obstetrical reasons many womenin preterm labor cannot be candidates for its use.
Treating surfactant deficiency by administer-ing exogenous natural or synthetic surfactant tothe lungs of very premature babies at or soon af-ter birth has the potential to greatly reduce theincidence of severe RDS. The basic biochemistryand physical chemistry of lung surfactant has beenknown for a long time, but research is ongoingfor the best surfactant mixture, the optimum dose,and the timing and frequency of administration.At least seven recent randomized, controlled clin-ical trials testing natural surfactants (recoveredfrom lung lavage of animals or humans) documentthat surfactant-treated infants have less severeRDS than control infants (51,74,84,102). Thestudies show a lower incidence of clinical RDS,lower ventilator requirements, and less oxygensupplementation in treated than in control infants.The treatment with human surfactant significantlydecreased the risk of death and bronchopulmo-nary dysplasia (102). Several of the studies usingbovine (cow) lung extract also showed decreasesin the risk of death (158). While one recent mul-ticenter trial in Great Britain using synthetic sur-factant found reductions in mortality and the needfor respiratory support (104), other studies to datewith synthetic surfactants have shown essentiallyno benefit for respiratory function (63,183).
In none of the studies do all infants respond tothe surfactant. Therefore, perfecting surfactantreplacement will not be a panacea for RDS. Re-searchers hypothesize that some infants have res-piratory distress from other causes, such as in-fection, or that, in extremely premature infants,
dysfunction might by caused by other structuralimmaturities (9). Large-scale, multicenter trials arebeing undertaken in Europe and the United Statesto continue to test surfactant experimentally. Itis probable that the necessary research and FDAapproval process will take from 1 to 5 years be-fore surfactant therapy will be generally availablefor preterm babies (8,149).
Intraventricular Hemorrhage
Along with RDS, intracranial hemorrhages, orbrain bleeds, are responsible for the most deathsin the neonatal nursery (11). The most danger-ous are intraventricular hemorrhages in whichblood seeps into the cerebral ventricles, small cavi-ties within the brain that secrete and convey cere-brospinal fluid, Almost all serious hemorrhagesoccur within the first or second day after birth(178). Once extensive brain damage has occurredthere is little medicine can offer to improve theprognosis (178). An infrequent additional com-plication for babies with hemorrhage is the de-velopment of hydrocephalus, the dangerous dis-tension of the head caused by the excessivebuildup of cerebral spinal fluid. Fortunately manycases of posthemorrhagic hydrocephalus resolvespontaneously or respond to medical therapy(153).
Premature infants’ blood vessels are particularlyfragile, and a prevalent medical opinion is thatthe capillaries rupture and hemorrhage becauseof fluctuations in cerebral blood flow. Along withother causes including asphyxia, seizures, andpneumothorax, the use of intermittent positivepressure ventilation has been associated withhemorrhage (42,178). It is believed by some thatthe infant’s own respiratory effort, out of syn-chrony with the ventilator, causes changes in thecerebral blood pressure (123). Recent research hasfocused on ways, like muscle paralysis during ven-tilation, to prevent such fluctuating patterns ofcerebral blood flow velocity (123).
Previously recognized conclusively only on au-topsy, the introduction of computed tomographyscanning and later of ultrasound brain scanningrevealed that 31 to 45 percent of infants weigh-ing under 1500 grams at birth have subependymalor intraventricular hemorrhages (42,123). Mosthemorrhages are graded mild and appear to cause

36
no lasting clinical problems. Estimates vary on theproportion of cerebral hemorrhages that are se-vere as well as on the subsequent mortality andmorbidity. Mortality is clearly higher in groupsof infants with hemorrhage, as compared withother infants matched for birthweight or gesta-tional age (101), A partial review of institutionalstudies completed in the 1970s reported that mor-tality from severe hemorrhage ranged between 50and 65 percent and that hydrocephalus developedin 45 to 100 percent of the survivors (153). Morerecent studies have shown much lower fatalityrates of 13 percent (42) and 6 percent (153) fromintraventricular hemorrhage. In one of thesestudies only one infant (6 percent of the survivors)developed progressive hydrocephalus (153), whilein the other study no infant required shunting forhydrocephalus (42).
The incidence and severity of hemorrhage arecorrelated with gestational age and birthweight.Infants born at less than 29 weeks gestation areespecially at risk (42,153). Before 32 weeks gesta-tion, a disproportionate amount of the total ce-rebral blood flow enters the periventricular cir-culation, and thus any disturbance of the bloodflow tends to cause hemorrhage in this region ofthe brain (178). While the association of hemor-rhage with gestational age is well established andfounded on physiological evidence, birthweightalone is not as good a predictor of the likelihoodof hemorrhage. Only one study reported resultsby birthweight category. At the Johns HopkinsHospital in 1980, 90 percent of the babies weigh-ing between 600 and 1000 grams had cerebralhemorrhages (36 percent of the babies had severehemorrhages), but only 26 percent of the infantsweighing between 1000 and 1600 grams had hem-orrhages (6 percent severe). This study found noevidence that the 600- to 800-gram babies hadmore severe hemorrhages than the other infantsin the under 1000-gram” category, although the ti-niest babies did have the highest overall incidenceof hemorrhage (49).
Neurodevelopmental Outcome
Infants with severe intraventricular hemor-rhages have a high rate of later neurodevelopmen-tal handicaps. The risk of developing neurodevel-opmental defects is correlated to the initial degree
Photo credit: March of Dimes Birth Defects Foundation
With appropriate therapy and support, the prognosisfor even seriously handicapped very low birthweight
infants improves over time.
of hemorrhage (30,88,121). In a study of infantsweighing under 1500 grams and born between1976 and 1981, Papile and her colleagues at theUniversity of New Mexico concluded that infantswith mild grades of cerebral hemorrhage had nopoorer outcomes than other babies of similarbirthweight groups without hemorrhage. But theyalso found a major handicap in 58 percent of theinfants with severe intraventricular hemorrhage,and multihandicaps in 45 percent of this group(121). An Australian study of extremely pretermbabies born between 23 and 28 weeks gestationin 1981 reported that 8 of 12 infants with severehemorrhage (67 percent) developed major dis-abilities (30). The study at Johns Hopkins Hospi-tal of low weight babies born in 1980 found lessdisastrous results. At 12- to 22-month followupexaminations, of 11 babies who had severe hemor-rhages, 6 were normal, 3 had moderately retardeddevelopment, and only 2 babies or 18 percent hadserious intellectual and motor impairment (153).

37
Retinopathy of Prematurity
Another affliction affecting premature infantsis retinopathy of prematurity (ROP). The diseaseoccurs in progressive stages beginning with reti-nal vasoconstriction, proliferation of blood ves-sels, scarring (cicatricial disease) of the retina, reti-nal detachment, and ultimately blindness (137).The disease is not invariably progressive andblindness is by no means an inevitable outcome.Many cases spontaneously regress to normal. Per-haps 25 percent of those with cicatricial diseasego on to blindness (124).
The epidemic of ROP between 1942 and 1953which resulted in about 10,000 blind children isperhaps the most widely known example of iatro-genic disease (156).5 Because of technological ad-vances, it was routine during that decade toadminister high concentrations of oxygen to es-sentially every premature infant, and it was notuntil 1954 that a large, multicenter cooperativestudy indicted oxygen as the culprit in the ex-ponential growth of ROP. The practice of rou-tine oxygen administration was quickly aban-doned, and the oxygen administered to infantswith respiratory distress was given in much lowerconcentrations. But while there was a sharp de-cline in the prevalence of ROP during the 1950sand 1960s, researchers started reporting results bythe early 1960s that created increasing uneasinesswith the blanket policy of oxygen restriction forall premature infants. When oxygen usage wascurtailed, studies showed that neonatal mortal-ity and the incidence of spastic diplegia (a formof cerebral palsy) increased among premature in-fants. It was later estimated that for every caseof blindness prevented, approximately 16 babiesdied due to inadequate oxygenation (37).
Today’s medical opinion is that the cause ofROP is unknown but likely multifactorial, withoxygen being but one critical factor. Other riskfactors suspected of playing a role in the etiologyof ROP include too little oxygen in utero, infec-tion, intraventricular hemorrhage, apnea, bloodtransfusions, hypercarbia, hypocarbia, patentductus arteriosus, prostaglandin synthetase inhi-
5At the time of the epidemic, the disease was called retrolentalfibroplasia. This term, still in use today, refers to the proliferationof scar tissue during the latter stages of the disease.
biters, vitamin E deficiency, assisted ventilation,lactic acidosis, and prenatal complications (97).But overwhelmingly the primary risk factor is ex-treme prematurity, with almost all cases confinedto this vulnerable group (137). The blood vesselsin the immature retina are still developing, andit is believed that any disturbance in retinal cir-culation, whether too much oxygen or too little,can lead to the vessels’ disordered and twistedgrowth. The very low birthweight, premature in-fant suffers from a number of the risk conditionsthat can disturb retinal circulation, and some casesof ROP appear to be unavoidable despite carefulattention to oxygen therapy and monitoring.
Advances in neonatal care methods and the sur-vival of more small and critically ill infants havecontributed to a resurgence of ROP, which somecall a second epidemic (137). Infants weighing un-der 1500 grams at birth are at greatest risk. Boththe incidence and the severity of retinal diseaseincreases with progressively lower birthweightand gestational age.
A 1981 review of the literature estimated thatamong infants weighing between 1000 to 1500grams at birth, 2,2 percent have scarring ROP and0.3 to 1.1 percent are eventually blinded. For in-fants under 1000 grams, approximately 22 to 42percent have cicatricial ROP and 5 to 11 percentare blinded (124). By contrast, a Canadian popu-lation-based study conducted from 1977 to 1980found that only 13 percent of infants under 1000grams developed cicatricial disease, but overall7 percent of the survivors were blinded (140). Twomore recent studies of infants in NICUs weigh-ing under 800 grams have reported that 25 per-cent (61) and 10 percent (80) developed cicatri-cial ROP. Finally, a controlled study investigatingROP from 1977 to 1980 in an Australian NICUfound a lower incidence of serious scarring in theextremely low birthweight group than previouslyreported. Among the infants weighing under 1000grams, only 3 percent developed scarring ROP;unfortunately all of them were blinded. This studyalso found in the 1000- to 1500-gram populationthat 2 percent developed cicatricial disease and1 percent was blinded (187). These incidencefigures agree with Phelps’ estimates.
Although no technological fix is on the hori-zon, there has been renewed interest since the

38
1970s in vitamin E as a preventive measure againstROP. Vitamin E was first used to prevent ROPin 1949. Although that initial study did find a sig-nificant effect, subsequent trials failed to confirmits efficacy, and when the role of oxygen was iden-tified by the collaborative trial in 1954, bothROP and its possible relation to vitamin E weredropped from the research agenda (125). Luceyand Dangman reviewed five recent clinical trialsthat used vitamin E prophylactically to treat ei-ther very low birthweight patients or patients withRDS. The results of these studies, though diffi-cult to compare, are conflicting. Some showed a
reduction in both incidence and severity of ROP,others showed a lessened severity with no effecton incidence, and still others found no significanteffect at all on the occurrence of ROP (97). Whilethese results offer the promise of at least reduc-ing the worst ROP, several researchers have urgedcaution and extensive further research. There aresuspicions that vitamin E treatment may exposepremature infants to increased risks of necrotiz-ing enterocolitis and intraventricular hemorrhage(97,125). The potential negative side effects ofvitamin E may outweigh the possible benefits.

Chapter 4
Financing Neonatal Intensive Care

Chapter 4
Financing Neonatal Intensive Care
INTRODUCTION
Neonatal intensive care is a very costly servicefor hospitals to provide. In the 12 children’s hos-pitals studied by the National Association ofChildren’s Hospitals and Related Institutions(NACHRI), neonates represented only 8 percentof the admissions, but 21 percent of the patientdays and 25 percent of the hospitals’ costs (110).Neonatal care was the most costly category ofservice provided by the children’s hospitals and,except for organ transplantation, involved themost extreme lengths of stay.
Because neonatal intensive care is so expensive,it is important to examine the mix of third-partypayers responsible for reimbursing providers andthe extent to which payments cover the costs ofproviding care. Few studies directly examine theinsurance status of neonatal intensive care unit(NICU) patients. Of 580 admissions to two NICUsin San Francisco in 1984, 30 percent were cov-ered by Medicaid, 47 percent by commercial in-surance, and the remaining 23 percent by otherpayers, self-pay, or were not covered under anyplan (126). Of course there is considerable varia-tion among hospitals. For example, while Med-icaid admissions constituted 24 percent of the to-tal cases in NACHRI’s study, the proportion ofMedicaid admissions to total admissions rangedfrom 11 to 42 percent in individual children’s hos-pitals (110).
In general, hospitals consider the Medicaid pro-gram to be a poor payer. Data from the Amer-ican Hospital Association survey show that whileMedicaid paid only 19.8 percent of total net rev-enues in children’s hospitals, Medicaid benefici-aries accounted for 23.3 percent of all inpatientdays (107). Especially in the past, hospitals havefinanced the provision of such uncompensatedcare—charity care and bad debts—by “cost-shift-ing” and charging private sector payers—commer-cial insurers, some Blue Cross plans, and patients
who pay their own bills—proportionately morethan their share of the costs of the care.
Hospitals typically charge a daily rate for gen-eral care in the NICU and add separate chargesfor ancillary and special services that accrue dur-ing the hospital stay. But these charges may beunrelated to actual costs. When particular serv-ices have unfavorable payer mixes or are so ex-pensive that their costs cannot be fully reimbursed,hospitals may underprice or not fully allocateoverhead costs to the services. In general, bothintensive care services and pediatric services ingeneral hospitals fall into this category. In prac-tice hospitals often subsidize these losses by pric-ing other services, which are used by a greaterproportion of charge-paying patients, much higherthan their actual costs. The emergence of com-petitive forces in today’s health care market, how-ever, is curtailing the ability of hospitals to sub-sidize uncompensated care through cost-shiftingamong payers.
One reason is that the proportion of patientspaying on the basis of charges is decreasing. Tokeep their occupancy levels high, more and morehospitals are participating in preferred providerorganizations (PPOs). In return for negotiatedlower prices, the PPO beneficiaries (usually formercharge-paying patients) agree to use the designated“preferred providers. ” A conservative estimate ofthe number of people enrolled in PPOs in the sum-mer of 1986 was about 16.5 million (40). Healthmaintenance organizations (HMOs), which typi-cally have risk-sharing or prospective paymentarrangements with their hospitals, have also in-creased their share of the marketplace. HMO sub-scribers increased from 3.5 million in 1972 to 27.7million by 1987 (73,169). Insurance companiesthat previously paid on the basis of charges formost patients are also using other methods to limithospital payments. Like the public payment pro-grams, Medicare and Medicaid, private insurers
4;’

42
are moving toward prospective methods of reim- but, as payment rates are tightened to eliminatebursement. Prospective payment can take many profit, all will ultimately limit the opportunity offorms (cavitation, per diem, or per case payment), providers to cost-shift.
REIMBURSEMENT PRACTICES
Since the enactment of the Medicare prospec-tive payment system in 1983, seven Blue Cross/Blue Shield (BC/BS) plans have implemented pay-ment systems based on diagnosis-related groups(DRGs), and another three plans are involved inpilot programs using DRGs (134). As of June 1985,13 States had also adopted some form of prospec-tive per case payment system in their Medicaidprograms (see also the following section on Med-icaid policies) (91). Although the mechanisms usedby these systems to calculate the payment amountsfor the DRGs usually differ from the Medicare sys-tem as well as among BC/BS plans and Medic-aid programs, there is considerable concern in theprovider community about how fairly DRG pay-ments would reimburse hospitals for neonatal in-tensive care (110,130).
NACHRI simulated 1984 Medicare DRG pay-ments in 12 children’s hospitals and found the hos-pitals suffered their greatest financial losses fromthe neonatal cases (110). Without heavy relianceon special payments for outliers (cases with sta-tistically unusual lengths of stay), Medicare’s pay-ments for neonatal cases would have fallen far be-low the hospitals’ operating costs. The neonatalcases involved the highest incidence of outliers ofany major DRG grouping in the children’s hos-pitals. Similarly, another study analyzing NICUadmissions in six teaching hospitals in Californiafound that when the Medicare program’s defini-tion of outliers was used, half of all admissionswere classified as outliers (130). A study of 1981newborn discharges in Maryland also found 50percent of charges in the three prematurity DRGswere generated by outliers (16).
NACHRI has proposed replacing Medicare’s 6neonatal DRGs with 30 new DRGs based on 6birthweight categories and further subdivided by
the presence of major diagnoses, surgery, and theprolonged use of mechanical ventilation. Theirproposed set of DRGs would explain 28 percentof the variation in length of stay among neona-tal cases while the current Medicare DRGs explainonly 16 percent of the variation (111). Overall,NACHRI concluded that, for children’s hospitals,the measurement of neonatal care is the most crit-ical issue in constructing a prospective paymentsystem, and that the volume of neonatal cases isa major factor in determining the balance of costsand revenues under the various reimbursementschemes (110).
Even if payments for neonatal care equal costsunder prospective payment methods, hospitalswill continue to have revenue shortfalls becauseof their eventual inability to cost-shift under thesepayment methods. Hospitals have recourse toother sources of revenue for uncompensated ne-onatal care. Block grant funds available to Statesunder the Maternal and Child Health ServicesProgram are sometimes used to directly fund ne-onatal intensive care for children whose familyincomes are not low enough to qualify them forMedicaid (135). Moreover, all States have gen-eral assistance programs that reimburse healthproviders for care rendered to certain Medicaid-ineligible population groups (12). The extent towhich these State and county payment programsactually cover hospital losses depends heavily ongeographic location, as States vary widely in cov-erage and level of payment. Finally, some Stateprograms, instead of targeting indigent individ-uals, directly support hospitals providing substan-tial amounts of indigent care. These States gen-erate revenues for uncompensated care throughtaxes or through surcharges on all hospitals’ rev-enues (12).

43
MEDICAID
The Medicaid program is the major source ofpublic funding for low-income women and babies.About 6 percent of all newborns whose deliver-ies are subsidized by Medicaid require neonatalintensive care, but this care is so expensive thatit represents about 30 percent of all Medicaid ex-penditures for maternity care (77). Medicaid paysfor about 10 percent of all births in the UnitedStates, but with wide variations across States.Within Federal guidelines, each State designs andadministers its own program. As a result there aresubstantial State-to-State differences in eligibilityrequirements, benefits, limits on services, andreimbursement policies,
Policies
Medicaid coverage for newborns is dependenton the eligibility of their mothers. Although theincome criteria for Medicaid eligibility are so strictthat many poor people are excluded from cover-age, family structure and employment status areno longer barriers to eligibility for pregnantwomen and their babies. Legislation passed in1984 and 1986 relaxed eligibility restrictions onfirst-time mothers and married pregnant womenwith some income from employment. The Defi-cit Reduction Act of 1984 (Public Law 98-369) alsorequired States automatically to cover the healthcosts of newborns in eligible families. Previously,each newborn infant had to be individually cer-tified as eligible for Medicaid, sometimes leadingto administrative delays in coverage with costlyramifications for providers (39), Furthermore, theConsolidated Omnibus Budget Reconciliation Actof 1986 (Public Law 99-272) mandates Medicaidcoverage for women and newborns for 60 dayspostpartum, regardless of changes in the eligibil-ity status of the mother. Thus, any newbornwhose mother met the income requirements forMedicaid prior to delivery is assured of at least60 days of automatic Medicaid coverage.
Inpatient hospital services, including neonatalintensive care, are mandated covered services un-der the Federal guidelines for Medicaid. However,some States place limits on the number of daysper admission or per year that a beneficiary is cov-
ered for inpatient care. As of June 1985, 13 Stateshad such day limits, although several programsallowed extensions for medical necessity (91).Coverage of inpatient days is also limited accord-ing to diagnosis in some Medicaid programs. Like-wise, States can limit the number of covered phy-sician visits. Thirteen States limit physicians’inpatient visits, but in general the limits are oneor two visits per day for allowable hospital days(171).
Prior to the Omnibus Budget Reconciliation Actof 1981, which freed States from following tradi-tional Medicare payment practices, States gener-ally used reasonable cost-based reimbursementprinciples. By June 1985 only 14 Medicaid pro-grams still used the retrospective per diem method(91). Because of both economic and political pres-sures, most States adopted alternative hospitalreimbursement strategies in their Medicaid pro-grams. As discussed earlier, 13 States use someform of prospective per case rate, either on a sim-ple per admission basis or a discharge diagnosisbasis. Except for Utah, all these programs useState-specific data, rather than Medicare data, tocalculate DRG weights (134). The data sourcesused include hospital cost report data, paid claimsfiles, and Medicaid claims data. Another 21 Statesuse a prospective per diem as the unit of payment(91). Although diagnosis is not taken into account,some of these systems do provide different perdiem rates for general inpatient care and for in-tensive care. Finally, five States use an annual-ized payment system whereby the hospitals re-ceive a negotiated or contractual global fee fromMedicaid. Twenty-four of the State Medicaid pro-grams have developed special adjustments thatrecognize costs associated with the provision ofuncompensated care.
Expenditures for NeonatalIntensive Care
Table 13 shows that of babies whose deliver-ies are reimbursed by Medicaid, the proportionrequiring neonatal intensive care varies widely byState. In the 13 States responding to a survey bythe Alan Guttmacher Institute, the proportion of

44
Table 13.—Medicaid Recipients in Neonatal Intensive Care Units (NICUs), and Medicaid Expenditures,Selected States, 1983-85a
Percent of total Total Medicaid Medicaid expenditureNumber of Medicaid Medicaid births expenditures for NICUs per infant
State and year infants in NICUsb treated in NICUs ($ x 1,000)b in NICU
California (FY84) . . . . . . . . .Florida (FY85). . . . . . . . . . . .Idaho (CY85) . . . . . . . . . . . . .Louisiana (CY83) . . . . . . . . .Maryland (FY85) . . . . . . . . . .Massachusetts (FY83). . . . .Michigan (FY85) . . . . . . . . .Missouri (FY85) . . . . . . . . . .Nevada (CY84) . . . . . . . . . . .North Carolina (FY84) . . . . .Ohio (FY85). . . . . . . . . . . . . .Oregon (FY85) . . . . . . . . . . .Pennsylvania (FY85) . . . . . .South Carolina (FY85) . . . . .Tennessee (FY85) . . . . . . . .Vermont (FY85) . . . . . . . . . .Washington (FY85) . . . . . . .Wisconsin (CY83) . . . . . . . .
6,1523,965
—395477
1,052790440
55——
2851,449
418——
359428
6.220.3
—4.34.38.82.64.63.7——6.26.65.7——2.93.2
$92,06912,256
8807,3229,703
—19,717
1,6231,6183,012
48,410578
8,6813,7182,101
4391,7762,164
$14,9663,091
—18,53820,341
—24,9583,689
29,414——
2,0285,9918,894
——
4,9475,056
aMethodology for estimates: Louisiana —estimated neonatal intensive care data furnished by State; Massachusetts—reported neonatal intensive care data based onpartial reporting by the State, reported dataon infants in neonatal intensive careas a percentageof Medicaid births are only for facilities reporting both kindsofdata; Ohio—reported neonatal intensive care expenditures, annualized from 13 months of data; South Carolhra and Washington—estimated neonatal intenswe caredata furnished by the State; Vermont—reported neonatal intensive care expenditures, annualized from 14 months of data,
bExcludes prepaid Plans
SOURCE A M Kenny, A. Torres, N Dittes, et al,, “Medicaid Expenditures for Maternity and Newborn Care in America, ” Family Planning Perspectives 18(3):103-110,May/June 1986
Medicaid babies admitted to NICUs averaged 6.1percent but ranged from only 2.6 percent in Mich-igan to an overwhelming 20.3 percent in Florida.The 6.1 percent average for all surveyed Statesis consistent with national data on the proportionof all newborns who receive intensive care. (Seech. 2.) Because the Medicaid population is gen-erally considered to be at higher risk, a greaterincidence might have been expected (77).
Table 13 also shows enormous differences inthe per-patient Medicaid payments for neonatalintensive care. Of the 12 Medicaid programsresponding to the 1985 survey, average NICUexpenditures range from $2,000 in Oregon to$29,400 in Nevada. The average expenditure inthe 12 States is $11,800 (77). The average Medic-aid expenditure is lower than the average hospi-tal costs reported for NICU infants in children’shospitals and teaching hospitals, but higher thanthe average costs for all sick neonates in Mary-land Level III hospitals. (See ch. 2.) The NACHRIstudy found that Medicaid patients in children’shospitals are more costly to treat than the gen-eral pediatric population and represent a more dif-ficult case mix (110).
It is difficult to draw conclusions from the dra-matic variation in expenditures among States inpart because the scope of each State program isso different and in part because of the nature ofneonatal intensive care. The NACHRI study ofchildren’s hospitals showed that neonatal care isthe most costly service provided by the pediatrichospitals and involves the longest lengths of stay.Therefore, in States that extend Medicaid bene-fits to the medically needy (people who do notmeet income requirements until they “spend-down’” on medical expenses) babies not normallyqualified for Medicaid may become eligible be-cause they are in neonatal intensive care units.In addition, the clinical composition of the Med-icaid NICU populations in the States respondingto the survey is unknown. Because extreme out-liers are common in neonatal intensive care, a fewcases with extraordinary costs could severely skewa State’s average expenditures in a single-yearreporting period.
‘Through the “spend-down” provision, families or individuals,who meet all the categorical requirements for Medicaid except in-come, can become eligible for Medicaid under the medically needyprogram if they have high medical expenses that reduce income be-low the medically needy maximum.

Chapter 5
Access to Neonatal Intensive Care

Chapter 5
Access to Neonatal Intensive Care
INTRODUCTION
The concept behind regional perinatal care isa coordinated, cooperative system of physiciansand hospitals in which maternity patients andtheir newborns at high risk are identified early andthe optimal techniques of obstetrics and pediatricsare appropriately applied (34). Numerous studiesdocument the higher survival rates for very lowbirthweight infants born in Level 111 hospitalsversus those born elsewhere within the same geo-graphic area. Table 14 summarizes these reportsand lists, for comparative purposes, neonatalmortality rates for several geographic regions andfor the United States as a whole. In those popu-lation-based studies that identify place of birth by
hospital type, the survival rates for very low birth-weight infants born in perinatal centers are sig-nificantly better than for those born in either LevelI or Level II hospitals. ’ In New York City, for ex-ample, Paneth and his colleagues concluded thatin 1978 preterm and low birthweight infants born
IThe single exception was a 1978 study in Iowa which found highersurvival rates in small Level I hospitals than in Level 111 hospitalsfor very low birthweight infants. Since this was after the regional-ized system was in place, a likely explanation is that physicians work-ing in the smallest hospitals referred the highest risk obstetric casesto the perinatal center (66). Moreover, a followup study showedthe survival advantage in small Level 1 hospitals disappeared after1978. Babies born in the Level 111 center were most likely to survive(67).
Table 14.— Regional Neonatal Mortality Ratesa for Very Low Birthweight Infants, 1976.81
Birthweight (grams)
Reference b Year of birth Population < 1000C
1001-1500C < 1500
Saigal (139)d. . . . . . . . . 1976-78
Paneth (119) . . . . . . . . . 1976-78
Vogt (175) . . . . . . . . . . . 1977Hein (66) . . . . . . . . . . . . 1978
Goldenberg (54). . . . . . 1976-80
Cordero (35) . . . . . . . . . 1977-79
Gortmaker (59). . . . . . . 1978-79
Shapiro (151) . . . . . . . . 1978-79Saigal (140)d. . . . . . . . . 1977-80
Kitchen (81)d . . . . . . . . 1979-80
Newns (1 14) . . . . . . . . . 1979-81
Buehler (26) . . . . . . . . . 1980-81U.S. Department of
Health and HumanServices (172)h. . . . . 1980
aDeathS Der 1.000 live births
Hamilton-Wentworth County, Ontario . . . . .New York City . . . . . . . . . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Southern California. . . . . . . . . . . . . . . . . . . . .Iowa. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Alabama . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Franklin County, Ohio . . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3 States Louisiana, . . . . . . . . . . . . . . . . . . . . .Tennessee, Washington . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8 geographic areas . . . . . . . . . . . . . . . . . . . . .McMasters Health Region . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Victoria, Australia . . . . . . . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .West Midlands, England . . . . . . . . . . . . . . . .Level Ill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Georgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
U.S.A. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
617——
628f
——
663497
521g
484g
—541462744710713522642
648
122529’487e
241——
212118
580e
470’185139
—————
276175161
187
343
371f
470440——
——
439————
417267—
431
bsee references in the back of this case study for full CitatlOnScsome studies repofled birthweight categories as 500-999 and 1000-14999dDeaths reported to hospital dischargeelncludes 501. to 1250-g InfantsfBi~hWelght Categories 701 to 1000 and 701 to 15009glncludes 750. to 1000-g infantshRates for singleton bidhs
SOURCE Off Ice of Technology Assessment, 1987
47

48
Photo credit: Yale University and March of Dimes Birth Defects Foundation
Identifying high-risk pregnancies and appropriatelyreferring mothers to perinatal centers is key
to regionalization.
outside Level III centers had a 24 percent higherrisk of dying (120). During the same time period,Gortmaker and associates studied birth and deathcertificates in four States and found that black in-fants with birthweights between 1000 and 1500grams were more than twice as likely to die dur-ing the neonatal period if they were born in a ru-ral hospital instead of in a perinatal center (59).2
One component of regionalization is the effi-cient transfer of sick newborns from their hospitalof birth to facilities capable of providing sophis-ticated critical care. But even a well-functioninginfant transfer system cannot erase the mortalitydifferences across hospital levels. In the New YorkCity study, deaths were assigned to hospital ofbirth to assess the effect of interhospital transporton neonatal mortality. Despite the transfer of 48percent of the low birthweight infants from theLevel I hospitals to Level 111 units, the neonataldeath rates were significantly higher in Level I hos-pitals (119). Thirty percent of all neonatal deathsin the study population occurred in the first 4hours of life. These early deaths cannot be influ-enced by infant transport and point to difficul-ties in the resuscitation and immediate neonatal
‘This was the most disadvantageous differential in survival re-ported in the study, and it should be noted that overall survivalamong black infants was greater than among white infants at thesame level of hospital care (59).
management of low birthweight infants in themore poorly equipped and staffed hospitals.
The advantages and disadvantages of neona-tal versus antenatal (maternal) transfer continueto be argued in the medical literature. Somestudies find no significant differences in mortal-ity (17,103) and others report advantages for thoseinfants referred prior to delivery (64,89), but allthe institutional studies report only on the infantswho reach the intensive care unit. The newbornsselected for transfer introduce bias into thesestudies. On the one hand, the sickest and mostpremature neonates may die at referring hospi-tals before transport can be arranged, and trans-fers could therefore be more viable than their co-hort. On the other hand, preterm infants withoutmorbidity are probably cared for at their hospi-tal of birth rather than being transferred. More-over, transported infants may suffer inadequatetemperature maintenance or delays in the initia-tion of mechanical ventilation before their admit-tance to the neonatal intensive care unit (NICU),leading to a relatively sicker group of transferredbabies (81).
Several population-based studies support ma-ternal over neonatal transport. In Hamilton-Wentworth County in Ontario, researchers esti-mate that the pre-delivery transfer of selectedpregnant women to the regional center accountedfor 28 percent of the improvement in survivalamong the very low birthweight babies born af-ter the introduction of neonatal intensive care(157). In the British Mersey Region in 1980, ne-onatal survival was significantly better for thosevery low birthweight infants who were transferredprior to birth than for infants who were not trans-ferred or were transferred after delivery (93).Moreover, the difference between the survival ratefor those infants transferred before delivery andthose infants born to mothers who had bookedat the perinatal center was not significant. Andin the State of Victoria, Australia in 1979 and1980, both survival and outcome were better fortertiary center births than for those born elsewhere(81). The Australian study, which examined onlyinfants with birthweights under 1000 grams,found a significantly higher prevalence of severefunctional handicaps in the outborn children thanin either the inborn or the antenatal transfer

49
groups. Several other institutional studies also re-port an increased incidence of intraventricularhemorrhage or respiratory distress syndrome ininfants transported neonatally as compared withinborn infants, implying these infants were not
LEVEL II HOSPITALS
Besides questioning the efficacy of relying onneonatal transport from Level I hospitals, thepopulation-based study in New York City alsoraises doubts about the effectiveness of neonatalintensive care in Level 11 facilities. The studyshowed that while there was a survival advan-tage for low birthweight babies in a Level II hos-pital over a Level I hospital during the first 4 hoursof life, that advantage disappeared by 28 days.Improvements in neonatal mortality rates from1976 to 1978 were statistically significant only forinfants born in Level III units. The researchersconcluded that intrapartum management andpostnatal stabilization were performed well inLevel II hospitals, but that the management oflater complications of low birthweight such as res-piratory failure was less expertly handled (119).
Paneth and his colleagues blamed the virtualabsence of infant transfers from Level II units toLevel 111 facilities for the discouraging mortalityrates (120). Support for these views comes fromthe State Division of Health Services in NorthCarolina. Their study of perinatal mortality ratesfrom 1969 to 1979 for very low birthweight in-fants in North Carolina found that by 1979 theLevel II centers had higher mortality rates thaneither of the other two hospital levels (117). Thisstudy also concluded that Level II hospitals sel-dom referred infants or maternity patients. Theauthor urged greater participation in a coordi-nated referral system.
One reason Level II hospitals might not referhigh-risk mothers and infants to nearby Level IIIhospitals is competition. A major way that hos-pitals compete for patients is through the scopeand quality of services. Childbirth is often a fam-ily’s first contact with hospitalization. Transferof mother or child to a nearby Level III hospitalcould jeopardize the family’s continuing relation-
adequately stabilized at birth (31,89,103). Al-though the birth of a premature infant cannot al-ways be anticipated, there is ample evidence that,ideally, pregnant women at high risk should betransferred to a perinatal center prior to delivery.
ship with the Level II institution. Particularly inurban settings, where competition among hospi-tals is keenest, Level II facilities may be reluctantto refer to Level III units (128).
Since the New York City and North Carolinastudies, there has been a nationwide movementto upgrade the capabilities of Level II units (144).Conversely, some Level II hospitals have termi-nated their specialized neonatal intensive careservices. In New York City, for example, the num-ber of facilities offering Level II nursery servicesdeclined from the study period high of 20 to only14 in 1982 (65,120). Moreover, the extent to whichthere is a problem may well be related to the re-gion of the country. For example, a Level II nurs-ery in Georgia, which published its experience for1976 to 1978, referred 62 percent of its newbornswith birthweights under 1500 grams to a Level IIIfacility (76). The Level II facility unit consideredthat its capabilities included the care of moder-ately ill newborns weighing 1500 grams or moreand convalescing neonates who had been returnedfrom the Level III facility.
The guidelines published by the Committee onPerinatal Health in 1977 and reiterated jointly bythe major professional associations in 1983 spe-cifically list gestation of less than 34 weeks orbirthweight of less than 2000 grams as indicationsfor transfer from Level II units to Level III units(4,34). But the American Academy of Pediatricsacknowledged the wide range of functional capa-bilities existing within the definition of a Level 11unit in a 1980 statement by its Committee on Fe-tus and Newborn (3). Some units provide careonly slightly more complex than Level I nurser-ies, while others have capabilities approachingLevel III centers. The referring practices of thesecenters may vary just as widely. And while theCommittee on Fetus and Newborn clearly states

50
that it is undesirable for Level II units to provide ing liaison and consultation with a Level III center.neonatal cardiology and surgery services, no men- Each Level II unit is urged to assess its own capa-tion is made of referring practices for low birth- bilities for delivering care in terms of personnelweight infants beyond the requirement for ongo- and facilities.
CONCENTRATION OF BIRTHS IN LEVEL Ill HOSPITALS
Although regionalization is often given creditfor many of the improvements in perinatal out-come over the last decade, little is known aboutthe extent to which high risk mothers and infantsare actually redistributed to the appropriate levelsof care. Several groups have reported compari-sons of areas that did or did not have a regional-ized program. In 1975, the Robert Wood JohnsonFoundation funded eight sites to promote coordi-
Photo credit: Kay Chernush, photographer,Children’s Hospital National Medical Center, Washington, DC
Time is crucial in the transport of very sick newborns.
nated systems of perinatal care for entire geo-graphically defined regions, comprising about 6percent of the births in the United States. Anevaluation compared mortality rates both beforeand after regionalization and in program and com-parison regions. Neonatal mortality rates declinedin both types of regions, but no greater reductionwas noted for the program-funded regional net-work. The investigators concluded that region-alization had become widespread and extendedinto the comparison areas without the encourage-ment of specific funding (100). Likewise, Siegeland colleagues looked at two comparable areasin North Carolina (one funded to develop a peri-natal system) and reached much the same con-clusions as the Robert Wood Johnson Foundationresearchers (155). However, a third programlaunched in 1979 specifically to improve perina-tal health care (including high-risk maternal refer-rals to Level III centers) in 10 rural areas with his-tories of high infant mortality did show sharpdeclines in neonatal mortality rates while rates incontrol areas did not change (58).
The Robert Wood Johnson Foundation evalu-ation also studied the extent to which high-riskbirths occurred in tertiary care centers. By 1979,almost 60 percent of all very low weight birthsin the demonstration areas were delivered inperinatal centers, compared with only 36 percentat the beginning of the decade. Similar changesoccurred in the comparison areas, although thepercentage of very low weight births in the LevelIII units was lower than in the demonstrationareas (100). Those results, along with the resultsof other studies examining the concentration ofvery low weight births in Level III units, areshown in table 15. All the studies demonstrateda shift in the site of delivery over time, with high-risk deliveries increasingly moved to the perina-tal centers. Such changes indicate that with region-alization some antenatal assessment of risk is

5 1—
occurring and that the management of high-riskpregnancies is being transferred to the Level IIIunits before delivery.
But table 15 shows there is wide variationamong areas in the extent to which infants of verylow birthweight are born in Level III hospitals.The largest area, the Robert Wood Johnson Foun-dation regions representing 6 percent of all birthsnationally, shows the highest concentration ofvery low weight births in tertiary centers. Iowa,a rural State, shows one of the lowest concentra-tions. However because of low population den-sity and distance considerations, a single Level IIIcenter serves the entire State, and Iowa is con-sidered to be successfully regionalized (66).
The degree to which access to Level III serv-ices varies within regions among different sub-groups in the population is difficult to determine.Gortmaker and colleagues examined racial andurban/rural differences in four States. (See table15. ) The lowest concentration of very low weight
births in Level 111 centers occurred among whitesin Louisiana and Ohio; 23 percent of white verylow birthweight infants were born in regionalcenters in these States. Black infants, in general,had better access to specialized services. In Ten-nessee more than 50 percent of the black very lowbirthweight infants were born in perinatal centers.Residents of rural areas were always less likelythan their urban counterparts to be born in LevelIII units, but again, black rural infants were morelikely than white rural infants to be born in spe-cialized centers (59).
These data on the concentration of very lowweight births in Level III centers do not fully de-scribe the extent to which sick newborns actuallyreceive services in Level 111 units. The contribu-tion of infant transport systems to increased ac-cess cannot be assessed. However, the wide vari-ation among geographic areas in the concentrationof high-risk births points to inequities in the avail-ability of neonatal intensive care.
Table 15.—Concentration of Births of Infants Weighing Less Than 1500 Grams in Level Ill Hospitals— —
Births in Level Ill hospitals
< 1500 grams All birthsReference a Year of birth Population (percent) (percent)
Hein (66) . . . . . . . . . . . . . . . . . . . . . . . . 1978 Iowa . . . . . . . . . . . . . . . . . . . . . . . . . . . 23 7Nugent (1 17) . . . . . . . . . . . . . . . . . . . . 1979 North Carolina . . . . . . . . . . . . . . . . . . 47McCormick (100) . . . . . . . . . . . . . . . . . 1978-79 8 Robert Wood Johnson
Foundation geographicareas. . . . . . . . . . . . . . . . . . . . . . . . . 59 43
Comparison Areas . . . . . . . . . . . . . . . 47 31Gortmaker (59) . . . . . . . . . . . . . . . . . . . 1978-79 LA: white, urban . . . . . . . . . . . . . . . 27
black, urban . . . . . . . . . . . . . . . 59white, rural . . . . . . . . . . . . . . . . 14black, rural . . . . . . . . . . . . . . . . 31
Ohio: white, urban . . . . . . . . . . . . . . . 26black, urban . . . . . . . . . . . . . . . 35white, rural . . . . . . . . . . . . . . . . 13black, rural . . . . . . . . . . . . . . . . 11
TN: white, urban . . . . . . . . . . . . . . . 40black, urban . . . . . . . . . . . . . . . 67white, rural . . . . . . . . . . . . . . . . 38black, rural . . . . . . . . . . . . . . . . 45
WA: white, urban . . . . . . . . . . . . . . . 42white, rural . . . . . . . . . . . . . . . . 44
Goldenberg (53) . . . . . . . . . . . . . . . . . . 1980 Alabama. . . . . . . . . . . . . . . . . . . . . . . . 56 32Lobb (93) . . . . . . . . . . . . . . . . . . . . . . . . 1980 Mersey, Great Britain . . . . . . . . . . . . 28Information Service Center (72). . . . . 1984 Maryland . . . . . . . . . . . . . . . . . . . . . . . 54 31asee ~~f~renCeS in the back of this case study for full citations
SOURCE Off Ice of Technology Assessment. 1987

52
BARRIERS TO MATERNAL AND NEONATAL TRANSPORT
Level III hospitals may refuse admission for aneonatal transfer for a number of reasons. Thelack of available beds is the reason proffered inmost instances. Although the average occupancynationwide in Level III units is only 73 percent,occupancy in some intensive care nurseries doesconsistently approach 100 percent. (See ch. 2.) Itis also likely that a few hospitals use the excuseof full occupancy to turn away infants whose carewould not be adequately reimbursed. As discussedin chapter 2, neonatal intensive care is one of themost costly services provided by hospitals and en-tails some of the longest lengths of stay. Uninsuredinfants may be deemed undesirable admissions bysome hospitals. Moreover, because Medicaid isoften considered a poor payer which does notfully reimburse a hospital’s costs, even Medicaidcoverage may not ensure entry. (See ch. 4.)
There is no legal requirement that forces hos-pitals to admit every child, regardless of abilityto pay. Depending on when a neonatal intensivecare service was started, the need for such serv-ices may have been analyzed by health plannersunder State certificate-of-need legislation. How-ever, once a certificate-of-need is granted, theState has no ongoing authority over how serv-ices are operated. The Joint Commission on Ac-creditation of Hospitals, which reviews the oper-ations of hospitals and lists staffing, equipmentand procedural guidelines for neonatal intensivecare units, does not address issues of access totreatment (75). Some hospitals are legally requiredto provide a certain amount of charity care to in-digent individuals if they received Federal fundsfor hospital construction and renovation underthe Hill-Burton Act of 1946. Currently, about4,200 hospitals in the United States are still ful-filling their Hill-Burton obligations (182).
Likewise, hospitals are not required to pread-mit high-risk pregnant women for their deliver-ies, even if the hospital serves as the designatedperinatal center for the region. In fact, most hos-pitals have policies requiring advance paymentin full for deliveries if the maternity patients donot have insurance. However, in March 1986 theConsolidated Omnibus Budget Reconciliation Actwas passed, and it prohibits any Medicare-par-
ticipating hospital from refusing to treat or fromtransferring any woman already in labor (50).
The same financial incentives operate for phy-sicians. Obstetricians and pediatricians may beleery of accepting non-paying or partial-pay pa-tients. Survey data show that obstetricians lag be-hind other specialties in the extent to which theyaccept Medicaid patients. The average Medicaidreimbursement rate for obstetrical care is at leastone-third lower than the average private fee, andthe gap between the two amounts is widening overtime (170).
On the other hand, obstetricians with payingmaternity patients may not want to refer high-risk cases to the perinatal center and risk losingtheir fees. Many of the Level III hospitals areuniversity-affiliated with closed medical staffs;non-faculty physicians are not allowed admittingprivileges.
The escalation in recent years of malpracticeactions, especially against obstetricians, has prob-ably had a side effect of improving access toperinatal services for high-risk women. Concernsabout possible malpractice litigation would en-courage community obstetricians to refer high-risk maternity cases to regional centers. Obstetri-cians might particularly employ such “defensivemedicine” tactics for low-income high-risk womenbecause the physicians have poor financial incen-tives to keep their patients.
Finally, the perceptions of physicians about ne-onatal mortality and outcome affect access to ne-onatal intensive care. Several studies show thatphysicians substantially underestimate the poten-tial survival of low birthweight infants (56,185).The obstetrician’s understanding of prognosis inturn influences his or her management of prema-ture labors, such as the decisions to utilize elec-tronic fetal monitoring, to perform cesarean sec-tions for fetal distress, or to transfer mother andbaby prior to delivery to a Level III facility (56).These early management decisions may determinewhether the newborn infant actually survives.
A survey of obstetrical residency programs in1981 found that at less than 28 weeks gestational

53
age there is still considerable variation among hos- deliveries under these conditions. (The averagepitals in how labor and delivery are managed. birthweight for a 27-week infant is between 950Based on the survey, about one-half of univer- and 1000 grams. ) This study points to a lack ofsity training programs consistently performed ce- consensus among obstetricians on how aggres-sarean sections for fetal distress at 27 weeks gesta- sively labor and delivery should be managed be-tional age and one-third of the nonuniversity tween 25 and 28 weeks gestational age (55).residency programs routinely performed cesarean
THE TINIEST BABIES
Once a low birthweight infant is in a Level IIIhospital, through birth or transfer, access to ne-onatal intensive care is almost assured. In prac-tice, the almost universally followed approach inthe NICU today is to initiate aggressive treatmentfor all infants at birth (160,165). Broad latitudehas traditionally been given to doctors and par-ents involved in making the difficult decisionsabout treatment for premature or sick neonates.But in part in reaction to the so-called “Baby Doe”rules, pediatricians, anxious about their legal lia-bility, are increasingly treating virtually all new-borns, including extremely premature infants withvery low birthweights. Although the rules cameabout in response to several “Baby Doe” cases in-volving selective nontreatment for infants withDown’s syndrome, spina bifida cystica, and othercongenital anomalies, the primary controversy inthe medical community revolves around the tiniestinfants who are born at the threshold of viability. s
The Department of Health and Human Serv-ices (DHHS) issued a “Notice to Health CareProviders” in May 1982 informing hospital ad-ministrators that, under Section 504 of the Reha-bilitation Act of 1973, they risked losing Federalfunds if treatment or nourishment was withheldfrom handicapped infants. The so-called “BabyDoe” rules were promulgated in interim regula-tions by DHHS the following March and in finalregulations in January 1984. Facilities were re-quired to post notices in nurseries and provide ac-cess to medical records for Federal investigators.Although the Supreme Court ruled in 1986 thatthe 1973 Rehabilitation Act could not be used to
‘Most experts believe that there is an anatomical threshold of fe-tal development (especially for lung and kidney development) atabout 23 to 24 weeks before which time fetal survival is not possi-ble even with modern techniques (148).
justify the regulations because there was no evi-dence that hospitals denied care to babies solelybecause of handicap, Congress had in the mean-time passed legislation dealing with medical ne-glect in the 1984 amendments to the Child AbusePrevention and Treatment Act (Public Law 98-457) (181). These amendments define medical ne-glect in the treatment of disabled infants as childabuse and give the oversight responsibility for im-plementing the law to the States’ child-abuse agen-cies (164). Both the American Academy of Pedi-atrics, which vehemently opposed the initial BabyDoe regulations, and Right to Life groups, whichsupported them, participated in reaching com-promise language. Regulations implementing thislegislation went into effect in June 1985.
The new regulations permit “reasonable medi-cal judgment” to be used in making decisionsabout the care of disabled newborns and explicitlylists three exceptions when withholding medicaltreatment (other than appropriate nutrition, hy-dration, or medication) is not “medical neglect”(106,164). The exceptions deal with situationswhere treatment would merely prolong dying orwould be “virtually futile” in terms of the survivalof the infant and, under these circumstances, thetreatment itself would be inhumane.
The regulations also encourage hospitals to setup Infant Care Review Committees. A 1985 sur-vey by the American Academy of Pediatrics ofhospitals with NICUs found that nearly 66 per-cent had an ethics body, up from 56 percent theprevious year. However, the survey also foundthat slightly more than half of the committees hadconsidered no cases during the previous year (1).Apparently, Baby Doe cases are relatively rarewith most conflicts resolved by parents and healthprofessionals (181),

54
Although the Baby Doe rules have raised pub-lic debate on the issue, their legal impact on treat-ment decisions for extremely premature infantsis unclear (90). Aside from the limited clout ofthe new regulations (withholding Federal dollarsfrom the State child protection service agency),the language is ambiguous and open to interpre-tation. In the case of extremely low birthweightinfants, “reasonable medical judgment” is dividedon whether it is “virtually futile” to offer treat-ment. The guidelines accompanying the regula-tions admit that “virtually futile” does not meanabsolute certainty and that the prospect of deathneed not be imminent (106). If most physiciansunderstand the law this way, a minimal effect ontreatment decisions might be expected. On theother hand, in today’s malpractice-wary climate,physicians may react by treating aggressively allbut the most clearly hopeless cases so as to avoidany possibility of liability for medical neglect(105).
In practice, physicians often employ guidelinesfor treatment based on their own observations ofprognosis. Under such informal policies, infantswho are born weighing less than 500 grams arenot resuscitated in most hospitals. In some insti-tutions, this boundary on treatment might extend
to babies under 600 grams or even under 750grams, Of course gestational age and the condi-tion of the infant are also taken into considera-tion. Without the application of sophisticated life-extending technologies, like respirators, these in-fants are almost certain to die. Although, as dis-cussed, the Baby Doe regulations do not forceevaluation of such policies, many neonatologistscite the Federal rule as a primary reason for theaggressive treatment of smaller and smaller ne-onates. At least one published report blames theintrusion of the Baby Doe regulations into theNICU for the unnecessary and costly treatmentof conjoined twins when there was no hope forsurvival (150).
Practicing defensive medicine is a negative in-centive for most physicians, and it should benoted that the same neonatologists who mentionlegal considerations also point to the now manypublicized successes with extremely tiny babies.The normal outcome for some of these infants en-courages imitation. More importantly, it is im-possible during the first weeks of life, even withtoday’s most sophisticated technology like ultra-sound brain scans, to predict accurately an infant’seventual outcome (21,163).

Chapter 6
Economic Analysis ofNeonatal Intensive Care

Chapter 6
Economic Analysis ofNeonatal Intensive Care
INTRODUCTION
This case study has shown that neonatal inten-sive care is a high-cost technology that demon-strably saves the lives of low birthweight babies.But the long-term consequences of providing in-tensive care are more difficult to evaluate. Overthe lifetimes of the infants treated in neonatal in-tensive care units (NICUs), are medical care costsincreased or reduced? Likewise, what are the ef-fects on the pain and suffering of patients and theirfamilies? Is it possible that some severe handicapsin children are considered by families to be worsethan death?
Cost-effectiveness analysis (CEA) can provideinsight to these issues by comparing the costs, ben-efits, and quality of life implications of neonatalintensive care in a single economic evaluation.Ideally, CEA compares the costs and the healtheffects of alternative strategies, such as the pro-vision of neonatal intensive care with another kindof intervention for low birthweight babies. Theexpected changes in health effects are arrayedagainst the net medical care costs incurred by pro-viding each alternative approach to neonatal care.
Unlike CEA, cost-benefit analysis attempts toplace dollar values on all consequences, both posi-tive (benefits) and negative (costs), arising fromalternative courses of action. The alternative with
the highest level of monetary net benefit (or lowestnet cost) is preferred to others. If the net benefitis greater than zero, the alternative is “cost sav-ing” and considered worthwhile on efficiencygrounds alone. Because it is so difficult to placea value on the benefits of a strategy, cost-benefitanalysis often proves inadequate. Some research-ers have calculated the lifetime economic produc-tivity of survivors, but this is certainly an incom-plete surrogate for the benefits of a life-savingintervention. How can a value be placed on thepain, suffering, anxiety, emotional distress, orgrief in patients and their families, especially whenthese consequences occur at different times in thefuture? These psychosocial benefits (or losses)defy measurement (179).
Cost-effectiveness analysis escapes the problemof trying to value benefits by using the effective-ness measure (e.g., quality-adjusted life years) asa proxy. Net costs per unit of health effectivenessare calculated and compared with other programswith similar health goals. The interpretation ofresults from cost-effectiveness analyses remainsproblematic, however, because methodologicaldifferences in study design make it difficult todirectly compare one CEA evaluation to another.
COST= EFFECTIVENESS AND COST-BENEFIT STUDIES
The earlier OTA study on neonatal intensivecare by Budetti and his colleagues concluded thatneonatal intensive care for infants weighing 1500grams or less was marginally cost saving whenthe value of the lifetime economic productivityof survivors was estimated. Treatment of the sub-group weighing under 1000 grams cost more innet medical costs than was saved in productivityif outcomes from 1971 to 1975 were used. When
mortality and morbidity rates from later in the1970s were used in the calculation, however, treat-ment of the extremely low birthweight infants alsobecame cost saving. The benefits accruing fromthe lifetime earnings of the increased number ofnormal survivors outweighed the costs incurredby the increase in the absolute number of severelyhandicapped (25).
57

58
Budetti and his colleagues compared the costsof neonatal intensive care with less intensive careof ill newborns. Using mortality and morbidityrates gleaned from the literature, they relied ona cost-benefit economic model that assigned dol-lar values based on the assumptions that normalsurvivors are economically productive; nonsur-vivors are relatively inexpensive; and seriouslydefective survivors are both expensive and notproductive. These hypothetical scenarios may nothave adequately mirrored the true life experienceof NICU survivors. In addition, their analysis didnot take into account the psychosocial costs andbenefits of neonatal intensive care that were dis-cussed previously.
The most comprehensive economic evaluationconducted to date was undertaken by a group ofCanadian researchers (19). They studied the mor-tality and morbidity of all very low weight in-fants born to the residents of a southern Ontariocounty before (1964 to 1969) and after (1973 to1977) the introduction of neonatal intensive care.The assessment of survivors’ health included aclassification of health states that measured phys-ical, social, role, and emotional function as wellas health problems. To take into account thesepsychosocial costs, a sample of parents was thensurveyed on the desirability or undesirability ofthe health states relative to one another. For ex-ample, parents rated some chronic dysfunctionalstates as worse than death. The survey resultswere then used to weight life-years for quality.These quality-adjusted life-years (QALYs) werethe measure used to adjust additional years of life(decreasing mortality) for the long-term disabili-ties that some survivors have as they live out theirlife expectancies.
Health outcomes were calculated for two birth-weight groups: infants weighing 1000 to 1499grams and infants weighing 500 to 999 grams. Likemany other studies, the Canadian group foundthat the rate of survival to hospital discharge in-creased with neonatal intensive care. And, whilethe introduction of neonatal intensive care alsoresulted in increases in quality-adjusted life-yearsfor the very low birthweight infants as a whole,for the subgroup of infants weighing less than1000 grams, the increase in quality-adjusted life-years was lower than the increase in unadjusted
additional life-years, implying a poor quality oflife for many of these tiniest surviving infants. Infact, although the proportion of serious handicapsamong survivors did not increase significantly,the increased absolute number of survivors re-sulted in a greater number of handicapped chil-dren (70).
Costs were estimated for all neonatal care andfor lifetime followup health care and other spe-cial services, such as institutional care or specialeducation. The results of the economic evaluationperformed by the Canadian group are shown intable 16. For the group weighing 1000 to 1499grams at birth, the incremental cost of neonatalintensive care was $82,969 per survivor at hospi-tal discharge. Similarly, for the 500- to 999-grambirthweight group, the neonatal intensive careprogram cost $142,929 per survivor.
By every economic measure, neonatal intensivecare for infants weighing 1000 to 1499 grams wasmore cost-effective than neonatal intensive carefor infants weighing under 1000 grams. Projectedover a lifetime,1 the neonatal intensive care pro-
I Neonatal intensive care requires the early expenditure of largesums of money to achieve later gains. Therefore, a discount rateof 5 percent was applied to costs, earnings, and effects (QALYs)occurring in the future in order to convert future values to theirequivalent present value.
Table 16.– Measures of Economic Evaluation ofNeonatal Intensive Care for Very Low Birthweight
Infants (5 Percent Discount Rate), 1984a
Birthweight (grams)
Period 1000-1499 500-999
To hospi ta l d ischarge: b
Cost/addi t ional surv ivor . . . . $82,969 $142,929To age 15 (projected):
Cost/life-year gained . . . . . . 8,506 17,012Cost/QALY gainedc. . . . . . . . 10,737 55,917
To death (projected):Cost/life-year gained . . . . . . 4,044 12,968Cost/QALY gainedc. . . . . . . . 4,462 31,235Net economic benefit
(Ioss)/live birth . . . . . . . . . . (3,626) (22,450)
Net economic cost/QALYgained c . . . . . . . . . . . . . . . . . . 1,394 24,403
avalues were converted to 19& U.S. dollars from 1978 Canadian dollars.bAll costs and effects occurred in Year one.CQALY denotes quality-adjusted life-years.
SOURCE: M.H. Boyle, G.W. Torrance, J.C. Sinclair, et al., “Economic Evaluationof Neonatal Intensive Care of Very -Low-Birlh-Weight Infants, ” N. Eng.J, Med. 308(22):1330-1337, June 2, 1983.

59
gram cost $4,462 per quality-adjusted life-yeargained for the 1000- to 1499-gram birthweightgroup and $31,235 per quality-adjusted life-yeargained for the under 1000-gram group. Borrow-ing from cost-benefit analysis, the researchers alsocalculated net economic benefit (or loss) by tak-ing into account the anticipated future earningsof survivors. In this analysis, there was a net eco-nomic loss in employing neonatal intensive careover nonintensive care for both weight groups.However, for infants weighing 1000 to 1499 grams
the increased costs of treatment were very nearlyoffset by increased lifetime earnings. When thediscount rate was set lower than 3½ percent, thenet economic benefit per live birth was positive.Not so for the birthweight group weighing under1000 grams. Gains in survival and quality-adjustedlife-years were obtained at a considerable increasein neonatal costs and subsequent health care costs.These costs could not be repaid through lifetimeearnings.
CONCLUSIONS AND POLICY IMPLICATIONS
The results of the Canadian study raise a num-ber of issues. One is whether the same conclusionswould be reached if the study were conductedtoday. For the time period studied, the mortal-ity, morbidity, and cost figures used by the Cana-dian group did not differ markedly from otherpopulation-based and institutional reports for thesame birthweight groups. However, since 1977there have been both substantial gains in survivaland increases in costs. During the period studiedby the Canadians, the risk of mortality declinedmore rapidly for the 1000- to 1500-gram birth-weight group than for smaller babies. Since then,the most rapid reduction in mortality risk has beenfor the 750- to 1000-gram birthweight group. (Seech. 3.) Better rates of survival would tend to im-prove the cost-effectiveness of neonatal intensivecare, and this impact would be greater for the un-der 1000-gram birthweight group.
OTA calculated the incremental cost of neona-tal intensive care in producing a survivor by usingthe recent data on mortality and hospital coststhat are developed in this case study (table 17).Baseline survival rates, prior to the introductionof neonatal intensive care, were taken for theyears 1961 to 1965 and compared with the mostrecent, available survivor rates, those for 1981 to1985. OTA’s results are remarkably similar tothose found in the Canadian study. (Both tables16 and 17 are in 1984 U.S. dollars. ) Comparedwith the Canadian costs, OTA found the cost peradditional survivor to be about $3,000 more ex-pensive for infants with birthweights between1000 and 1500 grams and about $24,500 less ex-
pensive for infants with birthweights under 1000grams. The impact of improved survival rates forextremely low birthweight infants was very strong,because the average hospital costs in the Cana-dian study for the under 1000-gram birthweightgroup were less than one-half the average costsused in the OTA calculation. If only mortality istaken into account, the cost-effectiveness of ne-onatal intensive care relative to no special carefor the smallest babies (those under 1000 grams)has improved since 1977.
Limitations of data prevented OTA from exam-ining the implications of long-term morbidity oncosts in a separate cost-effectiveness analysis. Theproportion of NICU survivors with serious han-dicaps has remained stable since the Canadianstudy, but the rate of severe disability increaseswith decreasing birthweight. (See ch. 3.) The re-cent declines in mortality mean that, especiallyamong the under 1000-gram birthweight group,
Table 17.—Cost of Neonatal Intensive CarePer Additional Survivor, 1984
Birthweight (grams)
1000-1499 500-999
Average hospital costa. . . . . . . $36,153 $ 49,617
Additional survivors per 1,000live births from 1960to 1980b . . . . . . . . . . . . . . . . . . 419 419
Cost per additional survivor . . $86,284 $118,418aFrom table 4, mean of the average hospital costs per Infant reported by the three
groups of hospitals.bF rom table g, change in inborn neonatal mortality rates per 1.~ Ilve births from
1961-65 to 1981-85.
SOURCE: Office of Technology Assessment, 1987

60
there are now both more normal survivors andmore handicap victims, (See figures 2 and 3 in ch.3.) It is unclear how the new mix of survivorswould affect the economic equation.
Costs have increased since 1978, and these in-creases have outpaced inflation by more than 75percent in the United States. Infants treated in ne-onatal intensive care use resources more inten-sively than previously, and resource use is in-versely correlated with birthweight. (See ch. 2.)These increases in medical care costs, though theycontribute to improved health outcomes, wouldtend to decrease the cost-effectiveness of neona-tal intensive care. Moreover, the lifetime costs forcustodial care for a severely disabled person haverisen too. A recent estimate of the cost for caringfor a severely handicapped child (in 1982 dollars)is $22,590 per year (170).
In all likelihood the conclusions of the Cana-dian study would still pertain today. Neonatal in-tensive care results in both increased survival andincreased costs, Moreover, neonatal intensive carebecomes more expensive as it is employed in in-creasingly marginal cases.
One way to increase the cost-effectiveness ofneonatal intensive care is to try to identify whichnewborns are most likely to survive, and, in par-ticular, experience higher quality lives (14). Forexample, because birthweight is such a powerfulpredictor of both survival and morbidity, analy-sis of birthweight groups by 100 gram incrementscan lead to refinements in the conclusions of theCanadian group. Researchers in Rhode Island ana-lyzed lifetime costs for infants weighing 500 to1000 grams and born between 1977 and 1981(180). Taking into consideration long-term ther-apeutic and custodial care for handicapped chil-dren as well as initial hospitalizations, they esti-mated costs in 1982 dollars ranging from $362,992
per survivor for infants with birthweights between600 and 699 grams to $40,647 per survivor forthose weighing 900 to 999 grams. Their cost-benefit analysis showed that when estimates oflifetime earnings were added to the equation, onlyinfants with birthweights from 900 to 999 gramshad future earnings that exceeded total costs.
Such analyses help to refine the economic equa-tions, but the question should not be whether todeny care to any particular infant on the basis ofhigh costs. It is expected that a successful inter-vention like neonatal intensive care will add tooverall medical costs. Moreover, there are manyethical, social, and legal reasons why intensivecare should not be withheld from a newborn, nomatter what its size and gestational age. (See ch.5.) Most importantly, neonatologists are unani-mous in stating that it is impossible to predict out-come at birth. Many healthy babies would be lostif blanket policies of withholding care were promul-gated. Doctors, in conjunction with parents, havetraditionally grappled with decisions about indi-vidual patients and they must continue to do so.Data on cost-effectiveness can be one componentof what are, ultimately, value judgments.
Policymakers can more directly use the resultsof cost-effectiveness analyses to guide prioritiesin expenditures for health care. For example, itis not clear that society is spending more perquality-adjusted life-year for neonatal intensivecare than for other programs such as dialysis, kid-ney transplantation, coronary artery bypass sur-gery, or bone-marrow transplantion (14,186). Insuch a comparative context, neonatal intensivecare can be judged to be more or less worth itscosts. Better cost-effectiveness information aboutdiverse programs can help both policymakers andphysicians make consistent and well-foundedchoices.

Appendixes

Appendix A
Glossary of Acronyms and Terms
List of Acronyms
AHA —American Hospital AssociationBPD —bronchopulmonary dysplasiaBC/BS —Blue Cross/Blue ShieldCEA —cost-effectiveness analysisCPAP —continuous positive airway pressureDRGs —diagnosis-related groupsECMO —extracorporeal membrane oxygenationHFV —high-frequency ventilationHMO —health maintenance organizationIVH —intraventricular hemorrhageMDC —major diagnostic categoryNACHRI—National Association of Children’s
Hospitals and Related InstitutionsNICU —neonatal intensive care unitNIH –National Institutes of HealthOTA –Office of Technology Assessment (U.S.
Congress)PEEP —positive end expiatory pressureP r o —preferred provider organizationQALY —quality-adjusted life-yearRDS —respiratory distress syndromeROP —retinopathy of prematuritySIDS —sudden infant death syndrome
Glossary of Terms
Antenatal transfer: The transport of pregnant womento the appropriate level of care prior to delivery.
Assisted ventilation: Mechanical assistance in perform-ing or controlling the breathing function.
Baby Doe rules: Federal regulations issued from 1982to 1984 under Section 504 of the Rehabilitation Actof 1973 that prohibited hospitals from withholdingnourishment or care from handicapped infants. TheSupreme Court ruled in 1986 that the 1973 act couldnot be used to justify the regulations. MeanwhileCongress passed the 1984 amendments to the ChildAbuse Prevention and Treatment Act that permitted“reasonable medical judgement” to be used in mak-ing decisions about treatment for disabled new-borns.
Birthweight: Weight of an infant at the time of deliv-ery. Birthweight can be recorded in either pounds/ounces or grams.
Birthweight-specific mortality rate: Deaths in a birth-weight category per 1000 live births in the samebirthweight category.
Bronchopulmonary dysplasia: A chronic lung diseasein newborns, often defined by a characteristicappearance of the lungs on X-ray and the use ofassisted ventilation for more than 4 weeks.
Case mix: A measure of the mix of cases being treatedby a particular health care provider that is intendedto reflect the patients’ different needs for resources.
Cerebral palsy: A paralysis of varying severity thatresults from nonprogressive damage to the brain ator around birth.
Congenital anomalies: Birth defects that result fromimperfect development during pregnancy.
Continuous positive airway pressure (CPAP): A res-piratory therapy technique that prevents alveolarcollapse by keeping up positive pressure on the lungsbetween breaths.
Cost-benefit analysis: An analytical technique thatcompares the costs of a technological application tothe resultant benefits, with both costs and benefitsexpressed by the same measure. This measure isnearly always monetary.
Cost-effectiveness analysis (CEA): An analytical tech-nique that compares the costs of a technology or ofalternative technologies to the resultant benefits,with cost and benefits/effectiveness not expressedby the same measure.
Cost saving: An economic concept referring to the re-sults of cost-benefit analysis when the net benefitis greater than zero.
Diagnosis-related groups (DRGs): A patient classifi-cation scheme based on the principal diagnosis, sec-ondary diagnoses, surgical procedures, age, and dis-charge status of the patients treated in hospitals.
Extremely low birthweight: Birthweight of less than1000 grams (2 lb 2 OZ).
Gestational age: The number of completed weekselapsed between the first day of the last normal men-strual period and the date of delivery.
Handicap rate: See serious handicap and moderatehandicap.
Health maintenance organization (HMO): A healthcare organization that, in return for prospective percapita payments, acts as both insurer and providerof comprehensive but specified medical services.
Hydrocephalus: The distension of the head caused bythe excessive buildup of cerebral spinal fluid.
Infant mortality: Death in the first year of life. It in-cludes neonatal mortality and postneonatal mor-tality.
Intracranial hemorrhage: Bleeding in the brain.
63

64
Intraventricular hemorrhage: Bleeding into the cere-bral ventricles, small cavities within the brain thatsecrete and convey cerebrospinal fluid.
Level I hospitals or facilities: Hospitals that provideonly normal newborn care under the regional sys-tem for perinatal services.
Level II hospitals or facilities: Hospitals in the regionalsystem for perinatal services that provide special-ized neonatal care but lack some components andexpertise found in Level III facilities.
Level III hospitals or facilities: Hospitals in the regionalsystem for perinatal services that provide the mostsophisticated neonatal intensive care.
Low birthweight: Birthweight of less than 2500 grams(5 lb 5 OZ).
Major diagnostic category (MDC): The 23 principaldivisions in the DRG patient classification scheme.The diagnoses in each MDC correspond to a singleorgan system or etiology and in general are associ-ated with a particular medical specialty.
Mechanical ventilation: See assisted ventilation.Medicaid: A federally aided, State-administered pro-
gram of medical assistance for low-income peoplemeeting categorical requirements.
Moderate handicap: Disabilities that include moder-ate mental retardation (IQ or developmental quo-tient between 70 and 80).
Morbidity: The condition of being diseased ordisabled.
Neonatal intensive care: The constant and continuouscare of the critically ill newborn.
Neonatal intensive care unit (NICU): A specializedhospital unit combining high technology and highlytrained staff that treats seriously ill newborns,
Neonatal mortality: Death in the first 28 days of life.Neonatal mortality rate: Deaths during the first 28
days of life per 1000 live births.Neonate: A newborn infant less than a month old.Neonatologist: A pediatrician specializing in newborn
care.Neurodevelopmental outcome: A measure of neuro-
logical and developmental status.Outliers: Hospital cases with statistically unusual
lengths of stay under the DRG patient classificationscheme.
Perinatal care: Medical care pertaining to or occurringin the period shortly before and after birth, vari-ously defined as beginning with the completion ofthe 20th to 28th week of gestation and ending 7 to28 days after birth.
Postneonatal mortality: Death between the first 28days and the end of the first year of life.
Postneonatal mortality rate: Postneonatal deaths (28days to under 1 year) per 1,000 neonatal survivors.
Preferred provider organization (PPO): A form ofhealth care delivery system in which an agreementis made between providers and purchasers that pa-tients who seek medical care from the “preferredproviders” will obtain benefits such as reduced costsharing. In return for the potential increase in vol-ume of patients, the preferred providers may agreeto discount their charges, to accept capitated pay-ments, or to submit to enhanced utilization review.
Preterm infant: A newborn whose gestational age isless than 37 completed weeks.
Prospective payment: Payment for medical care on thebasis of rates set in advance of the time period inwhich they apply. The unit of payment may varyfrom individual medical services to broader catego-ries, such as hospital case, episode of illness, or per-son (cavitation).
Pulmonary surfactant: A substance in the lung thatreduces the surface tension along the alveoli and pre-vents the collapse of the pulmonary air spaces.
Quality-adjusted life-year (QALY): An economicmeasure used in cost-effectiveness analysis to expressbenefits/effectiveness.
Regionalization: The organization and coordinationof perinatal services, including a three-tiered systemof hospital care, by geographic region.
Respiratory distress syndrome (RDS): An acute res-piratory disorder which, in premature infants, isthought to be caused by a deficiency of pulmonarysurfactant. When RDS is in severe form, patientsoften need mechanical assistance to breathe.
Retinopathy of prematurity (ROP): A retinal diseaseafflicting premature infants that can lead to retinalscarring, retinal detachment, and blindness,
Serious handicap: Disabilities that include severe men-tal retardation (IQ or developmental quotient be-low 70), cerebral palsy of significant degree, majorseizure disorders, or blindness.
Steroid treatment: A drug regimen administered topregnant women in preterm labor in order to accel-erate fetal lung maturation.
Surfactant: See pulmonary surfactant.Very low birthweight: Birthweight of less than 1500
grams (3 lb 3 oz).

Appendix B
Acknowledgments
The development of this case study was greatly aided by the advice and thoughtful review of a numberof people. Several individuals contributed unpublished data which permitted the calculation of recent estimateson the costs and effectiveness of neonatal intensive care. The author and other OTA staff would like to thankthe following people:
Mary Ellen AveryThe Children’s HospitalBoston, MA
Michael BoyleMcMaster UniversityHamilton, Ontario
Philip DavidsonUniversity of Rochester Medical CenterRochester, NY
John M. Driscoll, Jr.Columbia-Presbyterian Medical CenterNew York, NY
Marvin FeuerbergOffice of Technology AssessmentWashington, DC
Susan GoldbeckerThe Children’s Hospital at Albany Medical CenterAlbany, NY
Patty GoldbergInformation Service CenterBaltimore, MD
Maureen HackRainbow Babies and Children’s HospitalCleveland, OH
Elicia HerzOffice of Technology AssessmentWashington, DC
Jeffrey HorbarThe University of Vermont, College of MedicineBurlington, VT
L. Stanley JamesColumbia-Presbyterian Medical CenterNew York, NY
John KielySergievsky CenterColumbia UniversityNew York, NY
Howard KilbrideChildren’s Mercy HospitalKansas City, MO
Sharon KovzeloveChildren’s Hospital National Medical CenterWashington, DC
Ernest KraybillUniversity of North Carolina Medical SchoolChapel Hill, NC
Burton KushnerUniversity of Wisconsin Medical SchoolMadison, WI
John MuldoonNational Association of Children’s Hospitals and
Related InstitutionsAlexandria, VA
Karen E, PapeThe Hospital for Sick ChildrenToronto, Ontario
Ciaran S. PhibbsInstitute of Health Policy StudiesSan Francisco, CA
Elaine PowerOffice of Technology AssessmentWashington, DC
Richard SchreinerIndiana University School of MedicineIndianapolis, IN
Rachel SchwartzNational Perinatal Information CenterProvidence, RI
Donald ShapiroUniversity of Rochester Medical SchoolRochester, NY
Ann StewartUniversity College LondonLondon, Great Britain
George TorranceMcMaster UniversityHamilton, Ontario
65

References

References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
American Academy of Pediatrics, “Follow-upSurvey on IBRCS,” unpublished mimeo, ElkGrove Village, IL, June 1985.American Academy of Pediatrics, Committee onFetus and Newborn, Standards artd Recomrnen-dations for Hospital Care of IVewborn Infants,1974-1977, 6th ed. (Evanston, IL: AAP, 1977).American Academy of Pediatrics, Committee onFetus and Newborn, “Level II Neonatal Units, ”Pediatrics 66(5):810-811, 1980.American Academy of Pediatrics and AmericanCollege of Obstetricians and Gynecologists,Guidelines for Perinatal Care (Evanston, IL:AAP and ACOG, 1983).American Hospital Association, Hospital Statis-tics, 1984 Edition (Chicago, IL: AHA, 1984).Avery, M. E., Boston Children’s Hospital, Bos-ton, MA, unpublished data, July 1986.Avery, M. E., “Antepartum Glucocorticoids andPrevention of Respiratory Distress Syndrome, ”paper presented at the XVIII International Con-gress of Pediatrics, Honolulu, HI, July 7, 1986.Avery, M. E., Boston Children’s Hospital, Bos-ton, MA, personal communication, July 23,1986.Avery, M. E., Taeusch, H. W., and Floros, J.,“Surf actant Replacement,” IV. Eng. ]. Med.315(13):825-826, Sept. 25, 1986.Avery, M. E., Tooley, W. H., Keller, J. B., et al,,“Is Chronic Lung Disease in Low Birth WeightInfants Preventable? A Survey of Eight Centers, ”Pediatrics 79(1):26-30, January 1987.Barson, A. J., Tasker, M., Lieberman, B. A., etal., “Impact of Improved Perinatal Care on theCauses of Death,” Arch. Dis. Child. 59:199-207,1984.Bazzoli, G. J., “Health Care for the Indigent:Overview of Critical Issues, ” Health Services Re-search 21(3):353-392, August 1986.Bennett, F. C., Robinson, N. M., and Sells, C. J,,“Growth and Development of Infants WeighingLess Than 800 Grams at Birth, ” Pediatrics71(3):319-323, 1983.Bennett, K. J., Feeny, D., Guyatt, G. H., et al.,“Guidelines for Health Technology Assessment:The Efficacy, Effectiveness, and Efficiency of Ne-onatal Intensive Care, ” hzternat. J. of Tech. As-sess. in Filth. Care 1:873-892, 1985.Berenson, R. A., Intensive Care Units (ICUS);Clinical Outcomes, Costs, and Decisionmaking(Health Technology Case Study #28), preparedfor the Office of Technology Assessment, U.S.Congress, OTA-HCS-28 (Washington, DC: U.S.Government Printing Office, November 1984).
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Berki, S. E,, and Schneier, N. B., “Frequency andCost of Diagnosis-Related Group OutliersAmong Newborns, ” Pediatrics 79(6):874-881,June 1987.Beverley, D., Foote, K., Howel, D., et al., “Ef-fect of Birthplace on Infants With Low BirthWeight,” Br. Med. J. 293:981-983, 1986.Boyle, M. H., McMaster University, Hamilton,Ontario, personal communication, June 5, 1987.Boyle, M. H., Torrance, G. W., Sinclair, J. C., etal., “Economic Evaluation of Neonatal IntensiveCare of Very-Low-Birth-Weight Infants, ” IV.Eng. J. Med. 308(22):1330-1337, 1983.Boynton, B. R., “High Frequency Ventilation inNewborn Infants,” Respiratory Care 31(6):480-487, June 1986.Bozynski, M. E. A., Nelson, M. N., Matalon,T. A. S., et al., “Prolonged Mechanical Ventila-tion and Intracranial Hemorrhage: Impact onDevelopmental Progress Through 18 Months inInfants Weighing 1,200 Grams or Less at Birth, ”Pediatrics 79(5):670-676, May 1987.Brans, Y. W., Escobedo, M. B., Hayashi, R. H.,et al., “Perinatal Mortality in a Large PerinatalCenter: Five-Year Review of 31,000 Births, ” Am.J. Ob. Gyn. 148:284-289, 1984.Britton, S., Fitzhardinge, P., and Ashby, S., “IsIntensive Care Justified for Infants Weighing LessThan 801 Gm at Birth?” J. Pediatrics 99:937-942,1981,Buckwald, S., Zorn, W. A., and Egan, E. A.,“Mortality and Follow-Up Data for NeonatesWeighing 500 to 800 G at Birth,” AJDC 138:779-782, 1984.Budetti, P., McManus, P., Barrand, N., et al.,The Costs and Effectiveness of Neonatal Inten-sive Care (Health Technology Case Study #lO),prepared for the Office of Technology Assess-ment, U.S. Congress, PB 82-101411 (Springfield,VA: National Technical Information Service,August 1981).Buehler, J. W., Hogue, C. R. J., and Zaro, S. M.,“Postponing or Preventing Deaths? Trends in In-fant Survival, Georgia 1974 Through 1981,”JAMA 253(24):3564-3567, 1985.Buehler, J. W., Kleinman, J. C., Hogue, C. J. R.,et al., “Birth Weight-Specific Infant Mortality,United States, 1960 and 1980, ” Public HealthReports 102(2):151-161, 1987.Cane, R. D., and Shapiro, B. A., “MechanicalVentilator Support, ’’JAMA 254(1):87-92, July5, 1985.Capeless, E. L., and Mead, P. B., “Managementof Preterm Premature Rupture of Membranes;
69

70
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Lack of a National Consensus,” Am. J. 06. Gyn.157(1):11-12, July 1987.Catto-Smith, A. G., Yu, V. Y. H., Bajuk, B., etal., “Effect of Neonatal Periventricular Hemorr-hage on Neurodevelopmental Outcome, ” Arch.Dis. Child. 60:8-11, 1985.Clark, C. E., Clyman, R. I., Roth, R. S., et al.,“Risk Factor Analysis of Intraventricular Hemor-rhage in Low-Birth Weight Infants, ” J. Pediat~”cs99:625-628, 1981.Cohen, R. S., Stevenson, D. K., Ariagno, R. L.,et al., “Survival and Morbidity of Small Babies:Is There a Limit to Neonatal Care?” Pediatrics73:415-416, 1984.Cohen, R. S., Stevenson, D, K., Malachowski,N., et al., “Favorable Results of Neonatal Inten-sive Care for Very Low-Birth-Weight Infants, ”Pediatrics 69(5):621-625, 1982.Committee on Perinatal Health, Toward Im-proving the Outcome of Pregnancy (WhitePlains, NY: The National Foundation—Marchof Dimes, 1977).Cordero, L., Backes, C. R., and Zuspan, F. P.,“Very Low-Birth Weight Infant, I: Influence ofPlace of Birth on Survival,” Am. J. Ob. Gyn.143:533-537, 1982.Crombie, S. V., and Darlow, B. A., “Neurodevel-opmental Outcome for Infants of Very LowBirthweight Admitted to a Regional NeonatalUnit, 1979-1983,” N. Zealand Med. J. 99(799):223-226, April 1986.Cross, K. W., “Cost of Preventing RetrolentalFibroplasia, ” The Lancet ii:954-956, 1973.Davidson, P. W., Quinn, E., and Shapiro, D. L.,Rochester Regional Perinatal Center, Rochester,NY, unpublished data, May 21, 1987.Davidson, S. M., Simon, M. B., and Connelly,J. P., “Interstate Variation in Medicaid Coverageof Newborns: Report of Phase I,” prepared forthe American Academy of Pediatrics, Evanston,IL, May 1982.de Lissovoy, G., Rice, T., Gabel, J., et al., “Pre-ferred Provider Organizations One Year Later,”Inquiry 24:127-135, summer 1987.Dillon, W. P., and Egan, E. A., “Aggressive Ob-stetric Management in Late Second-TrimesterDeliveries,” Ob. Gyn. 58:685-690, 1981.Dolfin, T., Skidmore, M. B., Fong, K., et al., “In-cidence, Severity, and Timing of Subependymaland Intraventricular Hemorrhages in Preterm In-fants Born in a Perinatal Unit as Detected bySerial Real-Time Ultrasound, ” Pediatrics 71:541-546, 1983.
43.
44.
45.
46.
47.
48.
49.
50,
51.
52.
53.
54.
55.
Doran, T. A., Surfer, P., MacMurray, B., et al.,“Results of a Double-Blind Controlled Study onthe Use of Betamethasone in the Prevention ofRespiratory Distress Syndrome, ” Am. J. Ob.Gyn. 136:313-320, 1980.Doyle, L. W., Kitchen, W. H., Ford, G. W., et al.,“Effects of Antenatal Steroid Therapy on Mor-tality in Very Low Birth Weight Infants, ”J. Pedi-atrics 108:28 ?-292, 1986.Drillien, C. M., “The Incidence of Mental andPhysical Handicaps in School-Age Children ofVery Low Birthweight, ” Pediatrics 27:452-464,1961.Driscoll, J. M., Columbia-Presbyterian MedicalCenter, New York, NY, unpublished data,March 1987.Driscoll, J. M., Columbia-Presbyterian MedicalCenter, New York, NY, personal communica-tion, June 4, 1987.Driscoll, J.M, Driscoll, Y. T., Steir, M. E., et al.,“Mortality and Morbidity in Infants Less Than1,001 Grams Birth Weight,” Pediatrics 69(1):21-26, 1982.Freeman, J. M., and Shinnar, S., “Intraventricu-Iar Hemorrhage in the Premature Infant, ” letterto the editor, N. Eng. J. Med. 307(20):1274, Nov.11, 1982.Friedman, E., “Medicaid: Trying To Right aSometimes Rocky Ship,” Hospitals 60(20):50,oct. 20, 1986.Gitlin, J. D., Sol], R. F., Parad, R. B., et al., ”ARandomized Controlled Trial of Exogenous Sur-factant for the Treatment of Hyaline MembraneDisease,” Pediatric Research 20:429A, 1986.Goldberg, R. N., and Bancalari, E., “Bronchopul-monary Dysplasia: Clinical Presentation and theRole of Mechanical Ventilation, ” RespiratoryCare 31(7):591-596, 1986.Goldenberg, R. L., Hanson, S., Wayne, J. B., etal., “Vital Statistics Data as a Measurement ofPerinatal Regionalization in Alabama, 1970 to1980,” Southern Med. J. 78(6):657-660, June1985.Goldenberg, R. L., Humphrey, J. L., Hale, C. B.,et al,, “Neonatal Deaths in Alabama, 11: Policyand Research Implications Derived From a Com-parison of Birth Weight-Specific State and Med-ical Center Neonatal Mortality Rates, ” Am. J.Ob. Gyn. 146:450-455, 1983.Goldenberg, R. L., Nelson, K. G., Burton, M., etal., “Gestational Age and the Management ofPreterm Labor in Obstetric Programs, ” Am. J.Perinato]ogy 2(1):25-29, January 1985.

71
56,
57,
58.
59.
60,
61.
62.
63.
64.
65.
66.
67.
68.
Goldenberg, R. L., Nelson, K. G., Dyer, R. L., etal., “The Variability of Viability: The Effect ofPhysicians’ Perceptions of Viability on the Sur-vival of Very-Low-Birth Weight Infants, ” Am.J. Ob. Gyn. 143(6):678-684, 1982.Goldenberg, R. L., Nelson, K. G., Koski, J. F., etal., “Neonatal Mortality in Infants Born Weigh-ing 501 to 1000 Grams: The Influence of Changesin Birth Weight Distribution and Birth Weight-Specific Mortality Rates on Neonatal Survival,”Am. J. Ob. Gyn. 151:608-611, 1985.Gortmaker, S. L., Clark, C. J. G., Graven, S. N.,et al., “Reducing Infant Mortality in Rural Amer-ica: Evaluation of the Rural Infant Care Pro-gram, ” Fl]th. Services Research 22(1):91-116,April 1987.Gortmaker, S., Sobol, A., Clark, C., et al., “TheSurvival of Very Low Birth-Weight Infants byLevel of Hospital of Birth: A Population Studyof Perinatal Systems in Four States, ” Am. J. Ob.Gyn. 152:517-524, 1985.Hack, M., Rainbow Babies and Children’s Hos-pital, Cleveland, OH, personal communication,Mar. 10, 1987.Hack, M., and Fanaroff, A. A., “Changes in theDelivery Room Care of the Extremely Small In-fant ( <750 G)–Effects on Morbidity and Out-come, ” N. Eng. J. Med. 314(10):660-664, 1986.Hack, M., Fanaroff, A. A., and Merkatz, I. R.,“Current Concepts: The Low-Birth Weight In-fant—Evolution of a Changing Outlook, ” N.Eng. J. Med. 301:1162-1166, 1979.Halliday, H. L., McClure, G., Reid, M. McC.,et al., ’’Controlled Trial of Artificial SurfactantTo Prevent Respiratory Distress Syndrome,” TheLancet i:476-478, 1984.Harris, B. A., Wirtschafter, D, D., Huddleston,J. F., et al., “In Utero Versus Neonatal Transpor-tation of High-Risk Perinates: A Comparison, ”Ob. Gyn. 57(4):496-499, 1981.Health & Hospitals Corp., Office of Health CareStandards and Evaluation, “Report on NeonatalSpecial Care Services in New York City,” unpub-lished mimeo, New York, NY, February 1982.Hein, H. A,, “Evaluation of a Rural PerinatalCare System, ” Pediatrics 66:540-546, 1980,Hein, H. A., “The Status and Future of SmallMaternity Services in Iowa, ” JAMA 255(14):1899-1903, Apr. 11, 1986.Hirata, T,, Epcar, J. T., Walsh, A,, et al., “Sur-vival and Outcome of Infants 501 to 750 Gm:A Six-Year Experience,” J. Pediatrics 102(5):741-748, 1983.
69.
70,
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
Horbar, J. D., “A Multicenter Survey of 28 DaySurvival and Supplemental Oxygen Administra-tion in Infants 701-1500 Grams, ” paper presentedat the Ross Laboratories Special Conference onTopics in Neonatology, Washingon, DC, Dec.7-9, 1986.Horwood, S. P., Boyle, M. H., Torrance, G. W.,et al., “Mortality and Morbidity of 500- to 1,499-Gram Birth Weight Infants Live-Born to Resi-dents of a Defined Geographic Region Before andAfter Neonatal Intensive Care, ” Pediatrics69(5):613-620, 1982.Hoskins, E. M., Elliott, E., Sherman, A. T., et al.,“Outcome of Very Low-Birth Weight InfantsBorn at a Perinatal Center, ” Am. J. Ob. Gyn.145:135-140, 1983.Information Service Center, Inc., unpublisheddata, prepared under contract with the Office ofTechnology Assessment, Baltimore, MD, July1986.InterStudy, “The InterStudy Edge, ” Excelsior,MI, summer 1987.Jobe, A., “Surfactant Treatment for RespiratoryDistress Syndrome,” Respiratory Care 31(6):467-476, June 1986.Joint Commission on Accreditation of Hospitals,Accreditation ManuaZfor Hospitals, 1986 (Chi-cago, IL: Joint Commission on Accreditation ofHospitals, 1986).Kanto, W. P., Johnson, G., Sturgill, C., et al.,“Performance of a Level II Nursery in a NeonatalRegional Program,” Southern Med. J. 75(9):1043-1050, September 1982.Kenney, A. M., Torres, A., Dittes, N., et al.,“Medical Expenditures for Maternity and New-born Care in America, ” Family Planning Per-spectives 18(3):103-110, May/June 1986.Kiely, J. L., Paneth, N., Stein, Z., et al., “Cere-bral Palsy and Newborn Care, II: Mortality andNeurological Impairment in Low-Birthweight In-fants,” Dev. Med. Child Neurol. 23:650-659,1981.Kilbride, H. W., Children’s Mercy Hospital,Kansas City, MO, unpublished data, Nov. 4,1986.Kilbride, H. W., Claflin, K, S., Daily, D. K., etal., “Improved Survival of Infants <801 GramsBirthweight,” unpublished mimeo, Kansas City,MO, 1986.Kitchen, W. H., Ford, G., Orgill, A., et al., “Out-come in Infants With Birth Weight 500 to 999Gm: A Regional Study of 1979 and 1980 Births, ”J. Pediatrics 104:921-927, 1984.

72
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
Kitchen, W. H., Yu, V. Y. H., Lissenden, J. V., etal., “Collaborative Study of Very-Low-Birth-weight Infants: Techniques of Perinatal Care andMortality, ” The Lancet i:1454-1457, 1982.Knobloch, H., Malone, A., Ellison, P. H., et al.,“Considerations in Evaluating Changes in Out-come for Infants Weighing Less Than 1,501Grams,” Pediatrics 69:285-295, 1982.Konishi, M., Fujiwara, T., Naito, T., et al., “Sur-factant Replacement Therapy in Neonatal Res-piratory Distress Syndrome (RDS)—A Prospec-tive Collaborative Study,” paper presented at theXVIII International Congress of Pediatrics, Hon-olulu, HI, July 7, 1986.Koops, B. L., Morgan, L. J., and Battaglia, F. C.,“Neonatal Mortality Risk in Relation to BirthWeight and Gestational Age: Update, ” J. Pedi-atrics 101:969-977, 1982.Kraybill, E. N., Bose, C. L., and D’Ercole, A. J.,“Chronic Lung Disease in Infants With Very LowBirth Weight, ” Am. J. Dis. Child. 141:784-788,July 1987.Kraybill, E. N., Kennedy, C. A., Teplin, S. W.,et al., “Infants With Birth Weights Less Than1,001 G: Survival, Growth, and Development, ”Am. J. Dis. Child. 138:837-842, 1984.Krishnamoorthy, K. S., Shannon, D. C., Delong,G. R., et al., “Necrologic Sequelae in the Sur-vivors of Neonatal Intraventricular Hemor-rhage, “ Pediatrics 64:233-237, 1979.Lament, R. F., Dunlop, P. D. M., Crowley, P., etal., “Comparative Mortality and Morbidity ofInfants Transferred In Utero or Postnatally, ” J.Perinat. Med. 11:200-203, 1983.Lantos, J., “Baby Doe Five Years Later: Impli-cations for Child Health, ” IV. Eng. J. Med.317(7):444-447, Aug. 13, 1987.Laudicina, S. S., A Comparative Survey of Meal-icaid Hospital Reimbursement Systems for In-patient Services, State by State, 1980-198S(Washington, DC: The Urban Institute, Decem-ber 1985),Levi, S., Taylor, W., Robinson, L. E., et al.,“Analysis of Morbidity and Outcome of InfantsWeighing Less Than 800 Grams at Birth,” South-ern Med. J. 77:975-978, 1984.Lobb, M. O., Morgan, M. E. I., Bond, A. P., et al.,“Transfer Before Delivery on Merseyside: AnAnalysis of the First 140 Patients, ” Br. J. Ob.Gyn. 90:338-341, April 1983.Long, T. C., Phibbs, C. S., Gould, J. B., et al.,“Changes in Costs of Neonatal Intensive CareOver Five Years, ” abstract submitted to theAmerican Pediatric Society, 1985.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
Lubchenco, L. O., Homer, F. A., Reed, L. H., etal., “Sequelae of Premature Birth, ” Am. J. Dis.Child. 106:101-115, 1963.Lubeck, D. P., and Bunker, J. P., The ArtificialHeart: Costs, Risks, and Benefits (Health Tech-nology Case Study #9), prepared for the Officeof Technology Assessment, U.S. Congress, PB82-239971 (Springfield, VA: National Techni-cal Information Service, May 1982).Lucey, J. F., and Dangman, B., “A Reexamina-tion of the Role of Oxygen in Retrolental Fibro-plasia, “ Pediatrics 73:82-96, 1984.Markestad, T., and Fitzhardinge, P. M., “Growthand Development in Children Recovering FromBronchopulmonary Dysplasia, ” J. Pediatrics98(4):597-602, April 1981.Marlow, N., D’Souza, S. W., and Chiswick,M. L., “Neurodevelopmental Outcome in BabiesWeighing Less Than 2001 G at Birth, ” Br. Med.J. 294:1582-1586, June 20, 1987.McCormick, M. C., Shapiro, S., and Starfield,B. H., “The Regionalization of Perinatal Services:Summary of the Evaluation of a National Dem-onstration Program, ” JAMA 253(6):799-804,Feb. 8, 1985.Merit, L. R., “Prevention of Neonatal Intraven-tricular Hemorrhage, “N. Eng. J. Med. 312(21):1385-1387, May 23, 1985.Merritt, T. A., Hallman, M., Bloom, B. T., et al.,“Prophylactic Treatment of Very Premature In-fants With Human Surfactant,” N. Eng. J. Med.315(13):785-790, Sept. 25, 1986.Modanlou, H. D., Dorchester, W., Freeman,R. K., et al., “Perinatal Transport to a RegionalPerinatal Center in a Metropolitan Area: Mater-nal Versus Neonatal Transport, ” Am. J. Ob.Gyn. 138(8):1157-1164, 1980 .Morley, C. J., “Ten Centre Trial of Artificial Sur-factant (Artificial Lung Expanding Compound)in Very Premature Babies, ” Br. Med. J. 294:991-996, April 1987.Moskop, J. C., and Saldanha, R. L., “The BabyDoe Rule: Still a Threat, ” Hastings Center Re-port 16(2):8-14, April 1986.Murray, T. H., “The Final, Anticlimactic Rule onBaby Doe, ” Hastings Center Report 15:5-9, June1985.National Association of Children’s Hospitals andRelated Institutions, Inc., “Children’s Hospitals’Utilization, Personnel, and Finances and Chil-dren’s Hospitals’ Operating Indicators From the1984 AHA Annual Survey of Hospitals, ” unpub-lished mimeo, Alexandria, VA, December 1985.

108.
109.
110.
111,
112,
113.
114<
115.
116,
117,
118.
119.
120.
National Association of Children’s Hospitals andRelated Institutions, Inc., unpublished clata,Alexandria, VA, August 1986.National Association of Children’s Hospitals andRelated Institutions, Inc., “Children’s HospitalsCase Mix Classification Project, Classification ofNeonates, ” unpublished mimeo, Alexandria,VA, August 1986.National Association of Children’s Hospitals andRelated Institutions, Inc., Children’s HospitalsCase Mix Classification System Project Phase IIIReport (Alexandria, VA: NACHRI, September1986).National Association of Children’s Hospitals andRelated Institutions, Inc., Children’s HospitalsCase Mix Classification System Project Phase IIIReport Executive Summary (Alexandria, VA:NACHRI, September 1986).National Perinatal Information Center, unpub-lished data from the American Hospital Asso-ciation’s 1983 Annual Survey of Hospitals,Providence, RI, December 1986.Nelson, R. M., Resnick, M. B., and Eitzman,D. V., “Intensive Care and the Very-Low-Birth-weight Infant—Letter, ” The L.ancet ii: 737, 1979.Newns, B., Drummond, M. F., Durbin, G. M.,et al., “Costs and Outcomes in a Regional Neo-natal Intensive Care Unit, ” Arch. Dis. Child.59:1064-1067, 1984.Nichols, M. N., “Care of the Extremely Small In-fant, ” letter to the editor, N, Eng. J. Med.315(7):455, Aug. 14, 1986.Nickel, R. E., Bennett, F. C., and Lamson, F. N,,“School Performance of Children With BirthWeights of 1,000 G or Less, ” Am. J. Dis. Child.136:105-110, February 1982.Nugent, R. R., “Perinatal Regionalization inNorth Carolina, 1967-1979: Services, Programs,Referral Patterns and Perinatal Mortality RateDeclines for Very Low Birthweight Infants, ” N.Carolina Med. J. 43(7):513-515, July 1982.Orgill, A. A., Astbury, J., Bajuk, B . , e t a l . ,“Early Development of Infants 1000 G or Lessat Birth, ” Arch. Dis. Child. !57:823-827, 1982.Paneth, N., Kiely, J. L., and Susser, M., “Age atDeath Used To Assess the Effect of Interhospi-tal Transfer of Newborns, ” Pediatrics 73:854-861, 1984.Paneth, N., Kiely, J. L., Wallenstein, S., et al.,“The Choice of Place of Delivery: Birthweightand Gestational Age as Indicators of the Effectof Medical Care on Neonatal Mortality, ” unpub-lished mimeo, New York, NY, no date.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134,
135.
136.
Papile, L-A., Munsick-Bruno, G., and Schaefer,A., “Relationships of Cerebral IntraventricularHemorrhage and Early Childhood NecrologicHandicaps, ” J. Pediatrics 103:273-276, 1983.Perelman, R. H., and Farrell, P. M., “Analysis ofCauses of Neonatal Death in the United StatesWith Specific Emphasis on Fatal Hyaline Mem-brane Disease, ” Pediatrics 70:570-575, 1982.Perlman, J. M., Goodman, S., Kreusser, K. L., etal., “Reduction in Intraventricular Hemorrhageby Elimination of Fluctuating Cerebral Blood-Flow Velocity in Preterm Infants With Respira-tory Distress Syndrome, ” N. Eng. J. Med.312(21):1353-1357, May 23, 1985.Phelps, D. L., “Retinopathy of Prematurity: AnEstimate of Vision Loss in the United States—1979, ” Pediatrics 67:924-926, 1981.Phelps, D. L., “Vitamin E and RetrolentalFibroplasia in 1982,” Pediatrics 70:420-425, 1982.Phibbs, C. S., University of California, SanDiego, unpublished data, April 1986.Phibbs, C. S., University of California, SanDiego, unpublished data, March 1987.Phibbs, C. S., University of California, SanDiego, personal communication, May 1987.Phibbs, C. S., Williams, R. L., and Phibbs, R. H.,“Newborn Risk Factors and Costs of NeonatalIntensive Care, ” Pediatrics 68:313-321, 1981.Phibbs, C, S., Phibbs, R. H., Pomerance, J. J., etal., “Alternative to Diagnosis-Related Groups forNewborn Intensive Care, ” Pediatrics 78(5):829-836, 1986.Philip, A, G. S,, Little, G. A., Polivy, D. R., et al.,“Neonatal Mortality Risk for the Eighties: TheImportance of Birth Weight/Gestational Age .Groups,” Pediatrics 68(1):122-130, 1981.Pollara, B., Albany Medical Centerr Albany,NY, unpublished data, Dec. 18, 1986.Powell, T. G., Pharoah, P. O. D., and Cooke,R. W. I., “Survival and Morbidity in a Geographi-cally Defined Population of Low Birthweight In-fants,” The Lancet i:539-543, Mar. 8, 1986.Prospective Payment Assessment Commission,Medicare Prospective Payment and the Amer-ican Health Care System: Report to the Congress(Washington, DC: February 1986).Public Health Foundation, Public Health Agen-cies 1984, Vol. 4: An Inventory of Programs andBlock Grant Expenditures (Washington, DC:Public Health Foundation, July 1986).Raval, D., Krishnaswamy, R., Pildes, R. S., etal., “Neurodevelopmental Outcome in Very LowBirth Weight ( <1250 gins) Infants With Bron-

74
137.
138.
139.
140,
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
copulmonary Dysplasia, ” paper presented at theRoss Labortories Special Conference on Topicsin Neonatology, Washington, DC, Dec. 7-9,1986.Robin, E. D., and Burke, C. M., “The Recrudes-cent Epidemic of Retrolental Fibroplasia, ” Chest89:576-578, 1986.Ross Laboratories, unpublished data, Columbus,OH, December 1986.Saigal, S., Rosenbaum, P., Stoskopf, B., et al.,“Follow-up of Infants s01 to 1,sOO Gm BirthWeight Delivered to Residents of a Geographi-cally Defined Region With Perinatal IntensiveCare Facilities,” J. Pediatrics 100(4):606-613,1982.Saigal, S., Rosenbaum, P., Stoskopf, B., et al.,“Outcome in Infants s01 to 1000 Gm BirthWeight Delivered to Residents of the McMasterHealth Region,”J. Pediatrics 105:969-976, 1984.Sandhu, B., Stevenson, R. C., Cooke, R. W. I., etal., “Cost of Neonatal Intensive Care for Very-Low-Birthweight Infants, ” The Lancet i:600-603,1986.Schechner, S., “For the 1980s: How Small Is TooSmall?” Clinics in Perinatology 7(1):135-143,1980,Schreiner, R., Indiana University School ofMedicine, Indianapolis, IN, personal communi-cation, Mar. 10, 1986.Schwartz, R., National Perinatal InformationCenter, Providence, RI, personal communica-tion, Dec. 31, 1986.Schweitzer, S.0., and Scalzi, C. C., The Cost Ef-fectiveness of Bone Marrow Transplantation andIts Policy Implications (Health Technology CaseStudy #6), prepared for the Office of Technol-ogy Assessment, U.S. Congress, PB 81-221798(Springfield, VA: National Technical Informa-tion Service, May 1981).Sell, E. J., “Outcome of Very Very Low BirthWeight Infants, ” Clinics in Perinatology 13(2):451-459, June 1986.Shapiro, D. L., University of Rochester MedicalSchool, Rochester, NY, personal communica-tion, March 1986.Shapiro, D. L., “Report of the Subcommittee onFetal Extrauterine Survivability, ” unpublishedmimeo, Rochester, NY, May 20, 1987.Shapiro, D. L., University of Rochester MedicalSchool, Rochester, NY, personal communica-tion, June 1987.Shapiro, D. L., and Rosenberg, P., “The Effectof Federal Regulations Regarding HandicappedNewborns,” JAMA 252(15):2031-2033, 1984.
151.
152.
153.
154.
155.
156.
157.
158.
159.
160,
161.
162.
163.
164.
165,
166,
Shapiro, S., McCormick, M. C., Starfield, B. H.,et al., “Changes in Infant Morbidity AssociatedWith Decreases in Neonatal Mortality, ” Pedi-atrics 72(3):408-415, 1983.Sherman, A. T., and Milligan, J. E., “The Growthand Development of Infants Weighing 1,000 to2,OOO Grams at Birth and Delivered in a Perina-tal Unit, ” Am. J. Ob. Gyn. 136:273-275, 1980.Shinnar, S., Molteni, R. A., Gammon, K., et al.,“Intraventricular Hemorrhage in the PrematureIn fant,” N. Eng. J. Med. 306:1464-1468, 1982.Showstack, J. A., Stone, M. H., and Schroeder,S. A., “The Role of Changing Clinical Practicesin the Rising Costs of Hospital Care, ” N. Eng.J. Med. 313(19):1201-1207, November 1985.Siegel, E., Gillings, D., Campbell, S., et al., “AControlled Evaluation of Rural Regional Perina-tal Care: Impact on Mortality and Morbidity, ”AJPff 75(3):246-253, March 1985.Silverman, W. A., RetroZental Fibroplasia: AModern Parable (New York: Grune & Stratton,1980).Sinclair, J. C., Torrance, G. W., Boyle, M., et al.,“Evaluating Neonatal Intensive Care, ” letter tothe editor, The Lancet ii(8254):1052, Nov. 7,1981.Sol], R. F., “Surfactant and BronchopulmonaryDysplasia,” paper presented at the Ross Labora-tories Special Conference on Topics in Neona-tology, Washington, DC, Dec. 7-9, 1986.Stahlman, M. T., “Newborn Intensive Care: Suc-cess or Failure?” J. Pediatrics 105:162-167, 1984.Stevenson, D. K., Ariagno, R. L., Kutner, J. S.,et al., “The ‘Baby Doe’ Rule,” JAMA 255(14):1909-1912, 1986.Stewart, A. L., University College London, Lon-don, unpublished data, Apr. 13, 1987.Stewart, A. L., Reynolds, E. O. R., and Lipscomb,A. P., “Outcome for Infants of Very Low Birth-weight: Survey of World Literature, ” The L.an-cet i:1038-1041, May 9, 1981.Stewart, A. L., Reynolds, E. O. R., Hope, P. L.,et al., “Probability of Neurodevelopmental Dis-orders Estimated From Ultrasound Appearanceof Brains of Very Preterm Infants, ” Dev. Med.Child Neurol. 29:3-11, 1987.Strain, J. E., letter to the editor, N. Eng. J. Med.315(11):708, Sept. 11, 1986 .Strong, Carson, “The Tiniest Newborns, ” TheHasting Center Report 13:14-19, February 1983.Subramanian, C., Clark-Prakash, C., Dadina,Z. K., et al., “Intensive Care for High-Risk In-fants in Calcutta,” Am. J. Dis. Child. 140:885-888, September 1986.

167.
168.
169.
170.
171.
172.
173.
174.
175.
176.
177.
75
Tarnow-Mordi, W., and Wilkinson, A., “Me-chanical Ventilation of the Newborn, ” Br-. Med.J. 292:575-576, 1986.Taussig, L. M., “Bronchopulmonary Dysplasia, ”Follow-Up of the High Risk Newborn—A Prac-tical Approach, E.J. Sell (cd. ) (Springfield, IL:Charles C. Thomas, 1980).U.S. Congress, Office of Technology Assess-ment, Payment for Physician Services: Strategiesfor Medicare, OTA-H-294 (Washington, DC:U.S. Government Printing Office, February1986).U.S. Congress, Office of Technology Assess-ment, Healthy Children: Investing in the Future,OTA-H-344 (Washington, DC: U.S. Govern-ment Printing office, in press, 1987).U.S. Department of Health and Human Services,Health Care Financing Administration, Analy-sis of State Medicaid Program Characteristics,1984, HFCA Pub. No. 03204 (Baltimore, MD:HCFA, August 1985).U.S. Department of Health and Human Services,Public Health Service, Center for Disease Con-trol, “National Infant Mortality Surveillance(NIMS), ” unpublished tables, May 1986.U.S. Department of Health and Human Services,Public Health Service, National Center forHealth Statistics, “Advance Report of Final Na-tality Statistics, 1984, Table 24, ” Monthly VitalStatistics Report 35(4, suppl. ):37, July 18, 1986.U.S. Department of Health and Human Services,Public Health Service, National Institutes ofHealth, National Heart, Lung, and Blood Insti-tute, Prevention of Respiratory Distress Syn-drome, Effect of Antenatal Dexamethasone Admin-istration, NIH Pub. No. 85-2695 (Washington,DC: NIH, August 1985).Vogt, J. F., Chan, L. S., Wu, P. Y. K., et al., “Im-pact of a Regional Infant Dispatch Center onNeonatal Mortality,” AJPH 71:577-582, 1981.Vohr, B. R,, and Hack, M., “DevelopmentalFollow-Up of Low-Birth-Weight Infants, ” Peal.C]in. North Am. 29:1441-1454, 1982.Vohr, B. R., Bell, E, F., and Oh, W., “InfantsWith Bronchopulmonary Dysplasia, ” Am. J.Dis. Child, 136:443-447, May 1982.
178.
179.
180.
181.
182.
183,
184.
185.
186.
187.
188,
189.
Volpe, J. J., “Neonatal Intraventricular Hemor-rhage, ” N. Eng. J. Med. 304:886-891, 1981.Wagner, J. L., “The Economic Evaluation ofDrugs: A Review of the Literature, ” prepared forthe Pharmaceutical Manufacturer’s Association,Washington, DC, August 1982.Walker, D-J, B., Feldman, A., Vohr, B. R., et al.,“Cost-Benefit Analysis of Neonatal IntensiveCare for Infants Weighing Less Than 1,000Grams at Birth, ” Pediatrics 74(1):20-25, 1984.Washington Report on Medicine and Health,“Life and Death Decisions in the Nursery, ”Washington Report on Medicine and Health40(26 ):( Perspectives), June 30, 1986.Washington Report on Medicine and Health,“Briefly This Week, ” Washington Report onMedicine and Health 40(44):4, Nov. 10, 1986.Wilkinson, A,, Jenkins, P. A., and Jeffrey, J. A.,“Two Controlled Trials of Dry Artificial Surfac-tant: Early Effects and Later Outcome in BabiesWith Surfactant Deficiency, ” The L.ancet ii:287-291, 1985,Williams, R. L., and Chen, P. M., “Identifying theSources of the Recent Decline in Perinatal Mor-tality Rates in California, ” N. Eng. ]. Med.306(4):207-214, 1982.Wilson, A, L., Wellman, L. R., Fenton, L. J., et al.,“What Physicians Know About the Prognosis ofPreterm Newborns,” Am. J. Dis. Child. 137:551-554, 1983.Yu, V. Y. H., “The Case for Neonatal IntensiveCare,” Med. J. of Australia 142:353-355, 1985.Yu, V. Y. H., Hookham, D. M., and Nave, J. R. M.,“Retrolental Fibroplasia–Controlled Study of 4Years’ Experience in a Neonatal Intensive CareUnit,” Arch. Dis. Child. 57:247-252, 1982.Yu, V. Y. H,, Watkins, A., and Bajuk, B., “Neo-natal and Postneonatal Mortality in Very LowBirthweight Infants,” Arch. Dis. Child. 59:987-989, 1984.Zwischenberger, J. B., Cilley, R. E., Andrews,A. F., et al., “The Role of Extracorporeal Mem-brane Oxygenation in the Management of Res-piratory Failure in the Newborn, ” RespiratoryCare 31(6):491-495, June 1986.