Embed Size (px)
Citation preview

DOI: 10.1542/peds.2011-3212; originally published online January 30, 2012; 2012;129;e540Pediatrics
COMMITTEE ON FETUS AND NEWBORNMark L. Hudak, Rosemarie C. Tan, THE COMMITTEE ON DRUGS and THE
Neonatal Drug Withdrawal
http://pediatrics.aappublications.org/content/129/2/e540.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

CLINICAL REPORT
Neonatal Drug Withdrawal
abstractMaternal use of certain drugs during pregnancy can result in transientneonatal signs consistent with withdrawal or acute toxicity or causesustained signs consistent with a lasting drug effect. In addition, hos-pitalized infants who are treated with opioids or benzodiazepines toprovide analgesia or sedation may be at risk for manifesting signsof withdrawal. This statement updates information about the clinicalpresentation of infants exposed to intrauterine drugs and the thera-peutic options for treatment of withdrawal and is expanded to includeevidence-based approaches to the management of the hospitalized in-fant who requires weaning from analgesics or sedatives. Pediatrics2012;129:e540–e560
INTRODUCTION
Use and abuse of drugs, alcohol, and tobacco contribute significantlyto the health burden of society. The 2009 National Survey on Drug Useand Health reported that recent (within the past month) use of illicitdrugs, binge or heavy alcohol ingestion, and use of tobacco productsoccurred in 8.7%, 23.7%, and 27.7%, respectively, of the population12 years or older.1 Numerous case reports have documented the useof a variety of drugs by women of childbearing age (Table 1). In-trauterine exposure to certain drugs may cause congenital anomaliesand/or fetal growth restriction, increase the risk of preterm birth,produce signs of withdrawal or toxicity in the neonate, or impairnormal neurodevelopment.2 Fetal exposure to marijuana, the illicitdrug most commonly used by pregnant women, does not causeclinically important neonatal withdrawal signs but may have subtleeffects on long-term neurobehavioral outcomes.3 With the use ofcomputer-assisted interviewing techniques that preserved confiden-tiality, the 2009 National Survey on Drug Use and Health noted that4.5% of pregnant women 15 to 44 years of age reported recent useof illicit drugs (eg, marijuana, cocaine, hallucinogens, heroin, meth-amphetamines, and nonmedical use of prescription drugs). Binge orheavy drinking in the first trimester was reported by 11.9%, andrecent tobacco use was reported by 15.3%. Rates of recent illicit druguse and smoking were lower among pregnant compared with non-pregnant women across all age groups, except for those 15 to 17years of age. In the latter age group, the rates of illicit drug use andsmoking were higher among those who were pregnant comparedwith those who were not pregnant (15.8% vs 13.0% and 20.6% vs13.9%, respectively). The reported rates of illicit drug use most likelyunderestimate true rates, because the percentage of pregnant womenwho report the recent use of illicit drugs on screening interviews can
Mark L. Hudak, MD, Rosemarie C. Tan, MD,, PhD, THECOMMITTEE ON DRUGS, and THE COMMITTEE ON FETUS ANDNEWBORN
KEY WORDSopioid, methadone, heroin, fentanyl, benzodiazepine, cocaine,methamphetamine, SSRI, drug withdrawal, neonate, abstinencesyndrome
ABBREVIATIONSCNS—central nervous systemDTO—diluted tincture of opiumECMO—extracorporeal membrane oxygenationFDA—Food and Drug Administration5-HIAA—5-hydroxyindoleacetic acidICD-9—International Classification of Diseases, Ninth RevisionNAS—neonatal abstinence syndromeSSRI—selective serotonin reuptake inhibitor
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The guidance in this report does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account individual circumstances, may beappropriate.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-3212
doi:10.1542/peds.2011-3212
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
e540 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Guidance for the Clinician inRendering Pediatric Care
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

be substantially lower than that de-termined by drug screening using bi-ological samples. For infants, the useof International Classification of Dis-eases, Ninth Revision (ICD-9)-based hos-pital discharge databases to determinethe incidence of neonatal drug with-drawal secondary to intrauterine expo-sure has in the past underestimatedthe incidence of this condition.4 Datacompiled by the Agency for Health-care Research and Quality and by theFlorida Department of Health attest toan increased incidence and/or recog-nition of neonatal withdrawal syn-drome (ICD-9 code 779.5). Nationally, thenumber of infants coded at dischargewith neonatal withdrawal increasedfrom 7653 in 1995 to 11 937 in 2008. InFlorida, the number of newborns dis-charged with ICD-9 code 779.5 climbedby more than 10-fold, from 0.4 to 4.4discharges per 1000 live births, from1995 to 2009. An indeterminate part ofthese observed increases has resultedfrom more liberal use of prescriptionopiates in pregnant women to palliatea wide variety of etiologies of acute
or chronic pain. In a recent report,chronic use of narcotic prescriptions(use for ≥1 intrapartum month) amongpregnant women cared for at a singleclinic increased fivefold from 1998 to2008, and 5.6% of infants deliveredto these women manifested signs ofneonatal withdrawal.5
Signs characteristic of neonatal with-drawal have been attributed to intra-uterine exposure to a variety of drugs(Table 2). Other drugs cause signs inneonates because of acute toxicity.Chronic in utero exposure to a drug (eg,alcohol) can lead to permanent phe-notypical and/or neurodevelopmental-behavioral abnormalities consistentwith drug effect. Signs and symptomsof withdrawal worsen as drug levelsdecrease, whereas signs and symp-toms of acute toxicity abate with drugelimination. Clinically important neo-natal withdrawal most commonly re-sults from intrauterine opioid exposure.The constellation of clinical findingsassociated with opioid withdrawal hasbeen termed the neonatal abstinence
syndrome (NAS). Among neonates ex-posed to opioids in utero, withdrawalsigns will develop in 55% to 94%.6–9
Neonatal withdrawal signs have alsobeen described in infants exposed an-tenatally to benzodiazepines,10,11 bar-biturates,12,13 and alcohol.14,15
COCAINE AND OTHER STIMULANTS
An abstinence syndrome after intra-uterine exposure to central nervoussystem (CNS) stimulants such as co-caine and amphetamine has not beenclearly defined. Many studies that haveassessed behavior and neurologic signsin cocaine-exposed infants have usedscoring systems that were designedto evaluate opioid withdrawal. Neuro-behavioral abnormalities16,17 frequentlyoccur in neonates with intrauterinecocaine exposure, most frequently onthe second or third postnatal days.18
These abnormalities may include ir-ritability, hyperactivity, tremors, high-pitched cry, and excessive sucking.Because cocaine or its metabolitesmay be detected in neonatal urine
TABLE 1 Major Drugs of Abusea
Opioids CNS Stimulants CNS Depressants Hallucinogens
Agonists Amphetamines Alcohol Indolealkylamines (LSD, psilocin, psilocybin, DMT, DET)Morphine Dextroamphetamine (Dexedrine) Barbiturates Phenylethylamines (mescaline, peyote)Codeine Methamphetamine Benzodiazepines Phenylisopropylamines (MDA, MMDA, MDMA, MDEA)Methadone Amphetamine sulfate Other sedative-hypnotics InhalantsMeperidine (Demerol) Amphetamine congeners Methaqualone (Quaalude) Solvents and aerosols (glues, gasoline, paint thinner,
cleaning solutions, nail polish remover, Freon)Oxycodone (Percodan, OxyIR,
Percolone, Roxicodone,Percocet, OxyContin)
Benzphetamine (Didrex) Glutethimide (Doriden) Nitrites
Propoxyphene (Darvon) Diethylpropion (Tenuate) Chloral hydrate Nitrous oxideHydromorphone (Dilaudid) Fenfluramine CannabinoidsHydrocodone (Lortab, Vicodin) Phendimetrazine (Adipost, Bontril,
Prelu-2)Marijuana
Fentanyl (Sublimaze) Phentermine (Adipex-P, Zantryl) HashishTramadol (Ultram, Ultracet) CocaineHeroin Methylphenidate (Ritalin, Concerta)
Antagonists Pemoline (Cylert)Naloxone (Narcan) PhenylpropanolamineNaltrexone (ReVia) Phencyclidines
Mixed Agonist-Antagonists NicotinePentazocine (Talwin)Buprenorphine (Buprenex)
DET, diethyltryptamine; DMT, dimethyltryptamine; LSD, lysergic acid diethylamide; MDA, methylenedioxyamphetamine; MDEA, 3,4-methylenedioxyethamphetamine; MDMA, 3,4-methylene-dioxymethamphetamine (ecstasy); and MMDA, 3-methoxy-4,5-methylenedioxyamphetamine.a Adapted from Milhorn.160
PEDIATRICS Volume 129, Number 2, February 2012 e541
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

for as long as 7 days after delivery,18
observed abnormalities in exposed in-fants may reflect drug effect ratherthan withdrawal. In an unmasked study,6%, 14%, and 35% of infants exposedto cocaine only, heroin only, or cocaineplus heroin, respectively, qualified fortreatment on the basis of scoring.19
Several studies that used masked eval-uators found that cocaine-exposed in-fants had either no20,21 or minimal22
withdrawal signs compared with cocaine-naïve infants (ie, those never exposed).Eyler et al16 conducted a prospectivecontrolled study of 3 groups of infants:1 group had no documented exposureto cocaine by history or by maternaland infant urine testing; a second groupwas cocaine exposed but had negativeurine screening at birth; and a thirdgroup had cocaine metabolites de-tected in neonatal urine. Observersmasked to infant status performed as-sessments using the Brazelton Neo-natal Behavioral Assessment Scale.23
Infants who were positive for cocainemetabolites did not differ significantly
from metabolite-negative infants with ahistory of exposure nor from cocaine-naïve infants. These findings supportedneither a withdrawal nor a drug tox-icity syndrome. Cocaine-exposed infantshave been described as having a higherincidence of abnormal auditory brain-stem responses and EEGs, comparedwith nonexposed infants.24,25 In anotherstudy, infants with heavy exposure tococaine had similar Brazelton findingsat 2 to 3 days of age as did infantswith light or no exposure; however, by17 days of age, heavily exposed infantswere more excitable and demonstratedpoorer state regulation.26 No publishedstudies have carefully evaluated phar-macologic treatment of infants withsigns attributable to prenatal cocaineexposure.
Methamphetamine abuse has beenreported among pregnant women,27
although overall rates are low com-pared with cocaine and appear tohave decreased in the general popu-lation between 2006 and 2008.1 Meth-amphetamine is an extremely potent
sympathomimetic agent that induceseuphoria and increases alertness andself-confidence, because it produces amassive efflux of dopamine in the CNS.Pregnant women who abuse metham-phetamine are at increased risk of pre-term birth, placental abruption, fetaldistress, and intrauterine growth re-striction at rates similar to those forpregnant women who use cocaine. In1 study, only 4% of infants exposed tomethamphetamine were treated fordrug withdrawal, but it was not pos-sible to exclude concomitant abuse ofother drugs as contributory in allcases.27 There are reports of long-termadverse neurotoxic effects of in uteromethamphetamine exposure on behav-ior, cognitive skills, and physical dex-terity.28,29
SELECTIVE SEROTONIN REUPTAKEINHIBITORS
Selective serotonin reuptake inhibitors(SSRIs) are a class of antidepressantmedications that became available forwidespread clinical use in 1988. SSRIs
TABLE 2 Maternal Nonnarcotic Drugs That Cause Neonatal Psychomotor Behavior Consistent With Withdrawal
Drug Signs Onset of Signs Duration of Signsa Ref. No.
Alcohol Hyperactivity, crying, irritability, poor suck, tremors, seizures;onset of signs at birth, poor sleeping pattern, hyperphagia,diaphoresis
3–12 h 18 mo 14,15
Barbiturates Irritability, severe tremors, hyperacusis, excessive crying,vasomotor instability, diarrhea, restlessness, increased tone,hyperphagia, vomiting, disturbed sleep; onset first 24 h of lifeor as late as 10–14 d of age
1–14 d 4-6 mo with prescription 12,13
Caffeine Jitteriness, vomiting, bradycardia, tachypnea At birth 1-7 d 161Chlordiazepoxide Irritability, tremors; signs may start at 21 d Days–weeks 9 mo; 11/2 mo with prescription 11Clomipramine Hypothermia, cyanosis, tremors; onset 12 h of age 4 d with prescription 162Diazepam Hypotonia, poor suck, hypothermia, apnea, hypertonia,
hyperreflexia, tremors, vomiting, hyperactivity, tachypnea(mother receiving multiple drug therapy)
Hours–weeks 8 mo; 10–66 d with prescription 10
Ethchlorvynol Lethargy, jitteriness, hyperphagia, irritability, poor suck,hypotonia (mother receiving multiple drug therapy)
Possibly 10 d with prescription 163
Glutethimide Increased tone, tremors, opisthotonos, high-pitched cry,hyperactivity, irritability, colic
6 mo 164
Hydroxyzine Tremors, irritability, hyperactivity, jitteriness, shrill cry,myoclonic jerks, hypotonia, increased respiratory and heartrates, feeding problems, clonic movements (mother receivingmultiple drug therapy)
5 wk with prescription 58
Meprobamate Irritability, tremors, poor sleep patterns, abdominal pain 9 mo; 3 mo with prescription 165SSRIs Crying, irritability, tremors, poor suck, feeding difficulty,
hypertonia, tachypnea, sleep disturbance, hypoglycemia,seizures
Hours–days 1–4 wk 31–33,35
a Prescription indicates the infant was treated with pharmacologic agents, and the natural course of the signs may have been shortened.
e542 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

(eg, fluoxetine [Prozac], paroxetine[Paxil], sertraline [Zoloft], citalopram[Celexa], escitalopram [Lexapro], andfluvoxamine [Luvox]) are now the mostfrequently used drugs to treat depres-sion both in the general population andin pregnant women.30 Case reports,31
adverse drug reaction reports,32 andprospective studies33,34 linked third-trimester use of SSRIs in pregnantwomen to a constellation of neonatalsigns that include continuous crying, ir-ritability, jitteriness, and/or restlessness;shivering; fever; tremors; hypertonia orrigidity; tachypnea or respiratory dis-tress; feeding difficulty; sleep distur-bance; hypoglycemia; and seizures.35
The onset of these signs ranged fromseveral hours to several days afterbirth and usually resolved within 1 to 2weeks. In 1 infant exposed to parox-etine, signs persisted through 4 weeksof age.36 In severely affected infants, ashort-term course of chlorpromazineprovided measurable relief of symp-toms.36
Several authors have discussed whetherthese signs are better explained by se-rotonin syndrome (attributable to in-creased serotonin concentration in theintersynaptic cleft) or by SSRI with-drawal (attributable to a relative hypo-serotonergic state).30,32,35,37–40 In adults,treatment with a single SSRI maycause mild to moderate serotonin syn-drome, but severe signs are morelikely to occur when 2 or more drugsthat increase serotonin concentrationby different mechanisms are pre-scribed.35 In adults, serotonin syn-drome is characterized by the followingtriad of clinical signs: changes in men-tal status (agitation, confusion); auto-nomic hyperactivity (fever, tachycardia,tachypnea, diaphoresis, mydriasis); andneuromuscular abnormalities (tremor,clonus, hyperreflexia, hypertonia). Onthe other hand, serotonin withdrawalin adults manifests with subjective symp-toms that include anxiety, headache,
nausea, fatigue, low mood, and, rarely,extrapyramidal signs such as dysto-nia. Hence, in most cases, the clinicalsyndrome reported among neonatesborn to mothers on SSRI treatment isconsistent with a gradual resolution ofa hyperserotonergic condition ratherthan with the evolution of a hyposer-otonergic state. Still, in a few cases,drug withdrawal may be a better ex-planation.35
Biochemical studies that correlateserial serum SSRI (or active metabo-lite) concentrations and markers ofCNS serotonin activity (eg, 5-hydrox-yindoleacetic acid [5-HIAA], a metabo-lite of serotonin) with changes inclinical signs could be helpful in dif-ferentiating toxicity from withdrawal.In adults, cerebrospinal fluid concen-trations of 5-HIAA (but not serumconcentrations of serotonin) correlateinversely with increased CNS serotoninactivity that results from SSRI treat-ment. One prospective study comparedconcentrations of SSRI and activemetabolites at birth, 2 days of life, and2 weeks of life; cord blood monoamineand metabolite; and serial serotoner-gic scores in infants born to motherson treatment with SSRIs and thoseof SSRI-naïve control infants.39 The in-fants born to mothers on SSRIs hadan average serotonergic score four-fold greater than SSRI-naïve infants.Cord blood 5-HIAA concentrationswere inversely related to the initialserotonergic score, and the resolutionof neonatal signs correlated withrapid declines in serially measuredserum SSRI and metabolite concen-trations.39 These results do supportdrug toxicity rather than drug with-drawal as the cause of clinical signs.Recent authors have suggested theterms “serotonin discontinuation syn-drome”34 or “prenatal antidepressantexposure syndrome.”41
Although 1 study reported decreasedpain reactivity at 2 months of age
in infants with prenatal exposure toSSRIs,42 several recent reviews havenot identified adverse neurodevelop-mental outcomes among infants bornto women treated with SSRIs dur-ing pregnancy.30,34,43,44 SSRI treatmentshould be continued during preg-nancy at the lowest effective dose,because withdrawal of medicationmay have harmful effects on themother-infant dyad. Clinicians shouldbe aware that infants are at risk formanifesting clinical signs of drugtoxicity or withdrawal over the firstweek of life and arrange for earlyfollow-up after the initial hospital dis-charge. Ideally, recommendations aboutlactation and breastfeeding shouldbe made in consideration of what isknown about the differences amongdrugs in a therapeutic class vis-à-visthe ratio of human milk to maternalplasma drug concentration, the likelytotal daily infant drug dose (as afraction of the daily maternal drugdose normalized for weight), and theratio of infant to maternal plasmadrug concentration. However, in theabsence of known adverse effects (eg,diminished suck, sleep disturbances,decreased growth), what constitutesan acceptable fractional drug doseor ratio of plasma concentrations isarbitrary—is 0.10 acceptable but 0.20not? Paroxetine is the only SSRI forwhich the ratio of infant to maternalplasma concentrations is low anduniformly <0.10.45 Fortinguerra et al46
documented that paroxetine, sertra-line, and fluvoxamine are minimallyexcreted in human milk and providethe infant <10% of the maternal dailydose (normalized for weight). Yet,Weissman et al45 cite studies in which6% and 33% of the reported pairedinfant to maternal plasma concentra-tion ratios for sertraline and fluvox-amine, respectively, are >0.10. Amother on treatment with an SSRIwho desires to nurse her infantshould be counseled about the
PEDIATRICS Volume 129, Number 2, February 2012 e543
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

benefits of breastfeeding as well asthe potential risk that her infant maycontinue to be exposed to a measure-able level of the SSRI with unknownlong-term effects.
OPIOIDS
Opioids are a class of natural, en-dogenous, and synthetic compoundsthat activate primarily µ-opioid (butalso κ- and δ-opioid) receptors in theCNS to produce supraspinal analgesia.Other acute effects include sedation,euphoria, miosis, respiratory depres-sion, and decreased gastrointestinalmotility. Prolonged use results in phys-ical and psychological dependence. Asa class, opioids demonstrate a nar-row therapeutic index. On the otherhand, the interpatient range of dosenecessary to achieve a similar thera-peutic effect is fairly wide becauseof genetic differences in pharmacoki-netics and pharmacodynamics.47 Mor-phine is 1 of many natural opioidsthat can be extracted from the opiumpoppy. Codeine, heroin (diacetylmor-phine), hydromorphone (Dilaudid), fen-tanyl (Sublimaze), and methadone areexamples of synthetic opioids. Endog-enous opioids include enkephalins,endorphins, and endomorphins. Theterm opiate refers to a subclass ofalkaloid opioids. Methadone exertssecondary effects by acting as anN-methyl-D-aspartate receptor antago-nist, blocking the actions of glutamate,the primary excitatory neurotrans-mitter in the CNS. Opioids acutely in-hibit the release of noradrenaline atsynaptic terminals. With chronic opi-oid exposure, tolerance develops asthe rate of noradrenaline releaseover time increases toward normal.Abrupt discontinuation of exogenousopioids results in supranormal re-lease of noradrenaline and producesthe autonomic and behavioral signsand symptoms characteristic of with-drawal.
Opioid abuse in pregnant womenpresents additional risks for the fetusand newborn. Opioids are small lipo-philic molecular weight compoundsthat cross placental and blood-brainbarriers. Active or passive maternaldetoxification is associated with in-creased risk of fetal distress and fe-tal loss. Maintenance programs withmethadone (a full µ-opioid agonistand a Food and Drug Administration[FDA] schedule II controlled substance)for pregnant women can sustain opi-oid concentrations in the mother andfetus in ranges that minimize opioidcraving, suppress abstinence symp-tomatology, block heroin-induced eu-phoria, and prevent fetal stress. Otherbenefits from this once controversialtreatment are optimization of prenatalcare and general maternal physicaland mental health, as well as antici-pation of potential withdrawal signs inthe newborn infant. Disadvantages ofmethadone include the extremely un-likely achievement of successful de-toxification after delivery and a moresevere and prolonged course of NAScompared with heroin exposure. Theseissues have encouraged the develop-ment of other synthetic opioids as al-ternative treatments to methadone.
Subsequent to the Drug AddictionTreatment Act of 2000 that allowedoffice-based treatment of addiction byusing FDA schedule III to V drugs,the synthetic opioid buprenorphine(a partial µ-opioid agonist) was ap-proved by the FDA in 2002 as a sched-ule III controlled substance for thetreatment of opioid dependence. Nei-ther methadone nor buprenorphine isapproved for use in pregnant women,and both are categorized by the FDAas class C pregnancy drugs. None-theless, buprenorphine, either alone(Subutex) or in combination with nal-oxone (Suboxone), has been used bothas a first-line treatment of heroin ad-diction and as a replacement drug for
methadone. Recent results from theMaternal Opioid Treatment: HumanExperimental Research study suggestthat buprenorphine has some advan-tages to methadone as a treatment ofopioid addiction in pregnant women.Infants born to mothers treated withbuprenorphine had shorter hospitalstays (10 vs 17.5 days), had shortertreatment durations for NAS (4.1 vs9.9 days), and required a lower cumu-lative dose of morphine (1.1 vs 10.4 mg)compared with infants born to moth-ers on methadone maintenance.48
CLINICAL PRESENTATION OFOPIOID WITHDRAWAL
The clinical presentation of NAS varieswith the opioid, the maternal drughistory (including timing of the mostrecent use of drug before delivery),maternal metabolism, net transfer ofdrug across the placenta, placentalmetabolism (W. Snodgrass, MD, PhD,personal communication, 2008), infantmetabolism and excretion, and otherfactors. In addition, maternal use ofother drugs and substances suchas cocaine, barbiturates, hypnotics-sedatives, and cigarettes may influ-ence the severity and duration ofNAS. Because opioid receptors areconcentrated in the CNS and thegastrointestinal tract, the predom-inant signs and symptoms of pureopioid withdrawal reflect CNS irrita-bility, autonomic overreactivity, and gas-trointestinal tract dysfunction (Table 3).Excess environmental stimuli and hun-ger will exacerbate the perceived se-verity of NAS.
Onset of signs attributable to neonatalwithdrawal from heroin often beginswithin 24 hours of birth, whereaswithdrawal from methadone usuallycommences around 24 to 72 hours ofage.49 For both opioids, evidence ofwithdrawal may be delayed until 5 to7 days of age or later, which is typi-cally after hospital discharge.50 For
e544 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

infants exposed to buprenorphine, 1study found that onset of withdrawalpeaked at 40 hours and that signswere most severe at 70 hours ofage.51 The different time courses re-flect variations in the half-lives ofdrug elimination. However, if 1 weekor longer has elapsed between thelast maternal opioid use and deliveryof the infant, the incidence of neona-tal withdrawal is relatively low.52 Theincidence and severity of NAS aregreater in infants exposed to metha-done compared with those exposed tobuprenorphine48 or heroin. Still, se-vere withdrawal has been describedin 0 to 50% of buprenorphine-exposedinfants.53–55 In the acute phase, seiz-ures have occurred in 2% to 11% ofinfants withdrawing from opioids49,50,56;however, abnormal EEG results with-out overt seizure activity have beenreported in >30% of neonates.57,58
Subacute signs of opioid withdrawalmay last up to 6 months.59
Seizures also may be associated withwithdrawal from a variety of non-narcotic drugs (eg, barbiturates,12,14
alcohol,14 and sedative-hypnotics60,61).The mechanism and significance ofseizures associated with withdrawalare unclear. Withdrawal from ethanolbegins early, in general, during thefirst 3 to 12 hours after delivery.12,15
Diagnosis of sedative withdrawal ismore difficult, because classically itappears after the first few days of
life. Barbiturate withdrawal has a me-dian onset of 4 to 7 days, but a widerange from days 1 through 14.12,13
Other sedative-hypnotics have exhibi-ted even later onset, including as lateas day 12 for diazepam10 and day 21for chlordiazepoxide.11
Studies of the relationship betweenmaternal methadone dose and theincidence and severity of NAS haveprovided contradictory findings. Somestudies demonstrated that largermaternal methadone dosages in latepregnancy were associated with greaterneonatal concentrations and increasedrisk of withdrawal,8,9,62–68 but othersrefuted a correlation.69–74 This lack ofconsensus is explained in part by dif-ferent approaches to the managementof antenatal methadone maintenancetherapy. There were substantial var-iations in the mean and range of dailymethadone dose in the populationsstudied. Studies that found no corre-lation tended to enroll infants born tomothers who had been prescribedhigher doses of methadone (50–200mg/day), whereas those that did notea relationship between maternal doseand NAS sequelae reported lowermaternal doses (eg, <50 mg/day) orincluded women undergoing partialdetoxification.67 Another potential ex-planatory factor is the significant in-terindividual variability in maternalmethadone metabolism.75 As a re-sult, cumulative fetal exposure can
be expected to vary among infantsborn to mothers on equivalent metha-done regimens.
Methadone concentrations in cordblood and at 48 hours of age,72 as wellas the rate of decline in neonatal se-rum concentration,65 appear to corre-late with NAS signs. Kuschel et al72
found that infants who required rescuetreatment had lower cord blood meth-adone concentrations and that, in allbut 1 infant, methadone concentrationswere undetectable in the serum at48 hours. Doberczak65 noted that fasterdeclines in postnatal blood methadoneconcentrations were associated withmore severe CNS withdrawal.
Preterm Infants
Preterm infants have been describedas being at lower risk of drug with-drawal with less severe and/or pro-longed courses. Infants born at <35weeks’ gestation whose mothers re-ceived methadone maintenance hadsignificantly lower total and CNS ab-stinence scores than did term infantsof mothers receiving similar metha-done dosages.64 In a more recentstudy, lower gestational age corre-lated with a lower risk of neonatalwithdrawal.68 The apparent decreasedseverity of signs in preterm infantsmay relate to developmental immatu-rity of the CNS, differences in totaldrug exposure, or lower fat depotsof drug. Alternatively, the clinicalevaluation of the severity of absti-nence may be more difficult in pre-term infants, because scoring toolsto describe withdrawal were largelydeveloped in term or late preterminfants.76,77 In a retrospective study,Dysart et al78 compared the length ofhospital stay, duration of medication,and cumulative medication exposurefor preterm and term infants bornto mothers enrolled in a methadonemaintenance program. Infants wereevaluated by using an abstinencescoring system77 and treated uniformly
TABLE 3 Clinical Features of the Neonatal Narcotic Abstinence Syndrome
Neurologic Excitability Gastrointestinal Dysfunction
TremorsIrritabilityIncreased wakefulnessHigh-pitched cryingIncreased muscle toneHyperactive deep tendon reflexesExaggerated Moro reflexSeizuresFrequent yawning and sneezing
Poor feedingUncoordinated and constant suckingVomitingDiarrheaDehydrationPoor wt gainAutonomic signsIncreased sweatingNasal stuffinessFeverMottlingTemperature instability
PEDIATRICS Volume 129, Number 2, February 2012 e545
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

with a neonatal opiate solution. Alladverse outcomes were reduced in thepreterm cohort.
Abuse of Multiple Drugs
The abuse of multiple drugs duringpregnancy is not uncommon,79 but itseffect on the occurrence and severityof neonatal abstinence is controver-sial. In 1 study, abstinence scores ofinfants whose mothers abused co-caine and methadone were similar tothe scores of infants whose mothersreceived high-dose maintenance meth-adone.64 In another study, the neuro-behavioral scores of infants exposedto intrauterine cocaine were similarto those of infants exposed to bothcocaine and methadone.80 Conversely,an unmasked study reported higherabstinence scores in infants exposedto both cocaine and heroin in compar-ison with those exposed to heroin orcocaine alone.19 Infants born to moth-ers maintained on methadone whowere also heavy smokers (>20 ciga-rettes per day) demonstrated higherwithdrawal scores that peaked laterthan infants born to light smokers.81
A 1989 case report linked the adminis-tration of naloxone for the treatment ofapnea in a baby born to a mother withrecent methadone ingestion to the onsetof seizures. The seizures resolved aftermorphine treatment but did not respondto administration of phenobarbital ordiazepam.82 For this reason, maternaluse of opiates during pregnancy hasremained a relative contraindication tothe use of naloxone for the treatment ofapnea or hypoventilation during thetransition period after birth.
DIFFERENTIAL DIAGNOSIS
The presence of maternal character-istics known to be associated withdrug abuse during pregnancy can beconsidered an indication to screenfor intrauterine drug exposure. Thesecharacteristics include absent, late, or
inadequate prenatal care; a previouslydocumented or admitted history ofdrug abuse; a previous unexplained latefetal demise; precipitous labor; abruptioplacentae; hypertensive episodes; se-vere mood swings; cerebrovascularaccidents; myocardial infarction; andrepeated spontaneous abortions.80,83–88
The legal implications of testing and theneed for consent from the mother mayvary among the states.89 Each hospitalshould consider adopting a policy formaternal and newborn screening toavoid discriminatory practices and tocomply with local laws.
Withdrawal signs in the newborn maymimic other conditions, such as in-fection, hypoglycemia, hypocalcemia,hyperthyroidism, intracranial hemor-rhage, hypoxic-ischemic encephalopa-thy, and hyperviscosity.90 If none ofthese diagnoses is readily apparent,a detailed maternal drug historyshould be obtained that includesinterviewing the mother about druguse and abuse by her partner, friends,and parents, in addition to queriesabout the mother’s prescription andnonprescription drug use.90,91 Becausematernal self-reporting underestimatesdrug exposure and maternal urinescreening during pregnancy fails toidentify many cases of drug use,83
appropriate neonatal drug screeningshould be performed. Conversely, noclinical signs should be attributedsolely to drug withdrawal on the basisof a positive maternal history without acareful assessment to exclude othercauses.
Screening is most commonly accom-plished by using neonatal urine speci-mens. A urine sample must be collectedas soon as possible after birth, be-cause many drugs are rapidly me-tabolized and eliminated.90,92,93 Evenso, a positive urine screening resultmay only reflect recent drug use. Al-cohol is detectable in neonatal urinefor 6 to 16 hours after the last ma-
ternal ingestion. Amphetamines, ben-zodiazepines, cocaine metabolites, andopioids are usually cleared within 1 to3 days after birth. Marijuana and co-caine metabolites may be detectable forweeks, depending on maternal usage.94
Drugs that are excreted in the hep-atobiliary system as well as drugsexcreted by the fetal kidneys into theamniotic fluid are concentrated inmeconium. Hence, meconium analysisis most useful when the history andclinical presentation strongly suggestneonatal withdrawal, but the maternaland neonatal urine screening resultsare negative. Drawbacks of testing fordrugs in meconium are that it is nottypically performed by hospitals andthat results are often not available fordays to weeks. Meconium must becollected before it is contaminated bytransitional, human milk, or formulastools—otherwise, the assay may notbe valid or the reference laboratorymay reject the sample. Assay of me-conium, although not conclusive if theresults are negative, is more likelyto identify infants of drug-abusingmothers than is the testing of infantor maternal urine.95,96 Other speci-mens that have been tested in re-search laboratories are maternal andneonatal hair.97,98 Recently, testing ofumbilical cord tissue by using drugclass-specific immunoassays was shownto be in concordance with testing ofpaired meconium specimens at ratesof 97%, 95%, 99%, and 91% for thedetection of amphetamines, opiates, co-caine, and cannabinoids, respectively.99
The availability of this tissue from themoment of birth (in contrast to theinherent delay in collecting urine ormeconium) may foster the adoption ofthis method of testing.
ASSESSMENT ANDNONPHARMACOLOGIC TREATMENT
Several semiobjective tools are avail-able for quantifying the severity of
e546 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

neonatal withdrawal signs. Clinicianshave used discrete or serial scores toassist with therapeutic decisions. TheLipsitz tool, also known as the NeonatalDrug Withdrawal Scoring System,76
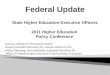
was recommended in the 1998 Amer-ican Academy of Pediatrics statement“Neonatal Drug Withdrawal,”100 prob-ably because it is a relatively simplemetric with good sensitivity for iden-tifying clinically important withdrawal.The modified Neonatal AbstinenceScoring System (Fig 1),101 is the pre-dominant tool used in the UnitedStates.102 This more comprehensiveinstrument assigns a cumulative scorebased on the interval observation of
21 items relating to signs of neonatalwithdrawal.103 In 1 study, administra-
tion of this scoring system with in-
fants verified not to have been exposed
to prenatal opiates by meconium anal-
ysis resulted in a stable median score
of 2 during each of the first 3 days of
life, with 95th percentile scores of 5.5
and 7 on days 1 and 2, respectively.104
Infants at risk for NAS should becarefully monitored in the hospitalfor the development of signs consis-tent with withdrawal. The appropriateduration of hospital observation isvariable and depends on a carefulassessment of the maternal drug
history. An infant born to a mother ona low-dose prescription opiate witha short half-life (eg, hydrocodone; av-erage half-life, 4 hours) may be safelydischarged if there are no signs ofwithdrawal by 3 days of age, whereasan infant born to a mother on an opiatewith a prolonged half-life (eg, metha-done) should be observed for a mini-mum of 5 to 7 days. Initial treatmentof infants who develop early signsof withdrawal is directed at minimiz-ing environmental stimuli (both lightand sound) by placing the infant in adark, quiet environment; avoiding auto-stimulation by careful swaddling; re-sponding early to an infant’s signals;
FIGURE 1Modified Finnegan’s Neonatal Abstinence Scoring Tool. Adapted from ref 101.
PEDIATRICS Volume 129, Number 2, February 2012 e547
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

adopting appropriate infant position-ing and comforting techniques (sway-ing, rocking); and providing frequentsmall volumes of hypercaloric formulaor human milk to minimize hunger andallow for adequate growth. Caloricneeds may be as high as 150 to 250cal/kg per day because of increasedenergy expenditure and loss of caloriesfrom regurgitation, vomiting, and/orloose stools.105,106 The infant needsto be carefully observed to recognizefever, dehydration, or weight losspromptly. The goals of therapy are toensure that the infant achieves ade-quate sleep and nutrition to establisha consistent pattern of weight gainand begins to integrate into a socialenvironment. Maternal screening forcomorbidities, such as HIV or hepatitisC virus infections and polydrug abuse,needs to be performed. Additionalsupportive care in the form of intra-venous fluids, replacement electro-lytes, and gavage feedings may benecessary to stabilize the infant’s con-dition in the acute phase and obviatethe need for pharmacologic interven-tion. When possible, and if not other-wise contraindicated, mothers whoadhere to a supervised drug treat-ment program should be encouragedto breastfeed so long as the infant con-tinues to gain weight. Breastfeeding orthe feeding of human milk has beenassociated with less severe NAS thatpresents later and less frequently re-quires pharmacologic intervention.107,108
Methadone is present in very low con-centrations in human milk. Cumula-tive daily intake of methadone in fullybreastfed infants has been estimatedto range from 0.01 to 0.15 mg/day inthe first 30 days of life109 and 0.15 to0.30 mg/day between 30 and 180 daysof age.110 Similarly, the amount ofbuprenorphine excreted in humanmilk is small. Although more informa-tion is needed to evaluate long-termneurodevelopmental outcome of in-fants exposed to small quantities of
buprenorphine, there is no clear rea-son to discourage breastfeeding inmothers who adhere to methadoneor buprenorphine maintenance treat-ment.111
Each nursery should adopt a protocolfor the evaluation and management ofneonatal withdrawal, and staff shouldbe trained in the correct use of anabstinence assessment tool. In a re-cent survey of accredited US neo-natology fellowship programs, only55% had implemented a written NASprotocol, and only 69% used a pub-lished abstinence scoring system.102
RATIONALE AND COMPARATIVEEVIDENCE FOR PHARMACOLOGICTREATMENT
Drug therapy is indicated to relievemoderate to severe signs of NAS and toprevent complications such as fever,weight loss, and seizures if an infantdoes not respond to a committedprogram of nonpharmacologic sup-port. Since the introduction of theabstinence scales in 1975, publishedreports have documented that thedecision to initiate pharmacologictreatment has been based on single orserial withdrawal scores. However, nostudies to date have compared the useof different withdrawal score thresh-olds for initiating pharmacologic in-tervention on short-term outcomes(eg, severity and duration of with-drawal signs, weight gain, duration ofhospitalization, need for pharmaco-logic treatment, or cumulative drugexposure). Withdrawal from opioidsor sedative-hypnotic drugs may belife-threatening, but ultimately, drugwithdrawal is a self-limited process.Unnecessary pharmacologic treatmentwill prolong drug exposure and theduration of hospitalization to the pos-sible detriment of maternal-infant bond-ing. The only clearly defined benefit ofpharmacologic treatment is the short-term amelioration of clinical signs.
Studies have not addressed whetherlong-term morbidity related to neona-tal drug withdrawal is decreased bypharmacologic management of affectedinfants, or whether continued postnataldrug exposure augments the risk ofneurobehavioral and other morbidities.It is possible that pharmacologic ther-apy of the infant may introduce or re-inforce a maternal disposition to relyon drugs for the treatment of infantdiscomfort or annoying behavior.112
Clinicians have treated NAS with a va-riety of drug preparations, includingopioids (tincture of opium, neonatalmorphine solution, methadone, andparegoric), barbiturates (phenobar-bital), benzodiazepines (diazepam,lorazepam), clonidine, and phenothia-zines (chlorpromazine). Informationpertinent to the use of these drugpreparations in infants is well sum-marized in the previous AmericanAcademy of Pediatrics statement.100
Recent surveys have documented that,in accord with the recommendationsof that statement, 94% of UK and 83%of US clinicians use an opioid (mor-phine or methadone) as the drug offirst choice. The majority of practi-tioners use phenobarbital as a seconddrug if the opiate does not adequatelycontrol withdrawal signs.102,113 Dailydoses of morphine ranged from 0.24mg/kg per day to 1.3 mg/kg per day.113
Paregoric is no longer used, becauseit contains variable concentrations ofother opioids, as well as toxic ingre-dients such as camphor, anise oil, al-cohol, and benzoic acid.100 The use ofdiazepam has also fallen into disfavorbecause of a documented lack of effi-cacy compared with other agents andbecause of its adverse effects on infantsuck and swallow reflexes.114–116
Meta-analyses of published trials re-garding the pharmacologic treatment ofneonatal withdrawal are available.117,118
In 2 Cochrane meta-analyses, either anopioid117 or a sedative118 drug treatment
e548 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

was compared with a control treatmentthat could include a nonpharmacologicintervention, a placebo treatment, oranother opioid and/or sedative drug.The authors prospectively designated4 primary outcomes (failure of treatmentto control withdrawal signs; incidenceof seizures; survival; and neurodevel-opmental outcome) for meta-analysis.Treatment failure was defined vari-ously as the inability of the treatmentto maintain abstinence scores withina preset “safe” level and/or the needto add another drug therapy. Somestudies did not report primary out-comes and instead quantified second-ary outcomes (eg, duration of treatment,duration of hospitalization, rate ofweight gain, etc).
Seven studies of opioid treatment thatenrolled a total of 585 infants wereidentified between 1983 and 2004.Methodologic flaws were common andincluded quasirandom patient alloca-tion; substantial and often unexplaineddifferences in allocation of patientsto treatment groups; imbalances ingroup characteristics after randomi-zation; failure to mask study treat-ments; and failure to mask outcomemeasurements. In the single study thatassessed oral morphine treatmentversus supportive therapy only, 3 con-secutive Finnegan scores ≥8 promp-ted institution of the intervention.119
No significant effect of morphine wasfound on the rate of treatment failure.Oral morphine significantly increasedthe duration of treatment and thelength of hospital stay, but it did re-duce the number of days required toregain birth weight and duration ofsupportive care. Four studies com-pared treatment failures of opioids(paregoric, oral morphine, or metha-done) with phenobarbitone.8,119–121
Neither the meta-analysis nor any in-dividual study identified a significantdifference in treatment failure. Onestudy reported a lower incidence of
seizures in the opioid (paregoric)treatment group.122 No consistenttrends in secondary outcomes wereobserved, although 1 study reporteda shorter duration of therapy in thephenobarbitone compared with theparegoric treatment group,123 andanother made the opposite observa-tion when the opioid used was oralmorphine.121 Three studies individuallyand in combination reported signifi-cantly lower rates of treatment failurein infants assigned to opioid (pare-goric or methadone) compared withdiazepam therapy8,114,120 but did notdefine differences in secondary out-comes. No studies reported mortalityor neurodevelopmental outcomes.
A second Cochrane review analyzed 6trials involving 305 infants publishedbetween 1969 and 2002 in which sed-ative treatment of NAS was comparedwith a nonopioid therapy. Methodologicconcerns were similar to the opioidtreatment trials. In the sole study ofphenobarbitone versus supportive care,no difference in treatment failure wasfound, but treatment significantly in-creased the duration of therapy andhospital stay.119 A small study thatallocated infants already treated withdiluted tincture of opium (DTO) to phe-nobarbitone as a second drug versusno additional treatment identified noinfants in either group with treatmentfailure but observed significant reduc-tions in the duration of hospitalization(38 vs 79 days) and the maximal dailydose of opioid in the phenobarbitone-treated infants.124 Infants were dis-charged from the hospital once theywere no longer taking opioids. How-ever, the mean duration of phenobar-bitone treatment was 3.5 months. Of3 studies that compared phenobarbi-tone and diazepam treatment, 1 founda significantly lower rate of treat-ment failure in the phenobarbitonegroup.8,114,120 One study of phenobar-bitone versus chlorpromazine125 found
no differences in primary or second-ary outcomes.
Since 2004, a number of small studiesof varying methodologic quality havecompared pharmacologic treatments.In a prospective randomized double-masked study, Langenfeld et al126
could not identify differences in du-ration of treatment, duration of hos-pitalization, or in weight gain (g/day)in infants treated with either DTO ororal morphine drops. A retrospectivestudy found no difference in length ofhospitalization in infants with NASwho were treated with methadone ororal morphine solution, but did cor-relate higher maternal methadonedoses with longer lengths of stay.127
Ebner et al128 examined the incidenceof NAS in infants born to mothersmaintained with methadone, morphine,or buprenorphine and compared phe-nobarbital and oral morphine treat-ments in affected infants. Sixty-eightpercent of infants born to mothersmaintained on methadone requiredpharmacologic treatment at a meanage of 58 hours, compared with 82%of infants at a mean age of 33 hoursin the morphine group and 21% ofinfants at a mean age of 34 hours inthe buprenorphine group. The dura-tion of treatment was significantlyshorter for infants who received mor-phine compared with infants who weretreated with phenobarbital. A random-ized comparison trial of sublingualbuprenorphine versus neonatal opiumsolution for the treatment of NASshowed a nonsignificant reduction inlength of treatment and duration ofhospitalization in the buprenorphinegroup.129 Buprenorphine therapy waswell tolerated.
Clonidine is an α2-adrenergic receptoragonist that has been used in combi-nation with an opioid or other drug inolder children and adults to reducewithdrawal symptoms.130,131 Via a neg-ative feedback mechanism, clonidine
PEDIATRICS Volume 129, Number 2, February 2012 e549
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

reduces CNS sympathetic outflow andpalliates symptoms of autonomic over-activity such as tachycardia, hyper-tension, diaphoresis, restlessness, anddiarrhea. Cessation of clonidine treat-ment can result in a rebound of auto-nomic activity. Reported experiencewith clonidine as a primary or ad-junctive treatment of NAS is limitedbut promising. In a small case series,6 of 7 infants with NAS showed signif-icant resolution of signs when treatedwith oral clonidine.132 In a randomizeddouble-masked controlled trial, Agtheet al133 compared the efficacy andsafety of treating NAS with DTO plusoral clonidine (1 µg/kg every 3 hours)versus DTO plus placebo in 80 infantswith prenatal exposure to methadoneand/or heroin. The combination ther-apy significantly reduced the medianlength of treatment of all infants andfor infants exposed to methadone,but more infants in the DTO/clonidinegroup required resumption of DTOafter initial discontinuation. The meantotal dose of morphine over the treat-ment course was ∼60% lower in thecombination therapy group. No clini-cally significant differences in feeding,weight gain or loss, heart rate, or bloodpressure were observed. In anothercase series, oral clonidine was ad-ministered either as a primary oradjunctive therapy for the preventionor treatment of narcotic withdrawalin infants on intravenous fentanyl orinfants with antenatal exposure toopiates.134 In all cases, treatment wassuccessful and clonidine was discon-tinued without sequelae after a meanduration of 7 days. In a retrospectivecase series, infants who had evidenceof NAS attributable to antenatal meth-adone exposure had lower severityscores and required fewer days of drugtherapy and hospitalization if they hadbeen treated with a combination ofclonidine and chloral hydrate ratherthan a combination of morphine andphenobarbital.135
A recently published case series fromFrance that used a historical cohortfor a comparison has suggested thatthe treatment of NAS with the pheno-thiazine, chlorpromazine, as a singledrug may be more effective than treat-ment with morphine.136 Infants treatedwith oral morphine had significantlylonger median durations of treatmentand hospitalization in comparison withinfants treated with chlorpromazine.No adverse affects were reported.
OUTCOME
Assessment of potential long-termmorbidity specifically attributable toneonatal drug withdrawal and itstreatment is difficult to evaluate. Fewstudies have followed drug-exposedchildren beyond the first few yearsof life. Confounding variables, such asenvironment and dysfunctional care-givers, complicates the interpretationof outcomes. In a small study, devel-opmental scores on the mental indexon the Bayley Scales of Infant Devel-opment were not affected by the se-verity of withdrawal or the treatmentchosen.114 Mean scores on the BayleyScales of Infant Development weresimilar for all infants treated forwithdrawal, including those receivingphenobarbital, paregoric, or a combina-tion therapy. Scores of infants whosewithdrawal was too mild to qualify forpharmacologic intervention were alsosimilar.
Fourteen drug-exposed infants withwithdrawal-associated seizures werereported by Doberczak et al.25 Theabstinence scores for 5 of theseinfants were <7 (the cutoff for treat-ment); hence, they received no phar-macologic therapy before the onset ofseizures. Thirteen of the 14 infantswere offspring of mothers enrolled ina methadone treatment program; how-ever, the success of maternal treat-ment was not described. Of the 14infants with seizures, 12 were available
for evaluation at 1 year of age; resultsof neurologic examinations were nor-mal in 9 of the 12 infants evaluated.EEG results were abnormal in 9 neo-nates; however, subsequent EEGs for7 of 8 of these infants normalizedduring follow-up. Mean scores on theBayley Scales of Infant Developmentwere also normal by 1 year of age,similar to matched controls that weredrug exposed, but in whom withdrawal-associated seizures did not develop.24
Withdrawal-associated seizures seemto be primarily myoclonic, to respondto opiates, and to carry no increasedrisk of poor outcome. Withdrawal-associated seizures in neonates aredifferent from those associated withother causes. Based on the depressionof norepinephrine and dopamine ob-served with methadone exposure in an-imal models, withdrawal seizures arespeculated to be attributable to low-ered levels of neurotransmitters.137,138
The normalization of the EEG and nor-mal neurologic development are be-lieved to reflect recovery of normalneurotransmitter concentrations dur-ing early infancy. Bandstra et al139
have comprehensively reviewed out-comes of infants and toddlers whowere exposed prenatally to opioidsand cocaine.
MANAGEMENT OF ACQUIREDOPIOID AND BENZODIAZEPINEDEPENDENCY
One of the cornerstones in caring forcritically ill children is to provide ad-equate and safe analgesia, sedation,amnesia, and anxiolysis by using bothpharmacologic and nonpharmacologicmeasures. Pharmacologic treatmenttypically includes medications in theopioid and benzodiazepine drug clas-ses. However, if these drugs cannotsafely be discontinued within a fewdays, physical dependence on 1 orboth of these classes of medicationcan develop and manifest with signs
e550 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

and symptoms of withdrawal on acutedosage reduction or cessation oftherapy. Infants who undergo complexsurgery, who require prolonged med-ical intensive care for conditions suchas respiratory failure or persistentpulmonary hypertension, or who aresupported with extracorporeal mem-brane oxygenation (ECMO) therapy areamong those at greatest risk of ac-quired drug dependency.
Extended treatment with opioids viacontinuous intravenous infusion re-sults in drug tolerance. Even short-term opioid exposure alters thenumber and affinity of receptors in keyneuronal centers so that an escala-tion of the opioid infusion rate (whichproduces an increase in opioid plasmaconcentrations) becomes necessary toachieve the same physiologic effect.140
By itself, the development of tolerancedoes not predict physical dependencyor withdrawal.141 Cumulative expo-sure to fentanyl, quantified by the to-tal dose in milligrams per kilogram orthe number of consecutive days oftreatment, correlated with the likeli-hood of withdrawal.140,142,143 By usinga multiple logistic regression analysis,Arnold et al140 found that the durationof ECMO therapy was an even morepowerful predictor of withdrawal thanwas cumulative fentanyl exposure.Katz et al142 reported that among 23mechanically ventilated children aged1 week to 22 months (mean, 6 months)who were treated for >24 hours witha continuous fentanyl infusion, 13 of23 children (57%) developed withdrawalas defined by a Finnegan score ≥8. Inthis prospective study, a cumulative fen-tanyl exposure in excess of 2.5 mg/kgor 9 days of therapy was 100% pre-dictive of withdrawal. More recently,in a prospective study of 19 neonatestreated with fentanyl for a minimumof 24 hours, Dominquez et al143 docu-mented that a cumulative fentanyl dose≥415 µg/kg predicted withdrawal with
70% sensitivity and 78% specificityand that an infusion duration ≥8 dayswas 90% sensitive and 67% specificfor withdrawal. In adults, concomitanttreatment with neuromuscular para-lytic agents or propofol for >24 hoursalso increased the likelihood of with-drawal.144 Signs and symptoms of with-drawal from fentanyl commence within24 hours of cessation of therapy.
The refinement of pain management inchildren over the past 2 decades haswitnessed an expansion of the use ofopioids in the intensive care setting.As a result, more children have beentreated for actual or potential with-drawal symptoms as a comorbidity ofhospitalization. Fentanyl, a pure µ-opioidreceptor antagonist, has become theopioid of choice because of its rapidonset of action, short duration of ef-fect (half-life of 0.5–1 hour), excellentpotency, and minimal acute adverseeffects. However, fentanyl has not beendemonstrated to be safer or more ef-fective than morphine for the provisionof long-term analgesia. Indeed, 1 studyhas reported that patients who weretreated prospectively with a continu-ous morphine infusion during ECMOexperienced a significantly lower needfor supplemental analgesia, a lowerrate of dependency, and a shorter hos-pital stay compared with a previousgroup of patients treated with fentanylduring ECMO.145
Practitioners have employed a varietyof strategies to treat or, in high-riskpatients, to prevent signs and symp-toms of opioid withdrawal in infantsand children. Carr and Todres146
reported success with a gradual taperof the opioid infusion rate. Childrenwho had received continuous opioidinfusions for more than a week re-quired 2 to 3 weeks for completeweaning. One disadvantage of thisapproach was that intravenous accesshad to be maintained for the entirecourse of treatment. Tobias et al147
were among the first investigators todescribe treatment of opioid with-drawal by conversion to enteralmethadone. Methadone was chosenas the opioid of choice because of itsexcellent oral bioavailability (70%–100%) and long half-life (19–41hours), which allowed for long inter-vals between doses.148 In this initialreport, 3 symptomatic patients whohad been exposed to continuous orbolus opioids for up to 7 weeks weretransitioned to a methadone regimenof 0.1 mg/kg, orally, every 12 hours.Dose reduction by 10% to 20% of theinitial dose per week resulted in suc-cessful weaning in 4 to 6 weeks.
In 2000, Robertson and et al149 re-ported the outcomes of 10 children6 months to 18 years of age who hadreceived >7 days of opioids (range, 7–53 days). An amount of methadone,equipotent to the existing daily fen-tanyl or morphine dose, was deter-mined. This amount was reduced bya factor of 6 because of the longerhalf-life of methadone to calculate theinitial total daily methadone dose.Protocols specified 2 different wean-ing schedules, depending on whetherthe patient had been treated withopioids (fentanyl or morphine) for ei-ther 7 to 14 days or for >14 days.Treatment intervals were graduallylengthened from every 6 hours to ev-ery 24 hours when methadone wasdiscontinued. Outcomes of these pa-tients were compared with recentcontrol patients who had also beentreated with enteral methadone butnot under a standard protocol. Amongthe protocol patients, there were notreatment failures. Weaning was ac-complished in a median of 9 days(range, 5–10 days), which was signif-icantly less than the median of 20days (range, 9–31 days) observed inthe nonprotocol children. Concurrentuse of benzodiazepines occurred in 6of the protocol children, compared
PEDIATRICS Volume 129, Number 2, February 2012 e551
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

with 3 of the nonprotocol group, sothat the decreased taper time onprotocol was unlikely to have beenconfounded by other drug therapy.Weaning and discontinuation frombenzodiazepines were successful dur-ing the methadone taper in all pro-tocol patients.
Meyer et al150 described a protocol forrescue therapy in 29 patients 1 day to20 years of age on admission whodeveloped withdrawal during thecourse of nonstandardized tapers ofprolonged continuous fentanyl in-fusion. Withdrawal was defined as theobservation of 3 consecutive Finneganscores ≥8 obtained at 2-hour inter-vals. The daily fentanyl dose for theperiod 24 to 48 hours before with-drawal symptoms was used to calcu-late an equipotent dose of morphinesulfate. Morphine was administeredas a bolus dose every 4 hours andtitrated to effect (Finnegan scoreconsistently <8) over 12 to 24 hours.An equipotent amount of methadonewas then determined by using theeffective morphine dose. Three load-ing doses of methadone at 12-hourintervals were administered. After-ward, doses were given every 24hours and weaned by 10% per day.Ten patients were receiving concomi-tant treatment with a benzodiazepineor chloral hydrate, but these medi-cations were not weaned during themethadone taper. Twenty-five of 29patients successfully completed thistaper over 10 days. Three patientsrequired 21 days, and 1 patient died ofsepsis. Sixteen of the patients weredischarged from the hospital andcompleted methadone tapers on anoutpatient basis. Nine of the patientshad been started on clonidine duringthe phase of nonstandardized opioidweaning in unsuccessful attempts toprevent withdrawal. A subsequent ran-domized double-blind follow-up studyby the same group of investigators151
found that in a group of 37 fentanyl-treated patients, a 5-day methadonetaper was as successful as the longer10-day course (13 of 16 vs 17 of 21[not significant]) in discontinuing opi-oid infusions without causing with-drawal. In contrast to their previousstudy, a standardized taper of lor-azepam was allowed in 17 of the 37patients while on the methadoneprotocol. Only 1 of these 17 patientswho underwent dual tapers requiredrescue treatment with an increaseddose of opioids.
Several factors potentially complicatethe adoption of the protocols reportedby Robertson, Meyer, and Berens (seeTable 4) into routine neonatal clinicalpractices. Most obvious is that thesestudies were conducted in a PICUsetting; few neonates were included,and their outcomes were not sepa-rately analyzed. Other investigatorshave emphasized that the Finneganinstrument common to all 3 studieshas been validated only in term in-fants undergoing withdrawal secondaryto in utero opioid exposure.152,153
Therefore, the use of this tool mayhave underestimated withdrawal symp-tomatology in an older pediatric pop-ulation. A third concern is that opioidsand benzodiazepines are often usedconcurrently in the same patient, yetsymptoms of opioid and benzodiaze-pine withdrawal overlap to a great ex-tent. Hence, current instruments willnot reliably differentiate whether with-drawal symptoms stem from relativeopioid or benzodiazepine abstinence.153
Other scales have been proposed forchildren and are in various stages ofevaluation, including the Opioid andBenzodiazepine Withdrawal Scale,151
the Sedation Withdrawal Score,154 andthe Sophia Benzodiazepine and OpioidWithdrawal Checklist.155
At this time, no optimal pharmacologicregimen for the prevention or treat-ment of acquired opioid and/or
benzodiazepine dependency can berecommended, because the necessarycomparative studies of safety and ef-ficacy are not available.156 Hence, it iseven more incumbent on the practi-tioner to prescribe pharmacologicinterventions with the goal of achiev-ing the desired therapeutic effect byusing the fewest drugs at the lowestdoses and for the shortest durationspossible.
Nonetheless, because many criticallyill infants and children do receive treat-ment with prolonged courses of opioidsand benzodiazepines, the followingpractices are reasonable based on theavailable evidence:
1. Each clinical unit can establisha threshold level of cumulativeexposure to opioids and benzodia-zepines above which drug depen-dency can be expected to occurwith a likelihood that justifies an-ticipatory initiation of a weaningprotocol. For example, setting athreshold at a cumulative fentanylexposure of >2 mg/kg or >7 days’duration would predict a likeli-hood of dependency >50% but<100%.141,142
2. Infants with a cumulative exposureto opioids or benzodiazepines be-low the thresholds for initiation ofweaning protocols can undergoa rapid taper of these medicationsover a 24- to 48-hour period. Manysuch children will not subsequentlyexhibit drug dependency.
3. Signs and symptoms of withdrawalwill develop within 24 hours of dis-continuation or during the courseof a rapid taper of an opioid. If thisoccurs, 1 of the rescue approachesin Table 4 can be chosen as a guideto facilitate conversion to enteralmethadone management and toinitiate a weaning strategy, with 2caveats. Infants on very high dailydoses of continuous intravenousopioid may require less than the
e552 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

TABLE 4 Weaning Protocols by Using Conversion of Continuous Opioid Infusions to Enteral Methadone and for Conversion of Midazolam (Versed)Infusion to Enteral Lorazepam (Ativan)
Robertson et al149
Conversion of continuous intravenous fentanyl of 7–14 d duration to enteral methadone:1. By using the current hourly infusion rate, calculate the 24-h fentanyl dose.2. Multiply the daily fentanyl dose by a factor of 100 to calculate the equipotent amount of methadone (ratio of potencies assumed to be fentanyl: methadone =
100:1).3. Divide this amount of methadone by 6 (a correction for the longer half-life of methadone) to calculate an initial total daily dose of methadone, and on day 1
provide this amount orally in 4 divided doses every 6 h for 24 h.4. Day 2: Provide 80% of original daily dose in 3 divided oral doses every 8 h for 24 h.5. Day 3: Provide 60% of original daily dose in 3 divided oral doses every 8 h for 24 h.6. Day 4: Provide 40% of original daily dose in 2 divided oral doses every 12 h for 24 h.7. Day 5: Provide 20% of original daily dose × 1.8. Day 6: Discontinue methadone.
Conversion of continuous intravenous fentanyl greater than 14 d duration to enteral methadone:1. Repeat steps 1–2 above.2. Days 1–2: Divide the dose of methadone by 6 (a correction for the longer half-life of methadone) and on day 1 provide this amount orally in 4 divided doses
every 6 h for 48 h.3. Days 3–4: Provide 80% of original daily dose in 3 divided oral doses every 8 h for 48 h.4. Days 5–6: Provide 60% of original daily dose in 3 divided oral doses every 8 h for 48 h.5. Days 7–8: Provide 40% of original daily dose in 2 divided oral doses every 12 h for 48 h.6. Days 9–10: Provide 20% of original daily dose once per day for 48 h.7. Day 11: Discontinue methadone.
For patients on continuous intravenous morphine, proceed as above but do not multiply the daily fentanyl dose by 100, because morphine and methadone arenearly equipotent.
Meyer and Berens150
Conversion of continuous intravenous fentanyl to intermittent intravenous morphine:1. By using the target hourly infusion rate of fentanyl, calculate the 24-h fentanyl dose.2. Multiply the daily fentanyl dose by a factor of 60 to calculate the equipotent dose of morphine (ratio of potencies assumed to be fentanyl: morphine = 60:1).3. Divide the dose of morphine by 4 (correcting for the longer half-life of morphine) and on day 1 administer this amount intravenously in 6 divided doses every
4 h.4. Titrate the morphine dose for adequate effect over 12 to 24 h.
Conversion of intermittent intravenous morphine to enteral methadone:1. Multiply the dose of morphine given every 4 h by 2 (ratio of potencies assumed to be morphine: methadone = 2:1) to determine an equipotent amount of
methadone.2. Provide this amount of methadone as an oral dose every 12 h for 3 doses.3. Double this amount of methadone and provide as a single oral dose per day at bedtime.4. Provide 90% of the initial dose on day 2, 80% on day 3, etc, so that the last dose of methadone (10% of the original dose) is given on day 10.
Protocols at Wolfson Children’s Hospital, Jacksonville, Florida
Conversion of continuous intravenous fentanyl >7 d duration to enteral methadone:1. By using the current hourly infusion rate, calculate the 24-h fentanyl dose.2. Multiply the daily fentanyl dose by a factor of 100 to calculate the equipotent amount of methadone (ratio of potencies assumed to be fentanyl: methadone =
100:1).3. Divide this amount of methadone by 8–12 (a correction for the longer half-life of methadone) to calculate an initial total daily dose of methadone (not to
exceed 40 mg/day).4. Days 1–2: Provide the total daily dose of methadone orally in 4 divided doses every 6 h for 48 h. At the time of the second methadone dose, reduce the fentanyl
infusion rate to 50%; at the time of the third dose, reduce the fentanyl infusion rate to 25%; and after the fourth methadone dose, discontinue the fentanylinfusion.
5. Days 3–4: Provide 80% of original daily dose in 3 divided oral doses every 8 h for 48 h.6. Days 5–6: Provide 60% of original daily dose in 3 divided oral doses every 8 h for 48 h.7. Days 7–8: Provide 40% of original daily dose in 2 divided oral doses every 12 h for 48 h.8. Days 9–10: Provide 20% of original daily dose once per day for 48 h.9. Day 11: Discontinue methadone.
Conversion of continuous intravenous midazolam >7 d duration to enteral lorazepam:1. By using the current hourly infusion rate, calculate the 24-h midazolam dose.2. Because lorazepam is twice as potent as midazolam and has a sixfold longer half-life, divide the 24 h midazolam dose by 12 to determine the daily lorazepam
dose.3. Divide the calculated lorazepam dose by 4 and initiate every 6 h oral treatments with the intravenous product or an aliquot of a crushed tablet.4. Wean lorazepam by 10% to 20% per day. The dosage interval can also be increased gradually to every 8 h, then every 12 h, then every 24 h, and then every
other day before lorazepam is discontinued.
PEDIATRICS Volume 129, Number 2, February 2012 e553
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

calculated methadone equivalentto achieve a successful conversion.Also, the rate of weaning should beadjusted on the basis of careful con-tinuing clinical assessment. Eightypercent of children can be success-fully weaned from methadone com-pletely within 5 to 10 days.
4. Signs and symptoms of withdrawalfrom benzodiazepine therapy canbe delayed. Intravenous benzodia-zepines can be converted to orallorazepam (Table 4). The requiredtime for weaning can be expectedto be proportional to the dura-tion of intravenous benzodiazepinetreatment.
5. Infants and children at risk forwithdrawal are prudently observedin the hospital for signs and symp-toms. Each clinical unit can choose1 assessment tool and train staff tominimize individual variability inscoring.
6. Discharge from the hospital forinfants and very young children isprudently delayed until they arefree of withdrawal signs and symp-toms for a period of 24 to 48 hoursafter complete cessation of opioids.Earlier discharge of an older childcan be individualized in consider-ation of the child’s overall clinicalstatus, the home environment, andthe availability of adequate andprompt follow-up.
7. No clinical studies to date supportthe premise that initiation of cloni-dine, chloral hydrate, or continuous
intravenous low-dose naloxone157,158
during the course of continuousopioid infusions will reduce thelikelihood or severity of opioiddependency.
CLINICAL HIGHLIGHTS
1) Each nursery that cares forinfants with neonatal withdrawalshould develop a protocol thatdefines indications and proce-dures for screening for maternalsubstance abuse. In addition, eachnursery should develop and ad-here to a standardized plan forthe evaluation and comprehensivetreatment of infants at risk for orshowing signs of withdrawal.
2) Screening for maternal substanceabuse is best accomplished by us-ing multiple methods, includingmaternal history, maternal urinetesting, and testing of newbornurine and/or meconium speci-mens that are in compliance withlocal laws. The screening of bio-logical samples is an adjunct toprovide additional informationhelpful in the ongoing medicalcare of the infant. The durationof urinary excretion of most drugsis relatively short, and maternalor neonatal urinary screening onlyaddresses drug exposure in thehours immediately before urinecollection. Thus, false-negative urineresults may occur in the pres-ence of significant intrauterine
drug exposure. Although new-born meconium screening alsomay yield false-negative results,the likelihood is lower than withurinary screening. The more recentavailability of testing of umbilicalcord samples may be considereda viable screening tool, because itappears to reflect in utero expo-sures comparable to meconiumscreening.
3) Drug withdrawal should be consid-ered in the differential diagnosisfor infants in whom compatiblesigns develop. Physicians shouldbe aware of other potential diag-noses that need to be evaluatedand, if confirmed, treated appro-priately.
4) Nonpharmacologic supportivemeasures that include minimiz-ing environmental stimuli, pro-moting adequate rest and sleep,and providing sufficient caloricintake to establish weight gainshould constitute the initial ap-proach to therapy.
5) Signs of drug withdrawal can bescored by using a published ab-stinence assessment tool. Infantswith confirmed drug exposure whoare unaffected or demonstratingminimal signs of withdrawal donot require pharmacologic ther-apy. Caution should be exercisedbefore instituting pharmacologictherapy that could lengthen theduration of hospitalization and inter-fere with maternal-infant bonding.
TABLE 4 Continued
Robertson et al149
Summary of Conversion Of Intravenous Opioids to Enteral Methadone
1. Tobias et al147: Converted 2 patients on morphine (0.1–0.15 mg/kg q3h) and 1 patient on fentanyl (1–2 µg/kg every 1–2 h) to methadone at a starting dose of0.2 mg/kg per day.
2. Robertson et al149: 1 µg/kg per h fentanyl = 0.4 mg/kg per day methadone.3. Meyer and Berens150: 1 µg/kg per h fentanyl = 0.24 mg/kg per day methadone.4. Wolfson Children’s Hospital: 1 µg/kg per h fentanyl = 0.2–0.3 mg/kg per day methadone.
e554 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

Together with individualized clini-cal assessment, the serial andaccurate use of a withdrawal as-sessment tool may facilitate a de-cision about the institution ofpharmacologic therapy and there-after can provide a quantitativemeasurement that can be usedto adjust drug dosing.
6) The optimal threshold score forthe institution of pharmacologictherapy by using any of the pub-lished abstinence assessment in-struments is unknown.
7) Breastfeeding and the provisionof expressed human milk shouldbe encouraged if not contraindi-cated for other reasons.111,159
8) Pharmacologic therapy forwithdrawal-associated seizuresis indicated. Other causes of neo-natal seizures must also be eval-uated.
9) Vomiting, diarrhea, or both asso-ciated with dehydration and poorweight gain in the absence ofother diagnoses are relative indi-cations for treatment, even in theabsence of high total withdrawalscores.
10) The limited available evidencefrom controlled trials of neonatalopioid withdrawal supports theuse of oral morphine solutionand methadone when pharmaco-logic treatment is indicated.Growing evidence suggests thatoral clonidine is also effective ei-ther as a primary or adjunctivetherapy, but further prospectivetrials are warranted. Dosing regi-mens are listed in Table 5. Withrespect to other drug treatments
and clinical situations, a numberof important caveats apply. Treat-ment with paregoric is contrain-dicated, because this preparationcontains multiple opiates in addi-tion to morphine, as well as otherpotentially harmful compounds(alcohol, anise). Morphine pre-scriptions should be written asmilligrams of morphine per kilo-gram and not as milliliters of DTOper kilogram. Tincture of opiumcontains a 25-fold higher concen-tration of morphine than do avail-able oral morphine solutions;hence, it increases the likelihoodof drug error and morphine over-dose. The relative efficacy andsafety of buprenorphine for thetreatment of NAS require addi-tional comparative study. The op-timal pharmacologic treatment ofinfants who are withdrawingfrom sedatives or hypnotics is un-known. Finally, there is also insuf-ficient evidence to state whetheran infant born to a mother withmultiple drug abuse who meetscriteria for pharmacologic ther-apy of withdrawal signs is besttreated with an opioid, a barbitu-rate, a medication from anotherdrug class, or a combination ofdrugs from different classes.
11) Physicians need to be aware thatthe severity of withdrawal signs,including seizures, has not beenproven to be associated with dif-ferences in long-term outcome af-ter intrauterine drug exposure.Furthermore, treatment of drugwithdrawal may not alter thelong-term outcome.
12) Given the natural history of with-drawal, it is reasonable for neo-nates with known antenatalexposure to opioids and benzo-diazepines to be observed in thehospital for 4 to 7 days. Afterdischarge, outpatient follow-upshould occur early and includereinforcement of the education ofthe caregiver about the risk oflate withdrawal signs.
13) Neonates cared for in ICUs whohave developed tolerance to opioidsand benzodiazepines as a resultof an extended duration of treat-ment can be converted to anequivalent regimen of oral meth-adone and lorazepam. Doses maybe increased as necessary toachieve patient comfort. Thesemed-ications can then be reduced by10% to 20% of the initial dose every1 to 2 days on the basis of clinicalresponse and serial assessmentsby using a standardized neonatalabstinence instrument.
14) Significant gaps in knowledgeconcerning the optimal treatmentstrategy (including the criteriafor instituting pharmacologic ther-apy, the drug of first choice, andthe strategy for weaning) of infantswith neonatal withdrawal shouldbe addressed in well-designedrandomized controlled studiesthat are adequately powered toassess short-term outcomes andto provide for long-term follow-up.
LEAD AUTHORSMark L. Hudak, MDRosemarie C. Tan, MD, PhD
TABLE 5 Drugs Used in the Treatment of Neonatal Narcotic Withdrawal
Drug Initial Dose Increment Maximum Dose Ref. No.
Oral morphine 0.04 mg/kg every 3–4 h 0.04 mg/kg per dose 0.2 mg/kg per dose 119,121,126,133Oral methadone 0.05–0.1 mg/kg every 6 h 0.05 mg/kg per dose To effect 127Oral clonidine 0.5–1 µg/kg every 3–6 h Not studied 1 µg/kg every 3 h 132–135
PEDIATRICS Volume 129, Number 2, February 2012 e555
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

COMMITTEE ON DRUGS, 2011–2012Daniel A. C. Frattarelli, MD, ChairpersonJeffrey L. Galinkin, MDThomas P. Green, MDMark L. Hudak, MDKathleen A. Neville, MDIan M. Paul, MDJohn N. Van Den Anker, MD, PhD
FORMER COMMITTEE ON DRUGSMEMBERSMary Hegenbarth, MDMark L. Hudak, MDMatthew Knight, MDRobert E. Shaddy, MDWayne R. Snodgrass, MD, PhD
LIAISONSJohn J. Alexander, MD – Food and Drug Ad-ministrationNancy C. Chescheir, MD – American College ofObstetricians and GynecologistsJanet D. Cragan, MD – Centers for DiseaseControl and PreventionMichael J. Rieder, MD – Canadian PaediatricSociety
Adelaide Robb, MD – American Academy ofChild and Adolescent PsychiatryHari C. Sachs, MD – Food and Drug Adminis-trationAnne Zajicek, MD, PharmD – National Institutesof Health
FORMER COMMITTEE ON DRUGSLIAISONSGeorge P. Giacoia, MD
STAFFMark Del Monte, JDRaymond J. Koteras, MHA
COMMITTEE ON FETUS ANDNEWBORN, 2011–2012Lu-Ann Papile, MD, ChairpersonJill E. Baley, MDVinod K. Bhutani, MDWaldemar A. Carlo, MDJames J. Cummings, MDPraveen Kumar, MDRichard A. Polin, MDRosemarie C. Tan, MD, PhD
Kasper S. Wang, MDKristi L. Watterberg, MD
FORMER COMMITTEE ON FETUS ANDNEWBORN MEMBERSDavid H. Adamkin, MD
LIAISONSCAPT Wanda D. Barfield, MD, MPH – Centers forDisease Control and PreventionGeorge Macones, MD – American College ofObstetricians and GynecologistsAnn L. Jefferies, MD – Canadian PaediatricSocietyRosalie O. Mainous, PhD, RNC, NNP – NationalAssociation of Neonatal NursesTonse N. K. Raju, MD, DCH – National Institutes ofHealth
FORMER COMMITTEE ON FETUS ANDNEWBORN LIAISONSWilliam H. Barth, Jr, MD
STAFFJim Couto, MA
REFERENCES
1. Results From the 2009 National Survey onDrug Use and Health: Volume I. Summaryof National Findings (Office of AppliedStudies, NSDUH Series H-38A, HHS Publi-cation No 10-4856Findings). Rockville, MD:Substance Abuse and Mental HealthServices Administration; 2010
2. Bada HS, Das A, Bauer CR, et al. Low birthweight and preterm births: etiologicfraction attributable to prenatal drugexposure. J Perinatol. 2005;25(10):631–637
3. Campolongo P, Trezza V, Palmery M, Tra-bace L, Cuomo V. Developmental exposureto cannabinoids causes subtle and en-during neurofunctional alterations. IntRev Neurobiol. 2009;85:117–133
4. Burns L, Mattick RP. Using population datato examine the prevalence and correlatesof neonatal abstinence syndrome. DrugAlcohol Rev. 2007;26(5):487–492
5. Kellogg A, Rose CH, Harms RH, Watson WJ.Current trends in narcotic use in preg-nancy and neonatal outcomes. Am JObstet Gynecol. 2011;204:259.e1–e4
6. Harper RG, Solish GI, Purow HM, Sang E,Panepinto WC. The effect of a methadonetreatment program upon pregnant heroinaddicts and their newborn infants. Pedi-atrics. 1974;54(3):300–305
7. Fricker HS, Segal S. Narcotic addiction,pregnancy, and the newborn. Am J DisChild. 1978;132(4):360–366
8. Madden JD, Chappel JN, Zuspan F, GumpelJ, Mejia A, Davis R. Observation andtreatment of neonatal narcotic with-drawal. Am J Obstet Gynecol. 1977;127(2):199–201
9. Ostrea EM, Chavez CJ, Strauss ME. A studyof factors that influence the severity ofneonatal narcotic withdrawal. J Pediatr.1976;88(4 pt 1):642–645
10. Rementería JL, Bhatt K. Withdrawalsymptoms in neonates from intrauterineexposure to diazepam. J Pediatr. 1977;90(1):123–126
11. Athinarayanan P, Pierog SH, Nigam SK,Glass L. Chloriazepoxide withdrawal in theneonate. Am J Obstet Gynecol. 1976;124(2):212–213
12. Bleyer WA, Marshall RE. Barbiturate with-drawal syndrome in a passively addictedinfant. JAMA. 1972;221(2):185–186
13. Desmond MM, Schwanecke RP, Wilson GS,Yasunaga S, Burgdorff I. Maternal barbi-turate utilization and neonatal withdrawalsymptomatology. J Pediatr. 1972;80(2):190–197
14. Pierog S, Chandavasu O, Wexler I. With-drawal symptoms in infants with the fetal
alcohol syndrome. J Pediatr. 1977;90(4):630–633
15. Nichols MM. Acute alcohol withdrawalsyndrome in a newborn. Am J Dis Child.1967;113(6):714–715
16. Eyler FD, Behnke M, Garvan CW, Woods NS,Wobie K, Conlon M. Newborn evaluationsof toxicity and withdrawal related toprenatal cocaine exposure. NeurotoxicolTeratol. 2001;23(5):399–411
17. Bauer CR, Langer JC, Shankaran S, et al.Acute neonatal effects of cocaine expo-sure during pregnancy. Arch PediatrAdolesc Med. 2005;159(9):824–834
18. Chasnoff IJ, Bussey ME, Savich R, StackCM. Perinatal cerebral infarction andmaternal cocaine use. J Pediatr. 1986;108(3):456–459
19. Fulroth R, Phillips B, Durand DJ. Perinataloutcome of infants exposed to cocaineand/or heroin in utero. Am J Dis Child.1989;143(8):905–910
20. Chiriboga CA, Bateman DA, Brust JC,Hauser WA. Neurologic findings in neo-nates with intrauterine cocaine exposure.Pediatr Neurol. 1993;9(2):115–119
21. Hadeed AJ, Siegel SR. Maternal cocaineuse during pregnancy: effect on thenewborn infant. Pediatrics. 1989;84(2):205–210
e556 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

22. King TA, Perlman JM, Laptook AR, RollinsN, Jackson G, Little B. Neurologic mani-festations of in utero cocaine exposure innear-term and term infants. Pediatrics.1995;96(2 pt 1):259–264
23. Brazelton TB. Neonatal Behavioral As-sessment Scale. Clinics in DevelopmentalMedicine. No 88. 2nd ed. Philadelphia, PA:JB Lippincott Co; 1984
24. Tan-Laxa MA, Sison-Switala C, RintelmanW, Ostrea EM Jr,. Abnormal auditorybrainstem response among infants withprenatal cocaine exposure. Pediatrics.2004;113(2):357–360
25. Doberczak TM, Shanzer S, Cutler R, SenieRT, Loucopoulos JA, Kandall SR. One-yearfollow-up of infants with abstinence-associated seizures. Arch Neurol. 1988;45(6):649–653
26. Tronick EZ, Frank DA, Cabral H, MirochnickM, Zuckerman B. Late dose-responseeffects of prenatal cocaine exposure onnewborn neurobehavioral performance.Pediatrics. 1996;98(1):76–83
27. Smith L, Yonekura ML, Wallace T, BermanN, Kuo J, Berkowitz C. Effects of prenatalmethamphetamine exposure on fetalgrowth and drug withdrawal symptoms ininfants born at term. J Dev Behav Pediatr.2003;24(1):17–23
28. Billing L, Eriksson M, Steneroth G, Zetter-ström R. Predictive indicators for ad-justment in 4-year-old children whosemothers used amphetamine duringpregnancy. Child Abuse Negl. 1988;12(4):503–507
29. Cernerud L, Eriksson M, Jonsson B, Sten-eroth G, Zetterström R. Amphetamine ad-diction during pregnancy: 14-year follow-up of growth and school performance.Acta Paediatr. 1996;85(2):204–208
30. Alwan S, Friedman JM. Safety of selectiveserotonin reuptake inhibitors in preg-nancy. CNS Drugs. 2009;23(6):493–509
31. Dahl ML, Olhager E, Ahlner J. Paroxetinewithdrawal syndrome in a neonate. Br JPsychiatry. 1997;171:391–392
32. Sanz EJ, De-las-Cuevas C, Kiuru A, Bate A,Edwards R. Selective serotonin reuptakeinhibitors in pregnant women and neo-natal withdrawal syndrome: a databaseanalysis. Lancet. 2005;365(9458):482–487
33. Chambers CD, Johnson KA, Dick LM, FelixRJ, Jones KL. Birth outcomes in pregnantwomen taking fluoxetine. N Engl J Med.1996;335(14):1010–1015
34. Galbally M, Lewis AJ, Lum J, Buist A. Se-rotonin discontinuation syndrome follow-ing in utero exposure to antidepressantmedication: prospective controlled study.Aust N Z J Psychiatry. 2009;43(9):846–854
35. Haddad PM, Pal BR, Clarke P, Wieck A,Sridhiran S. Neonatal symptoms followingmaternal paroxetine treatment: serotonintoxicity or paroxetine discontinuationsyndrome? J Psychopharmacol. 2005;19(5):554–557
36. Nordeng H, Lindemann R, Perminov KV,Reikvam A. Neonatal withdrawal syn-drome after in utero exposure to selectiveserotonin reuptake inhibitors. Acta Pae-diatr. 2001;90(3):288–291
37. Boyer EW, Shannon M. The serotoninsyndrome. N Engl J Med. 2005;352(11):1112–1120
38. Isbister GK, Dawson A, Whyte IM, Prior FH,Clancy C, Smith AJ. Neonatal paroxetinewithdrawal syndrome or actually seroto-nin syndrome? Arch Dis Child Fetal Neo-natal Ed. 2001;85(2):F147–F148
39. Laine K, Heikkinen T, Ekblad U, Kero P.Effects of exposure to selective serotoninreuptake inhibitors during pregnancy onserotonergic symptoms in newborns andcord blood monoamine and prolactinconcentrations. Arch Gen Psychiatry. 2003;60(7):720–726
40. Austin MP. To treat or not to treat: ma-ternal depression, SSRI use in pregnancyand adverse neonatal effects. PsycholMed. 2006;36(12):1663–1670
41. Gentile S. On categorizing gestational,birth, and neonatal complications follow-ing late pregnancy exposure to anti-depressants: the prenatal antidepressantexposure syndrome. CNS Spectr. 2010;15(3):167–185
42. Oberlander TF, Grunau RE, Fitzgerald C,Papsdorf M, Rurak D, Riggs W. Pain re-activity in 2-month-old infants after pre-natal and postnatal serotonin reuptakeinhibitor medication exposure. Pediatrics.2005;115(2):411–425
43. Nordeng H, Spigset O. Treatment with se-lective serotonin reuptake inhibitors inthe third trimester of pregnancy: effectson the infant. Drug Saf. 2005;28(7):565–581
44. De las Cuevas C, Sanz EJ. Safety of selec-tive serotonin reuptake inhibitors inpregnancy. Curr Drug Saf. 2006;1(1):17–24
45. Weissman AM, Levy BT, Hartz AJ, et al.Pooled analysis of antidepressant levelsin lactating mothers, breast milk, andnursing infants. Am J Psychiatry. 2004;161(6):1066–1078
46. Fortinguerra F, Clavenna A, Bonati M.Psychotropic drug use during breast-feeding: a review of the evidence. Pedi-atrics. 2009;124(4). Available at: www.pediatrics.org/cgi/content/full/124/4/e547
47. Somogyi AA, Barratt DT, Coller JK. Phar-macogenetics of opioids. Clin PharmacolTher. 2007;81(3):429–444
48. Jones HE, Kaltenbach K, Heil SH, et al.Neonatal abstinence syndrome aftermethadone or buprenorphine exposure.N Engl J Med. 2010;363(24):2320–2331
49. Zelson C, Rubio E, Wasserman E. Neonatalnarcotic addiction: 10 year observation.Pediatrics. 1971;48(2):178–189
50. Kandall SR, Gartner LM. Late presentationof drug withdrawal symptoms in new-borns. Am J Dis Child. 1974;127(1):58–61
51. Lejeune C, Simmat-Durand L, Gourarier L,Aubisson S, ; Groupe d’Etudes Grossesseet Addictions (GEGA). Prospective multi-center observational study of 260 infantsborn to 259 opiate-dependent mothers onmethadone or high-dose buprenophinesubstitution. Drug Alcohol Depend. 2006;82(3):250–257
52. Steg N. Narcotic withdrawal reactions inthe newborn. AMA J Dis Child. 1957;94(3):286–288
53. Schindler SD, Eder H, Ortner R, Rohr-meister K, Langer M, Fischer G. Neonataloutcome following buprenorphine main-tenance during conception and through-out pregnancy. Addiction. 2003;98(1):103–110
54. Kayemba-Kay’s S, Laclyde JP. Buprenor-phine withdrawal syndrome in newborns:a report of 13 cases. Addiction. 2003;98(11):1599–1604
55. Lacroix I, Berrebi A, Chaumerliac C,Lapeyre-Mestre M, Montastruc JL, Damase-Michel C. Buprenorphine in pregnantopioid-dependent women: first results ofa prospective study. Addiction. 2004;99(2):209–214
56. Herzlinger RA, Kandall SR, Vaughan HG Jr,.Neonatal seizures associated with nar-cotic withdrawal. J Pediatr. 1977;91(4):638–641
57. Pinto F, Torrioli MG, Casella G, Tempesta E,Fundarò C. Sleep in babies born tochronically heroin addicted mothers. Afollow up study. Drug Alcohol Depend.1988;21(1):43–47
58. van Baar AL, Fleury P, Soepatmi S, UlteeCA, Wesselman PJ. Neonatal behavior af-ter drug dependent pregnancy. Arch DisChild. 1989;64(2):235–240
59. Desmond MM, Wilson GS. Neonatal absti-nence syndrome: recognition and di-agnosis. Addict Dis. 1975;2(1–2):113–121
60. Prenner BM. Neonatal withdrawal syn-drome associated with hydroxyzine hy-drochloride. Am J Dis Child. 1977;131(5):529–530
PEDIATRICS Volume 129, Number 2, February 2012 e557
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

61. Feld LH, Negus JB, White PF. Oral mid-azolam preanesthetic medication in pe-diatric outpatients. Anesthesiology. 1990;73(5):831–834
62. Harper RG, Solish G, Feingold E, Gersten-Woolf NB, Sokal MM. Maternal ingestedmethadone, body fluid methadone, andthe neonatal withdrawal syndrome. Am JObstet Gynecol. 1977;129(4):417–424
63. Strauss ME, Andresko M, Stryker JC,Wardell JN. Relationship of neonatalwithdrawal to maternal methadone dose.Am J Drug Alcohol Abuse. 1976;3(2):339–345
64. Doberczak TM, Kandall SR, Wilets I. Neo-natal opiate abstinence syndrome in termand preterm infants. J Pediatr. 1991;118(6):933–937
65. Doberczak TM, Kandall SR, Friedmann P.Relationship between maternal metha-done dosage, maternal-neonatal metha-done levels, and neonatal withdrawal.Obstet Gynecol. 1993;81(6):936–940
66. Rosen TS, Pippenger CE. Disposition ofmethadone and its relationship to sever-ity of withdrawal in the newborn. AddictDis. 1975;2(1–2):169–178
67. Dashe JS, Sheffield JS, Olscher DA, ToddSJ, Jackson GL, Wendel GD. Relationshipbetween maternal methadone dosage andneonatal withdrawal. Obstet Gynecol.2002;100(6):1244–1249
68. Liu AJ, Jones MP, Murray H, Cook CM,Nanan R. Perinatal risk factors for theneonatal abstinence syndrome in infantsborn to women on methadone mainte-nance therapy. Aust N Z J Obstet Gynaecol.2010;50(3):253–258
69. Brown HL, Britton KA, Mahaffey D, BrizendineE, Hiett AK, Turnquest MA. Methadonemaintenance in pregnancy: a reappraisal.Am J Obstet Gynecol. 1998;179(2):459–463
70. Mack G, Thomas D, Giles W, Buchanan N.Methadone levels and neonatal with-drawal. J Paediatr Child Health. 1991;27(2):96–100
71. Berghella V, Lim PJ, Hill MK, Cherpes J,Chennat J, Kaltenbach K. Maternal meth-adone dose and neonatal withdrawal. AmJ Obstet Gynecol. 2003;189(2):312–317
72. Kuschel CA, Austerberry L, Cornwell M,Couch R, Rowley RS. Can methadoneconcentrations predict the severity ofwithdrawal in infants at risk of neonatalabstinence syndrome? Arch Dis Child Fe-tal Neonatal Ed. 2004;89(5):F390–F393
73. Seligman NS, Almario CV, Hayes EJ, DysartKC, Berghella V, Baxter JK. Relationshipbetween maternal methadone dose atdelivery and neonatal abstinence syn-drome. J Pediatr. 2010;157(3):428–433, e1
74. Cleary BJ, Donnelly J, Strawbridge J, et al.Methadone dose and neonatal abstinencesyndrome—systematic review and meta-analysis. Addiction. 2010;105(12):2071–2084
75. Drozdick J, III, Berghella V, Hill M, Kalten-bach K. Methadone trough levels inpregnancy. Am J Obstet Gynecol. 2002;187(5):1184–1188
76. Lipsitz PJ. A proposed narcotic with-drawal score for use with newborninfants. A pragmatic evaluation of its ef-ficacy. Clin Pediatr (Phila). 1975;14(6):592–594
77. Finnegan LP, Kron RE, Connaughton JF,Emich JP. Assessment and treatment ofabstinence in the infant of the drug-dependent mother. Int Clin PharmacolBiopharm. 1975;12(1–2):19–32
78. Dysart K, Hsieh HC, Kaltenbach K, Green-span JS. Sequela of preterm versus terminfants born to mothers on a methadonemaintenance program: differential courseof neonatal abstinence syndrome. J Peri-nat Med. 2007;35(4):344–346
79. Johnson K, Gerada C, Greenough A.Treatment of neonatal abstinence syn-drome. Arch Dis Child Fetal Neonatal Ed.2003;88(1):F2–F5
80. Chasnoff IJ, Burns WJ, Schnoll SH, BurnsKA. Cocaine use in pregnancy. N Engl JMed. 1985;313(11):666–669
81. Choo RE, Huestis MA, Schroeder JR, ShinAS, Jones HE. Neonatal abstinence syn-drome in methadone-exposed infants isaltered by level of prenatal tobacco ex-posure. Drug Alcohol Depend. 2004;75(3):253–260
82. Gibbs J, Newson T, Williams J, DavidsonDC. Naloxone hazard in infant of opioidabuser. Lancet. 1989;2(8655):159–160
83. Frank DA, Zuckerman BS, Amaro H, et al.Cocaine use during pregnancy: preva-lence and correlates. Pediatrics. 1988;82(6):888–895
84. Chasnoff IJ, Burns KA, Burns WJ. Cocaineuse in pregnancy: perinatal morbidity andmortality. Neurotoxicol Teratol. 1987;9(4):291–293
85. Mitchell M, Sabbagha RE, Keith L, Mac-Gregor S, Mota JM, Minoque J. Ultrasonicgrowth parameters in fetuses of motherswith primary addiction to cocaine. Am JObstet Gynecol. 1988;159(5):1104–1109
86. Cregler LL, Mark H. Medical complicationsof cocaine abuse. N Engl J Med. 1986;315(23):1495–1500
87. Chasnoff IJ, Griffith DR, MacGregor S,Dirkes K, Burns KA. Temporal patterns ofcocaine use in pregnancy. Perinatal out-come. JAMA. 1989;261(12):1741–1744
88. Cocaine abuse: implications for preg-nancy. ACOG Committee opinion: Commit-tee on Obstetrics: Maternal and FetalMedicine number 81—March 1990. Int JGynaecol Obstet. 1991;36(2):164–166
89. Horowitz RM. Drug use in pregnancy: totest, to tell—legal implications for thephysician. Semin Perinatol. 1991;15(4):324–330
90. Chasnoff IJ. Prenatal substance exposure:maternal screening and neonatal identi-fication and management. NeoReviews.2003;4(9):e228–e235
91. Chasnoff IJ, Neuman K, Thornton C, CallaghanMA. Screening for substance use in preg-nancy: a practical approach for the pri-mary care physician. Am J Obstet Gynecol.2001;184(4):752–758
92. Chan D, Klein J, Koren G. New methods forneonatal drug screening. NeoReviews.2003;4(9):e236–e244
93. Beauman SS. Identification and manage-ment of neonatal abstinence syndrome.J Infus Nurs. 2005;28(3):159–167
94. Reinarz SE, Ecord JS. Drug-of-abuse test-ing in the neonate. Neonatal Netw. 1999;18(8):55–61
95. Ostrea EM, Jr,Brady MJ, Parks PM, AsensioDC, Naluz A. Drug screening of meconiumin infants of drug-dependent mothers: analternative to urine testing. J Pediatr.1989;115(3):474–477
96. Ryan RM, Wagner CL, Schultz JM, et al.Meconium analysis for improved identifi-cation of infants exposed to cocaine inutero. J Pediatr. 1994;125(3):435–440
97. Ostrea EM, Jr,Knapp DK, Tannenbaum L,et al. Estimates of illicit drug use duringpregnancy by maternal interview, hairanalysis, and meconium analysis. J Pediatr.2001;138(3):344–348
98. Vinner E, Vignau J, Thibault D, et al. Neo-natal hair analysis contribution to es-tablishing a gestational drug exposureprofile and predicting a withdrawal syn-drome. Ther Drug Monit. 2003;25(4):421–432
99. Montgomery D, Plate C, Alder SC, Jones M,Jones J, Christensen RD. Testing for fetalexposure to illicit drugs using umbilicalcord tissue vs meconium. J Perinatol.2006;26(1):11–14
100. American Academy of Pediatrics, Com-mittee on Drugs. Neonatal drug with-drawal. Pediatrics. 1998;101(6):1079–1088
101. Finnegan LP. Neonatal abstinence. In: Nel-son NM, ed. Current Therapy in Neonatal–Perinatal Medicine. 2nd ed. Toronto,Ontario: BC Decker Inc; 1990
102. Sarkar S, Donn SM. Management of neo-natal abstinence syndrome in neonatal
e558 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

intensive care units: a national survey.J Perinatol. 2006;26(1):15–17
103. Green M, Suffet F. The Neonatal NarcoticWithdrawal Index: a device for the im-provement of care in the abstinence syn-drome. Am J Drug Alcohol Abuse. 1981;8(2):203–213
104. Zimmermann-Baer U, Nötzli U, Rentsch K,Bucher HU. Finnegan neonatal abstinencescoring system: normal values for first 3days and weeks 5-6 in non-addictedinfants. Addiction. 2010;105(3):524–528
105. Hill RM, Desmond MM. Management of thenarcotic withdrawal syndrome in the neo-nate. Pediatr Clin North Am. 1963;10:67–86
106. Wilson GS. Somatic growth effects ofperinatal addiction. Addict Dis. 1975;2(1–2):333–345
107. Abdel-Latif ME, Pinner J, Clews S, Cooke F,Lui K, Oei J. Effects of breast milk on theseverity and outcome of neonatal absti-nence syndrome among infants of drug-dependent mothers. Pediatrics. 2006;117(6). Available at: www.pediatrics.org/cgi/content/full/117/6/e1163
108. Isemann B, Meinzen-Derr J, Akinbi H. Ma-ternal and neonatal factors impactingresponse to methadone therapy in infantstreated for neonatal abstinence syn-drome. J Perinatol. 2011;31(1):25–29
109. Jansson LM, Choo R, Velez ML, et al.Methadone maintenance and breastfeed-ing in the neonatal period. Pediatrics.2008;121(1):106–114
110. Jansson LM, Choo R, Velez ML, Lowe R,Huestis MA. Methadone maintenance andlong-term lactation. Breastfeed Med. 2008;3(1):34–37
111. Jansson LM, ; Academy of BreastfeedingMedicine Protocol Committee. ABM clini-cal protocol #21: guidelines for breast-feeding and the drug-dependent woman.Breastfeed Med. 2009;4(4):225–228
112. Bays J. The care of alcohol- and drug-affected infants. Pediatr Ann. 1992;21(8):485–495
113. O’Grady MJ, Hopewell J, White MJ. Man-agement of neonatal abstinence syn-drome: a national survey and review ofpractice. Arch Dis Child Fetal Neonatal Ed.2009;94(4):F249–F252
114. Kaltenbach K, Finnegan LP. Neonatal ab-stinence syndrome, pharmacotherapy anddevelopmental outcome. Neurobehav Tox-icol Teratol. 1986;8(4):353–355
115. Kron RE, Litt M, Eng D, Phoenix MD, Fin-negan LP. Neonatal narcotic abstinence:effects of pharmacotherapeutic agentsand maternal drug usage on nutritivesucking behavior. J Pediatr. 1976;88(4 pt1):637–641
116. Schiff D, Chan G, Stern L, et al. Diazepam(Valium) for neonatal narcotic with-drawal: a question of safety. Pediatrics.1972;49(6):928–930
117. Osborn DA, Jeffery HE, Cole MJ. Opiatetreatment for opiate withdrawal in new-born infants. Cochrane Database Syst Rev.2005;(3):CD002059
118. Osborn DA, Jeffery HE, Cole MJ. Sedativesfor opiate withdrawal in newborn infants.Cochrane Database Syst Rev. 2005;(3):CD002053
119. Khoo KT. The Effectiveness of Three Treat-ment Regimens Used in the Managementof Neonatal Abstinence Syndrome [thesisfor PhD]. Melbourne, Australia: Universityof Melbourne; 1995
120. Finnegan LP, Michael H, Leifer B, Desai S.An evaluation of neonatal abstinencetreatment modalities. NIDA Res Monogr.1984;49:282–288
121. Jackson L, Ting A, McKay S, Galea P,Skeoch C. A randomised controlled trial ofmorphine versus phenobarbitone for neo-natal abstinence syndrome. Arch Dis ChildFetal Neonatal Ed. 2004;89(4):F300–F304
122. Kandall SR, Doberczak TM, Mauer KR,Strashun RH, Korts DC. Opiate v CNS de-pressant therapy in neonatal drug absti-nence syndrome. Am J Dis Child. 1983;137(4):378–382
123. Carin I, Glass L, Parekh A, Solomon N,Steigman J, Wong S. Neonatal methadonewithdrawal. Effect of two treatment regi-mens. Am J Dis Child. 1983;137(12):1166–1169
124. Coyle MG, Ferguson A, Lagasse L, Oh W,Lester B. Diluted tincture of opium (DTO)and phenobarbital versus DTO alone forneonatal opiate withdrawal in term in-fants. J Pediatr. 2002;140(5):561–564
125. Kahn EJ, Neumann LL, Polk GA. The courseof the heroin withdrawal syndrome innewborn infants treated with phenobar-bital or chlorpromazine. J Pediatr. 1969;75(3):495–500
126. Langenfeld S, Birkenfeld L, Herkenrath P,Müller C, Hellmich M, Theisohn M. Therapyof the neonatal abstinence syndrome withtincture of opium or morphine drops.Drug Alcohol Depend. 2005;77(1):31–36
127. Lainwala S, Brown ER, Weinschenk NP,Blackwell MT, Hagadorn JI. A retrospectivestudy of length of hospital stay in infantstreated for neonatal abstinence syndromewith methadone versus oral morphinepreparations. Adv Neonatal Care. 2005;5(5):265–272
128. Ebner N, Rohrmeister K, Winklbaur B, et al.Management of neonatal abstinence syn-drome in neonates born to opioid main-
tained women. Drug Alcohol Depend. 2007;87(2–3):131–138
129. Kraft WK, Gibson E, Dysart K, et al. Sub-lingual buprenorphine for treatment ofneonatal abstinence syndrome: a random-ized trial. Pediatrics. 2008;122(3). Avail-able at: www.pediatrics.org/cgi/content/full/122/3/e601
130. Gold MS, Redmond DE, Jr,Kleber HD. Clo-nidine blocks acute opiate-withdrawalsymptoms. Lancet. 1978;2(8090):599–602
131. Yaster M, Kost-Byerly S, Berde C, Billet C.The management of opioid and benzodi-azepine dependence in infants, children,and adolescents. Pediatrics. 1996;98(1):135–140
132. Hoder EL, Leckman JF, Poulsen J, et al.Clonidine treatment of neonatal narcoticabstinence syndrome. Psychiatry Res.1984;13(3):243–251
133. Agthe AG, Kim GR, Mathias KB, et al. Clo-nidine as an adjunct therapy to opioidsfor neonatal abstinence syndrome: a ran-domized, controlled trial. Pediatrics. 2009;123(5). Available at: www.pediatrics.org/cgi/content/123/5/e849
134. Leikin JB, Mackendrick WP, Maloney GE,et al. Use of clonidine in the preventionand management of neonatal abstinencesyndrome. Clin Toxicol (Phila). 2009;47(6):551–555
135. Esmaeili A, Keinhorst AK, Schuster T, BeskeF, Schlösser R, Bastanier C. Treatment ofneonatal abstinence syndrome with clo-nidine and chloral hydrate. Acta Paediatr.2010;99(2):209–214
136. Mazurier E, Cambonie G, Barbotte E, GrareA, Pinzani V, Picaud JC. Comparison ofchlorpromazine versus morphine hydro-chloride for treatment of neonatal absti-nence syndrome. Acta Paediatr. 2008;97(10):1358–1361
137. Slotkin TA, Whitmore WL, Salvaggio M,Seidler FJ. Perinatal methadone addictionaffects brain synaptic development ofbiogenic amine systems in the rat. Life Sci.1979;24(13):1223–1229
138. McGinty JF, Ford DH. Effects of prenatalmethadone on rat brain catecholamines.Dev Neurosci. 1980;3(4–6):224–234
139. Bandstra ES, Morrow CE, Mansoor E,Accornero VH. Prenatal drug exposure:infant and toddler outcomes. J Addict Dis.2010;29(2):245–258
140. Arnold JH, Truog RD, Scavone JM, FentonT. Changes in the pharmacodynamic re-sponse to fentanyl in neonates duringcontinuous infusion. J Pediatr. 1991;119(4):639–643
141. Arnold JH, Truog RD, Orav EJ, Scavone JM,Hershenson MB. Tolerance and dependence
PEDIATRICS Volume 129, Number 2, February 2012 e559
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

in neonates sedated with fentanyl duringextracorporeal membrane oxygenation.Anesthesiology. 1990;73(6):1136–1140
142. Katz R, Kelly HW, Hsi A. Prospective studyon the occurrence of withdrawal in criti-cally ill children who receive fentanyl bycontinuous infusion. Crit Care Med. 1994;22(5):763–767
143. Dominguez KD, Lomako DM, Katz RW, KellyHW. Opioid withdrawal in critically illneonates. Ann Pharmacother. 2003;37(4):473–477
144. Cammarano WB, Pittet JF, Weitz S, Schlo-bohm RM, Marks JD. Acute withdrawalsyndrome related to the administration ofanalgesic and sedative medications inadult intensive care unit patients. CritCare Med. 1998;26(4):676–684
145. Franck LS, Vilardi J, Durand D, Powers R.Opioid withdrawal in neonates after con-tinuous infusions of morphine or fentanylduring extracorporeal membrane oxygen-ation. Am J Crit Care. 1998;7(5):364–369
146. Carr DB, Todres ID. Fentanyl infusion andweaning in the pediatric intensive careunit: toward science-based practice. CritCare Med. 1994;22(5):725–727
147. Tobias JD, Schleien CL, Haun SE. Metha-done as treatment for iatrogenic narcoticdependency in pediatric intensive careunit patients. Crit Care Med. 1990;18(11):1292–1293
148. Anand KJ. Pharmacological approaches tothe management of pain in the neonatalintensive care unit. J Perinatol. 2007;27(suppl 1):S4–S11
149. Robertson RC, Darsey E, Fortenberry JD,Pettignano R, Hartley G. Evaluation of anopiate-weaning protocol using methadone
in pediatric intensive care unit patients.Pediatr Crit Care Med. 2000;1(2):119–123
150. Meyer MM, Berens RJ. Efficacy of an en-teral 10-day methadone wean to preventopioid withdrawal in fentanyl-tolerant pe-diatric intensive care unit patients.Pediatr Crit Care Med. 2001;2(4):329–333
151. Berens RJ, Meyer MT, Mikhailov TA, et al. Aprospective evaluation of opioid weaningin opioid-dependent pediatric critical care pa-tients. Anesth Analg. 2006;102(4):1045–1050
152. Franck LS, Naughton I, Winter I. Opioid andbenzodiazepine withdrawal symptoms inpaediatric intensive care patients. In-tensive Crit Care Nurs. 2004;20(6):344–351
153. Ista E, van Dijk M, Gamel C, Tibboel D, deHoog M. Withdrawal symptoms in childrenafter long-term administration of seda-tives and/or analgesics: a literature re-view. “Assessment remains troublesome”.Intensive Care Med. 2007;33(8):1396–1406
154. Cunliffe M, McArthur L, Dooley F. Managingsedation withdrawal in children who un-dergo prolonged PICU admission afterdischarge to the ward. Paediatr Anaesth.2004;14(4):293–298
155. Ista E, van Dijk M, Gamel C, Tibboel D, deHoog M. Withdrawal symptoms in criti-cally ill children after long-term admin-istration of sedatives and/or analgesics:a first evaluation. Crit Care Med. 2008;36(8):2427–2432
156. Simons SH, Anand KJ. Pain control: opioiddosing, population kinetics and side-effects.Semin Fetal Neonatal Med. 2006;11(4):260–267
157. Cheung CL, van Dijk M, Green JW, TibboelD, Anand KJ. Effects of low-dose naloxoneon opioid therapy in pediatric patients:
a retrospective case-control study. In-tensive Care Med. 2007;33(1):190–194
158. Darnell CM, Thompson J, Stromberg D,Roy L, Sheeran P. Effect of low-dose nal-oxone infusion on fentanyl requirementsin critically ill children. Pediatrics. 2008;121(5). Available at: www.pediatrics.org/cgi/content/full/121/5/e1363
159. Gartner LM, Morton J, Lawrence RA, et al;American Academy of Pediatrics Sectionon Breastfeeding. Breastfeeding and theuse of human milk. Pediatrics. 2005;115(2):496–506
160. Milhorn HT Jr,. Pharmacologic manage-ment of acute abstinence syndromes. AmFam Physician. 1992;45(1):231–239
161. McGowan JD, Altman RE, Kanto WP Jr,.Neonatal withdrawal symptoms afterchronic maternal ingestion of caffeine.South Med J. 1988;81(9):1092–1094
162. Musa AB, Smith CS. Neonatal effects ofmaternal clomipramine therapy. Arch DisChild. 1979;54(5):405
163. Rumack BH, Walravens PA. Neonatal with-drawal following maternal ingestion ofethchlorvynol (Placidyl). Pediatrics. 1973;52(5):714–716
164. Reveri M, Pyati SP, Pildes RS. Neonatalwithdrawal symptoms associated withglutethimide (Doriden) addiction in themother during pregnancy. Clin Pediatr(Phila). 1977;16(5):424–425
165. Desmond MM, Rudolph AJ, Hill RM, Clag-horn JL, Dreesen PR, Burgdorff I. Behav-ioral alterations in infants born tomothers on psychoactive medicationduring pregnancy. In: Farrell G, ed. Con-genital Mental Retardation. Austin, TX:University of Texas Press; 1969:235–244
e560 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2011-3212; originally published online January 30, 2012; 2012;129;e540Pediatrics
COMMITTEE ON FETUS AND NEWBORNMark L. Hudak, Rosemarie C. Tan, THE COMMITTEE ON DRUGS and THE
Neonatal Drug Withdrawal
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/129/2/e540.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/129/2/e540.full.hfree at:This article cites 160 articles, 45 of which can be accessed
Subspecialty Collections
cs_and_toxicologyhttp://pediatrics.aappublications.org/cgi/collection/therapeutiTherapeutics & Toxicology
_on_fetus__newbornhttp://pediatrics.aappublications.org/cgi/collection/committeeCommittee on Fetus & Newborn
_on_drugshttp://pediatrics.aappublications.org/cgi/collection/committeeCommittee on Drugsthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Health Internetwork on March 2, 2012pediatrics.aappublications.orgDownloaded from