Embed Size (px)
Citation preview

NOC
PTteaaocbtt4rd
tgcatcttff
DA
1d
avigated Total Knee Arthroplasty as anption in Cases of Extra-Articular Deformity
arlos A. Higuera, MD, Alison K. Klika, MS, John Bottros, MD, and Wael K. Barsoum, MD
The use of corrective osteotomy of angular deformity and total knee arthroplasty hastraditionally been considered the treatment of choice for patients with arthritis and ipsilat-eral extra-articular deformity. We believe there is sufficient evidence that computer-as-sisted navigation can be used in lieu of this approach to recreate an acceptable mechanicalaxis in patients with distorted anatomical landmarks for total knee arthroplasty. The use ofthis technology in extra-articular deformity provides an option that decreases the need formultiple operations and gives better guidance in restoring the normal lower limb mechan-ical axis. This article describes the use of this technique and other potential applications.Semin Arthro 20:35-37 © 2009 Published by Elsevier Inc.
KEYWORDS TKA, navigation, extra-articular deformity
oSn
ntvntsttat
icaslt
ftepdei
roper axial and rotational alignments are fundamental inthe successful outcome of total knee arthroplasty (TKA).1,2
o accomplish proper alignment, the traditional instrumen-ation used in TKA employs the anatomical axis of the lowerxtremity. This method imposes a challenge when an extra-rticular deformity in the femur and or tibia is present. Teternd coworkers3 showed the influence of the tibial deformityn the accuracy of intra- and extramedullary tibial alignmentutting systems. More specifically, when a significant tibialowing deformity is present in the coronal or sagittal plane,he passage of the intramedullary (IM) rod parallel to theibial mechanical axis is impossible. Cuts with greater than a° error done using IM alignment showed that the IM guideod directly led to nonmechanically neutral cuts when passedown the middle of the tibial shaft in the coronal plane.3
There are some series in the literature that describe variousechniques for managing this problem. Krackow and Holt-rewe4 described the use of extensive soft tissue balancing inonjunction with a minimally constrained TKA for the man-gement of severe valgus deformity of the knee after highibial osteotomy. Lonner and coworkers5 used simultaneousorrective osteotomy and TKA in 11 patients with knee ar-hritis and extra-articular deformity of the femur secondaryo fracture malunion or rickets. The osteotomy was per-ormed at the level of the fracture site or the metaphysis. Theyollowed these patients for an average of 46 months and
epartment of Orthopaedic Surgery, Cleveland Clinic, Cleveland, OH, USA.ddress reprint requests to Wael K. Barsoum, MD, Department of Ortho-
paedic Surgery, Cleveland Clinic, 9500 Euclid Avenue, A41, Cleveland,
tOH 44195. E-mail: [email protected]045-4527/09/$-see front matter © 2009 Published by Elsevier Inc.oi:10.1053/j.sart.2008.11.012
btained a significant postoperative improvement in Kneeociety scores, with a mechanical axis restored to within 2° oformal.5
While the results in those series are excellent, the simulta-eous osteotomy and TKA is a complex procedure with mul-iple challenges. In cases in which the tibial anatomy is se-erely distorted, even a custom-made prosthesis may beeeded.6 This technique is difficult to reproduce, requireswo separate procedures to be successful, and the amount ofurgical time and soft tissue dissection is substantial. Addi-ionally, it necessitates protected weight bearing postopera-ively that limits rehabilitation. This technique is also associ-ted with significant complications, including nonunion athe osteotomy site and arthrofibrosis.7
Wang and Wang8 proposed an alternative technique usingntra-articular bone resection and soft-tissue balancing inonjunction with TKA in patients with arthritis of the kneessociated with extra-articular deformity. They enlisted twopecific rules to approximate the amount of the intra-articu-ar bone needed to be resected to perform a TKA and correcthe limb deformity.
The first rule applies to extra-articular deformities on theemoral side and consists of drawing a line from the center ofhe femoral head to the center of the knee using a lowerxtremity full-length weight-bearing radiograph. A seconderpendicular line is then drawn through the femoral con-yles. If the perpendicular line does not cross the insertion ofither of the collateral ligaments, then they use this as anndication to resect intra-articular bone and balance the soft
issue using an IM guide, if possible. However, they admit35

mrpeoatwrgo
adadT2psR1ftdp
utcctpd
arrtaaa3datjrttTTwtl
tt
tcugatpiaaifi
sRmdoefch
FttiB
36 C.A. Higuera et al
ore frequent use of an extramedullary guide. Also, a cor-ective extra-articular osteotomy is performed if the antici-ated femoral condylar resection violated the insertion ofither the medial or the lateral collateral ligaments. The sec-nd rule is for extra-articular deformities on the tibial sidend consists of drawing a line from the medullary canal onhe distal part of the tibia to the knee joint. If the line passesithin the tibial condyle, a TKA with intra-articular bone
esection is usually performed using an extramedullaryuide. A corrective osteotomy is indicated if the line passesutside the tibial condyles.This technique was used in 15 patients with knee arthritis
nd extra-articular deformity. Seven patients had a femoraleformity with an average angle of 15.1° in the coronal planend 8.1° in the sagittal plane and 8 patients had a tibialeformity with an average angle of 19° in the coronal plane.he average follow-up they reported was 38 months (range,4-60 months). The average Knee Society score (KSS) im-roved from 22 to 92 points and the average KSS functioncore improved from 28 to 83 points at the last follow-up.ange of motion (ROM) improved from an average of 77° to04°, and the average mechanical axis of the knee improvedrom 22° of varus to essentially a normal 0.3° of varus.8 Thisechnique is limited when there is an extra-articular varuseformity of �20° in the femur and �30° in the coronallane in the tibia.Computer-assisted navigation (CAN) has proven to be a
seful tool in the restoration of the mechanical alignment ofhe lower limb in TKA.9,10 The use of CAN is an alternative inases of severe extra-articular deformity.11,12 The versatility ofurrent imageless CAN technology and the reproducibility ofhe results make this technique a useful alternative in TKArocedures in patients with knee arthritis and extra-articulareformity.At our own institution, Bottros and coworkers12 described
series of seven patients (9 knees) with knee arthritis and aadiographic femoral extra-articular deformity that was cor-ected using imageless CAN to perform TKA. Standing an-eroposterior (AP) radiographs were obtained both preoper-tively and 3 months postoperatively, and the mechanicalxis deviation was measured using the method of Morelandnd coworkers.13 With this method, the deviation is based on-ft standing radiographs with calculations derived from a linerawn from the center of the femoral head to the center of the anklend compared with a line drawn from the center of the knee tohe center of the femoral head or to the center of the ankleoint. The femoral anatomical axis was measured using APadiographs by first drawing a line from the greater trochan-er to the middle of the distal femur. A second line was drawnangent to the articular surface of the distal femoral condyles.he angle at the intersection of these two lines was measured.he tibial anatomical axis was measured using a line drawnithin the shaft of the tibia and another line drawn along the
ibial baseplate. The angle at the intersection of these twoines was then measured.12
Computer-assisted navigation (the Stryker Navigation Sys-em) was used for each arthroplasty and was calibrated using
he center of the hip and ankle as reference points to establish rhe mechanical axis. All arthroplasties were performed ac-ording to the manufacturer’s guide. This navigation systemses a surface mapping guide for the placement of the cuttinguides and asks the surgeon to map the AP axis of the femurnd the medial and lateral epicondyles to determine rota-ional alignment. Tracking devices are affixed to a universalositioning block, and the pointing instrument allows these
nstruments to be tracked and displayed in real time. Thisllows for intraoperative evaluation of lower limb alignmentnd kinematics. The components used in all of these casesnclude the Stryker Duracon cruciate substituting system inour cases and the Stryker Triathlon cruciate retaining systemn five cases (Stryker Orthopaedics, Mahwah, NJ).12
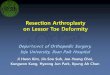
The patients’ clinical postoperative outcomes were as-essed using KSS, including knee and function scores, andOM. The average follow-up was 19 months (range, 12-30onths). Postoperatively, the mechanical axis deviated me-ially by a mean of 1.38 � 0.98° (Fig. 1).12 Early patientutcomes showed a significant increase in the average preop-rative to postoperative KSS from 62 to 92, function scoresrom 52 to 83, and ROM from 4-74° to 0.6-98°.12 In someases, using a conventional femoral IM rod technique wouldave been impossible secondary to the femoral deformity,
igure 1 Postoperative anteroposterior standing radiograph of a pa-ient with distal femur extra-articular deformity corrected with aotal knee arthroplasty using computer-assisted navigation, includ-ng mechanical axes (A) and joint line (B). In the series reported byottros and coworkers,12 this patient represents the most accurate
estoration of the mechanical axis, measuring 3° valgus.
ucparooncIgwadtva
eactTtawacchnCwmtaw
amtcadaceo
oc
stio
cpst
R
1
1
1
1
1
1
Using navigation for TKA deformity 37
nless it was first corrected with an osteotomy. The use ofonventional techniques may have increased the chances of aoor clinical outcome such as aberrant patellar tracking,symmetric patellofemoral joint contact, incorrect valgus/va-us positioning in flexion, difficulties in rotational alignmentf the tibia in extension, and the possibility of anterior fem-ral notching.14 It is important to note, in all of these cases,avigation was not used for femoral rotation alignment be-ause of the rotational malalignment inherent in the femurs.nstead, femoral rotation was based on balancing the flexionap to the tibial cut surface. The tibial rotation was confirmedith the use of CAN in all of the cases. This technique is
menable to most cases of knee arthritis with extra-articulareformity, but likely not all cases. It is especially amenable tohose on the femoral side because the deformity is usually inarus and the femur is a longer bone, which allows for moredaptability to correct the deformity.
Other authors have similar results in correcting the lowerxtremity alignment using CAN in TKA cases with extra-rticular deformities.11,15 Klein and coworkers11 described aase series of five patients whose TKA surgeries used naviga-ion to compensate for extra-articular femoral deformities.hey were able to restore near-collinear mechanical axes of
he tibia and femur in all patients. Fehring and coworkers15
ddressed whether CAN surgery could properly align TKAhen use of traditional instrumentation was not possible or
ppropriate. They identified 16 patients (18 knees) whoould not be treated using traditional instrumentation be-ause of posttraumatic femoral deformity, retained femoralardware, a history of osteomyelitis, or severe cardiopulmo-ary disease. The overall mechanical axis of the limb usingAN surgery was acceptable in 16 of 17 knees. One patientith a major posttraumatic biplanar deformity had an overallechanical axis in 4° of varus.15 Computer-assisted naviga-
ion was helpful in these difficult situations in which accuratelignment remained essential, yet traditional instrumentationas not applicable.In summary, traditional techniques used to address knee
rthritis with extra-articular deformity are difficult and haveany potential complications. Computer-assisted navigation
echnology is a safe, potential alternative for this subset ofases with reproducibility and good outcomes. Computer-ssisted navigation is used under the premise that, based onigital mapping, the alignment of the components is moreccurate and reliable. It can safely be used to improve me-hanical alignment and clinical function without the use ofxtramedullary femoral alignment tools or a femoral osteot-my.However, this procedure may not be applicable to all cases
f extra-articular deformity. Deformity that compromises the
ollateral ligaments or is very close to the joint line would beignificantly more challenging to correct through the jointhan above the joint. Alternatively, deformity near the prox-mal end of the femur would be challenging to correct with ansteotomy, also necessitating a more complicated procedure.While CAN may help to restore the mechanical axis in
ases with significant deformity, it is not a substitute forroper surgical technique, judgment, or experience. Furthertudies are needed to establish the specific indications of thisechnique and the long-term outcome of this intervention.
eferences1. Berger RA, Rubash HE, Seel MJ, et al: Determining the rotational align-
ment of the femoral component in total knee arthroplasty using theepicondylar axis. Clin Orthop Relat Res 286:40-47, 1993
2. Wasielewski RC, Galante JO, Leighty RM, et al: Wear patterns on re-trieved polyethylene tibial inserts and their relationship to technicalconsiderations during total knee arthroplasty. Clin Orthop Relat Res299:31-43, 1994
3. Teter KE, Bregman D, Colwell CW Jr: Accuracy of intramedullary ver-sus extramedullary tibial alignment cutting systems in total knee ar-throplasty. Clin Orthop Relat Res 321:106-110, 1995
4. Krackow KA, Holtgrewe JL: Experience with a new technique for man-aging severely overcorrected valgus high tibial osteotomy at total kneearthroplasty. Clin Orthop Relat Res 258:213-224, 1990
5. Lonner JH, Siliski JM, Lotke PA: Simultaneous femoral osteotomy andtotal knee arthroplasty for treatment of osteoarthritis associated withsevere extra-articular deformity. J Bone Joint Surg Am 82:342-348,2000
6. Windsor RE, Insall JN, Sculco TP: Bone grafting of tibial defects inprimary and revision total knee arthroplasty. Clin Orthop Relat Res205:132-137, 1986
7. Cameron HU, Welsh RP: Potential complications of total knee replace-ment following tibial osteotomy. Orthop Rev 17:39-43, 1988
8. Wang JW, Wang CJ: Total knee arthroplasty for arthritis of the kneewith extra-articular deformity. J Bone Joint Surg Am 84:1769-1774,2002
9. Bathis H, Perlick L, Tingart M, et al: Alignment in total knee arthro-plasty: A comparison of computer-assisted surgery with the conven-tional technique. J Bone Joint Surg Br 86:682-687, 2004
0. Chauhan SK, Scott RG, Breidahl W, et al: Computer-assisted kneearthroplasty versus a conventional jig-based technique: A randomized,prospective trial. J Bone Joint Surg Br 86:372-377, 2004
1. Klein GR, Austin MS, Smith EB, et al: Total knee arthroplasty usingcomputer-assisted navigation in patients with deformities of the femurand tibia. J Arthroplasty 21:284-288, 2006
2. Bottros J, Klika AK, Lee HH, et al: The use of navigation in total kneearthroplasty for patients with extra-articular deformity. J Arthroplasty23:74-78, 2008
3. Moreland JR, Bassett LW, Hanker GJ: Radiographic analysis of the axialalignment of the lower extremity. J Bone Joint Surg Am 69:745-749,1987
4. Anouchi YS, Whiteside LA, Kaiser AD, et al: The effects of axial rota-tional alignment of the femoral component on knee stability and patel-lar tracking in total knee arthroplasty demonstrated on autopsy speci-mens. Clin Orthop Relat Res 287:170-177, 1993
5. Fehring TK, Mason JB, Moskal J, et al: When computer-assisted kneereplacement is the best alternative. Clin Orthop Relat Res 452:132-136,
2006
![Total Knee Arthroplasty in Severe Valgus Osteoarthritis ...downloads.hindawi.com/journals/crior/2017/9301017.pdf · arthroplasty (TKA) [1]. Valgus deformity is classified in 3 grades:gradeI(80%ofcases)withanaxialdeviationof6–](https://img.dokumen.tips/doc/110x75/606355869091dd26a33d8da2/total-knee-arthroplasty-in-severe-valgus-osteoarthritis-arthroplasty-tka-1.jpg)