Embed Size (px)
Citation preview

1404
Natural History and Age at Onset of Hereditary Breast Cancer Henry T. Lynch, MD, Patrice Watson, PhD, Theresa A. Conway, BSN, and Jane F. Lynch, BSN
Hereditary breast cancer (HBC) is noteworthy for certain unique facets of its natural history and heterogeneity. In- terfamily heterogeneity in age at initial breast cancer diagnosis was investigated in 217 family members with HBC. The mean age at diagnosis was 44.9 years (standard deviation f 12.5 years). A one-way analysis of variance in ages at diagnosis, using the family as a random effect factor, indicated that between-family differences were significant (P < 0.002) and accounted for approximately 18% of the variance in ages at diagnosis. A subset of fami- lies with HBC was characterized by an extraordinarily early onset of breast cancer. A knowledge of the natural history of HBC with particular attention to age at onset allows for the development of more accurately targeted surveillance, genetic counselling, and management strate- gies. Cancer 1992; 69:1404-1407.
Hereditary breast cancer (HBC) is believed to account for between 5% and 9% of the total breast cancer bur- den.',' The natural history of HBC differs strikingly from that of its sporadic counterpart by several objec- tive parameters, particularly age at d i a g n ~ s i s ~ - ~ and fre- quency of bilaterality.4,6,7 Claus et al.' found that age at diagnosis of breast cancer was the strongest indicator of the presence of a possible genetic subtype of breast cancer.
We describe interfamily heterogeneity in age at diagnosis of breast cancer in HBC and discuss the im- portance of this knowledge for surveillance strategies.
Material and Methods
Ascertainment
This study was approved by the institutional review board of Creighton University. Patients with breast
From the Department of Preventive Medicine/Public Health, Creighton University School of Medicine, Omaha, Nebraska.
Supported by a grant from the National Cancer Institute (1 R01 48802) and from the Council for Tobacco Research (1297CR2).
The authors thank Diane Stanley for technical assistance. Address for reprints: Henry T. Lynch, MD, Department of Pre-
ventive Medicine, Creighton University School of Medicine, Califor- nia at 24th Street, Omaha, NE 67178.
Accepted for publication June 11, 1991.
cancer were either referred through the oncology clinic at Creighton University or by their physicians, or volun- teered on their own. The patients were interviewed with particular attention given to their family history of cancer. Formal, signed permission was obtained that enabled us to contact first-degree and second-degree relatives. These relatives received letters explaining the study, along with questionnaires. Returned question- naires were used for cross-checking the genealogy and medical information and for updating and extending the pedigree. Signed permission from living patients with cancer or their legal next of kin allowed the release of primary medical and pathologic documents. When extensive information on family history was obtained showing a high frequency of breast cancer in a pattern consistent with HBC, the family was added to the HBC family registry. The number of affected women was evaluated in light of the number of women in the fam- ily. An early diagnosis of breast cancer, bilateral breast cancer, or associated tumors such as ovarian cancer was taken as evidence in favor of HBC.
Description of Families
In this report, HBC is operationally defined as a pattern of cancer distribution within a particular family that is suggestive of mendelian segregation of an autosomal dominant disease susceptibility gene.'s9 This definition also embraces the concept of tumor All of the cases in the current study came from families where the predominant tumor was in the breast, in- cluding hereditary site-specific breast cancer' and he- reditary breast/ovary cancer syndrome." Families with evidence of other hereditary syndromes, where breast cancer was an integral but not predominant tumor (e.g., the sarcoma, breast cancer, brain tumors, leukemia, lung, laryngeal, adrenal cortical carcinoma [SBLA] syn- drome),' were excluded. No patients were known to have Cowden's disease.'
Procedures
All patients with breast cancer who were members of the HBC families were included in this study if medical

Natural History and Age at Onset of HBCILynch et al . 1405
and/or pathology records verifying their initial breast cancer diagnosis were available. All diagnoses were pri- mary carcinomas of the breast. All families in the HBC family registry at Creighton University were included if at least two breast cancer cases in the family could be so verified. Because the distribution of age at diagnosis was positively skewed, log-transformed ages were used to normalize the distribution. The random effects model for one-way analysis of variance was used to evaluate whether significant differences in age existed among families and to determine what proportion of variance in age at diagnosis was attributable to interfa- mily differences. Correlation/regression enabled us to determine how well the age at diagnosis of one family member could be predicted from the mean age at diag- nosis of the other family members. Analysis was carried out with the use of the SPSS-X program (SPSS Inc., Chicago, IL).I3
Results
Within 57 HBC families, 484 women had a diagnosis of breast cancer. Of these cases, 267 were excluded be- cause documentation of the initial diagnosis was lack-
85
80
75
70
85
60
E [13 55 0 z C3 50 s c3 45
2 w 40 0
35
30
25
20
t
f
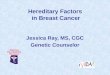
ing. Two hundred seventeen cases of HBC were in- cluded in the analysis. The mean age at diagnosis was 44.9 years (range, 22 to 83 years). An analysis of vari- ance for interfamily differences showed that there was significant variation among families in age at diagnosis (F[56,160] = 1.86; P < 0.002); approximately 18% of the variance in ages at diagnosis was accounted for by in- terfamily differences. The variation within and be- tween families is seen in Figure 1.
Figure 1 shows a positive skew in the data, and the Kolmogorov-Smirnov goodness of fit test supported this viewpoint (z = 1.24; P < 0.10). The log-trans- formed ages were more symmetrically distributed (z = 0.64; P < 0.90). Bartlett’s test was applied to the transformed data within the analysis of variance, and the result was nearly significant (F = 1.25; P = 0.10).
Correlation coefficients between the age at diagno- sis of a selected family member and the mean age at diagnosis of all other family members were found to be dependent on the selection process. We observed a sig- nificant but weak association between the age of a ran- domly selected family member and the mean age of other family members (r = 0.25; P < 0.03), and between the age of the family member with the most recent diagnosis and the mean age of the other family
T
I
t I ;II FAMILIES (ORDERED BY MEAN AGE AT DIAGNOSIS)
Figure 1. Age a t first diagnosis of breast cancer in 217 patients from 57 HBC families. Untransformed ages are shown to facilitate interpretation. Each vertical line represents one family; these are ordered by the mean age at diagnosis in the family. Ages in individual cases are represented by crossbars on the vertical lines. The horizontal line indicates the mean age at diagnosis in the family.

1406 CANCER March 25, 2992, Volume 69, No. 6
members (r = 0.25; P < 0.03). However, we observed a stronger association between the age in the youngest case in the family and the age in the other cases (r = 0.54; P < 0.0001).
We explored the relationship between other vari- ables and age at diagnosis. Eight of the 57 families were classified as breast/ovarian carcinoma syndrome be- cause at least 2 cases of verified ovarian cancer occurred in women with breast cancer and their first-degree rela- tives; 16 families had just one case of ovarian cancer. No significant differences in the mean age of the family members at breast cancer diagnosis were observed among these three groups (P > 0.4). Age at diagnosis was found to be strongly associated with year of birth (r = - 0.71) as a result of the relatively narrow span of years of diagnosis among the eligible cases. An analysis of variance of the residuals from the regression of (log) age on year of birth produced a result similar to that of the analysis of (log) ages (F = 1.6; P < 0.02). Age at diagnosis was not associated with year of diagnosis (r = 0.05). In many families, one member who was much older than the other members with disease also would have disease. We thought that this might be, in some cases, a case of sporadic breast cancer occumng coinci- dentally in members of an HBC family. If so, exclusion of these cases should increase the proportion of vari- ance due to interfamily differences. Thus, we per- formed our analyses again, this time excluding the old- est age at diagnosis in each family. However, no sub- stantial difference resulted (data not shown). Finally, we observed that 20 families had only 2 eligible cases. A subsequent analysis of the data from the 37 larger fami- lies produced a similar result (e.g., in the analysis of variance for interfamily differences: F = 2.1; P < 0.002).
Discussion
These observations increase our understanding of the natural history of HBC and may improve surveillance/ management strategies. We previously discussed an HBC subset that is noteworthy for a remarkably young age at ~ n s e t . ~ , ~ , ' ~ We investigated the relationship be- tween age at onset of breast cancer in 328 consecutive patients from our oncology clinic and breast cancer in- cidence and age at onset in their female relatives. We found that a family history of early onset of breast cancer was associated with a higher risk of early onset of breast cancer. A family history of early onset of breast cancer occurred more frequently among young (< 40 years of age) patients with breast cancer than older (2 40 years of age) patients with breast cancer (P < 0.001; odds ratio = 23). This relationship was particu- larly evident when the analysis was restricted to the
patients with breast cancer who were members of HBC families (P < 0.001; odds ratio = 44).
Mettlin et d . 1 5 recently reported a similar phenome- non in the general population. In their case-control study, they found that an elevated risk for early onset of breast cancer was not associated with a positive family history of breast cancer in general, but more specifically with a family history of early onset of breast cancer.
In the current study, we extended our previous re- sults in an attempt to estimate the size of the effect of interfamily differences. Because familial aggregation in age at diagnosis had been observed only in the families classified as HBC or probable HBC (and not in non- HBC cases with a positive family history) in our pre- vious study, we focused our attention on HBC. To esti- mate the size of the effect, we studied a greater number of hereditary families and larger families and included more cases of breast cancer with documented ages for the patients. These features of the HBC family registry enabled us to estimate the proportion of the variance in ages that could be attributed to interfamily differences, and the "predictive" value of the mean age at diagnosis in the family. Our results reinforce our previous obser- vations of interfamily heterogeneity that is consistent with a subset of extraordinarily young age of ~ n s e t . ~ - ~ Intrafamily variation also is notable. Figure 1 shows that cases of very young age at diagnosis occurred in many of those families that concomitantly showed an older mean age at diagnosis. These findings indicate that this older age at diagnosis of breast cancer does not preclude HBC or accompanying cases of early onset.
Ideally, surveillance strategies should be based on experimental results showing significant improvement in survival (or other endpoint) in the group being ob- served. However, such results are not available for women younger than 40 years of age. Thus, we recom- mend strategies that reflect the age of patients at the onset of HBC. Mammography for all patients at high risk of HBC should be initiated by 25 years of age, and performed annually thereafter. However, in those fami- lies with a history of breast cancer diagnoses in the third decade of life, we recommend that mammography be initiated by 20 years of age. Breast self-examination and semiannual physician examination is important. We believe that compliance with these recommendations will be improved through educating women about the natural history of HBC several years before they are old enough for mammography. Mammography has not been thoroughly studied in asymptomatic young women. Although it may be difficult to interpret the mammograms of these young women (compared with older women) because of increased breast density, re- cent evidence indicates that grouped microcalcifica- tions, as the sole indicator of malignancy, occur with

Natural History and Age at Onset of HBCILynch et al . 1407
greater frequency in these young women and can be detected in the presence of increased parenchymal den- sity.'6-'8
Our findings should be interpreted cautiously. Our data on age at diagnosis of breast cancer included only verified cases, which limited the number of cases avail- able for analysis. In certain families, the ages of only two patients could be verified. However, further analy- ses that excluded the smallest families produced essen- tially the same results. By relying on cases that were documented by pathology reports and medical records, the accuracy of age values was insured. However, this created an artifactual association between year of birth and age at diagnosis because of the relatively narrow span of years from which such documentation was available. This raised the possibility that structural dif- ferences among families could account for the inter- family heterogeneity in age at diagnosis. For example, consider a family including a sibship of women born in the 1920s and their daughters who were born in the 1950s and compare it with an identical family with women born in the 1910s and 1940s. If diagnoses can only be verified (and included) if they occurred after 1960, then eligible cases from the second family would tend to involve older women even if the ages at diagno- sis were identical in the two families. However, an anal- ysis of ages that had been statistically corrected for the effect of year of birth still showed significant interfa- mily differences. Finally, we stress that interfamily het- erogeneity does not necessarily have a genetic basis. One must also consider secular and structural differ- ences and environmental heterogeneity among fami- lies.
Preliminary results from genetic linkage studies on HBC families" have indicated that even within a small group of families prone to the same types of tumors, genetic heterogeneity may be observed. Five breast/ ovarian cancer families were studied for linkage to the CMM86 marker on chromosome 17q, and significant linkage (P < 0.003) and heterogeneity (P < 0.025) were observed. We believe that such findings support the view that HBC is a heterogeneous entity. Careful docu- mentation of the clinical phenotype within each family, and study of variability between families, may assist in defining etiologically distinct subsets.
Many questions remain unanswered concerning our observations of heterogeneity of age at diagnosis. Several issues need to be resolved: if extraordinarily young age at diagnosis of breast cancer is a specific marker of hereditary susceptibility to breast cancer in a single patient, whether age at onset differs among the various HBC syndromes, and whether the hypothe- sized extraordinarily early onset of the HBC variant
is distinguishable by specific pathologic/molecular markers. Answers to such questions may improve both treatment for women at high risk of breast cancer and understanding of the phenomenon of breast cancer sus- ceptibility.
References
1. Lynch HT. Genetics and Breast Cancer. New York: Van Nos- trand Reinhold, 1981;9.
2. Lynch HT, Lynch JF. Breast cancer genetics in an oncology clinic: 328 consecutive patients. Cancer Genet Cytogeriet 1986;
3. Lynch HT, Guirgis HA, Brodkey F et al. Early age of onset in familial breast cancer: Genetic and cancer control implications. Arch Surg 1976; 111:126-131.
4. Lynch HT, Watson P, Conway T, Fitzsimmons ML, Lynch J. Breast cancer family history as a risk factor for early onset breast cancer. Breast Cancer Res Treat 1988; 11:263-267. Lynch HT, Conway T, Fitzgibbons RJ Jr et al. Age of onset hetero- geneity in hereditary breast cancer: Minimal clues for diagnosis. Breast Caricer Res Treat 1988; 12275-285.
6. Anderson DE, Badzioch MD. Risk of familial cancer. Cancer
7. Hams RE, Lynch HT, Guirgis HA. Familial breast cancer: Risk to the contralateral breast. / Not/ Cancer Inst 1978; 60:955-960.
8. Claus EB, Risch NJ, Thompson WD. Age at onset as an indicator of familial risk of breast cancer. Am / Epiderriiol 1990; 131:961- 972.
9. Go RCP, King MC, Bailey-Wilson J, Elston RC, Lynch HT. Ge- netic epidemiology of breast and associated cancers in high risk families: Parts 1 and 11. Natl Cancer Inst 1983; 71:455-467.
10. Lynch HT, Krush A], Lemon HM, Kaplan AR, Condit PT, Bot- tomley RH. Tumor variations in families with breast cancer.
11. Lynch HT, Harris RE, Guirgis HA, Maloney K, Carmody L, Lynch IF. Familial association of breast/ovarian cancer. Cancer
12. Lynch HT, Mulcahy GM, Hams RE et a[. Genetic and pathologic findings in a kindred with hereditary sarcoma, breast cancer, brain tumors, leukemia, lung, laryngeal, and adrenal cortical carcinoma. Cancer 1978; 41:2055-2064.
13. SPSS lnc. SPSS-X Information Analysis System, Release 2.1, 1986. Chicago: SPSS Inc.
14. Lynch HT, Conway T, Watson P, Schreiman J, Fitzgibbons RJ Jr. Extremely early onset hereditary breast cancer (HBC): Surveil- lance/management implications. N Engl / Med 1988; 73:97-100.
15. Mettlin C, Groghan I, Natarajan N, Lane W. The association of age and familial risk in a case-control study of breast cancer. Am / Epidemiol 1990; 131:973-983.
16. Hermann G, Janus C, Schwartz IS et a/ . Occult malignant breast lesions in 114 patients: Relationship to age and the presence of microcalcifications. Radiology 1988; 169:321-324.
17. Meyer JE, Kopans DB, Oot R. Breast cancer visualized by mam- mography in patients under 35. Radiology 1983; 147:93-94.
18. Sickles EA. Mammographic features of 300 consecutive nonpal- pable breast cancers. AIR 1986; 146:661-663.
19. Narod SA, Feunteun J, Lynch HT et a/ . Familial breast-ovarian cancer locus on chromosome 17q12-q23. Lancet 1991; 33832- 83.
23:369-372.
5.
1985; 561383-387.
/AMA 1972; 220:1631-1635.
1978; 41~1543-1548.