Embed Size (px)
Citation preview

Plan for the national Greek Health Examination Survey
Prepared by the: Hellenic
Health Foundation
In collaboration with the
Hellenic Center for Diseases Control and Prevention (HCDCP)
Hellenic Ministry of Health and Social Solidarity (MOH)

This manual has been prepared by national experts from Greece. Antonia Trichopoulou with her team from the Hellenic Health Foundation (http://www.hhf-greece.gr/) wrote this manual based on experience gained during the EHES Pilot Project 2010-2011.
The EHES Pilot Project has received funding from the European Commission / DG Sanco. The views expressed here are those of the authors and they do not represent the Commission’s official position.
More information about the EHES Pilot Project: http://www.ehes.info

Table of Contents Introduction .......................................................................................................................................... 6 1. Survey planning and management ................................................................................................... 8
1.1 Survey process............................................................................................................................ 8
1.2 Aims and objectives of the survey ............................................................................................. 8 1.3 Implementing EHES standards in the Greek national HES ....................................................... 9 1.4. Survey management .................................................................................................................. 9
1.4.1. Personnel requirements....................................................................................................... 9 1.4.2. Organization structure ...................................................................................................... 10
2. Target population and sample size................................................................................................. 12
2.1 Target population ..................................................................................................................... 12 2.2 Sample size............................................................................................................................... 12 2.3 The EHIS definition ................................................................................................................. 13
2.4 People living in institutions ...................................................................................................... 13 3. Sampling procedures...................................................................................................................... 14
3.1 General considerations ............................................................................................................. 14
3.2 Sampling frames....................................................................................................................... 15 3.3 Sampling design for Stage 1..................................................................................................... 16
3.3.1 Creating the PSUs.............................................................................................................. 16 3.3.2 Size of the PSUs ................................................................................................................ 17
3.3.3 Stratification of the PSUs .................................................................................................. 17 3.3.4 Sample sizes at Stage 1...................................................................................................... 17 3.3.5 Inclusion probabilities for the PSUs .................................................................................. 19
3.3.6 Sampling ............................................................................................................................ 19 3.3.7 Distribution of PSUs over time ......................................................................................... 19
3.4 Sampling design for Stage 2..................................................................................................... 19
4. Legal and ethical issues.................................................................................................................. 23 4.1 Legislation and guidelines........................................................................................................ 23 4.2 Role of ethics committees - Ethical approval........................................................................... 23
4.3 Data confidentiality – Data protection ..................................................................................... 24 4.4 Informed consent ...................................................................................................................... 24
5. Selecting the measurements ........................................................................................................... 25
5.1 Criteria for selecting the measurements ................................................................................... 25 5.2 The core measurements ............................................................................................................ 26
5.2.1 The core physical assessments .......................................................................................... 26 5.2.2 The core analyses of blood samples (clinical assessments)............................................... 27
5.2.3 The core questions ............................................................................................................. 27
1
2
6. Timing of the fieldwork and order of measurements..................................................................... 29 6.1 Periodicity ................................................................................................................................ 29 6.2 Length and time of year for the fieldwork ............................................................................... 29
6.3 Weekdays and time of day ....................................................................................................... 29 6.4 Order of measurements ............................................................................................................ 30
6.4.1 Clinical measurements....................................................................................................... 30
6.4.2 Questionnaires and interviews ........................................................................................... 30 7. Selecting the examination site........................................................................................................ 31
7.1 The Greek HES examination sites............................................................................................ 31
7.2 Additional options .................................................................................................................... 31 8. Questionnaire design and administration ....................................................................................... 33
8.1 Questionnaire design ................................................................................................................ 33
8.1.1 Language and wording ...................................................................................................... 33 8.1.2 Recall bias.......................................................................................................................... 33 8.1.3 Order of the questions........................................................................................................ 33
8.1.4 Length of the questionnaire ............................................................................................... 34 8.1.5 Layout of the questionnaire ............................................................................................... 34
8.2 Questionnaire administration ................................................................................................... 34 8.2.1 Interviews .......................................................................................................................... 34
8.2.2 Use of proxies ................................................................................................................... 35 9. Selection of the fieldwork staff ...................................................................................................... 36
9.1. General principles and criteria for recruitment ....................................................................... 36
9.2. Professional groups ................................................................................................................. 37 9.3 Fieldwork teams ....................................................................................................................... 37
10. Blood samples and laboratory analyses ....................................................................................... 38
10.1 Selection of the national laboratory........................................................................................ 38 10.2 Selection of measurements on blood samples ........................................................................ 38 10.3 Blood collection ..................................................................................................................... 38
10.4 Critical issues concerning the blood collection ...................................................................... 39 10.4.1 Fasting before the sample collection ............................................................................... 39 10.4.2 Position of the participant and details on arterial puncture ............................................. 39
10.4.3 Use of a tourniquet .......................................................................................................... 39 10.4.4 Effects of seasonal variation ............................................................................................ 39 10.4.5 Effect of physical training ............................................................................................... 39
10.5 Equipment for drawing blood samples................................................................................... 40 10.5.1 Type and order of blood tubes ......................................................................................... 40 10.5.2 Equipment for handling, transfer and storage of blood samples ..................................... 40

3
10.6 Processing, storage and transport of blood samples............................................................... 40 10.6.1 Processing ........................................................................................................................ 41 10.6.2 Storage of serum, plasma, whole blood and buffy coat tubes ......................................... 41
10.6.3 Transport.......................................................................................................................... 41 10.7 Guidelines on laboratory performance ................................................................................... 42
10.7.1 Performance of laboratories............................................................................................. 42
10.7.2 Standardization of analytical data.................................................................................... 42 10.7.3 Recommendation for analytical methods ........................................................................ 43 10.7.4 Quality Control ................................................................................................................ 43
10.7.5 Accuracy (bias) and external quality assessment (EQA) .............................................. 43 10.7.6 Corrective measures......................................................................................................... 43
11. Quality assurance ......................................................................................................................... 45
11.1 Adequate overall management ............................................................................................... 45 11.2 Agreement on survey procedures ........................................................................................... 45 11.3 Training .................................................................................................................................. 46
11.4 Piloting the HES ..................................................................................................................... 46 11.5 Quality Control....................................................................................................................... 47
11.5.1 Quality control of the planning of the HES ..................................................................... 47 11.5.2 Organizing quality control for the survey procedures ..................................................... 47
11.5.2.1 Internal quality control ................................................................................................. 47 11.5.2.2 External quality assessment .......................................................................................... 48
11.6 Evaluation of the achieved quality ......................................................................................... 48
12. Data management......................................................................................................................... 49 12.1 Basic work and data flow ....................................................................................................... 49 12.2 Subject Identification ............................................................................................................. 50
12.3 Data sources ........................................................................................................................... 50 12.3.1 Sample selection, recruitment and appointment scheduling............................................ 50 12.3.1.1 Sample selection ........................................................................................................... 50
12.3.1.2 Recruitment .................................................................................................................. 51 12.3.1.3 Scheduling appointments.............................................................................................. 51 12.3.2 Survey data ...................................................................................................................... 51
12.3.2.1 Sources.......................................................................................................................... 51 12.3.2.2 Forms of data collection ............................................................................................... 52 12.3.2.3 Preparation of the fieldwork ......................................................................................... 52
12.4 Error checking, correction and documentation of the data .................................................... 53 12.5 Transfer and storage of the data ............................................................................................. 54
12.5.1 Data transfer and interface to import the data ................................................................. 54

4
12.5.2 Data security .................................................................................................................... 54 12.5.3 Back-up............................................................................................................................ 55
12.6 Recommended standards, techniques and tools ..................................................................... 55
12.6.1 Database........................................................................................................................... 55 12.6.2 Development tools, use of statistical software and XML................................................ 56 12.6.3 Data encryption................................................................................................................ 56
12.7 Local data management and the EHES Reference Centre ..................................................... 56 12.7.1 Services offered by the EHES Reference Centre's data transfer and management system .................................................................................................................................................... 57 12.7.2 The architecture of EHES data transfer and management system................................... 57
13. Recruitment of participants .......................................................................................................... 58 13.1 Recruitment process ............................................................................................................... 58
13.1.1 First contact attempt ........................................................................................................ 58
13.1.2 Re-contact attempts ......................................................................................................... 58 13.2 Participation rate..................................................................................................................... 59
13.2.1 Definition of participation ............................................................................................... 60
13.2.2 Target participation rate................................................................................................... 61 13.2.3 Ways to increase participation......................................................................................... 61 13.2.3.1 Selection and training of personnel .............................................................................. 61 13.2.3.2 Factors affecting participation rate .............................................................................. 61
13.2.3.3 Partnership for enhancing participation........................................................................ 61 13.3 Non-participation.................................................................................................................... 62 13.4 Data to be recorded................................................................................................................. 62
14. Dissemination and publicity ........................................................................................................ 63 14.1 Why is dissemination and publicity needed? ......................................................................... 63 14.2. Target groups for dissemination............................................................................................ 64
14.3 Message to disseminate .......................................................................................................... 65 14.3.1 Examples of messages ..................................................................................................... 65
14.4 Brand building ........................................................................................................................ 65
14.5 Means of dissemination.......................................................................................................... 66 14.6 Dissemination plan ................................................................................................................. 67
14.6.1 Active vs. passive publicity ............................................................................................. 68
14.6.2 Preparing for unintended publicity .................................................................................. 68 15. Training program ......................................................................................................................... 69
15.1 The training program of the European HES........................................................................... 69 15.2 The national training program ................................................................................................ 70
15.2.1 Outline for the national training seminars ....................................................................... 70

5
15.2.2 Procedure, Duration and Timing of the training.............................................................. 71 15.2.3 Use of training materials and different training methods ................................................ 72 15.2.4 Selection of the national trainers ..................................................................................... 72
16. Preparation of the survey budget ................................................................................................. 73 16.1 Calculation of the budget on the basis of the main stages of the survey................................ 73
16.1.1 Planning and preparations ............................................................................................... 73
16.1.2 Coordination .................................................................................................................... 73 16.1.3 Sampling .......................................................................................................................... 74 16.1.4 Training ........................................................................................................................... 74
16.1.5 Dissemination of information .......................................................................................... 75 16.1.6 Piloting............................................................................................................................. 75 16.1.7 Recruitment of participants for the full-size HES ........................................................... 75
16.1.8 Fieldwork ......................................................................................................................... 76 16.1.9 Laboratory handling, analysis and sample storage for the Greek HES ........................... 76 16.1.10 Data entry and cleaning ................................................................................................. 77
16.1.11 Quality control ............................................................................................................... 77 16.1.12 Analysis and reporting ................................................................................................... 78

6
Introduction Personal characteristics and lifestyle choices are well-documented health determinants. Monitoring thus the attributes and habits of a representative sample of individuals is of importance, particularly if the results are extrapolated to the general population. In addition, documenting the health of a population requires the availability of biological samples, anthropometric measurements, as well as of data on personal health-related characteristics collected through questionnaires. The evaluation of health in this multi-faceted context is, however, demanding in terms of time and financial resources and this has led to the conduction of only a limited number of this type of national surveys in Europe. Nevertheless, the European Union (EU) is in need of such data that would further allow comparisons between countries. In this context, the European Commission (EC) has supported two projects with the aim to investigate the feasibility of a standardized European health examination survey (HES) and to test the methodology of such a survey in Europe. Namely, these two projects are the Feasibility European Health Examination Survey (FEHES, http://www.ktl.fi/fehes/) and the European Health Examination Survey Pilot Joint Action (EHES Pilot JA, www.ehes.info). Recently, a National Nutrition and Health Examination Survey in Greece received support through the National Strategic Reference Framework (2007-2013, http://www.espa.gr). The survey is named HYDRIA after HYgeia, Diet, Research In All, is planned to be conducted over a period of 28 months and is coordinated by the Hellenic Health Foundation (HHF).
In Greece, recent data on the health indicators of a representative population sample are not available. This information is, however, essential to highlight factors associated to health and to produce solid data towards the development of a national public health policy. The HHF acknowledging the importance of the issue represents Greece in both the aforementioned projects (FEHES and EHES Pilot JA). Members of the HHF Board, personnel and collaborators have a long-lasting experience in coordinating and undertaking population-based epidemiological studies. The DAFNE-ANEMOS initiative aiming to register and monitor the food habits and their related socio-demographic determinants of representative population samples in 28 European countries has been coordinated by HHF personnel. The DAFNE-ANEMOS initiative has been receiving funding from the European Commission since the early 1990s and it has been recognized as a success story in the European food research area. Furthermore, HHF is coordinating the Greek participation in the European Prospective Investigation into Cancer and nutrition (the EPIC study), a prospective cohort study involving more than 28500 Greek adults and elderly around the country. Recently, in collaboration with the Hellenic Center for Diseases Control and Prevention (HCDCP) of the Hellenic Ministry of Health and Social Solidarity, HHF participated in the EC-supported pilot study “European Health Examination Survey Joint Action -EHES”, coordinated by the National Institute for Health and Welfare, Helsinki, Finland (the EHES Reference Centre) (http://www.ehes.info/). This study aimed to standardize national procedures in order to proceed to a full-size HES in Greece covering a representative sample of the Greek population through which internationally comparable data will be collected.
The present manual provides the structure and organization of the Greek HES reflects the planning and preparation of the HES in Greece.

7
The present document has been developed on the basis of guidelines provided by the EHES RC. A preliminary version of this manual was provided to the EHES RC in February 2011 and the current version builds upon comments received by the EHES RC personnel, as well as the experience accumulated through the Greek pilot HES study, which was undertaken by the HHF from November 2010 to July 2011 in a sample of approximately 120 adult residents in five areas of the Attiki prefecture. The pilot was also conducted under the guidance of the EHES RC, who monitored and evaluated processes and procedures in several occasions, including a 3-day site visit in March 2011.
Overall responsibility and editing of the manual was shared between Androniki Naska and Valentini Konstantinidou. The following persons contributed in one or more of the chapters of the manual (listed in alphabetical order): George Antarakis, Vardis Dilis, Eirini Fragogeorgi, Ioulia Goufa, Pericles Karathanasis, Philippos Orfanos, Dimitra Soultanou, Kostas Tsiotas, Elisavet Valanou and Dimosthenis Zilis.

8
1. Survey planning and management This chapter focuses on national activities in the planning and preparation of the national survey, which require an efficient survey management.
1.1 Survey process
The first step in planning and preparation includes defining the survey’s aims and objectives, which will be the basis for selecting the measurements and actions to be included in the data collection. Apart from national and European level health policies and information needs, previous national health interview surveys (HIS) and HES, as well as other major health surveys need to also be considered. In general, the survey planning process needs to follow the following six main stages:
1. Survey design, which will lead to the first version of the survey proposal. In this initial
stage, commitment from key governmental and non-governmental organizations can be sought. In addition, the survey management structure and a preliminary time schedule can also be defined.
2. Detailed planning of the sampling, survey contents, fieldwork and data collection, data management as well as a preliminary plan for analysis and reporting. The output is a detailed survey plan, including the budget, and a first draft of the survey manual including the questionnaires, measurement protocols and other materials (information leaflets, consent forms). At this stage, researchers need to seek ethical approval based on the detailed proposal.
3. Pre-testing and piloting, in order to finalize the survey manual, as well as all survey materials.
4. Setting up the fieldwork and data collection system. 5. Fieldwork and data collection. 6. Finalizing the data sets, documenting data characteristics, performing the data
analysis, as well as reporting and disseminating results.
1.2 Aims and objectives of the survey
Clearly defined and specified aims and objectives guide the survey planning and fieldwork. The aim of the Greek HES needs to rely on national and european level health policies and information needs. Relevant and valid health information is needed for evidence-based health policy and health services. In addition, national health care systems, previous national HIS, HES or other major health-related surveys and expertise available in the country need to also be considered in order to assess the feasibility of different options for carrying out the survey.
The information derived from a national HES is typically used to:

9
• assess the prevalence of major diseases and their risk factors; • assess health status and its association with health promotion and disease prevention; • monitor changes at an individual (if follow up of the participants is possible) and population
level (with regularly repeated surveys); • predict future health status in the population, based on objective information on major
chronic disease risk factors (such as blood lipid levels, obesity); • analyze equity in health, health care and well-being by providing objective data, comparable
in all groups in the population; • estimate met and unmet needs for health care, social security benefits and rehabilitation, and
to forecast future scenarios concerning the need for health care and • social security benefits; • develop national standards and reference values for the measurements; • develop a valuable data source for epidemiological studies and health sciences research.
At the European level, the scope of the core HES is limited to the health of the adult population. At national level, however, the survey can be extended to also cover the elderly as the core measurements are feasible with similar methods among the elderly, but their specific needs should be taken into account.
1.3 Implementing EHES standards in the Greek national HES
A HES making use of a nationally representative population sample has never been conducted in Greece. Nor is there a sustainable infrastructure of a running national survey, in which the Greek HES could be integrated. Therefore, a new national HES needs to be built on the basis of EHES standards for survey planning and implementation. A national Greek HES should aim at collecting data on core measurements, as these were defined through the previously indicated ECHI and EHES projects and enriching the information generated in order to address particular country’s needs. The inclusion and collection of additional measurements, however, should also respect the EHES standards.
1.4. Survey management
1.4.1. Personnel requirements
The planning, design, implementation and evaluation of the survey need to be undertaken by an interdisciplinary team. In addition, a core group of key experts is needed to ensure that different aspects are taken into account. For an efficient survey management, work needs to be organized in different teams, led by members of the core group or others closely involved in the survey.
It is also recommended to involve different stakeholders such as the Public Health Authorities, the Academia and media-related professionals to promote the survey for fund raising and raising interest among the population to participate and to disseminate and communicate the results.
10
1.4.2. Organization structure
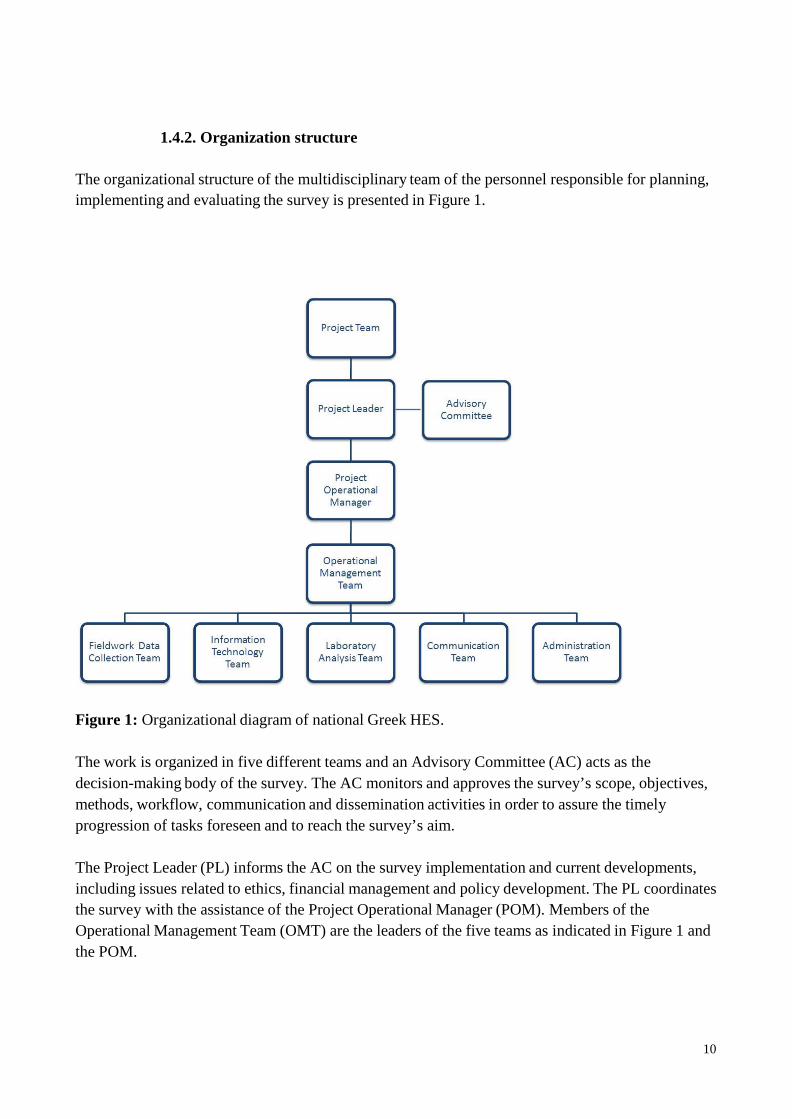
The organizational structure of the multidisciplinary team of the personnel responsible for planning, implementing and evaluating the survey is presented in Figure 1.
Figure 1: Organizational diagram of national Greek HES. The work is organized in five different teams and an Advisory Committee (AC) acts as the decision-making body of the survey. The AC monitors and approves the survey’s scope, objectives, methods, workflow, communication and dissemination activities in order to assure the timely progression of tasks foreseen and to reach the survey’s aim.
The Project Leader (PL) informs the AC on the survey implementation and current developments, including issues related to ethics, financial management and policy development. The PL coordinates the survey with the assistance of the Project Operational Manager (POM). Members of the Operational Management Team (OMT) are the leaders of the five teams as indicated in Figure 1 and the POM.

11
The five distinct teams which collaborate for the implementation of the project are: (a) the fieldwork team; (b) the IT team, (c) the laboratory team (d) the communication team and (e) the administration team.

12
2. Target population and sample size 2.1 Target population
The target population is the population of individuals which we are interested in describing and making statistical inferences about. The EHES RC suggests the following definition for the target population of a country:
The core target population is the set of all persons aged at least 25 years and at most 64 years and having permanent residence in the country. Each country can extend the eligible age group with a lower bound of 18 years and with no limitation for the upper bound.
The international EHES is a survey of adults and the EHES RC has defined adults as persons of age 18 years and more. This definition describes the ideal target population. In order to draw a sample from a population one needs a sampling frame from which the sample will be drawn. Comparisons of survey results across countries should in principle only be done for population groups that are covered in all countries. It is not recommended to leave out population groups difficult to contact or who do not, for example, speak major languages of the country.
Based on the above recommendations, the target population for a Greek HES on adults could be defined to include men and women aged 18 years and more (one day after their 18th birthday), residents of the country. It is also recommended that individuals who permanently reside in collective houses (hospitals, hotels, asylums, houses of old people, orphanages etc) or are imprisoned at the time of data collection will not be included in the target population, since their inclusion may force the implementation of complicated sampling procedures.
2.2 Sample size
Based on previous experience, a minimum of 6500 persons is recommended to be invited for the sample constitution, when setting a future HES in Greece, covering seven adult age groups (18-24, 25-34, 35-44, 45-54, 55-64, 65-74 and 75+), based on the most recent data available (the most recent Greek census refers to 2011). Each of the 14 corresponding age-sex domains should have at least ~460 representatives in the sample.
The sample size calculation is based on a participation rate of 50-60 percent (%). According to recent experience of selecting a sample in 2010 for the pilot phase, which was based on the already out dated 2001 Greek census, the participation rate was lower than 60%. Although the recommended national sample size is to include at least 4000 participants, a larger sample is expected to enable valid comparisons between regions or socioeconomic groups within a country.

13
The sample size relates to the statistical precision of the survey results, whereas bias is the concern related to low response rate. The relative benefit from higher precision, and therefore higher number of participants, is better if the response rate is high. On the other hand, if the expected response rate is low, it will be better to spend resources on increasing the response rate than to increase the total sample size.
2.3 The EHIS definition
For the European Health Interview Survey (EHIS) the Task Force III report on sampling issues suggests the following definition of the target population: For the EHIS, the target population should contain all adults (15 years old and over) living in the country at the place of their usual residence (the place where they mainly live). The sample may not include individuals at a place of residence where they do not mainly live. Such individuals must be treated as not eligible, and the interview stated as terminated. Apart from defining a wider age range, this definition does not specify a reference point in time for the target population. There is also concern on whether the reference to 'place of their usual residence' is relevant. The EHIS definition may seem to exclude persons not having a residence (homeless people). It is not clear whether this is intentional. However, such persons can be difficult to reach and are not likely to be interviewed or examined anyway.
2.4 People living in institutions
In Greece, as in many countries, the sampling frames used so far by the Hellenic Statistical Authority only cover persons living in private households. Covering institutions requires special designed sampling frames and complicated sampling procedures. Furthermore, it is often difficult to obtain participation in surveys from people living in institutions.

14
3. Sampling procedures The goal of a HES is to produce statistics for various heath indicators in a population. This should be done in such a way that the estimates obtained from the survey are, as much as possible, statistically unbiased estimates of true averages of these indicators. There are many potential sources of bias in a HES. Sampling bias is one of them, but it is also one of the sources of error that can be almost entirely within the control of the survey taker. At the same time as avoiding bias, purely random errors in the estimates should be made as small as possible.
Control of sampling errors, both systematic (bias) and random, requires a good sampling design. Scientific surveys make use of probability sampling. This means that every eligible individual or household should have a known probability of being sampled. In probability sampling, randomization techniques and (pseudo) random mechanisms are used to select the individuals to be invited to the survey. Survey sampling is a science which should be carried out or monitored by professional statisticians. In Greece, statisticians of the Hellenic Statistical Authority (EL.STAT; www.statistics.gr) have expertise in implementing survey sampling. The procedures for estimating the health indicators rely on probability sampling.
There are many ways to select a probability sample. The method to choose will depend on the features of the actual survey and the sampling frames available. A two stage sampling design is recommended for HES in European countries, except possibly the smallest ones. This is recommended also for Greece. Depending on the sampling frame available, more than two stages (e.g. sampling individuals within households within examination areas) might be necessary in order to reach down to the individual people to be invited to participate in the survey.
3.1 General considerations
In a HES where participants are invited to an examination site, it is essential that the distance to the clinic is as short as possible. Short distances are also important when mobile clinics are used to visit invitees closer to their homes (e.g. in rural districts) or when there are home visits by field work staff. Both situations call for a clustering of the invitees in a limited number of examination areas that do not cover the entire country but may be selected from a larger set of potential examination areas which do cover the entire country. In agreement with the general terminology of survey sampling, the examination areas will be called Primary Sampling Units (PSUs). The design for sampling of PSUs is Stage 1 of the total sampling design. The individual participants are sampled from the PSUs that have been selected at Stage 1 (figure 1). These units (individuals) will be termed Secondary Sampling Units (SSUs).
It is essential that all information related to each stage of sampling in all strata is stored both for those who participate and those who do not, along with the data collected in the survey. No information should be discarded. This information is needed for proper analysis, estimation and variance calculations later.

15
Figure 1. The principle for a two-stage design
An important issue that should be taken into consideration when planning a HES is the substitution of non-responding sampling units. The EHIS Task Force III report discusses advantages and limitations for substituting non-responding sampling units as well as practices applied in EU Member States and recommends not using substitution of non-respondents in population health surveys. In a HES it is expected that the state of health of the invited people will often be a factor causing non-participation among the invitees. This will bias the estimates from the survey. Moreover, when substitutions are being used, the inclusion probabilities, that is the probabilities of being selected to the sample, can no longer be exactly calculated. For these reasons it is recommended not to use substitutions in HES. However, reason for non-participation of the respective individuals should be recorded in detail.
3.2 Sampling frames
When a survey is carried out in more than one stage, a sampling frame for each stage will be required. The frame for Stage 1 should be a list of all PSUs that can be selected with information on their population sizes (individuals or households/dwellings). If updated statistics are not available for all PSUs the best available estimates, e.g. the last census, can be used. If feasible, the population sizes should be broken down to age by sex groups. There should also be information about which stratum each PSU belongs to. The PSUs and the strata should be equipped with a unique digital number as well as names.
The Stage 2 sampling frame in a two-stage sampling design is the list of units (e.g. individuals) from which a sample of such units can be taken. A Stage 2 frame should be established at least for all the PSUs selected at Stage 1. It is recommended that the Stage 2 frame is updated as closely as

16
possible to the time when the PSU will be visited by the survey. It can therefore be an advantage waiting as long as possible before taking the Stage 2 sample for a selected PSU. Different kinds of frames for Stage 2 are recommended depending on availability. The best recommendation would be a central file with the most recent and best coverage of the people in the target population. Ideally, this will be a population register. Recently collected census data is very useful as a sampling frame and should be considered for the national HES.
If a quality frame with individuals is not available, an updated address file or list of housing units can be used as an alternative. However, a postal address can either address a dwelling directly or a house with many dwellings. The two situations require somewhat different approaches to sampling.
Whenever the general Stage 2 frame does not cover all individuals that should be eligible the various kinds of under-coverage should be explained and the size of the under-coverage estimated, preferably by sex and age. If for instance parts of the institutionalized population are not covered by the main frame for the survey (as it is in general the case in Greece), an overview of such institutions by category should be made available.
3.3 Sampling design for Stage 1.
3.3.1 Creating the PSUs Whatever sampling frame for Stage 2 will be used, the sampling frame for Stage 1 (the PSUs) should be established approximately as follows:
Partition of the Greek geographical areas into a set of disjoint areas, the PSUs. Each PSU should be small enough to be served by one examination site and with acceptable travel distances to the site for all people living in the PSU or for field work team and mobile units to travel between the homes of all potential invitees. The PSUs should be areas for which statistics for total population sizes (number of persons) are accessible. Small census tracts, municipalities, electoral districts and post code areas are examples of PSUs. The Hellenic Statistical Authority in Greece has detailed population statistics by sex and age for all administrative units and sometimes also for smaller units defined for statistical purposes and such information is freely available on their web-site (www.statistics.gr) and can be downloaded as excel files. If more detailed statistics is needed the statistical office should be contacted.
From a statistical point of view it is desirable that PSUs, at least those within the same stratum, are statistically as similar as possible so that which PSUs are actually selected will affect the survey results as less as possible. As a PSU will have to be a contiguous area that meets practical constraints there will always be limits to how similar these can be. They should however not be smaller than necessary to meet the practical demands since small PSUs will often tend to be internally more homogenous and therefore less similar to their neighbours. The sizes of the PSUs can vary within the same stratum, but not to a large extent.

17
N
i
N
3.3.2 Size of the PSUs A measure of size should be established for all PSUs. This will usually be the number of SSUs (e.g. individuals) in the PSU according to the Stage 1 frame. If the SSUs are households, dwellings or postal addresses, their numbers in the PSUs should be used as the measure of size. If the number of dwellings at each postal address is known, it will be better to use the number of dwellings than the number of addresses as the size measure of the PSU. If it is feasible to select dwellings directly rather than addresses the need for Stage 3 to select dwellings at multi-dwelling addresses can be avoided or reduced. In households with a large number of eligible individuals, it may be necessary to limit the number of participants.
3.3.3 Stratification of the PSUs
The PSUs should be stratified by grouping together relatively similar PSUs, e.g. urban PSUs versus rural PSUs. Good stratification increases the precision of the survey estimates. Although the PSUs in a stratum do not need to be geographically contiguous, geography is important. It is therefore desirable that these regions consist of complete strata. When considering how many strata to create, think about how many PSUs is natural to select. Generally to facilitate variance estimation in a two- stage design, two PSUs should be selected per stratum. PSUs that are very large in population can be strata alone. Very large PSUs can either be cities where it can be seen as appropriate to sample in one stage or are those that are assigned a probability larger than one according to formula (3.5).
3.3.4 Sample sizes at Stage 1 For each stratum, the number m of PSUs to be selected at Stage 1 and the number p of SSUs to be invited within each PSU at Stage 2 can be decided directly. If the PSUs are selected with Probability Proportional to Size (PPS), which is recommended, the Stage 2 sample size p should be the same within every sampled PSU in the same stratum.
Let Y be a survey variable. For a given stratum, let Yij be the value of this variable associated with SSU no. j in PSU no. i. Let Ni be the size (no. of main frame units) of PSU no. i. Let
i ∑ j =1
ij i
µ = i Y / N = average of Y within PSU i and (3.1)
σ 2 =
i (Y − µ )2 / N
= variance of Y within PSU i. i ∑ j =1 ij i i
Let VAmong be the (weighted) variance of μi (across PSUs) of the within PSU averages and let VWithin
be the (weighted) average (across PSUs) of the within PSU variances σ 2 , that is

18
2
N N = ∑ i∈S i =
total number of frame units in all PSUs in stratum S
µ = ∑ i∈S
Ni µi / N = average of Y in stratum S
(3.2)
VAmong = ∑ i∈S Ni (µi − µ )2 / N = variance among the PSUs of their averages
VWithin = ∑ i∈S Niσ i / N = average of the within PSU variances
We wish to sample n units within a stratum to estimate the average µ of Y in that stratum using a two-stage sample where every final unit has the same probability of being selected. When the PSUs are selected with probability proportional to size such an equal probability sample is obtained by allocating the sample size n equally with p = n/m units to each of the m sampled PSUs. The variance of the simple sample mean estimator µ̂ = ∑ ij∈sample
Yij / n is then
V V Var(µ̂ ) = Among + Within m n
(3.3)
The number of individuals p to be invited within a PSU and the number m of PSUs to be drawn to minimize the Var(µ̂ ) (given n and C) is given by the formula
popt = VWithin
VAmong
CPSU , CSSU
m = n popt
(3.4)
The value of popt obtained with formula (3.4) will be different for different Y-variables. If formula (3.4) is to be made operational, VWithin and VAmong must be calculated or estimated for some
compromise calculation variable. Using a variable available in the frame is best. Age is a recommended variable for this purpose since health in general depends strongly on age.
Note that popt does not depend on the total number of units (n) to be sampled in the stratum, but m does. Formula (3.4) says that if the sample size n of SSUs is to be increased within a stratum then this should be done by taking a larger sample of PSUs, not by selecting more SSUs within each PSU. Note also that popt may be calculated larger than n. Since m must be 2 or more, formula (3.4) will only play a role if popt is calculated to be less than roughly 40 percent of n. m and p also need to be rounded to integers.
Assessing the costs CPSU and CSSU is a part of the budgeting of the survey. The variances will differ among the variables and some compromised calculation values must be established to apply formula (3.4). Note however that it is basically the ratios CPSU / CSSU and VWithin / VAmong that are
needed to calculate popt. If nothing else can be assumed, CPSU / CSSU
can be set equal for all strata. If information about age distribution within the PSUs comes with the sampling frame it is possible to establish values for VWithin / VAmong based on the age distribution within and across the PSUs. An
example on calculation of VWithin
and VAmong
based on age distribution is given in section 3.1.

19
Before calculating m, the number n of units (individuals) to be sampled in the stratum must be set. In an equal probability sample the total sample size should be allocated to the strata proportional to the number of units in the frame and this should be the basis for calculating m.
3.3.5 Inclusion probabilities for the PSUs The sampling of Primary Sampling Units at the first stage should be done with Probability Propor- tional to Size (PPS-sampling). This means that the probability π i stratum is
π = m Ni . (3.5)
for selecting PSU no. i in the
i N
Note that if m is large and there is significant variation in the sizes of the PSUs, formula (3.5) can assign the largest PSUs probabilities greater than one. This should be avoided if possible, and setting a minimum size for the PSUs aims at that. PSUs that are ‘too large’ in the sense that (3.5) produces a probability larger than 1, are automatically assigned π i = 1 .
3.3.6 Sampling When all the preparations described have been completed, sampling can proceed. PPS-sampling is rather technical and there are several methods available.
3.3.7 Distribution of PSUs over time A Greek HES may be carried out over a long period of time, often a year, covering all four seasons. Teams may travel and visit each sampled PSU, one at a time. The examination site will be in operation for a limited period, from one day to a couple of weeks and then the team will move to another PSU. The order in which the PSUs are being visited is relevant. There are for instance seasonal variations in people’s health caused by varying temperatures and weather conditions. This should be considered when timing the survey. Ideally, a randomization of the order in which the sampled PSUs are visited is recommended but can be difficult to implement. If teams have to move across the country in a completely random order carrying a heavy cargo of equipment, the cost of travelling can be high both in terms of time and money.
3.4 Sampling design for Stage 2
Simple random sampling is proposed for sampling persons within each PSU selected at Stage 1. Simple random sampling should also be used within each age-sex domain in each selected PSU. However, age-sex stratification complicates the issue of sample sizes.
Stratification by age-sex domains

20
i
Results from a Greek HES need to be comparable to those of other countries using data collected within the same time frame and age-sex domains. The seven age domains proposed (18-24, 25-34, 35-44, 45-54, 55-64, 65-74 and 75+ years) will be crossed with sex to form 14 domains. It is desirable to guarantee all 14 domains a minimum sample size. With a minimum number of 6500 individuals invited to participate (considering a 60% response rate) this means at least 460 persons will be included in each domain.
The 14 age-sex domains will intersect the PSUs. Stratification with respect to domains that intersect the PSUs in a two-stage design is not common, but can be carried out so that every person in the same domain in the same stratum has the same inclusion probability. This is recommended when the total sample size for the survey is not large enough to by itself warrant the minimum sample size for each domain. When age-sex stratification is used, then the sample sizes will not be fully fixed.
Age-sex stratification cannot be applied if the SSUs are addresses, dwellings or households.
Sample sizes at Stage 2 - with and without age-sex domains.
We first consider the simplest case, without age-sex stratification. The goal is for all units within a stratum to have the same selection probability after two stages. This will be achieved if the Stage 2 sample sizes are calculated as:
ni = n Ni
Nπ i
(3.6)
If all PSUs are selected with probability less than one, the same sample sizes ni
be equal: at Stage 2 will all
n ni =
m
(3.7)
for all i (PSUs) selected at Stage 1. The selection probability at Stage 2 is then
n ϕi =
Ni = n
mNi
(3.8)
If the largest PSU, say PSU no. 1, is selected with probability π1 = 1 , then PSU no. 1 will have a different sample size that is calculated first:
n = n N1 1 N
(3.9)
where N1 is the total number of sampling units in PSU no. 1. In this case φ1 = n/N. The ni s calculated are usually not integers. This does not matter. When sampling, each PSU gets a sample

21
d
d
d
d
d
size which is ni rounded either up or down in such a way that they sum to n and no PSU is statistically favoured.
If individuals are sampled and age-sex stratification is used at stage 2, we recommend a solution where every person in the same age-sex domain in the same stratum has the same selection probability after two stages whichever PSU the person belongs to in the stratum. But the inclusion probabilities for the PSUs at Stage 1 have been set based on the total population in each PSU, not the population in each age-sex domain. Therefore, the total sample size for an age-sex domain within a stratum will depend somewhat on which PSUs have been selected at Stage 1 and so will the total sample size across all age-sex domains and PSUs in a stratum. Different domain definitions in different strata can be allowed, but different domain definitions in different PSUs in the same stratum is not allowed.
Starting at the top we define a desired sample size for an age-sex domain within a stratum, say n*
for domain d in the actual stratum. For instance, if you want a total sample size n for a stratum, and there are eight domains and you want to have approximately equal sample sizes for each domain you can choose n*
= n / 8 . Or if you want every member of domain d in the country to have the
same probability of being selected, n*
should be set by allocating the nationally desired sample size proportional to the stratum size of domain d. In order to obtain equal probability sampling within the domain, the sample size for domain d within PSU no. i if PSU no. i is being selected must be
nid N n*
= id d Nd π i
(3.10)
If all π i < 1 this amounts to
n* N N nid
= d id (3.11) m Nd Ni
Here Nd is the size of the age-sex domain d in the stratum, Ni is population size of PSU i across all domains and Nid is the population in domain d in PSU no. i in the Stage1 frame. The Stage 2 inclusion probabilities for all eligible individuals in domain d in PSU i is
ϕid = nid
Nid
(3.12)
The sample sizes nid are calculated for all PSUs before sampling at Stage 1. Their sum over the
selected PSUs constitutes the actual sample size nd in domain d in PSU no. i and depends on which
PSUs have been selected. The actual sample size is therefore random and usually different from n* ,
but is equal to n*
in expectation.

22
The variation of nid should be kept as small as possible. Variation in age distribution and to some extent the sex distribution across the PSUs within strata will contribute to variability of the domain sample sizes. This is a strong argument for considering age distribution when stratifying the PSUs, whether age-sex stratification is being applied or not. We must expect to find considerable variation in age distribution across PSUs. Typically, recently established housing areas and areas with considerable immigration have a much younger population than districts where there is emigration and a declining population. It is most often the young population that moves.
In practice it may be possible that the Stage 2 samples will often be selected later that the date when the stage 1 frame was constructed and one PSU by one based on local registers. These local registers will show up PSU-sizes and domain-sizes that are different from the sizes Ni and Nid that we used when taking the Stage 1 sample and calculating ϕ id . Correctly done, ϕ id will be applied to the local registers to do the actual Stage 2 sampling. The real sample sizes will result from this process and they will be somewhat different from nid in formulae (3.11) - (3.12). Never the less, the method will provide a sample where the selection probability π iϕ id is the same for all individuals in the same age-sex domain in the same stratum whichever PSU (i) the person belongs to in the stratum.
When the Stage 1 frame is approximate
The sampling frame used to establish the Stage 1 frame and proceed to the calculations described above may be approximate in relation to the actual sampling process. The selection of the PSUs will have to take place well before the survey is carried and may be based on population statistics that are not up-to-date. A Stage 2 sampling frame with the desired SSUs may also exist only locally and not centralised at national level. Furthermore, since the survey will have to take place over a year or more, those selected at the beginning of the survey period may have died or moved from the PSU at the time when the survey team operates an examination centre in the area. Therefore, it is desirable to take the Stage 2 sample for a PSU as close as possible to the time when the PSU will be visited. This may mean that the Stage 2 samples have to be taken at different times for different PSUs. When considering eligibility and age-sex domains, the age of a person included in the Stage 2 frame should then be taken as the age at the middle of the data collection period in the actual PSU. Then the sizes of the PSUs (Ni ) and the age-sex domains (Nid ) may have changed slightly and the anticipated Stage 2 sample sizes calculated in section 3.4.2 will be adjusted somewhat according to that.

23
4. Legal and ethical issues Any type of research on humans must be conducted according to ethical standards, which are defined by legislation, safeguarding participant's privacy and health (physical or mental), as well as acquiring his/her informed consent. Although performing a HES does not pose any serious risk to health, the safeguarding of privacy and acquiring informed consent are crucial ethical aspects.
4.1 Legislation and guidelines
All national HESs must be conducted according to ethical standards, which for all human research, are regulated by national and international guidelines and legislation. The Declaration of Helsinki, “Ethical Principles for Medical Research Involving Human Subjects” (WMA 2008) is considered as the pillar of ethical standards. Other important reference documents include: the Belmont Report (“Ethical Principles and Guidelines for the Protection of Human Subjects of Research”, NIH 1979) an act of the Council of Europe: the Recommendation of the Committee of Ministers No R.(90) 3
concerning medical research on human beings (Committee of Ministers 1990); and the Oviedo Convention on Human Rights and Biomedicine. (Oviedo 1997)
In Europe, the protection of personal information is governed through the Directive 95/46/EC of the European Parliament and the EU Council (1995) on the protection of individuals with regard to the processing and free movement of personal data. The respective national legislation in Greece, incorporating the European Directive, is covered by Law 2472/1997. This law further establishes the Hellenic Data Protection Authority (HDPA) (http://www.dpa.gr) with the mission to protect personal data and the privacy of individuals in Greece. The HHF (coordinator of the Greek pilot and the national HES) complies with HDPA's requirements and has received the Authority's approval to collect, store and analyze data, records and files from studies conducted by HHF.
4.2 Role of ethics committees - Ethical approval
An Ethics Committee is a body that is responsible for evaluating research proposals from an ethical standpoint. In particular, this committee, which can be local, regional, or national, evaluates the given proposal in terms of its compliance with national legislation and regulations. The evaluation covers not only the performance of the research itself (i.e., that the participant will not be harmed or placed at risk) but also the contents of the informed consent and how it is obtained, the safeguarding of privacy, and the use of data and biological materials, both for the research being conducted and any future purposes. The HES cannot be started before approval is obtained.
Since obtaining ethical approval can be a time-consuming process, the procedures need to start as early as possible, sometimes even during the beginning of the planning phase. The process broadly includes three stages:

24
1. identify the appropriate Ethics Committee and prepare the documentation required to apply for approval
2. discussing with experts may be needed in the consultation phase 3. insert modifications if requested by the Committee
4.3 Data confidentiality – Data protection
Performing a HES includes collecting individual level data which are also sensitive personal data (i.e., sensitive data regarding health status). For this reason, the HES protocol must comply with the given country’s Data Protection Act and cover all aspects of data protection, in particular: access to data, the exchange of data, record linkage, and anonymisation procedures.
4.4 Informed consent
The participant’s entry to the survey is signaled by signing an informed consent form. It is a process of communication between a potential participant and the HHF fieldwork staff, aiming to ensure that the individual fully understands the scope of the study, the methods adopted and how the data are going to be used. Prior to the visit at the study centre, the study candidate is provided with information on the survey through the invitation (postal) letter and a survey brochure explaining, in general, what the study is about, its importance, and how and when the candidate will be contacted. During the study visit, issues related to the survey’s aim and procedures are again discussed and clarifications are provided. If the individual agrees to participate, acceptance and compliance to the survey procedures is assured through signing and initialing the informed consent form. Each participant is fully informed about his/her rights and is able to consent fully or partly to the study objectives.

25
5. Selecting the measurements
The Greek HES collects measurements through physical and clinical assessments, questionnaires and analysis of blood samples. Measurements are divided into core and additional. Core measurements need to be included in every national HES to ensure comparability between counties. Subject to national needs for information and available funding, additional measurements can be considered to be included in the survey.
The chapter describes core measurements to be included in the Greek HES and further provides criteria and the rationale for their selection.
5.1 Criteria for selecting the measurements
The selection of measurements is based on the survey’s objectives, research questions and analysis plan. Furthermore, for selecting a measurement to be included in the survey the criteria in Table 5.1 need to be met.
Table 5.1: Criteria for selecting the HES measurements
The criteria for selecting the measurements
Rationale and importance of the criteria
Availability of internationally standardized measurement protocols
The availability of internationally standardized measurement protocols ensures the comparability of results between countries and in time.
Clear interpretation of the results Results need to be reliable.
Practicality/easy administration Measurements feasible at population level by health professionals.
Motivation of the participants Some measurements may act as incentives for participation and thus may increase the participation rate. Personal results can be interpreted and used to estimate needs for care and preventive actions for the individual.
Acceptable by the respondent Measurements should not be very time consuming, causing extra burden, pain or discomfort to the participants.
Ethical acceptability Measurements need to be ethically approved and safe for the participants, as well as accepted by health care professionals. If deviations from normal values are identified, access to care and preventive services should be assured.

26
Costs A balance between the costs of the measurement and the amount of available funds need to be assured.
Public health importance Selected measurements should address key public health problems.
5.2 The core measurements
The core measurements (including the physical and clinical examinations, the questions and the analyses of blood samples) aim to assess the prevalence of major chronic diseases (e.g. cardiovascular diseases and diabetes) and their risk factors (e.g. obesity, high blood pressure, high serum cholesterol, low physical activity and smoking) which are preventable at both individual and community level.
5.2.1 The core physical assessments
Physical assessments are necessary since self-reported data are not sufficiently reliable to follow population trends and to make comparisons between populations. The core physical assessments selected to be included in the Greek HES have been used in previous national European HESs and are the following:
• Height • Weight • Waist circumference • Blood pressure
Irrespective of the information each one independently conveys, weight and height are used to estimate the Body Mass Index (BMI), an indicator widely used to assess obesity. BMI is defined as the individual's body weight (in kg) divided by the square of his/her height (in m). The increasing prevalence of obesity and overweight among the population is one of the most important public health issues. Overweight and obesity are known to be risk factors for several chronic diseases as there is a clear association between obesity and type 2 diabetes, hypertension and dyslipidaemia.
Waist circumference is an indicator of abdominal obesity and recent evidence suggest that it is the preferred measurement in population studies. It is significantly associated with the risk of incident cardiovascular events and type 2 diabetes.
Measuring blood pressure provides an estimation of the prevalence of actual and potential hypertensives. A single-occasion blood pressure measurement has been shown to be a strong indicator of coronary and cerebrovascular risk. The diagnosis of hypertension, however, requires the assessment of high blood pressure on several occasions.

27
5.2.2 The core analyses of blood samples (clinical assessments) Blood samples are collected to perform the following core measurements: ° Total cholesterol ° HDL cholesterol ° Fasting (8-14 hours) glucose
High (serum) total cholesterol and low HDL cholesterol are major risk factors for cardiovascular diseases. Increased glucose level in blood may indicate insulin deficiency or insulin resistance which is a risk factor for diabetes.
It is advisable to collect blood samples in a fasting state. Τhe minimum overnight fasting time is 8 hours, but the fasting should not exceed the 14 hours. Because of potential difficulties in acquiring a fasting blood sample from all participants, te glucose may cover only a sub-sample of the survey.
5.2.3 The core questions The HES core questions need to be based on those used in the Greek national Health Interview Survey (HIS), which is part of the European Health Interview Survey (EHIS) and was conducted by the Hellenic Statistical Authority (www.statistics.gr). Slight modifications, as well as additions of questions can, however, be accepted. The HHF (coordinating centre of the Greek national HES) should keep track of revisions in the EHIS questionnaires.
The EHES core questionnaire includes questions on:
• Household size • Sex • Age • Marital status • Socioeconomic status • Height and weight • General health • Chronic diseases • Use of medication • Smoking
- Age and sex enable reporting the HES results by sex and age group and the age-adjustment or standardization of the results for comparison between populations.
- Education and occupation are needed for the estimation of socioeconomic differences in the population.

28
- Even though height and weight are measured during the physical examination, self-reports are also included in the questionnaires. Self-reports are needed to investigate people’s perception and to enable comparisons between measured and self-reported values at the European level. Additionally, self-reported height and weight may provide the only anthropometric data for participants who do not take part in the physical examination.
- The three questions on general health form the Minimum European Health Module (MEHM) are used in order to link results among surveys according to these standard health characteristics of the population. More generally, the three questions can be used for the calculation of the prevalence of perceived health, self-reported longstanding illnesses or health problems and long-term activity limitations.
- The questions on chronic diseases measure the main public health concerns, which are also a major reason for using the health care services. Measuring chronic morbidity is not only useful for the overall evaluation of health and health status, but also for the study of health care systems in terms of evaluation, policy formulation and assessment of needs for health care.
- Smoking is an important risk factor for lung diseases and cancer as well as for other cancers and diseases of the circulatory system and therefore a major determinant of health outcomes. In addition, policy activities are implemented in the country in order to limit tobacco smoking and information on this indicator can provide a feedback for the policy evaluation.
Several of the above questions supplement the information collected during the clinical examination. For instance, cholesterol and glucose levels in blood are often combined with related questions. It is therefore important that the answers to the questions on specific diseases and smoking habits are given by the same person to whom physical and clinical examinations are undertaken.

29
6. Timing of the fieldwork and order of measurements This chapter describes general issues related to timing of the fieldwork and order of measurements that need to be taken into account when planning the survey. Timing of the examinations will affect participation rates. General principles for the order of measurements need to be considered when estimating the time needed to carry out the fieldwork. These issues will all have an effect on personnel resources and other survey costs.
6.1 Periodicity
If adequate funding is available, the recommendation is to repeat a national HES (including the EHES core measurements) about every five years. The option, however, of repeating some additional measurements less frequently (e.g. every 10 years) can be considered. Currently, a system of continuous data collection is not under consideration.
6.2 Length and time of year for the fieldwork
The study’s time plan should assure maximum participation rates. The collection of data all year round assures coverage of seasonal variations in health determinants (e.g. leisure-time physical activity) and biological measures (e.g. blood pressure); allows the estimation of time-trends in the case of repeated surveys and, last but not least, enhances comparability between regions within the country, as well as international comparability.
6.3 Weekdays and time of day
Appointments for carrying out the measurements need to be scheduled all weekdays. Moreover, to allow easy access for participants and to minimize the effect of timing to measurement results, morning, day and evening appointments are necessary. Data collections on Saturdays and Sundays need to also be foreseen, since according to the experience gained in the Greek HES pilot, individuals (especially in urban areas) with busy working schedules prefer to visit the examination centres during the weekends.
Many of the HES measurements, such as blood pressure and some blood analyte concentrations have diurnal variation. In the case of lipids, for instance, it is difficult to dissociate changes in their concentration from the effects of a meal. This is best adjusted for by spreading the measurements throughout the day, and in any case by recording the time of the day when the sample is taken.

30
6.4 Order of measurements The order of measurements has often constraints because of logistical requirements, such as composition of the survey staff and fieldwork teams, participant flow, costs and duration of the examination. Nevertheless, the following requirements need to be taken into account to ensure valid measurements and comparability between surveys.
To determine the order of measurements, the following need to be carefully considered: Importance of the measurement: most important measurements need to be made early in the session in case the participant is unable to follow the full examination protocol (e.g. because of time constraints, limitations in functional capacity etc.). The EHES core measurements are always conducted first, before additional measurements. Sensitivity of questions: uncontroversial questions can preferably be asked early in the interview to allow participants to become relaxed and feel comfortable with the procedures. Stressfulness of a procedure: blood pressure measurement need to precede venipuncture and other potentially (mentally or physically) stressful tests/interviews. Other effects on measurement results: based on survey’s objectives and previous experience in data collection.
6.4.1 Clinical measurements Unless good reasons exist for change, the following order for clinical measurements should be maintained during the whole survey:
1) Blood pressure measurement 2) Anthropometric measurements 3) Blood samples drawing
6.4.2 Questionnaires and interviews The questionnaires used in the Greek HES are interviewer-administered. To avoid respondent burden, the questionnaires may be split into different parts administered before, during and after the clinical measurements and somatometric examinations. In this case, the selection of questions to different phases of data collection should be based on the following principles: (a) questions affected by clinical measurements, EHES core questions and non-sensitive questions to be asked before the measurements, (b) questions on acute symptoms during the measurements, and (c) less important and sensitive questions after the examination.

31
7. Selecting the examination site This section describes the examination sites selected to be used in the Greek HES, their advantages and disadvantages and provides options to deal with possibly encountered problems.
7.1 The Greek HES examination sites
The examination sites of the Greek HES are at the premises of the local Health Centers of the National Health System, which provide primary health services to the population of their region. Centers are selected on the basis of proximity to participants’ residence. In Greece, particularly in rural and semi-urban areas, Health Centres form integral part of local communities which are generally familiar with visiting the centre of their region. Nevertheless, access by participants may require effort, might involve travel costs and cause environmental burden. In case the Health Centre is not located within walking distance, public transportation is always an option.
Furthermore, using the premises and facilities of the Health Centers has the following advantages: availability of a laboratory to perform the aliquoting of blood samples, before having them transported to the National HES laboratory (NHESL) access of participants with limited functional ability privacy, quietness and comfortable room temperature health professionals available in case of emergency better controlled safety of fieldwork staff.
The use of local Health Centres, however, requires traveling of the fieldwork staff, (with the related burden to the survey’s budget), as well as time and cost for setting up the examination site.
7.2 Additional options
In cases where access to the Health Centers is difficult or impossible, other local sites with the potential to operate as examination centers will be used. For instance, public premises (town hall, peripheral doctors' office), teaching premises (colleges, libraries, gymnastic halls), open care community centers for the elderly (KAPI), community clinics and/or mobile health care units will be used. A mobile unit with facilities to perform anthropometric measurements, personal interviews, blood drawing and processing is strongly recommended to facilitate participation, in case a participant is unable or unwilling to reach the study centre. Mobile units significantly enhance access to participants and can provide private, quiet and well-controlled examination environments. On the other hand, the space provided is often limited; they are demanding in terms of time and cost to setting up, operating and maintaining a mobile unit; and cause environmental burden.
In cases where severe mobility incapacities hindering participation exist, home visits can also be scheduled. Sometimes, asking participants to visit a health care environment might initiate a

32
stressful feeling, something that is prevented at their home environment. At participant's home there in no difficulty in access, no cost for the participant and the relaxed environment/atmosphere is assured. Home visits, however, are not always accepted (particularly if individuals are not willing to let unknown health care personnel at their home) and may lack privacy, if other household members are present. In addition, home visits restrict the type of measurements that can be conducted (only measurements that do not require equipment that is heavy or otherwise difficult to transport, or have other special requirements are feasible); the standardization and calibration of the equipment and the measurement protocol may not always be assured; and restrictions for handling and properly storing the blood samples may compromise their quality. Special attention is also needed in relation to the safety of the fieldwork staff and precautions (e.g. involving more than one member of the fieldwork staff) may increase the survey’s budget. Home visits are generally avoided and proposed as an option only when no other possibility for participation exists.

33
8. Questionnaire design and administration 8.1 Questionnaire design
Every national HES includes a questionnaire. Upon its development, the questionnaire was pilot- tested in order to assess its feasibility, understand and possible evaluate how the questionnaire design affected the participation rate, the reliability and the accuracy of the information provided by the respondent. After the completion of the pilot-testing, questions were modified and improved, based on the experience gained during the pilot.
8.1.1 Language and wording The wording of the Greek HES questions are simple, straightforward and avoiding ambiguity, in order to ensure that the respondent understands the questions correctly. Professional or highly technical terms, slang, abbreviations or words which may be considered as insulting have been avoided. Questions have been selected and phrased so as to address only one issue each. For the questions adopted from the national HIS questionnaires, the official Greek translation of the National Statistical Office was used.
8.1.2 Recall bias When formulating the questions, effort has been invested to minimize the effect of recall bias, which is often unavoidable particularly when the recall period is long. For that reason, questions are ordered in a logical sequence and recall of the events is assisted.
8.1.3 Order of the questions All the EHES core questions are included in the Greek HES questionnaire and are grouped in the following thematic modules:
• Personal Characteristics • Health Determinants • Health status • Use of health care and services
Each thematic module starts with easy questions and more difficult ones are placed at the end of the section. Starting with the easy questions, the interviewer aims to build a trusting relationship with the respondent, so as to facilitate the response in more difficult questions later on in the section.

34
8.1.4 Length of the questionnaire The Greek HES questionnaire is interviewer-administered and current recommendations suggest that face-to-face interviews should be limited to 30 minutes.
8.1.5 Layout of the questionnaire The questionnaires and data collection forms used in the Greek HES are web-based. In the case, when internet access is not available, paper versions of the questionnaires will be used and data entry will follow.
8.2 Questionnaire administration
8.2.1 Interviews In the Greek HES, data will be collected through face-to-face interviews, using computer-assisted administration (CAPI).
Face-to-face interview is usually the most demanding method in terms of both time and resources and might be subject to bias from socially desirable answers, but has several advantages. In particular:
• the questionnaire could include more demanding questions that would be difficult to reply if
the questionnaire was self-administered • the interviewer defines the order of the questions • the interviewer has the possibility to check personal records
(e.g. medication) • personal contact may increase the response rate, • avoid bias by asking the questions verbatim, • through the personal contact, the participant can feel familiar and build trust with the
interviewer gaining thus confidence to reply on sensitive questions (e.g.: questions about health),
• the interviewer can avoid errors on personal information (e.g. date of birth or last name) by checking the identity card of participant,
• the interviewer can give examples or use visual aids when needed, to avoid a wrong reply in an unclear question
• language barriers or literacy issues could be overcome • The possibility of missing responses in questions is very low.

35
8.2.2 Use of proxies There is evidence that the use of proxies can introduce systematic bias, affecting national disability estimates and the incidence of several chronic conditions, as well as their trends in repeated surveys. Proxy responses and self-reports differ significantly depending on the type of questions, age and gender of both the proxy and the selected person, and relationship between the selected person and the proxy. For younger persons there is evidence that proxies tend to under-report chronic conditions, disability and medication use, while for older persons the bias may be opposite, proxies reporting more impairment than self-respondents.
In EHES data collection, proxy use during the interviews is only allowed when the selected person him/herself is unable to respond due to major limitations in communication skills and/or cognitive ability. The reason for proxy use and type of proxy (spouse, child or other relative/significant other, or nurse for e.g. institutionalized persons) is always recorded. When a proxy is used, particular attention needs to be given on whether the proxy him/herself is capable to provide informed consent. Efforts need however to be invested to avoid proxy use through proper resources during data collection and scheduling adequate time to contact all selected persons.

36
9. Selection of the fieldwork staff In the Greek HES the selection of fieldwork staff can be based on general requirements and competences needed to carry out the measurements. Characteristics of the national health care system, as well as national guidelines for the responsibilities of different health professionals need to also be considered.
9.1. General principles and criteria for recruitment
To select the fieldwork staff, the following general principles need to be considered:
• General appearance, since a non-provocative, calm and neutral appearance, good manners, friendliness, respect and interest shown towards the participants may affect participation and the survey’s results. Cultural norms need to also be taken into account.
• Willingness and possibility to travel around the country • Professional and broad competence of the staff members is also an important factor affecting
survey response. Experience in previous large-scale data collection in the country (e.g. the EPIC-Greece study) and/or experience in the pilot of the Greek HES will be highly appreciated. Since data collection is taking place all-year round, the recruitment of staff members with broader competence, who can also substitute other team members in case of absences (e.g. sick-leaves) is important.
• Fluency in national language(s), and if needed, languages of the major migrant groups. Fieldwork staff can be recruited. In addition, specially trained personnel from the local health centers (operating as examination sites) and/or the Hellenic Centre for Diseases Control and prevention (HCDCP), rural clinics and hospitals could also be involved, in an attempt to enhance the sustainability of a Greek HES. An issue worth considering, however, is that the use of regular personnel from local health centres, clinics or hospitals may affect survey results by the differences in willingness of the survey participants to disclose personal issues to practitioners they are familiar with. This familiarity may both enhance and restrict open communication.
The Greek HES will combine the above two groups of personnel. Specially trained personnel travelling from one site to another will be responsible to carry out the measurements that are most challenging to standardize (e.g. blood pressure measurements) and for collecting data on sensitive personal matters. These specific survey staff may also supervise the personnel at the examination centres responsible for other tasks. The local personnel may be more efficient in recruiting participants.

37
9.2. Professional groups The professional groups which should be considered for most of the measurements include physicians and other health professionals and laboratory technicians. The presence of a medical doctor is also needed for back-up.
9.3 Fieldwork teams
Since data collection needs to be evenly distributed across seasons and cover the whole country, the number of fieldwork teams depends on the length of the fieldwork period in each region and the distances between the selected examination sites. Normally, two or three data collection teams are expected to carry out the data collection, one of which will solely focus on the Attica region.
Support and supervision from the Project Operational Management Team needs to be ensured. Well-defined leadership within the team is also essential. Each fieldwork team should have a specified leader who manages the work progress among all team members, adheres to the survey’s standard procedures and reports accordingly to the survey’s Operational Management Team.

38
10. Blood samples and laboratory analyses This chapter gives guidelines and describes requirements for selecting the survey laboratory; for collecting, processing and storing the blood samples; and for performing the laboratory analyses. Moreover, quality requirements of analytical laboratories and guidelines for the standardization of methods are described.
10.1 Selection of the national laboratory
All analyses pertaining to the core measurements are performed by one laboratory, hereafter called the National HES Laboratory (NHESL). The NHESL is selected on the basis of its performance in RIQAS - The Randox International Quality Assessment Scheme. The NHESL is currently in the procedure of accreditation by the Hellenic Accreditation system S.A. under the distinctive title ''ESYD'' according to the accredidation standard ΕΛΟΤ ΕΝ ISO 15189: 2007. The long-term storage of all samples lies on the responsibility of the survey coordinating centre. The long-term storage of all samples lies on the responsibility of the HHF (survey coordinating centre).
10.2 Selection of measurements on blood samples
Total cholesterol, high density lipoprotein (HDL) cholesterol and fasting glucose are the core measurements included in all national HESs. For this purpose, the collection of ~ 20 ml of blood per participant is required. This quantity covers the 25% excess needed to assure the performance of laboratory techniques and to reserve an extra aliquot in cases where analyses have to be repeated or various additional measurements are made.
10.3 Blood collection
The collection of blood samples in order to perform the core measurements is described below.
• Total and HDL cholesterol: These lipids are measured in serum collected in plain gel
tubes. Fasting is not necessary. • Glucose: Glucose is measured in plasma collected in fluoride-citrate tubes. Minimum 8-
hour fasting is necessary for assessing glucose. Because of potential difficulties in requiring fasting from all participants, measurements of fasting glucose may cover only a subsample of the survey.

39
10.4 Critical issues concerning the blood collection
10.4.1 Fasting before the sample collection The samples for total and HDL cholesterol can be taken at any time of the day, with the participant in a fasting or non-fasting state. For measuring fasting glucose, however, the samples are collected after a fasting period of at least 8 hours and at most 14 hours (excessively long fasting causes major changes in energy metabolism).
In practice, this means that fasting is preferably overnight (8h and at most 14h) and that blood collection is performed in the morning. Therefore, participants are encouraged to visit the study centre in the morning. Information on the length of time from the last meal in full hours should be documented.
10.4.2 Position of the participant and details on arterial puncture
All blood samples are drawn with the participant in a sitting position preceded by a 10-15 min rest. Arterial puncture should NOT be performed from the arm that is used for blood pressure measurement.
10.4.3 Use of a tourniquet
Prolonged venous occlusion can cause changes in concentrations of blood constituents. Therefore, the use of a tourniquet should be minimized down to absolute necessity and should in any case be limited to less than one minute.
10.4.4 Effects of seasonal variation Diurnal effects on the concentrations of the analytes are varied. In the case of lipids it is difficult to dissociate changes in their concentration from the effects of a meal. Studies suggest that cholesterol concentrations are higher in autumn and winter than in spring and summer. Seasonal variation is fully captured, since the Greek HES recruiting period is extended to cover a whole year.
10.4.5 Effect of physical training Excessive physical training may cause dehydration resulting in raised serum electrolytes and several enzymes of muscle origin. Except for dehydration, other effects are difficult to estimate. Therefore, participants need to be asked to abstain from heavy physical activity or training for 8 hours preceding phlebotomy. If, however, this is not possible (e.g. if the person is a heavy manual worker and visits the study centre after his work) the length of time since the physical activity in full hours needs to be documented.

40
10.5 Equipment for drawing blood samples
10.5.1 Type and order of blood tubes The blood collection kit, including tubes and equipment needed for the procedure, is planned and prepared in such a way that all parts are compatible, provided by a single supplier and that all tubes are evacuated.
The KIT is composed of: 1) plain gel tube (Nominal vol. 10ml /Draw vol. 8 ml) used for total and HDL cholesterol (Gel+ Clot Act. serum) 2) fluoride-citrate ( Nominal vol. 5ml/ Draw vol. 3 ml) tube used for glucose (FC-plasma) 3) test tube rack or tube holder 4) needles and vacutainers for blood sampling 5) cryotubes (2.0ml) for long-term storage -70°C 6) storage boxes (for cryotubes) 7) sheet of bar code labels (for cryotubes and storage boxes) 8) tourniquet, skin cleaner, automatic pipettes of adjustable volume, disposable plastic tips, skin tape, sodium chloride (0.9%) etc. 9) biological waste container for sharps (e.g. syringes with needle) or biological material (e.g. blood).
Items 4 and 5 should be compatible with the systems of both NHESL and the EHES Reference Laboratory. For instance, the cryotubes must be straight-walled and the bar code sticker has to be placed vertically in order to enable the reading of the code and to allow visual inspection of the content of the tube.
10.5.2 Equipment for handling, transfer and storage of blood samples
• Portable centrifuge, capable of 3,000g with a swinging bucket rotor. • Test tube racks. • Insulated rubber foam boxes (Styrofoam boxes) are used to ship the biological samples with
dry ice for tube transfer from the examination site to the central storage • Set of (bar code) labels (both numerical and literal) with identification codes not vulnerable
to freezing. • Freezer for short-term storage -20 °C. • Freezer for long-term storage -80 °C.
10.6 Processing, storage and transport of blood samples
In the Greek HES, the participants’ physical and clinical examination and subsequent data collections are generally performed in local Health Centers (HES examination centers). If this is not feasible, public premises (town hall, peripheral doctors' office), teaching premises (colleges, libraries, gymnastic halls), open care community centers for the elderly (KAPI), community clinics

41
and/or mobile health care units will be used. A mobile unit with facilities to perform anthropometric measurements, personal interviews, blood drawing and processing is strongly recommended to facilitate participation, in case a participant is unable or unwilling to reach the study centre. All blood samples are collected, centrifuged, aliquoted and temporarily stored at -20°C on site. Afterwards, they are placed in styrofoam boxes and transported to the premises of HHF (the survey coordinating centre) for storage at deep freeze (-80°C). The NHESL receives suitable batches for the necessary analysis. In no circumstances samples are defrosted before they are delivered to NHESL.
10.6.1 Processing
• Immediately after venipuncture, bar coded labels are placed on blood collection tubes which have successfully been filled with blood.
• Centrifuge tubes at room temperature (20-25°C) for 10 min at 2000 g. • Plain serum gel tubes are centrifuged within 30 - 60 min from venipuncture. Adherence to
the time range and room temperature is necessary for complete clotting. • Plasma tubes are centrifuged together with the plain serum tube within 60 min from
venipuncture. Simultaneous centrifugation of both serum and plasma tubes ensures the identification and aliquoting of samples from the same subject.
• The caps should not be removed before centrifugation • Immediately after centrifugation remove the caps. Place bar code labels on serum and
plasma storage tubes. The labels should be fixed upright. • Transfer with pipette serum or plasma into the storage tubes according to a prefixed scheme. • When using gel-containing tubes, it is convenient to pool the serum before pipetting into
aliquots. Cap the tubes tight.
10.6.2 Storage of serum, plasma, whole blood and buffy coat tubes Samples intended to be analysed within six months from the blood drawing can be frozen at -20°C. Samples intended to be analysed after a six month period must be frozen at -80°C.
BEFORE placing the storage boxes in the freezer, they should be labelled with the two appropriate bar code labels. Otherwise the labels will not stick. An inventory of all stored specimen must be documented daily at the examination site.
10.6.3 Transport a) Transport of specimens from the examination centre to the premises of the Coordinating Centre Frozen samples are sent in suitable batches during or at the end of the fieldwork from the examination centres to HHF (the Coordinating Centre). The insulated rubber foam boxes are

42
transported in dry ice. This procedure ensures that temperature will not exceed -20oC during transfer.
The transportation is organized well in advance. A courier company provides the service including necessary paper work for "door-to-door" transport. Before sending the shipment, the consignee needs to be informed on the date, courier and tracking details (by phone and e-mail). The consignee should acknowledge receiving the shipments by phone or e-mail. The Coordinating Centre (HHF) keeps a log book of all shipments, where also the acknowledgments are recorded. For study centres closely located to HHF (the Coordinating Centre), samples are transported by car, stored in dry ice.
b) Transport of specimens from the Coordinating Centre to the NHESL The NHESL receives the frozen batches for analysis. Transportation is organised well in advance, ensuring that the laboratory is prepared to analyse the specimens immediately. Frozen samples are transferred from HHF (the Coordinating Centre) to the NHESL in a portable freezer with ice-packs.
A courier company can again provide the service. Before sending the shipment, the consignee needs to be informed on the date, courier and tracking details (by phone and e-mail). Upon receiving the shipment, the consignee should inform the Coordinating Centre’s (HHF) personnel by phone and e- mail. These shipments and related acknowledgements should also be kept in the Coordinating Centre’s (HHF’s) log book of shipments.
10.7 Guidelines on laboratory performance
10.7.1 Performance of laboratories Data on the following three levels of accuracy (bias) performance for core measurements is monitored by the central EHES RL:
• Bias in EQA programmes of the NHESL related to the core measurement methods during the preceding year
• Bias between the NHESL and EHES RL, providing that a random 5 to 10% of actual survey samples are transported and reanalyzed at the EHES RL and results are compared to those obtained in the NHESL.
• Bias between the EHES RL and the Centres for Disease Control (CDC, Atlanta). The CDC values are considered as the golden standards.
The accumulated data are reported annually.
10.7.2 Standardization of analytical data A pilot calibration between the NHESL and the EHES RL needs to be carried out before the beginning of the survey. The EHES RL sends serum and plasma specimens to the NHESL and core measurements are performed. If the pilot calibration is not satisfactory and does not provide

43
convergent results, the pilot calibration loop is repeated until an accepted level of agreement is reached.
10.7.3 Recommendation for analytical methods
No recommendation to use a specific method is given, provided that the method is validated and the procedures are documented. The documentation for each method used in the survey should be available at both the NHESL and the EHES RL.
10.7.4 Quality Control
Data on the accuracy of methods within and between days (series) are kept with a computer-aided protocol. The precision limits provide guidelines for the performance of a method. The limits are based in part on data from instrument manufacturers and experience of the EHES RL.
10.7.5 Accuracy (bias) and external quality assessment (EQA)
Data and documentation on accuracy of the methods are provided by participating regularly in national or international EQA programmes. It is recommended to check and document the performance of all instruments (clinical chemistry analyzer, photometers, balances and pipettes, eg.) once a year. As with all components of a method, the traceability of calibrators should be documented in order to ensure high quality.
The recommended goal and acceptable bias values for the core analytes are shown in Table 10.1. The data on bias take into account the biological variation of the analyte.
Table 10.1: Recommended goals for bias and precision of methods
Bias (%) CV(%)
Core analytes Goal Acceptable Goal Acceptable
Serum total cholesterol 3 5 2 3
Serum HDL-cholesterol 5 10 2 3
Plasma glucose 4 8 1 2
10.7.6 Corrective measures
When the bias of a method exceeds the acceptable value, corrective measures should be taken. Possible sources of errors include the following:
• erroneous calibrators, • change of reagents (kits),

44
• malfunctioning instruments, • wrong type of sample (e.g. serum-plasma-whole blood) • reagents not compatible with the instrument • introduction of new calibrators
Note that a change of the selected method (technique) may provide remedy. The NHESL must document all changes introduced to methods or procedures and report them promptly to HHF (the survey’s Coordinating Centre) which will subsequently report them to the central EHES RL.

45
11. Quality assurance A well-planned quality assurance system of the national HES is essential in order to obtain high quality data which will be comparable to those obtained from other European HESs over time, so that reliable long-term trends could be calculated in the future. The basic components of quality assurance are:
• Adequate overall management of the survey. • Agreement on survey procedures that ensure standardized stable measurements. • Training of the survey personnel on using the standard procedures. • Piloting the fieldwork phase. • Quality control, which refers to measures taken to monitor the survey process, so that any
problems can be detected at an early stage. The term 'quality control' also includes the action taken to correct the detected problems. In the ideal case, the problem will be detected early enough so that it can still be remedied. The term quality assessment is used to refer to monitoring and documenting the quality, but does not include the corrective action taken. Accordingly, a part of quality control is quality assessment.
• Evaluation of the achieved quality. This step is necessary so that the results of the survey can be interpreted correctly, taking into account the limitations of the survey quality. This step is also important for the documentation of the experiences, so that similar problems can be avoided in future surveys.
11.1 Adequate overall management
A well-defined survey organization is essential. This includes a management structure, clearly defined responsibilities of the survey personnel and professional coordination.
A careful risk analysis helps the survey management to anticipate and prevent many problematic situations, which could otherwise have serious implications to the quality of the survey. Risk analysis could be performed in the planning stage of the survey and reviewed periodically during the survey. The risk management strategy is initially tested during the pilot phase of the study as a forerunner of the risk analysis to be applied on the full-size survey. Based on this feedback, the risk analysis for the actual survey will be modified and improved.
11.2 Agreement on survey procedures The manual describes the procedures to be used in the national HES, which are standardised based on European guidelines.
Whenever a procedure deviates from the European recommendation, the issue needs to be discussed with the EHES RC. The decided deviations together with the justifications need to be documented in the survey manual.

46
11.3 Training Training is needed for acquiring the skills to follow the survey procedures. The survey’s coordinating centre (HHF) is responsible for training the survey personnel. Specific training is necessary in particular for the persons performing measurements in the field. If the fieldwork is expected to last for more than few months, re-training sessions may be needed. Re-training will reinforce the use of the standard procedures.
11.4 Piloting the HES Piloting the HES and detailed evaluation of the pilot is crucial to ensure a successful data collection and fieldwork phase of the HES.
The HHF carried out a pilot survey prior to the full-size Greek HES. The purpose of the pilot survey was to evaluate the entire survey process and to obtain additional information for the planning of the actual survey. The pilot survey also helped in making the fieldwork personnel familiar with potential practical problems.
The aims and content of the pilot survey depend on the contents of the survey, previous experience and frequency of surveys. The following issues need at least be considered:
• Identifying the need for further quality assurance activities, such as further specification of the recruitment, measurement and training procedures. This facilitates planning the training of the survey personnel and finalizing the survey manuals.
• Getting feedback from the invited participants. This may concern the willingness to participate, recruitment process and information leaflets, informed consent and experiences on the measurements. It is also useful to observe the respondents' reactions. The feedback is needed to develop different ways to motivate participation in the population.
• Recording timing and calculating average duration of interviews and examinations per participant. This is needed to estimate the need for personnel resources (which has implications to budgeting) and potential burden to participants.
• Testing the use of equipment, computer programmes, data management, and the processing, transferring and storing of blood samples. This is needed to avoid problems in data and sample collection and management and to assess the need for storage space, equipment and logistics.
• Familiarizing staff with potential practical problems. This helps to avoid problems during fieldwork, and may give rise to refine practices and add further specifications to the national HES manual.
The questionnaire is evaluated in regard to:
• the length of recall period, • clarity of concepts and definitions, • the question wording and the response alternatives, • the sensitivity of topics, • the questionnaire layout, • the choice of administration mode, and

47
• the respondents' burden. An optimal timing for the pilot survey is 3-6 months before the full-size HES, so that there will be sufficient time to evaluate the pilot and to make the necessary adjustments to procedures before the full-size survey. The Greek HES was initially planned to use data from the Census of 2001. However due to the several limitations occurring during the pilot phase, it was decided to wait for the completeness of Census 2011 in order to benefit from the utilization of most recent data. Consequently, the recommended time period between the pilot (based on Census 2001) and the full- size (based on Census 2011) surveys could not be achieved. The pilot survey in Greece was conducted by the personnel who will be involved the full-size survey which is to be conducted in approximately one year after the completion of the pilot.
11.5 Quality Control The term "quality control" refers to the measures taken to monitor the survey process so that any problems can be detected at an early stage. Well-planned and conducted quality control will save resources as it is expected to minimize the time and resources needed for detecting and solving problems and for repeating tasks. It will also minimize the need to reject survey data because of data loss or poor quality. Quality control is also needed to convince the users of the data about their good quality.
11.5.1 Quality control of the planning of the HES
The main quality control activities of the planning stage are: • to check that the plan for the preparatory phase of the survey covers all relevant aspects with
sufficient detail; and • to monitor the time schedule of the planning and preparatory phase.
The EHES RC assists the coordinating centre (HHF) on the organization of the Greek HES.
11.5.2 Organizing quality control for the survey procedures Most of the quality control of the Greek HES is carried out by the survey’s Advisory Committee. This is called internal quality control. In addition, it is important to have the survey observed and assessed by an independent outside body. This is called external quality assessment.
11.5.2.1 Internal quality control In principle, quality control is relevant for all phases where data are transferred from one form or place to another. Therefore, quality control is relevant for:
• the interview and measurement instruments and procedures, • data and sample handling and transfer, and • the data management.
A wrong remedy may add a new component to the measurement bias. For measurements which involve a subjective component, such as interview or blood pressure measurement, the way of

48
approaching the measurer needs to be planned carefully in order to prevent over correction. The best action can be for example a routine retraining of all personnel performing that measurement.
The activities of internal quality control within the Greek HES is documented in a log book, together with any concerns detected and the action taken to correct problems.
11.5.2.2 External quality assessment
External quality assessment is never a substitute for the internal quality control. It complements the internal quality control by providing an independent review of the performance, checking that the national standards are similar to those of other European countries and over time, as well as overseeing that the internal quality control functions as planned.
The EHES RC coordinates and carries out external quality assessment in EHES. Additional sources of external quality assessment are used in the Greek HES, such as the evaluation of the Greek HES organizer (HHF) from the Hellenic Organization for Standardization (www.elot.gr). The EHES RC is informed of this.
11.6 Evaluation of the achieved quality
The evaluation and documentation of the achieved quality involves analytical investigation of:
• the actual survey procedures used, • the data generated in the survey, and • the data and information generated though external quality control.
The evaluation report is an essential prerequisite for the analysis and correct interpretation of the survey data. As part of the planning of the survey, there is a need to ensure that the data collection in the survey includes all data needed for the evaluation.

49
12. Data management A well-organized data management is an essential part of a HES. It must be designed to ensure the following:
1. the data will be available for analysis and that the available data should be
• complete. No data collected from the survey participants should be lost. • correct. Only justified differences between the values which were originally measured and
the values in the final data storage should exist. • verifiable. The relationship between the original data collected and the data in the final data
storage should be well documented and described.
2. the data analysis will be:
• done using the correct data and other information which are relevant for the data analysis. • done without errors. • documented in such a way that the whole analysis or a part of it can be repeated later. If the
documentation is not done properly, it may be difficult or impossible to reach the same results when similar analyses are repeated in other situations.
3. the confidentiality of the data must be secure.
Point one above involves data collection, checking of data, error correction, data transfer from the field to the final storage (database), documentation and back-up of the data. Point two concerns analysis of the final data to obtain survey results. Separation of the data management into these two stages is recommended and a well-planned data management facilitates the availability of good quality data for analysis.
Therefore it is necessary to create a detailed plan for the data management including all phases of the survey.
12.1 Basic work and data flow
When organizing the management of the Greek HES data, the following topics have to be considered:
• sample selection and recruitment of participants • scheduling appointments • collecting the survey data • error checking, correction, and documentation of the data • transfer and storage of the data.

50
A database to store the collected data has to be designed, developed and maintained locally in the country, complying with the laws underlying data protection. The database needs to be prepared to store individual level data on the national HES measurements (including the questionnaire part), information on the quality of the data, as well as sampling data of each survey respondent.
12.2 Subject Identification
The subject records in the Greek HES need to be identified using multiple-level coding. For instance a recommended system of a four-level codification should include: EHES: To specify that the survey is a part of the EHES framework.
COUNTRY: To identify the country of the survey, using the EU-coding. Greece is EL
SURVEY: A two-digit number code to identify different EHES-surveys in the country. It should be confirmed with EHES RC before applying.
SERIAL NUMBER: To identify the different individuals selected to participate. It must follow to the following principles: SERIAL NUMBER is given to everybody selected to the sample (i.e. not only to those eventually found eligible or to the survey participants) It is unique within the survey. Only one person selected to the survey can have the same SERIAL NUMBER. The maximum length of the SERIAL NUMBER is 12 characters. Because errors in the SERIAL NUMBER usually lead to a loss of the record, it is strongly recommended that the SERIAL NUMBER includes a check digit (or check digits). The serial number should not include information which makes it possible to identify the person in the population.
12.3 Data sources
12.3.1 Sample selection, recruitment and appointment scheduling
12.3.1.1 Sample selection The first major data management issue relates to sample selection and recruitment. Τhe following information needs to be recorded for every individual selected for the sample:
• SERIAL NUMBER, which should be given to everybody selected to the sample and used to identify the individual throughout the survey and data management.
• Sampling information. • Contact details, such as the person's home address, telephone number and any other
information useful to contact the person. • Additional information, such as sex and age are also often available from the sampling
frame.

51
The individuals selected to the sample form the basis for the control of the data completeness through the data management process. The survey history of every individual should be verifiable from the final database.
12.3.1.2 Recruitment
At the recruitment stage, attempts made to contact each individual need to be monitored and the outcome of the recruitment needs to also be recorded. For each person invited to participate in the Greek HES, a record of the following information needs to be kept:
• Eligibility status • Number and type of contact attempts • Contact status • Participation status • The reason for non-participation
12.3.1.3 Scheduling appointments Organizing the appointment schedule is closely linked to the recruitment phase. For example in a case when an appointment was fixed, but the subject was unable to participate to the survey, this changes not only the appointment schedule, but also the participation status (or even eligibility status) in the recruitment data.
In this case the following information should at least be logged:
• The subject identification (see Section 12.2) • The contact information (name, address, phone number) • The appointment information (time, place) • The recruitment information (the record of participation)
Regarding the future surveys it might also be important to keep a record of changed appointment times. Appointment scheduling should keep track of all appointments and related data. There are several commercial applications for scheduling; some of them are web-based services, while others are standalone client software.
12.3.2 Survey data
12.3.2.1 Sources Recording the survey measurements and gathering data from different examination sites to the common database are essential parts of the national HES data management. The following should be included:
• completed interviewer-administered questionnaires • values of physical measurements • biological sampling, processing and transfer to the laboratory • recording the laboratory results

52
• transfer of paper forms and/or electronic records from the examination site or laboratory to the common database
• getting the data into electronic format Three main challenges for the data management during these steps are to ensure that:
• no errors are made in recording the results; • the data records are complete; • no records are lost neither are different persons' records mixed up.
Errors and incompleteness of the records are prevented by good design of the record forms and by routine checking of the forms and the data. The earlier the errors will be detected, the easier their correction is. When feasible, detection of errors should be done when the subject is still at the examination site.
Relevant data which are not obtained from the subject should not be left blank, but a specific code for missing data is used. Subsequently, the incompleteness of the data can be detected as blanks in the data forms.
To prevent the loss of records, it is important that the subject identification is correctly recorded at all stages and the Subject Identification code is used. Laboratory samples (biological samples, storage tubes and storage boxes) are also labeled with bar codes with a reference to the correct Subject Identification code.
12.3.2.2 Forms of data collection The Greek HES (implemented by HHF) will apply computer-assisted data collection. In addition, the system was tested in the pilot study conducted by the HHF and was found reliable. Nevertheless, paper forms are always on hand as back-up in case of power failure or other problems with computer devices. In computer-assisted data collection, provisions need to be made for automatic built-in checks for responses, in order to reduce the possibility of errors during data entry.
12.3.2.3 Preparation of the fieldwork The preparation of the fieldwork phase includes:
• Planning of the data management and data transfer system for the fieldwork (i.e. computers, network, software, and other equipment needed) and testing these
• Arranging the training, responsibilities and support of fieldwork teams. Things that require particular attention are data security, data transfers, and back-up of the data to avoid any losses of data in case of a system flaw. Questions arising are:
• Shall a private LAN/WLAN be established for each fieldwork team? • What computer equipment will be needed?

53
• What software will be needed? • Planning software update procedures during the fieldwork • Planning data back-up equipment and procedures • Planning the transfer of the data • Data security (locking of computers, usernames and passwords to access the computers,
encrypting data on computers, how to store paper forms on the field, etc.)
Regarding the software all workstation computers are recommended to be identical to each other and thereby easy to replace if broken. Server computers (if any) in the fieldwork can be designed to be stand-alone, independent portable computers, easy to relocate or replace in case that one of them is broken. A backup mirror can be implemented between servers, in which case the data on the first server are copied to the second one.
The equipment and data transfer and storage systems should be tested thoroughly prior to the training of fieldwork personnel. Time needs to be reserved both for testing and analyzing the test results.
12.4 Error checking, correction and documentation of the data
After the data collection the data should be checked as soon as possible for:
1. strange values, i.e. for values which have not been defined, and also for values which are possible but rare;
2. consistency between the values of different data items; 3. completeness, i.e. that all data items have been recorded and no records have been missed.
When potential errors are detected, they should be investigated for correctness, and corrected only if it is found that they really are errors. It is advisable to authorize only those who have made the errors to correct them, since they are usually in the best position to tell if there is really an error and are often the only ones who know the correct value. Each error and its possible correction should be documented.
The frequency of errors, which were not possible to remedy should be documented. The same concerns the results of the quality control during the data collection, any deviations from the survey protocol, and any other information which may be relevant for the interpretation of the results. Knowledge of these issues is essential to those who analyze the data and interpret the results.
Each data transfer and import into the central national HES database should include at least a routine check for each data variable.

54
12.5 Transfer and storage of the data
12.5.1 Data transfer and interface to import the data
Data transfer and import into the national HES database depends on whether the data are collected using computer-assistance or manually by using paper forms. Whenever data or samples are transferred from one place to another, it is important that the data transfer is logged properly. All data transfers should be traceable whether they are computerized or manual. The recipient of the data or samples should be able to check that he or she has received exactly the same records which were sent and the person sending the data should make sure that everything was received. The transfer of the data into the central data storage, the national HES database, should be done regularly and via a secure data transfer medium.
Good ways to transfer computerized data are through Internet via a secure connection and data encryption or by storing data on disks delivered via a secure mail. The final data storage should be completed through a user interface that integrates the following options:
• Web application - a dedicated web software should be designed to interact with the national HES database or other database from which the data are further transferred into the national HES database. This kind of an application typically functions on the clients' web browser.
• Standalone client PC application, operating on dedicated computers. • Other - e.g. direct import from data files. The data will be delivered to the HES coordinating
centre (HHF) on a dedicated medium from which data files are uploaded into the central HES database.
12.5.2 Data security
The core principles of information security are data confidentiality, integrity and availability regardless of the form the data may take: electronic, print, or other forms. (Table 12.2)
Table 12.1. The principles of data security
Security principle Description
Confidentiality
Ensuring that information is accessible only to those authorized to have access. This is necessary for maintaining the privacy of the people whose personal information the system holds and to prevent the disclosure of information to unauthorized individuals or systems.
Integrity
Safeguarding the accuracy and completeness of information and processing methods from intentional, unauthorized, or accidental changes. Maintaining data integrity is essential to the privacy, security, and reliability of the data. Data integrity can be compromised by malicious users, hackers, software

55
errors, computer virus infections, hardware component failures, and by human error in entering or transferring data. Therefore, the access to protected information should be done only through proper identification and authentication of the users.
Availability (the degree to which the system is operable)
Ensuring that authorized users do have access to information when required, i.e. the information is available. This can be accomplished utilizing data back-up plans and continuity/recovery plans.
To ensure data confidentiality and integrity it is necessary to use technical controls - e.g. passwords, network firewalls, access control lists, and/or data encryption - to monitor and control access to the computing systems and collected data. Only authorized persons should have access to the subject’s personal identification code and data and all of them must understand the importance of the confidentiality of the data. After data collection, the information from which a person can be identified and the code which connects this information to the subject identification of the survey records, should be stored separately from the survey data, and maintained e.g. on encrypted hard drive. Normally only few people need access to the person identification information, whereas the rest of the survey data will need to be accessed by all who analyze the data. Specific precautions should be defined for the handling and storage of paper forms in the examination site and elsewhere when these are used.
12.5.3 Back-up
All data in electronic format should be routinely backed up. During the fieldwork in the pilot study undertaken by HHF, secure connections providing Remote Desktop capability to the interviewers were tested. Through this technology all the data are already in the server and the local computer is acting as a terminal only.
Back-ups are needed not only for data in electronic format, but also for important paper documents, such as log books of the survey examinations.
12.6 Recommended standards, techniques and tools
12.6.1 Database
The national HES database will be structured and implemented using a well established database management platform designed for scalability and extensibility.

56
12.6.2 Development tools, use of statistical software and XML Several programming languages and development environments, as well as dynamic web content technologies exist to be used to implement an appropriate application logic and user interface for the national HES database ranging from Java to .NET solutions. The choice will depend on the local facilities, existing practice and the expertise available.
It is recommended to use the XML-based general standards when implementing dynamic web content output and/or interchanging data over the Internet. In the survey data analysis it is recommended to produce analysis and reports by a well-established statistical software, such as R or SPSS.
12.6.3 Data encryption The system should enforce security through data access control and auditing:
• Access control to restrict access to the data. • Auditing to log the actions and changes which have been performed, when and by whom.
Data encryption may be necessary. To secure and encrypt data connection e.g. the following techniques can be used:
• SSH (Secure Shell network protocol) • SSL (Secure Sockets Layer) or TLS (Transport Layer Security) • AES (Advanced Encryption Standard) • Blowfish (Fast block cipher)
A web application can be built on an information server with SSL/ TLS support to ensure encrypted connections to the server. Recommended protocols for data transfer between client and web server are HTTP/ HTTPS (by SSL/ TLS) and FTP through SSH.
12.7 Local data management and the EHES Reference Centre
The collection of anonymous individual level data from each country to a centralized database at the EHES Reference Centre is necessary for data quality assessment and for assessing the success of the standardization and documentation of country-specific characteristics of the data. Collection of data in one database also facilitates the joint analysis and reporting. For instance, a database at the Pilot EHES Reference Centre has been established for this purpose to store individual level data on EHES core measurements and to serve as the central repository for the data, used for evaluation of the surveys and for analyzing the survey results.
The data exported from the national HES database will be transferred in an XML format using services offered by the EHES Reference Centre data transfer and management system depicted below. The system will allow checking of the data variables for accuracy and consistency locally in

57
the country before sending. It ensures security and confidentiality of the data and provides secure data transfer on Internet by enforcing a dedicated user authentication and security protocol with data encryption.
12.7.1 Services offered by the EHES Reference Centre's data transfer and management system
A) Services for data management and transfer
• storing, retrieving, updating and reporting descriptions and data on the survey procedures in each country
• uploading, updating and retrieving of individual level data on the EHES measurements B) Checking the data to be imported
• checking the individual level data on the EHES measurements locally in the country before uploading these to the EHES data management system. This data check is formal (e.g. checking that given data conforms to a certain value range) and does not involve data analyses.
• creating a report on the data checking C) Generating reports
• producing tables/figures for the survey evaluation and data quality assessment • producing tables/figures for the basic reports on results of the country
12.7.2 The architecture of EHES data transfer and management system The general architecture of the EHES data transfer and management system consists of three main parts:
• Web Application • Data Checking Application, and • Reports Application

58
13. Recruitment of participants A high participation rate is fundamental to the reliability and validity of results and conclusions drawn from the HES. The participation rate strongly depends on the success of participants’ recruitment. Furthermore, proper recruitment is necessary for the HES to be ethically acceptable. This chapter describes the recruitment process of individuals sampled to participate in the Greek HES.
13.1 Recruitment process
The purpose of the recruitment process is to ensure as high participation rate as possible. The recruitment process includes all stages where selected participants are contacted to provide information and to make appointments to examination visits.
13.1.1 First contact attempt The recruitment process is as follows:
1. An invitation letter is sent to the sampled individuals. In brief, this letter describes the objectives and procedures of the survey and how the way the individual was selected. It also addresses confidentiality issues, lists the benefits of participation participants and provides information on practicalities (e.g. contact information for scheduling an appointment).
2. An information leaflet is sent together with the invitation letter
3. One to two weeks after the invitation letter is sent (depending on the mail delivery system in each region) the team member, responsible for the participants’ recruitment (usually a health visitor) arranges an appointment through a telephone contact.
13.1.2 Re-contact attempts If the first phone call is not successful for recruiting the selected person, additional calls are made as long as the data collection is ongoing in the area. The selected person is identified as not contacted if all attempts to contact the person or next of kin are unsuccessful by the time the data collection is completed in the specific area and the fieldwork team leaves the region.
If the participant refuses to visit the study center, examination at a mobile unit or home visits are provided as options. If a selected person refuses to participate in the survey, this is respected and recruitment attempts end at that point.

59
Substitution of a non-contact with, for example, a neighbor or a person with similar characteristics (e.g. of the same gender and age), is not acceptable. Obtaining information from proxies is generally not acceptable (e.g., information on health issues provided by the spouse), unless the participant cannot be reached or is unable to answer because of limited cognitive functions for instance.
Figure 13.1 summarises the different stages from the original sample to recruitment of a survey participant.
Original Sample
A) Invitation letter
B) Telephone contact (additional calls as long as data collection is ongoing in the area)
Contacted Not contacted
•Invitation returned
Eligible
Not eligible
• moved abroad
Participant Non‐participant
•Refusal
•Unable to arrange an appointment
•Appointment made-no show up
•other
Figure 13.1: From the original sample to the survey participant 13.2 Participation rate
Participation rates are calculated separately for the interview/questionnaire administration and the examinations, whenever feasible.

60
13.2.1 Definition of participation A person is coded as
• contacted if: o a successful contact has been made by phone and/or o the person itself drops in after letter delivery and before telephone contact.
Each person will be asked if (s)he has read the invitation letter. A person is coded as:
• not contacted if the invitation letter was returned to the central office and/or contact through phone was not possible.
A person contacted is coded as
• eligible or • not eligible depending on whether (s)he belongs to the target population.
If after contacting a person, it becomes evident that (s)he does not belong to the target population (e.g. outside the sample’s age range) this is noted. A large proportion of non eligible individuals provides indications on the quality of the sampling frame.
An eligible person is coded as
• participant if (s)he has at least one valid measurement, such as height and weight, in addition to some questionnaire results.
• Non-participant is an eligible individual, who refused or otherwise did not participate after the invitation was assumed to have been received and/or other contact was established. For each non-participant a record of the reasons for refusal is kept.
The formula to calculate participation rate and other fractions including co-operation rate, refusal rate, non-participation rate and non-contact rate are shown in Table 13.1. Participation and contact rates do not include not eligible individuals. Persons who were temporarily absent during the data collection period are included in the denominator, as they form part of the target population.
Table 13.1 Calculating participation rates
Participation rate = number of participants / number of eligible AND unresolved individuals
Co-operation rate = number of participants / number of eligible individuals
Contact rate= number of eligible individuals / number of eligible AND unresolved individuals

61
The co-operation rate is higher than the participation rate and provides an estimate of how willing contacted individuals were to participate to the survey. The difference between these two rates informs us about the quality of the sampling frame and contact efforts.
13.2.2 Target participation rate The ultimate goal during the recruitment process is to obtain the highest possible participation rate so that the sample is representative of the target population. The participation rate should be at least 70% (but preferably higher). If participants appear to differ from non-participants on important variables such as health factors, the rate should be closer to 80% or over.
13.2.3 Ways to increase participation
13.2.3.1 Selection and training of personnel • The personnel involved in recruitment needs to be competent and highly motivated. • Sufficient training is provided to the personnel, including instructions on how to treat
potential participants in a professional, friendly, respectful and caring manner. • Proper training to manage telephone calls is also important
13.2.3.2 Factors affecting participation rate Participation is enhanced through offering a degree of flexibility. Re-scheduling an appointment, offering appointments on weekends, possibility for selected persons to drop in without an appointment and easy access to the examination site are examples of alternative options. Some indicative factors that may also affect the participation rate are:
• Relevance and importance: Highly relevant surveys raise the participation rate • Personal fulfillment: The feeling of being valued and appreciated affects to the willingness
of the individual to participate. Furthermore, having the invitation letter signed by a respected person in the field of public health is expected to increase this feeling of being valued.
• Requests for help: The phrase "it would really help us..." is used in the invitation letter and is repeated during the contact attempts in order to appeal to people that tend to follow a norm of social responsibility and are usually more willing to take part in a health survey.
• Leaving messages on telephone: Staff members who will contact participants by phone are advised to leave messages on an answering machine, as it has been noted to increase participation especially among women of upper socioeconomic class.
13.2.3.3 Partnership for enhancing participation Partnership and collaboration with local organizations, professionals and communities help to raise awareness on the importance of the survey, and to arrange easy access to the examinations. In particular:

62
• the participants’ employers are encouraged to allow their employees to participate in the survey during working hours
• co-operation with regional or local hospitals, non-governmental organizations, research centers and universities may increase the interest in participation
• national and local health authorities and health professionals are informed prior to the survey
• governmental organizations are notified to ensure the community's understanding and support
• the public is notified using mass media around the same time that the invitations are sent. 13.3 Non-participation
In order to assess the non-participation bias, it is important to collect information on non- participants to evaluate potential biases in estimates. Whenever someone refuses to participate a non-participant questionnaire is recommended to be filled in from survey personnel through telephone interview. The questionnaire could include questions on the individual’s sex, age, highest educational level, health condition, height, weight and smoking habits.
13.4 Data to be recorded
For each individual invited to participate in the HES, a record of the participation status is kept. In this record, the number and type of contact attempts are entered.
• If the person is contacted, records are kept on whether the person participated, refused or dropped out after having agreed to participate. Information on completed and not completed participations is also kept.
• If the person refuses to participate, the reason is written down if provided by the person.

63
14. Dissemination and publicity The terms dissemination, communication and publicity are closely linked and are often used interchangeably. In the present document, the terms are defined as follows:
• Dissemination is the transmission of the information to the public without direct feedback
from the audience. Dissemination can be for example a seminar presentation, newsletter or a newspaper article.
• Communication refers to the activity of conveying meaningful information in the way that
there is specified sender and an intended receiver of the information/message. The difference between dissemination and communication is often blurred.
• Publicity is the deliberate attempt to manage the public’s perception on the issues.
Promotion of the survey can be considered as a form of publicity. Dissemination, communication and publicity form integral parts of a HES. Through these, survey organizers keep all stakeholders informed about the survey plans, progress and outcomes.
The dissemination of information can have four objectives:
• to increase knowledge, • to instruct, • to facilitate informed decision making, and • to persuade.
14.1 Why is dissemination and publicity needed?
Dissemination and publicity are needed to:
• Support the decisions to carry out the HES by effectively communicating its benefits o Support the fund raising
• Support the collaboration with local authorities by constructing active lines communication • Motivate the invitees
o letter of invitation o General public - information about the HES, health topics to media and public
discussion o NGOs (employer organizations, trade unions, GPs, etc.)
• Disseminate and marketing results to: o participants o funders o general public o policy makers o health care authorities

64
o NGOs o scientific community
14.2. Target groups for dissemination
The groups to be targeted in the dissemination/publicity process and the key stakeholders whose support or consent is essential to successfully carrying out the HES may include (in alphabetical order):
• funders, • general public, • health care authorities, • health care personnel, • individuals invited to participate, their relatives, intimates • media, national and regional • non-governmental organizations (NGOs), • policy makers • the research community.
Funders are needed in order to be able to conduct a national HES. There can be different kinds of funders for the survey. Often, the core part of the survey, which is mainly used for the health monitoring in the country is funded through the national ministries. Potential funders need to be informed about the survey plans well in advance in order to make informed decisions in time. Nowadays some funders require a dissemination plan for the projects they consider funding as part of the application.
The general public is a key partner in the HES. Informing the general public about the survey may increase awareness and through that, enhance participation rates.
Collaboration with local health care centres, general practitioners and physicians is needed when conducting a national HES. Local physicians should be kept well informed about the survey since people invited to participate may contact their own physician to ask more about the survey and seek their advice on whether they should participate.
Media is not directly gaining from the HES but they are delivering information about HES to other stakeholders.
NGOs like health-related foundations and associations are survey stakeholders for a number of reasons. They can be partial funders; they have channels to distribute information about the survey to the general public; and integrate survey results to prevention activities.
National health policy makers, regional health authorities, or heads of local health care centres need valid and reliable information about the health behavior and health status of the population. Since the HES will provide representative and reliable health information, policy makers in all levels are

65
considered as important end-users of the results. Often policy makers, like ministries of health are also funders of the HES.
The research community can have valuable input to the survey’s content and methods. Also after the survey is completed, the research community is needed to analyze the results and disseminate the findings to the research community for further use.
14.3 Message to disseminate
The message to be disseminated depends on the target group. Messages need to be easy to remember and repeated in various situations so that members of the organizing team are all providing a consistent and coherent message.
The letter of invitation should provide the information the invitees need before giving their consent. A leaflet can easily be annexed to the letter of invitation, and it is a useful way to give basic information to the survey’s stakeholders:
14.3.1 Examples of messages Key messages used in a national HES may for instance be:
• Health surveys are vital for understanding the health situation and behavior of the population and they provide evidence-base to construct health policies.
• Identifying health differences between population groups is a prerequisite in the effort to narrow health inequalities
• To support healthy aging we need to know the current health status of adults and children. • The national HES is conducted by a reliable authority, the methods are secure and science-
based, and the results do not serve any other interests but the public benefit. • Information about people’s health is vital to building an efficient health care system geared
to the population’s health needs and that of their families. Each individual’s contribution is important in making the study representative.
• The physical examination will complement data collected through other health questionnaires and registries.
14.4 Brand building
To help the dissemination and increasing the awareness about the national HES, it is important to pay attention on how the survey is represented. This includes all survey materials prepared and distributed, as well as messages given out from the survey. This can be considered as a brand building of the national HES.
The brand of the survey is used to identify the survey from others. The brand building intends to provide a uniform and professional message and image about the survey.

66
This includes issues like: • name of the survey, acronym • logo of the survey • slogan • colors to be used in survey materials • fonts to be used in survey materials • template for the presentations (e.g. PowerPoint) • template for other published materials
o letters o posters o questionnaires
• web site layout • image of the fieldwork team (name tags, possibly clothing) • signs how to come to the examination site
14.5 Means of dissemination
After defining the messages to be conveyed as well as their potential recipients, the most appropriate means of dissemination need to be chosen. There are numerous ways to disseminate the information about HES. In particular:
• face-to-face discussions, • seminars, • letters, • leaflets and brochures, • newsletters, • press releases or press conferences, • web sites, • social media, • posters, • reports, • TV and radio advertisement, • information desks on public places,
In a public health examination survey the availability of basic information about the survey is critical. Easy access to good quality information will bring about confidence in the survey, as well as attracting the attention of stakeholders. Thus, the quality of the most important outputs (e.g. the invitation letter, the HES leaflet, the survey website and press material) needs to be maintained.
Quality in dissemination is measured by how clear and relevant the messages are for the interests and concerns of the selected target groups.

67
In areas where computers and the internet are widely available, a website or a blog are preferable ways to provide basic information. If, however, the website or the blog are poorly developed, the impression could easily be that the survey is not being done in a professional manner. The websites of collaborating organizations could serve as a solution to communicate to different target audiences.
The media culture differs from one country to another and it’s important that a skilled communication officer is included in the survey’s team. Reporters, in an attempt to serve their audiences, keep an eye on authorities, national or international. In this context, it is essential to state the benefits to the country in press releases so that the concrete benefits are visible and relevant to the average citizen.
Likewise, possible negative press should be anticipated. The main message to the media, should be flexible but focused for the whole survey duration. Consider organizing a press conference so that the survey catches media attention or if it appears to have been misunderstood or misrepresented.
If these means of communication are inadequate, the following means can be considered:
• telephone information service to the participants • radio broadcastings, advertisements or supporting programmes • roadshows, information desks in public places, etc.
14.6 Dissemination plan
All the aforementioned elements should be put into a concrete time scale, indicating what will be done, when and by whom. A pre-prepared dissemination plan helps to ensure that the dissemination is done properly, in a timely manner and without giving rise to constant concerns. The survey management or other person defined for this task has to follow up the implementation of the dissemination plan.
The outline of the dissemination plan could be:
1. the role and main objectives of dissemination in the national HES. 2. key messages. What is the message to be disseminated in different time points to different
target groups? 3. key target groups for dissemination. 4. means of dissemination. 5. time scale and concrete actions. 6. organization of dissemination. Who will do what, when and how.
Dissemination is a strategic part of the survey and may contribute to the success or failure of the entire project. Successful project leaders are fully committed to the goals of dissemination. It is usually beneficial that the national survey team includes a skilled communication officer who has an overview of the dissemination strategy of the HES. Her/his duties may include:

68
• preparation of the dissemination plan; • follow-up of the implementation of the plan; and • contacts with the media.
14.6.1 Active vs. passive publicity Decision about the publicity strategy should be made at the same time when preparing the dissemination plan. Are we targeting actively for publicity or do we have more passive strategy where we wait and see what comes out?
14.6.2 Preparing for unintended publicity In case of unintended publicity, which quite often is negative, there should be a plan on how to react. This plan should include information about whom from the team has the main responsibility to respond to the unintended publicity. This responsibility may be divided to several persons (e.g. by topic). In all communication, the response should come openly and timely after the unintended publicity. Do not start hiding the issue but confront it calmly with facts. Make sure that the message is the same all the time regardless on who from the team provides it and on which forum.

69
15. Training program This chapter outlines key issues that need to be considered when planning and preparing the national training program for the staff of the Greek HES, including the staff from the local examination centers who take part in the data collection. The details of the training program need to be decided in the early stages of the survey planning, since they affect the survey budget (training costs) and are central in the timing, standardization and quality assurance of data collection.
15.1 The training program of the European HES
In order to ensure standardization and share experiences between countries, the EHES training includes two dimensions:
• Europe-wide training seminars for the persons responsible for planning and organizing the
national HES and for those responsible for training of the national survey personnel, and • Outline for the training of the national survey personnel actually conducting the survey,
which is to be conducted nationally.
In this context, the EHES training program includes three training seminars. In particular:
1. Training seminar covering issues relating to the planning and preparing for the EHES at national level.
The target group for this seminar includes those who plan and prepare national surveys in EU Member States and EFTA/EEA countries. The objective of the seminar is to train the participants for planning a national HES according to the EHES standards. Other objectives of the seminar are to raise awareness on EHES in all European countries, to receive feedback from the participants on the EHES standards and the EHES Manual, and to discuss possible national adaptations.
2. Training seminar covering issues relating to the fieldwork of the national health
examination surveys.
The target group for this seminar includes those who will train the national fieldwork team members in each country. The objective of the seminar is to promote the use of the standard EHES training materials and to otherwise ensure that the training for the fieldworkers will be organized following the EHES standards with a focus on core measurements.
3. Training seminar focusing on data analysis, reporting and dissemination of results.
The target group of this seminar includes statisticians, researchers and survey organizers responsible for the data analysis, reporting and dissemination of the results. The aim is to

70
promote comparison of the national results, to develop European level reports and to support both national and European dissemination of the results.
The first two seminars have already been organized in the context of the EHES pilot Joint Action and were attended by HHF staff, participating in the pilot.
15.2 The national training program
The training program of the Greek HES aims to:
• inform members of the staff about the EHES standardized procedures • inform members of the staff about specific characteristics of the Greek national HES • allow practicing international and national procedures in role playing exercises.
All members of the national survey team, both those working at the central office and all fieldwork staff members have to participate in the national training programme. It is essential for the quality of the survey that everyone, including secretaries and assistants working at the central survey office, those who contact the selected persons, send the invitations and schedule the visits, data managers, statisticians and all fieldwork staff members know and understand the aims of the survey and the whole data collection process. A recommendation, therefore, for all staff members is to read the survey manual before attending the training seminars.
15.2.1 Outline for the national training seminars The outline of the training seminars for the Greek national HES presented below are based on the training seminars organized and implemented by HHF staff through their participation in the EHES Pilot Joint Action, as well as the experience accumulated through the conduct of the EPIC-Greece investigation, a prospective cohort study including extended data collection among more than 28,000 individuals all over the country.
The national training programme includes both general issues for all staff members, general fieldwork skills and practices for the fieldwork staff, and specific training for each selected measurement. For staff members with previous experience in collection of similar data, some parts of the general training may only be short refresher lectures. Practical measurement sessions are needed also for the experienced staff members to ensure that the standards are followed correctly.
The training seminars cover the following issues:
• Background and aims of the survey • Ethical issues and confidentiality • Random samples and the importance of high participation rates • Standardization and quality assurance • Survey organization • Collaboration with the local health care professionals

71
• Communication skills, publicity rules and working with local media • Data management • Training on fieldwork • Safety of the fieldwork team members
In addition, the training of the fieldwork personnel carrying out the measurements should at least include the following:
• procedures for each interview module or instrument, • rationale why these measurements are taken, information on measurement techniques,
including practical training and certification, if needed, • giving feedback to participants concerning measurement results.
15.2.2 Procedure, Duration and Timing of the training Every new staff member needs to be trained on survey procedures. The training procedure includes:
• theoretical training (how to approach the participant and how to take an interview),
• a real interview is carried out in the presence of the instructor, • practicing an interview alone.
Feedback sessions between the members of the fieldwork team are regularly carried out to:
• ensure standardization, • discuss arising problems • exchange ideas on problem-solving.
The program is targeted to all survey staff, including:
• laboratory experts • IT (information technology) experts • communication experts • the fieldwork team • the Project's Operational Management team
Training is always organized before the fieldwork starts and includes sessions for a minimum of two days and maximum two weeks. Some additional sessions may also be needed during the fieldwork. To allow substitution among fieldworkers when needed and rotating tasks, it is recommended that each team member will be trained to handle several measurements. Retraining during fieldwork should be organized if the fieldwork lasts for more than two or three months to ensure that standards are kept. Retraining is essential also if observer-effects or non-adherence to survey standards are observed.

72
15.2.3 Use of training materials and different training methods The survey manual forms the basis for all training material, which include:
• PowerPoint presentations. • Videos and photos on interviewing and measurement techniques. • Web-based education tools. • Lectures and open discussions. • Newspaper articles and reports from previous surveys, which may help to understand the
importance of the survey and how data will be utilized. • Interviewing skills: including rules for accepting proxy responses; reading questions
verbatim; recording answers correctly, especially in case of open-ended questions. • Role-playing exercises
All training material and learning tasks need to be kept in a discussion forum in the Internet (e.g. a specific survey extranet site), so that all staff members will have up-to date information available throughout the fieldwork period. Open discussions between all field work members and other survey staff members are encouraged during the training sessions.
15.2.4 Selection of the national trainers A national trainer should meet the following criteria:
• participate in the training seminars provided by the EHES RC or having followed training programs and being involved in national HES in at least two previous occasions.
• be well informed both on the aims of the national survey as well as on EHES standards (if for instance he/she is a member of the national survey project team).
• have specific expertise in the subject area (e.g.: survey ethics, blood pressure measurements).

73
16. Preparation of the survey budget The type and amount of resources needed to conduct a national HES depends on the number of survey participants, the measurements to be undertaken and the overall survey setting. The preparation of the budget has to ensure adequate resources for the planning, preparation, fieldwork, data analysis and reporting. The present chapter provides general principles in estimating the core costs of the different phases of the HES in Greece.
16.1 Calculation of the budget on the basis of the main stages of the survey
The following stages need to be considered when estimating the budget of a national HES:
1. Planning and preparation 2. Coordination 3. Training of personnel 4. Dissemination 5. Piloting 6. Sampling 7. Recruitment of participants 8. Fieldwork, including transfer of collected materials from the examination site to the
coordinating center/laboratory and in case of home visits, costs of fieldworkers when traveling from house to house
9. Laboratory analysis and sample storage 10. Data entry and cleaning 11. Quality assurance 12. Analysis and reporting
When the measurements to be included in the national HES are selected and the survey setting is decided, the time needed to collect the data of one survey participant needs to be estimated as it may be needed in the budget estimations.
16.1.1 Planning and preparations The main resource needed for the planning and preparation stage is personnel, including (for instance) senior researchers to advise on the selection of measurements and the preparation of survey questionnaires and manuals, IT experts, statisticians, experts on measurements, laboratory techniques, legal or ethical issues.
16.1.2 Coordination The core resources needed for the survey coordination is to cover personnel needs and basic equipment. The minimal personnel requirements for coordination include:

74
• Project leader • Project operational manager • Operational management team • Legal advisor • Financial administrator • Secretary
The coordination team needs at least computers with internet connection, telephones/mobile phones, printers, software licenses and office materials. In several cases, members of the coordination team may need to travel to the survey sites to promote the survey and monitor the work progress. The travel and subsistence allowances need to be accordingly budgeted.
When planning the needs for the survey coordination, it is essential to remember that the coordination crosses over the entire survey process and is an integral part of fieldwork.
16.1.3 Sampling In the Greek HES, sampling is performed by the Hellenic Statistical Authority in collaboration with the survey statistician. Therefore, the following personnel is needed:
• Survey statistician • Database manager to form a database where the sample information is stored.
Computers, software licenses and other costs to establish the survey database need to be considered in the survey’s budget.
16.1.4 Training The trainers, the trainees, the equipment needed and other costs like preparation of the training materials are budgeted in this section. Examples of experts that can contribute in training the fieldwork personnel include:
• Instructors on the physical examination procedures • IT support and/or data management person(s) to train personnel on how to use the IT
programs in the fieldwork and on how the data management is organized. • Communication expert to point out actions to promote the survey • Statistician to inform the fieldwork staff about the sample selection as participants on the
field may ask how they got selected to this survey. • Legal and ethical expert to explain the importance of data confidentiality and how to obtain
the informed consent.

75
16.1.5 Dissemination of information The survey’s Communication team is responsible for planning and supervising the survey’s dissemination strategy. For this section, budget may need to be foressen to employ a graphic designer who will prepare the survey’s brochure and other promotional material. Printing costs of promotional leaflets and other material, scientific congresses and other promotion events need to also be budgeted in this section. If incentives offered to participants to increase the participation rate include printed material, their costs need to also be considered.
16.1.6 Piloting The piloting process requires both personnel resources, equipment and other resources. For the personnel resources, at least the following is needed:
• Full fieldwork teams to conduct examinations of the pilot sample • IT support to assist with the computer programs in use on the field. • Laboratory personnel to process, transfer and storage of the blood samples and to carry the
laboratory analysis of the collected samples. • Data manager to handle the incoming data. • Statistician to assess and analyze the pilot survey data.
Other costs that may occur during the pilot are the printing costs of the invitation letters, phone bills, travel costs and subsistence of the fieldwork and coordination personnel and transportation of the material to and from the field. Additional costs for the pilot phase come from the evaluation of the success of the pilot and from possible needs to change the survey protocol, to correct the computer programs, and to re-train the fieldwork personnel.
16.1.7 Recruitment of participants for the full-size HES The recruitment strategy needs to be set and implemented with careful consideration to maximize the benefits of the survey taking into account national circumstances.
The minimum requirements for personnel for the recruitment of participants include:
• Assistant, responsible to prepare the invitation letters and mail them out • A designated person, named as the contact person who can provide additional information
and clarifications about the survey when a candidate participant requires that and who makes the required phone calls to arrange appointments at the examination site. Since phone calls may have to also be done outside the usual working hours, two designated contact persons are needed to work in different shifts.
• Data manager or assistant, responsible to ensure that the status of the recruitment and contacts is recorded to the survey database.
It is however recommended to set up a recruitment team at the stage of piloting.

76
Computers and software licenses are needed to prepare invitations. A telephone number to which survey participants can call for further information or to change their examination time needs to be established and its cost needs to be budgeted in this section. Costs for maintaining and updating the survey web site, personnel, equipment, and other relating costs have to be budgeted as well.
16.1.8 Fieldwork The costs for this phase of the survey need to include the cost of interviewers for the questionnaires’ administration. In cases where the examinations are conducted at the participant's home, the travel expenses for the fieldwork staff have to be adjusted.
For the fieldwork, at least the following personnel is needed:
• Full fieldwork teams to collect the survey measurements • A laboratory technician to administer the collection, handling and storage of the blood
samples as well as the communication with the Reference Laboratory • IT support to assist in the use of computer programs used in the fieldwork • Data manager to handle the incoming data
Although several of the needed equipment has already been obtained during the training and pilot phase, additional sets of equipment may be needed for the fieldwork teams.
Additional to personnel and equipment costs, the budget for the fieldwork needs to also consider:
• costs for the transport of materials to and from the examination site • transport of the personnel • accommodation and subsistence of the personnel during the fieldwork (if needed) • storage of material in the field (if needed) • data transfer • phone and internet connection • cost of the feedback to participants about their results.
16.1.9 Laboratory handling, analysis and sample storage for the Greek HES The blood collected in the field is transported to the laboratory for analysis and storage. A decision on what is analyzed immediately and how much of the samples are stored for future analysis affects the budget.
For the laboratory sample handling, the minimum personnel requirement includes:
• Laboratory personnel • Data manager to handle the incoming data from the laboratory analysis
In case of abnormal results, participants will be advised to contact their Medical Doctor for further consultation.

77
Τhe following laboratory consumables need to also be budged: • aliquot tubes, • pipettes, • storage track and • reagents.
For long time storage, specific tubes that endure -80oC, storage boxes and deep freezers of -80oC are also needed. For the deep freezers a security system to ensure the safety of the samples during power breaks or any other freezers’ malfunction need to also be budgeted so as to be installed. In addition, a log book of the stored samples is needed and has to be established.
16.1.10 Data entry and cleaning The survey data collected in the field have to be stored in the database. Data are collected directly through computer programs, (CAPI - computer aided personal interview) at site and the data are transferred to the central database. For data entry and cleaning, at least the following personnel is needed: Data manager to design, maintain and update the survey database Data manager to work on data checking and cleaning In case the signed informed consents and/or data forms are scanned, the scanning costs have to also be included in the budget. Computers, software licenses and server space needed for the maintenance of the database needs to also be considered in this section of the survey budget.
16.1.11 Quality control Quality control includes checking of the survey plans, training of the personnel, measurement quality control and site visits/audits during the fieldwork, checking of the data during and after the survey as well as laboratory quality control. Quality control should involve individuals who know well the activities being controlled, but are not in any way involved in performing these activities (to reserve impartiality).
For quality control, the minimum personnel requirements include:
• Senior researchers/epidemiologist who know the survey protocol well and can identify deviations from it
• Data manager to detect possible systematic errors in the data after being entered to the database and to perform basic checks in the data entered to the database
• Laboratory personnel to perform both internal and external quality control of the laboratory handling procedure and analysis
Computers and software licenses need to be budgeted in this section. There may be a need to budget some travel and subsistence costs for the personnel conducting the quality control during the

78
fieldwork. There may also be costs of the external quality control, such as for laboratory measurements.
16.1.12 Analysis and reporting This section includes costs to report results back to the survey participants, the funders and other stakeholders, general public and the scientific community.
For the data analysis and reporting, at least the following personnel are needed:
• Data manager to maintain and share the survey data • Statistician to conduct the statistical analysis • Researchers to set out the research questions to be addressed and to interpret and report the
results of the analysis • Communication expert, responsible to implement the survey’s dissemination strategy
Additional to the personnel, computers and software licenses are also needed. In case the basic results are published in form of a glossy publication and/or periodic newsletters, the material’s layout and printing costs need to also be budgeted. Often results are published on the web and a web manager is needed to develop and maintain the survey’s website including the preparation of material to be uploaded to the web.