Embed Size (px)
DESCRIPTION
nasotracheal intubation
Citation preview

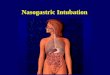
Nasotracheal intubation was first described by Magill in the 1920s and the basic technique has
changed little over the years. Modifications have been described that increase the success rate and limit
complications. The tube may be placed blindly or with the aid of a laryngoscope or bronchoscope. Blind
nasotracheal intubation can be one of the more technically demanding airway approaches, with the
outcome being heavily dependent on the skill and experience of the operator. The primary advantage of
blind nasotracheal intubation is that it minimizes neck movement and does not require opening the mouth.
General Indications and Contraindications
Nasotracheal intubation is technically more difficult than oral intubation, but it has definite advantages. It is
especially suitable for the patient with a short, thick neck or other anatomic characteristics that would
make orotracheal intubation difficult. Patients with clenched teeth or suspected cervical spine injury can
be intubated with minimal preparation. Cervical spine films, jaw spreading, or paralyzing agents as
preliminaries to airway control are unnecessary.
Blind nasotracheal intubation is possible with the patient in the sitting position, a distinct advantage when
intubating the patient with congestive heart failure who cannot tolerate lying flat. In fact, patients in
respiratory distress are the easiest to intubate blindly because their air hunger results in increased
abduction of the vocal cords, which facilitates tube entry into the trachea. The drug overdose patient with
a decreased level of consciousness is a candidate for nasotracheal intubation. These patients are often
intubated before gastric lavage and may be sufficiently awake to make orotracheal intubation difficult
without paralyzing agents.
A nasotracheal tube has advantages that extend beyond the immediate difficulties of airway control. The
patient cannot bite the tube or manipulate it with the tongue. Oral injuries may be cared for without
interference by the tube. A nasotracheal tube is more easily stabilized and generally easier to care for
than an orotracheal tube. It is better tolerated by the patient, permitting easier movement in bed, and
produces less reflex salivation than do oral tubes.
Nasal intubation should be avoided in patients with severe nasal or midface trauma. In the presence of a
basilar skull fracture, a nasotracheal tube may inadvertently enter the brain through a basilar skull
fracture. [41] The technique should be avoided in patients in whom thrombolytic therapy is being
considered. Nasal intubation is relatively contraindicated if the patient is taking anticoagulants or is known
to have a coagulopathy.
Blind Placement
Blind nasotracheal intubation is the most common form of nasotracheal intubation in the emergency
setting. Danzl and Thomas reported a success rate of 92% in a large series of emergency department
patients.
Indications and Contraindications
Any patient requiring airway control who has spontaneous respirations is a candidate for blind
nasotracheal intubation. Specific indications that favor this approach over others are (1) short, thick neck,

(2) inability to open the mouth, (3) inability to move the neck, (4) gagging or resisting the use of the
laryngoscope, and (5) oral injuries.
Apnea is the major contraindication to blind nasotracheal intubation. Attempts to place the tube without
respirations as a guide are futile. Relative contraindications include basilar skull fracture and nasal injury.
Furthermore, significant bleeding may occur if the patient is receiving anticoagulants or has a
coagulopathy. Blind nasotracheal intubation should be avoided in patients with expanding neck
hematomas. Patient combativeness, if not controlled with sedation, is also a contraindication.
Some would argue that the inability to open the mouth is a relative contraindication, because emesis may
be induced that could not be cleared. The operator must exercise judgment in the individual case and be
prepared to use neuromuscular blocking agents or to bypass the upper airway with a surgical technique if
such a complication develops.
Procedure
The patient is placed in the "sniffing" position with the proximal neck slightly flexed and the head extended
on the neck. In preparation for intubation, the operator constricts the nasal mucosa of both nares, using
either 0.25 to 1.0% phenylephrine drops, oxymetazoline (Afrin) spray, or 4% cocaine spray. Topical
anesthesia of the nares, oropharynx, and hypopharynx with lidocaine spray (10%) is also indicated if time
permits. If available, cocaine is ideal because it is both a vasoconstrictor and an anesthetic; caution is
necessary in hypertensive patients. The most patent nostril is chosen. In the cooperative patient, this can
be determined simply by occluding each nostril and asking the patient which one is easier to breathe
through. The most patent nostril can also be identified by direct vision, or by gently inserting a gloved
finger lubricated with viscous lidocaine, full length into the nostrils. If time is not an issue, an effective
method to dilate the nasal cavity and administer the anesthetic is to pass a lidocaine gel-lubricated
nasopharyngeal airway (nasal trumpet) into the selected nostril. This
airway is left in place for several minutes, and progressively larger trumpets are introduced.
After preparation of the nostril, a well-lubricated endotracheal tube with a 7.0 or 7.5 mm ID is inserted
along the floor of the nasal cavity. The tube is not directed cephalad, as one might expect from the
external nasal anatomy, but rather is directed straight back toward the occiput, corresponding with the
nasal floor. Twisting the tube may help bypass soft tissue obstruction in the nasal cavity. It is sometimes
recommended that the bevel of the tube be oriented toward the septum to avoid injury to the inferior
turbinate. However, such an event is rare. At 6 to 7 cm, one usually feels a "give" as the tube passes the
nasal choana and negotiates the abrupt 90° curve required to enter the nasopharynx. This is the most
painful and traumatic part of the procedure and must be done gently. If resistance is encountered that
persists despite continued gentle pressure and twisting of the tube, the passage of a suction catheter
down the tube and into the oropharynx may allow for successful passage of the tube over the catheter.
[44] If this fails, the other nostril should be tried. In an attempt to avoid this difficulty from the outset, a
controllable-tip tracheal tube (Endotrol, Mallinckrodt Medical Inc, St Louis) may be used that allows the
operator to increase the flexion of the tube and facilitates passage past this tight curve. One study found
the Endotrol tube to enhance first attempt success with blind nasotracheal intubation.

As the tube is advanced through the oropharynx and hypopharynx and approaches the vocal cords,
breath sounds from the tube become louder, and fogging of the tube may occur. At the point of maximal
breath sounds, the tube is lying immediately in front of the laryngeal inlet. The tube is most easily
advanced into the trachea during inspiration because that is when the vocal cords are maximally open. As
the patient begins to breathe in, the tube is advanced in one smooth motion. If a gag reflex is present, the
patient usually coughs and becomes stridulous during this maneuver, suggesting successful tracheal
intubation. The absence of such a response should alert the operator to probable esophageal passage. If
there is a delay in advancing the tube, oxygen can be added to the end of the tube to increase inspired
oxygen. Once the tube is in the trachea, moaning and groaning should cease. If they continue,
esophageal intubation is likely. Breath sounds coming from the tube and tube fogging are other signs of
endotracheal placement. Reflex swallowing during blind nasotracheal intubation may direct the tube
posteriorly toward the esophagus. If this occurs, the conscious patient should be directed to stick out the
tongue to inhibit swallowing and prevent consequent movement of the larynx. Application of laryngeal
pressure may also help avoid esophageal passage.
Following intubation, both lungs are auscultated while positive-pressure ventilation is applied. If only one
lung is being ventilated, the tube is withdrawn until breath sounds are heard bilaterally. The optimum
distance from the external nares to the tube tip is about 28 cm in males and 26 cm in females. After
verification of tracheal placement, the cuff is inflated and the tube is secured.
Technical Difficulties
The nasotracheal tube may slide smoothly through the hypopharynx and into the trachea on the first pass.
Unfortunately, this is not always the case; in the operating room, the first attempt was successful in <50%
of cases. When the initial pass is unsuccessful, there are 4 potential locations of the tip of the tube: (1)
anterior to the epiglottis in the vallecula, (2) on the arytenoid or vocal cord, (3) in the piriform sinuses, or
(4) in the esophagus.
Observation and palpation of the soft tissues of the neck during attempted passage of the nasotracheal
tube are helpful in determining the location of the misplaced tube. This is ideally done by the operator but
may also be performed by an experienced attendant. Before reattempting placement, the tube is
withdrawn slightly; it is not removed from the nose, because this will create additional trauma to the nasal
soft tissues. The possibility of cervical spine injury must be kept in mind when considering corrective
maneuvers. Any maneuver that moves the neck significantly should not be used if alternatives are
available. Methods for achieving success when difficulties with tube placement are encountered include
the following:
Anterior to the epiglottis.
Difficulty advancing the tube beyond 15 cm or palpation of the tube tip anteriorly at the level of the hyoid
bone suggests an impasse anterior to the epiglottis in the vallecula. Withdrawing the tube 2 cm,
decreasing the degree of neck extension, and readvancing the tube will frequently remedy this problem.

Arytenoid cartilage and vocal cord.
Contrary to the classic teaching, recent studies have demonstrated a propensity for a nasotracheal tube,
when placed through the right nares, to lie posteriorly and to the right as it approaches the larynx. It is not
surprising, then, that the most common obstacles to advancement of the nasotracheal tube are the right
arytenoid and vocal cord. No data are available on the common obstacles encountered if the tube is
placed in the left nares. If the tube appears to be hanging up on firm, cartilaginous tissue, withdraw the
tube 2 cm, rotate it 90° counterclockwise, and readvance the tube. This maneuver orients the bevel of the
tube posteriorly and frequently results in successful passage . Another technique is to pass a suction
catheter down the tube; it often will pass through the larynx without difficulty and the tube can then be
advanced over the catheter.
Piriform sinus.
Bulging of the neck lateral and superior to the larynx indicates tube location in a piriform sinus. The tube
should be withdrawn 2 cm, rotated slightly away from the bulge, and readvanced. An alternate method is
to tilt the patient's head toward the side of the misplacement and reattempt placement.
Esophageal placement.
Esophageal placement is indicated by a smooth passage of the tube with the loss of breath sounds. The
larynx may be seen or felt to elevate as the tube passes under it. Assisted ventilation will usually produce
gurgling sounds when the epigastrium is auscultated. The tube should be withdrawn until breath sounds
are clearly heard, and passage should be reattempted while pressure is applied to the cricoid. Increased
extension of the head on the neck during placement may help. If attempts continue to result in esophageal
misplacement, the following maneuver may result in successful tracheal intubation: from the precise point
at which breath sounds are lost, the endotracheal tube is withdrawn 1 cm. The cuff is inflated with 15 mm
of air, resulting in an elevation of the tube off the posterior pharyngeal wall and angling it toward the
larynx. The tube is then advanced 2 cm; continued breath sounds indicate probable intralaryngeal
location. At this point, the cuff is deflated and the endotracheal tube is advanced into the trachea . This
technique may be particularly useful in the patient with cervical spine injury, because it requires no
manipulation of the head or neck. This maneuver, when used on the first pass in 20 patients in the
operating room, was successful in 75% of cases. One should bear in mind, however, that these patients
were paralyzed and thus did not experience the laryngospasm that may be encountered in a breathing
patient. The use of topical anesthesia is recommended. Alternatively, if a controllable-tip endotracheal
tube (Endotrol) is used, the tip can be flexed anteriorly to help avoid esophageal placement. Remember
that the tip is very responsive to pulling on the ring. A common mistake is to exert too much force on the
ring, resulting in the tube curling up short of the larynx, thus preventing tube advancement.
Laryngospasm.
Laryngospasm is common when attempting nasotracheal intubation. It is usually transient. The tube is
withdrawn slightly and the operator should wait for the patient's first gasp; advancement of the tube at this

precise moment is frequently successful, as the vocal cords are widely abducted during forced inhalation.
Laryngeal anesthesia should also be assessed, and if IV and nebulized lidocaine have already been
administered without success, transcricothyroid anesthesia (e.g., 2 mL of 4% lidocaine) should be
considered. Occasionally, a jaw lift is necessary to break prolonged spasm. Another option is to use a
smaller tube.
Placement Under Direct Vision
This technique combines elements of oral and nasotracheal intubation. The indications and precautions
are similar, and the importance of considering cervical spine injury is identical. Likewise, the need for jaw
opening by physical or pharmacologic means is unchanged. This method is preferred to orotracheal
intubation if the presence of an orotracheal tube might interfere with the repair of an oral injury. It is also
useful when blind nasotracheal intubation has failed.
Preparation of the nose and nasopharynx and passage of the tube into the oropharynx are the same as
described for blind nasotracheal intubation. It is with the introduction of the laryngoscope that the
technique changes.
Laryngoscopy, as described with orotracheal intubation, is used to visualize the vocal cords and the tip of
the endotracheal tube. With the Magill forceps in the right hand, the endotracheal tube is grasped proximal
to the cuff (to avoid damage to the balloon) and directed toward the larynx . An assistant advances the
tube gently while the operator directs the tip into the larynx and trachea. Cricoid pressure may facilitate
the passage. Often the larynx can be manipulated sufficiently with the laryngoscope so that the physician
can advance the tube with the right hand and guide it between the cords without using the Magill forceps.
Occasionally, the natural curve of the tracheal tube guides it through the cords without any manipulation.
The cuff is inflated, and both lungs are auscultated to ensure ventilation. When placement is satisfactory,
the tube is secured.
Complications
Epistaxis is the most common complication of nasotracheal intubation. However severe epistaxis was
encountered in only 5 of 300 cases reported by Danzl and Thomas. [42] Tintinalli and Claffey reported
severe bleeding in 1 of 71 cases and less serious bleeding in 12 others. [54] Bleeding is usually not a
problem unless it provokes vomiting or aspiration, a serious potential problem in obtunded patients with a
clenched jaw or a decreased gag reflex. Other immediate complications include turbinate fracture,
intracranial placement through basilar skull fracture, retropharyngeal laceration or dissection, and delayed
or unsuccessful placement. Unsuccessful placement may be minimized by selection of a smaller tube and
by gentle technique.
Sinusitis in patients with nasotracheal tubes is common and can be an unrecognized cause of sepsis.
Rare but potentially fatal delayed complications include mediastinitis following retropharyngeal abscess
and massive pneumocephalus.
Because most of the complications occur during tube advancement through the nasal passage and
proximal nasopharynx, the complications of blind nasotracheal intubation and placement under direct

vision are largely the same. However, retropharyngeal laceration and esophageal intubation are more of a
threat in blind placement techniques because they are more likely to go unrecognized. One unique
problem associated with nasotracheal intubation is damage of the tube cuff with the Magill forceps.
Delayed nasotracheal placement under direct vision deserves special discussion. Manipulation of the
endotracheal tube through the nose and with the Magill forceps during the direct vision technique involves
additional steps that require time. Because time is of the essence in the resuscitation of the critically ill
patient, orotracheal intubation may be preferable.
Summary
Nasotracheal intubation is being used less frequently than in the past, because practitioners are
increasingly comfortable using oral intubation in the patient with potential cervical spine injury. In addition,
emergency physicians frequently use paralytics to facilitate orotracheal intubation. Nevertheless,
nasotracheal intubation remains an effective and potentially life saving approach to the difficult airway and
should be a dependable part of the armamentarium of all providers who are active in emergency airway
management.

Nasotracheal intubation may be performed in patients undergoing maxillofacial surgery or dental procedures or when orotracheal intubation is not feasible (eg, patients with limited mouth opening). Nasotracheal intubation (see the video below) used to be the preferred route for prolonged intubation in critical care units, but nasal damage, sinusitis,[1] and local abscesses have limited its use. Because of the necessity of longer and narrower tubes for the nasal route, pulmonary toilet is more difficult and airway resistance is greater. The nasal route in the spontaneously ventilating patient was once considered a technique of choice for emergency operations, but orotracheal intubation under direct vision following the rapid sequence induction of anesthesia is now the technique of choice.
Indications Most commonly, this technique is employed in the operating room for dental procedures and
intraoral (eg, mandibular reconstructive procedures or mandibular osteotomies) and oropharyngeal surgeries. Some authors advocate using nasotracheal intubation for minor otolaryngologic and maxillofacial surgeries, as they believe the technique is underused in the current practice.[2]
Other indications include securing the airway in patients with questionable cervical spine stability or severe degenerative cervical spine disease (using awake fiberoptic intubation technique), patients with intraoral mass lesions or structural abnormalities, and patients with limited mouth opening (eg, trismus).
ContraindicationsAbsolute contraindications
Suspected epiglottitis Midface instability Coagulopathy Suspected basilar skull fractures Apnea or impending respiratory arrest (Any patient with advanced upper airway obstruction, who
is apneic or having difficulties maintaining his or her airway, should not be subjected to any form of awake intubation.)Relative contraindications
Large nasal polyps Suspected nasal foreign bodies Recent nasal surgery Upper neck hematoma or infection History of frequent episodes of epistaxis Prosthetic heart valves (increased risk of bacteremia during the insertion)
Anesthesia General anesthesia : If no difficulties are suspected in securing the airway, based on the physical
examination or prior history of intubation, general anesthesia and neuromuscular blockade can be induced. General anesthesia is routinely induced using rapid-acting hypnotic or induction agents (eg, propofol, etomidate, thiopental, ketamine).
Assess mask ventilation before neuromuscular blockade: After anesthesia induction, assess the ability to mask-ventilate the patient prior to giving neuromuscular blockers (except in the case of rapid sequence induction, when mask ventilation is not attempted, and succinylcholine or rocuronium is administered simultaneous to the hypnotic agent). After the neuromuscular blocker drug is administered and given time to achieve maximal effect, perform direct laryngoscopy or blind intubation.
Prepping nasal passages: Lubricants and vasoconstrictors are commonly applied to the nasal passages prior to introduction of an endotracheal tube. Various vasoconstrictors are available, such as cocaine 4% solution (not to exceed 1.5 mg/kg), oxymetazoline 0.05% nasal spray (Afrin), or phenylephrine nose drops 0.25-1% (Neo-Synephrine). The choice of vasoconstrictor is usually at the anesthetist's preference. Applying lidocaine jelly or water-soluble lubricant allows for smoother advance as well as better transfer of rotation along the endotracheal tube's length during directional manipulation.
Fiberoptic intubation : If awake, fiberoptic intubation is necessary; prepare the patient's nasal passages as described above. Additionally, in awake or sedated patients, topical anesthesia to the patient's larynx and pharynx is also required. This can be accomplished by a number of techniques, such as transoral application of a local anesthetic agent or use of superior laryngeal nerve block with 4%

lidocaine (up to 3 mg/kg) administered transtracheally or sprayed down the fiberscope's lumen intermittently in advance of the scope's passage. Incomplete topical anesthesia not only causes patient discomfort, it makes the procedure much more difficult and may lead to patient morbidity. An antisialagogue drug is administered (eg, glycopyrrolate 0.2-0.3 mg IV) to improve the visualization of the field. Small amounts of sedation are advocated as well, keeping in mind that sedation is not a substitute for a well anesthetized airway.
Equipment Endotracheal tube (Nasal Rae [see image below] or the regular endotracheal tube)
Nasal Rae endotracheal tube. Lidocaine jelly or any other water-soluble lubricant
Magill forceps (see image below) Magill forceps. Afrin spray (oxymetazoline 0.05%) Nasal trumpets Syringe to inflate the cuff Suction Intubation equipment (eg, laryngoscope, Glide-scope, fiberoptic scope) Commercial airway device adjuncts are available. A novel intubation system, GlideScope Video
Laryngoscope (GVL, Verathon Medical Inc., Bothell, Wa) has an established role in routine and difficult orotracheal intubation not only by experienced handlers but also by novices.[3, 4] In a recent study, authors showed GVL superiority compared to direct laryngoscopy in improvement of time to successful intubation and in regard to lower incidence of moderate to severe sore throat postoperatively.[5]
Positioning For the induction of general anesthesia, the patient should be in the supine position. If awake fiberoptic intubation (or any other awake intubation) is pursued, often the most practical
position may be sitting (on the operating room table), as it prevents the larynx from falling posteriorly as it does in the supine position.
Technique

Establish patency of the nares with a well-lubricated nasal trumpet (see images below).
Inserting nasal trumpet. Notice that insertion angle is almost perpendicular to the
face. Nasal trumpet insertion (continued). Insert a well-lubricated tube with fully deflated cuff via a patent, lubricated naris, at a right angle to
the face (see image below). Direct laryngoscopy with Miller blade. Insert Nasal Rae endotracheal tube and advance it a little prior to putting the laryngoscope in the mouth.
Some resistance is commonly encountered, most likely due to the right arytenoid. This is usually overcome with slight counterclockwise rotation of the tube.
Once the tube is beyond the nasopharynx, introduce the laryngoscope into the oral cavity and
advance the tube under direct vision (see images below). Once the vocal cords are seen, the endotracheal tube is advanced by the laryngoscopist or an assistant.
Magill forceps directing the endotracheal tube (above the cuff) for its advance through the vocal cords.

Sometimes, to avoid tearing the cuff with the forceps, Magill forceps are needed to guide the tube through the vocal cords; if this is the case, an assistant advances the tube (see image below).
The endotracheal tube is advanced using Magill forceps by the laryngoscopist. An assistant helps advance the tube by slowly pushing it in.
Complications Epistaxis: This is the most common complication, resulting from abrasion of the nasal mucosa
when the tube is passed posteriorly. If bleeding is noticed but intubation could still be achieved, then it should be completed. An endotracheal tube in proper position allows tamponade of the bleeding and protects the airway. If repeated attempts are needed, then the tube should be withdrawn until the cuff is positioned to be inflated in order to tamponade the bleeding (usually in the postnasal space). Another option is to withdraw the tube completely and pinch the nostrils together.
Damage to nasal cavity (avulsion of nasal polyps, fracture of the turbinates, septal abscesses) Aspiration Vagal stimulation Laryngospasm Vocal cord damage[6]
Bacteremia from introduction of nasal flora to the trachea Pneumothorax
http://emedicine.medscape.com/article/1663655-overview#showall