Embed Size (px)
Citation preview

725
Nasopharyngeal and Temporal Bone Blastomycosis: CT and MR Findings Edward E. C. Angtuaco ,1 Edgardo J . C. Angtuaco,1 Charles M. Glasier,1 ·
2 and Wanda 1. Benitez1
Blastomycosis is a fungal disease endemic to the Mississippi and Ohio River valleys and to the southeastern United States [1 ]. From the time blastomycosis was first isolated from the skin by Gilchrist in 1896 [2] , numerous epidemiologic, laboratory, and clinical data have been collated in an attempt to fully define this disease process. There is wide variability in the clinical presentation, depending on the organ of involvement. Pulmonary, skin, and CNS involvement are well documented in the literature. However, a review of published reports revealed no previous cases of extensive nasopharyngeal and temporal bone involvement from disseminated disease. We present two case reports of patients with strikingly similar clinical and radiologic presentations.
Case Reports
Case 1
A. W. is a 43-year-old woman who initially presented with skin lesions in the right upper leg. She was treated with antibiotics and antifungal medications, and partial improvement was noted. Six months later, she was admitted with symptoms of recurrent neck pains and headaches with right ear pain and right facial weakness . Physical examination revealed bi lateral otitis media, left worse than right , and right facial weakness. Multiple skin lesions were also seen. A chest radiograph showed a fine nodular pattern throughout both lungs. Initial head CT scan showed two ring-enhancing lesions in both cerebral hemispheres near the basal ganglia. Sections through the nasopharynx demonstrated an enhancing soft-tissue density in the right nasopharynx extending into the nasal cavity , right maxillary , and sphenoid sinuses (Fig . 1 A). High-resolution temporal bone sections showed abnormal soft-tissue density filling the entire middle ear and mastoid air cells. There was destruction of the base of the skull and petrous temporal bone (Figs . 1 B and 1 C). Cultures of the middle ear fluid grew budding yeasts identified as Blastomyces dermatitidis . The patient was started on amphotericin B. A subsequent cranial MR study again showed the presence of a smaller nasopharyngeal mass. This extended into the adjacent maxi llary sinus and pterygopalatine fossa. On the T2-weighted images, tissue w ith increased signal intensity filled the entire cavity of the right middle ear and mastoid antrum (Fig. 1 D) . A contrast-enhanced study showed two enhancing
masses in the left cerebellar peduncle and right thalamus (Fig. 1 E) . A follow-up head CT study after 1 month of treatment showed improvement in the size of the brain enhancing lesions.
Case 2
M. R. is a 12-year-old boy who was admitted on January 11 , 1990, following a 6-month history of headaches, neck pains , right ear drainage, and intermittent fever. Physical examination showed bilateral purulent ear discharge w ith tenderness on the right side of the neck. No skin findings were noted. An initial chest radiograph showed an infiltrate in the left infrahilar region , and a chest CT scan confirmed the presence of a left lower lobe infiltrate and also showed hilar adenopathy. Sinus radiographs showed airway deformity in the right parapharyngeal area and soft tissue in the medial portion of the right maxillary sinus. A CT scan of the neck showed a 3-cm nasopharyngeal mass on the right extending into the parapharyngeal space (Fig. 2A). On bone windows , destruction of the skull base was noted (Fig . 28). Fluid in the right middle ear was also seen. MR images of the head and neck revealed a large exophytic nasopharyngeal mass extending into the parapharyngeal space. This mass extended into the right posterior nasal cavity , base of the skull , middle cranial fossa , and right external auditory canal (Figs. 2C-2F). High signal on T2-weighted images was also seen in the middle ear and right mastoid air cells. Owing to the aggressive nature of the mass, it was initially believed to represent a rhabdomyosarcoma. The patient underwent an intraoperative biopsy , which revealed thick-walled budding yeast identified as Blastomyces dermatitidis. The patient was started on amphotericin B and a repeat MR scan 17 days later demonstrated marked improvement in the size of the nasopharyngeal mass.
Discussion
Blastomycosis is a granulomatous fungal infection caused by a dimorphic fungus , Blastomyces dermatitidis. Except for occasional reports of laboratory inoculation , the fungus is primarily acquired by inhalation of spores from the environment. From the lungs, the disease disseminates via hematogenous and lymphatic routes to involve other organ systems [4]. The cl inical presentation can be classified as acute, chronic , or disseminated. Laskey and Sarosi [5] reported
Received July 26 , 1990; revision requested November 10, 1990; revision received December 17, 1990; accepted January 5, 1991. ' Department of Radiology, University of Arkansas for Medical Sciences, 4301 W. Markham St. , Little Rock, AR 72205. Address reprint requests to E. E. c.
Angtuaco. 2 Department of Radiology, Arkansas Children 's Hospital , 800 Wolfe St., Little Rock , AR 72204 .
AJNR 12:725-728, July/August 1991 0195-6108/91 /1204-0725 © American Society of Neuroradiology

726 ANGTUACO ET AL. AJNR :12, July/August 1991
A B c
D E
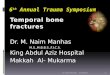
Fig. 1.-Case 1: 43-year-old woman. A, Contrast-enhanced CT scan shows thickened right nasopharyngeal wall (arrow) with soft-tissue mass in posterior nasal cavity. A soft-tissue mass
is also noted in right maxillary sinus. B, High-resolution temporal bone CT scan shows lytic destruction of clivus, right pterygoid plates, and body of sphenoid. There are soft-tissue masses
in nasal cavity, maxillary sinus, and pterygopalatine fossa. C, Higher CT section shows soft-tissue densities in middle ear and mastoid air cells on the right. Involvement of both sphenoidal sinuses is also noted. D, T2-weighted MR image (2700/80) shows high signal intensity in right middle ear and mastoid air cells, as well as a mass with intermediate signal
intensity in right naso- and parapharyngeal regions. E, Postcontrast T1-weighted MR image (500/20) shows two enhancing areas in right thalamus and left midbrain.
endogenous reinfection in three patients who presented initially with primary lung involvement.
Skin lesions are classically painless, nodular or papular initially, but may later enlarge to form large abscesses if left untreated (6] . Deeper lesions are also associated with the cutaneous manifestations. Owing to the similarity of the blastomycosis lesions with other fungal and bacterial skin lesions, definite identification of the organism by means of a variety of available laboratory techniques [7] is essential before treatment is instituted.
The chest radiograph findings of blastomycosis are well described. Halvorsen et al. [4] classified the pulmonary findings into air-space disease, nodular masses, interstitial disease, and cavitary lesions. Stelling et al. (8] described a miliary pattern of lung involvement by blastomycosis. However, the clinical predictive value of the various patterns of lung involvement remains a source of controversy.
CNS involvement by blastomycosis was estimated by Parker et al. [9] to constitute 2.5% of all cerebral mycosis. Intracerebral involvement results from either hematogenous spread in disseminated disease or from contiguous spread from the sinuses or, as in our cases, from a primary focus in the nasopharynx. Initially, it was thought that parenchymal involvement with blastomycosis originated from a diffuse leptomeningitis [9]. However, purely parenchymal involvement and purely leptomeningitic lesions have been described [1 0] . The predominant CNS infecting form is the yeast form, which generally produces noncaseating granulomas and appears as nodular enhancing lesions on brain CT scans (11] . Major differential diagnoses for primary leptomeningitic involvement include tuberculosis , cryptococcosis, metastatic cancers, various vasculitides, and sarcoidosis (12]. A single parenchymal abscess may be confused with tumor on imaging studies. CSF cultures or smears, biopsy specimens, and

AJNR :12, July/August 1991 CT AND MR OF BLASTOMYCOSIS 727
A B C
D E F
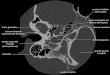
Fig. 2.-Case 2: 12-year-old boy. A, Contrast-enhanced CT scan shows large right nasopharyngeal soft-tissue mass (arrow) obliterating parapharyngeal space and extending into
pharyngeal airway. B, CT scan with bone windows of higher region shows destruction of right petrous apex. Note soft-tissue mass in right middle ear and mastoid air cells. C, T2-weighted MR image (2000{100) shows nasopharyngeal mass with intermediate signal intensity extending into nasal cavity and pterygoid region.
Hyperintense signal is seen in right maxillary sinus. D, Higher-section T2-weighted MR image (2000/100) shows extension into sphenoidal sinus with intermediate signal intensity medially and higher
signal intensity laterally. Also note high signal intensity in right middle ear, external ear, and mastoid air cells. E, Postcontrast axial T1-weighted MR image (800/20) shows enhancement of soft-tissue mass in right middle ear and mastoid air cells. Enhancement
in both sphenoidal sinuses and right posterior ethmoid is also noted. F, Postcontrast coronal T1-weighted MR image (900{20) reveals enhancement of floor of right middle cranial fossa extending into cavernous sinus
(arrow). Also note mass in sphenoidal sinus with discontinuity of the floor of the body of the sphenoid.
correlative clinical data will aid in the accurate diagnosis of blastomycosis.
Blastomycosis, being a systemic illness, has also been reported to involve other sites. There are isolated reports of blastomycosis affecting bone, liver, heart, adrenal glands, genitourinary tract, and several sites in the extracranial head and neck region [13-15). These rare sites of involvement are of special interest because of the increased likelihood of delayed diagnosis and treatment. The predominance of other diseases as well as the atypical presentation of blastomycosis in those sites hinders correct early diagnosis with resultant severe sequelae.
Our two cases highlight the complementary role of CT and MR in diagnosing lesions involving the base of the skull. CT,
aside from its detection of soft-tissue masses, clearly showed the bony destruction of the skull base. On the other hand, MR imaging provided better characterization of the mass, primarily because of the absence of bone artifact. The contrast-enhanced MR studies revealed the intracranial dissemination of blastomycosis (intracranial abscesses and contiguous epidural spread). Likewise, spread of the infection into the pterygopalatine fossa was clearly shown in both cases. In case 2, on the axial T2-weighted images, there was a softtissue mass adjacent to the area of bone destruction above the floor of the sphenoid sinus. This mass had intermediate signal intensity on T2-weighted images and most likely represented the mycetoma. Zinreich et al. [16) reported a characteristic hypointense signal in the sinuses on T2-weighted

728 ANGTUACO ET AL. AJNR:12, July/August 1991
sequences in cases of fungal sinusitis. This finding was attributed to increased concentration of iron and manganese in these infections. The bright signal in the adjacent middle ear and mastoids may represent retained secretions associated with the obstruction caused by the nasopharyngeal mass. The MR signal characteristics of inflammation are typically similar to that of water, although variation from this has been reported and extensively studied [17, 18].
The role of gadopentetate dimeglumine in extracranial head and neck imaging is still under investigation. The preliminary reports have been mixed and the indications are still in question . Contrast medium has been reported to be of use in detecting small nasal and paranasal tumors, perineural infiltration at the skull base, and leptomeningeal extension of lesions [19). Recently, Vogl et al. [20] noted that contrast enhancement of inflammatory tissues exceeds that of tumor and that, potentially, this can be used as a differentiating point. In our cases, contrast-enhanced images were useful primarily to demonstrate leptomeningeal and brain parenchymal involvement. The abnormal areas in the nasopharynx and sinuses were well shown on the routine spin-echo T1- and T2-weighted images. However, with future availability of fatsuppressed T1-weighted sequences, contrast-enhanced images may better characterize the spread of infection in the skull base.
These two cases are of interest because of the unique nature and similarity of their radiologic presentation. In both cases, the primary focus of hematogenous dissemination was in the nasopharyngeal soft tissues. Owing to the infiltrative nature of this mycotic inflammatory process, the infection spread to the base of the skull and the epidural space, the temporal bone, pterygopalatine fossa, and paranasal sinuses. In the first case, there was hematogenous spread into the brain parenchyma. This pattern of infiltration of the nasopharyngeal space is indistinguishable from the aggressive appearance of other fungal diseases [21 ), which closely mimics the spread of malignant nasopharyngeal tumors. Mancuso and Hanafee [22] described and classified lesions of the nasopharynx on the basis of their imaging characteristics. These cases would be categorized as deep infiltrating lesions, and the major diagnostic consideration would be malignant neoplasms, primarily squamous cell carcinomas of either the lymphoepitheliomatous or transitional cell type. Other malignant tumors in this region include rhabdomyosarcoma, adenocarcinoma, adenoid cystic carcinoma, lymphoma, sarcoma, and metastatic disease. Bohman et al. [23] cited benign causes of such infiltrative spread and included mucormycosis [21 ), postoperative edema, and postbiopsy hemorrhage. Extension from a malignant otitis media can also present in a similar fashion. To this list of benign infiltrative nasopharyngeal
lesions, we submit disseminated blastomycosis as another consideration.
REFERENCES
1. Furcolow ML, Balows A, Menges RW, Pikar D, McClellan JT, Soliba A. Blastomycosis: an important medical problem in the Central United States. JAMA 1966;198:529-532
2. Gilchrist TC. Protozoan dermatitis. J Cutan Genitourin Dis 1894;12:496 3. Howard DH . The epidemiology and ecology of blastomycosis, coccidiodo
mycosis and histoplasmosis. Zentralbl Hyg Umweltmed 1984;257:219-227
4. Halvorsen RA, Duncan JD, Merten OF, Gallis HA, Putman CE. Pulmonary blastomycosis: radiologic manifestations. Radiology 1984;150: 1-5
5. Laskey W, Sarosi GA. Endogenous activation in blastomycosis. Ann lnt Med 1978;88:50-52
6. Meyer RD. Cutaneous and mucosal manifestations of the deep mycotic infections. Acta Derm Venereol1986;121 :57-72
7. Tang TT, Marsik FJ, Harb JM, Williams JE, Frommell GT, Dunn OK. Cerebral blastomycosis: an immunodiagnostic study. Am J Clin Pathol 1983;82:243-246
8. Stelling CB, Woodring JH, Rehn SR , Hopper OW, Noble RC. Miliary pulmonary blastomycosis. Radiology 1984;150:7-13
9. Parker JC, McCloskey JJ , Lee RS. The emergence of candidosis. The dominant postmortem cerebral mycosis. Am J Clin Pathol1978;70:31-36
10. Cooper K, Lalloo UG, Naran HK. Cerebral blastomycosis. S Afr Med J 1988;74:521-523
11 . Whelan MA, Stern J, de Napoli RA. The computed tomographic spectrum of intracranial mycosis, correlation with histopathology. Radiology 1981;14: 703-707
12. Kravitz HR. Davies SF, Eckman MR. Sarosi GA. Chronic blastomycotic meningitis. Am J Med 1981 ;71 :501-505
13. Witorsch P, Utz JP. North American blastomycosis: a study of 40 patients. Medicine 1968;47 : 169-200
14. Gerwin JM, Myer CM Ill. Intranasal blastomycosis. Am J Otolaryngol 1981;2:267-273
15. Berkowitz I, Diamond TH . Disseminated blastomyces demartidis infection on a non-endemic area. S Afr Med J 1987;71 :717-718
16. Zinreich SJ, Kennedy OW, Malat J, et al. Fungal sinusitis: diagnosis with CT and MR imaging. Radiology 1988;169:439-444
17. Som PM , Dillon WP, Fullerton GO, Zimmerman RA, Rajagopalan B, Marom Z. Chronically obstructed sinonasal secretions: observations on T1 and T2 shortening. Radiology 1989;172:515-520
18. Dillon WP, Som PM , Fullerton GO. Hypointense MR signal in chronically inspissated sinonasal secretions. Radiology 1990;174 :73-78
19. Robinson JD, Crawford SC, Teresi LM , Schiller VL, Lufkin RB. Extracranial lesions of the head and neck: preliminary experience with Gd-DTPA enhanced MR imaging. Radiology 1989;172: 165-170
20. Vogl T, Dresel S, Bilaniuk L T, Grevers G, Kang K, Lissner J. Tumors of the nasopharynx and adjacent areas, MR imaging with Gd-DTPA. AJNR 1990;11: 187-194, AJR 1990;154: 585-592
21. Centeno RS, Bentson JR, Mancuso AA. CT scanning in rhinocerebral mucormycosis and aspergillosis. Radiology 1981 ;140:383-389
22. Mancuso AA, Hanafee WN. Computed tomography and magnetic resonance imaging of the head & neck, 2nd ed. Baltimore: Williams & Wilkins. 1985
23. Bohman LG , Mancuso AA, Thomason J, Hanafee WN. CT approach to benign nasopharyngeal masses. AJR 1981 ; 136: 173-180