Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Dermatology 2010;221(suppl 1):15–22 DOI: 10.1159/000316171
Nailing down the Genetic and Immunological Basis for Psoriatic Disease
Dennis McGonagle a Natalia Palmou Fontana c Ai Lyn Tan a Michael Benjamin b
a Section of Musculoskeletal Disease, Leeds Institute of Molecular Medicine, University of Leeds and Chapel Allerton Hospital, Leeds , and b School of Biosciences, Cardiff University, Cardiff , UK; c Rheumatology Department, Complejo Hospitalario Universitario A Coruña, La Coruña , Spain
lead to activation of aberrant innate immune responses. These observations that stem from nail disease point toward a relative differential involvement of adaptive and innate im-munity in the psoriatic disease spectrum and offer a fresh perspective on the pathophysiology of psoriatic disease and how it can be classified along the immunological disease continuum of self-directed inflammation.
Copyright © 2010 S. Karger AG, Basel
Introduction
From the original description of the association be-tween psoriasis and psoriatic arthritis (PsA) more than 50 years ago, it became immediately evident that the link between joint and nail disease was much more striking than that between skin and nail disease [1, 2] . This is rath-er surprising, given that nails are epidermal derivatives. However, a joint-nail relationship has been repeatedly de-scribed as a feature of PsA, and it is therefore curious that few dermatologists have explored the possibility of ana-tomical links between the nail and the distal interphalan-geal (DIP) joint.
In recent years, the shared and overlapping features of skin and joint disease have led to the proposal that we should consider skin-, nail- and joint-related involvement that is associated with psoriasis under the guise of psori-
Key Words Psoriasis � Nail psoriasis � Nail and joint � HLA-Cw6 � Pathophysiology
Abstract Psoriatic disease encompassing skin, joint and nail involve-ment is largely viewed as autoimmune – a finding supported by data from animal models, the human leucocyte antigen (HLA)-Cw6 disease association in man, T-lymphocyte infil-tration in lesional skin and the favourable skin response to T-cell-directed therapies. However, this immunopathoge-netic model only applies to the skin, as recent studies failed to demonstrate a HLA-Cw6 association with the nails or joints. Furthermore, the nails and joints are intimately associ-ated with inflammation at points of ligament or tendon in-sertion (i.e., enthesitis), so it is now appreciated that both of these sites also share a common microanatomical basis. Moreover, inflammation at insertion sites and nails does not appear to be associated with a particular antigenic territory but is quite diffuse in nature. This suggests that an aberrant response to tissue stressing of the integrated nail-joint ap-paratus, rather than autoimmunity, is driving the inflamma-tory process. Therefore, HLA-Cw6-associated type 1 psoria-sis is more closely linked to autoimmunity, whereas nail and joint disease may be linked to tissue-specific factors, includ-ing tissue biomechanical stressing and microtrauma, that
Published online: August 9, 2010
Prof. Dennis McGonagle Section of Musculoskeletal Disease Leeds Institute of Molecular Medicine, Chapel Allerton Hospital Chapeltown Road, Leeds LS7 4SA (UK) Tel. +44 113 3924 747, Fax +44 113 3924 991, E-Mail d.g.mcgonagle @ leeds.ac.uk
© 2010 S. Karger AG, Basel1018–8665/10/2215–0015$26.00/0
Accessible online at:www.karger.com/drm
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

McGonagle /Palmou Fontana /Tan /Benjamin
Dermatology 2010;221(suppl 1):15–2216
atic disease [3] . Nail involvement represents an important subset of psoriasis or PsA-related disease, and nail disease has been difficult to treat effectively [4] . The purpose of this article is to synthesise the emerging microanatomi-cal and genetic data on nail involvement in psoriatic dis-ease to show how these data offer new perspectives on psoriatic disease pathophysiology.
Anatomy of the Nail, Including Skeletal Appendage Integration
The nails are plates of hard keratin covering the dorsal surface of the distal phalanx of each finger or toe. Their named parts are shown in figure 1 and are briefly ex-plained below. For more comprehensive accounts, the reader is referred to the literature [5–7] . The visible region of each nail is the nail plate, which lies on an epithelium that represents a modified deep region of the epidermis (the nail bed). The plate itself is the counterpart of the stratum corneum, although keratohyalin granules are not involved in its formation [6] . The nail plate is bound-ed at its base and sides by proximal and lateral nail grooves. Much of a healthy nail plate is pink and semi-translucent, revealing the underlying blood vessels. How-ever, the proximal part of the nail plate (the lunula) is opaque and white. The lunula consists of newly formed keratin and is overlapped by the stratum corneum of the proximal nail fold, which forms an eponychium or cuti-cle. There is a further reflection of stratum corneum un-der the distal free edge of the nail plate (the hyponychi-um). The proximal part of the nail bed acts as a nail ma-trix, which is responsible for producing the nail plate itself. The thickness of the nail plate reflects the proxi-mal-distal length of the matrix [5, 6] . The lunula is the distal part of this matrix.
As it grows, the nail plate slides horizontally over the nail bed while managing to maintain continuous attach-ment to it. As with the epidermis elsewhere, the surface area of contact between the nail bed and the underlying dermis is greatly increased. However, in the nail bed, the underlying dermis knits into the epithelium as a series of very deep longitudinal ridges, rather than as dermal pa-pillae in the neighbouring matrix. The ridges are tallest toward the free end of the nail and become shorter and more numerous (via splitting) as the lunula is approached [8] . As discussed later, such anatomical variations could be relevant to a better understanding of psoriatic nail changes such as subungual hyperkeratosis and onycholy-sis.
With respect to the integration of the nail with the lo-cal tendon and ligament insertions, collectively termed entheses, several authors have commented that the exten-sor tendon attaches to the distal phalanx at a site that is very close to the nail matrix. However, we and others have shown that fibres from the tendon actually attach direct-ly to the matrix [9, 10] . We have also drawn attention to a further fascial extension from the enthesis that contrib-utes to a thickening of the periosteum on the adjacent
a
b
Fig. 1. a Parts of the nail. The nail plate (NP) rests on the nail bed (not visible) and has a proximal opaque, whitish semilunar region called the lunula (L). It is bounded at its base and sides by the proximal (PG) and lateral (LG) nail grooves. A fold of stratum corneum (the eponychium, E) overlaps the lunula proximally, and a further reflection of stratum corneum (the hyponychium, H) underlies the free distal edge of the nail plate. b A transverse his-tological section (stained with haematoxylin and eosin) through a nail plate showing the nail plate itself (NP) and the deep longi-tudinal furrows (arrows) that knit the nail bed (NB) to the under-lying dermis like an elaborate series of tongue-and-groove joints. Numerous thin-walled blood vessels (BV) are evident in the der-mis itself. These deep ridges are characteristic of the nail plate but not the matrix. This is interesting, since they correspond to the location of splinter haemorrhages.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

Nail in Psoriatic Disease Dermatology 2010;221(suppl 1):15–22 17
dorsal surface of the terminal phalanx [5, 10] . As the der-mis beneath the nail bed is also anchored to the perios-teum, this means that the extensor tendon is both direct-ly and indirectly connected to the nail unit, so the nail plate can be viewed as a skeletal appendage. Importantly, these anatomical studies show that the nail is indirectly attached to the skeleton via the tendon and ligaments’ periosteum links [11] . As we shall see later, this bone and enthesis integration is key to an understanding of nail and adjacent joint disease.
Magnetic Resonance Imaging Studies and Histological Studies in Psoriatic Disease
The resolution of conventional 1.5 T magnetic reso-nance imaging (MRI) is of limited value for assessing the nail and DIP joint. Consequently, we optimised high-resolution MRI to explore the link between the skin and the DIP joint and noted that polyenthesitis and osteitis were virtually universal in patients with PsA but not in normal individuals [12] . What is particularly significant in the context of the anatomy outlined above is that the PsA-related DIP joint inflammatory reaction was very extensive, enveloped the nail matrix and often extended to the nail bed. Therefore, the inflammatory reaction does not seem to involve a particular tissue or putative autoantigen distribution, but rather the entire joint and nail structure, including bone ( fig. 2 ). These enthesitis-related imaging findings in the DIP joint had been previ-
ously shown in other joints, including the knee and oth-er hand joints [13, 14] .
Based on normal nail histology and MRI in early dis-ease, we have proposed that the pattern of DIP joint-nail disease is better explained as an aberrant inflammatory reaction at sites of mechanical stress, with the epicentre at the enthesis [15] . Attachment points or entheses are sites of high mechanical stress, which is dissipated over a wide area, including the adjacent bone trabecular net-works and periosteum of the distal phalanx [16] . We have also noted that large-joint, normal cadaveric entheses demonstrate conspicuous microdamage, microinflam-matory changes and associated tissue repair responses, both in the enthesis-bone interface and in the soft tissue components of the enthesis [17, 18] .
The combined imaging and anatomical studies indi-cate that the enthesis is the likely primary basis for joint and skeletal disease localisation in PsA and that other musculoskeletal features, including synovitis and oste-itis, can also be conceptualised in relationship to en-thesitis [19] . The histological findings of microdamage at normal entheses are reminiscent of the Koebner re-sponses that are well known to dermatologists in the setting of both skin psoriasis and nail disease [20, 21] . The recognition of the functional integration between the nail and enthesis including the bone therefore offers a better understanding of rare psoriatic disease variants, such as acral pustular psoriasis, that have been reported with resorptive osteolysis (deep Koebner phenomenon) [22] .
a b
Fig. 2. T1-weighted fat-suppressed post-contrast high-resolution MRI of the DIP joint in a 23-year-old man with PsA DIP joint disease in the coronal ( a ) and axial ( b ) planes. These images show the extent of inflammation seen in PsA-related DIP joint disease. Although the enthesis is the epicentre of the inflammatory reaction, there are inflammatory changes extend-ing to involve the adjacent nail-related tis-sues (black asterisks) and bone (white as-terisk). This likely relates to the complex structure of insertions that envelop the nails and to the fact that the nail and en-thesis network act as a functional unit.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

McGonagle /Palmou Fontana /Tan /Benjamin
Dermatology 2010;221(suppl 1):15–2218
Nail Psoriasis Phenotypes: Nail Matrix Lesions
Thus far, the relationship between nail lesions in pso-riasis and the nail-enthesis functional unit has not been considered, and these lesions are briefly considered from the enthesis perspective. Dermatologists have long recog-nised that the clinical features of nail psoriasis can be split into those involving the nail matrix and the nail plate. In the nail matrix, these features include nail pit-
ting, crumbling, splitting and leuconychia. Nail pitting ( fig. 3 a, b) is indicative of superficial nail abnormalities, and its presence implies that the proximal part of the nail matrix is involved, since this area is responsible for pro-ducing the superficial layers of the nail plate. Histologi-cally, the pits often represent local areas of parakeratosis where poorly adherent cells are desquamated from the nail plate [5] . Pits may be randomly distributed or uni-formly arranged in series along one or several longitudi-
a b
c d
Fig. 3. Abnormalities associated with the nail: regular pitting of the nail ( a ), irregu-lar pitting of the nail ( b ), onycholysis ( c ) and splinter haemorrhages ( d ). The com-mon nail matrix changes of pitting and nail bed changes of onycholysis have not been conceptualised in relation to the re-gional nail-enthesis connections. The ex-tensor tendon is attached to the nail matrix in an interdigitating fashion, which could be relevant to understanding linear pit-ting. Likewise, the collateral ligaments fuse with a lateral lamina to anchor the nail. It remains to be seen what role these play in nail-related pathology. It seems that some changes, including subungual hy-perkeratosis, are related to keratinocyte abnormalities and are not obviously linked to the enthesis.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

Nail in Psoriatic Disease Dermatology 2010;221(suppl 1):15–22 19
nal lines or may appear in an orderly crisscross pattern (rippled pitting). Given that the extensor tendon may be attached to the nail matrix in an interdigitating pattern, this could be relevant to understanding linear pitting. Nail plate crumbling suggests extensive involvement of the nail matrix in the psoriatic process [23] . Nail splitting suggests that the distal part of the matrix is implicated, for it is here that the deeper layers of the nail plate are made [5] . Leuconychia may also involve the nail matrix, with the area of involvement thought to be on the under-surface of the nail plate [4] . Electron microscopy studies have shown clear vacuoles located on the white part of the nail; however, they were not seen on the distal part. These observations confirm the probable participation of parakeratosis and keratin abnormalities in this pa-thology but also suggest an important role of lipid vacu-oles [24] .
Nail Psoriasis Phenotypes: Nail Bed Lesions
Onycholysis (separation of the nail plate from the nail bed) ( fig. 3 c) represents a common nail lesion that is thought to involve the hyponychium. It allows air to get under the distal end of the nail plate, accounting for the whitish colour. Accumulation of large amounts of serum-like exudate containing glycoprotein under the affected nail may explain the colour change in onycholysis [7] and may therefore be linked to keratinocyte dysfunction. The entire nail plate loses its normal mechanical properties and lifts off the nail bed, leaving the latter exposed [25, 26] .
‘Oily spot’ or ‘salmon patch’ nail plate lesions may start in the middle of the nail. There is usually a yellow-ish-brown margin visible between the pink, normal nail and the white, oily spot-salmon patch lesion. Nail separa-tion may start here rather than at the hyponychium [4] .
Macroscopically, splinter haemorrhages appear as small linear structures, usually not greater than 2 or 3 mm long, arranged at the end of the nail. They are com-monly found in the first three fingers of both hands and develop at the line of separation of the nail plate from the nail bed. It is thought that the elongated form of splinter haemorrhages reflects the rupture of wide-calibre vessels beneath the hyponychium and tracking of extravasated blood down the longitudinal furrows beneath the nail plate [5] .
We have proposed that the enthesis-nail complex could be a key to understanding different patterns of pso-riatic nail disease [11] . However, these nail phenotypes
have yet to be explored in relation to perturbation of the enthesis network around the nail, including extensor ten-dons, the lateral lamina or dermal ligaments. It seems likely that some abnormalities, such as nail hypertrophy and subungual hyperkeratosis, can be fairly clearly linked to the skin phenotype. Whilst this seems to be clearly skin-related, with keratinocyte hyperplasia, it is fair to say that the microanatomical and immunopathological basis for these nail changes in relation to the extensive enthesis network around the fingers is incompletely un-derstood. Certainly, the relationship between nail chang-es and unrecognised enthesitis in the digits remains to be defined [4, 23, 26, 27] . This is something that high-reso-lution imaging in man may achieve.
The Role of Inflammation in Skin and Nail Psoriasis
It is evident that the entire psoriatic disease spectrum has a prominent inflammatory component, but this is difficult to directly investigate in the nail. It is clear from imaging the DIP joints with high-resolution MRI thatthe nail matrix is involved in the inflammatory response as determined by Gd-DTPA (gadolinium-diethylenetri-amine pentaacetic acid) enhancement [11] . However, we are not aware of specific histological studies of the nail matrix in psoriasis subjects with nail disease.
Imaging to Establish Subclinical Evidence of Enthesitis in Psoriasis
Subclinical enthesitis appears to be very common in patients with psoriasis but not arthritis. Based on more than three decades of research, it has become evident that subjects with psoriasis but without arthritis may have subclinical skeletal-related pathology. The original stud-ies by Namey and Rosenthall [28] showed that subjects with psoriasis had increased isotope uptake along the periosteum – an observation that in hindsight supports the presence of enthesitis and osteitis [29] . Several other studies have replicated this finding, with the most recent ultrasound imaging study showing that subclinical en-thesitis of the large joints in the lower limbs was common in subjects with psoriasis, none of whom had joint symp-toms [29] . The key question is whether nail disease rep-resents a type of subclinical enthesitis that might be rel-evant to the future prediction of widespread musculo-skeletal disease.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M
McGonagle /Palmou Fontana /Tan /Benjamin
Dermatology 2010;221(suppl 1):15–2220
Indeed, preliminary imaging studies in psoriasis-re-lated pathology have shown a clear link with enthesitis and related osteitis. Psoriatic onychopachydermoperi-ostitis (POPP) is an uncommon variant of the psoriatic disease spectrum that may present to either rheumatol-ogists or dermatologists. The changes associated with POPP consist of nail dystrophy, periungual swelling and a periosteal reaction in the terminal phalanx on radiog-raphy [30–32] . The mechanism of bony damage has been conceptualised in relation to inflammation pass-ing from the subungual dermis to the bone [33, 34] . The MRI description of POPP clearly attests to a nail-enthe-sis-bone apparatus diffuse inflammatory disorder [35] . This is highly reminiscent of the diffuse digital inflam-mation, including enthesis-bone involvement, that we have commonly seen in PsA of the DIP joints in the hand [13, 36] .
Common Genetic Traits between Nail and Skin Disease
Thus far, we have argued that there is a common mi-croanatomical basis for joint and nail disease in subjects with psoriatic disease. If this is a tenable theory, then emerging immunogenetics might similarly show a rela-tionship between joint and nail disease but not skin dis-ease. The association of type 1 psoriasis with human leu-cocyte antigen (HLA)-Cw6 within the major histocom-patibility complex appears very robust [37] . Patients with type 1 psoriasis who carry the HLA class I allele HLA-Cw6 not only have an earlier onset, but also more exten-sive and severe skin disease.
However, it is now evident that nail disease does not share this HLA-Cw6 association, which has been dem-onstrated in both Caucasian and Chinese populations [38, 39] . Likewise, in a recent case-controlled association
Autoantibody-associated
autoimmunity
MHC class 1-associated
autoimmunity
Polygenic innateimmune-mediated
inflammation
Adaptive immunity boundary(main tissue players: primary and secondary lymphoid organs)
True autoimmune skin disease, e.g.pemphigus, pemphigoid, cutaneous lupus,
dematitis herpetiformis
HLA-Cw6-associated
psoriasis (type 1)
Non-HLA-Cw6-associatedpsoriasis(type 2)
Innate immunity boundary(main tissue players: target tissues of immune response, e.g. skin commensals,skin injury, regulation of keratinocyte growth; joint tissue-specific factors, e.g.
enthesis stressing and microdamage)
Psoriaticarthritis
Naildisease
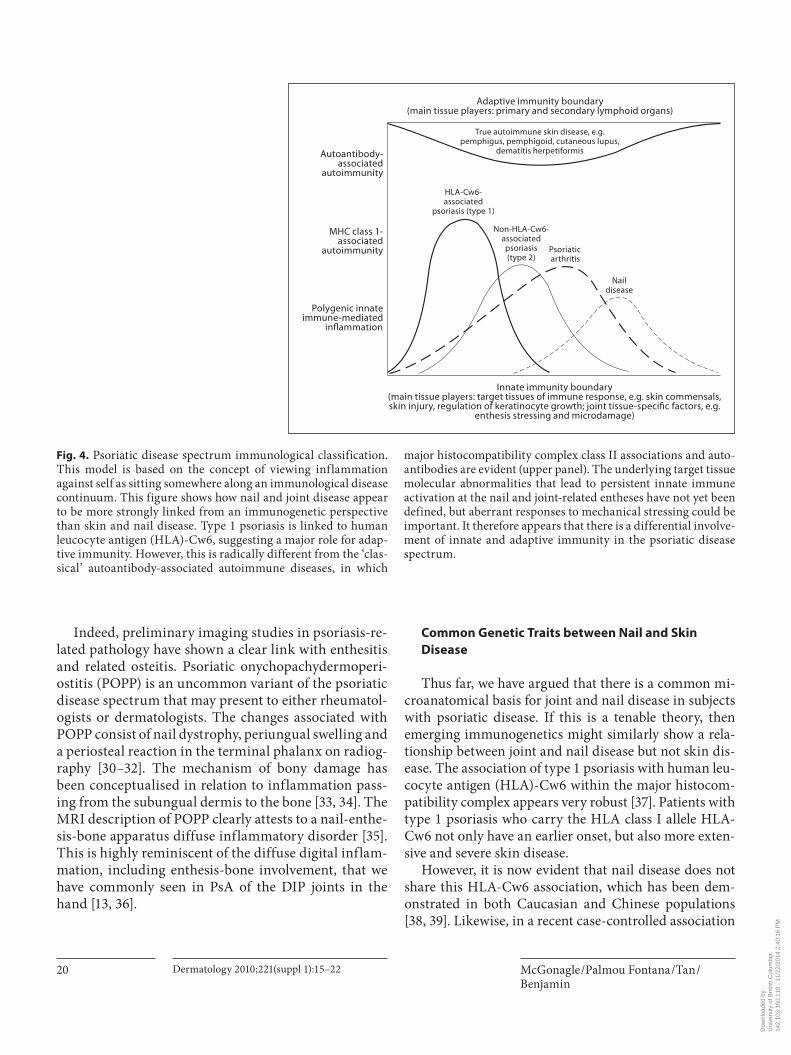
Fig. 4. Psoriatic disease spectrum immunological classification. This model is based on the concept of viewing inflammation against self as sitting somewhere along an immunological disease continuum. This figure shows how nail and joint disease appear to be more strongly linked from an immunogenetic perspective than skin and nail disease. Type 1 psoriasis is linked to human leucocyte antigen (HLA)-Cw6, suggesting a major role for adap-tive immunity. However, this is radically different from the ‘clas-sical’ autoantibody-associated autoimmune diseases, in which
major histocompatibility complex class II associations and auto-antibodies are evident (upper panel). The underlying target tissue molecular abnormalities that lead to persistent innate immune activation at the nail and joint-related entheses have not yet been defined, but aberrant responses to mechanical stressing could be important. It therefore appears that there is a differential involve-ment of innate and adaptive immunity in the psoriatic disease spectrum.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

Nail in Psoriatic Disease Dermatology 2010;221(suppl 1):15–22 21
study, the HLA-Cw6 phenotype frequencies were com-pared between patients with PsA and type 1 and 2 pso-riasis alone, and it was concluded that carrying the HLA-Cw6 gene was associated with psoriasis alone and not PsA [40] . The same group investigated the interleukin (IL)-23R and IL-12B genetic polymorphisms that have been linked to psoriasis [41] . The group concluded that the recently described IL-23R/IL-12B genetic associa-tions were ‘primarily associated with psoriasis suscepti-bility’ [41] . It will be intriguing to see whether psoriasis-related nail disease is linked to the IL-12/IL-23 genetic polymorphisms.
Improved Classification of Psoriatic Disease Based on an Understanding of the Nail
The classically recognised autoimmune diseases, such as rheumatoid arthritis and diabetes, invariably attack one antigenic territory and progress inexorably until it is destroyed. However, we feel that the pattern of psoriasis and PsA and nail disease points to a radically different immunopathology. Psoriasis has been considered an au-toimmune disease. However, there has been a ‘swinging pendulum’ of academic dermatology research that has oscillated between the concept of a T-cell-mediated dis-order versus a keratinocyte-mediated disorder. Based in part on our research in PsA, we have proposed a new clas-sification for human inflammatory disease that is termed the immunological disease continuum [42] . This contin-uum sets boundaries for adaptive immune-driven dis-ease at one extreme and innate immune-driven disease at the other. This classification scheme accommodates both T-cell and keratinocyte paradigms of psoriasis [43] . Tis-sue-specific factors, many of which are likely to be ill-defined but include trauma responses and host-microbe interactions, are likely to underscore the psoriatic disease spectrum of disorders. It has further been proposed that in the case of type 1 psoriasis, the innate immune activa-tion taking place in the skin may break tolerance for a specific hitherto undefined antigen, leading to T-cell im-munoreactivity [43] , and this represents the autoimmune part of the psoriatic disease spectrum. But in the case of nail and joint disease, the innate immune response may play a much greater role in disease [43] ( fig. 4 ).
So far, it appears that T-cell responses are more domi-nant in skin disease but that innate immune responses are more dominant in joint and nail disease, which is sup-ported by the observation that T-cell-directed therapies may be useful for the skin but not the joints [42] . In sup-
port of these concepts, innate immune cytokine pathway blockade with infliximab and other anti-tumour necrosis factor (TNF) agents may be more efficacious in joint and nail disease [44] , since lower dosing is more effective than in skin disease, in which a larger dose is generally needed.
Conclusions
In this article, we argue that a relatively ignored skin and musculoskeletal appendage, the nail, appears to hold the key to understanding the genetic and immunological basis for psoriatic disease. Although much has been writ-ten about animal models of psoriasis, these have tended to ignore the nail phenotype in human psoriasis. The ad-vent of high-resolution imaging in man to explore the nail, coupled with emerging immunogenetics and thera-pies, holds the key to a better understanding of nail dis-ease and indeed systemic disorders that afflict the nail in man. The emerging data showing excellent response of psoriatic nail disease to anti-TNF therapies [44–46] that act principally on the innate arm of the immune response further support the idea of local innate immune respons-es in the nail-enthesis-bone apparatus as underscoring disease mechanisms at that site.
Conflicts of Interest
Dennis McGonagle serves as a scientific speaker for Schering Corporation, a subsidiary of Merck & Co., Inc. Editorial support for the development of this publication was provided by Schering Corporation, a subsidiary of Merck & Co., Inc.
References 1 Wright V: Psoriasis and arthritis. Ann Rheum Dis 1956; 15: 348–356.
2 Gisondi P, Tinazzi I, El-Dalati G, et al: Lower limb enthesopathy in patients with psoriasis without clinical signs of arthropathy: a hos-pital-based case-control study. Ann Rheum Dis 2008; 67: 26–30.
3 Scarpa R, Ayala F, Caporaso N, Olivieri I: Psoriasis, psoriatic arthritis, or psoriatic dis-ease? J Rheumatol 2006; 33: 210–212.
4 Jiaravuthisan MM, Sasseville D, Vender RB, Murphy F, Muhn CY: Psoriasis of the nail: anatomy, pathology, clinical presentation, and a review of the literature on therapy. J Am Acad Dermatol 2007; 57: 1–27.
5 Zaias N: Nail in Health and Disease, ed 2. London, Appleton and Lange, 1990.
6 de Berker DA, Andre J, Baran R: Nail biology and nail science. Int J Cosmet Sci 2007; 29: 241–275.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M

McGonagle /Palmou Fontana /Tan /Benjamin
Dermatology 2010;221(suppl 1):15–2222
7 Fleckman P: Structure and function of the nail unit; in Scher RK, Daniel CR III (eds): Nails: Diagnosis, Therapy, Surgery, ed 3. Philadelphia, Elsevier, 2005, pp 13–26.
8 Martin BF, Platts MM: A histological study of the nail region in normal human subjects and in those showing splinter haemorrhages of the nail. J Anat 1959; 93: 323–330.
9 Frenz C, Fritsch H, Hoch J: Plastination his-tologic investigations on the inserting pars terminalis aponeurosis dorsalis of three - sec-tioned fingers. Ann Anat 2000; 182: 69–73.
10 Tan AL, Benjamin M, Toumi H, et al: The relationship between the extensor tendon enthesis and the nail in distal interphalan-geal joint disease in psoriatic arthritis – a high-resolution MRI and histological study. Rheumatology (Oxford) 2007; 46: 253–256.
11 McGonagle D, Tan AL, Benjamin M: The nail as a musculoskeletal appendage – impli-cations for an improved understanding of the link between psoriasis and arthritis. Der-matology 2009; 218: 97–102.
12 Tan AL, Grainger AJ, Tanner SF, Emery P, McGonagle D: A high-resolution magnetic resonance imaging study of distal interpha-langeal joint arthropathy in psoriatic arthri-tis and osteoarthritis: are they the same? Ar-thritis Rheum 2006; 54: 1328–1333.
13 McGonagle D, Gibbon W, O’Connor P, Green M, Pease C, Emery P: Characteris-tic magnetic resonance imaging entheseal changes of knee synovitis in spondylar-thropathy. Arthritis Rheum 1998; 41: 694–700.
14 Jevtic V, Watt I, Rozman B, Kos-Golja M, Demsar F, Jarh O: Distinctive radiological features of small hand joints in rheumatoid arthritis and seronegative spondyloarthritis demonstrated by contrast-enhanced (Gd-DTPA) magnetic resonance imaging. Skele-tal Radiol 1995; 24: 351–355.
15 McGonagle D: Imaging the joint and enthe-sis: insights into pathogenesis of psoriatic ar-thritis. Ann Rheum Dis 2005; 64:ii58–ii60.
16 Benjamin M, McGonagle D: The anatomical basis for disease localisation in seronegative spondyloarthropathy at entheses and related sites. J Anat 2001; 199: 503–526.
17 Benjamin M, McGonagle D: Histopatholog-ic changes at ‘synovio-entheseal complexes’ suggesting a novel mechanism for synovitis in osteoarthritis and spondylarthritis. Ar-thritis Rheum 2007; 56: 3601–3609.
18 Benjamin M, Toumi H, Suzuki D, Redman S, Emery P, McGonagle D: Microdamage and altered vascularity at the enthesis-bone in-terface provides an anatomic explanation for bone involvement in the HLA-B27-associat-ed spondylarthritides and allied disorders. Arthritis Rheum 2007; 56: 224–233.
19 McGonagle D, Lories RJ, Tan AL, Benjamin M: The concept of a ‘synovio-entheseal com-plex’ and its implications for understanding joint inflammation and damage in psoriatic arthritis and beyond. Arthritis Rheum 2007; 56: 2482–2491.
20 Raychaudhuri SP, Jiang WY, Raychaudhuri SK: Revisiting the Koebner phenomenon: role of NGF and its receptor system in the pathogenesis of psoriasis (comment). Am J Pathol 2008; 172: 961–971.
21 Baker BS, Powles AV, Lambert S, Valdimars-son H, Fry L: A prospective study of the Koebner reaction and T lymphocytes in un-involved psoriatic skin. Acta Derm Venereol 1988; 68: 430–434.
22 Sahin GO, Akyol M, Ozcelik S: An unusual Koebner phenomenon secondary to PPD with pustular and arthropathic psoriasis. Eur J Dermatol 2007; 17: 446.
23 Fawcett RS, Linford S, Stulberg DL: Nail ab-normalities: clues to systemic disease. Am Fam Physician 2004; 69: 1417–1424.
24 Marcilly MC, Balme B, Haftek M, et al: Sub-total hereditary leukonychia, histopatholog-ical and electron microscopy study of ‘milky’ nails. Ann Dermatol Venereol 2003; 130: 50–54.
25 Samman PD, Fenton DA (eds): The Nailin Disease. London, William Heinemann, 1986.
26 Baran R, Dawber RPR (eds): Diseases of the Nail and Their Management. Oxford, Black-well Scientific Publications, 1984.
27 Lewin K, DeWit S, Ferrington RA: Pathology of the finger nail in psoriasis: a clinicopatho-logical study. Br J Dermatol 1972; 86: 555–563.
28 Namey TC, Rosenthall L: Periarticular up-take of 99mtechnetium diphosphonate in psoriatics: correlation with cutaneous activ-ity. Arthritis Rheum 1976; 19: 607–612.
29 McGonagle D, Marzo-Ortega H, Benjamin M, Emery P: Report on the Second In-ternational Enthesitis Workshop. Arthritis Rheum 2003; 48: 896–905.
30 Mahoney JM, Scott R: Psoriatic onychopach-ydermoperiostitis (POPP): a perplexing case study. J Am Podiatr Med Assoc 2009; 99: 140–143.
31 Resnick D, Broderick TW: Bony prolifera-tion of terminal toe phalanges in psoriasis: the ‘ivory’ phalanx. J Can Assoc Radiol 1977; 28: 187–189.
32 McGonagle D, Conaghan PG, Emery P: Pso-riatic arthritis: a unified concept twenty years on. Arthritis Rheum 1999; 42: 1080–1086.
33 Jury CS, Fleming C, Kemmett D: Severe nail dystrophy associated with painful finger-tips. Diagnosis: psoriatic onychopachyder-moperiostitis (POPP). Arch Dermatol 2000; 136: 925–930.
34 Srivastava M, Solomon G, Strober B: Psori-atic onycho-pachydermo periostitis. Derma-tol Online J 2007; 13: 20.
35 Bongartz T, Harle P, Friedrich S, et al: Suc-cessful treatment of psoriatic onycho-pachy-dermo periostitis (POPP) with adalimumab. Arthritis Rheum 2005; 52: 280–282.
36 Marzo-Ortega H, McGonagle D, Rhodes LA, et al: Efficacy of infliximab on MRI-deter-mined bone oedema in psoriatic arthritis. Ann Rheum Dis 2007; 66: 778–781.
37 Elder JT: Genome-wide association scan yields new insights into the immunopatho-genesis of psoriasis. Genes Immun 2009; 10: 201–209.
38 Gudjonsson JE, Karason A, Antonsdottir AA, et al: HLA-Cw6-positive and HLA-Cw6-negative patients with psoriasis vulga-ris have distinct clinical features. J Invest Dermatol 2002; 118: 362–365.
39 Fan X, Yang S, Sun LD, et al: Comparison of clinical features of HLA-Cw * 0602-positive and -negative psoriasis patients in a Han Chinese population. Acta Derm Venereol 2007; 87: 335–340.
40 Ho PY, Barton A, Worthington J, Thomson W, Silman AJ, Bruce IN: HLA-Cw6 and HLA-DRB1 * 07 together are associated with less severe joint disease in psoriatic arthritis. Ann Rheum Dis 2007; 66: 807–811.
41 Filer C, Ho P, Smith RL, et al: Investigation of association of the IL12B and IL23R genes with psoriatic arthritis. Arthritis Rheum 2008; 58: 3705–3709.
42 McGonagle D, McDermott MF: A proposed classification of the immunological diseases. PLoS Med 2006; 3:e297.
43 McGonagle D, Georgouli T: The importance of ‘Mechnikov’s thorn’ for an improved un-derstanding of 21st century medicine and immunology: a view from the eye. Scand J Immunol 2008; 68: 129–139.
44 Lawry M: Biological therapy and nail psoria-sis. Dermatol Ther 2007; 20: 60–67.
45 Rigopoulos D, Gregoriou S, Stratigos A, et al: Evaluation of the efficacy and safety of in-fliximab on psoriatic nails: an unblinded, nonrandomized, open-label study. Br J Der-matol 2008; 159: 453–456.
46 Rich P, Griffiths CEM, Reich K, et al: Base-line nail disease in patients with moderate to severe psoriasis and response to treatment with infliximab during 1 year. J Am Acad Dermatol 2008; 58: 224–231.
Dow
nloa
ded
by:
Uni
vers
ity o
f Brit
ish
Col
umbi
a
14
2.10
3.16
0.11
0 -
11/2
2/20
14 2
:40:
16 P
M