Embed Size (px)
Citation preview

5/05/2015
Copyright Stephen Janz 2015 1
Stephen Janz BN BAc GCCHM MPH
Clinic Director: Kenmore Centre for Health (Qld)
Notes available at http://www.kenmorecentreforhealth.com.au/links/670-2/
Password is MAY2015
Copyright Stephen Janz 2015
About these notes� These notes have been developed for use by acupuncturists
registered with the Chinese Medicine Board of Australia who have attended the workshop in person.
� Contra-indications, cautions and treatment recommendations are not intended to comprehensively consider all aspects of acupuncture, rather they highlight aspects specifically relevant to trigger point acupuncture.
� Always use your professional judgement and work within your skills, knowledge and experience.
� References provide useful additional guidance.� Consider accessing additional training, or referring
patients to a suitably qualified practitioner if you are not confident the principles outlined in this workshop.
Copyright Stephen Janz 2015
Myofacial Trigger Points (MTrPs)� “hyperirritable spots in skeletal muscle that
are associated with a hypersensitive palpable nodule in a taught band.”(Travall and Simons 1999)
� Consist of a bundle of contracted muscle fibres
� Produce local or referred pain or paresthesia
when active.
� Fairly predictable referral patterns.
� Muscle twitch and jump sign when needled
(deep needling).
Copyright Stephen Janz 2015
Role of Trigger Point Charts� A reminder to consider if an active trigger point may
be involved. Not exact locations – must Palpate.
� 1. If the problem is in the front, look in the back.
� 2. If the problem is in the back, look in the front.
� 3. If the problem is above, look below.
� 4. If the problem is below, look above
Copyright Stephen Janz 2015
Types of trigger points� Active TP – pressing point reproduces current
symptoms.
� Latent – not currently producing symptoms, but has potential to become active if recurrent strain etc. egpainful Co 10 on palpation on patient with tennis elbow on non-painful arm.
� Primary – often located around the centre of a motor unit. Treating this will have a broader effect
� Secondary – develop in response to primary. May not be in same muscle. Often will be in antagonist muscle as well.
Copyright Stephen Janz 2015
Why are trigger points important?� Their presence indicates unresolved past injury, or ongoing
trauma eg, postural strain, radiculopathy, stress.
� They cause shortening of the muscle fibres and impact on function (eg reduced joint ROM), increasing further compensatory patterns and Qi & Blood stagnation; increases risk of future injury/pathology.
� They may cause the presenting symptom.
� Treating trigger points has ANS and central neural impacts, not just local impacts. (central sensitisation, allodynia, hyperalgesia: remember, many are standard acupuncture points as well).
� Better, faster results.
Copyright Stephen Janz 2015

5/05/2015
Copyright Stephen Janz 2015 2
Treating trigger points� Massage (Tuina, Acupressure, Shiatsu etc.)
� Streching
� Injection: local anaesthetic/saline
� Acupuncture
Copyright Stephen Janz 2015
Acupuncture techniques� Deep needling – typical technique used to evoke
twitch response and typical “Ashi!” reaction. Increased risk of organ puncture and pneumothorax. The subject of this workshop
� Superficial needling – insertion from 5-10 mm over a trigger point. Typically no twitch response. Typically used where vessel puncture a risk eg anterior neck points; or sensitive patient.
� Electro-stimulation; -points connected via electro stimulator at 4 Hz or dense –disperse. Good for tight bands eg lumbar Bladder points, forearm.
Copyright Stephen Janz 2015
Trigger Point acupuncture
and Risks� Characterised by deep techniques with high risk of
organ puncture.
� Increased risk of bleeding/bruising compared to some other acupuncture methods.
� Typically painful during treatment & up to 24 hr-48hours post treatment.
� Serious risks linked to duration of training (Janz & Adams 2011).
Copyright Stephen Janz 2015
Pneumothorax Risk� MTrP needling favours deep techniques that are
typically painful at the time and can result in 24 hours post treatment pain.
� Inherently higher risk of pneumothorax with deep techniques .(Gunn 1989)
� Pneumothorax is the most common cause of death from acupuncture .(Ernst 2010)
� Guild Insurance (WA) notes pneumothorax associated with physiotherapy acupuncture and advocates improved training. (Baker 2006)
Copyright Stephen Janz 2015
Iatrogenic pneumothorax: safety concerns when using
acupuncture or dry needling in the thoracic region (2011) by
Leigh McCutcheon & Michael Yelland
� Pneumothoraxes have been reported from needling the following points and region ST11 and ST12 in the supraclavicular region; LU2, ST2, and KI27 in the infraclavicular region; KI22 and KI27, ST12 to ST18 in the mid-clavicular line, and BL41 to BL50, rhomboids, serratusposterior superior, levator scapulae, splenius cervicus, longissimus thoracis, iliocostalis thoracis, semispinalisthoracis, cervicus and capitus in the medial scapular. This paper is available at: http://www.researchgate.net/publication/233574856_Iatrogenic_pneumothorax_safety_concerns_when_using_acupuncture_or_dry_needling_in_the_thoracic_region
Copyright Stephen Janz 2015
Lung Fields� 1. Anterior border : Apex=3-4 cm above inner third of
clavicle, Base=rests on diaphragm (6th rib)
� 2. Posterior border:
� Apex=C7, Base=T10
� 3. Lateral border:
� Apex=axilla down to 7-8th rib
http://quizlet.com/44972349/fscj-ha-unit-2-thorax-and-lungs-assessment-flash-cards/
Copyright Stephen Janz 2015

5/05/2015
Copyright Stephen Janz 2015 3
Posterior Lung Fields
C7 to T10
Copyright Stephen Janz 2015
Pneumothorax Signs & Symptoms� Small pneumothoraces are occasionally asymptomatic.
� Symptoms of pneumothorax include dyspnea and pleuritic chest pain. � Dyspnea may be sudden or gradual in onset depending on the rate of
development and size of the pneumothorax.� Pain can simulate pericarditis, pneumonia, pleuritis, pulmonary
embolism, musculoskeletal injury (when referred to the shoulder), or an intra-abdominal process (when referred to the abdomen).
� Pain can also simulate cardiac ischemia, although typically the pain of cardiac ischemia is not pleuritic.
� If the pneumothorax is large, the affected side may be enlarged with the trachea visibly shifted to the opposite side. With tension pneumothorax, hypotension can occur.
� http://www.merckmanuals.com/professional/pulmonary_disorders/mediastinal_and_pleural_disorders/pneumothorax.html
Copyright Stephen Janz 2015
Pneumothorax Treatment� Immediate needle decompression for tension
pneumothoraces
� Observation and follow-up x-ray for small, asymptomatic, primary spontaneous and iatrogenic pneumothoraces� ie follow-up chest x-rays done at about 6 and 48 h show
no progression.
� Catheter aspiration for large or symptomatic primary or iatrogenic spontaneous pneumothoraces
� Tube thoracostomy for secondary and traumatic pneumothoraces
Copyright Stephen Janz 2015
Pneumothorax first aid� Management of a Penetrating Chest Wound: � 1. Follow DRSABCD. � 2. Place patient in whatever position makes breathing easiest.
� The most comfortable position, which will assist breathing, is half-sitting, leaning to the injured side.
� 3. Cover the wound – use the patient’s or your own gloved hand. � 4. Cover wound with a dressing, such as plastic sheet, bag,
aluminium foil or sterile dressing. � 5. Seal with tape on three sides (not bottom), to allow fluid to
escape. � 6. Call triple zero for an ambulance
� http://e-firstaid.stjohn.org.au/text_alt/topic_12/index.html
� Remember symptoms may not manifest for several hours after injury.
Copyright Stephen Janz 2015
Method for Deep needling.
� Consider patient position wrt point selection.� Palpate to locate the trigger point. � Isolate the trigger point with the left hand (pinching up point
preferred if over sensitive underlying structures eg lungs).� Insert needle into trigger point. � Lift and thrust with pecking action to elicit twitch response.� May need to use chicken feet method to find active Tp.� Retention time – 30 seconds to as long as a typical acupuncture
treatment.� Only stimulate to patients acceptance “Would you like me to use
some more points or is that enough for today?”.� Swab essential to control any post treatment bleeding.� May need to use at least one gloved hand.
Copyright Stephen Janz 2015
Contra-indications for Deep
Needling of Trigger Points � Sensitive patient (consider massage or superficial
needling instead)
� Bleeding disorder/anti-coagulants
� Weak constitution
� Anxious patient – strong sensations rarely acceptable.
� ? pregnancy
Copyright Stephen Janz 2015

5/05/2015
Copyright Stephen Janz 2015 4
Cautions� Points overlying the Lungs and pleura
� Avoid intercostal spaces
� Points overlying other internal organs
� Points overlying major vessels & nerves
� Avoid leaving patient alone with needles insitu at Gb21 or other similarly potentially vulnerable locations when deep needling techniques are used.
� If it is desirable for needles to be retained and the patient left unattended consider partial withdrawal following initial needling.
Copyright Stephen Janz 2015
Post treatment� Stretch treated muscle post-treatment for best results.� Remind patient that may be achy in the treated area for one
or two days and that this is typical of this specific technique.
� Record in patient notes if a trigger point has been used egGb21 T
� Educate that follow-up treatment is necessary to achieve a lasting result, and points become less reactive as pathology resolves.
� Consider giving written advice regarding the different types of acupuncture methods you use, and that you also use other non-painful techniques. Trigger points are just one part of the toolkit.
Copyright Stephen Janz 2015
Trigger Point Acupuncture� Don’t forget, your acupuncturists!
� Use appropriate distal points where indicated.
� Resolving symptoms associated with trigger points may give rapid initial relief – now look to what's left.
� Postural issues leading to Qi & Blood stagnation? –exercise and counselling
� Stress issues leading to Qi & Blood stagnation? (ANS) -acupuncture/herbs/exercise/counselling
� Referral
Copyright Stephen Janz 2015
Locating Points� Palpation
� Guided by charts of common referral patterns
� Can take a purely anatomical approach or regional approach.
� Points are often not at the location of pain:
� If symptoms on front – look to back
� If symptoms below – look above etc.
� Compressing a trigger point produces a pattern of pain or paresthesia, often distal to the point.
Copyright Stephen Janz 2015
Local Twitch Response� Dispersing stagnant blood
� Allows circulation of Qi
� Local spinal reflex arc
� Motor end plate
Copyright Stephen Janz 2015
Jianjing GB21� Noteworthy Peculiarities About This Point Holmes Keikobad Acupuncture
Today June, 2004, Vol. 05, Issue 06I. It is the highest point on the trapezius in the sagittal plane.II. It sits astride on the very apex of the lung, which rises in a dome, bilaterally.III. If an insertion is done using a perpendicular trajectory, an injury is likely.IV. Any usage must factor in the rise of lung tissue at inspiration.V. If the point is needled in any position but prone, the risk increases greatly.VI. If the patient coughs or sneezes, the danger becomes manifold.VII. In tall men, and in smokers between the ages of 20-40, the risk of
spontaneous pneumothorax is significant.VIII. Constant supervision is necessary at all times during treatment if this point
is used.IX. The risk of accident increases if the risk was not explained to the patient.X. In a bony, thin man or woman, the hazard increases greatly.XI. In a person with concomitant scoliosis, lordosis and kyphosis, risk increases.
Copyright Stephen Janz 2015
5/05/2015
Copyright Stephen Janz 2015 5
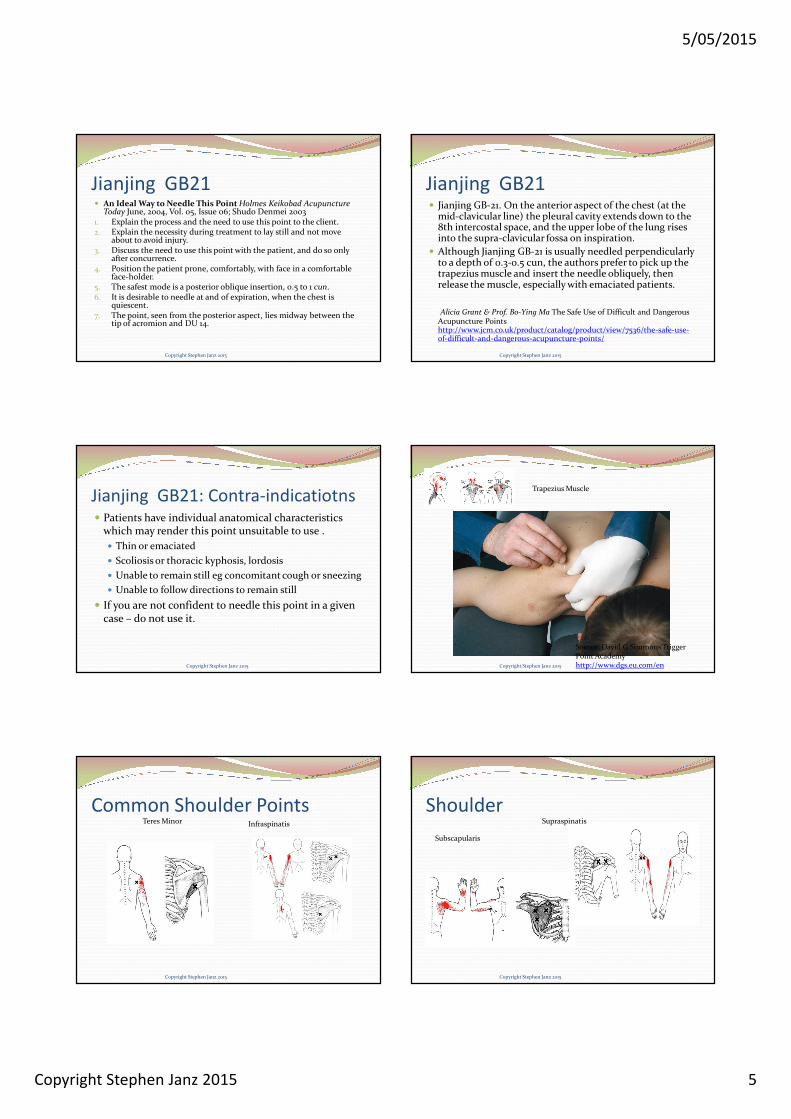
Jianjing GB21� An Ideal Way to Needle This Point Holmes Keikobad Acupuncture
Today June, 2004, Vol. 05, Issue 06; Shudo Denmei 20031. Explain the process and the need to use this point to the client.2. Explain the necessity during treatment to lay still and not move
about to avoid injury.3. Discuss the need to use this point with the patient, and do so only
after concurrence.4. Position the patient prone, comfortably, with face in a comfortable
face-holder.5. The safest mode is a posterior oblique insertion, 0.5 to 1 cun.6. It is desirable to needle at and of expiration, when the chest is
quiescent.7. The point, seen from the posterior aspect, lies midway between the
tip of acromion and DU 14.
Copyright Stephen Janz 2015
Jianjing GB21� Jianjing GB-21. On the anterior aspect of the chest (at the
mid-clavicular line) the pleural cavity extends down to the 8th intercostal space, and the upper lobe of the lung rises into the supra-clavicular fossa on inspiration.
� Although Jianjing GB-21 is usually needled perpendicularly to a depth of 0.3-0.5 cun, the authors prefer to pick up the trapezius muscle and insert the needle obliquely, then release the muscle, especially with emaciated patients.
Alicia Grant & Prof. Bo-Ying Ma The Safe Use of Difficult and Dangerous Acupuncture Points http://www.jcm.co.uk/product/catalog/product/view/7536/the-safe-use-of-difficult-and-dangerous-acupuncture-points/
Copyright Stephen Janz 2015
Jianjing GB21: Contra-indicatiotns� Patients have individual anatomical characteristics
which may render this point unsuitable to use .
� Thin or emaciated
� Scoliosis or thoracic kyphosis, lordosis
� Unable to remain still eg concomitant cough or sneezing
� Unable to follow directions to remain still
� If you are not confident to needle this point in a given case – do not use it.
Copyright Stephen Janz 2015
Source: David G Simmons Trigger Point Academy http://www.dgs.eu.com/en
Trapezius Muscle
Copyright Stephen Janz 2015
Common Shoulder PointsTeres Minor Infraspinatis
Copyright Stephen Janz 2015
ShoulderSupraspinatis
Subscapularis
Copyright Stephen Janz 2015

5/05/2015
Copyright Stephen Janz 2015 6
TMJLateral Pterygoid Masseter
Copyright Stephen Janz 2015
Shin Splints/AchiliesSoleusGastrocnemius
Copyright Stephen Janz 2015
Hip/Glut points
Copyright Stephen Janz 2015
Forearm
Copyright Stephen Janz 2015
References and Further reading� Baldry P. Trigger Point Acupuncture. In: Filshie J, White A, editors.
Medical Acupuncture. A western scientific approach. Edinburgh: Churchill Livingstone; 1998
� Chou, L., Kao, M., Lin, J. Probable mechanisms of needling therapies for myofascial pain control. Evidenced based complementary and alternative medicine. Vol 2012, Article ID 705327 DOI:10.1155/2012/705327
� Denmai, S. Finding effective acupuncture points(2003) Brown. S (translator). Eastland Press. Seattle.
� David G Simmons Trigger Point Academy http://www.dgs.eu.com/en� Dommerholt, J., Cesar Fernandez-de-las-Penas (ed) Trigger Point Dry
Needling (2013) Churchill Livingstone� Grant, A., Ma, B. The Safe Use of Difficult and Dangerous Acupuncture
Points http://www.jcm.co.uk/product/catalog/product/view/7536/the-safe-use-of-difficult-and-dangerous-acupuncture-points
Copyright Stephen Janz 2015
References and Further reading
cont� Janz, S., Adams. J., Acupuncture by Another Name: Dry Needling
in Australia. AJACM 2011 6(2)
� Legge, D. Close to the Bone: The Treatment of Musculo-skeletal Disorder with Acupuncture and other Traditional Chinese Medicine 1st and 3rd ed (1990; 2011) Sydney College Press.
� Nugent-Head, A. Ashi Points in Clinical Practice. Journal of Chinese Medicine no.101. Feb 2013.
� Quinter J., Bove M., Cohen M. A Critical evaluation of the trigger point phenomenon. Rheumatology. Advance access Dec 3 2014.
� The Trigger Point and Pain Referral Guide http://www.triggerpoints.net/
� www.kenmorecentreforhealth.com.au/links/670-2/ (seminar downloads) password May2015
Copyright Stephen Janz 2015





























