-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
1/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
CURRENTOPINION Muscle wasting: a nutritional criterion to
prioritizepatients for liver transplantation
Aldo J. Montano-Loza
Purpose of review
Cirrhosis is the result of the progression of necroinflammatory
liver diseases leading to fibrosis, portalhypertension, and a
catabolic state, which might cause muscle wasting or sarcopenia. In
this review, weanalyze the methods for muscularity assessment, the
incidence and clinical impact of muscle wasting, andpotential novel
therapeutic strategies in cirrhosis. Finally, we evaluate the value
of muscle wasting inclusionto conventional systems for liver
transplant prioritization.
Recent findings
Muscle wasting is present in up to 45% of patients with
cirrhosis and is associated with higher risk of
sepsis-related death rather than liver failure mortality.
Despite the fact that muscle wasting is not included inthe scores
for prognosis in cirrhotic patients, as in the case of Model for
End-Stage Liver Disease (MELD) orChild-Pugh, its presence should
alert clinicians to the same extent as other complications do, such
asascites, hepatic encephalopathy, or variceal bleeding. Two
studies have shown increased mortality riskafter liver
transplantation in patients with muscle wasting, whereas one study
did not. Modification of MELDto include muscle wasting is
associated with a modest improvement in the prediction of mortality
in patientswith cirrhosis.
Summary
Muscle wasting is a frequent complication in cirrhosis and
contributes to increased risk of sepsis-relatedmortality. The
impact on mortality of muscle wasting after liver transplantation
is controversial and needsfurther study. The MELD-sarcopenia score
is associated with improvement in mortality prediction;
however,prior to the widespread use of this composite score,
validation in larger cohorts of patients with cirrhosis
isnecessary.
Keywordscirrhosis, liver transplant, organ allocation,
sarcopenia, scores for prognosis
INTRODUCTION
Cirrhosis is the result of the progression of manyforms of
necroinflammatory liver diseases leading tofibrosis, vascular
remodeling, portal hypertensiondevelopment and its complications,
and ultimatelyliver failure [1]. As currently there is no
effective
treatment to revert cirrhosis, management is gener-ally focused
on treating the primary liver disease,screening and controlling the
complications of por-tal hypertension, and considering liver
transplan-tation in patients with decompensated cirrhosis.Even
though liver transplantation may be con-sidered curative for
cirrhosis, this therapeutic optiondoes not exist for the majority
of patients.
Muscle wasting or sarcopenia is one of the mostcommon
complications in cirrhosis [2,36], anddespite the important role it
plays in the prognosisof cirrhosis, it is frequently overlooked,
mainly as
the nutrition assessment could be complex in cir-rhosis with
fluid retention and/or overweight[7,8].
At present, several methods are available toevaluate the body
composition and muscle massestimation of patient with cirrhosis;
however, mostof these techniques have limitations, primarily
because of lack of objectivity and reproducibility.In this
regard, muscularity assessment with cross-sectional imaging studies
[computed tomography
Division of Gastroenterology and Liver Unit, University of
Alberta
Hospital, Edmonton, Alberta, Canada
Correspondence to Aldo J. Montano-Loza, MD, MSc, PhD,
Assistant
Professor, Zeidler Ledcor Centre, 130 University Campus,
University of
Alberta, Edmonton, AB T6G 2X8, Canada. Tel: +1 780 248 1892;
fax: +1 780 248 1895; e-mail: [email protected]
Curr Opin Clin Nutr Metab Care 2014, 17:219225
DOI:10.1097/MCO.0000000000000046
1363-1950 2014 Wolters Kluwer Health | Lippincott Williams &
Wilkins www.co-clinicalnutrition.com
REVIEW
mailto:[email protected]:[email protected]
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
2/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
(CT) scan, or MRI] has become an attractive index ofnutritional
status evaluation in cirrhosis. These CTor MRI analyses are not
biased by the fluid overloadstatus that frequently presents in
decompensatedcirrhosis, and muscle wasting reflects a
chronicdetriment in the general physical condition, ratherthan
acute severity of the liver disease [9
&
].Muscle wasting in cirrhosis is part of the frailty
complex present in these patients, characterized bya decreased
reserve and resistance to stressors result-ing from cumulative
declines across multiplephysiologic systems, and predisposition to
poor out-comes[1012].
In this review, we discuss the currently acceptedand new
potential methods to evaluate the prog-nosis in cirrhotic patients.
We also discuss thecurrent evidence regarding frequency and
clinical
impact of muscle wasting in cirrhosis in order topromote
recognition of this complication and leadto strategies in an effort
to try to improve survivaland reduce morbidity associated with
cirrhosis.
PROGNOSTIC EVALUATION OF
CIRRHOSIS
The prognostic assessment of patients with cirrhosisremains a
complex challenge as the natural historyis particularly variable
because of several factors,including cause of the cirrhosis, liver
synthetic func-
tion, presence and degree of portal hypertension,the possibility
of resolution of the underlying dam-aging process, and the
occurrence of hepatocellularcarcinoma[13].
Child-Pugh and Model for End-Stage LiverDisease (MELD)[14]scores
constitute the most fre-quent tools to predict mortality in
patients withcirrhosis. Child-Pugh score was originally designedto
predict cirrhosis-related mortality during surgery,and has been
shown to be useful in determiningprognosis, treatment response, and
necessity forliver transplant. MELD was originally developed as
a prognostic model of early mortality in patientswith cirrhosis
who received a transjugular intra-hepatic portosystemic shunt
(TIPS). The originalMELD has subsequently been simplified
andcurrently it is widely used to predict short-termmortality in
different patient populations withcirrhosis. Moreover, in most
liver transplant centers,
MELD score has replaced the Child-Pugh score forpriority organ
allocation, and since 2002, the MELDscore has been used for the
prioritization of poten-tial liver transplant recipients in North
America,mainly because MELD was developed in a statisticalfashion
and includes only objective laboratoryparameters. Since
implementation of the MELDscore, there have been reports of
reductions in thenumber of patients listed for liver
transplantation,waiting time for liver transplant, and deaths on
thewaiting list.
Although MELD score has the advantage overChild-Pugh score of
being based on objective vari-ables [serum bilirubin, international
normalizedratio (INR) of prothrombin time, and serum creati-nine]
rather than on subjective evaluation of theseverity of clinical
findings (ascites and encephal-opathy), the MELD score also has
limitations, mostimportant of which are the variability of
bio-chemical parameters and lack of evaluation of thenutritional
and functional status.
PREVALENCE AND ORIGIN OF MUSCLE
WASTING IN CIRRHOSIS
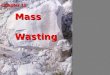
Muscle wasting in cirrhosisseemsto be secondary to
amultifactorial process and generally is more frequentas liver
disease progresses as the factors that lead tomalnutrition in the
first place become more prom-inent. The most important factors
associated withmuscle wasting in cirrhosis include metabolic
abnor-malities, insufficient oral intake (mainly because ofearly
satiety in moderate-severe ascites), malabsorp-tion, and impaired
capacity of the liver to metabolizeand save nutrients, among others
(Fig. 1).
The frequency of malnutrition in cirrhosis hasbeen estimated to
affect between 40 and 90% of
patients. This wide range is explained in part as thereare
significant differences in the operational defi-nition of
malnutrition in cirrhosis. For example, it isdifficult to establish
the presence of calorie malnu-trition, and as adipose tissue is the
largest pool ofcalories, fat malnutrition is generally defined
asreduction in body fat mass. However, as mostproteins are located
in the skeletal muscle, a properdefinition of clinical protein
malnutrition shoulduse primarily loss of skeletal muscle [15
&
].Recent studies have found that muscle wasting,
established by cross-sectional imaging studies, is
KEY POINTS
Muscle wasting is a frequent complication in cirrhosisand
contributes to increased mortality, mainly related tosepsis-related
death.
Cross-sectional imaging studies with computedtomography or MRI
constitute the gold standard
techniques to quantify skeletal muscle mass and identifymuscle
wasting in cirrhosis.
Inclusion of muscle wasting to MELD score is associatedwith a
modest improvement in the prediction ofshort-term mortality in
patients with cirrhosis.
Translational research in wasting diseases
220 www.co-clinicalnutrition.com Volume 17 Number 3 May 2014
http://-/?-http://-/?-
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
3/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
present in up to 45% of patients with cirrhosis[2,3,5,6] (Table
1) [26,16]. Importantly, being over-weight and obesity are now
endemic in Westerncountries. Patients with cirrhosis may develop
sim-ultaneous loss of skeletal muscle and gain of adipose
tissue, culminating in the condition of sarcopenicobesity.
Moreover, muscle depletion is characterizedby both a reduction in
muscle size and increasedproportion of intermuscular and
intramuscular fat[17].
Sarcopenia in
cirrhosis
Diminished
nutrient intake
Early satiety
- Impaired gastric accommodation
- Ascites
Impaired digestion and nutrient
absorption
- Portal hypertensive enteropathy
Loss of appetite
- Cytokines (TNF-)
Hospitalizations
- Lack of regular meals for examinations
and procedures
Hyperdynamic circulation
- Increase use of macronutrients and
micronutrients
Cytokine-driven hypermetabolism
- High energy expenditure and demand
Compromised gut barrier function
- Bacterial translocation
- Infections
Loss of body protein
- Inadequate synthesis
- Diminished storage capacity
- Affected enterohepatic circle
- Multiple paracentesis
Decrease hepatic glycogen reserves
- Early switch to gluconeogenesis
- Mobilization of amino acids from the
skeletal muscles
Hypermetabolic
state
Inadequate
synthesis or
absorption ormicro-
macronutrients
FIGURE 1. Factors associated with muscle wasting development in
patients with cirrhosis.
Table 1. Clinical studies describing the prevalence and clinical
significance of muscle wasting in patients with cirrhosis
Author/year n
Frequency
of musclewasting (%)
Definition
of musclewasting
Method for
muscularityassessment
Clinicalsignificance
Englesbe et al.[6]2010
163 25 Lowest quartile TPA CT Low TPA was associated
withmortality after liver transplant
Montano-Lozaet al.[2]2012
112 40 L3 SMI 38.5cm2/m2
for women and 52.4cm2/m2
for men
CT Sarcopenia was independentlyassociated with mortality
Meza-Junco et al.[3]2013
116 30 L3 SMI 38.5cm2/m2
for women and 52.4cm2/m2
for men
CT Sarcopenia was independentlyassociated with mortality
Kaido et al.[4]2013
124 38 Low skeletal muscle mass BIA Low skeletal mass associated
withpost-transplant mortality in patientsundergoing LDLT
Krell et al.[5]2013
207 33 Lowest tertile TPA CT Lower TPA was associated with
higherrisk for post-transplant infectiouscomplications and
mortality
Hayashi et al.[16]2013
50 40 SMMI 6.87kg/m2 for menand 5.46kg/m2 and/or musclestrength
(hand grip); 24kg formen and 14kg for women
BIA andhandgripstrength
Patients with sarcopenia had lowvalues of energy intake per
idealbody weight and number of steps
BIA, bioelectrical impedance analysis; CT, computed tomography;
HR, hazard ratio; LDLT, living donor liver transplantation; SMMI,
skeletal muscle mass index;TPA, total psoas area.
Muscle wasting: a criterion for liver transplantMontano-Loza
1363-1950 2014 Wolters Kluwer Health | Lippincott Williams &
Wilkins www.co-clinicalnutrition.com 221
http://-/?-http://-/?-
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
4/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
We have found that 20% of our patients withcirrhosis being
evaluated for liver transplantationhad sarcopenic obesity, and low
muscle attenuationreflective of muscle fat infiltration was present
inmore than 50% of patients[17].
BODY COMPOSITION EVALUATION IN
CIRRHOSIS
Cirrhotic patients commonly have significantchanges in their
body composition mainly charac-terized by increase in the
extracellular fluids anddecrease in muscle and adipose tissue;
however,clinical identification of body composition changesin
cirrhotic patients with ascites and edema might bechallenging, as
fluid gains hide muscle and adiposetissue losses. It seems that
cirrhotic male patientshave more muscle wasting, whereas female
patientstend to have more depletion of fat tissue, and thereare
studies that have shown that changes in bodycomposition may
progress with thecourseof the liverdisease and correlate with the
Child-Pugh score.
Numerous indirect methods have been usedto quantify body
composition in cirrhosis, suchas total body electrical
conductivity, bioelectricalimpedance, dual energy x-ray
absorptiometry, airdisplacement plethysmography, and
magneticresonance spectroscopy. These methods are basedon the
principle that body fat mass and lean masshave specific components,
such as water, proteins,and minerals. Therefore, by establishing
the totalbody weight and fat mass, the remaining weightshould be
lean mass. Unfortunately, most of these
methods lack either availability and/or reproduci-bility, and
their accuracy may be limited in thepresence of fluid
retention.
Other techniques include the skin-fold thick-ness measurement
that quantifies fat mass in theupper arm (mid-arm muscle area)
using a caliper;however, there have been conflicting reports inthe
accuracy for predicting malnutrition in cirrhosisbecause of
interobserver variability, and thismethod does not correlate with
Child-Pugh score.A recent study showed that low respiratory
quotientoccurs in cirrhosis, and even this finding did not
predict mortality; the author reported a direct andsignificant
relation between respiratory quotientand muscle area, which
suggests that altered skeletalmuscle protein turnover contributes
to this meta-bolic response [18
&
].
MUSCLE WASTING EVALUATION IN
CIRRHOSIS
CT scan and MRI are the gold standard tools toquantify skeletal
muscle mass[19]and, hence, con-stitute a good resource for
objective nutritionalassessment of cirrhotic patients and detection
of
muscle wasting. Recently, our group performed ananalysis of the
frequency and clinical impact ofmuscle wasting in cirrhotic
patients being evaluatedfor liver transplant[2]. We used CT scans
at the 3rdlumbar (L3) vertebrae analyzed with the SliceOmaticV4.3
software (Tomovision, Montreal, Quebec,Canada), which enables
specific tissue demarca-
tion using previously reported Hounsfield unitthresholds.
Skeletal muscle was identified and quan-tified by Hounsfield unit
thresholds of29 to 150,and cross-sectional area of muscle and
adipose tissuewas normalized for stature (cm2/m2) as reported
inprevious studies[20]. The L3 skeletal muscle index(L3 SMI) was
expressed as cross-sectional musclearea/height2, and cut-offs for
muscle wasting werebased on a CT-based sarcopenic study for
patientswith solid malignancies (L3 SMI: 38.5 cm2/m2
for women and 52.4 cm2/m2 for men) [21].In addition, we recently
set up new cut-off valuesfor cirrhotic patients, and values were
similar com-pared with patients with malignancies (L3 SMI:42cm2/m2
for women and 50cm2/m2 for men)[22]. We also found that muscle
wasting is notexclusively present in underweight patients,
andconstitutes a hidden condition that can be presentin cirrhotic
patients with any BMI.
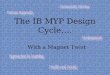
To exemplify that there is no adequate corre-lation of classical
anthropometric measurement andmuscle wasting, in Fig. 2 we present
images of the L3SMI analysis of two cirrhotic patients with
identicalBMI, but one with and another without musclewasting.
COMPLICATIONS OF MUSCLE WASTING
IN CIRRHOSIS
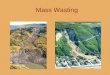
Muscle wasting is associated with mortality inpatients with
cirrhosis. We have reported thatmedian survival for cirrhotic
patients being eval-uated for liver transplantation was
significantlyworse in the presence of muscle wasting (196vs. 3411
months, log-rank, P0.005) (Fig. 3).Six-month probability of
survival was 71% in sarco-penic, and 90% in nonsarcopenic patients,
and thishigher mortality risk was related to sepsis-related
death rather than liver failure mortality [2]. Thismay explain
why conventional scores that reflectmainly liver function, such as
MELD and Child-Pugh do not detect mortality risks associated
withmuscle wasting.
THERAPEUTIC OPTIONS FOR MUSCLE
WASTING IN CIRRHOSIS
In patients with cirrhosis, increased protein intakehas been
demonstrated to be safe, well tolerated,and beneficial; however,
the long-term effects onmuscle mass are not completely elucidated.
Other
Translational research in wasting diseases
222 www.co-clinicalnutrition.com Volume 17 Number 3 May 2014
http://-/?-http://-/?-http://-/?-http://-/?-
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
5/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
strategies that have been evaluated include late-evening snacks,
repeated snacks, branched chainamino acid, and protein
supplementation in generalwith beneficial results, but their impact
on musclemass needs further investigation[16,23,24].
Intake of leucine-enriched essential amino acidnutrient may be
useful in the treatment of musclewasting in cirrhosis. Leucine is
an essential aminoacid that serves as substrate for protein
synthesis,and has a key role in the regulation of the
skeletalmuscle anabolism, protein synthesis, and auto-phagy. The
activation of anabolic signaling occursvia the mammalian target of
rapamycin (mTOR)through an undefined mechanism [25,26]. These
data suggest a potential role for leucine-rich supple-ments in
the management of muscle depletionin cirrhosis.
Exercise, including aerobic and resistancephysical activity are
important for the musclemetabolism. However, patients with
cirrhosis fre-quently have complications of portal
hypertension,such as ascites or hepatic encephalopathy, or
symp-toms associated to chronic illness, including signi-ficant
fatigue and reduced maximum exercisecapacity, which significantly
reduce the physicalactivity. In addition to this, even moderate
exercise
augments the portal pressure and may increase therisk of
variceal bleeding in patients with esophagealvarices; therefore,
cirrhotic patients with portalhypertension should be advised of
potential risksduring exercise, and patients who are able
andwilling to enter in an exercise program may benefitfrom
pharmacological or endoscopic prophylaxis.
An interesting therapeutic approach in cirrhoticmuscle wasting
could be the use of TIPS. A recentstudy showed that TIPS may
reverse muscle wasting,and failure to improve muscle mass after
TIPS isassociated with higher mortality [27,28]; however,
the utility of TIPS as an intervention to reversemuscle wasting
should be evaluated in futureprospective studies.
Myostatin is a member of the transforminggrowth factor (b)
superfamily that is an extremelypotent negative regulator of muscle
mass. Prelimi-nary investigations showed that myostatin plas-matic
levels in cirrhotic patients compared withhealthy controls [29],
and animal model studieshave shown that myostatin expression can
bereversed with administration of follistatin (func-tional
antagonist of myostatin) without impairmentof liver function [30];
however, new treatments toreverse muscle wasting in cirrhotic
patients, includ-
ing myostatin antagonists are waiting to be eval-uated in
randomized controlled trials.
MUSCLE WASTING AND LIVER
TRANSPLANTATION
The group from the University of Michigan hasreported that
muscle wasting was associated witha higher risk for post-transplant
infectious compli-cations and mortality[5,6]. A recent study
showedthat muscle wasting measured by bioelectrical impe-dance was
associated with higher post-transplant
mortality in patients undergoing living donor
livertransplantation [4].
Our group recently reported that muscle wastingwas predictive of
longer length of hospitalizationand higher risk of perioperative
bacterial infectionafter liver transplantation, but was not
associatedwith increased mortality [31]. Further prospectivestudies
will be necessary to clarify the impact ofmuscle wasting after
liver transplantation.
Interestingly, in a subanalysis of nonprotocolCT after liver
transplant, we found that in patientswith muscle wasting before the
transplant,
(a) (b)
FIGURE 2. Computed tomography images used for the L3 skeletal
muscle index (L3 SMI) assessment of two patientswith cirrhosis with
identical BMI of 32 kg/m2. (a) Patient at the left is sarcopenic
with L3 skeletal muscle index (L3 SMI) of50cm2/m2. (b) Patient at
the right is not sarcopenic with a L3 SMI of 71cm2/m2. Dark gray
color indicates skeletal muscles.Reproduced with permission
from[2].
Muscle wasting: a criterion for liver transplantMontano-Loza
1363-1950 2014 Wolters Kluwer Health | Lippincott Williams &
Wilkins www.co-clinicalnutrition.com 223
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
6/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
sarcopenia resolved in at least 28% in a median timeof 43 months
following transplantation, defined asan increase in the L3 SMI more
than 38.5cm2/m2 forwomen and more than 52.4 cm2/m2 for men
afterliver transplant.
Failure of reversal of muscle wasting after livertransplantation
is not well elucidated. A recent
review summarizes the changes in indirect measuresof skeletal
muscle mass after transplantation andsome studies reported an
initial rapid postoperativeloss of muscle mass followed by
incomplete recovery.Potentialreasons for failure to reverse muscle
wastinginclude the use of immunosuppression that impairsskeletal
muscle growth, repeated hospitalizations,and post-transplant
infections, among others[32].
A recent study from our group showed thatmodification of MELD
score to include muscle wast-ing is associated with a modest
improvement in theprediction of 3-month and 6-month mortality
inpatients with cirrhosis. The c-statistics for 3-monthand 6-month
mortality were 0.72 (95% confidenceinterval, CI 0.630.82, P
-
8/9/2019 Muscle Wasting: A Nutritional Criterion to Prioritize
Patients for Liver Transplantation
7/7Copyright Lippincott Williams Wilkins. Unauthorized
reproduction of this article is prohibited.
17. Montano-Loza AJ, Meza-Junco J, Prado CMM, et al.Sarcopenic
obesity andmuscle fat infiltration are associated with higher
mortality in patients withcirrhosis. Hepatology 2013; 58
(S1):865A.
18.
&
Glass C, Hipskind P, Tsien C, et al. Sarcopenia and a
physiologically lowrespiratory quotient in patients with cirrhosis:
a prospective controlled study.J Appl Physiol 2013; 114:559565.
This is study that demonstrated that low respiratory quotient
occurs in cirrhosis,and there is a direct and significant relation
between respiratory quotient andmuscle area.19. Heymsfield SB.
Development of imaging methods to assess adiposity and
metabolism. Int J Obes (Lond) 2008; 32 (Suppl 7):S76S82.20.
Mourtzakis M, Prado CM, Lieffers JR,et al.
A practical and precise approachto quantification of body
composition in cancer patients using computedtomography images
acquired during routine care. Appl Physiol Nutr Metab2008;
33:9971006.
21. Prado CM, Lieffers JR,McCargarLJ, et al. Prevalenceand
clinical implicationsof sarcopenic obesity in patients with solid
tumours of the respiratory andgastrointestinal tracts: a
population-based study. Lancet Oncol 2008;9:629635.
22. Montano-Loza AJ, Meza-Junco J, Prado CMM, et al. New cutoff
values forsarcopenia for predicting 6-months mortality in cirrhotic
patients. J Hepatol2013; 58 (S1):95A.
23. Vaisman N, Katzman H, Carmiel-Haggai M, et al. Breakfast
improves cognitivefunction in cirrhotic patients with cognitive
impairment. Am J Clin Nutr 2010;92:137140.
24. Kachaamy T, Bajaj JS. Diet and cognition in chronic liver
disease. Curr OpinGastroenterol 2011; 27:174179.
25. Drummond MJ, RasmussenBB. Leucine-enriched nutrientsand the
regulationof mammalian target of rapamycin signalling and human
skeletal muscleprotein synthesis. Curr Opin Clin Nutr Metab Care
2008; 11:222226.
26. Dreyer HC, Drummond MJ, Pennings B, et al. Leucine-enriched
essentialamino acid and carbohydrate ingestion following resistance
exerciseenhances mTOR signaling and protein synthesis in human
muscle. Am JPhysiol Endocrinol Metab 2008; 294:E392E400.
27. Tsien C, Shah SN, McCullough AJ, Dasarathy S. Reversal of
sarcopeniapredicts survival after a transjugular intrahepatic
portosystemic stent. Eur JGastroenterol Hepatol 2013; 25:8593.
28. Dasarathy J, Alkhouri N, Dasarathy S. Changes in body
composition after
transjugular intrahepatic portosystemic stent in cirrhosis: a
critical review ofliterature. Liver Int 2013; 31:12501258.29.
Garcia PS, Cabbabe A, Kambadur R,et al.Brief-reports: elevated
myostatin
levelsin patients with liver disease a potentialcontributor to
skeletal musclewasting. Anesth Analg 2010; 111:707709.
30. Dasarathy S, McCullough AJ, Muc S, et al. Sarcopenia
associated withportosystemic shunting is reversed by follistatin. J
Hepatol 2011; 54:915921.
31. Montano-Loza AJ, Meza-Junco J, Baracos VE, et al. Muscle
wasting is notassociated with higher mortality after liver
transplantation. Hepatology 2012;56 (S1):651A.
32. Dasarathy S. Posttransplant sarcopenia: an underrecognized
early conse-quence of liver transplantation. Dig Dis Sci 2013;
58:31033111.
33. Montano-Loza AJ, Meza-Junco J, Prado CMM, et al. Inclusion
of sarcopeniawithin MELD (MELD-Sarcopenia) and the prediction of
mortality in patientswith cirrhosis. Hepatology 2013; 58
(S1):1041A.
Muscle wasting: a criterion for liver transplantMontano-Loza
1363-1950 2014 Wolters Kluwer Health | Lippincott Williams &
Wilkins www.co-clinicalnutrition.com 225