Embed Size (px)
Citation preview
Journal ofNeurology, Neurosurgery, and Psychiatry, 1978, 41, 719-725
Muscle hypertrophy after partial denervation: ahuman case
JAMES L. BERNAT, AND JOSE L. OCHOA
From the Division of Neurology, Department of Medicine, Dartmouth Medical School, HanoveI,New Hampshire, USA
S U M M ARY While undergoing long-term physiotherapy, a 41 year old woman with a chronicSi radiculopathy developed progressive, painless enlargement of the weak calf. Gastrocnemiusmuscle biopsy disclosed changes of partial denervation and reinnervation, with small groups oftype I and type II atrophic muscle fibres and abundant hypertrophic fibres of both types butmostly type II. It is postulated that, in addition to compensatory work-induced type II musclefibre hypertrophy, there was an element of (type I) stretched-induced hypertrophy of denervatedfibres, a condition well recognised experimentally but not documented in man.
Morpurgo (1897) first showed that muscle fibreswill hypertrophy when subjected to increased workload. Sola and Martin (1953) showed that musclefibre hypertrophy will occur with stretch, even inthe absence of innervation. While muscle hyper-trophy after nerve injury has been the subject ofmuch experimental work, only rarely have humancases been documented. We present a patient whodeveloped true muscle fibre hypertrophy in thesetting of partial denervation and exercise, andpropose that in this case the denervation predis-posed to muscle hypertrophy from a combinationof work and stretch.
Case report
A 41 year old woman was admitted to the MaryHitchcock Memorial Hospital because of pro-gressive right calf enlargement. Two years earliershe had developed low back pain which radiatedinto the right buttock and foot. Her physicianfound that she had hypalgesia over the lateralaspect of the right foot and absent right anklereflex. Lumbosacral roentgenography disclosednarrowing of the L5-SI disc space. She was treatedwith strict bed rest and the pain resolved, leavingonly residual foot numbness. The pain recurredthereafter only while coughing, sneezing, and
Address for reprint requests: Dr J. L. Bernat, Division of Neurology,Department of Medicine, Dartmouth Medical School, Hanover, NewHampshire 03755, USA.Accepted 18 February 1978
straining. The patient then started a vigorousexercise programme of walking and running whichshe continued regularly to the time of admission.Nine months before admission she noted that
her right calf was getting larger. This growth in-creased steadily and did not seem to be accom-panied by similar growth in the left leg. Shedenied pain or tenderness of the enlargingextremity but noted a worsening of the old rightbuttock and foot pain and persistence of rightfoot numbness. There was no family history ofneuromuscular disease, and the patient had nochildren.Examination on admission showed her to be a
moderately obese woman in excellent generalhealth. There was no back tenderness or lumbarmuscle spasm. Right straight leg raising to 600reproduced her buttock and foot pain. The rightleg had normal colour, temperature, and arterialpulses. The circumference of the right calf,150 mm distal to the patella, was 370 mm as com-pared to 335 mm on the left. There was no muscletenderness or other abnormality to palpation,and the gastrocnemius idiomuscular response wasnormal. Muscle strength was normal except fortrace weakness of the right extensor hallucislongus and moderate weakness of ankle plantarflexion demonstrable on repetitive toe standing.There was no myotonia. There was hypalgesia topinprick over the right leg and foot as illustratedin Fig. 1. Deep tendon reflexes were normal exceptfor an absent right ankle reflex. Plantar responseswere flexor.
719
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from
James L. Bernat, and Jose L. Ochoa
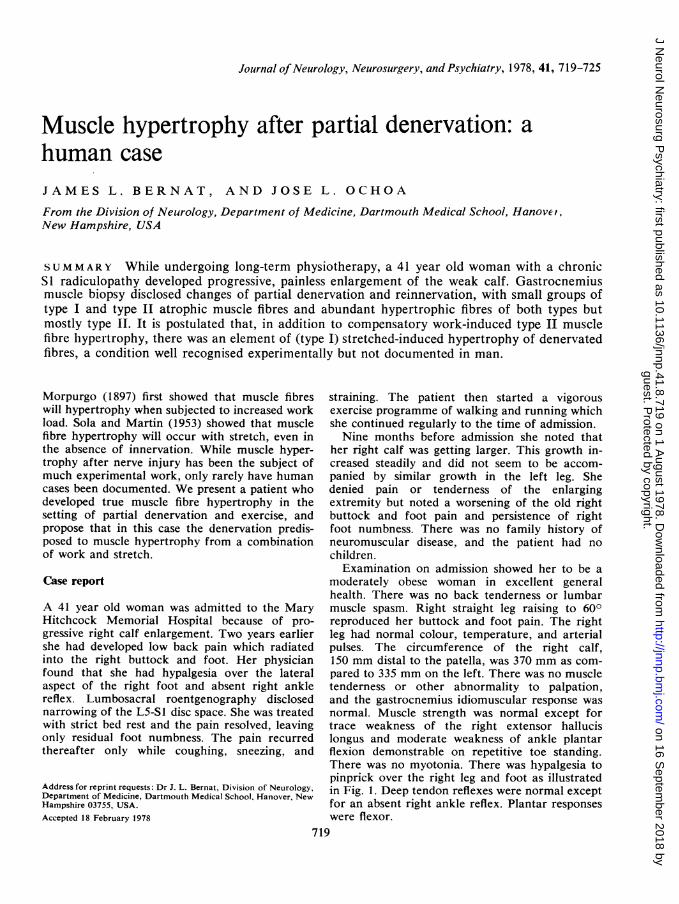
Fig. 1 Photographs of patient's legs revealing the enlarged right calf. The cross-hatched zone representsdiminished sensation to pinprick.
Complete blood count was normal. Creatinephosphokinase (CPK) measured on two separateoccasions was 126 IU/l and 85 IU/l (normal range5-70 IU/l). Plain radiographs of the right calffailed to disclose a cystic cavity. Computed tomo-graphy (CT) scan of the right calf (Fig. 2) showedhypertrophy of the muscles of the posterior com-partment. Electromyography (EMG) of the medialand lateral heads of the right gastrocnemiusshowed motor unit potentials up to 10 mV inamplitude with a reduced voluntary patterndespite a normal firing rate. No myotonic dis-charges were present and there was no spon-taneous electrical activity. Electromyograms ofthe right tibialis anterior and the right vastusmedialis were normal.
Biopsy of the right gastrocnemius lateral head(Fig. 3) showed abnormal variation of musclefibre size with atrophy and hypertrophy. Therewas atrophy, hypertrophy, and a tendency to typegrouping of both type I and II fibres. There weremany target fibres, a moderate number of centralnuclei, and rare examples of fibre splitting andrimmed vacuoles. There was no infiltration withinflammatory cells, collagen, or fat. Hypertrophicfibres were abundant and occupied most of thevolume of the muscle. These fibres reached 140,um in diameter and were of both types, but pre-dominantly type II. Atrophic fibres were also ofboth types, but predominantly type I. Upon sub-typing muscle fibres of type II, it became apparentthat subtypes IIA and IIB were equally hyper-
720
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from
Muscle hypertrophy after partial denervation: a human case
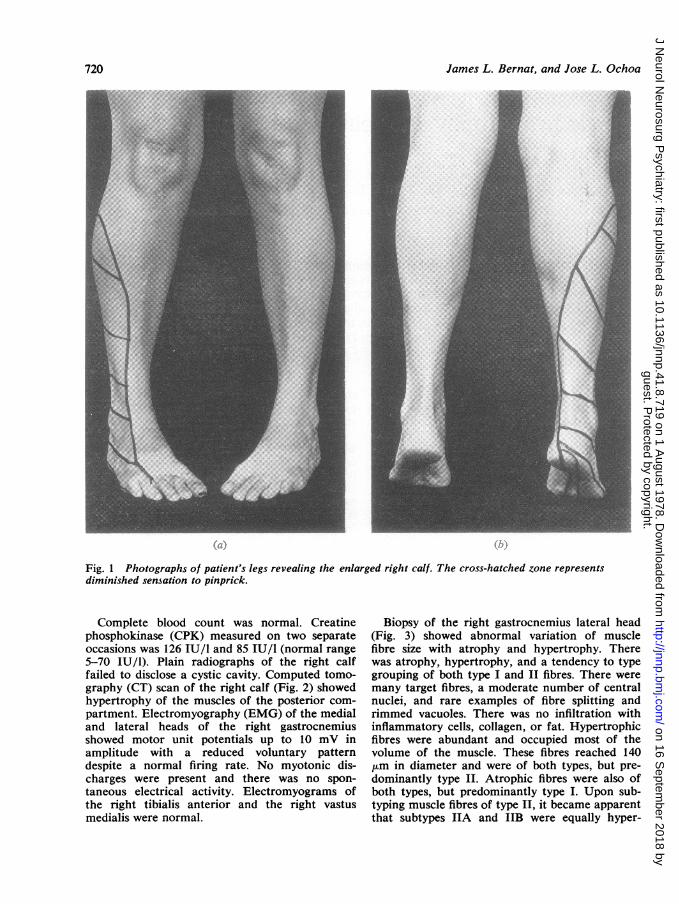
Fig. 2 Computed tomography scan takentransversely across the proximal third ofthe patient's legs. Enlargement on theright is due to the increased bulk of calfmuscles.
trophic, whereas few IIA were atrophic. Due tothe difficulty in the recognition of subtle colourchanges in very small fibres, it was not possible todiscern whether the type II atrophic fibres were oftypes IIB, IIC, or both. The size-frequency histo-gram for the fibre types is shown in Fig. 4.Lumbosacral myelography disclosed a right
sided extradural defect at the L5-S1 disc spacewith severe compression of the right first sacralnerve root.At surgery, a calcified free fragment of the
L5-S1 disc was identified adherent to and com-pressing the SI nerve root. The scar tissue wasdivided with difficulty and the disc fragment wasexcised.
Postoperatively the patient was entirely free ofpain and, when last examined four months aftersurgery, her ankle plantar flexion strength hadimproved objectively, and repeat measurements ofcalf girth were unchanged on the control side butwere 10 mm less on the involved side. Electromyo-graphy was unchanged.
Discussion
A 41 year old woman developed painless enlarge-ment of the right calf. Computed tomography scanshowed this enlargement to be the result of musclehypertrophy of the posterior compartment. Para-doxically, the enlarged muscles were weak andneurological and electromyographic examinationswere diagnostic of a SI radiculopathy. Surgeryconfirmed the myelographic findings of rightposterolateral herniation of the L5-S1 inter-vertebral disc. Right gastrocnemius muscle biopsyrevealed only evidence of partial denervation
and reinnervation in addition to striking andrather type-selective muscle fibre atrophy andhypertrophy.Enlargement of a muscle may result from an
increase in the number or the size of muscle fibres(true hypertrophy) or from infiltration of themuscle by collagen, fat, parasites, tumour or in-flammatory cells (pseudohypertrophy). True musclehypertrophy occurs physiologically in work-induced hypertrophy, and pathologically in avariety of disorders including myotonia congenita,dystonias, acromegaly, and hypertrophia muscu-lorum vera (Adams, 1975). Focal myositis andprimary muscle neoplasm were initial diagnosticconsiderations in this case as the hypertrophy waspainless and unilateral. The CT scan of the calfdisclosed that the muscles of the right postero-lateral compartment had normal density and con-figuration but were diffusely enlarged. Thisappearance was more consistent with true hyper-trophy than with pseudohypertrophy or neoplasm,as muscle infiltration in the latter conditionsusually produces an alteration in CT density (Wein-berger and Levinsohn, 1978). Muscle neoplasmwas felt to be an unlikely explanation as the hyper-trophy was generalised and uniform in the affectedmuscles. The electromyographic findings indicatedchronic partial denervation of both heads of theright gastrocnemius without similar involvementof neighbouring muscles innervated by nerve rootsother than S1.The muscle biopsy showed atrophy and grouping
of both type I and IL fibres, characteristic ofchronic partial denervation and reinnervation.Some central nuclei were seen and there wereoccasional areas of fibre splitting. While these
D
721
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from

James L. Bernat, and Jose L. Ochoa
*... ...... ... ...
C
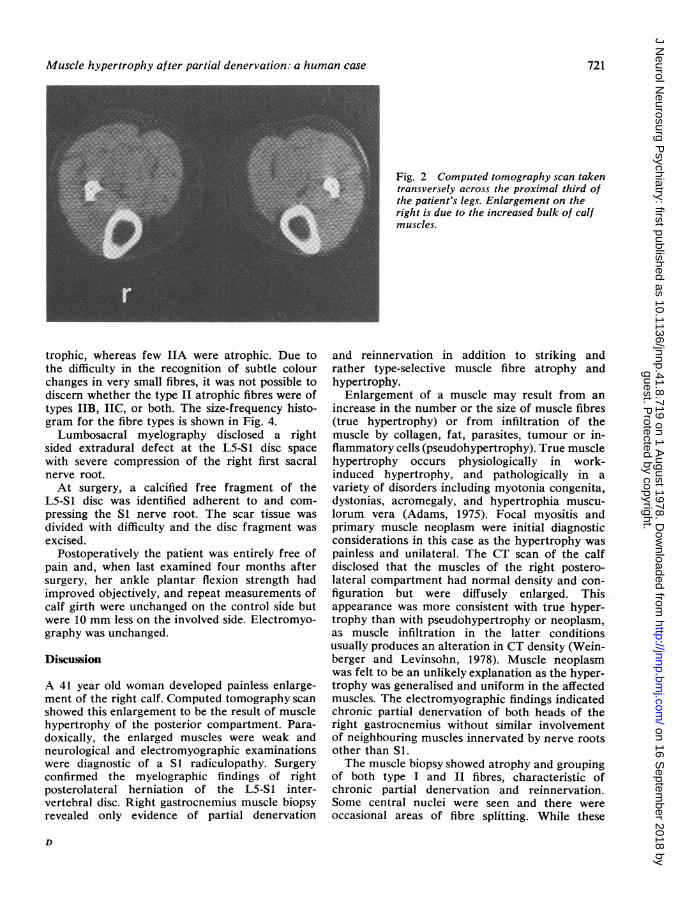
Fig. 3 Photomicrographs of biopsied rightgastrocnemius muscle-a: routine A TPase at pH 9.4;b: identical section with ATPase preincubated at
pH 4.6; c: identical section with A TPase preincubatedat pH 4.3. These sections show four features:hypertrophy predominantly involving type II fibres;atrophy predominantly involving type I fibres; type IIfibre atrophy relatively sparing type IIA fibres;Predominance of type II among the non-atrophicfibres. d: NADH-TR reaction shows several targets
e
within grouped type I fibres; e: A TPase at pH 4.6shows pseudomyopathic changes including centralnuclei, fibre splitting, and fibre size variation withoutangular appearance. All bars represent 100 pm.
... .. ...". ;.'.s...-.
.....
dL-.,T
mom. 4%
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from

Muscle hypertrophy after partial denervation: a human case
latter findings generally suggest a myopathic dis-order, they may be seen in partially denervatedmuscles (Drachman et al., 1967) and also inmuscles subjected to increased work load (Hall-
240
210
180
150
120
90
60
30
240
- 210
E 12090
UN 910
t 60n
J30
z
240
210
180
150
120
90
60
30
120 140
Craggs, 1972). The most remarkable finding in themuscle biopsy sample was the enormous increasein size of many muscle fibres, especially those oftype II. Giant muscle fibres are known to resultfrom an increased work load on the muscles(Denny-Brown, 1960; Goldspink and Howells,1974). In work-induced hypertrophy, muscle fibresmay exceed 100 ,um in diameter (Adams, 1968)and are usually type II (Dubowitz and Brooke,1973). Thus, in the present case, the histologicalprofile of the muscle and the history of strenuousleg exercise are consistent with the pathogenesisof work hypertrophy.The acceptance of work hypertrophy as the sole
pathogenesis of muscle enlargement leaves un-answered the issues of why the enlarged musclewas weak and why only the affected muscle en-larged, given equal exercise to the two legs. Theparadox of muscle weakness despite increasedmuscle volume can be explained on the basis thata large number of fibres were atrophic, that a pro-portion of the hypertrophic fibres were denervated,and that the innervated hypertrophic fibres couldnot compensate for the denervated hypertrophicand atrophic fibres.That only the partially denervated leg enlarged,
despite equal exercise in the legs, suggests thatchronic partial denervation somehow facilitateswork hypertrophy. A possible explanation for thisfacilitation is that the work performed by thepartially denervated muscle produced greaterhypertrophy in the remaining innervated musclefibres because there were fewer of them to per-form the work than in the unaffected leg. Alter-natively, there may have been a trophic influencefrom the partially denervated neuromuscular ap-paratus producing excess growth of the innervatedmuscle fibres.While the model of work hypertrophy accounts
for the type II fibre enlargement, the animal modelof denervation hypertrophy may account for thetype I fibre enlargement. Denervation-inducedhypertrophy was first described as a transientevent in the experimentally denervated rat dia-phragm (Sola and Martin, 1953), and has sincebeen described as a more permanent effect in ex-
Fig. 4 Musle fibre diameter spectra based uponA TPase reactions. Top: type I fibres; middle: type IIAfibres; bottom: type IIB and IIC fibres. The bar undereach histogram represents the range of normal musclefibre diameters for the adult female (based uponDubowitz and Brooke, 1973, Fig. 4.2, page 76). Notethat most of the hypertrophic fibres are type II, moreof the atrophic fibres are type I, very few type IIAfibres are atrophic, and that the atrophic type 11 fibresare smaller than the atrophic type I fibres.
20 40 60 80 100
Diameters (,um)
723
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from
724
perimentally denervated muscle preparations of avariety of other species (Stewart et al., 1972; Solaet al., 1973; Asmussen and Kiessling, 1975, 1976;Sarnat et al., 1977). Sola et al. (1973) demonstratedthat a denervated muscle subjected to constantstretch undergoes hypertrophy. They also foundthat a normally innervated muscle subjected to thesame stretch undergoes even greater hypertrophy.They concluded that a muscle hypertrophies inproportion to the degree of stretch imposed on it,and that denervation does not necessarily pre-dispose to hypertrophy if the stretch remains con-stant. Experimental models of denervation hyper-trophy in the chicken, frog, and pigeon have shownthat the hypertrophic fibres are usually type I(Cherian et al., 1966; Jirmanova and Zelena, 1970;Sarnat et al., 1977).We propose that the type I fibre hypertrophy
seen here was produced by increased stretching ofthe weak partially denervated muscle by itsstronger antagonists during exercise. It is possiblethat a proportion of hypertrophic 2 fibres weresimilarly produced.
This case is consistent in some respects withcases that in the past have been termed hyper-trophia musculorum vera. However, the entityhypertrophia musculorum vera does not have a
unique pathology and appears to be a generaldesignation for cases of acquired muscle enlarge-ment caused by muscle fibre hypertrophy of di-verse aetiologies. In this sense, the current casecould be considered hypertrophia musculorumvera resulting from denervation and exercise.There are only a few previous reports of patients
with muscle hypertrophy after nerve injury.Graves (1848) reported a man with sciatica andsubsequent leg enlargement. L'Hermitte (1918)reported a man with a bullet injury to the sciaticnerve and subsequent calf enlargement. McComas(1977) reported a woman with calf enlargementafter analgesic injections into the sciatic nerve.The only previously reported case with musclebiopsy was that of Lapresle et al. (1973). Theyreported a man with a L4-5 herniated interverte-bral disc with subsequent calf myotonia and hyper-trophy. Gastrocnemius muscle biopsy, as in ourcase, revealed muscle fibre hypertrophy withoutincrease in collagen. In contrast to our case, therewas selective type I hypertrophy and type IIatrophy, which closely approximate the experi-mental model of stretch-induced denervationhypertrophy but which the authors explained asdenervation atrophy and compensatory hyper-trophy. Although type specific atrophy is notgenerally regarded as a feature of denervation, thepresence of target fibres and a known nerve injury
James L. Bernat, and Jose L. Ochoa
does support a primarily denervating process.The unifying principle in the two reported cases
of biopsy proved true muscle hypertrophy afternerve injury is that the muscles were repeatedlystretched. In the current case, repeated musclestretching and work were induced by strenuousexercise of the partially denervated limb. Althougha history of exercise was not present in the case ofLapresle et al., myotonia may have accounted forrepeated stretching of the partially denervatedmuscles. It seems reasonable to conclude thatmuscle hypertrophy is either work hypertrophyinduced by repeated muscle contraction or stretchhypertrophy induced passively. Partial denervationmay predispose to hypertrophy when some inner-vated fibres are overworked or when some inner-vated or denervated fibres are stretched.
We are grateful to Miss Elizabeth Boogusch forinvaluable help with the muscle fibre counts.
References
Adams, R. D. (1968). The giant muscle fiber: its placein myopathology. In Modern Neurology: Papers inTribute to D. Denny-Brown, pp. 225-240. Edited byS. Locke. Little, Brown, and Company: Boston.
Adams, R. D. (1975). Diseases of Muscle. A Study inPathology, Third Edition. Harper and Row: Hagers-town, Maryland.
Asmussen, G., and Kiessling, A. (1975). Hypertrophyand atrophy of mammalian extraocular musclefibres following denervation. Experientia, 31, 1186-1188.
Asmussen, G., and Kiessling, A. (1976). Kaliberver-anderungen der muskelfasertypen des musculusobliquus inferior oculi des kaninchens nach dener-vierung. Acta Anatomica, 96, 386-403.
Cherian, K. M., Bokdawala, F. D., Vallyathan, N. V.,and George, J. C. (1966). Effects of denervation onthe red and white fibres of the pectoralis muscle ofthe pigeon. Journal of Neurology, Neurosurgery, andPsychiatry, 29, 299-309.
Denny-Brown, D. (1960). Experimental studies per-taining to hypertrophy, regeneration and degenera-tion. Research Publications: A ssociation for Re-search in Nervous and Mental Disease, 38, 147-196.Williams and Wilkins: Baltimore.
Drachman, D. B., Murphy, S. R., Nigam, M. P., andHills, J. R. (1967). "Myopathic" changes in chroni-cally denervated muscle. Archives of Neurology(Chicago), 16, 14-24.
Dubowitz, V., and Brooke, M. H. (1973). MuscleBiopsy: A Modern Approach. W. B. Saunders andCompany: London.
Goldspink, G., and Howells, K. F. (1974). Work in-duced hypertrophy in exercised normal muscles ofdifferent ages and the reversibility of hypertrophyafter cessation of exercise. Journal of Physiology,239, 179-193.
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from
Muscle hypertrophy after partial denervation: a human case
Graves, R. J. (1848). Clinical Lectures on the Practiceof Medicine. Second Edition Vol. 1, p. 498. Fanninand Company: Dublin.
Hall-Craggs, E. C. B. (1972). The significance of longi-tudinal fibre division in skeletal muscle. Journal ofthe Neurological Sciences, 15, 27-33.
Jirmanova, I., and Zelena, J. (1970). Effect of dener-vation and tenotomy on slow and fast muscles of thechicken. Zeitschrift fiir Zellforschung und Mikro-skopische Anatomie, 106, 333-347.
Lapresle, J., Fardeau, M., and Said, G. (1973).L'hypertrophie musculaire vraie secondaire a uneatteinte nerveuse peripherique: etude clinique ethistologique d'une observation d'hypertrophie dumollet consecutive a une sciatique. Revue Neuro-logique, 128, 153-160.
L'Hermitte, J. (1918). Hypertrophie des muscles de lajambe consecutive a une lesion du nerf sciatique parballe. Revue Neurologique, 25, 56-58.
McComas, A. J. (1977). Neuromuscular Function andDisorders. Butterworths: London.
Morpurgo, B. (1897). Ueber Activitats-Hypertrophieder Willkurlichen Muskeln. Virchows Archiv fiur
Pathologische Anatomie und Physiologie, 150, 522-554.
Sarnat, H. B., Portnoy, J. M., and Chi, D. Y. K.(1977). Effects of denervation and tenotomy on thegastrocnemius muscle in the frog: a histologic andhistochemical study. Anatomical Record, 187, 335-346.
Sola, 0. M., and Martin, A. W. (1953). Denervationhypertrophy and atrophy of the hemidiaphragm ofthe rat. American Journal of Physiology, 172, 324-332.
Sola, 0. M., Christensen, D. L., and Martin, A. W.(1973). Hypertrophy and hyperplasia of adultchicken anterior latissimus dorsi muscles followingstretch with and without denervation. ExperimentalNeurology, 41, 76-100.
Stewart, D. M., Sola, 0. M., and Martin, A. W.(1972). Hypertrophy as a response to denervation inskeletal muscle. Zeitschrift fur VergleichendePhysiologie, 76, 146-167.
Weinberger, G., and Levinsohn, E. M. (1978). Com-puted tomography in the evaluation of sarcomatoustumours of the thigh. American Journal of Roent-genology, 130, 115-118.
725
guest. Protected by copyright.
on 16 Septem
ber 2018 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.8.719 on 1 A
ugust 1978. Dow
nloaded from