Embed Size (px)
Citation preview
Multimodality Imaging in the Assessment of the Aorta
Parag R. Patel, MD
Staff Cardiologist
Centennial Medical Center; Nashville, TN
• None
Disclosures

• Aortic Root/Asc Aorta – AS/TAVR
– Type A Pathology • Dissection/IMH
• Aneurysm
• Arch/Isthmus – Arch branch vessels
• Descending Aorta – Type B Pathology
• Abdominal Aorta – Visceral branch vessels
– LE bifurcation
Normal Aortic Anatomy
J Am Coll Cardiol2010;55:1509–44.3

Aortic Dimensions

• Echocardiography – Transthoracic Echocardiography
– Transesophageal Echocardiography
– 3D TEE
• Multi-detector CT (MDCT)
• Magnetic Resonance Imaging (MRI/MRA)
• Aortography
• Others: – Chest X ray
– Intravascular Ultrasound
Imaging Modalities

• Intima: – Endothelial layer on a
basement membrane
• Media: – Internal elastic lamina,
layers of elastic fibers and smooth muscle cells and external elastic lamina
• Adventitia: – Collagen layer with vasa
vasorum and nerves.
Normal Aortic Anatomy
J Am Coll Cardiol2010;55:1509–44.3

Rationale: Substitute for Direct Visualization

Imaging Modalities 3-D
data
Intra-
operative
Functional
Assessment
Spatial
Resolution
Temporal
Resolution
Contrast Radiation
Exposure
Angiography - +
+ +++ +++ + +
Rotational
Angiography
+ +
- ++
+ + ++
2-D Echo-
cardiography
- +
+ ++ ++ - -
3-D Echoc-
ardiography
+ +
+ + + - -
CT ++ -
(+) ++
+ + ++
MRI -/+ (+)
+ + + + (Gd) -

• True and false (pseudoaneurysm)- based on pathologic features.
• True aneurysms: – all three layers of the aortic wall are involved in aneurysm formation
without disruption of any layers.
• False (or pseudo-) aneurysms: – intima is disrupted (and often, the media as well), and blood is
contained by the adventitia and peri-adventitial tissues.
• Trauma related pseudo-aneurysms are usually seen in the aortic isthmus.
• Penetrating aortic ulcer occurs in the descending aorta in most cases .
Pathology - Aneurysm

Pathology – Penetrating Ulcer
May progress to
• IMH
• Aortic dissection
• Pseudoaneurysm
• Saccular
anerusym
• Rupture

Pathology – Dissection
BRAVERMAN A. Cleveland Clinic Journal of Medicine 2011;78:685-696

• Easily available and permits rapid bedside assessment, however limited use in Acute aortic syndromes (AAS)
• Primary role is to rule out other etiologies- MI (wall motion abnormalities), PE (right ventricular dysfunction)
• Information about complications from AAS such as pericardial effusion/tamponade and aortic valve regurgitation
• Negative TTE exam does not exclude AAS!
Transthoracic Echocardiography (TTE)

• Highly specific and sensitive for detection of ascending and descending aortic dissection
• Oscillating dissection flap with true and false lumen • Assessment of true and false lumen flow • Complications of AAS: Aortic regurgitation, pericardial
effusion, coronary dissection, underlying etiology such as Bicuspid AV
• Limitations: - Need qualified personnel (tech +/- anesthesia) - Artifacts: Mirror image and reverberation - Limited assessment of distal asc aorta and arch
Transesophageal Echocardiography (TEE)

• Independently mobile and oscillating flap.
• True and false lumen - size, systolic expansion of the true and diastolic expansion of the false lumen.
• Rapid flow in the true vs sluggish flow (spontaneous echo contrast “smoke”) and thrombosis of the false lumen.
• 3D-TEE may help in assessment of entry tear and morphology of spiral dissection flap.
Echo Findings – Acute Aortic Syndrome


• 61 year-old female presented to an regional hospital with chest discomfort after lifting her grandchild.
• STE antero/lateral on ECG – cath lab activated via EMS.
• PMHx otherwise remarkable for HLD and hypothyroidism.
Case





• 50 year-old female from Russia who presents for evaluation of cardio-embolic source.
• She has pan-valvular disease (severe MS, mod-severe TR, moderate AI).
• Recent stroke and seeing neurology.
• TEE ordered after negative TTE/saline study.
Case


• Universal availability • Image the entire aorta including lumen, wall, and periaortic
regions • Identify anatomic variants and branch vessel involvement • Distinguish among types of acute aortic syndromes (i.e.,
intramural hematoma [IMH], penetrating atherosclerotic ulcer [PAU], and acute aortic dissection);
• Fast • 3-dimensional data set • Electrocardiogram-gated techniques generate motion-free
images of the aortic root and coronary arteries • Newer-generation multidetector helical CT scanners have
sensitivities of up to 100% and specificities of 98% to 99%
Computerized Tomography (CT)

• For intra-mural hematoma (IMH): – Non-contrast study should be included to detect subtle
changes of IMH. – Followed by a contrast study to delineate the presence
and extent of the dissection flap, identify regions of potential malperfusion, and demonstrate contrast leak indicating rupture.
• Imaging from the thoracic inlet to the pelvis, including the iliac and femoral arteries, provides sufficient information to plan surgical or endovascular treatment
Computerized Tomography (CT)
J Am Coll Cardiol2010;55:1509–44.3

• Need for iodinated contrast
– patients with AKI/CKD, contrast allergy
• Radiation
– Improvements in scanning strategies such as prospective ECG triggering, decreased tube voltage, dose modulation and iterative reconstruction have led to substantial reduction in radiation dose
• Motion related artifacts
Computed Tomography (CT) - Limitations
J Am Coll Cardiol2010;55:1509–44.3

Mark DB, Berman DS, Budoff MJ, et al. ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010exprt consensus document on coronary computed tomographic angiography: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;55:2663-99.
Cardiovascular Imaging and Radiation Exposure

a. Predictors for radiation dose are presented as % change in DLP (mGy x cm) b. Electrocardiographically controlled tube current modulation c. The Siemens single-source 64-slice CT system with the lowest median DLP in this study was used as a reference. The association with DLP is shown for the remaining four 64-slice systems within the linear regression analysis.
Predictors Effects
(%)
p
Patient weight, 10-kg increase 5 <0.001
Scan length, 1-cm increase 5 <0.001
Automated exposure control 0 0.97
ECTCMb -25 <0.001
Tube voltage 100 kV vs >120 kV or greater -46 <0.001
Sequential vs spiral scanning -78 <0.001
Site experience in CCTA, 12-mo increase -1 0.03
Hausleiter J et al. JAMA 2009; 301: 500-507
Predictors for Estimated Radiation Dose in a Multivariate Linear Regression Analysis

CT Acquisition
• Modern scanner
• cranio-caudal = Z - coverage
• Prospective triggering
• Dose modulation with Retrospective Gating
• Reduced tube voltage (kV): 100 vs. 120 kv
• Low tube current (mAs)
• Iterative reconstruction

Spiral Acquisition with Retrospective Gating
EC
G
Time
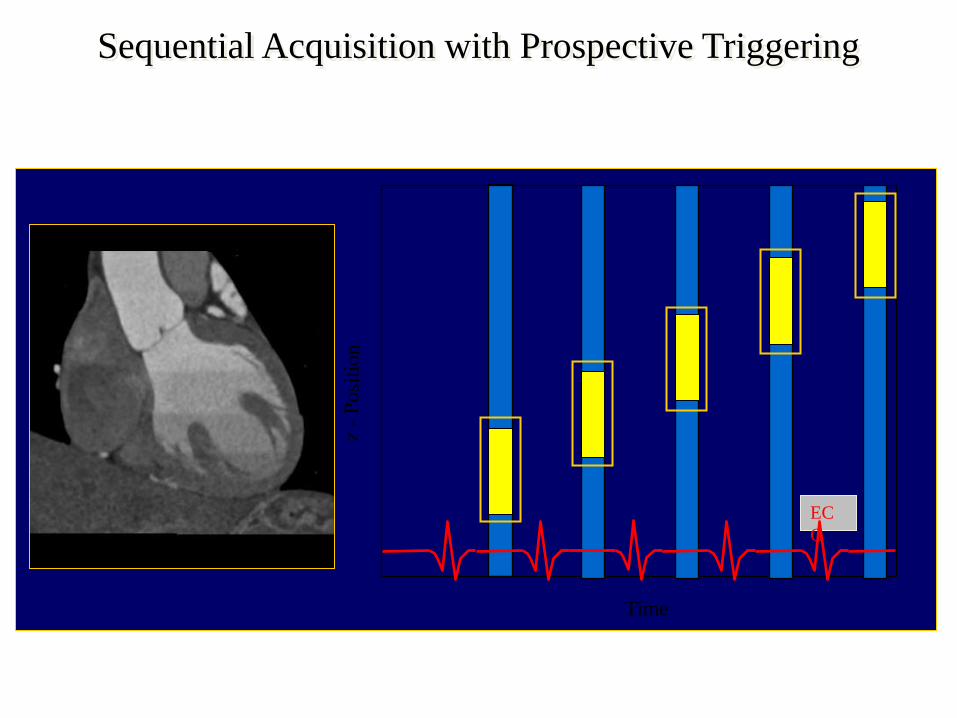
Sequential Acquisition with Prospective Triggering
EC
G
Time

Iterative Reconstruction

CT SCAN PROTOCOL
Mode = prospective triggered (or
retrospectively gated)
- both are synchronized to heart
beat) with slice thickness = 3
mm
Dual Source Scanner
temporal resolution = 75 ms
or 256-slice scanner = 135 ms
Mode = spiral, non-gated
slice thickness = 3 mm
80-150 ml iodinated contrast-material

Aortic Root Reconstruction in 3-dimensional dataset: Multi-planar reconstruction

Reconstruction in 3-dimensional dataset: Center-line Measurements
Schoenhagen P, Numburi U, Halliburton SS, et al. Three-dimensional imaging in the context of minimally invasive and transcatheter cardiovascular inteventions using multi-detectore computed tomography: from pre-operative planning to intra-operative guidance. Eur Heart J. 2010 Aug 25. [Epub ahead of print]

Schoenhagen P, Numburi U, Halliburton SS, et al. Eur Heart J. 2010
Reconstruction in 3-dimensional dataset: Volume Rendered Imaging

Copyright ©2008 American Heart Association
Burman, E. D. et al. Circ Cardiovasc Imaging 2008;1:104-113
Cine image, end diastolic frame, showing the levels of annulus, sinus, and sinotubular junction measurements (white arrow, black line, and black arrow, respectively)
Measurement Technique: Aortic Annulus, Aortic Root and Sinotubular Junction

Height of the Coronary Ostia

Type-A –ascending aorta = Immediate Surgical Consult

BRAVERMAN A C Cleveland Clinic Journal of Medicine 2011;78:685-696
Dissection with Flap
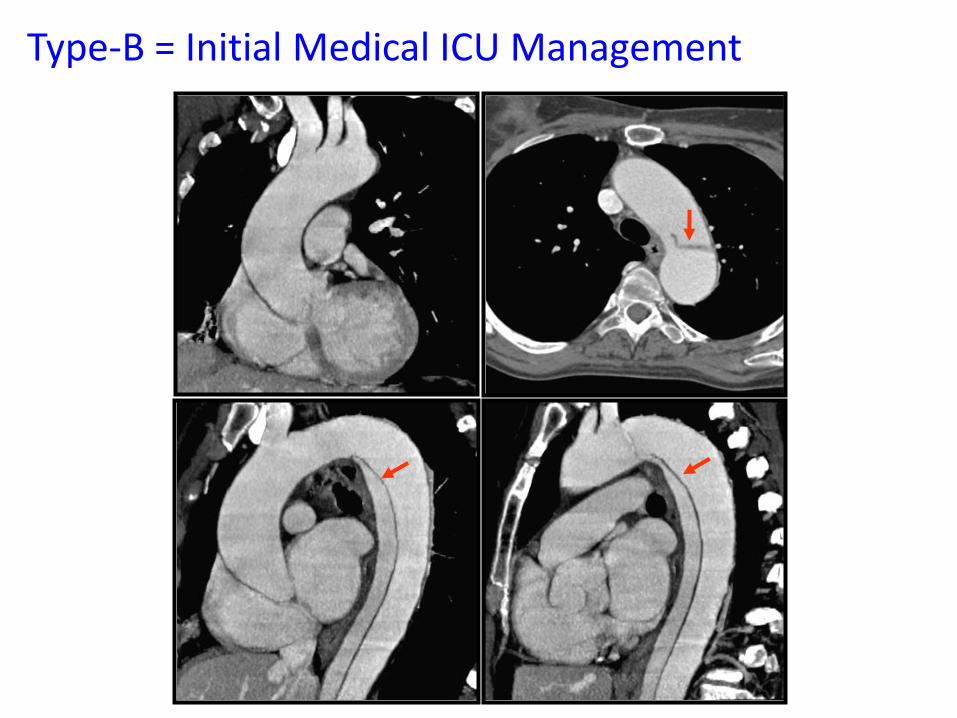
Type-B = Initial Medical ICU Management

Complicated Type-B = Surgical Consult

Intramural Hematoma (IMH) = Dissection

Moral et al. JACC 69: 1, 2017; 28-39
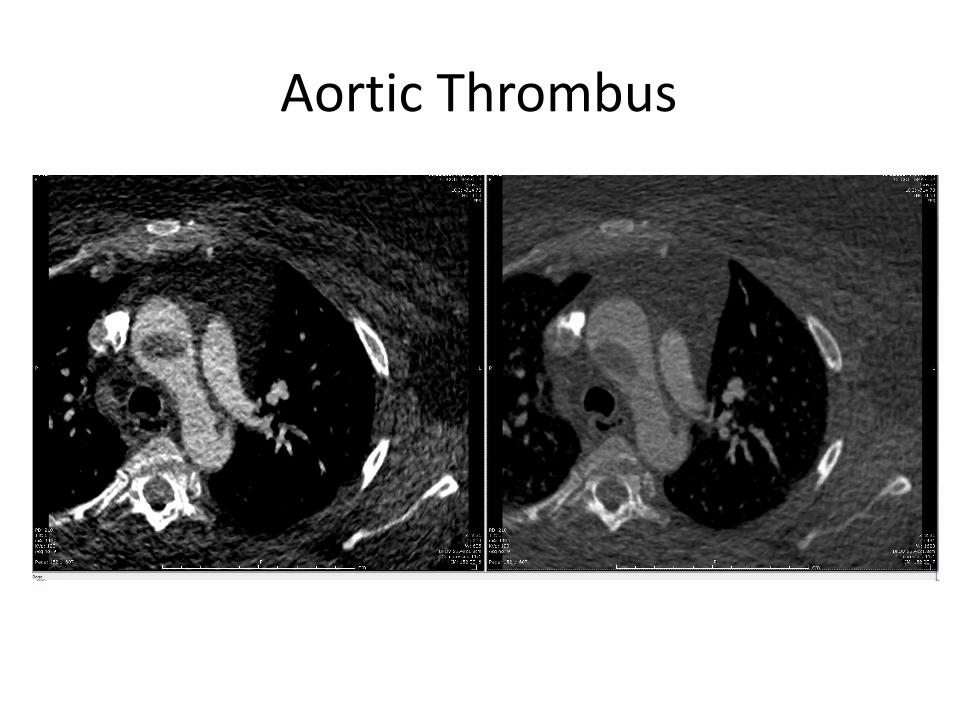
Aortic Thrombus
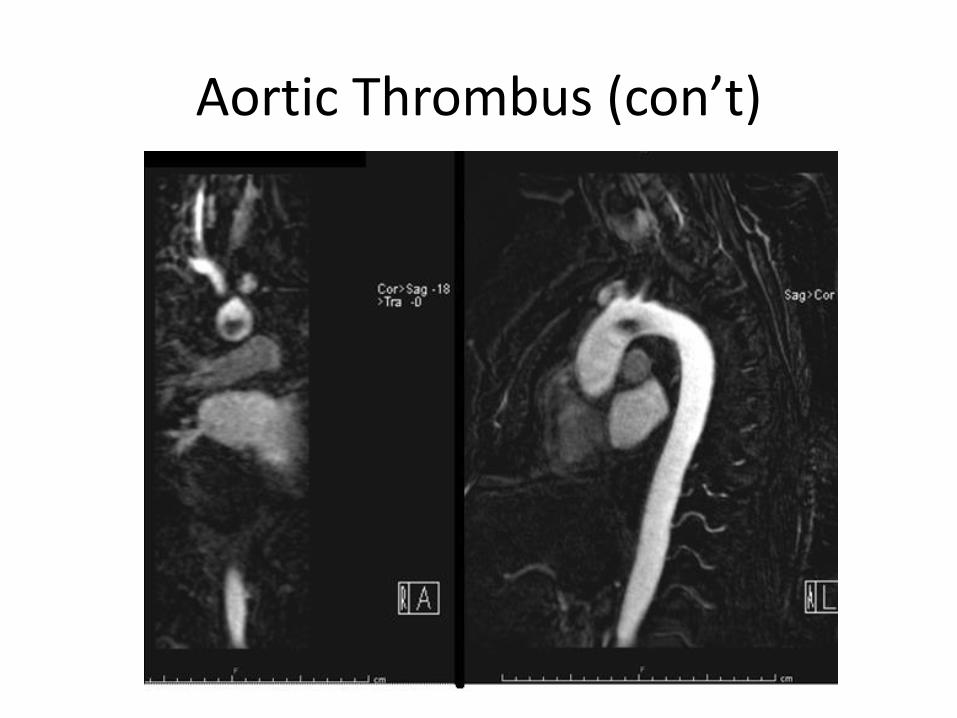
Aortic Thrombus (con’t)
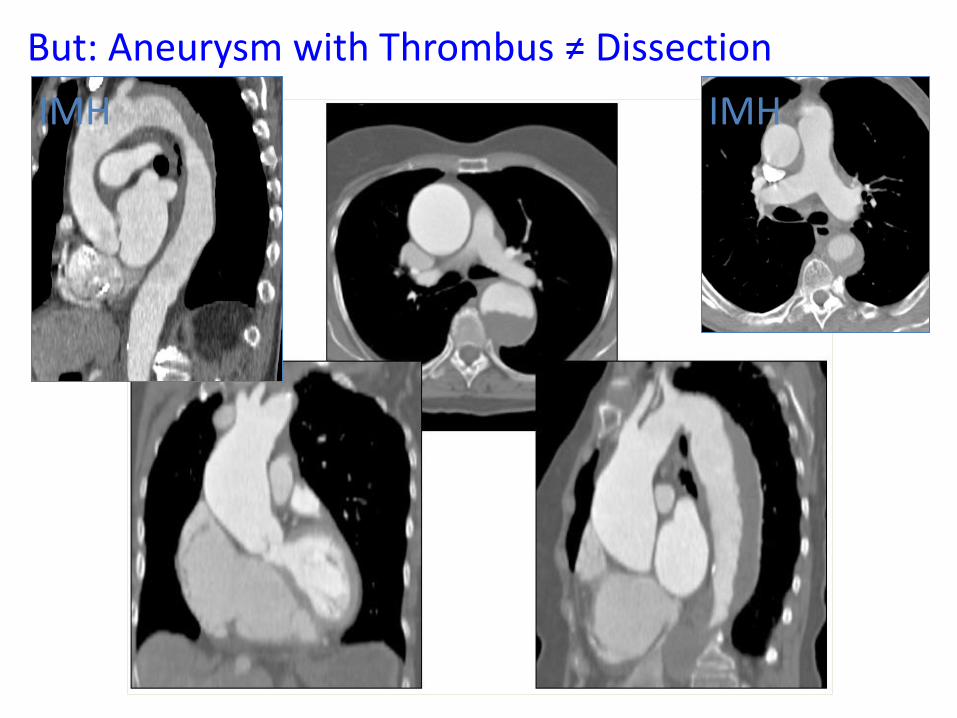
But: Aneurysm with Thrombus ≠ Dissection
IMH IMH

BRAVERMAN A C Cleveland Clinic Journal of Medicine 2011;78:685-696
Intramural Hematoma (IMH) = Dissection

IMH Progression
Moral et al. JACC 69: 1, 2017; 28-39

Chronic Penetrating Ulceration

BRAVERMAN A C Cleveland Clinic Journal of Medicine 2011;78:685-696
Penetrating Ulceration – Significance and Presentation

Ulceration with Leakage/Rupture = Dissection

Bicuspid Valve, Prominent Root, dilated Ascending Aorta

Skeletal Abnormalities: Pectus and Dural Ectasia/Tarlov Cyst

Type-B Pathology


White GH, et al. Journal of Endovascular Therapy 1998;5:305-9

Magnetic Resonance Imaging

• Advantages:
– Ability to identify anatomic variants of Aortic dissection (IMH and PAU)
– Assess branch artery involvement, and diagnose aortic valve pathology and left ventricular dysfunction
– No radiation or iodinated contrast.
– Accurate in the diagnosis of thoracic aortic disease, with sensitivities and specificities that are equivalent to or may exceed those of non-gated CT and TEE
Magnetic Resonance Imaging (MRI)
J Am Coll Cardiol2010;55:1509–44.3

• Disadvantages:
– (Longer) duration of image acquisition
– Inability to use gadolinium contrast in patients with renal insufficiency/ESRD.
– Contraindication in patients with claustrophobia, metallic implants or ICD/pacemakers
– Lack of widespread availability on an emergency basis
– Artifacts
Magnetic Resonance Imaging (MRI)
J Am Coll Cardiol2010;55:1509–44.3

• Black-blood sequences (spin echo sequences): – define morphology and wall characteristics
– T2-STIR (short tau inversion recovery) for edema-weighted imaging.
• Cine MR (gradient echo and SSFP sequences): – high temporal resolution cine images of flow in true and
false lumen as well as valvular stenosis/regurgitation.
• Flow mapping helps quantify aortic flow.
• MR angiography: 3D dataset to assess aortic dimensions and branch vessels
Magnetic Resonance Imaging (MRI)
J Am Coll Cardiol2010;55:1509–44.3

Ripley DP, et al. Heart 2016;102:1589–1603.

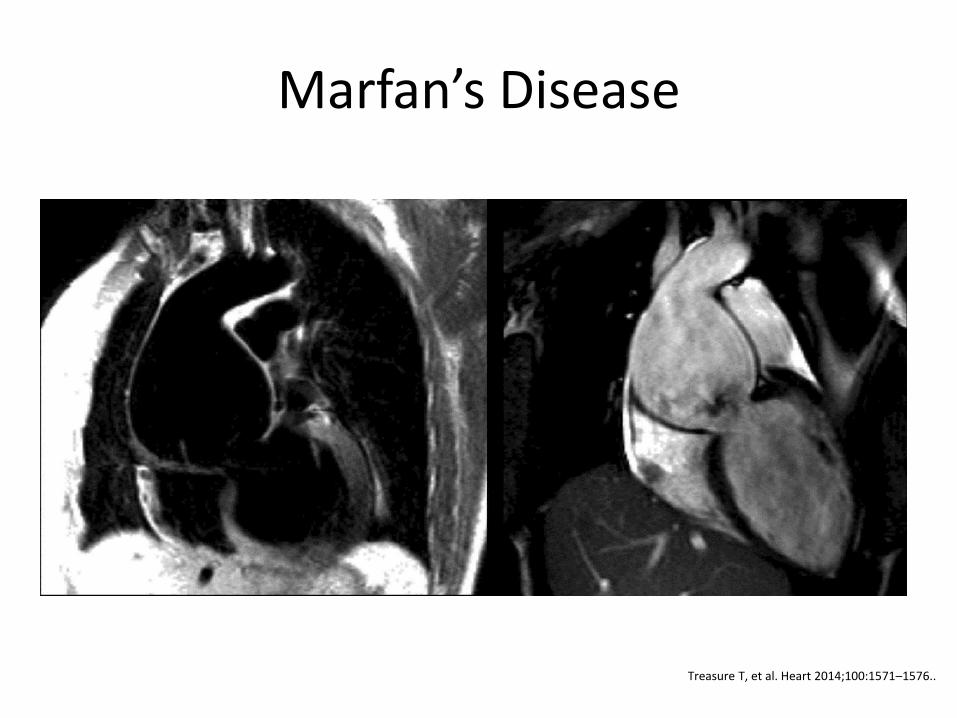
Marfan’s Disease
Treasure T, et al. Heart 2014;100:1571–1576..

CTA vs MRA
Treasure T, et al. Heart 2014;100:1571–1576..

Marfan’s Syndrome - PEARS
Treasure T, et al. Heart 2014;100:1571–1576..

Source: www.radiopaedia.org

• Largely replaced by other techniques (TEE, CT and MRI) due to invasive nature
• Currently used intra-operatively to guide endovascular or structural heart stent placement including side branch visualization and prosthetic endo-leak assessment.
Aortography
J Am Coll Cardiol2010;55:1509–44.3

Imaging and TAVR
• Central role for pre-, and intra-procedural imaging
• Focus on 3-D data • CT and MRI contribute to understanding and
evolution • Extensive data about pre-operative planning with
CT • Multi-modality imaging = selection of most
appropriate modality • Standardization of Imaging Approach

Imaging for TAVR
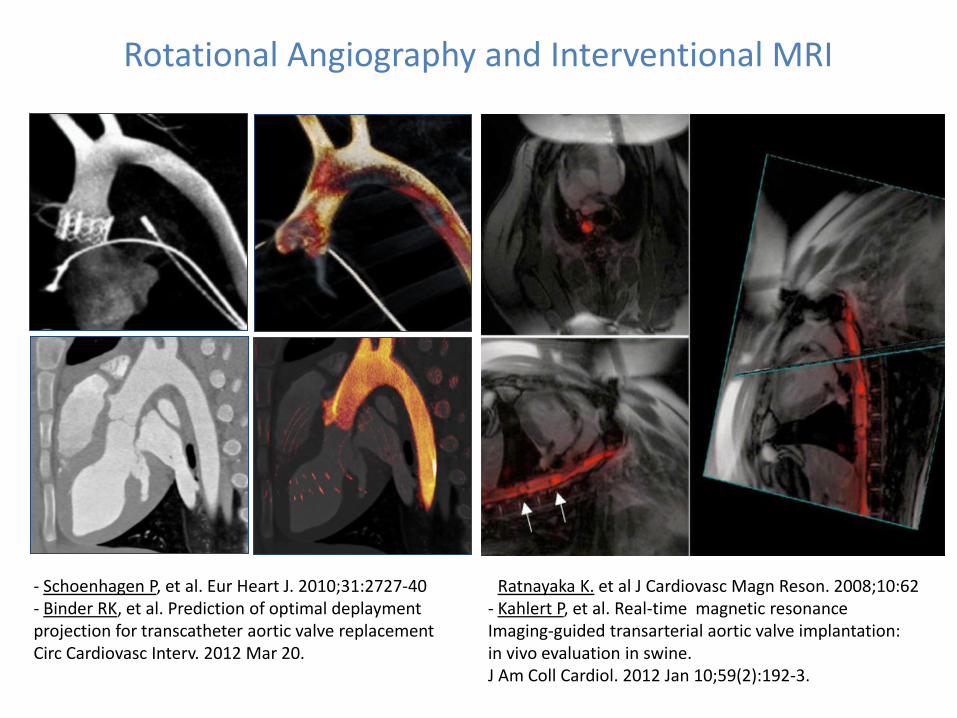
Rotational Angiography and Interventional MRI
- Ratnayaka K. et al J Cardiovasc Magn Reson. 2008;10:62 - Kahlert P, et al. Real-time magnetic resonance Imaging-guided transarterial aortic valve implantation: in vivo evaluation in swine. J Am Coll Cardiol. 2012 Jan 10;59(2):192-3.
- Schoenhagen P, et al. Eur Heart J. 2010;31:2727-40 - Binder RK, et al. Prediction of optimal deplayment projection for transcatheter aortic valve replacement Circ Cardiovasc Interv. 2012 Mar 20.


• Multi-modality imaging plays an important role in diagnosis of aortic syndromes.
• ECG-GATING !!!!! • Both CT and MRA are useful for post operative and long-term
follow up. – Radiation and iodinated contrast are drawbacks for CT. – Push for judicious use of CT/CTA (especially for routine followup of
non-surgical conditions, ie BAV, mild aortic ectasia, etc) – MRI/MRA now being utilized at our institution for routine followup
• TEE/CT and MRI are being used in the evaluation of TAVR patients.
• Long scan times and limited availability previously limited use of MRI. Newer scan protocols and selective use of contrast now decrease scan times to help increase utilization
Take Home Messages

Questions?