Embed Size (px)
Citation preview
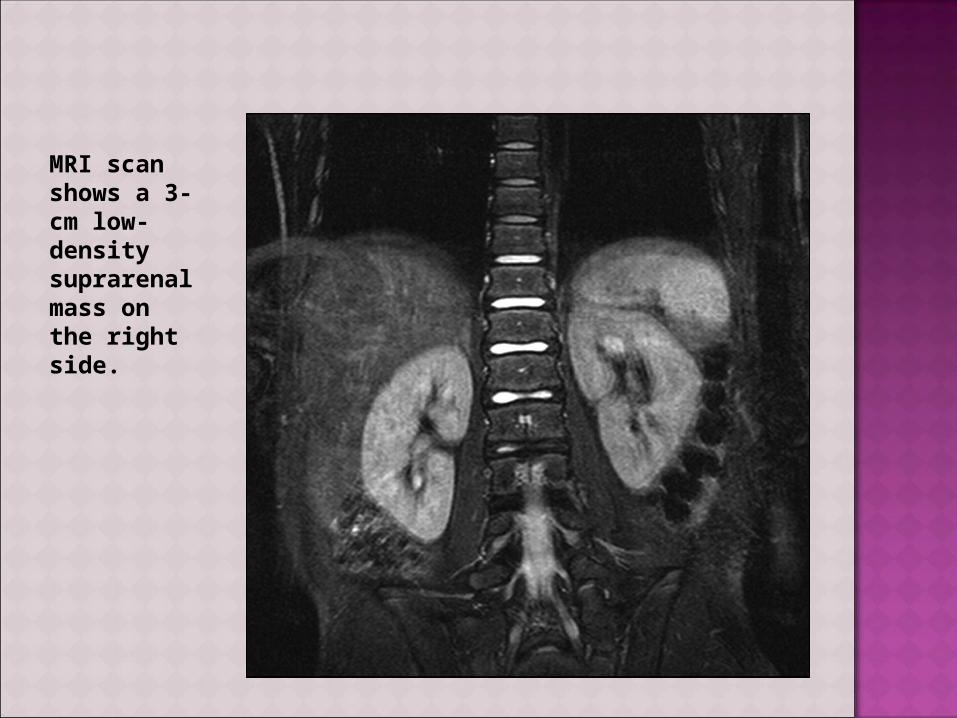
MRI scan shows a 3-cm low-density suprarenal mass on the right side.

Myra Lalas Pitt

Catecholamine-secreting tumors that arise from chromaffin cells located in the adrenal medulla and sympathetic chain.
Associated with neurofibromatosis type 1, familial paraganglioma, von Hippel-Lindau disease, tuberous sclerosis, Sturge-Weber syndrome, and multiple endocrine neoplasia (MEN 2A, 2B).

Inherited, AD syndrome manifested by a variety of benign and malignant tumors

MEN 2AHeritable predisposition to medullary thyroid cancer, pheochromocytoma, and primary parathyroid hyperplasia.
MEN 2BPredisposition to medullary thyroid cancer, pheochromocytoma, mucosal neuromas
Constipation, megacolon, developmental abnormalities, Marfanoid habitus, myelinated corneal nerves

Sweating Episodic headaches Tachycardia Hypertension Pallor Nausea/vomiting Weakness Abdominal pain Anxiety Chest pain
Classic triad

Glomerulonephritis Renal vein thrombosis Coarctation of the aorta Hyperthyroidism Cushing Syndrome Meds (TCA’s) Cocaine use Neuroblastoma Acute intermittent porphyria Idiopathic Intracranial Hypertension

Plasma free metanephrine (100% sensitive; 96.7% specific with negative predictive value 100%)
24-h urine for epinephrine, norepinephrine, dopamine, metanephrines, homovanillic acid, vanillylmandelic acid, creatinine (sensitivity of 87.5% and a specificity of 99.7%)
Adrenal CT MRI- preferred due to the high sensitivity
for adrenal tumors and better ability to localize extra-adrenal pheochromocytomas
Chem 10 123I-metaiodobenzylguanidine (MIBG) scan
to screen the body- used to locate and confirm pheochromocytoma and rule out metastatic disease
PET scan.

Large left adrenal mass and a lesion in the right hepatic lobe

Laparoscopic surgery is now the technique of first choice for resection adrenal and extra-adrenal pheochromocytomas.
All patients receive appropriate preoperative medical management to block the effects of released catecholamines.

After adequate alpha-adrenergic blockade has been ensured (PHENOXYBENZAMINE), beta-adrenergic blockade is started, which typically occurs 2-3 days preoperatively.
Beta-adrenergic blockade should never be started first.
Blockade of vasodilatory peripheral beta-adrenergic receptors with unopposed alpha-adrenergic receptor stimulation can lead to a further elevation in blood pressure.

A 14-yo female undergoing evaluation for persistent headaches and vomiting complains of double vision with lateral gaze. On PE, she is alert, but fundoscopic exam reveals blurring of the disk margin and absence of venous pulsations. A head MRI is normal. LP reveals an elevated opening pressure, with normal glucose, protein, and cells.

What is the most common long term complication of this girl’s condition?
a. Progressive hemiparesisb.Generalized seizuresc. Urinary incontinenced.Visual losse. Facial nerve palsy

Pseudotumor cerebri:Optic nerve atrophy and visual loss are
significant complications.

Chernausek SD, Stratakis CA. Chapter 537. Endocrine Neoplasia Syndromes. In: Rudolph CD, Rudolph A, Lister GE, First L, Gershon A, eds. Rudolph's Pediatrics. 22nd ed. New York: McGraw-Hill; 2011. http://www.accesspediatrics.com/content/7054216. Accessed February 2, 2012.
Lowry AW, Bhakta KY, Nag PK. Chapter 14. Endocrinology. In: Lowry AW, Bhakta KY, Nag PK, eds. Texas Children's Hospital Handbook of Pediatrics and Neonatology. New York: McGraw-Hill; 2011. http://www.accesspediatrics.com/content/7436745. Accessed February 2, 2012.
Pediatrics in Review Vol. 32 No. 6 June 1, 2011 pp. 257 -263 (doi: 10.1542/pir.32-6-257)
www.uptodate.com