Embed Size (px)
Citation preview

cervical junction El 11. It provides a direct, noninvasive demonstration of bony subluxation and distortion of the spinal cord and brainstem. Our experience sug- gests that MRI is helpful in screening for AA dislo- cation in patients with PA and other spondyloar- thropathies. In centers where MRI is unavailable, computed tomographic myelography can be utilized E12J
The operation for severe AA dislocation is usually posterior fusion, the approach used for our patient. Transoral odontoidectomy has recently been used and has the advantage of early mobilization 112).
We conclude that AA subluxation and basilar in- vagination may occur as a monoarthropathy early in the course of PA, predating the onset of systemic ar- thritis, and that MRI should be used when the condi- tion is suspected.
References 1. Killebrew K, Gold RH, Skolkoff SD. Psoriatic spondylitis.
Radiology 1973;708:9-16 2. Peterson CC Jr, Silbiger ML. Reiter's syndrome and psoriatic
arthritis: their roentgen spectra and some interesting similarities. Am J Roentgenol Radium Ther Nucl Med 1967;101:860-871
3. Arnett FC. Psoriatic arthritis: relationship to other spondyloar- thropathies. In: Gerber LH, Espinota LR, eds. Psoriatic ar- thritis. Orlando: Grune & Stratton, 198595-108
4. Resnick D. Hyperostosis and ossification of the cervical spine. Arthritis Rheum 1984;2 7: 5 64-5 69
5. McCormack GD, Barth W. Classification and diagnosis of psoriatic arthritis. Orlando: Grune & Stratton, 1985:59-82
6. Resnick D, Niwayama G. Physical injury. In: Resnick D, Niwayama G, eds. Diagnosis of bone and joint disorders. Phila- delphia: Saunders, 1981 :2292-2296
7. Yeadon C, Dumas JM, Karsh J. Lateral subluxation of the cervi- cal spine in psoriatic arthritis: a proposal mechanism. Arthritis Rheum 1984;27:564-569
8. Martel W. The occipito-atlanto-axial joints in rhematoid arthritis and ankylosing spondylitis. Am J Roentgenol Radium Ther Nucl Med 1961;86:223-240
9. Little H, Swinson DR, Cruickshank B. Upward subluxation of the axis in ankylosing spondylitis. Am J Med 1976;60:279-285
10. Fam AG, Cruickshank B. Subaxial cervical subluxation and cord compression in psoriatic spondylitis. Arthritis Rheum
11. Sze G, Brant-Zawadzki MN, Wilson CR, et al. Pseudotumor of the cranio-vertebral junction associated with chronic subluxa- tion. MR imaging studies. Radiology 1986;161:391-394
12. Stevens JM, Kendall EB, Crockard HA. The spinal cord in rheumatoid arthritis with clinical myelopathy: a computed my- elographic study. J Neurol Neurosurg Psychiatry 1986;49: 140- 155
1982;25:101-106
Motor Neuron Syndrome and Monoclonal IgM with Antibody Activity Against Ganghosides GM 1 and GDlb Ettore Nardelli, MD,' Andreas J. Steck, MD," Thomas Barkas, PhD,* Myriam Schluep, MD,* and Felix Jerusalem, MDt
~~~ ~
We demonstrated that an IgM M-protein from a patient with motor neuron syndrome had antibody activity against gangliosides GM1, GDlb, and asialo GM1. Stud- ies with a sugar-binding lectin suggested that the epi- tope in the patient's M-IgM involved the Gal(p1-3) GalNAc moiety. Immunohistological techniques dem- onstrated staining of axons in the lumbar roots, granular cells, and white matter in the cerebellum by the pa- tient's M-IgM. We propose that, in this case, an autoim- mune mechanism of motor neuron syndrome associated with a monoclonal protein is most likely.
Nardelli E, Steck AJ, Barkas T, Schluep M, Jerusalem F. Motor neuron syndrome and
monoclonal IgM with antibody activity against gangliosides GM1 and GDlb.
Ann Neurol 1988;23:524-528
Attention has been directed toward a possible relation- ship between monoclonal protein (M-protein) and neoplasia with motor ' neuron disease. The patho- genesis of motor neuron disease is still obscure, but an association with serum M-protein El-31 has been found. We report a patient with a motor neuron syn- drome and an IgM M-protein with autoantibody activ- ity against gangliosides GM1, GDlb, and asialo GM1.
Case Report A 64-year-old woman developed progressive generalized muscle weakness and wasting 2 years prior to admission. She had undergone mastectomy for breast cancer 15 years ago. The general physical examination revealed no abnormalities. On neurological examination, muscle atrophy and fascicula- tions in all limbs were evident. Muscle weakness was sym- metrical and more marked proximally; trunk muscles were also affected but there was no involvement of bulbar mus- cles. Tendon reflexes were decreased, and a Babinski's sign was equivocal on the left side. Sensation was normal.
From the *Department of Neurology, Centre Hospitalier Univer- sitaire Vaudois, Lausanne, Switzerland, and the "Department of Neurology, University of Bonn, Bonn, West Germany. Received Jul 10, 1987, and in revised form Oct 16. Accepted for publication Nov 17, 1987. Address correspondence to Dr Steck, Department of Neurology, CHUV, 1011 Lausanne, Switzerland.
524 Copyright 0 1988 by the American Neurological Association

Laboratory data showed no abnormalities except for mild normochromic anemia. Serum protein electrophoresis showed an IgM kappa monoclonal protein. Serum IgM con- tent was elevated (7.60 &) with normal levels of IgG and IgA. Bone marrow examination was normal. Computed to- mography scan of the abdomen was negative. Lght and elec- tron microscopic studies of a surd nerve biopsy specimen showed a moderate number of myelinated fibers undergoing acute axonal degeneration and a few smal l groups of re- generating fibers. In a few nerve fascicles, about 50% of the nerve fibers were affected. Motor (m) and sensory (s) nerve conduction velocities were as follows: left tibial nerve (m) 38 dsec ; left tibial nerve (s) 26.8 dsec ; left surd nerve (s) 43.2 dsec ; right surd nerve (5) 37.8 dsec . Electromyogram revealed widespread fibrillations and fasciculations (biceps brachii, extensor digitorum communis, tibialis anterior); the amplitudes of the motor action potentials varied between 4 and 12 mV, and the interference pattern was reduced. The mean action potential duration was 18.7 msec in the tibialis anterior muscle of the right side.
Methods Purification and Labeling of Patient’s IgM M-Protein The IgM M-protein was purified from the serum of the pa- tient with motor neuron syndrome of a control patient with an IgM kappa M-protein and no neurological involvement using gel filtration on an AcA 22 (LKB, Bromma, Sweden) column in phosphate-buffered saline (PBS), pH 7.0; precipi- tation with 50% ammonium sulfate for 2 hours at 4°C; and centrifugation. The pellet was redissolved in PBS containing 0.5 M NaC1, dialyzed against distilled water, and lyophilized. The column-purified IgM from the patient was radioiodi- nated by the chloramine T method 147.
Preparation and Analysis of Gangliosides Gangliosides were isolated from human sciatic nerve and human brain taken at autopsy according to Folch and as- sociates 151. Purified ganghosides (GM1, GDIb, GDla, asialo GMl) from calf brain were a gift from Dr G. Toffano (Fidia Research Laboratories, Abano Terme, Italy). GM2 and Folch extract of gangliosides were purchased from Supelco (Bellefonte, PA).
Gangliosides were analyzed by thin-layer chromatography (TLC) on Polygram-Sil G plates (Macherey-Nagel, Diiren, West Germany). The plates were developed in a solution of chloroform, methanol, and 0.2% CaCl2 (55,45, and 10 v/v, respectively) and the ganghosides were detected with acid (acetic acid, sulfuric acid, and anisaldehyde; 50, 1, and 0.3 v/v, respectively). Binding of antibody to individual ganglio- sides was investigated by incubating the TLC plate for 18 hours with lZ5I-M-IgM (3-6 x lo5 cpm) essentially accord- ing to Ilyas and associates, but omitting the polyisobutyl- methacrylate coating 161. Autoradiography was performed for 4 to 12 hours at - 70°C with the use of X-Omat AR film (Easunan Kodak Co, Rochester, NY) and an intensifying screen. Binding to gangliosides was also determined with an enzyme-linked immunosorbent assay (ELISA) 171.
Immunoabsoetion and Competition Studies For depletion experiments, 1251-M-IgM was incubated with undiluted normal rabbit serum or rabbit anti-human IgM
serum (k chain specific, Nordic, Tilburg, Netherlands) and the final volume adjusted to 100 pl with 2% bovine serum albumin (BSA) in PBS. An equal volume of 10% (v/v) Stapbyl’ococcus aurera in PBS with 0.1 % BSA and 1% Triton X 100 was then added and incubated for 30 minutes at room temperature. After centrifugation, the precipitate and the supernatant were then tested for antibody activity against ganghosides.
For competition studies, the binding of peroxidase-labeled peanut lectin from Aracbis bypogaea (Sigma, S t . Louis, MO) (0.1 mg/d in PBS-BSA) to gangliosides was analyzed on TLC plates with or without preincubation with patient’s M-IgM (1 4 2 . 5 ml). Liposomes were prepared in chloro- form-methanol from a lipid mixture containing phospha- tidylcholine (Sigma), cholesterol, and dicetylphosphate (P-L Biochemicals, Pharmacia, Uppsala, Sweden) in a molar ratio of 2 : 1.5 : 0.22 187. Single gangliosides (1 mg/ml) or agangho- side extract (Supeko) dissolved in methanol were added, and the mixture was sonicated for 15 minutes. Three hundred microliters of patient’s serum (diluted 10-fold in PBS) was mixed with 100 pI of liposomes and then incubated for 24 hours at 4°C. After centrifugation (10,000 g, 15 min) the supernatant was used.
Tissue Specimens and Immunoperoxidae Specimens of cerebellum, spinal cord, and lumbar roots ob- tained from autopsy not more than 24 hours after death were used for the indirect immunoperoxidase technique 191. Blocking studies on tissue specimens included the use of the liposome preparation described above.
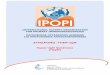
Results Total ganglioside fractions extracted from human cen- tral nervous system, as well as purified ganglioside frac- tions GDlb, GDla, GM1, asialo GM1, GM2, and GM3, were fractioned on TLC plates and stained or reacted with ‘251-IgM. As shown in Figure 1, the pa- tient’s M-IgM reacted with the ganghosides GM1, GDlb, and asialo GM1, and not with GDla, GM2, or GM3. Similar results were obtained in an ELISA test using plates coated with purified gangliosides. In this system, binding of the patient’s serum to GM1 and GDlb was detected to a dilution of 1 : lo6 (data not shown).
Further TLC experiments showed that (1) the bind- ing of the patient’s serum was specifically restricted to kappa light chains (data not shown); (2) the binding of the patient’s ‘251-M-IgM was abolished by the prein- cubation of the TLC plates with unlabeled patient’s M-IgM, whereas comparable amounts of control hu- man IgM failed to inhibit the binding of the patient’s serum 1251-M-IgM (Fig 2); (3) absorption with anti- human IgM antiserum specifically abolished the reac- tivity of the patient’s ‘251-M-IgM with the gangliosides (Fig 2); and (4) preincubation with the patient’s M-IgM inhibited the binding of peroxidase-labeled peanut lec- tin to GM1 and G D l b but not to asialo GM1 (data not shown).
Brief Communication: Nardelli et al: Motor Neuron Syndrome and IgM 525

Pig 1, Gangliosides separated b~ thin-hyer chromatography (TLC): (upper pane0 stained with acid. Immuno-TLC overlay with patient’s 1251-M-IgM ( h e r panel).
By immunocytochemistry, the patient’s serum IgM immunostained only axons in the lumbar roots (Fig 3A), whereas the sections of the cerebellum (Fig 3B) showed marked staining of the white matter and of fibers entering the granular layer. In the cerebellum, higher power magnification demonstrated a rim of stain on the surface of the granular cells, sometimes thicker on adjacent surfaces or near the stained fibers (Fig 3C). Absorption of the patient’s serum with lipo- somes containing GMl abolished the reaction (data not shown).
Discussion Our results provide good evidence that the IgM M- protein reacts specifically with the gangliosides GM 1, GDlb, and asialo GM1. In this case, the clinical syndrome with proximal muscle weakness, wasting, and fasciculations suggested the diagnosis of a motor neuron disorder. In regard to motor neuron disease, particularly amyotrophic lateral sclerosis, it has become clear that mild reduction of motor nerve conduction velocities, as well as degenerative changes in nonmotor systems, may occur [lo, 111. In many instances, as in this case, electrophysiological studies may not allow an exact separation between neuronal degeneration (motor neuron disease) and axonal degeneration (motor neuropathy). It may thus be appropriate to use the more broad term motor nezlmn syndrome in these patients.
An identical pattern of reactivity against GMl,
Fig 2. Gangliosirtes GMl, GDl b, andasialo GMl separated ly thin-layer chromatography (TLC) stained with acid (A), and immuno-TLC OverLays preincubated with unhbeled pa- tient’s M-IgM (B) or control human M-IgM (C) or afer selective depletion a t h e patient’s M-IgM with rabbit anti-human IgM (D) or control rabbit serum (El , then probed with 12JI-M-lgM.
GDlb, and asialo GM1 was observed by Freddo and associates [12) and Shy and associates [2] in 2 patients with motor neuron disease and IgM M- protein. Though these authors provided no clinical data on their cases, we suggest that we all are dealing with a new distinct entity with clinical features of a motor neuron disease associated with IgM M-protein with autoantibody activity against gangliosides GM1, GDlb, and asialo GM1. Freddo and associates 1121 speculated that the reactive epitope is the galactosyl (pl-3) N-acetylgalactosaminyl moiety, which is shared by the gangliosides GM1, GDlb, and asialo GM1. The lectin inhibition studies indicate a similar specificity in our patient. Since the Gal(f31-3)GalNAc epitope may represent the shared moiety between sialomucins in normal, as well as neoplastic, breast tissue [13, 14) and
526 Annals of Neurology Vol 23 No 5 May 1988

Fig 3 . Indirect immunoperoxidase staining with patient’s serum. (a) Ctyostat longitudinal sections from human lumbar roots. Numerous axon cylindws are strongly stained while myelin sheaths observed by phase contrast microscopy were completely un- Jtained. (x 360 before 25% reduction.) (6) Dqfuse staining of white matter and of numerous fibers in the granukar kayers while Purkinje cells and the cells of the molecukar kayer are unstained. (x GO befire 25% reduction.) (c) At higher magnification, dark rim of staining on the surJace of numerous granule cells. ( x I80 btfore 25% reduction.)
the &osides present in nervous tissue {15, 161, the history of breast tumor in this patient may be relevant to the pathogenesis of the motor neuron syndrome. Little is known about the origin of monoclonal protein, but it may be related to a chronic antigenic stimulation. In this case, it is possible that the primary antigen was a tumor cell determinant and that cross-reactivity of the antibody against sugar determinants present on nerve
cells could lead to the so-called remote effect of cancer on the nervous system.
Several elements of the central or peripheral ner- vous systems are the potential targets of immune- mediated paraneoplastic syndromes 1171. In our case, the immunohistological findings confirming the spe- cific localization of gangliosides GM1 and GDlb both in the granular layer and the white matter of the cere- bellum {lS], as well as in the axons {l8], are in keep- ing with their distribution as membrane constituents. The mechanism of motor nerve injury is not known, nor is the reason for the predominant involvement of the peripheral nervous system. Peripheral neurons may be especially susceptible to antibody that reacts with cell surface receptors such as gangliosides because binding at the nerve terminal may result in internalita- tion and retrograde transport of the antibody to the
Brief Communication: Nardelli et al: Motor Neuron Syndrome and IgM 527

cell soma. The significance of this mechanism will re- main unclear until direct experimental evidence of nerve injury by anti-GM1 and GDlb M-antibodies can be demonstrated.
This work was supported in part by the Swiss National Science Foundation, the Swiss Multiple Sclerosis Society, and the Puccini Foundation.
We thank Dr D. A. Figlewicz for help and Mrs G. Perruisseau for technical assistance. We are grateful to Prof J. M. Schroeder, Aachen, for providing the analysis of the nerve biopsy.
References 1. Iatov N. Plasma cell dyscmias and motor neuron disease. In:
Rowland LF', ed. Human motor neuron disease. New York: Raven, 1982:273-279
2. Shy ME, Rowland LP, Smith T, et al. Motor neuron disease and plasma cell dyscrasia Neurology 1986;36:1429-1436
3. Rudnicki S, Chad DA, Drachman DA, et al. Motor neuron disease and paraproteinemia Neurology 1987;37:335-337
4. Hunter WM. Preparation of Iodine-1 3 1 labelled human growth hormone of high specific activity. Nature 1962;194:495-496
5. Folch J, Lees M, Sloane-Stanley FGH. A simple method for the isolation and purification of total lipids from animal tissues. J Biol Chem 1957;226:497-509
6. Ilyas AA, Quarles RH, MacIntosh TD, et al. IgM in human neuropathy related to paraproteinemia binds to a carbohydrate determinant in the myelin associated glycoprotein and to a gan- ghoside. Proc Natl Acad Sci USA 1984;81:1225-1229
7. Endo T, Scott DD, Stewart SS, et al. Antibodies to glycosphin- golipids in patients with multiple sclerosis and SLE. J Immunol
8. Kinsky SC, Haxby JA, Zopf DA, et al. Complement dependent damage to liposomes prepared from pure lipids and Forssmann hapten. Biochemistry 1969;8:4149-4158
9. Sternberger LA. Immunocytochemistry. 2nd ed. New York: Wiley, 1979
10. Bradley WG, Good P, Rasool CG, et al. Morphometric and biochemical studies of peripheral nerves in amyotrophic lateral sclerosis. Ann Neurol 1983;14:267-277
11. Staberg E. Electrophysiological studies of reinnervation in ALS. In: Rowland LP, ed. Human motor neuron disease. New York Raven, 1982:47-59
12. Freddo L, Yu RK, Latov N, et al. Ganghosides GM1 and GDlb are antigens for IgM M-protein in a patient with motor neuron disease. Neurology 1986;36:454-458
13. Feizi T. Demonstration by monoclonal antibodies that carbohy- drate structures of glycoproteins and glycolipids are onco-devel- opmental antigens. Nature 1985;314:53-57
14. Walker RA. Mucoid carcinomas of the breast: a study using mucin histochemistry and peanut lectin. Histopathology 1982;
15. h e v H, Rapport MM, Mahadik SP, Silverman AJ. Immunohis- tological localization of ganglioside in rat cerebellum. Brain Res 1978;157: 136-14 1
16. Momoi T, Momoi MY, Kurata T. Peanut agglutinin receptor is a marker of myelin in rat brain. Developmental changes in its distribution. J Neurochem 1986;46:229-234
17. DhibJalbut S, Liwnict BH. Immunocytochemical binding of serum IgG from a patient with oat cell tumor and paraneoplastic motoneuron disease to normal human cerebral cortex and molecular layer of the cerebellum. Acta Neuropathol (Berl)
18. Roisen FJ, B d e l d H, Nagele R, Yorke G. GangLoside stimu- lation of axonal sprouting in vitro. Science 1981;214:577-578
1984;132:1793-1797
6571-579
1986;69:96- 102
An Antineuronal Autoantibody in Paraneoplastic Op soclonus Corinna Budde-Steffen, MD,*$ Neil E. Anderson, MB, ChB,'f Mark K. Rosenblum, MD,'FS Francesc Graus, MD,P David Ford, MD)' Beth J. L. Synek, MB, ChB," Shirley H. Wray, MD, PhD? and Jerome B. Posner, MD't
~~ ~~ ~~ ~~ ~~ ~ ~~ ~~ ~~ ~~ ~~ ~~ ~~ ~- ~
Sera from 7 patients with paraneoplastic opsoclonus were examined for antineuronal autoantibodies. An antibody against neuronal nuclei was found in serum from a patient with breast cancer, opsoclonus, and ataxia This antibody recognized 53- to 61-kDa and 79- to 84-kDa antigens in imunoblots of neurons. Anti- neuronal antibodies were not found in other patients with paraneoplastic opsoclonus.
Budde-Steffen C, Anderson NE, Rosenblum MK, Graus F, Ford D, Synek BJL, Wray SH, Posner JB.
An antineuronal autoantibody in paraneoplastic opsoclonus. Ann Neurol 1988;23:528-531
Opsoclonus, often associated with myoclonus, truncal ataxia, and encephalopathy, occurs as a remote effect of neuroblastomas in children El) and as a paraneo- plastic syndrome in adults 121. The discovery of anti- neuronal autoantibodies in patients with other para- neoplastic syndromes has suggested that these diseases may have an autoimmune etiology [3]. To determine if antineuronal antibodies occur in patients with paraneo- plastic opsoclonus, we examined serum from 6 adults and an infant with opsoclonus and a cancer.
Patients and Methods Serum was obtained from 7 patients with paraneoplastic op- soclonus (Table). The clinical and pathological features of Patients 2 through 6 with opsoclonus (see Table) have been reported in detail elsewhere [Z,7]. Control subjects included 5 patients with opsoclonus or ocular flutter and ataxia but without cancer; 1 patient with small-cell lung carcinoma, sub- acute sensory neuropathy (SSN), and an anti-Hu anti-
From the Departments of 'Neurology and ?Pathology (Neuro- pathology), Memorial Sloan-Kettering Cancer Center and $Cornell University Medical College, New York, NY; #the Department of Neurology, Hospital Clinic i Provincial de Barcelona, Spain; "the Department of Pathology, Auckland Hospital, Auckland, New Zea- land; and the *Department of Neurology, Massachusetts General Hospital, Boston, MA. Received Aug 5, 1987, and in revised form Nov 17. Accepted for publication Nov 18, 1987. Address correspondence to Dr Posner, Department of Neurology, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021.
528 Copyright 0 1988 by the American Neurological Association