Handout for the Neuroscience Education Institute (NEI) online activity
Mood Disorders A Spectrum Analysis
Learning Objectives
bull Utilize evidence-based strategies to identify where patients lie on the mood disorder spectrum
bull Optimize treatment strategies for patients based on where they lie along the mood disorder spectrum
PrePoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Pretest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
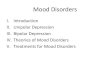
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
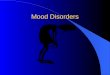
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
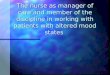
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
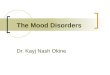
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Learning Objectives
bull Utilize evidence-based strategies to identify where patients lie on the mood disorder spectrum
bull Optimize treatment strategies for patients based on where they lie along the mood disorder spectrum
PrePoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Pretest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
PrePoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Pretest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Pretest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Pretest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Pretest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Pretest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
The Mood Disorder Spectrum
bull Although categorical classifications may be useful for clinical practice the overwhelming majority of the evidence points to a dimensional (spectrum) view of mood disordersndash eg treatment response (antidepressant vs mood stabilizing
agent) and links with family history of BP
bull Individuals with unipolar depression and a little bit of mania are more likely to have an eventual diagnostic conversion to bipolar disorder
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Benazzi F Eur Psychiatry 20082340-8 Hu J et al Primary Care Companion CNS Disord 201416(2)PCC13r01599 Sato T et al J Affective Disord 200481103-13
Vieta E Valenti M J Affective Disord 201314828-36
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
So You Think Its Unipolar Depression
bull Over one-third of unipolar patients are eventually re-diagnosed as bipolar
bull As many as 60 of patients with BPII are initially diagnosed as unipolar
bull Presence of even subthreshold (hypo)mania symptoms is strongly associated with conversion to bipolar disorderndash Each (hypo)mania symptom increases risk by ~30
Akiskal HS Benazzi J Affective Disord 200373113-22 Dudek D et al J Affective Disord 2013144(1-2)112-5 Fiedorowicz JG et al Am J Psychiatry 201116840-8
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
N=550 individuals followed for gt1 year (mean follow-up 175 years) after a diagnosis of major depression at intake
196 of patients converted to bipolar disorder during follow-up
Fiedorowicz JG et al Am J Psychiatry 201116840-8
Time to Hypomania or ManiaTime to Hypomania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
070 1040 1300 1560
08
780520260
Time to Mania
Prop
ortio
n W
ithou
t H
ypom
ania
or M
ania
Weeks to Follow-up
10
09
050 1040 1300 1560
08
780520260
ge3 Symptomslt3 Manic symptoms
06
07
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Unipolar Bipolar
Psychotic features
Family history of bipolar disorder
Hostility
Early age at onset of first depressive episode (lt25 years)
of lifetime affective episodes
Atypical depressive symptoms
Subsyndromal hypomanic symptoms
Impulsivity
Aggression
Worse response to antidepressants
Antidepressant-induced hypomania
Postpartum depressive episodes
Rapid onset of depressive episodes
of hospitalizations
Clues Across The Spectrum
Dervic K et al Eur Psychiatry 201530(1)106-13 Angst J et al Arch Gen Psychiatry 201168(8)791-9 Musetti L et al CNS Spectrums 201318(4)177-87
Clin
ical
His
tory
Trea
tmen
t H
isto
rySy
mpt
oms
Greater severity of depressive episodes
Comorbid SUD
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Converters328
Non-Converters672
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
34
36
38
40
42
44
Non-Converters Converters
Age
of I
llnes
s O
nset
(yrs
)
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
6
65
7
75
8
85
Non-Converters Converters
of
Dep
ress
ive
Epis
odes
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
0
10
20
30
40
Non-Converters Converters
o
f Pat
ient
s R
esis
tant
to
Ant
idep
ress
ants
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
005
115
225
335
4
Non-Converters Converters
of
Hos
pita
lizat
ions
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
0
5
10
15
20
25
30
Non-Converters Converters
Wee
ks S
pent
in a
Ps
ychi
atric
Hos
pita
l
Dudek D et al J Affective Disord 2013144(1-2)112-5
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
DIAGNOSIS ALONG THE SPECTRUM
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
A Rose By Any Other Namehellip
DSM-5 DIAGNOSIS
Major depressive
disorder (unipolar
depression)
Bipolar disorder II
Depression Mixedstates
Mania with subsyndromal depression
Depression with subsyndromal mania
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Bipolar disorder I
With mixed features if subthreshold (hypo)manic symptoms co-occur
with depressive episodes
With mixed features if subthreshold depressive symptoms co-occur with
manic episodes
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Evolution of the DSM
bull DSM-IV mixed episodendash Diagnostic criteria for major depression and mania
met at the same timebull DSM-5 mixed features specifier
ndash Recognizes the presence of subthreshold (hypo)manic symptoms during a depressive episode
ndash Specifier may be applied to major depressive disorder bipolar II or bipolar I
APA Diagnostic and Statistical Manual of Mental Disorders 4th ed Text Rev 2000APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
DSM-5 Mixed Features Specifier
bull Full criteria for a MDE and ge 3 of these manic symptoms
APA Diagnostic and Statistical Manual of Mental Disorders 5th ed 2013
bull Elevated expansive moodbull Inflated self-esteem or grandiositybull More talkative than usual or pressure to keep talkingbull Flight of ideas or racing thoughtsbull Increase in energy or goal-directed activity (socially at work or
school or sexually)bull Increased or excessive involvement in activities that have a high
potential for painful consequences (eg engaging in unrestrained buying sprees sexual indiscretions foolish business investments)
bull Decreased need for sleep
bull Diagnosis may be complicated by comorbid conditions including untreated ADHD personality disorders and substance abuse
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
McIntyre RS et al J Affective Disord 2015172C259-64
Mixed Features The Exception or the Rule
260340 338
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
n=149 n=65 n=49
MDD BPII BPI
Mixed Features Commonly Encountered in Adults With Both Major Depressive Disorder and Bipolar Disorder
The International Mood Disorders Collaborative Project
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Chart1
Column3
of Individuals Who Met Criteria For Mixed Features During an Index Major Depressive Episode
026
034
0338
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
MDD
BD-I
BD-II
Sheet1
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Column3
Column1
Column2
MDD
260
BD-I
340
BD-II
338
Depression With Mixed Features (DMX)
bull Associated withndash Family history of BPndash Suicidalityndash Antidepressant-induced
maniandash Young age of onsetndash Long duration of illnessndash Poor prognosisndash Severe depressionndash Antidepressant resistancendash Femalesndash Comorbid anxietyndash Comorbid SUDndash Impulse control
The prognosis for depression with co-occurring
(hypo)mania (DMX) is much worse than for pure unipolar
depression or bipolar depression without mixed
features
Akiskal HS Benazzi F J Affective Disord 200373113-22 Angst J et al Am J Psychiatry 20101671194-201 Goldberg JF et al Am J Psychiatry 2009166173-81
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Ruminationbull Initial or middle insomniabull Dramatic expressions of
sufferingbull Impulsivitybull Risky behaviors
Akiskal HS Banazzi F J Affective Disord 20058245-58 Benazzi F Akiskal HS Psychiatry Res 200614181-8 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Faedda GL et al J Affective Disord 201517618-23 Goldberg JF et al Am J Psychiatry 2009166173-81 Olgiati P et al Depression
Anxiety 200623389-97 Maj M J Clin Psychiatry 201576(3)e381-2 Perugi G et al J Clin Psychiatry 201576(3)e351-8 Sani G et al J Affective Disord 201416414-8 Suppes T et al Am J Psychiatry 2015
Epub ahead of print Takeshima M Oka T Psychiatry Clin Neurosci 201568109-16
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Symptoms Most Commonly Seen in DMX
0
10
20
30
40
50
60
Freq
uenc
y Am
ong
Patie
nts
With
DM
X
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
DMX Diagnostic Criteria
bull Although irritability distractibility and psychomotor agitation are among the most common symptoms of DMX they are excluded from DSM-5 mixed features criteria due to the overlap of these symptoms with other disorders (eg anxiety disorders) and between mania and depression
bull Some argue that these 3 particular symptoms are the defining features of DMX and that excluding them will lead to misdiagnosis and dangerous treatment strategiesndash Imagine if we excluded psychosis as a
diagnostic feature of schizophrenia
Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Mahli GS et al J Affective Disord 20141588-10
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Non-DSM Criteria for DMX
bull Do not exclude agitation irritability or distractibilityndash Benazzi criteriandash Koukopoulos criteriandash Research-based diagnostic criteria
bull Consider family historybull Consider age of onset of depression
Koukopoulos A Sani G Acta Psychiatr Scand 20141294-16 Benazzi F EurPsychiatry 20082340-8 Mahli GS et al J Affective Disord 20141588-10 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16 Perugi G et al J Clin Psychiatry
201576(3)e351-8
Non-DSM Criteria for DMX
0
5
10
15
20
25
30
DSM-5 CRITERIA RBDC CRITERIA
75
291
o
f Dep
ress
ed P
atie
nts I
dent
ified
as D
MX
4X as many cases of DMX identified using research-based diagnostic criteria
Perugi G et al J Clin Psychiatry 201576(3)e351-8
0
10
20
30
40
50
60
70
80
90
100
DSM-5 CRITERIA BENAZZI CRITERIA
1000
872
51
551
Specificity Sensitivity Sensitivity
Non-DSM Criteria for DMX
Benazzi F Eur Psychiatry 20082340-8 Takeshima M Oka T Psychiatry Clin Neurosci 201569(2)109-16
bull ~10 of patients identified as DMX will not actually have DMX
bull Less than 50 at risk of receiving inappropriate treatment
bull All patients identified as DMX will indeed have DMX
HOWEVERbull Only 51 of
individuals who have DMX will be identified
bull ~95 at risk of receiving inappropriate treatment
Which is potentially more detrimental Misdiagnosing someone who is pure unipolar as DMX
orTreating unidentified DMX with antidepressants
SensitivitySpecificity
Consequences of MisdiagnosisInappropriate Treatment
bull Years (often a decade or more) of unnecessary suffering
bull Treatment resistancebull Reduced likelihood of responding to eventual
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Treatment Resistance
bull Patients with DMX are less likely to respond to treatment-as-usual for major depressive disorder
bull Diagnostic conversion from unipolar to bipolar is significantly related to treatment resistancendash As many as two-thirds of patients whose diagnosis is converted from
unipolar to bipolar disorder are treatment resistant
bull Approximately half of patients with treatment-resistant unipolar depression may actually be bipolar
bull Repeated exposure to antidepressants may lead to resistance to mood stabilizers and poorer outcomes in patients without pure unipolar depressionndash It may also be that patients with more antidepressant trials were
always going to be resistantAngst J et al Am J Psychiatry 20101671194-201 Dudek D et al J Affective Disord 2013144(1-2)112-5 Sharma V et al J Affective Disord 200584(2-3)251-7 Rihmer Z Gonda X Depression
Res Treatment 20112011906426 Amsterdam JD Shults J J Affective Disord 2009115(1-2)234-40 Post RM et al J Clin Psychiatry 201273(7)924-30
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Treatment-Emergent Activation Syndrome (TEAS)
bull Over 20 of patients may experience TEAS related to antidepressants
bull Most common with serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
bull Hypothetically related to high noradrenergic potency
bull The presence of even minor subthreshold (hypo)mania during a depressive episode increases the risk of TEAS
Angst J et al Arch Gen Psychiatry 201168(8)791-9 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Post RM et al J Clin Psychiatry
201273(7)924 Akiskal HS et al J Affective Disord 20058245-58
(Hypo)mania
Agitation
Anxiety
Panic attacks
Irritability
Hostilityaggression
Impulsivity
Insomnia
Suicidality
Higher Risk of TEAS
bull Bipolar I gt bipolar IIbull History of antidepressant-
induced maniabull Mixed depressionbull Low TSH with TCA usebull Hyperthymic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Bond DJ et al J Clin Psychiatry 2008691589-601 Frye MA et al Am J Psychiatry 2009166164-72 Salvadore G et al J Clin Psychiatry 2010711488-501
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
DMX and Suicidality
bull Non-euphoric (hypo)manic symptoms (including psychomotor agitation impulsivity irritability and racingcrowded thoughts) combined with depressive symptoms (ie DMX) = recipe for suicidality
bull Presence of mixed features increases risk of suicidality by 4X in both unipolar and bipolar depression
bull DMX may underlie the connection between antidepressant use and suicidalityndash Most notably in the pediatric population in which DMX is often
the rule rather than the exceptionndash Both young age of onset of depression and DMX symptoms
indicate bipolarity
Akiskal HS Benazzi F Psychopathology 200538273-80 Balazs J et al J Affective Disord 200691133-8 Benazzi F Lancet 2007369935-45 Olgiati P et al Depression Anxiety 200623389-97 Swann AC et al
Bipolar Disord 20079(3)206-12 Rihmer Z Gonda X Depression Res Treatment 20112011906426
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Every time
One of the Most Important Questions to Ask Any Patient With Depression
Any maniahypomania
symptoms andor
family history of bipolar disorder
Every patient
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
DMX and Family History
bull Family history of BPndash 4X higher in DMX than in pure unipolar depressionndash Highly associated with patients who have 2+
(hypo)manic symptoms during major depressive episodes (MDEs)
ndash As common in DMX as in BPndash Supports the idea of DMX as a soft bipolar disorder
and a dimensional rather than a categorical view of mood disorders
Prieto ML et al J Affective Disord 2015172355-60 Axelson D et al Am J Psychiatry 2015172(7)638-46
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Tools for Assessing DMX
bull Bipolar Depression Rating Scale (BDRS)ndash Clinician-administered assessment of current symptoms
bull Mini International Neuropsychiatric Interview (MINI)bull Patient self-report assessing current (hypo)manic symptoms
bull Clinically Useful Depression Outcome Scale with DSM-5 Mixed (CUDOS-M)ndash Patient self-report assessing current (hypo)manic symptoms
bull Hypomania Checklist (HCL-32)ndash Patient self-report that screens for lifetime (hypo)manic
symptoms
See APPENDIX for more details on each assessment tool
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
TREATMENT ALONG THE SPECTRUM
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Mania
Mania withsubsyndromaldepression
MixedStates
Depression withsubsyndromal
mania
Depression
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mania Depression
MixedStates
Mania withsubsyndromaldepression
Depression withsubsyndromal
mania
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Issues With Existing Treatment Guidelines for DMX
bull Any existing guidelines (and FDA approvals) for mixed bipolar disorder refer to DSM-IV criteria (co-occurring threshold-level MDE + threshold-level mania)ndash Recommendations are to treat as mania
bull A diagnosis of MDD implies the use of unipolar depression treatment guidelinesndash Possibly ineffective and potentially harmful
bull Treatment guidelines for bipolar depression are likely the most applicable to DMXndash Many are not up to date with the latest clinical trial data (ie
atypical antipsychotics with mood-stabilizing properties)
bull Very few studies have yet to focus specifically on DMX
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Increasing severity of manic symptoms Increasing severity of depressive symptoms
Mania
Only those patients with essentially NO
symptoms of (hypo)mania should be considered for
antidepressant monotherapy
Unipolar depressionBipolar disorderDoes it matter in terms of choosing the best treatment
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
See DMX treatment guidelines
NoAntidepressant monotherapy
Therapeutic response to
antidepressant monotherapy
Yes
No
Switch to alternate
antidepressant monotherapy
Any maniahypomania symptoms andor family history of
BP
Continue antidepressant monotherapy
No
Resistant to 2 antidepressant monotherapy
trials
Any maniahypomania symptoms andor family history of
BP
Yes
No Yes
Treatment Algorithm for Depression Without Mixed
Features
Follow APA treatment
guidelines but consider DMX
treatment guidelines
Yes
Any maniahypomania symptoms andor family history of
BP
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Patient on antidepressant monotherapyYes NoDiscontinuetaper
antidepressant
Initiate atypical antipsychotic
Continue as maintenance
therapy
Therapeutic response
No
Add or switch to mood stabilizer
or switch to different atypical
antipsychotic
Therapeutic responseNo
Add antidepressant
Therapeutic response
No
Yes
Consider ECT and novelexperimental options
Treatment Algorithm for Depression With Mixed
Features (DMX)
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Atypical Antipsychotics
Cerullo M et al CNS Spectrums 201318(4)199-208 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Fountoulakis KN et al Int J Neuropsychopharmacol
2012151015-26 Grunze H Azorin JM World J Biol Psychiatry 201415(5)355-68 Vieta E ValentiM J Affective Disord 201314828-36 Fornaro M et al Int J Mol Sci 201617(2)241
doi103390ijms17020241 Stahl SM Prescribers Guide 5th ed Cambridge University 2014
Evidence ofEfficacy in
DMX
FDA-Approved for
BP Depression
FDA-Approved for
BP Mania
FDA-Approved for
BP Maintenance
FDA-Approved for
MDD
Aripiprazole (adjunct)
Asenapine Lurasidone Olanzapine
(with fluoxetine)
(with fluoxetine)
Quetiapine (adjunct)
Risperidone Ziprasidone
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Asenapine in DMX
Berk M et al J Clin Psychiatry 201576(6)728-34
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Placebo (n=100)
-64
Lurasidone (n=108)
-112
-64
-112
Placebo (n=100)
-54
Lurasidone (n=108)
-99
-54
-99
Placebo (N=100)
-49
Lurasidone (N=108)
-70
-49
-7
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
21
Placebo (N=100)
0
-38
-69
-88
-104
-122
-13
-669
Lurasidone (N=108)
0
-55
-97
-139
-162
-19
-205
Baseline
Baseline
Week 1
Week 1
Week 2
Week 2
Week 3
Week 3
Week 4
Week 4
Week 5
Week 5
Week 6
Week 6
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Cut-offs used to define depressive symptom severity in patients with ge3 depressive features mild (score ge1 for MADRS items and ge2 for PANSS items) moderate (score ge2 MADRS ge3 PANSS) and severe (score ge3 MADRS ge4 PANSS) symptoms remission defined as MADRS le12 post hoc analysis
McIntyre et al J Affective Disord 2013150(2)378-83
ple005 ple001 vs placebo
Placebo (n=69)Asenapine (n=113)Olanzapine (n=132)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Placebo (n=12)Asenapine (n=12)Olanzapine (n=16)
Mild depressive symptoms Moderate depressive symptoms Severe depressive symptoms
Improvement of depressive symptoms at Week 3
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Rem
issi
on ra
te (
)
Placebo (n=40)Asenapine (n=56)Olanzapine (n=66)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
MADRS responder rates (6-week LOCF-endpoint) groups with and without subsyndromal hypomania
Change from baseline in YMRS score groups with and without subsyndromal hypomania
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Patients on atypical antipsychotics should be regularly monitored for side effects including BMI
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Mood Stabilizers for DMX
bull No mood stabilizer is actually approved for use in depression of any kind (unipolar mixed bipolar)
bull There are some data for the efficacy of lamotrigine or valproate for bipolar depression
bull Lithium is well known for its anti-suicide effects however neither lithium nor carbamazepine monotherapy is recommended for the treatment of bipolar depression
Evidence ofEfficacy in
DMX
FDA-Approved for BP
Depression
FDA-Approved for BP Mania
FDA-Approved for BP
Maintenance
FDA-Approved for MDD
Carbamazepine Lamotrigine Lithium Valproate
Stahl SM Prescribers Guide 5th ed Cambridge University Press 2014 Goodwin GM et al J Psychopharmacol200923(4)346-88 Connolly KR Thase MD Primary Care Companion CNS Disord 201113(4)PCC10r01097
Fountoulakis KN et al Eur Arch Clin Neurosci 2012262(suppl 1)S1-48 Musetti L et al CNS Spectrums 201318(4)177-87
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Antidepressant Monotherapy for DMX
bull Nobull Dontbull Seriously just dont do it
bull Antidepressant monotherapy should probably NOT be used in patients with even the slightest hint of (hypo)mania (or a family history of bipolar disorder)
bull You will most likely not know if your depressed patient has ever had any (hypo)manic symptoms andor family history of bipolarity unless you askndash Every patient Every time
bull Any patient on antidepressant monotherapy should be regularly monitored for response and emergence of hypomania
Combination Therapy
bull The treatment of DMX may require a combination of medicationsbull Common combinations for BP depression include
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Olanzapine-fluoxetine combination in particularndash Mood stabilizer + antidepressant
bull The combination of olanzapine or risperidone and carbamazepine is not recommended always check the safety of any particular combination
bull If an antidepressant is prescribed for DMX it should be used in conjunction with a mood-stabilizing agent (atypical antipsychotic or mood stabilizer)
bull It is questionable whether adding an antidepressant to a mood stabilizer or an atypical antipsychotic has any therapeutic benefit
Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2 Nivoli AMA et al J Affective Disord
2012140125-41 Yatham LN et al Bipolar Disord 200911225-55
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
No significant benefit from adding fluoxetine to olanzapine
Benazzi F et al J Clin Psychiatry 200970(10)1424-31
Response defined as ge 50 reduction in the MADRS total score and lt 2 concurrent manichypomanic symptoms (measured by the YMRS)
0
5
10
15
20
25
30
35
40
45
PLACEBO OLANZAPINE OFC
o
f Res
pond
ers
(p=00006)
(p=0014)
(p=0065)NS
n=166 n=173 n=37
No Faster Recovery From Mixed Depression in Bipolar Disorder When Antidepressants Are Added to Mood
Stabilizers (STEP-BD)
Goldberg et al Am J Psychiatry 2007164(9)1348-55
355 STEP-BD entrants with major depression + 1 or more manic symptoms
n=145
n=190
Other Adjunctive Pharmacological Treatment Strategies
bull Modafinilarmodafinilndash Stimulants may worsen
symptoms (including irritability agitation and TEAS) in patients with DMX
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
bull Omega-3 fatty acidsbull Ramelteonbull Celecoxibbull Topiramate for weight
managementbull Benzodiazepines (short-
term) for anxiety and agitation
DellOsso B Ketter TA Int J Neuropsychopharmacol 20131655-68 Fountoulakis KN et al Eur Arch Psychiatry Clin Neurosci 2012262(suppl 1)S1-48 Goodwin GM J Psychopharmacol 200923(4)346-88 Grunze H et al
World J Biol Psychiatry 201011(2)81-109 Magiria S et al In Ritsner MS ed Use of Polypharmacy in the Real World New York NY Springer 2013 Polypharmacy in Psychiatry Practice vol 2
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Nonpharmacological Interventions
bull Electroconvulsive therapy (ECT)bull Transcranial magnetic stimulation (TMS)bull Sleep deprivationbull Individual or group psychoeducation
ndash Focus on early warning signs of relapsebull Interpersonal and family therapybull Cognitive behavioral therapy
Connolly KR Thase ME Primary Care Companion CNS Disord201113(4)PCC10r01097 Goodwin GM J Psychopharmacol 200923(4)346-88
Grunze H et al World J Biol Psychiatry 201011(2)81-109 Yatham LN et al Bipolar Disord 2013151-44
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Summary
bull Not all patients with depression should be given an antidepressant
bull The inappropriate overprescribing of antidepressants has contributed to drug-induced (hypo)manic episodes treatment resistance suicidality and overall poor quality of life for many patients suffering from depression
bull If there are any symptoms of (hypo)mania or a family history of bipolar disorder an antipsychotic with mood-stabilizing properties may be the best option
bull You will not know if a depressed patient has (hypo)manic symptoms or a positive family history of bipolar disorder unless you ask Every patient Every time
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
PostPoll Question
How many patients do you see with symptoms of mixed depression each week
1 02 1-53 6-104 11-155 16-206 21 or more
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Posttest Question 1
Sarah is a 20-year-old patient who presents with symptoms of depression (including sadness feelings of worthlessness and suicidal ideation) occurring every day for the past month Which class of medication would be most suitable for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 Either 1 or 25 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Posttest Question 2
Clinical interview with Sarah reveals that she has a maternal aunt with bipolar disorder I Further assessment reveals that Sarah feels distracted and as though her thoughts are racing Upon speaking with her mother it is discovered that Sarah has at times been more talkative than usual and irritable with her friends and family Which class of medication would NOT be recommended as monotherapy for this patient
1 An antidepressant2 A mood stabilizer3 An antipsychotic4 There is not enough information about this patients case to
make an informed treatment decision
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Posttest Question 3
Stacey is a 25-year-old patient with bipolar depression who tends to endorse some manic symptoms during depressive episodes Of the following symptoms which is the most common subsyndromal mania symptom in patients with mixed depression
1 Decreased need for sleep2 Inflated self-esteem3 Distractibility4 Increased goal-directed activity5 High-risk activity
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Posttest Question 4
A 33-year-old obese patient with treatment-resistant depression has agreed to a trial of an atypical antipsychotic Considering this patients current weight and the wish to avoid any treatment-induced weight gain which of the following approved treatments would be the least optimal treatment for this patient
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Mini International Neuropsychiatric Interview (MINI)
bull Patient self-report assessing current (hypo)manic symptoms
Herqueta T Weiller E Int J Bipolar Disord 2013121 Young AH Ebergard J Neuropsychiatr Dis Treatment 2015111137-43
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Frequency of each symptom during the prior week
0 1 2 3 4
Not at all Rarely Sometimes Often Almost always
I felt so happy and cheerful it was like a high
I had many brilliant creative ideas
I felt extremely self-confident
I slept only a few hours but woke full of energy
My energy seemed endless
I was much more talkative than usual
I spoke faster than usual
My thoughts were racing through my mind
I took on many new projects because I felt I could do everything
I was much more social and outgoing than usual
I did wild impulsive things
I spent money more freely than usual
I had many more thoughts and fantasies about sex
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
bull Patient self-report assessing current (hypo)manic symptoms
Zimmerman M et al J Affective Disord 2014168357-62
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic
Asenapine in Mania With Depressive Symptoms (DSM-5 Specifier)
Lurasidone in Bipolar Depression With Hypomanic Symptoms (DSM-5 Specifier)
Lurasidone Efficacy in DMXMontgomery-Aringsberg Depression Scale (MADRS)
Lurasidone Efficacy in DMXYoung Mania Rating Scale (YMRS)
Lurasidone Efficacy in DMXHamilton Anxiety Rating Scale (HAM-A)
Lurasidone Efficacy in DMXSheehan Disability Scale (SDS)
Lurasidone Efficacy in DMXSuicide and TEAS
Efficacy of Olanzapine Monotherapy in the Treatment of Bipolar Depression With Mixed Features
Quetiapine Efficacy in DMXClinical Global Impression (CGI-BD)
Quetiapine Efficacy in DMX MADRS
Quetiapine Efficacy in DMX YMRS
Ziprasidone Monotherapy for DMX Improvement in Depressive Symptoms
Ziprasidone Monotherapy for DMX No Improvement in Manic Symptoms
Tolerability of Atypical Antipsychotics
Mood Stabilizers for DMX
Antidepressant Monotherapy for DMX
Combination Therapy
Olanzapine-Fluoxetine Combination in the Treatment of Bipolar Depression With Mixed Features
Slide Number 65
Other Adjunctive Pharmacological Treatment Strategies
Nonpharmacological Interventions
Summary
PostPoll Question
Posttest Question 1
Posttest Question 2
Posttest Question 3
Posttest Question 4
APPENDIX
Bipolar Depression Rating Scale (BDRS)
Mini International Neuropsychiatric Interview (MINI)
Clinically Useful Depression Outcome Scale With DSM-5 Mixed Features (CUDOS-M)
Hypomania Checklist (HCL-32)
Hypomania Checklist (HCL-32)
bull Patient self-report that screens for lifetime (hypo)manic symptoms
Prieto ML et al J Affective Disord 2015172355-60 Altinbas K et al J Affective Disord 2014152-154L478-82httpwwwoacbddorgclientuploadsDocs2010Spring20HandoutsSession20220bpdf
Mood Disorders A Spectrum Analysis
Learning Objectives
PrePoll Question
Pretest Question 1
Pretest Question 2
Pretest Question 3
Pretest Question 4
The Mood Disorder Spectrum
So You Think Its Unipolar Depression
Progression to Bipolar Disorder From MDD With Subthreshold Hypomania
Clues Across The Spectrum
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Which Patients With Unipolar Depression Will Convert to Bipolar Disorder
Diagnosis along the spectrum
A Rose By Any Other Namehellip
Evolution of the DSM
DSM-5 Mixed Features Specifier
Mixed Features The Exception or the Rule
Depression With Mixed Features (DMX)
Symptoms Most Commonly Seen in DMX
Symptoms Most Commonly Seen in DMX
DMX Diagnostic Criteria
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Non-DSM Criteria for DMX
Consequences of MisdiagnosisInappropriate Treatment
Treatment Resistance
Treatment-Emergent Activation Syndrome (TEAS)
Higher Risk of TEAS
DMX and Suicidality
One of the Most Important Questions to Ask Any Patient With Depression
DMX and Family History
Tools for Assessing DMX
Treatment along the spectrum
Major Depressive EpisodesA Trace of Depression Means Treat With an Antidepressant
Major Depressive EpisodesA Trace of Mania Means Treat With an Antipsychotic