Embed Size (px)
Citation preview
Monodisciplinary, Multidisciplinary, Interdisciplinary, and Transdisciplinary
Approaches to Reproductive Health Research
William A. Fisher, Ph.DDepartment of Psychology
Department of Obstetrics and GynaecologyUniversity of Western Ontario
London Ontario Canada
Center for Health Intervention and PreventionUniversity of ConnecticutStorrs Connecticut USA
Monodisciplinary, Multidisciplinary, Interdisciplinary, and Transdisciplinary Approaches to
Reproductive Health Research
• Objectives– Define monodisciplinary, multidisciplinary,
interdisciplinary, and transdisciplinary approaches.
– Provide examples of transdisciplinary approaches.
– Discuss transdisciplinary research team creation and functioning.
Science = Explanation
• The only reason to do something in scientific research is to increase our:– Understanding– Prediction– Control
Monodisciplinary Approaches
• Exploiting the knowledge base, research methodology, and research personnel of a single established scientific discipline.
• Traditional research paradigm.
Monodisciplinary Approaches
• Advantages: cumulative disciplinary knowledge base, mature disciplinary research methodology, availability of experienced research personnel, homogeneous research culture.
• Disadvantages: narrow focus on restricted dimensions of potentially complex and multilevel reproductive health research questions; lack of comprehensive scope to provide complete understanding of reproductive health research problem.
Multidisciplinary Approaches
• Multidisciplinary research involves scientists from different disciplines who work independently and in parallel on different and separate aspects of a reproductive health research question.
• For example, stem cell researcher and an ethicist form a multidisciplinary team to study stem cell issues and publish papers on different aspects of this topic in special issue of a journal.
– After Sorrels-Jones, 1997
Multidisciplinary Approaches• Advantages: more comprehensive
understanding of a reproductive health research question may accumulate; no research approach, knowledge base, or research culture heterogeneity to challenge researchers.
• Disadvantage: “Discoordiante parallel play” fails to exploit and integrate scientific viewpoints and expertise of multiple disciplines; gains in comprehensiveness somewhat random and at best additive.
Interdisciplinary Approaches
• “Interdisciplinary research is a cooperative effort by a team of investigators, each expert in the use of different methods and concepts, who have joined in an organized program to attack a challenging problem. Ongoing communication and reexamination of postulates among team members promote broadening of concepts and enrichment of understanding. Although each member is primarily responsible for the efforts in his or her own discipline, all share responsibility for the final product.”
– Institute of Medicine, 2002
Interdisciplinary Approaches
• Advantages: Exploits an array of relevant disciplinary knowledge bases, methodologies, and perspectives to gain comprehensive understanding of complex and multilevel reproductive health research problem.
• Disadvantages: Leaves unanswered the question of how the multiple relevant disciplinary aspects of the reproductive health research question will be identified and how the interdisciplinary contributions will be reassembled to represent a complex understanding of the reproductive health problem.
Transdisciplinary Approach
• Transdisciplinary research involves active and collaborative analysis of a reproductive health research question to:– identify its potentially multiple relevant disciplinary
dimensions; – identify the interdisciplinary team needed to address the
problem;– construct a working model of the multiple determinants
and consequences of a reproductive health condition or treatment
• Transdisciplinary research incorporates and goes beyond interdisciplinary approach.
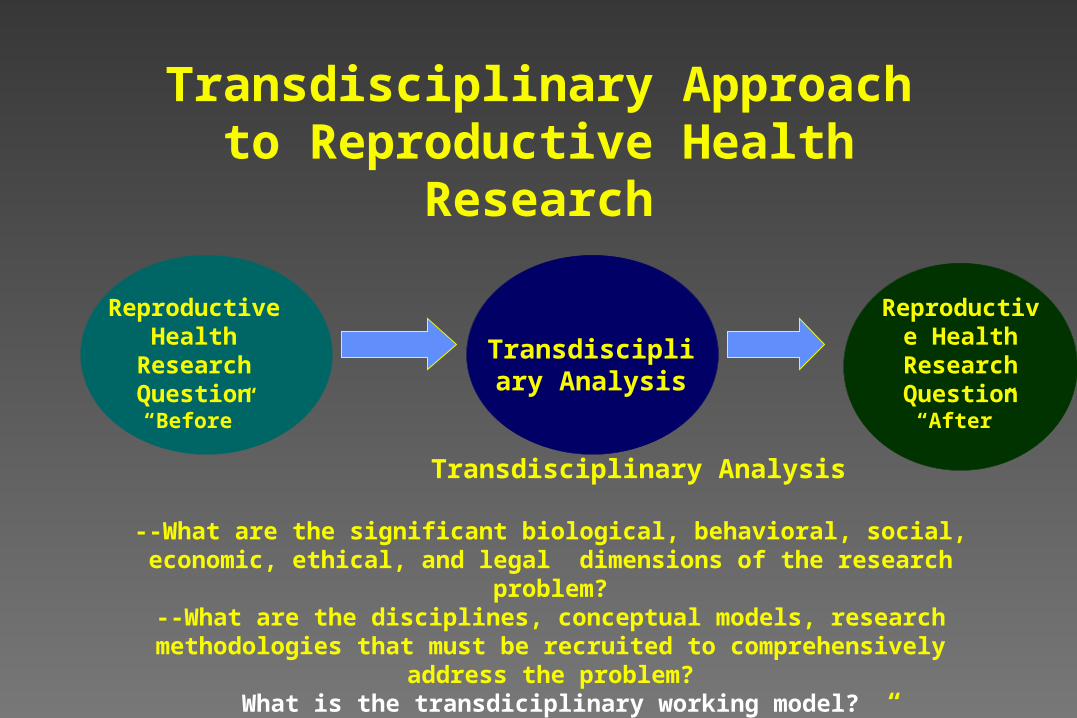
Transdisciplinary Approach to Reproductive Health Research
Reproductive Health Research
Question“Before”
Transdisciplinary Analysis
--What are the significant biological, behavioral, social, economic, ethical, and legal dimensions of the research problem?
--What are the disciplines, conceptual models, research methodologies that must be recruited to comprehensively address the problem?
What is the transdiciplinary working model?Results in “Interdisciplinarity Done Well”
Transdiscipliary Analysis
Reproductive Health
Research Question
“After”
Transdisciplinary Approach
• Advantages: actively identifies a working conceptual model incorporating multiple relevant determinants of reproductive health phenomena and multiple relevant outcomes of reproductive health interventions.
• Advantage: Provides comprehensive understanding of reproductive health research question.
Transdisciplinary Approach
• Disadvantage: Requires understanding of multiple disciplinary knowledge bases, methodologies, approaches, and research perspectives and cultures.
• Disadvantage: Requires commitment to the idea that transdisciplinary approach, where appropriate, may comprise superior science.
• Disadvantage: No one, within graduate school or residency, is trained to do transdiciplinary research.
Transdisciplinary Approach to Research on Erectile Dysfunction:
UrologyPharmacology
Molecular BiologyPsychology
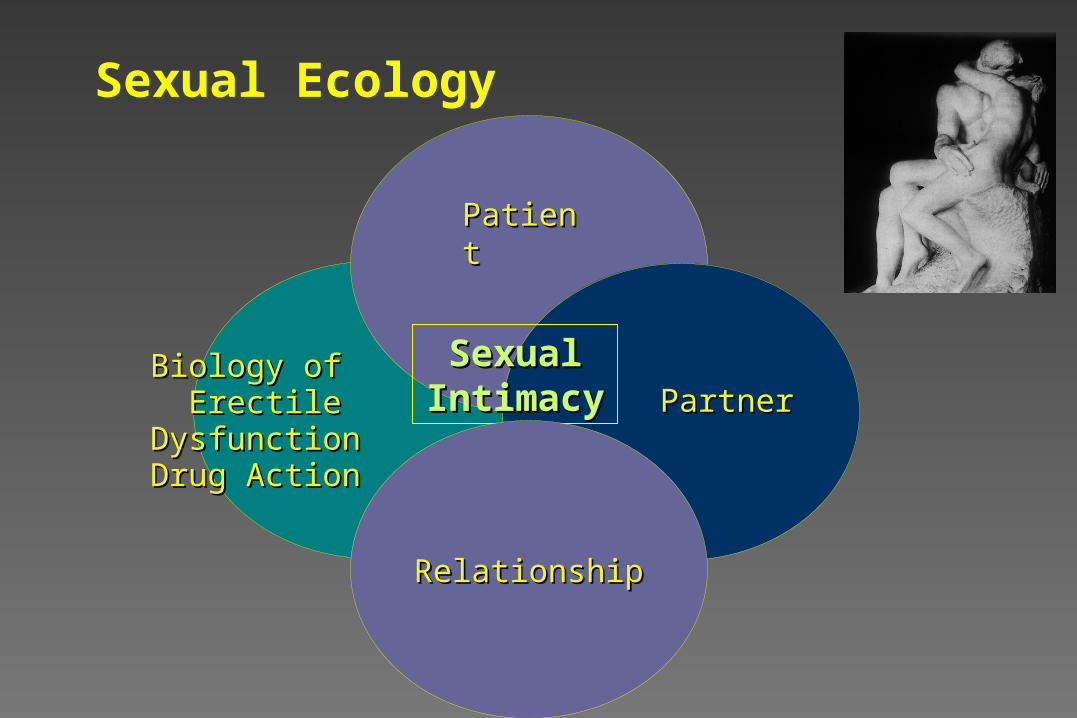
Sexual Ecology
Biology of Biology of Erectile DysfunctionErectile Dysfunction
Drug ActionDrug Action
PatientPatient
PartnerPartnerSexual Sexual
IntimacyIntimacy
RelationshipRelationship
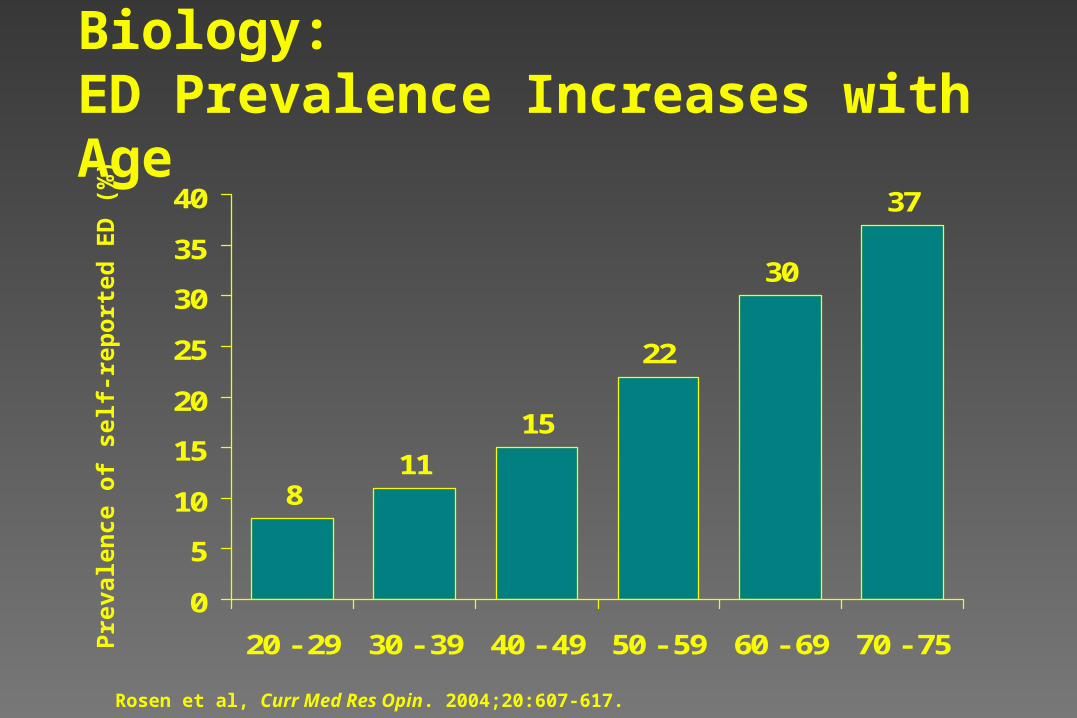
Biology:ED Prevalence Increases with Age
811
15
22
30
37
0
5
10
15
20
25
30
35
40
20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 75
Pre
vale
nce
of
self
-rep
ort
ed E
D (
%)
Rosen et al, Curr Med Res Opin. 2004;20:607-617.
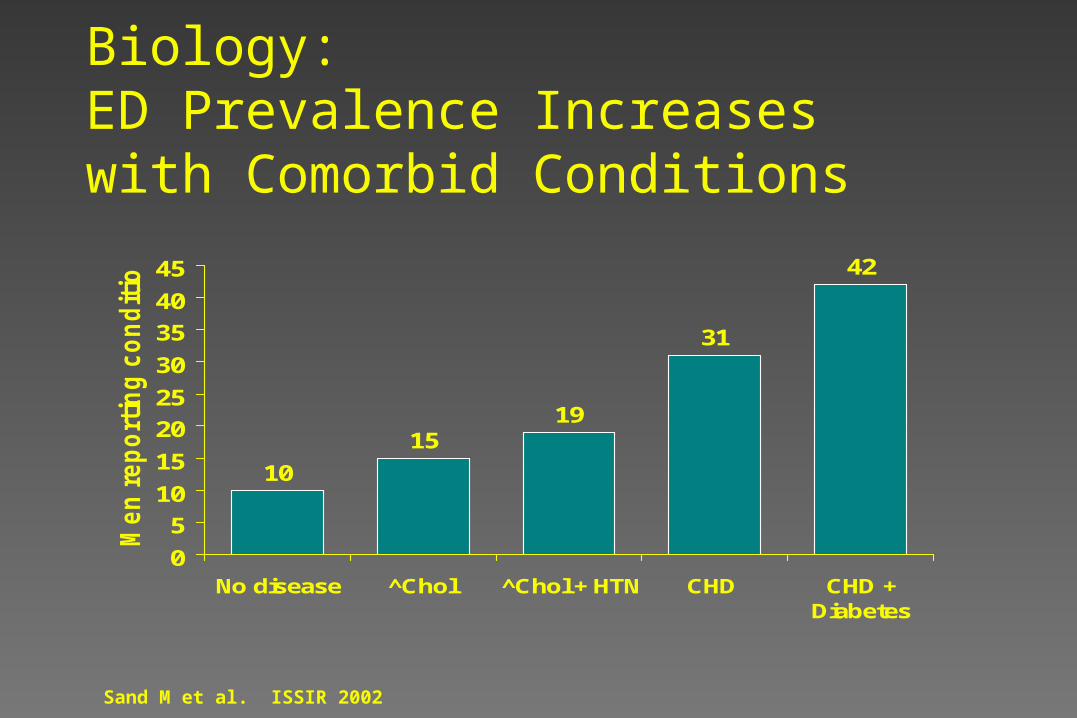
10
1519
31
42
0
5
10
15
20
25
30
35
40
45
No disease ^Chol ^Chol + HTN CHD CHD +Diabetes
Men
rep
ort
ing
co
nd
itio
n (
%)
Biology:ED Prevalence Increases with Comorbid Conditions
Sand M et al. ISSIR 2002
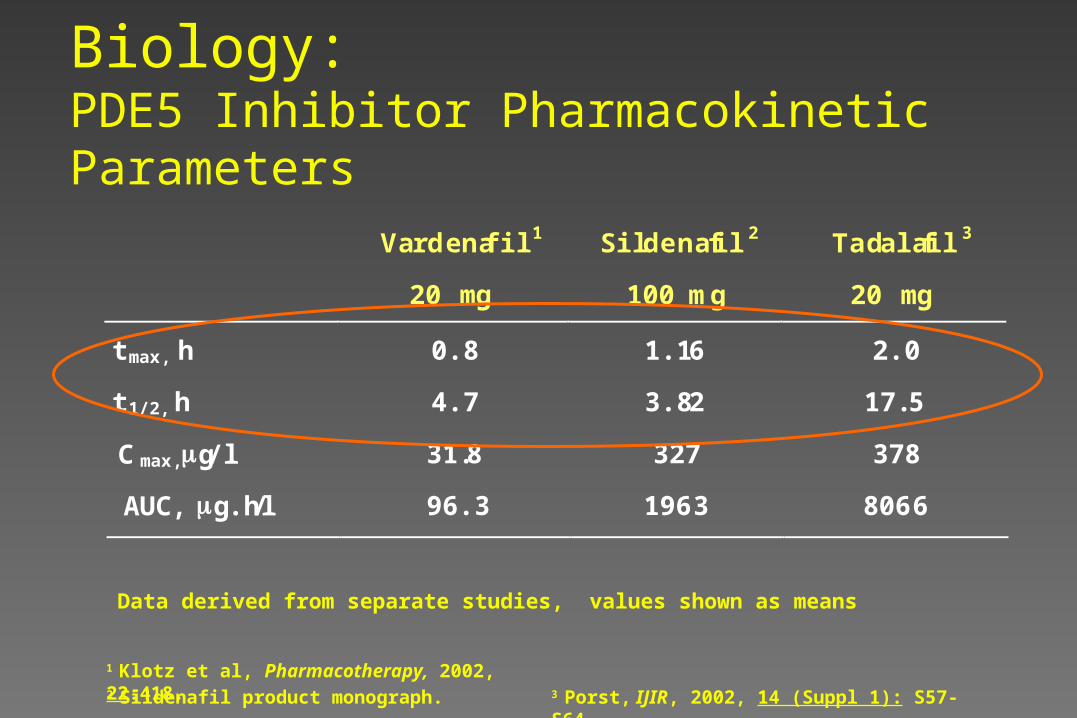
Biology:PDE5 Inhibitor Pharmacokinetic Parameters
1 Klotz et al, Pharmacotherapy, 2002, 22:418. 2 Sildenafil product monograph. 3 Porst, IJIR, 2002, 14 (Suppl 1): S57-S64.
Data derived from separate studies, values shown as means
Vardenafil 1 Sildenafil 2 Tadalafil 3
20 mg 100 mg 20 mg
0.8 1.16 2.0
4.7 3.82 17.5
31.8 327 378
tmax, h
t 1/2, h
C max,g/l
AUC, g.h/l 96.3 196 3 806 6
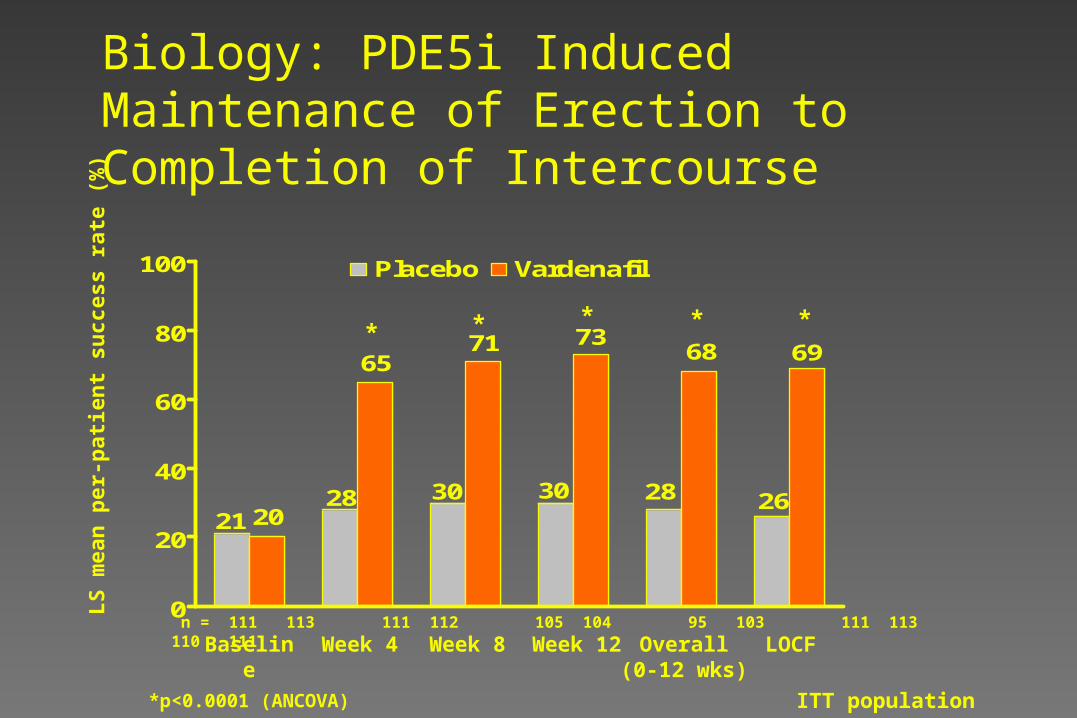
ITT population
21 2028
65
30
71
30
73
28
68
26
69
0
20
40
60
80
100 Placebo Vardenafil
n = 111 113 111 112 105 104 95 103 111 113 110 111
*p<0.0001 (ANCOVA)
LS
mea
n p
er-p
atie
nt
succ
ess
rate
(%
)
* * * *
Biology: PDE5i Induced Maintenance of Erection to Completion of Intercourse
*
Baseline Week 4 Week 8 Week 12 Overall(0-12 wks)
LOCF
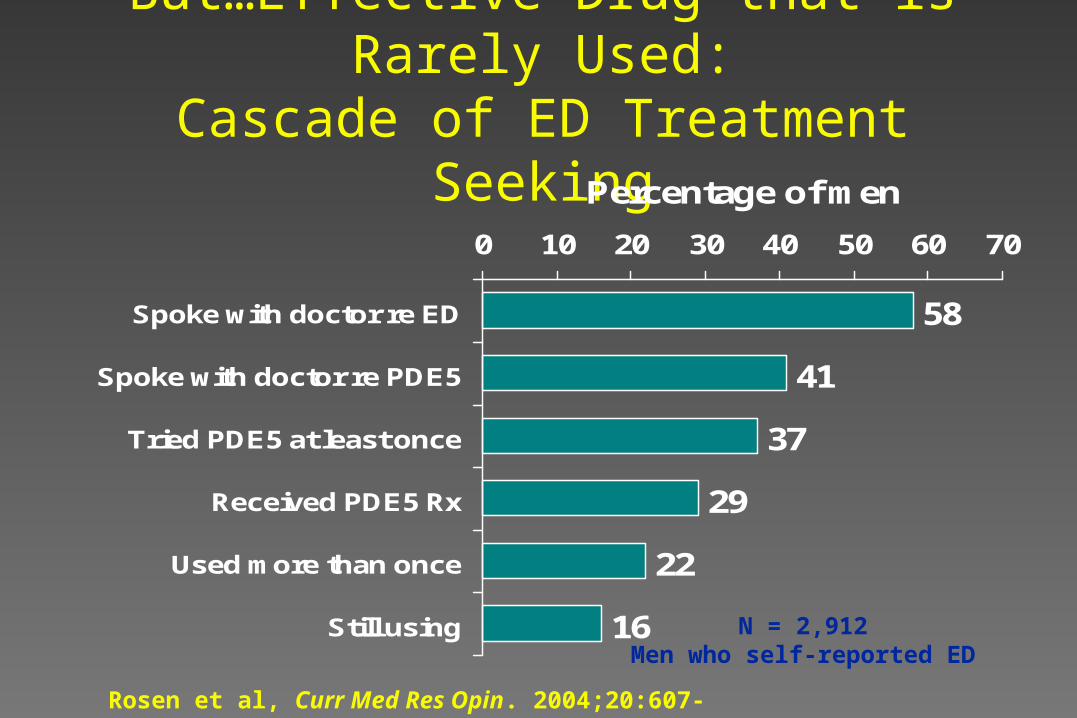
But…Effective Drug that is Rarely Used:Cascade of ED Treatment Seeking
58
41
37
29
22
16
0 10 20 30 40 50 60 70
Spoke with doctor re ED
Spoke with doctor re PDE5
Tried PDE5 at least once
Received PDE5 Rx
Used more than once
Still using
Percentage of men
N = 2,912Men who self-reported ED
Rosen et al, Curr Med Res Opin. 2004;20:607-617.
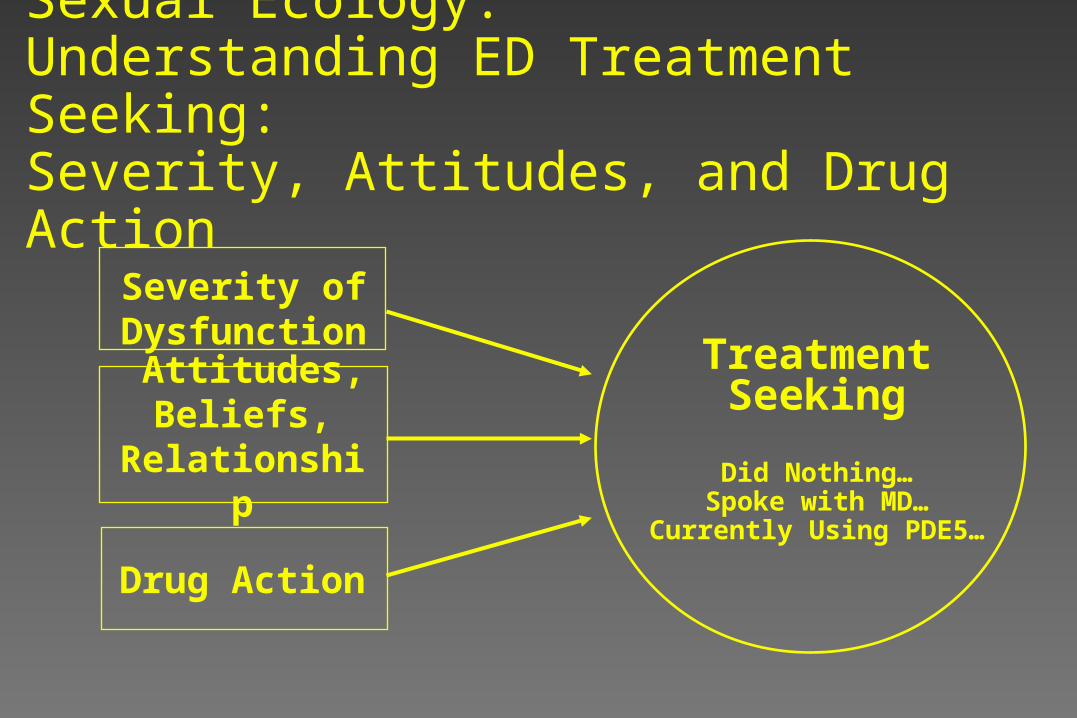
Severity of Dysfunction
Attitudes, Beliefs,
Relationship
Drug Action
Treatment Seeking
Did Nothing…Spoke with MD…
Currently Using PDE5…
Sexual Ecology:Understanding ED Treatment Seeking:Severity, Attitudes, and Drug Action
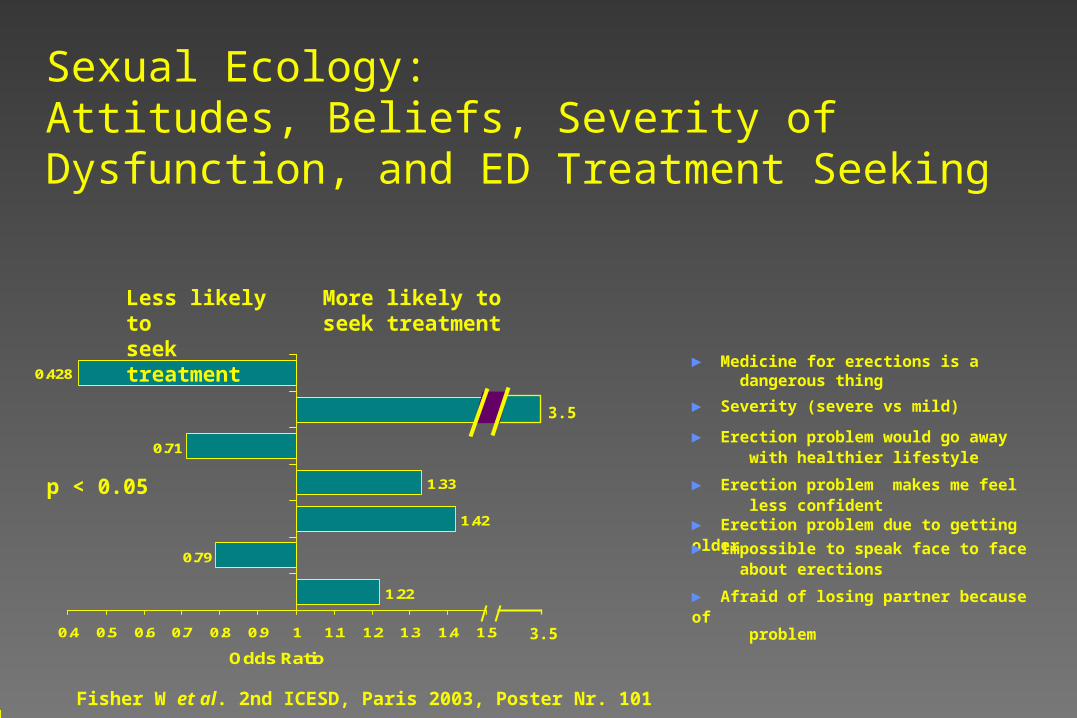
Sexual Ecology:Attitudes, Beliefs, Severity of Dysfunction, and ED Treatment Seeking
► Medicine for erections is a dangerous thing
► Erection problem would go away with healthier lifestyle
► Erection problem makes me feel less confident► Erection problem due to getting older
► Impossible to speak face to face about erections
► Afraid of losing partner because of problem
Fisher W et al. 2nd ICESD, Paris 2003, Poster Nr. 101
1.22
0.79
1.42
1.33
0.71
0.428
0.4 0.5 0.6 0.7 0.8 0.9 1 1.1 1.2 1.3 1.4 1.5
Odds Ratio
Less likely to seek treatment
More likely to seek treatment
3.5
3.5
p < 0.05
► Severity (severe vs mild)
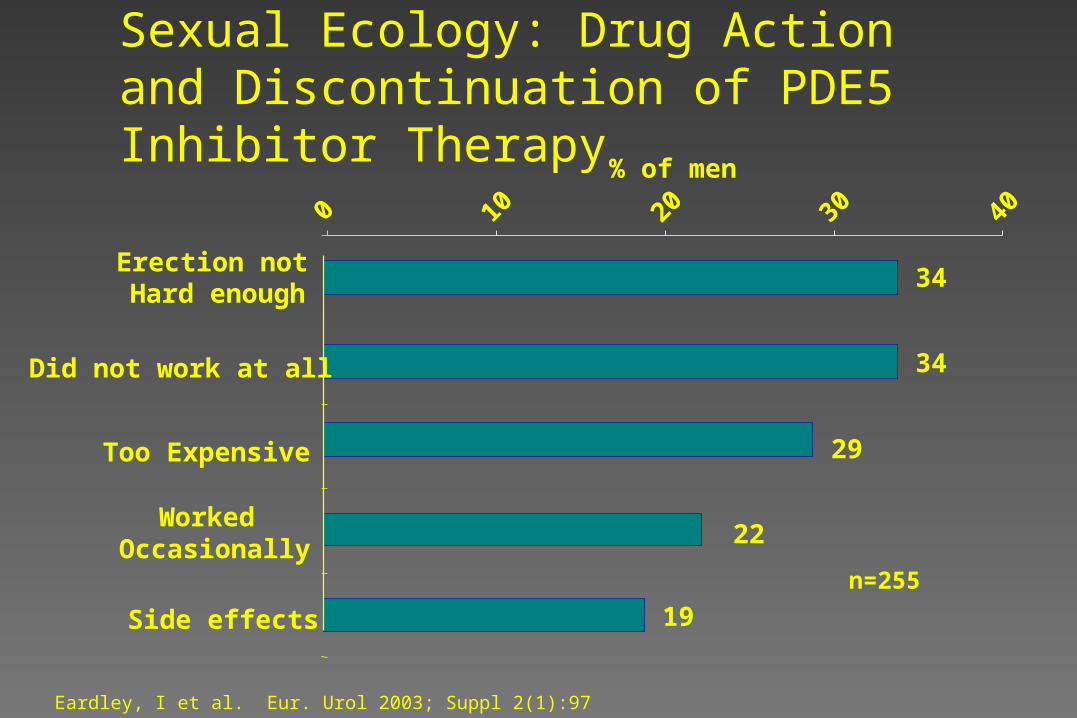
Sexual Ecology: Drug Action and Discontinuation of PDE5 Inhibitor Therapy
19
22
29
34
34
0 10 20 30 40
Side effects
Worked Occasionally
Too Expensive
Did not work at all
Erection not Hard enough
% of men
n=255
Eardley, I et al. Eur. Urol 2003; Suppl 2(1):97
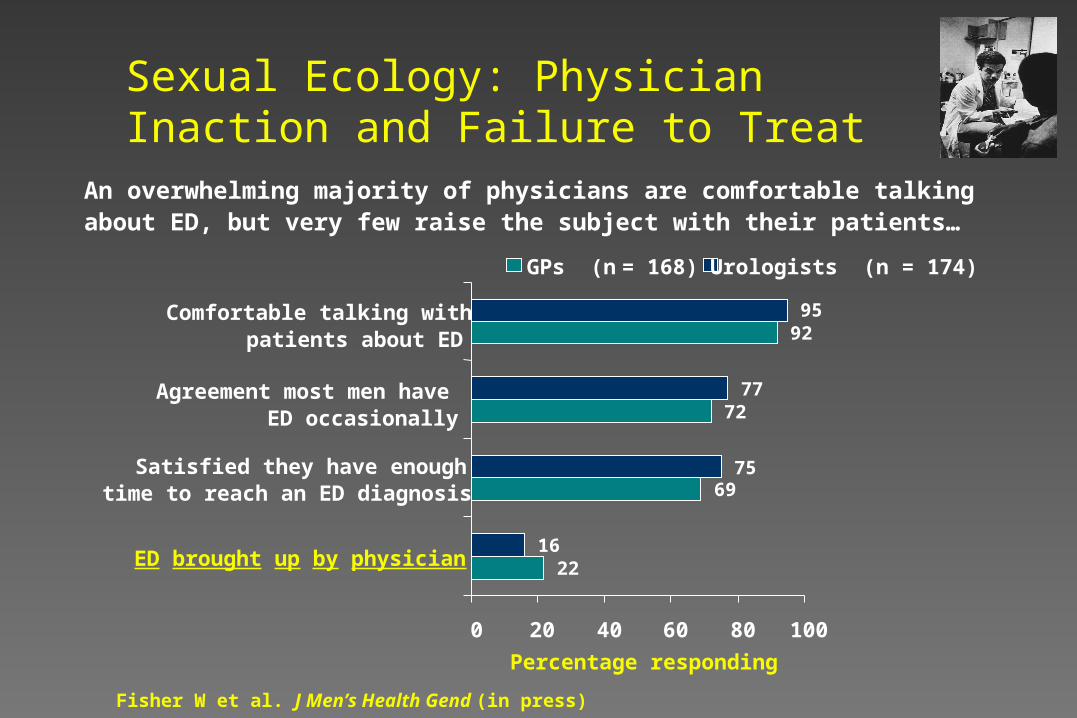
Sexual Ecology: Physician Inaction and Failure to Treat
An overwhelming majority of physicians are comfortable talking about ED, but very few raise the subject with their patients…
22
69
72
92
16
75
77
95
0 20 40 60 80 100
ED brought up by physician
Satisfied they have enoughtime to reach an ED diagnosis
Agreement most men haveED occasionally
Comfortable talking withpatients about ED
GPs (n = 168) Urologists (n = 174)
Percentage responding
Fisher W et al. J Men’s Health Gend (in press)
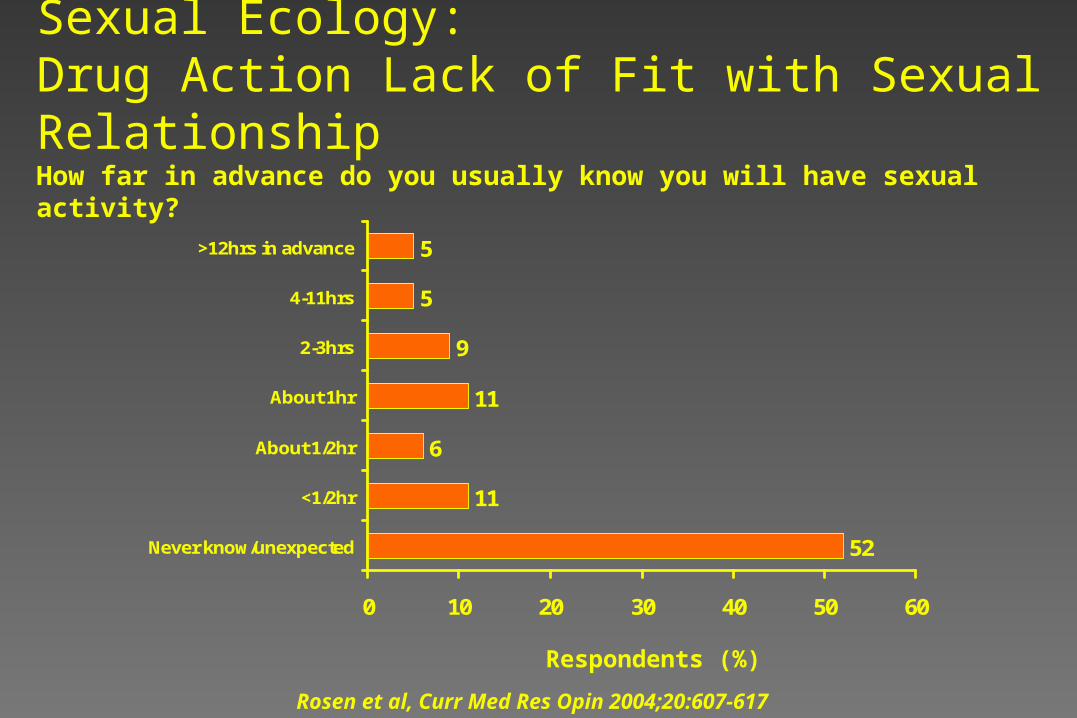
52
11
6
11
9
5
5
0 10 20 30 40 50 60
Never know/unexpected
<1/2hr
About 1/2hr
About 1hr
2-3hrs
4-11hrs
>12hrs in advance
Sexual Ecology:Drug Action Lack of Fit with Sexual RelationshipHow far in advance do you usually know you will have sexual activity?
Respondents (%)
Rosen et al, Curr Med Res Opin 2004;20:607-617
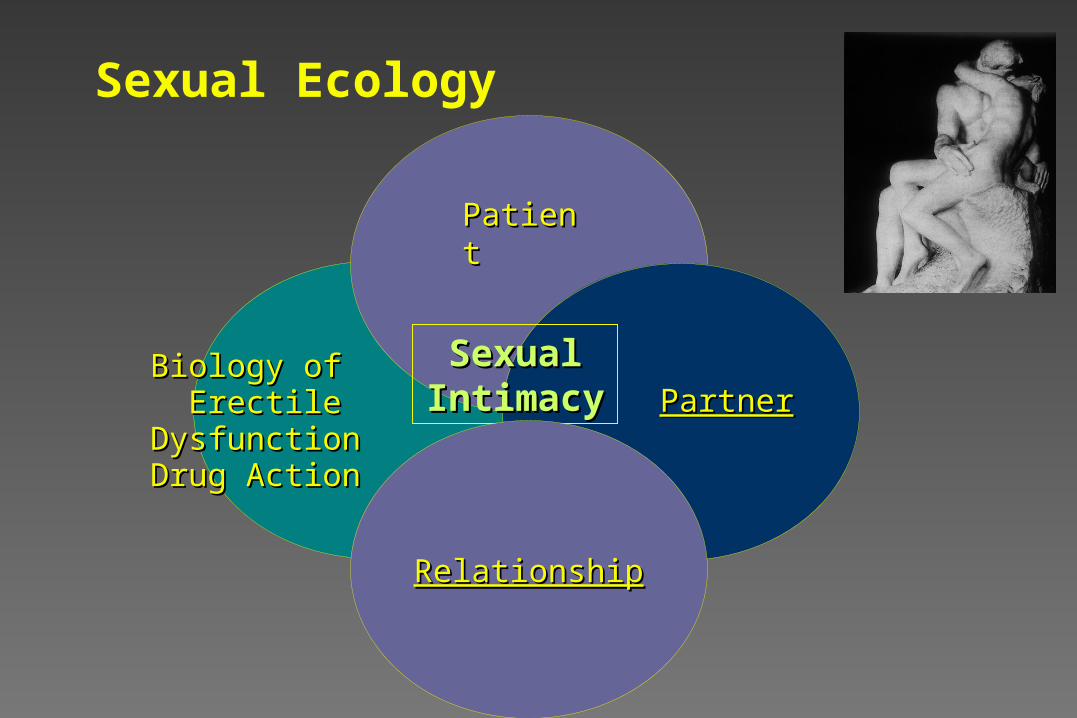
Sexual Ecology
Biology of Biology of Erectile DysfunctionErectile Dysfunction
Drug ActionDrug Action
PatientPatient
PartnerPartnerSexual Sexual
IntimacyIntimacy
RelationshipRelationship
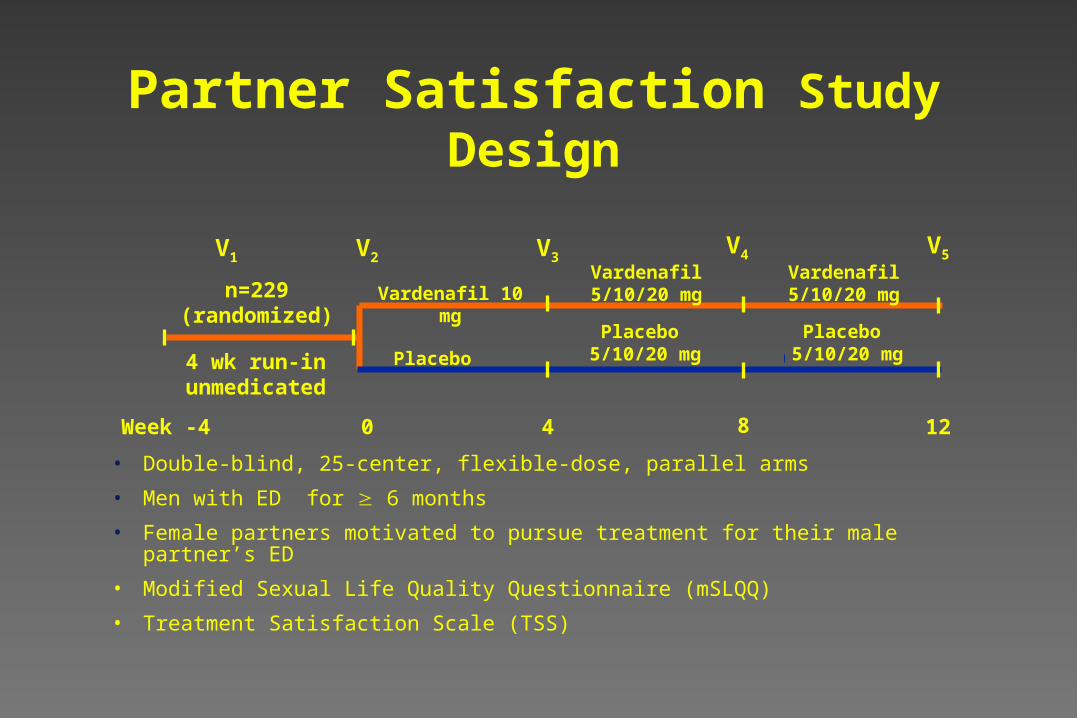
n=229 (randomized)
4 wk run-inunmedicated
Week -4 0 4 8 12
Placebo
Placebo 5/10/20 mg
Vardenafil 10 mgVardenafil 5/10/20
mg
V1 V2 V3V4 V5
Placebo 5/10/20 mg
Vardenafil 5/10/20 mg
Partner Satisfaction Study Design
• Double-blind, 25-center, flexible-dose, parallel arms
• Men with ED for 6 months
• Female partners motivated to pursue treatment for their male partner’s ED
• Modified Sexual Life Quality Questionnaire (mSLQQ)
• Treatment Satisfaction Scale (TSS)
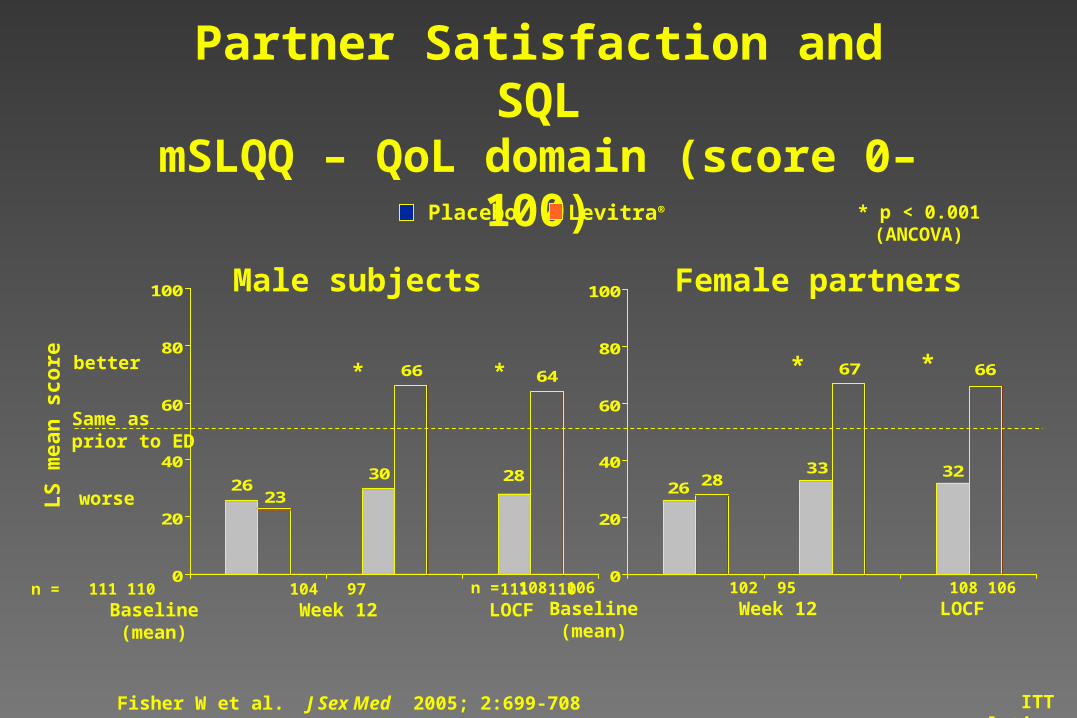
2623
30
66
28
64
0
20
40
60
80
100
Partner Satisfaction and SQLmSLQQ – QoL domain (score 0–100)
26 2833
67
32
66
0
20
40
60
80
100
n = 111 110 104 97 111 110 Baseline Week 12 LOCF (mean)
* p < 0.001(ANCOVA)
n = 108 106 102 95 108 106 Baseline Week 12 LOCF (mean)
Male subjects Female partners
Same asprior to ED
worse
better
Levitra®Placebo
LS
mea
n s
core * * * *
ITT populationFisher W et al. J Sex Med 2005; 2:699-708
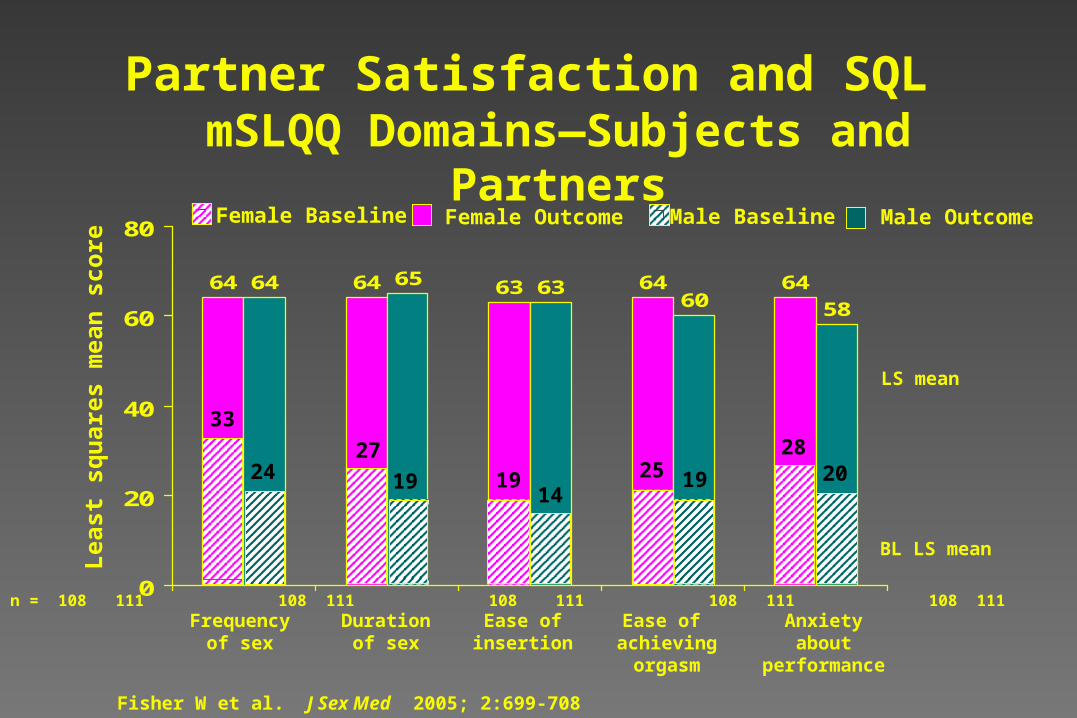
64 64 63 64 6464 65 6360 58
0
20
40
60
80
Frequencyof sex
Durationof sex
Ease ofinsertion
Ease of achievingorgasm
Anxietyabout
performance
n = 108 111 108 111 108 111 108 111 108 111
Lea
st s
qu
ares
mea
n s
core
Female Baseline Male Baseline
BL LS mean
LS mean
201914
1924
33
27
19 2528
Partner Satisfaction and SQL mSLQQ Domains—Subjects and Partners
Fisher W et al. J Sex Med 2005; 2:699-708
Female Outcome Male Outcome
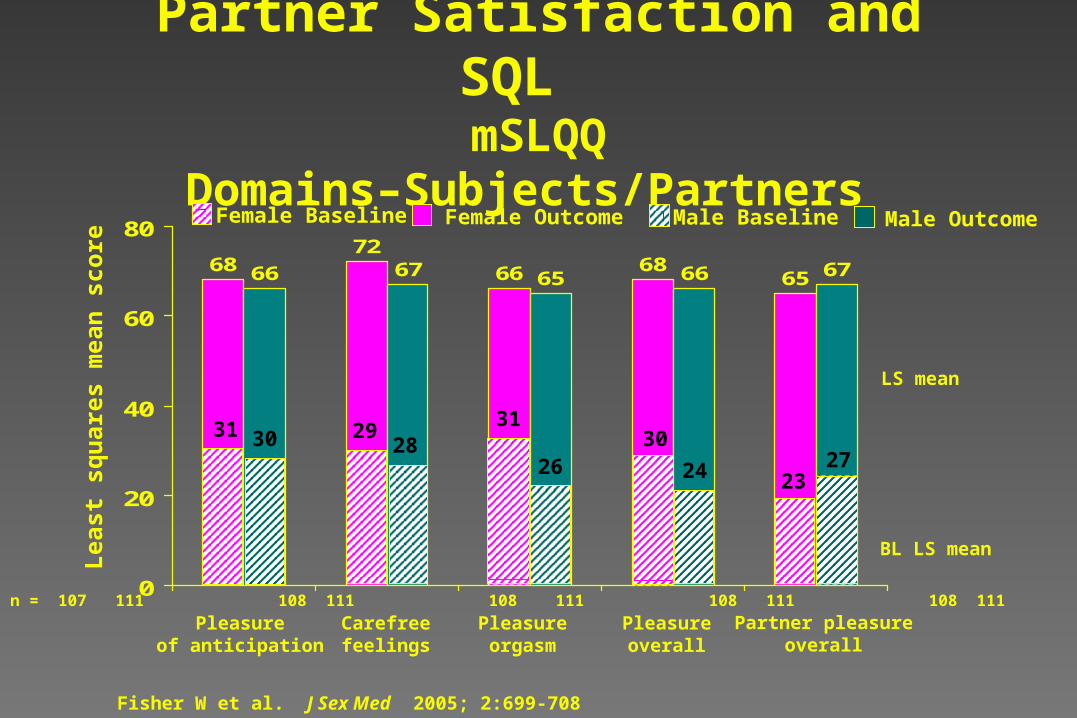
6872
66 686566 67 65 66 67
0
20
40
60
80
Pleasureof anticipation
Carefreefeelings
Pleasureorgasm
Pleasureoverall
Partner pleasureoverall
n = 107 111 108 111 108 111 108 111 108 111
Lea
st s
qu
ares
mea
n s
core
BL LS mean
LS mean
272426283031 29
3130
23
Partner Satisfaction and SQL mSLQQ Domains–Subjects/Partners
Fisher W et al. J Sex Med 2005; 2:699-708
Female Baseline Male BaselineFemale Outcome Male Outcome
0
20
40
60
80
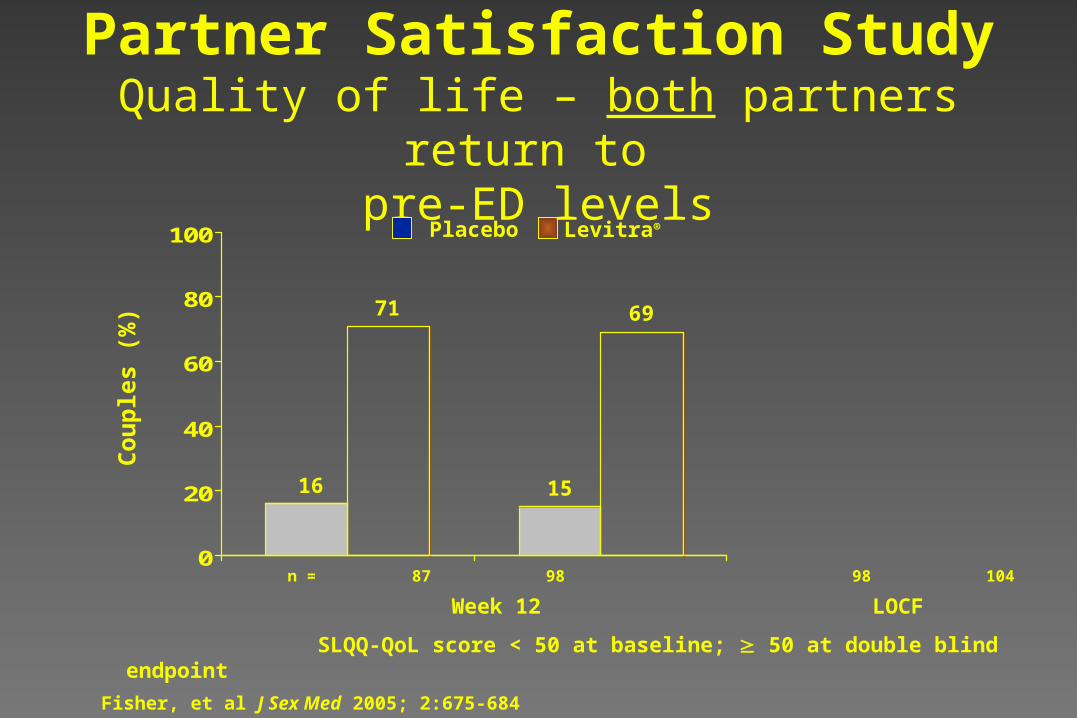
100
n = 87 98 98 104
Week 12 LOCF
SLQQ-QoL score < 50 at baseline; 50 at double blind endpoint
71
16
69
15
Co
up
les
(%)
Partner Satisfaction StudyQuality of life – both partners return to
pre-ED levelsLevitra®Placebo
Fisher, et al J Sex Med 2005; 2:675-684