Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2012) 65, e169ee174
INVITED COMMENTARY
Modification of flap design for total mobile tonguereconstruction using a sensitive antero-lateralthigh flap
Nicolas Leymarie*, Guillaume Karsenti, Benjamin Sarfati,Francoise Rimareix, Frederic Kolb
Division of Plastic Surgery, Institut Gustave Roussy, 114 rue Edouard Vaillant, 94800 Villejuif, France
Received 29 July 2011; accepted 7 November 2011
KEYWORDSMobile tonguereconstruction;Cathedral triptychdesign
* Corresponding author. Tel.: þ33 (042 11 52 73.
E-mail addresses: nicolas.leymaryahoo.fr (N. Leymarie).
1748-6815/$-seefrontmatterª2011Bridoi:10.1016/j.bjps.2011.11.012
Summary Reconstruction of large carcinologic tongue defect is mandatory to recoveradequate speech and swallowing. Free flaps provide thin and pliable tissues needed torestore the shape and the volume of the tongue but their functional outcomes, especiallyin case of total mobile tongue reconstruction, are still limited. The authors describe a modi-fication of flap design called the ‘cathedral triptych’ used with the antero-lateral thigh flap.This modified design recreates a near normal neotongue shape with more projected tip andvertical bulk that can contact the palate and the upper lip. Ten patients underwent totalmobile tongue reconstruction with a sensitive antero-lateral thigh flap and a ‘cathedraltriptych’ design. This modification of flap shaping and folding optimises postoperative oralfunction.ª 2011 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Because the tongue is one of the most specialised organs,the reconstructive surgeon can only count on inadequatesubstitutes to recreate large tongue defects. This leads toimperfect functional results when the latest represents the
) 1 42 11 46 03; fax: þ33 (0) 1
[email protected], nicolas.leymarie@
tishAssociationofPlastic,Reconstruc
main goal of any tongue reconstruction. This is the reasonwhy ‘humility’ guides every reconstruction and instead oflooking for hypothetical total tongue restoration, the firstgoal of the reconstructive surgeon is to preserve and sustainthe functions of the remaining tongue.
Guidelines for tongue reconstruction as well as tech-niques to respect them have been previously presented.Tongue defects can be classified in groups of defects, andwe commonly use the one proposed by Urken.1 Humilitydemands no reconstruction for small defects to leave the
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

e170 N. Leymarie et al.
remaining function intact, when results obtained for totalto near total defects are deceiving as no perfect replace-ment tissues are available. Free flaps provided promisingsolutions for middle-size defects1e4 interesting the mobiletongue as classical loco-regional flaps, such as the pector-alis major or latissimus dorsi, were far from being idealsolutions where thin and pliable tissues were needed.Problems presented by the group of ‘half mobile tongue’defects were advantageously addressed by the forearmfree flap using the well-known ‘bilobated design’ proposedby Urken.5,6 This technique still remains today the classicalsolution for this type of defect. The group defined by totalmobile tongue defect which is obtained by transverseresection of this organ and usually includes the entire floorof the mouth has, in our experience, the second worstfunctional result after the total tongue defect group. Theseresults were deceiving and contradictory as we could relyon the remaining function of the tongue base. Humilitydemands the reconstructive surgeon to sustain thisremaining function by bringing a light and pliable tissue,which can be mobilised and brought forward by the muscleof the tongue base. Other accessory reconstructive goalshave to be addressed. Stable and sufficient volume isnecessary to allow lip, dental and palatal contact. Thetethering effect7 has to be avoided by recreating the floorof the mouth fold, which allows forward propulsion of theneomobile tongue and dental rehabilitation. However, ithas to stay limited to avoid the pooling effect.7 Our firsttechnique of reconstruction extended the indications of theforearm free flap or alternatively used the latissimus dorsiwhen the resection interested part of the tongue base orwhen the patient was thin. The design of our flap wasinspired from Haughey.4 The analysis of our results led us topoint out that two major drawbacks were responsible forthe poor functional outcomes in this group. The firstproblem came from the volume of our flaps. The radialforearm flap often does not provide enough tissues and thelatissimus dorsi muscle leads to unstable results as it shrinksmore than 70% especially after radiotherapy. The seconddisadvantage was related with the flap design inspired byHaughey,4 which did not allow for adequate folding of theskin paddle to obtain proper volume and projection of theneomobile tongue.
These problems were addressed by changing both theflap and its pre-established design. The antero-lateral thighflap (ALT) was selected and a new pre-established drawing,named the ‘cathedral triptych’, was designed. We presenthere these modifications.
Table 1 Free flap reconstruction of the tongue from 1992 to 2
Oral defecta Antero-lateralThigh Flap
RadFla
TM nf (n Z 33) 22 7TM 1/2 (n Z 49) 24 23TB 1/2 � TM 1/2 (n Z 37) 9 19TB 3/4 (n Z 24)TG (n Z 9)a Oral defects are described using Urken’s classification: total mobi
tongue base and half of the mobile tongue (TB 1/2 þ TM 1/2), subto
Patients and methods
Since 1998, we have reconstructed 152 tongue resections byusing a free flap. Table 1 presents the type of resection bygroup of defect and the type of free flap used. Total mobiletongue resection represents a small group of 33 patients.From this one, we reviewed the charts of the 10 patientswhich were reconstructed by an ALT flap with the ‘cathedraltriptych’ design. Between February 2008 and June 2011, 10patients (seven men and three women) underwent totalmobile tongue reconstruction with a sensate ALT flap. Theaverage age was 54.4 years. All patients had a squamous cellcarcinoma of the mobile tongue (or ‘oral tongue’) and theextension of the lesion has indicated at least a glossectomyof the total mobile tongue. The medical charts werereviewed retrospectively for information regarding patientscharacteristics, size of the oral defect (using Urken’s clas-sification1), flap dimension, number and type of perforators(using Nakajima’s classification8), operative time, ischaemiatime, vessels used for the anastomosis, method of thigh’sclosure, postoperative course and complications. Swallow-ing and speech intelligibility were assessed postoperatively.The ALT flap sensitivity has been evaluated with qualitativeand quantitative standardised tests: SemmeseWeinsteinmonofilament of 10 g for proprioceptive sensitivity assess-ment (Touch-Test� Sensory Evaluator Size 5.07, BiomedixI.T.&M.), thermal ‘heat-cold sensation’ test for protopathicsensitivity and two-point static discriminatory test forepicritic sensitivity.
Flap design
The ‘cathedral triptych’ design is as follows (Figure 1): thewidth of the flap is standardised. The length of the flapvaries according to the resection of the mobile tongue butis around 7e8 cm. The central part of the triptych makesthe dorsum of the mobile tongue; the two lateral panels arefolded underneath to create its ventral side. Two additionalskin sleeves recreate the floor of the mouth. This flapdesign recreates a near normal neotongue shape with moreprojected tip and vertical bulk that can contact the palateand the upper lip.
Surgical technique
No perforator mapping is used preoperatively. A longmedial incision of the thigh identifies all the perforators
011.
ial Forearmp
LatissimusDorsi Flap
Rectus AbdominisFlap
427 2
17 73 6
le tongue (TM nf), half of the mobile tongue (TM 1/2), half of thetal glossectomy (TB 3/4), total glossectomy (TG).

Figure 1 Flap design for total mobile tongue reconstruction:the “cathedral triptych” design: the central part recreates thedorsal side of the mobile tongue (TM d), the two lateral panelsrebuild the ventral side of the mobile tongue (TM v), points Aare sutured together to form the tip of the tongue, two lateraladditional skin sleeves recreate the floor of the mouth (FOM).
Modification of flap design for total mobile tongue reconstruction e171
emerging from the descending and transverse branches ofthe lateral circumflex femoral pedicle. The pre-establisheddesign is then centred over the best perforator. If possible,more than one is dissected and included in the flap topermit more aggressive folding. Then, the dissectionproceeds as usual. Distal and proximal perforators arerespected to allow advancement flaps for donor site closure(Figure 2, below right).
Figure 2 Intraoperative photographs of a total mobile tongue rectriptych” design. (Above, left) “cathedral triptych” design drawnviews of the flap folded. (Below, right) Distal and proximal perforclosure.
A sensitive branch from the lateral femoral cutaneousnerve is included in the flap to allow the resensitisation ofthe neotongue by the lingual nerve. The flap is harvestedand shaped at the thigh site (Figure 2, above right andbelow left). Depending on the patient’s morphology, theflap can be thinned or ultra-thinned to adjust the flapvolume to the surgical resection.9,10
The flap is then transferred to the oral cavity defect,sutured into place before the microanastomosis is per-formed. This decreases the overall operative time.
Results
The tongue resection involved not less than a total mobiletongue: ‘TM nf’ according to Urken’s classification1 (Table2). In two cases, a partial resection of the tongue basewas also performed: ‘TM nf, TB 1/2’ and ‘TM nf, TB 1/4’. Inthree cases, the carcinologic resection was extended to theanterior floor of the mouth.
The average ALT flap size was 8 � 6 cm. In all cases, theperforators were originated from the descending branchesof the lateral circumflex femoral pedicle. Most of the flaps(six cases) have been harvested with two perforators (Table2). Two flaps had three perforators and most of the perfo-rators (70%) were type D according to Nakajima’s classifi-cation.8 In two obese patients, we had to thin the flap todecrease the volume of the excessive subcutaneous fatlayer. The average operative time was 522 min (range490e680 min) and the average flap’s harvesting time was95 min (range 45e130 min). The vascular microanastomoses
onstruction with an antero-lateral thigh flap and the “cathedralon the thigh. (Above, right) Frontal and (below, left) lateralators are respected to allow advancement flaps for donor site

Table
2Demographic
characteristicsandearlypostoperative
outcomes.
Case
No
Age
/Sex
TNM
Classifica
tion
Oraldefect
aNumberof
perforators
Flap
Resensitisation
Closure
of
thethigh
Flapstatus
Complica
tions
Deca
nnulation
interval(days)
Oralalimetation
interval(days)
134
/MT4a
N1M
0TM
nfþ
FOM
2Yes
Direct
closure
Survived
e8
112
60/M
T4a
N2c
M0
TM
nfþ
FOM
2Yes
Direct
closure
Survived
e8
113
56/F
T3N
0M0
TM
nf
2Yes
Direct
closure
Survived
e14
174
47/F
T3N
0M0
TM
nf
2Yes
Direct
closure
Survived
e7
95
72/M
T3N
0M0
TM
nf
3Yes
Skin
graft
Survived
e7
96
66/M
T4a
N0M
0TM
nfþ
TB1/
41
Yes
Adva
nce
mentflap
Survived
e10
157
35/M
T4a
N2b
M0
TM
nfþ
TB1/
21
Yes
Skin
graft
Survived
e7
98
62/F
T4a
N2C
M0
TM
nfþ
FOM
3Yes
Direct
closure
Survived
Saliva
ryfistula
79
943
/MT4a
N1M
0TM
nf
2Yes
Skin
graft
Survived
e8
1110
69/M
T4a
N0M
0TM
nf
2Yes
Adva
nce
mentflap
Survived
e12
15aOraldefectsare
describedusingUrken’sclassifica
tion1:totalmobiletongu
e(TMnf),base
ofthetongu
e(TB),floorofthemouth
(FOM).
e172 N. Leymarie et al.
were performed on cervical vessels: the lateral circumflexfemoral artery was anastomosed with the facial artery(four cases), the lingual artery (three cases), the superiorthyroid artery (two cases) and the external carotid (onecase); the lateral circumflex femoral vein was anasto-mosed with the thyro-linguo-facial trunk (eight cases), theexternal jugular vein (one case) and the internal jugularvein (one case). The average time of flap ischaemia was40 min (range 25e50 min).
The donor site defect was closed primarily in fivepatients, with two advancement perforator flaps intwo cases, and left for secondary healing in threecases.
Postoperative course was uneventful except for onesurgical revision due to a salivary fistula (Table 2). All flapssurvived and we do not report any flap revision. The meanhospital stay was 18.7 days and the mean decannulationinterval was 8.8 days. All patients returned to oral dietwith solid food (Table 3). In one case, mixed diet wasnecessary. No patient required a gastrostomy. Speechintelligibility was assessed as ‘always understable’ in fourcases, ‘needing repetition’ in four cases and ‘difficult tounderstand’ in two cases where the tongue base waspartially resected. Most of the patients recovered a sensi-tivity of the neotongue (seven cases). In one case, therecovery of sensation was limited to proprioceptive andepicritic sensitivity. For the last two cases, the lack ofsensitivity is related to a short postoperative outcome(less than 3 months).
All flaps kept a normal tongue shape and volume, evenafter radiotherapy, permitting a satisfactory dental andpalatal contact (Figure 3 and see Video, SupplementalDigital Content 1, demonstrating the neotongue mobility).This had a direct effect on the quality of speech anddeglutition of our patients.
Supplementary data related to this article can be foundonline at doi:10.1016/j.bjps.2011.11.012.
Discussion
Total mobile tongue defects are responsible for severefunctional sequelae. Our previous functional results werenot satisfactory. Trading our former technique for the ALTflap tailored with an original design, the ‘cathedral trip-tych’, allowed improving our reconstruction outcome.
The ALT flap is today a workhorse technique in headand neck reconstruction,11 and some consider it to be thebest flap available.12 While we have not eliminated allother free flap from our practice, we found that the ALTflap presents interesting qualities especially for tonguereconstruction. Its location facilitates a two-teamapproach. It provides more volume than the radial fore-arm flap, especially in occidental patients and, unlikemusculocutaneous flap, remains stable even after radio-therapy. We recommend it for medium to large tonguedefects.
The ‘cathedral triptych’ design restores a near normalmobile tongue shape and volume which increase thecontact of the neotongue with the palate, cheek andteeth. This has direct consequence on elocution and ondeglutition with a better processing of the food bolus and
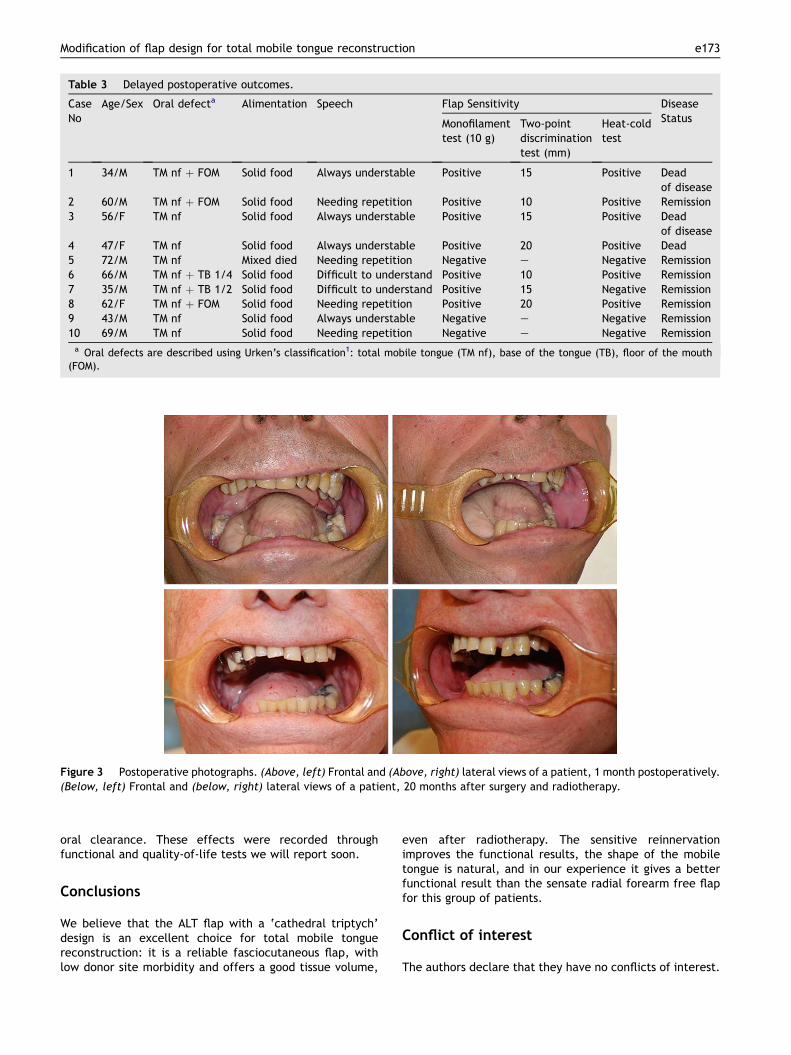
Table 3 Delayed postoperative outcomes.
CaseNo
Age/Sex Oral defecta Alimentation Speech Flap Sensitivity DiseaseStatusMonofilament
test (10 g)Two-pointdiscriminationtest (mm)
Heat-coldtest
1 34/M TM nf þ FOM Solid food Always understable Positive 15 Positive Deadof disease
2 60/M TM nf þ FOM Solid food Needing repetition Positive 10 Positive Remission3 56/F TM nf Solid food Always understable Positive 15 Positive Dead
of disease4 47/F TM nf Solid food Always understable Positive 20 Positive Dead5 72/M TM nf Mixed died Needing repetition Negative e Negative Remission6 66/M TM nf þ TB 1/4 Solid food Difficult to understand Positive 10 Positive Remission7 35/M TM nf þ TB 1/2 Solid food Difficult to understand Positive 15 Negative Remission8 62/F TM nf þ FOM Solid food Needing repetition Positive 20 Positive Remission9 43/M TM nf Solid food Always understable Negative e Negative Remission10 69/M TM nf Solid food Needing repetition Negative e Negative Remissiona Oral defects are described using Urken’s classification1: total mobile tongue (TM nf), base of the tongue (TB), floor of the mouth
(FOM).
Figure 3 Postoperative photographs. (Above, left) Frontal and (Above, right) lateral views of a patient, 1 month postoperatively.(Below, left) Frontal and (below, right) lateral views of a patient, 20 months after surgery and radiotherapy.
Modification of flap design for total mobile tongue reconstruction e173
oral clearance. These effects were recorded throughfunctional and quality-of-life tests we will report soon.
Conclusions
We believe that the ALT flap with a ‘cathedral triptych’design is an excellent choice for total mobile tonguereconstruction: it is a reliable fasciocutaneous flap, withlow donor site morbidity and offers a good tissue volume,
even after radiotherapy. The sensitive reinnervationimproves the functional results, the shape of the mobiletongue is natural, and in our experience it gives a betterfunctional result than the sensate radial forearm free flapfor this group of patients.
Conflict of interest
The authors declare that they have no conflicts of interest.

e174 N. Leymarie et al.
Funding
None.
Acknowledgments
The authors thank doctors Francois Janot and StephaneTemam, surgeons of the Department of Head and NeckOncology of Institut Gustave Roussy, for their support andadvice in this study.
References
1. Urken ML, Moscoso JF, Lawson W, Biller HF. A systematicapproach to functional reconstruction of the oral cavityfollowing partial and total glossectomy. Arch Otolaryngol HeadNeck Surg 1994;120:589e601.
2. Soutar DS, Scheker LR, Tanner NS, McGregor IA. The radialforearm flap: a versatile method for intra-oral reconstruction.Br J Plast Surg 1983;36:1e8.
3. Salibian AH, Allison GR, Armstrong WB, et al. Functionalhemitongue reconstruction with the microvascular ulnar fore-arm flap. Plast Reconstr Surg 1999;104:654e60.
4. Haughey BH. Tongue reconstruction: concepts and practice.Laryngoscope 1993;103:1132e41.
5. Urken ML, Biller HF. A new bilobed design for the sensate radialforearm flap to preserve tongue mobility following significantglossectomy. Arch Otolaryngol Head Neck Surg 1994;120:26e31.
6. Haughey BH, Taylor SM, Fuller D. Fasciocutaneous flap recon-struction of the tongue and floor of mouth: outcomes andtechniques. Arch Otolaryngol Head Neck Surg 2002;128:1388e95.
7. Sultan MR, Coleman 3rd JJ. Oncologic and functional consid-erations of total glossectomy. Am J Surg 1989;158:297e302.
8. Nakajima H, Fujino T, Adachi S. A new concept of vascularsupply to the skin and classification of skin flaps according totheir vascularization. Ann Plast Surg 1986;16:1e19.
9. Koshima I, Fukuda H, Yamamoto H, Moriguchi T, Soeda S,Ohta S. Free anterolateral thigh flaps for reconstruction ofhead and neck defects. Plast Reconstr Surg 1993;92:421e8.discussion 9e30.
10. Kimura N, Satoh K. Consideration of a thin flap as an entity andclinical applications of the thin anterolateral thigh flap. PlastReconstr Surg 1996;97:985e92.
11. Chana JS, Wei FC. A review of the advantages of the antero-lateral thigh flap in head and neck reconstruction. Br J PlastSurg 2004;57:603e9.
12. Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH. Have wefound an ideal soft-tissue flap? An experience with 672 ante-rolateral thigh flaps. Plast Reconstr Surg 2002;109:2219e26.discussion 27e30.





























