Embed Size (px)
DESCRIPTION
Vol.13 No.10 | The Triple Aim:A prescription for health care-John Finnegan, PhD | Neuropathy-Steven Stein, MD | A lifelong guide to exercise-Mike Dixey, PT | Organ, eye & tissue donation-Susan Gunderson & William Payne, MD | What is eczema? A focus on allergic reactions-Charles Crutchfield, MD | Dietary supplements: A look at an unregulated industry-Marsha Millonig, MBA,BPharm | Hysterectomy: Alternative surgical approaches-Jon Nielsen, MD,FACOG | Indoor mold: Risks and remediation-Kelly Smeltzer, MPH | Neck & head cancer: Detection & treatment-Deepak Kademani, DMD,MD,FACS | Male osteoporosis: Preventing fractures as we age-Catherine Niewoehner, MD
Citation preview

October 2015 bull Volume 13 Number 10
Lifelong exerciseMike Dixey PT
Organ donationBy Susan Gunderson and William Payne MD
Male osteoporosisBy Catherine B Niewoehner MD
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
2 Minnesota HealtH care news OctOber 2015
OctOber 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 PhysICaL FITNess a lifelong guide to exercise
By Mike Dixey PT DPT Cert MDT PES CSCS
14 COmmUNITy heaLTh Organ eye and tissue donation
By Susan Gunderson and William Payne MD
16 DeRmaTOLOgy what is eczema
By Charles E Crutchfield III MD
18 CaLeNDaR
20 Take CaRe Dietary supplementsmdashread the label
By Marsha K Millonig MBA BPharm
22 wOmeNrsquos heaLTh hysterectomy
By Jon Nielsen MD FACOG
24 eNVIRONmeNTaL heaLTh
Issues with indoor mold
By Kelly Smeltzer MPH
26 ONCOLOgy Cancers of the neck and head
By Deepak Kademani DMD MD FACS
30 meNrsquos heaLTh male osteoporosis
By Catherine B Niewoehner MD
OctOber 2015 bull VOlume 13 Number 10
John R Finnegan Jr PhD
University of Minnesota School of Public Health
Steven D Stein MD
Minneapolis Clinic of Neurology
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
N e ws
PrairieCare to Leave MedicaOptum NetworkPrairieCare has announced that it will not be an in-network provider with MedicaOptum for hospital-based psychiatric services as of October 20
ldquoPrairieCare leadership believes that MedicaOptum has burdened members and clinicians with un-reasonable barriers to accessingreceiving care and has made no meaningful efforts to resolve sub-stantive concerns raised regard ing unreasonable utilization manage-ment policiesrdquo according to a PrairieCare statement
The organization claims that re-viewers with MedicaOptum pushed for patients to be discharged sooner than their treating psychologists deemed medically appropriate
ldquoAlthough about 20 percent of our patients have MedicaOptum in-surance our utilization review staff
spends more than 80 percent of their time struggling with MedicaOptum utilization management staff fight-ing to get authorization for critical psychiatric carerdquo said Joel Oberstar MD PrairieCare CEO ldquoIn our opinion their utilization manage-ment approach is well outside the community standard and creates a real barrier to carerdquo
PrairieCare is sending notices to current and recent patients with Medica Optum insurance letting them know their plans will no longer cover services at PrairieCare starting October 20 and that while they will still be able to receive care at PrairieCare costs to them will likely be higher
Minnesotarsquos Uninsured Rate Dropped in 2014Minnesotarsquos uninsured rate fell 28 percent from 2013 to 2014 accord-ing to data recently released from
the US Census Bureau The unin-sured rate was 82 percent in 2013 and 59 percent in 2014 meaning 123000 people who were previously uninsured gained health insurance in one year
Minnesota had the fifth-lowest uninsured rate and was one of only six states to reduce its rate to about 7 percent or less along with Mas-sachusetts Vermont Hawaii Iowa and Connecticut
ldquoThis dramatic drop in the num-ber of Minnesotans without health insurance is an indisputable success of MNsure and the Affordable Care Actrdquo Gov Mark Dayton said in a statement ldquoIt means better more affordable health care for them and their families and lower indirect health care costs for everyone elserdquo
About 317000 Minnesotans still donrsquot have health insurance ac-cording to the data Uninsured rates varied widely among different pop-ulationsmdashthe uninsured rate was 15 percent among black Minnesotans
23 percent among American Indians and 29 percent among Hispanics
Minnesotarsquos decrease in unin-sured rates reflects a nationwide trend There were decreases in rates across all 50 states and the District of Columbia Overall the US uninsured rate fell 29 percentage points from 133 percent in 2013 to 104 percent in 2014 meaning 33 million Americans did not have health insurance Massachusetts had the lowest rate of uninsured in 2014 (33 percent) followed by Vermont (5 percent) and Hawaii and the District of Columbia (both at 53 percent) Texas had the highest uninsured rate (191 percent) closely followed by Alaska (172 percent) and Florida (166 percent) Kentucky showed the greatest improvement decreasing its uninsured population by 41 percent from 2013 to 2014
The data shows that states that elected to expand Medicaid andor developed their own health insur-ance marketplaces had the greatest decreases in uninsured
4 MINNESOTA HEAlTH CArE NEwS OctOber 2015
MDH Investigating Impact of Medications in WaterThe Minnesota Department of Health (MDH) has determined screening values for 119 of the most commonly prescribed medications in order to better evaluate potential health concerns for humans from pharmaceuticals in Minnesota waters
Traces of a variety of pharma-ceuticals have been found in Minne-sotarsquos wastewater lakes rivers and groundwater according to MDH This has caused concern about the health of aquatic life In addition some of this water may be used as a source for drinking water which has also caused concern about the pharmaceuticalsrsquo effect on humans
The first step in evaluating potential human health impacts is to determine the level of each phar-maceutical in drinking water that poses no expected risk according to MDH The values can be monitored to determine which pharmaceuticals need to be evaluated more closely as well as to help prioritize future mon-itoring and risk assessment efforts They can also help determine needs for improved laboratory techniques
ldquoIt is important that we know more about the presence of phar-maceuticals in waterrdquo said Pam Shubat supervisor of the Contami-nants of Emerging Concern Pro-gram at MDH ldquoPharmaceuticals are designed to affect the health of people and may harm aquatic life This work will aid in understand-ing which pharmaceuticals may be of greater or lesser concern to Minnesotansrdquo
According to MDH only a portion of the pharmaceuticals they developed screening values for have been found in Minnesota waters And they havenrsquot been detected yet in the water from public water systems They hope the newly determined screening values will help keep the pharmaceutical levels below health concerns
The Minnesota Pollution Con-trol Agency (MPCA) conducts some of the surface and groundwater testing and is working with MDH to evaluate the potential impact of pharmaceuticals and other contami-nants on aquatic life
ldquoGiven the number of pharma-ceuticals being detected in Minne-sotarsquos surface and groundwater it is very helpful for MPCA and others to have some context with which to review the monitoring results wersquove gottenrdquo said Katrina Kessler water assessment section manager at MPCA ldquoThis information will help advance the MPCArsquos work to protect Minnesotarsquos environmentrdquo
Essentia Health Allows Patients to See Caregiver NotesEssentia Health has announced that as of July 1 it began allowing patients who have access to their medical records through MyHealth to also access notes made by their caregivers during clinical appoint-ments and urgent care visits
ldquoresearch shows that patients value this type of transparency and partnership with their healthcare teamrdquo said Tom wiig MD chief medical information officer at Essen-tia Health ldquoItrsquos in the best interest of our patientsrsquo health to make this in-formation easily accessible to themrdquo
To access the information patients or caregivers with My-Health accounts may log in and click ldquoVisit Notesrdquo This allows them to revisit what was covered at each visit and better understand their health and medical condition according to Essentia Health It can also improve communication and patient education
Blue Cross Partnering to Offer Dental PlansBlue Cross and Blue Shield of Min-nesota has announced an agreement with Pennsylvania-based United Concordia Dental to offer dental products to Minnesotans in 2016
The new dental portfolio is called Blue Cross Dental and will include a variety of products to individuals and businesses Details for 2016 coverage options will be re-leased later this fall after regulatory review and approval by the Minne-sota Department of Commerce
News to page 6 OctOber 2015 MINNESOTA HEAlTH CArE NEwS 5
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
2 Minnesota HealtH care news OctOber 2015
OctOber 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 PhysICaL FITNess a lifelong guide to exercise
By Mike Dixey PT DPT Cert MDT PES CSCS
14 COmmUNITy heaLTh Organ eye and tissue donation
By Susan Gunderson and William Payne MD
16 DeRmaTOLOgy what is eczema
By Charles E Crutchfield III MD
18 CaLeNDaR
20 Take CaRe Dietary supplementsmdashread the label
By Marsha K Millonig MBA BPharm
22 wOmeNrsquos heaLTh hysterectomy
By Jon Nielsen MD FACOG
24 eNVIRONmeNTaL heaLTh
Issues with indoor mold
By Kelly Smeltzer MPH
26 ONCOLOgy Cancers of the neck and head
By Deepak Kademani DMD MD FACS
30 meNrsquos heaLTh male osteoporosis
By Catherine B Niewoehner MD
OctOber 2015 bull VOlume 13 Number 10
John R Finnegan Jr PhD
University of Minnesota School of Public Health
Steven D Stein MD
Minneapolis Clinic of Neurology
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
N e ws
PrairieCare to Leave MedicaOptum NetworkPrairieCare has announced that it will not be an in-network provider with MedicaOptum for hospital-based psychiatric services as of October 20
ldquoPrairieCare leadership believes that MedicaOptum has burdened members and clinicians with un-reasonable barriers to accessingreceiving care and has made no meaningful efforts to resolve sub-stantive concerns raised regard ing unreasonable utilization manage-ment policiesrdquo according to a PrairieCare statement
The organization claims that re-viewers with MedicaOptum pushed for patients to be discharged sooner than their treating psychologists deemed medically appropriate
ldquoAlthough about 20 percent of our patients have MedicaOptum in-surance our utilization review staff
spends more than 80 percent of their time struggling with MedicaOptum utilization management staff fight-ing to get authorization for critical psychiatric carerdquo said Joel Oberstar MD PrairieCare CEO ldquoIn our opinion their utilization manage-ment approach is well outside the community standard and creates a real barrier to carerdquo
PrairieCare is sending notices to current and recent patients with Medica Optum insurance letting them know their plans will no longer cover services at PrairieCare starting October 20 and that while they will still be able to receive care at PrairieCare costs to them will likely be higher
Minnesotarsquos Uninsured Rate Dropped in 2014Minnesotarsquos uninsured rate fell 28 percent from 2013 to 2014 accord-ing to data recently released from
the US Census Bureau The unin-sured rate was 82 percent in 2013 and 59 percent in 2014 meaning 123000 people who were previously uninsured gained health insurance in one year
Minnesota had the fifth-lowest uninsured rate and was one of only six states to reduce its rate to about 7 percent or less along with Mas-sachusetts Vermont Hawaii Iowa and Connecticut
ldquoThis dramatic drop in the num-ber of Minnesotans without health insurance is an indisputable success of MNsure and the Affordable Care Actrdquo Gov Mark Dayton said in a statement ldquoIt means better more affordable health care for them and their families and lower indirect health care costs for everyone elserdquo
About 317000 Minnesotans still donrsquot have health insurance ac-cording to the data Uninsured rates varied widely among different pop-ulationsmdashthe uninsured rate was 15 percent among black Minnesotans
23 percent among American Indians and 29 percent among Hispanics
Minnesotarsquos decrease in unin-sured rates reflects a nationwide trend There were decreases in rates across all 50 states and the District of Columbia Overall the US uninsured rate fell 29 percentage points from 133 percent in 2013 to 104 percent in 2014 meaning 33 million Americans did not have health insurance Massachusetts had the lowest rate of uninsured in 2014 (33 percent) followed by Vermont (5 percent) and Hawaii and the District of Columbia (both at 53 percent) Texas had the highest uninsured rate (191 percent) closely followed by Alaska (172 percent) and Florida (166 percent) Kentucky showed the greatest improvement decreasing its uninsured population by 41 percent from 2013 to 2014
The data shows that states that elected to expand Medicaid andor developed their own health insur-ance marketplaces had the greatest decreases in uninsured
4 MINNESOTA HEAlTH CArE NEwS OctOber 2015
MDH Investigating Impact of Medications in WaterThe Minnesota Department of Health (MDH) has determined screening values for 119 of the most commonly prescribed medications in order to better evaluate potential health concerns for humans from pharmaceuticals in Minnesota waters
Traces of a variety of pharma-ceuticals have been found in Minne-sotarsquos wastewater lakes rivers and groundwater according to MDH This has caused concern about the health of aquatic life In addition some of this water may be used as a source for drinking water which has also caused concern about the pharmaceuticalsrsquo effect on humans
The first step in evaluating potential human health impacts is to determine the level of each phar-maceutical in drinking water that poses no expected risk according to MDH The values can be monitored to determine which pharmaceuticals need to be evaluated more closely as well as to help prioritize future mon-itoring and risk assessment efforts They can also help determine needs for improved laboratory techniques
ldquoIt is important that we know more about the presence of phar-maceuticals in waterrdquo said Pam Shubat supervisor of the Contami-nants of Emerging Concern Pro-gram at MDH ldquoPharmaceuticals are designed to affect the health of people and may harm aquatic life This work will aid in understand-ing which pharmaceuticals may be of greater or lesser concern to Minnesotansrdquo
According to MDH only a portion of the pharmaceuticals they developed screening values for have been found in Minnesota waters And they havenrsquot been detected yet in the water from public water systems They hope the newly determined screening values will help keep the pharmaceutical levels below health concerns
The Minnesota Pollution Con-trol Agency (MPCA) conducts some of the surface and groundwater testing and is working with MDH to evaluate the potential impact of pharmaceuticals and other contami-nants on aquatic life
ldquoGiven the number of pharma-ceuticals being detected in Minne-sotarsquos surface and groundwater it is very helpful for MPCA and others to have some context with which to review the monitoring results wersquove gottenrdquo said Katrina Kessler water assessment section manager at MPCA ldquoThis information will help advance the MPCArsquos work to protect Minnesotarsquos environmentrdquo
Essentia Health Allows Patients to See Caregiver NotesEssentia Health has announced that as of July 1 it began allowing patients who have access to their medical records through MyHealth to also access notes made by their caregivers during clinical appoint-ments and urgent care visits
ldquoresearch shows that patients value this type of transparency and partnership with their healthcare teamrdquo said Tom wiig MD chief medical information officer at Essen-tia Health ldquoItrsquos in the best interest of our patientsrsquo health to make this in-formation easily accessible to themrdquo
To access the information patients or caregivers with My-Health accounts may log in and click ldquoVisit Notesrdquo This allows them to revisit what was covered at each visit and better understand their health and medical condition according to Essentia Health It can also improve communication and patient education
Blue Cross Partnering to Offer Dental PlansBlue Cross and Blue Shield of Min-nesota has announced an agreement with Pennsylvania-based United Concordia Dental to offer dental products to Minnesotans in 2016
The new dental portfolio is called Blue Cross Dental and will include a variety of products to individuals and businesses Details for 2016 coverage options will be re-leased later this fall after regulatory review and approval by the Minne-sota Department of Commerce
News to page 6 OctOber 2015 MINNESOTA HEAlTH CArE NEwS 5
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

OctOber 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 PhysICaL FITNess a lifelong guide to exercise
By Mike Dixey PT DPT Cert MDT PES CSCS
14 COmmUNITy heaLTh Organ eye and tissue donation
By Susan Gunderson and William Payne MD
16 DeRmaTOLOgy what is eczema
By Charles E Crutchfield III MD
18 CaLeNDaR
20 Take CaRe Dietary supplementsmdashread the label
By Marsha K Millonig MBA BPharm
22 wOmeNrsquos heaLTh hysterectomy
By Jon Nielsen MD FACOG
24 eNVIRONmeNTaL heaLTh
Issues with indoor mold
By Kelly Smeltzer MPH
26 ONCOLOgy Cancers of the neck and head
By Deepak Kademani DMD MD FACS
30 meNrsquos heaLTh male osteoporosis
By Catherine B Niewoehner MD
OctOber 2015 bull VOlume 13 Number 10
John R Finnegan Jr PhD
University of Minnesota School of Public Health
Steven D Stein MD
Minneapolis Clinic of Neurology
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
N e ws
PrairieCare to Leave MedicaOptum NetworkPrairieCare has announced that it will not be an in-network provider with MedicaOptum for hospital-based psychiatric services as of October 20
ldquoPrairieCare leadership believes that MedicaOptum has burdened members and clinicians with un-reasonable barriers to accessingreceiving care and has made no meaningful efforts to resolve sub-stantive concerns raised regard ing unreasonable utilization manage-ment policiesrdquo according to a PrairieCare statement
The organization claims that re-viewers with MedicaOptum pushed for patients to be discharged sooner than their treating psychologists deemed medically appropriate
ldquoAlthough about 20 percent of our patients have MedicaOptum in-surance our utilization review staff
spends more than 80 percent of their time struggling with MedicaOptum utilization management staff fight-ing to get authorization for critical psychiatric carerdquo said Joel Oberstar MD PrairieCare CEO ldquoIn our opinion their utilization manage-ment approach is well outside the community standard and creates a real barrier to carerdquo
PrairieCare is sending notices to current and recent patients with Medica Optum insurance letting them know their plans will no longer cover services at PrairieCare starting October 20 and that while they will still be able to receive care at PrairieCare costs to them will likely be higher
Minnesotarsquos Uninsured Rate Dropped in 2014Minnesotarsquos uninsured rate fell 28 percent from 2013 to 2014 accord-ing to data recently released from
the US Census Bureau The unin-sured rate was 82 percent in 2013 and 59 percent in 2014 meaning 123000 people who were previously uninsured gained health insurance in one year
Minnesota had the fifth-lowest uninsured rate and was one of only six states to reduce its rate to about 7 percent or less along with Mas-sachusetts Vermont Hawaii Iowa and Connecticut
ldquoThis dramatic drop in the num-ber of Minnesotans without health insurance is an indisputable success of MNsure and the Affordable Care Actrdquo Gov Mark Dayton said in a statement ldquoIt means better more affordable health care for them and their families and lower indirect health care costs for everyone elserdquo
About 317000 Minnesotans still donrsquot have health insurance ac-cording to the data Uninsured rates varied widely among different pop-ulationsmdashthe uninsured rate was 15 percent among black Minnesotans
23 percent among American Indians and 29 percent among Hispanics
Minnesotarsquos decrease in unin-sured rates reflects a nationwide trend There were decreases in rates across all 50 states and the District of Columbia Overall the US uninsured rate fell 29 percentage points from 133 percent in 2013 to 104 percent in 2014 meaning 33 million Americans did not have health insurance Massachusetts had the lowest rate of uninsured in 2014 (33 percent) followed by Vermont (5 percent) and Hawaii and the District of Columbia (both at 53 percent) Texas had the highest uninsured rate (191 percent) closely followed by Alaska (172 percent) and Florida (166 percent) Kentucky showed the greatest improvement decreasing its uninsured population by 41 percent from 2013 to 2014
The data shows that states that elected to expand Medicaid andor developed their own health insur-ance marketplaces had the greatest decreases in uninsured
4 MINNESOTA HEAlTH CArE NEwS OctOber 2015
MDH Investigating Impact of Medications in WaterThe Minnesota Department of Health (MDH) has determined screening values for 119 of the most commonly prescribed medications in order to better evaluate potential health concerns for humans from pharmaceuticals in Minnesota waters
Traces of a variety of pharma-ceuticals have been found in Minne-sotarsquos wastewater lakes rivers and groundwater according to MDH This has caused concern about the health of aquatic life In addition some of this water may be used as a source for drinking water which has also caused concern about the pharmaceuticalsrsquo effect on humans
The first step in evaluating potential human health impacts is to determine the level of each phar-maceutical in drinking water that poses no expected risk according to MDH The values can be monitored to determine which pharmaceuticals need to be evaluated more closely as well as to help prioritize future mon-itoring and risk assessment efforts They can also help determine needs for improved laboratory techniques
ldquoIt is important that we know more about the presence of phar-maceuticals in waterrdquo said Pam Shubat supervisor of the Contami-nants of Emerging Concern Pro-gram at MDH ldquoPharmaceuticals are designed to affect the health of people and may harm aquatic life This work will aid in understand-ing which pharmaceuticals may be of greater or lesser concern to Minnesotansrdquo
According to MDH only a portion of the pharmaceuticals they developed screening values for have been found in Minnesota waters And they havenrsquot been detected yet in the water from public water systems They hope the newly determined screening values will help keep the pharmaceutical levels below health concerns
The Minnesota Pollution Con-trol Agency (MPCA) conducts some of the surface and groundwater testing and is working with MDH to evaluate the potential impact of pharmaceuticals and other contami-nants on aquatic life
ldquoGiven the number of pharma-ceuticals being detected in Minne-sotarsquos surface and groundwater it is very helpful for MPCA and others to have some context with which to review the monitoring results wersquove gottenrdquo said Katrina Kessler water assessment section manager at MPCA ldquoThis information will help advance the MPCArsquos work to protect Minnesotarsquos environmentrdquo
Essentia Health Allows Patients to See Caregiver NotesEssentia Health has announced that as of July 1 it began allowing patients who have access to their medical records through MyHealth to also access notes made by their caregivers during clinical appoint-ments and urgent care visits
ldquoresearch shows that patients value this type of transparency and partnership with their healthcare teamrdquo said Tom wiig MD chief medical information officer at Essen-tia Health ldquoItrsquos in the best interest of our patientsrsquo health to make this in-formation easily accessible to themrdquo
To access the information patients or caregivers with My-Health accounts may log in and click ldquoVisit Notesrdquo This allows them to revisit what was covered at each visit and better understand their health and medical condition according to Essentia Health It can also improve communication and patient education
Blue Cross Partnering to Offer Dental PlansBlue Cross and Blue Shield of Min-nesota has announced an agreement with Pennsylvania-based United Concordia Dental to offer dental products to Minnesotans in 2016
The new dental portfolio is called Blue Cross Dental and will include a variety of products to individuals and businesses Details for 2016 coverage options will be re-leased later this fall after regulatory review and approval by the Minne-sota Department of Commerce
News to page 6 OctOber 2015 MINNESOTA HEAlTH CArE NEwS 5
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

N e ws
PrairieCare to Leave MedicaOptum NetworkPrairieCare has announced that it will not be an in-network provider with MedicaOptum for hospital-based psychiatric services as of October 20
ldquoPrairieCare leadership believes that MedicaOptum has burdened members and clinicians with un-reasonable barriers to accessingreceiving care and has made no meaningful efforts to resolve sub-stantive concerns raised regard ing unreasonable utilization manage-ment policiesrdquo according to a PrairieCare statement
The organization claims that re-viewers with MedicaOptum pushed for patients to be discharged sooner than their treating psychologists deemed medically appropriate
ldquoAlthough about 20 percent of our patients have MedicaOptum in-surance our utilization review staff
spends more than 80 percent of their time struggling with MedicaOptum utilization management staff fight-ing to get authorization for critical psychiatric carerdquo said Joel Oberstar MD PrairieCare CEO ldquoIn our opinion their utilization manage-ment approach is well outside the community standard and creates a real barrier to carerdquo
PrairieCare is sending notices to current and recent patients with Medica Optum insurance letting them know their plans will no longer cover services at PrairieCare starting October 20 and that while they will still be able to receive care at PrairieCare costs to them will likely be higher
Minnesotarsquos Uninsured Rate Dropped in 2014Minnesotarsquos uninsured rate fell 28 percent from 2013 to 2014 accord-ing to data recently released from
the US Census Bureau The unin-sured rate was 82 percent in 2013 and 59 percent in 2014 meaning 123000 people who were previously uninsured gained health insurance in one year
Minnesota had the fifth-lowest uninsured rate and was one of only six states to reduce its rate to about 7 percent or less along with Mas-sachusetts Vermont Hawaii Iowa and Connecticut
ldquoThis dramatic drop in the num-ber of Minnesotans without health insurance is an indisputable success of MNsure and the Affordable Care Actrdquo Gov Mark Dayton said in a statement ldquoIt means better more affordable health care for them and their families and lower indirect health care costs for everyone elserdquo
About 317000 Minnesotans still donrsquot have health insurance ac-cording to the data Uninsured rates varied widely among different pop-ulationsmdashthe uninsured rate was 15 percent among black Minnesotans
23 percent among American Indians and 29 percent among Hispanics
Minnesotarsquos decrease in unin-sured rates reflects a nationwide trend There were decreases in rates across all 50 states and the District of Columbia Overall the US uninsured rate fell 29 percentage points from 133 percent in 2013 to 104 percent in 2014 meaning 33 million Americans did not have health insurance Massachusetts had the lowest rate of uninsured in 2014 (33 percent) followed by Vermont (5 percent) and Hawaii and the District of Columbia (both at 53 percent) Texas had the highest uninsured rate (191 percent) closely followed by Alaska (172 percent) and Florida (166 percent) Kentucky showed the greatest improvement decreasing its uninsured population by 41 percent from 2013 to 2014
The data shows that states that elected to expand Medicaid andor developed their own health insur-ance marketplaces had the greatest decreases in uninsured
4 MINNESOTA HEAlTH CArE NEwS OctOber 2015
MDH Investigating Impact of Medications in WaterThe Minnesota Department of Health (MDH) has determined screening values for 119 of the most commonly prescribed medications in order to better evaluate potential health concerns for humans from pharmaceuticals in Minnesota waters
Traces of a variety of pharma-ceuticals have been found in Minne-sotarsquos wastewater lakes rivers and groundwater according to MDH This has caused concern about the health of aquatic life In addition some of this water may be used as a source for drinking water which has also caused concern about the pharmaceuticalsrsquo effect on humans
The first step in evaluating potential human health impacts is to determine the level of each phar-maceutical in drinking water that poses no expected risk according to MDH The values can be monitored to determine which pharmaceuticals need to be evaluated more closely as well as to help prioritize future mon-itoring and risk assessment efforts They can also help determine needs for improved laboratory techniques
ldquoIt is important that we know more about the presence of phar-maceuticals in waterrdquo said Pam Shubat supervisor of the Contami-nants of Emerging Concern Pro-gram at MDH ldquoPharmaceuticals are designed to affect the health of people and may harm aquatic life This work will aid in understand-ing which pharmaceuticals may be of greater or lesser concern to Minnesotansrdquo
According to MDH only a portion of the pharmaceuticals they developed screening values for have been found in Minnesota waters And they havenrsquot been detected yet in the water from public water systems They hope the newly determined screening values will help keep the pharmaceutical levels below health concerns
The Minnesota Pollution Con-trol Agency (MPCA) conducts some of the surface and groundwater testing and is working with MDH to evaluate the potential impact of pharmaceuticals and other contami-nants on aquatic life
ldquoGiven the number of pharma-ceuticals being detected in Minne-sotarsquos surface and groundwater it is very helpful for MPCA and others to have some context with which to review the monitoring results wersquove gottenrdquo said Katrina Kessler water assessment section manager at MPCA ldquoThis information will help advance the MPCArsquos work to protect Minnesotarsquos environmentrdquo
Essentia Health Allows Patients to See Caregiver NotesEssentia Health has announced that as of July 1 it began allowing patients who have access to their medical records through MyHealth to also access notes made by their caregivers during clinical appoint-ments and urgent care visits
ldquoresearch shows that patients value this type of transparency and partnership with their healthcare teamrdquo said Tom wiig MD chief medical information officer at Essen-tia Health ldquoItrsquos in the best interest of our patientsrsquo health to make this in-formation easily accessible to themrdquo
To access the information patients or caregivers with My-Health accounts may log in and click ldquoVisit Notesrdquo This allows them to revisit what was covered at each visit and better understand their health and medical condition according to Essentia Health It can also improve communication and patient education
Blue Cross Partnering to Offer Dental PlansBlue Cross and Blue Shield of Min-nesota has announced an agreement with Pennsylvania-based United Concordia Dental to offer dental products to Minnesotans in 2016
The new dental portfolio is called Blue Cross Dental and will include a variety of products to individuals and businesses Details for 2016 coverage options will be re-leased later this fall after regulatory review and approval by the Minne-sota Department of Commerce
News to page 6 OctOber 2015 MINNESOTA HEAlTH CArE NEwS 5
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

MDH Investigating Impact of Medications in WaterThe Minnesota Department of Health (MDH) has determined screening values for 119 of the most commonly prescribed medications in order to better evaluate potential health concerns for humans from pharmaceuticals in Minnesota waters
Traces of a variety of pharma-ceuticals have been found in Minne-sotarsquos wastewater lakes rivers and groundwater according to MDH This has caused concern about the health of aquatic life In addition some of this water may be used as a source for drinking water which has also caused concern about the pharmaceuticalsrsquo effect on humans
The first step in evaluating potential human health impacts is to determine the level of each phar-maceutical in drinking water that poses no expected risk according to MDH The values can be monitored to determine which pharmaceuticals need to be evaluated more closely as well as to help prioritize future mon-itoring and risk assessment efforts They can also help determine needs for improved laboratory techniques
ldquoIt is important that we know more about the presence of phar-maceuticals in waterrdquo said Pam Shubat supervisor of the Contami-nants of Emerging Concern Pro-gram at MDH ldquoPharmaceuticals are designed to affect the health of people and may harm aquatic life This work will aid in understand-ing which pharmaceuticals may be of greater or lesser concern to Minnesotansrdquo
According to MDH only a portion of the pharmaceuticals they developed screening values for have been found in Minnesota waters And they havenrsquot been detected yet in the water from public water systems They hope the newly determined screening values will help keep the pharmaceutical levels below health concerns
The Minnesota Pollution Con-trol Agency (MPCA) conducts some of the surface and groundwater testing and is working with MDH to evaluate the potential impact of pharmaceuticals and other contami-nants on aquatic life
ldquoGiven the number of pharma-ceuticals being detected in Minne-sotarsquos surface and groundwater it is very helpful for MPCA and others to have some context with which to review the monitoring results wersquove gottenrdquo said Katrina Kessler water assessment section manager at MPCA ldquoThis information will help advance the MPCArsquos work to protect Minnesotarsquos environmentrdquo
Essentia Health Allows Patients to See Caregiver NotesEssentia Health has announced that as of July 1 it began allowing patients who have access to their medical records through MyHealth to also access notes made by their caregivers during clinical appoint-ments and urgent care visits
ldquoresearch shows that patients value this type of transparency and partnership with their healthcare teamrdquo said Tom wiig MD chief medical information officer at Essen-tia Health ldquoItrsquos in the best interest of our patientsrsquo health to make this in-formation easily accessible to themrdquo
To access the information patients or caregivers with My-Health accounts may log in and click ldquoVisit Notesrdquo This allows them to revisit what was covered at each visit and better understand their health and medical condition according to Essentia Health It can also improve communication and patient education
Blue Cross Partnering to Offer Dental PlansBlue Cross and Blue Shield of Min-nesota has announced an agreement with Pennsylvania-based United Concordia Dental to offer dental products to Minnesotans in 2016
The new dental portfolio is called Blue Cross Dental and will include a variety of products to individuals and businesses Details for 2016 coverage options will be re-leased later this fall after regulatory review and approval by the Minne-sota Department of Commerce
News to page 6 OctOber 2015 MINNESOTA HEAlTH CArE NEwS 5
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Conference Addresses Prescription Painshykiller ProblemMore than 1000 Minnesota law enforcement officials public health officials health care professionals attorneys drug court representa-tives medical students govern-ment staff and recovering addicts gathered in Minnesota on Aug 25 to discuss the statersquos prescription painkiller problem and develop solutions to address it
The conference called PainPillProblem featured six panels on the topics of the impact of opioid addic-tion prescribing and pain culture pharmacy and distribution law enforcement opioid treatment and recovery prevention and the role of the community Several speakers took the floor including Gov Mark Dayton Minnesota Department of Human Services Commissioner lu-cinda Jesson Sen Amy Klobuchar
rep Tom Emmer US Attorney Andrew luger Hennepin County sheriff rich Stanek former rep Mary Bono University of Minneso-ta President Eric Kaler and others Some recommended developing a system to more closely monitor patients who are using painkillers as well as utilizing alternative pain management techniques such as acupuncture massage exercise and nutrition more often
ldquoNarcotic painkillers are being over-prescribed in Minnesota lead-ing to addiction abuse and serious consequencesrdquo said Jesson ldquoIn the last decade overdose deaths have more than doubled Painkillers now cause more deaths than heroin and cocaine combined we need to have a conversation as a society about how we can treat pain in ways that restores function and this conference is a step in the right directionrdquo
ldquoThis gathering today proves wersquore all in this togetherrdquo said Nick Motu vice president of the Hazelden Betty Ford Institute
for recovery Advocacy ldquowersquove made addressing the opioid crisis a bedrock of the advocacy efforts at our organization and by coming to-gether with others around solutions like we did today we can make real progress against this epidemicrdquo
St Therese and North Memorial Team Up on Transitional CareSaint Therese and North Memorial Medical Center have announced that they are partnering on a program to help transition patients from the hospital to their homes Transitional Care by Saint Therese will open on the fourth floor of North Memorial Medical Center in robbinsdale in spring 2016 and will include about 32 private rooms for patients transitioning from hospital to their homes after illness injury or surgery
Patients will receive care from a team of care professionals including
specialized physicians nurse prac-titioners dieticians and physical occupational and speech therapists
Senior Memory Care Neighborhood to Open in BurnsvilleThe rivers and its managing part-ner Des Moines Iowa-based life Care Services have announced the grand opening of a memory care neighborhood within its senior living community in Burnsville on August 29 The neighborhood called the rivers landing is an alternative to at-home care for people with Alzheimerrsquos and other forms of dementia
The memory care neighborhood is specially designed for adults with progressive cognitive disorders of-fering a memory care program and staff who have undergone training to help residents manage dementia symptoms like sundown syndrome wandering or combativeness
News from page 5
6 MINNESOTA HEAlTH CArE NEwS OctOber 2015
If yoursquore a Baby Boomer age 65 or older itrsquos time to fi nd your groove with Medicare UCare is ready with health plans that are as fl exible and forward-thinking as you are
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOU STILL HAVE ALL THE RIGHT MOVES WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_Hippieindd 1 91415 903 AM
Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Stephanie Krejcarek Childs MD has joined Radiation Oncology at the Maplewood Cancer Cen-ter Childs earned her medical degree at Harvard Medical School completed an internship at Brigham and Womenrsquos Hospital in Boston and completed a residency in the Harvard Radiation Oncology Residency Program Childs was awarded a Ful-bright Fellowship from the Fulbright Foundation of Sweden Previously she was an assistant professor of radiation oncology at the Mayo College School of
Medicine and senior associate consultant in the Mayo Clinic Depart-ment of Radiation Oncology
Amy Hammers MD has joined Clinic Sofia an OBGYN clinic with offices in Edina and Ma-ple Grove Hammers earned her medical degree at Creighton University School of Medicine in Omaha Neb and completed her residency at the Universi-ty of Florida College of Medicine in Jacksonville Fla She is a member of the American Congress of Obstetricians and Gynecologists (ACOG) and the American Medical Association Hammers will see patients primarily in Clinic Sofiarsquos Maple Grove location but will also be available for appointments in Edina one day a week
Peter Polski DC has joined Hennepin County Medical Center (HCMC) in the department of integrative health Polski earned his doctorate of chiropractic from Northwestern Health Sciences University In addition to his chiropractic education Polski has pursued additional training in acupunc-ture rehabilitation and neuromuscular retraining In addition to spinal and extrem-
ity complaints Polski treats conditions such as headache disorders TMJ dysfunction Bellrsquos Palsy and mechanical foot problems Laura Schrag MD has also joined HCMC in the department of emergency medicine Schrag earned her medical degree at Chicago Medical School and completed an internship and residency in emergency medicine at HCMC
Jean Wood executive director of the Minnesota Board on Aging and director of the Aging and Adult Services Division at the Minnesota Department of Human Services (DHS) has received the first Execu-tive Directorrsquos Award from the National Association of States United for Aging and Disabilities (NA-SUAD) for her national leadership and commitment to the association She first served as a staff member
then as a long-standing member of the NASUAD Board of Directors Her work helped the association move from serving only state aging agencies to serving state agencies on disabilities and aging
Peo Ple
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 7
Amy Hammers MD
laura Schrag MD
Peter Polski DC
Jean Wood
Stephanie Krejcarek Childs
MD
For directions or additional information about the Minneapolis Clinic of Neurology
Visit us online at wwwminneapoliscliniccom
Exceptional Personalized Neurologic Care
Burnsville 9524358516
Coon Rapids 7634278320
Edina 9529207200
Golden Valley 7635880661
Maple Grove 7633024114
Outreach Clinics throughout MN amp western WI
For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

For more than 30 yearsmdashlong before the 2010 Af-fordable Care Act (ACA)mdashthe US has spent more on health care than any other nation but achieved
less Of the trillions spent on health more than 85 percent has gone to medical services yet other forces including environment genetics and social determi-nants account for some 80 percent of the factors that create and sustain health Investment in prevention and health promotion has been painfully inadequate
The Triple Aim articulated by Donald Berwick former head of the Centers for Medicare and Medicaid Services set a three-part agenda for health reform in 2008 improve population health improve the health care experience and reduce cost
The subsequent journey has been one of enormous uncertainty major change and dysfunctional national politics
The Triple AimAccess Emphasized more than
other Triple Aim components under the ACA access to care has been a roaring success Only Texas has an uninsured rate higher than 20 percent Almost 90 percent of Americans now have health insurance with large but improving disparities among the poor young and minorities Until now the US has historically been among the few developed nations unwilling to provide affordable basic health care
Cost containment There also has been progress on cost New incentives nudge health care from ldquofee- for- servicerdquo to ldquofee-for-performancerdquo for some this means home-based outpatient care not the more costly hospital-based inpatient care The ACA imposes Medicare penalties for patient readmissions within 30 days for conditions such as heart failure Penalties started at 1 percent and are now up to 3 percent In fiscal 2016 more than 75 percent of subject hospitals could be penalized for readmissions within 30 days
There is also some good news regarding increases in health insurance rates States like Minnesota that require pre-approval of rate increases have seen their costs rise 10 percent less than states without such regulation
Population health The ACA mandated some $145 billion be spent over a ten-year period for prevention and for programs to improve health and restrain in-creases in health care costs But that funding has taken some major hits With Congress and the president trading off population health for protecting physician cuts in Medicare payments less than half of the origi-nal amount remained for population strategies in 2015 Nationally wersquore still spending only about 3 percent of health dollars on public health
Health care organizations with hospitals are re-quired by the end of fiscal 2015 to conduct and publish a Community Health Needs Assessment (CHNA) or face an excise tax from the IRS They must follow with a three-year action plan mandating that they focus on everyone in their primary market areas not just their own patients It also drives them toward community organizational and public health partnerships to address the neglected factors that shape community health and wellness
The road in MinnesotaTwo years before the ACA Minnesota passed a
health reform law aspiring to the Triple Aim Long a bellwether for health innovation Minnesota has been more efficient in spending health care dollars and in its focus on public health Driving this in part is the statersquos tra-dition of not-for-profit health care and its Institute for Clinical Systems Improvement (ICSI) and Minnesota Community Measurement both launched by the statersquos major health plans Data and evidence
sharing performance transparency and innovation have been vital to Minnesotarsquos leadership in health
Another vital component has been Minnesotarsquos greater focus and investment in public health The Minnesota Department of Health runs the Statewide Health Improvement Program (SHIP) that makes grants to communities for projects designed to change factors driving preventable illness and foster smarter choices The program has stimulated community partnerships across the state
Nearly all of the statersquos major health care organiza-tions engage with communities in health improvement initiatives For example Allina Community Benefit and Engagement is well known for its Backyard Initiative and New Ulm Heart Health Program
Minnesota may have an advantage in health re-form by history and politics yet all is not rosy Longevi-ty and health outcomes are generally better for whites Disparities in health are among some of the worst in the US for American Indians people of color and all who live in poverty offending our Minnesota values of fairness and equity The health reform solutions that have eluded us so far will require even greater collaboration and partnership We must all contribute to building a culture of health and wellness both rural and urban This crosses public health and health care public and private sectors professional and disciplinary boundaries and all the ways we have siloed ourselves unintentionally and reduced our joint effectiveness It will be a continuing journey not a destination
The Triple AimA prescription for health care
Pe rsPeC T ive
8 Minnesota HealtH care news OctOber 2015
John r Finnegan Jr PhD
University of Minnesota School of Public Health
Dr Finnegan is professor and dean of the University of Minnesota School of Public Health Founded in 1944 the school is ranked among the top five public schools in the US in research learning and community engagement It graduates some 300 students each year serving the public health workforce in Minnesota the US and all over the world
We must all contribute to
building a culture of health and
wellness
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
ldquoIrsquove trusted the health care providers at Essentia Health for yearsrdquoldquoThatrsquos why Irsquom excited about EssentiaCarerdquoIntroducing EssentiaCare a new Medicare plan from UCare and Essentia Health EssentiaCare combines the health care you know and trust from Essentia Health with smart health coverage from UCare Benefits include no or low copays for doctor visits prescription drug coverage dental coverage travel coverage fitness programs and more If yoursquore eligible for Medicaremdashwhether or not yoursquore a current Essentia Health patientmdashfind out about an affordable new choice
Get plan details now for coverage beginning in January 2016 at EssentiaCareorg or call 218-722-4783 1-855-432-7027 toll free or TTY 1-800-688-2534 toll free 8 am to 8 pm daily
Paid Actor Portrayal
Limitations copayments and restrictions may apply This information is not a complete description of benefits Contact the plan for more information Benefits andor copayments may change on January 1 of each year EssentiaCare is a PPO plan with a Medicare contract Enrollment in EssentiaCare depends on contract renewal copy 2015 UCare H0735_091515_2 CMS Accepted (09202015) OctOber 2015 Minnesota HealtH care news 9
10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

10 Questions
What is neuropathy Neuropathy refers to a disturbance in the function of a nerve or multiple nerves It is a broad descriptive term and does not refer to a single specific disease The expression ldquoperipheral neurop-athyrdquo refers to an alteration in the function of the peripheral nerves which typically would start in the feet and then start mov-ing up the legs
What are the classifications of neu-ropathy Neuropathy can be classified in many different ways For example it may be classified as to whether it involves a single nerve or whether groups of nerves are affected It may be classified as to causation if a specific cause can be determined For neurologists it is often helpful to classify based upon which portion of the nerve is primarily affected For example the two prime components of a nerve consist of the central portion known as the axon and an insulating por-tion known as myelin Conditions that affect axon versus myelin can display different types of clinical symptoms and often respond to different treatment regimens
What causes neuropathy There is a very long list of conditions that may cause neuropathy Some neuropathies may be due to a compression of the nerve such as carpal tunnel syndrome where there is a pinched nerve at the wrist Activ-ities that include repetitive use of the hands and wrists may lead to the development of carpal tunnel syndrome Some neuropathies may be related to other medical conditionsmdashdiabetes would be a com-mon example There are some individuals who may develop neuropathy several years before diabetes be-comes manifest Some neuropathies may be related to vitamin deficiencies including vitamin B deficiencies Some neuropathies may be related to infections such as Lyme disease Some neuropathies may be related to inflammation of the nerves Some neuropathies may be related to hereditary conditions Some neuropathies may be
caused by medications including some antibiotics used to treat infections Individuals who receive chemotherapy as part of cancer treatment may develop neuropathy Some neuropathies may be caused as a remote effect of certain cancers Certain ldquotoxinsrdquo may contribute to the devel-
opment of neuropathy This could include the excessive use of alcohol Finally there are a large number of
individuals with neuropathy for whom a specific cause may not be identified
What are the signs and symptoms The typical symptoms of neuropathy may include numbness tingling and pain If nerves that supply muscles are involved weakness can also be a symptom When the nerves in the feet and legs are involved common symptoms can in-clude loss of balance and coordination Sometimes neuropathy can cause very painful symptoms sometimes described as burning or electric-like shocks If neuropathy involves nerves that help control blood pressure symptoms may include lightheadedness upon standing Occasionally certain types of neurop-
athy may also affect bowel and bladder function The signs of neuropathy that a physician may find on examination often
include abnormalities when testing sensation in the arms or legs as well as changes in the deep
tendon reflexes
How do you test for and diagnose neu-ropathy The evaluation always begins with the medical history looking for clues of possible exposure history medications other medical con-ditions or hereditary factors that may be relevant The findings on physical examination may provide further clues as to the type of neuropathy that may be involved and can sometimes narrow down diag-nostic possibilities Blood tests and urine tests can be performed to look for specific causative factors A spinal fluid examination may be considered particularly if an inflammatory cause is suspected A test that is often useful for getting more objec-tive information about nerve function is called an electromyogram or EMG This test can sometimes help confirm the presence of neuropathy and may occasionally provide clues as to causation Finally in select cases a biopsy may be considered as there are some causes that may be apparent under microscopic examination
How is neuropathy treated If a specific cause such as a vitamin deficiency can be identified treat-ment would often focus on correcting that cause In situations of compressive neuropathies such as car-pal tunnel syndrome surgical decompression may be required In circumstances where the cause of a
NeuropathySteven D Stein MDDr Stein is a neurologist with the Minneapolis Clinic of Neurology practicing in Edina Minn He is board-certified in electrodiagnostic medicine He received his medical training at the University of Minnesota and his neurology training at the Mayo Clinic
10 MINNESOTA HEALTH CArE NEWS OctOber 2015
neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

neuropathy cannot be determined or if the cause is not treatable treatment focuses primarily on symptoms There are several medica-tions available to treat nerve-related discomfort including amitripty-line gabapentin pregabalin and duloxetine These medications are typically most beneficial for pain and discomfort that may be asso-ciated with neuropathy Individuals who have significant neuropathy in their feet must be very careful to prevent further damage as a result of lessened sensation Toenails should be cut by a professional and special stockings and shoes may also be of benefit As a rule it is best to avoid going barefoot to avoid damage to the feet due to the loss of sensation
Are there ways to reduce the likeli-hood of acquiring neuropathy In most cases there may not be preventive tactics to avoid the development of neuropathy Consuming adequate vitamins and other nutrients can help guard against nutritional deficiencies If an individual is predisposed towards diabetes weight loss and exercise may help limit the development of some of these conditions and may be of some benefit in minimizing symptoms
How is neuropathy linked to other diseases As noted above neuropathy may be associated with other medical conditions For example individuals with diabetes will often develop neuropa-thy The precise mechanism by which this occurs is not well under-stood In fact peripheral neuropathy may develop even before the diagnosis of diabetes Neuropathy may also be associated with other
medical conditions that produce inflammation in the body or are associated with alterations in the bodyrsquos immune system This would include conditions such as rheumatoid arthritis or lupus Neuropa-thy can be associated with various infections either as a direct effect or as an indirect effect The presence of neuropathy may also be associated with certain types of cancer
Why did it take so long for medical science to recognize neuropathy as a legitimate disease
Because the symptoms of neuropathy may sometimes be fairly vague and subjective the presence of neuropathy may not always be easily recognized Also since there has often been a conception that little can be done to help neuropathy it has sometimes been pushed aside or ignored as a diagnosis In some situations people may assume that
the development of numbness or pain in the feet is simply a normal phenomenon of aging
Can neuropathy be cured Neuropathy may be ldquocuredrdquo if a treatable cause is found Compressive neuropathies such as carpal tunnel syndrome may be ldquocuredrdquo as long as the degree of nerve damage has not been overwhelming This involves decompressing the nerve at the wrist In most circumstances we may not be able to cure the neuropathy but our treatment focuses on controlling the symptoms of the neuropathy
OctOber 2015 MINNesoTA HeAlTH CAre News 11
Individuals with diabetes will often
develop neuropathy
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Physical Fitness
With the seasons changing you may be eager to show everyone the body yoursquove worked on all summer Havenrsquot been sculpting lifting spinning and hiking as
often as you had planned Well then letrsquos get to it
Federal guidelines recommend that adults get at least 25 hours of moderate-intensity aerobic activity or 125 hours of vigorous-in-tensity activity each week or a combination of both According to the Centers for Disease Control and Prevention (CDC) the people most likely to exercise are between 18 and 24 years of age (almost 31 percent of total exercisers) Those least likely to engage in physical activity are ages 65 and older (only 16 percent of exercisers) That leaves 53 percent of total exercisers in the 25 to 64-year-old range
After a long day of work caring for the family and taking the kids to their sporting events wherersquos the time left for exercise Surely that reasoning has to do with the fact that 80 percent of Americans do not fit the recommended times for exercise into their daily and weekly schedules As a result we may try to cram our exercise program into a shorter period of time We might skip a few meals because wersquore not exercising as we should Or we might start an exercise program thatrsquos more intense than our current program Whatever it is we want the changes to occur tomorrow and we often do drastic things to make that happen This article addresses the steps needed to prevent injuries from occurring the focus of exercise based on your age and the signs that you are overdoing it Letrsquos start at the beginning the warm-up and work our way through the entire workout
Warming upAthletes weekend warriors and gym rats all need to perform some sort of dynamic (moving) warm-up to improve performance and decrease risk of injury Gone are the days of walking on the treadmill for five minutes or doing a few stretches before exercising and telling yourself that you did a good warm-up As a matter of fact static stretching (holding a stretch for a length of time) has been shown to weaken the muscle for a period of time following the stretch Therefore it is not recommended to perform this type of stretching until after your workout (when the body temperature is elevated and the muscles can stretch better) Instead movements such as High-Knee Skipping Butt Kicks Frankenstein Walks and Cariocas should be utilized as part of a thorough dynamic warm-up How many exercises should you do and for how long Research tells us that a dynamic warm-up consisting of various exercises lasting 10ndash15 minutes is adequate to increase performance and get the body ready for activity A good starting program is as follows (all exercisesmdashdescriptions and videosmdashcan be found online with a simple search or by visiting wwwyoutubecom)
bullSkipping 20 metersbull High-Knee MarchingRunning 20 metersbullButt Kicks 20 metersbullSmall Two-Footed Jumps 20 metersbullCariocas 20 metersbullFrankenstein Walk 20 metersbullLunges 20 meters
When first starting this type of program the ldquowarm-uprdquo may be more difficult than your previous or current exercise routines
A lifelong guide to exerciseGoals and precautions for all agesBy Mike Dixey PT DPT Cert MDT PES CSCS
12 MInneSOTA HeALTH CARe neWS october 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Thatrsquos OK Work into it slowly Before you know it yoursquoll be able to complete the warm-up without much difficulty and still have the energy you need to crush your workout
As we ageHow intense should your exercise program be When people see me in my clinic I often hear ldquoI used to be able to do that program no problem Why is it so difficult nowrdquo Or ldquoWhy did I get hurtrdquo While there is no clear-cut answer the truth is that we are not who we once were As we age our fitness levels quality of muscle and body composition all change In our 20s we have a great ability to perform intense heavy frequent exercise Our 20s represent the best time to build muscular power (generate maximum force as quickly as possible) The 30s are a time when we learn from what we did in our 20s and design better routines based on what worked and what didnrsquot work We exercise smarter and as a result see great improvement
Look at professional athletes for most the 30s are the prime years of their careers endurance athletes also do very well in their 30s A 2007 analysis of marathon times by German researchers re-vealed that runners donrsquot slow down at all in their 30s even though their hearts start losing stroke volume and their VO2 max levels which measure the maximum rate of oxygen consumption during exercise and reflect aerobic fitness begin to even out Our 40s
should be the time when we start caring more for our bodies when exercising According to research our nerve fibers lose their effectiveness which diminishes coordination and can lead to injury if we are not careful Our hearts also beat more slowly cutting down the blood flow that delivers nutrients to and removes waste from our joints and muscles If thatrsquos not enough wersquore also losing 05 percent of our muscle mass each year Beyond age 50 the focus should move away from looking good (although thatrsquos still a goal) to staying functional exercising
regularly is very important during this time exercise protects the heart relaxes the arter-ies builds muscle strengthens bones fights cancer and boosts the immune system To break it down exercise program goals based on age should look something like this
Decade of life Goals20s Power amp Agility
30s Strength amp Stamina
40s Flexibility amp Strength
50s+ Balance amp Mobility
Focusing on this chart can help take advantage of what our bodies need It can also remind us not to overdo it
A lifelong guide to exercise to page 34
october 2015 MInneSOTA HeALTH CARe neWS 13
Find a physical activity you enjoy
V Low- and high-risk obstetrics
including older moms-to-be
V Certified nurse midwifery
V Gynecologic care including well-woman screenings and in-office procedures
V Gynecologic surgeries including minimally invasive surgeries and robotics for conditions such as endometriosis and pelvic organ prolapse
V Menopause Clinic including management of peri-menopause
V Center for Urinary and Pelvic Health including urodynamics (urinary leaking evaluation)
V Nutrition and wellness consultations
V Infertility evaluation and treatment
Patient-friendly early morning evening and Saturday hours
Appointments
763-587-7000
Clinics in Maple Grove Plymouth and Crystal
wwwOakdaleOBGYNcom
The Best Choice for Womenrsquos Health Care
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
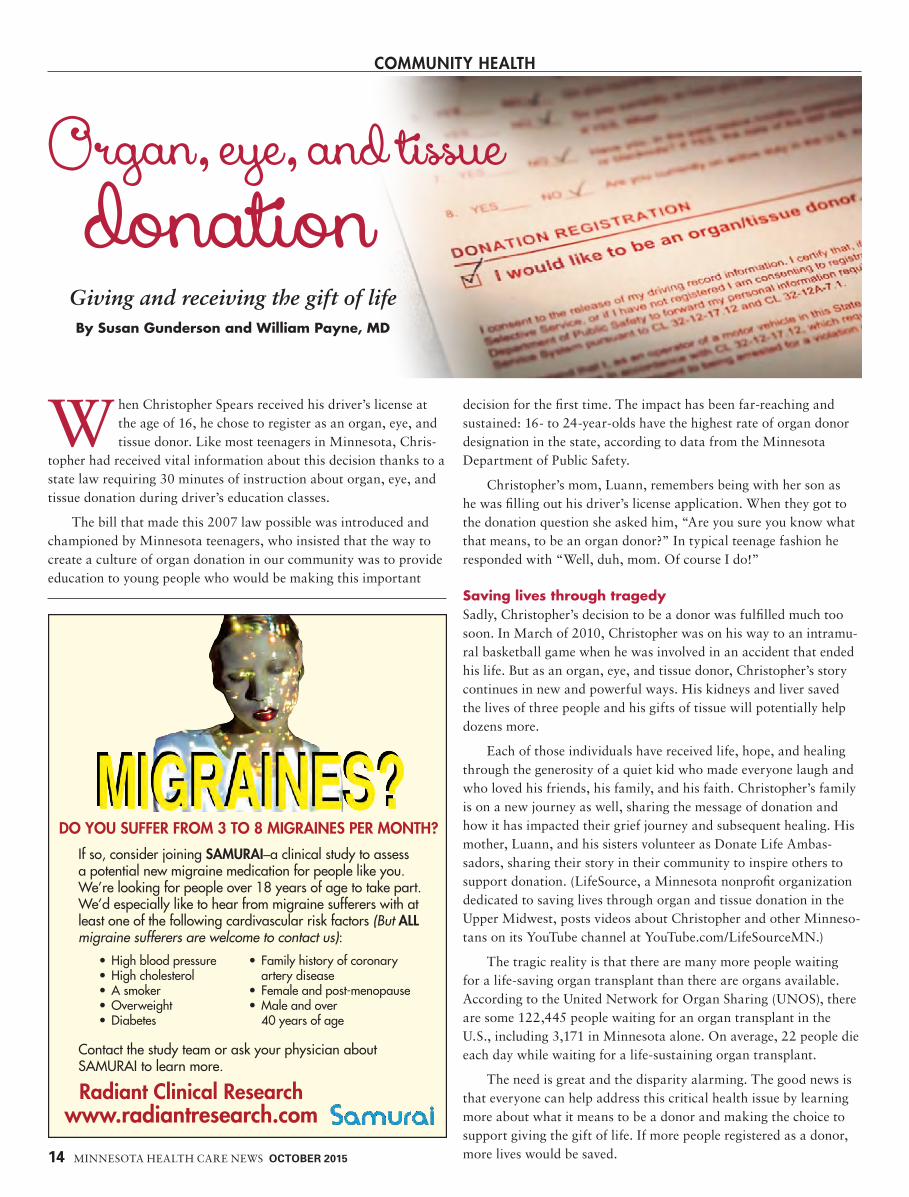
Community HealtH
When Christopher Spears received his driverrsquos license at the age of 16 he chose to register as an organ eye and tissue donor Like most teenagers in Minnesota Chris-
topher had received vital information about this decision thanks to a state law requiring 30 minutes of instruction about organ eye and tissue donation during driverrsquos education classes
The bill that made this 2007 law possible was introduced and championed by Minnesota teenagers who insisted that the way to create a culture of organ donation in our community was to provide education to young people who would be making this important
decision for the first time The impact has been far-reaching and sustained 16- to 24-year-olds have the highest rate of organ donor designation in the state according to data from the Minnesota Department of Public Safety
Christopherrsquos mom Luann remembers being with her son as he was filling out his driverrsquos license application When they got to the donation question she asked him ldquoAre you sure you know what that means to be an organ donorrdquo In typical teenage fashion he responded with ldquoWell duh mom Of course I dordquo
Saving lives through tragedySadly Christopherrsquos decision to be a donor was fulfilled much too soon In March of 2010 Christopher was on his way to an intramu-ral basketball game when he was involved in an accident that ended his life But as an organ eye and tissue donor Christopherrsquos story continues in new and powerful ways His kidneys and liver saved the lives of three people and his gifts of tissue will potentially help dozens more
Each of those individuals have received life hope and healing through the generosity of a quiet kid who made everyone laugh and who loved his friends his family and his faith Christopherrsquos family is on a new journey as well sharing the message of donation and how it has impacted their grief journey and subsequent healing His mother Luann and his sisters volunteer as Donate Life Ambas-sadors sharing their story in their community to inspire others to support donation (LifeSource a Minnesota nonprofit organization dedicated to saving lives through organ and tissue donation in the Upper Midwest posts videos about Christopher and other Minneso-tans on its YouTube channel at YouTubecomLifeSourceMN)
The tragic reality is that there are many more people waiting for a life-saving organ transplant than there are organs available According to the United Network for Organ Sharing (UNOS) there are some 122445 people waiting for an organ transplant in the US including 3171 in Minnesota alone On average 22 people die each day while waiting for a life-sustaining organ transplant
The need is great and the disparity alarming The good news is that everyone can help address this critical health issue by learning more about what it means to be a donor and making the choice to support giving the gift of life If more people registered as a donor more lives would be saved
Organ eye and tissue donation
Giving and receiving the gift of lifeBy Susan Gunderson and William Payne MD
14 MINNESOTA HEALTH CArE NEWS OctOber 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Minnesotans have an incredibly high donor designation rate with about 63 percent of adults registered as organ eye and tissue donors on their driverrsquos license or state identification card This is much higher than the national average of 51 percent according to Donate Life America
Facts and figuresAlthough the state ranks high when com-pared nationally there is room for improve-ment LifeSourcersquos goal is to reduce deaths on the transplant waiting list by saving lives and offering hope and healing by facilitating organ and tissue donation Here are the top ten facts about organ eye and tissue donation
Your life is always first If you are taken to the hospital after an accident or injury it is the hospitalrsquos number one priority to save your life Your status as a donor is not even considered until every effort has been made to try to save your life and death has been declared
Anyone can register to be a donor Your age or health should not prevent you from registering to be an organ eye and tissue donor Most health conditions do not prevent donation and age is not a factormdash the oldest organ donor in the US was 92
All faiths agree All major US religions support organ and tissue donation and consider it a generous act of caring Individuals looking for specific guidance should talk with their clergy or reli-gious leader
There is no cost to your family If you decide to be an organ eye and tissue donor your family will not have to pay for any medical expenses associated with the donation
One donor can save up to 60 people One person can save and heal up to 60 lives through organ eye and tissue donation Solid organs that can be donated include heart lungs liver kidneys pancreas and intestines Tissues include eyes bone skin veins connective tissue and heart valves
Everyone is equal When it comes to waiting in line for an organ transplant we are all created equal Wealthy or famous individuals cannot and do not get bumped up higher on the national transplant waiting list Factors such as blood type body size location severity of illness and length of time on the waiting list are used to determine the best candidate for an organ
Yoursquoll be treated with respect Organ eye and tissue donors are heroes and are treated as such The medical professionals who perform the recovery surgeries treat donors with the utmost respect just as they would for any other patient An open casket funeral or viewing should not be affected by organ and tissue donation
Your family will be well supported Donor families receive com-passionate care at the time of donation and in the months and years following their loved onersquos death LifeSource offers a comprehensive donor family aftercare program providing grief resources the ability to participate in remembrance events and the opportunity to connect with other grieving families whose loved ones gave the gift of life
Your decision will be honored When you register to become an organ and tissue donor you are making a legal decision and even
after your death your decision will be honored Itrsquos important to talk with your family to make sure they are prepared to honor your decision at the time of your death
If you donrsquot make a decision your family will If you havenrsquot registered to be an organ and tissue donor your family will be asked to
make a decision about donation on your behalf Therefore it is import-ant that you have a conversation about donation and share your wishes with your loved ones
Become a donorregistering to be an organ eye and tissue donor is simple You can
register online at wwwDonateLifeMNorg or you can check the box to register to be a donor when you apply for or renew your driverrsquos license state identification card or learnerrsquos permit
Susan Gunderson is chief executive officer of LifeSource a Minnesota nonprofit that has provided organ and tissue donation services to more than 8000 families for 26 years William Payne mD is medical director for LifeSource
OctOber 2015 MINNESOTA HEALTH CArE NEWS 15
On average 22 people die each day while waiting for a life-sustaining organ transplant
INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Dermatology
Eczema is a term for ldquoinflammation of the skinrdquo Inflamed skin is itchy red swollen and flaky In extreme cases it can even crack weep and blister Dermatitis is another name
for eczema Eczema and dermatitis are synonyms and are used interchangeably
Dermatitis can have many causes These include allergic re-actions irritation prolonged exposure to heat and moisture prolonged exposure to dryness (especially in winter) and genetic
factors For now we will focus on rashes caused by allergic reac-tions often referred to as ldquoAllergic contact dermatitisrdquo
Allergic contact dermatitisThe intense itching and blistering of allergic contact dermatitis can occur after contact with a substance that causes an allergic reaction This substance is referred to as an ldquoallergenrdquo These reactions typi-cally appear within a few days of exposure The person experiencing the allergic reaction must be exposed on a prior occasion for the first reaction to occur As one ages the reactions to specific allergens may lessen
Common allergens include nickel rubber antibiotics poison ivy hair dyes preservatives chemicals used in clothing manufactur-ing natural oils ingredients in skin care products and many others
Common allergensNickel Found in many metal products nickel is a common
cause of skin allergy Chrome-plated objects may also contain enough nickel to produce an allergic rash in people sensitive to nickel Nickel is also in stainless steel but the metallic structure of stainless steel keeps the nickel from being released and the rash from forming in nickel-sensitive people Perspiration may exacerbate nickel allergy
Earrings watch strap buckles and clothing fasteners such as belt buckles jean buttons zippers and metallic clips that contain nickel can cause earlobe lower-stomach and wrist dermatitis These are very common problems in people allergic to nickel Only stain-less steel earrings should be worn and nylon accessories and plastic buttons can be used instead of nickel for many clothing items
Rubber Rubber products including latex are a common of-fender that is well known to cause allergic contact dermatitis Chem-ical components required to process rubber usually cause the allergic reaction Latex gloves have become a real problem and those with a latex allergy can experience a life-threatening condition called ana-phylactic shock Vinyl or other synthetic gloves may be substituted for those with a rubber or latex allergy
Additionally elastic in clothing (spandex in clothing is a com-mon offender) can be problematic Allergic contact dermatitis from
A focus on allergic reactions
By Charles E Crutchfield III MD
16 MINNEsOTA HEALTH CARE NEws OctOber 2015
eczemawhat is
shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

shoes are commonly caused by ingredients used in rubber processing or any number of materials used in the construction of the shoes such as glues dyes or certain fabrics that are chemically processed
Hair and clothing dyes Most people can dye their hair without any problem Paraphenylenediamine (PPD) a common ingredient in many permanent hair colors acts as a potent allergen PPD is com-monly mixed with peroxide to activate Be sure to always do a small spot test with any permanent dye to make sure that you are not allergic Most temporary colorants can be tolerated but still need a pre-test some people may also react to dyes found in some clothing Also a distant relative to PPD is the anesthetic lidocaine About 20 percent of people allergic to PPD have allergy problems with anesthetics like benzocaine Henna tattoos may also now contain PPD and may cause allergy problems
Antibiotic ointments Triple antibiotic ointment contains bac-itracin neomycin and Polymyxin B All of these can cause allergic reactions but reactions to bacitracin and neomycin are most com-mon The longer one uses these antibiotics the more likely one is to develop an allergy to them Consult with your dermatologist before using any over-the-counter topical antibiotic especially on a long-term basis
Skin care products Perfumes fragrances creams lotions and cosmetic products may cause allergic contact dermatitis some al-lergies are a result of the chemical used as fragrance others may be from the ingredients used as preservatives Although many products will proclaim that they are ldquofragrance freerdquo ldquoor ldquounscentedrdquo they rarely are It is easy to determine if you can tolerate such products put a small amount twice daily on your forearm for three to five
days if no rash forms it is a good indicator that the product is safe to use without an aller-gic reaction Your dermatologist can perform more extensive allergic contact testing
Chromates Chromates contain chromium and are common sources of allergic contact dermatitis Chromates are found in cement match tips leather tanning some paints and products that combat rust Because chromates are found in so many products people in many occupations can experience chromate allergies
Tattoo inks There are now hundreds of pigments used in the tattoo industry but some of the common color pigments in tattoo ink that cause allergies are
bullRedcinnabar bullYellowcadmium
bullBluecobalt bullGreenchromicoxide
bullPurplemanganese bullWhitetitaniumandzincoxide
(Eczema) can have many causes
OctOber 2015 MINNEsOTA HEALTH CARE NEws 17
What is eczema to page 19
To schedule an appointment at any of our 13 locations please call 763-780-6699 or visit wwwsgsmncom
RemaRkable caRewhen it counts
we realize that any surgery is a major event in your life thatrsquos why we make every effort to make you feel at ease when you visit specialists in General surgery yoursquoll receive care that is tailored to you as an individual From discussing the details of your surgery in familiar terms to helping answer any questions our coordinated team of surgeons and staff will be with you every step of the way
at specialists in General surgery you can count on us to provide you the surgical expertise you need and the remarkable care you deserve
suRGical eXPeRtisebreast cancer
weight loss surgery (bariatrics)
Gallbladder
hernia
endocrine (parathyroid thyroid and adrenal)
Gastric Reflux
bowel (colon resections)
oncologycancer
technoloGYRobot
advanced laparoscopy
endoscopy
National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

National Depression Screening Day
An estimated 67 percent of adults in the US or about 148 million people experience major depression according to the National Alliance on Mental Illness Depression and other mood disorders are the third most common cause of hospitalization for youth and adults ages 18 to 44
Symptoms vary for everyone but the most common warning signs include changes in sleep and eating patterns lack of concentration loss of energy low self esteem feelings of hopelessness and physical aches and pains Depression can be caused by trauma genetics life circumstances or other medical conditions It can affect people of any gender age or ethnicity
Depression is a serious mental health condition However it responds very well to treatment Early detection and diagnosis and an individual treatment plan consisting of medications therapy and lifestyle changes help many people improve
18 Minnesota HealtH care news OctOber 2015
Calendar Oct-Nov 2015Oct10 Food Allergy Resource Fair
amp Trick-or-Treating The Food Allergy Support Group of Minnesota presents this free activity for families with food allergies Learn how to have a safe Halloween for your child with food allergies and bring them in costume to trick-or-treat at information booths for allergy-friendly candy Free but a $5 donation per family is encouraged For more information visit wwwfoodallergysupportmnorg Saturday Oct 10 9 amndash12 pm Eisenhower Community Center 1001 Hwy 7 Hopkins
20 Pancreas Cancer Support GroupAllina Health hosts this free support
group for those living with pancreas cancer and their families Come share information and gain support from others on a similar path Meetings are facilitated by a nurse coordinator and oncology social worker No registration required call (612) 863-7553 with questions or to learn about other meeting dates Tuesday Oct 20 4ndash6 pm Abbott Northwestern Hospital Piper Building 913 E 26th St Ste 602 Minneapolis
23 Advance Care Planning Class Park Nicollet presents this free class for
those who are ready to start the advance care planning process Come learn how to select a health care agent begin a family conversation and complete a health care directive Registra-tion required Call (952) 993-3454 to sign up or for more informationFriday Oct 23 1ndash230 pm Park Nicollet ClinicmdashSt Louis Park Senior Services Conference Room 3850 Park Nicollet Blvd St Louis Park
26 Seizure Recognition amp Response ClassThe Epilepsy Foundation of Minnesota
offers this free class to teach how to recog-nize the four main types of seizure first aid response for someone experiencing a seizure and basic information on epilepsy seizure triggers and more Call (651) 287-2300 to register or for more information Monday Oct 26 630ndash730 pm Southwest High School 3414 W 47th St Minneapolis
Nov 2 Growth Through GrievingHealthEast offers this group
to anyone who is grieving the loss of a loved one While grieving can be painful and lonely sharing experiences and support with others going through similar losses can help Contact Ted at (651) 232-7397 or theinhealtheastorg for more information Monday Nov 2 4ndash530 pm Maplewood Professional BuildingmdashSt Johnrsquos Hospital Watson Education Center Ste 202 1575 Beam Ave Maplewood
4 Memory ScreeningsThe Alzheimerrsquos Foundation of America is
offering free 10-minute memory screenings for those concerned about memory loss experiencing warning signs of dementia at risk due to family history or those who want to check their memory for future comparisons Call (763) 277-1008 to set up an appointment Wednesday Nov 4 8 amndash12 pm Copperfield Hill 4200 40th Ave N Robbinsdale
7 Brain Injury ConferenceThe Minnesota Brain Injury Alliance hosts
this free ldquoJourney to Wellnessrdquo conference for individuals with a brain injury family members and loved ones Come participate in work-shops and sessions focusing on innovations in the world of brain injury care therapy and rehabilitation Registration required by Nov 3 For more information or to RSVP call (612) 378-2742 Saturday Nov 7 1ndash4 pm New Life Presbyterian Church 965 Larpenteur Ave W Roseville
17 Heart SafeHennepin County Library and the Rotary
Club of Plymouth offer this free class for any-one who would like to learn the symptoms of cardiac arrest and receive training for CPR and the use of an automated external defibrillator (AED) Call (612) 543-5825 to sign up or for more information Tuesday Nov 17 7ndash8 pm Plymouth Library 15700 36th Ave N Plymouth
Online Screening for Depression
Screening for Mental Health is a nonprofit that first introduced the concept of large-scale mental health screenings in 1990 in conjunction with its first National Depression Screening Day To take an anony-mous online depression screening and educate yourself on the signs and symptoms of mental illness visit helpyourselfhelpothersorg
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Poison ivy and its relatives Every year 30 million people in the Us experience dermatitis from poison ivy Poison ivy poison oak and poison sumac are three related American plants of the genus Rhus They contain an oil (urushiol) which is the allergen and cause of allergic contact dermatitis A hint for diagnosis is that often the very itchy rash is composed of linear blisters marking the area where the plant brushed up against the skin Allergies to these three plants may make people sensitive to certain tree oils mango husks pistachios and cashew shells from overseas The skin has enzymes that naturally break down the oils over four to six hours after exposure After that you canrsquot spread the dermatitis by rubbing it or breaking blisters The only exception if it gets on animal fur or clothing that does not contain the enzyme to break it down it can be touched later and cause the reaction
TreatmentPeople with allergic contact dermatitis should
bull Avoid the allergen that causes the reaction and chemicals that cross-react with it Your dermatologist can help you identify items to avoid
bull substitute products that do not cause allergic reactions Your dermatologist can provide you with a comprehensive list of sug-gested alternatives
bull Treatment is directed to relieve symptoms Topical or oral ste-roids cool compresses and other non-steroidal anti-itch medi-
cines will be recommended by your derma-tologist Next it is important to investigate identify and removeavoid the cause of the allergic skin reaction Your dermatologist may recommend skin patch tests contain-ing different allergens to test for reactions This information can be employed to avoid future skin reactions
bull Dermatologists may initiate more aggressive treatments using prescription strength anti-itch medicines topical and oral ste-roid treatments and light (phototherapy) treatments if the rash is severe
bull Note that most allergic reactions need to be treated for three weeks
If you suspect an allergic contact dermatitis see your dermatolo-gist for the appropriate evaluation and treatment
Charles e Crutchfield III mD is a board-certified dermatologist and Clinical Professor of Dermatology at the University of Minnesota Medical School He also has a private practice in Eagan Minnesota
OctOber 2015 MINNEsOTA HEALTH CARE NEws 19
What is eczema from page 17
Most allergic reactions need to be treated for
three weeks
read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

read the labelDietary supplementsmdash
Take Care
More than half of all Americans take a vitamin dietary or mineral supplement each day driving annual sales of these products to more than $30 billion Consumers may
believe these supplements will improve their health but that doesnrsquot mean they heard it from their doctor indeed many consumers do not even discuss or disclose their supplement usage with health care providers If they did they might hear that supplements may be ineffective may interact negatively with other over-the-counter (OTC) and prescription medicines and may present health risks if overused Many consumers would be surprised to learn that such supplements are not subject to the same government oversight and regulation as OTC and prescription drugs
Buy nowSupplement makers spend more than $1 billion advertising their products through a variety of media channels and studies show that this advertising spurs consumer sales At the same time more than 40 percent of consumers say they are confused by the number and variety of supplements on the market nearly 40 percent believe they all work the same and nearly one-third say they switch supplement brands frequently based on news reports
Health care professionals including pharmacists physicians and nurses could provide valuable information on choosing quality supplements but many consumers do not ask In a 2010 survey of Americans over age 50 conducted by the American Association of Retired Persons (AARP) and the National Institutes of Health (NIH) 37 percent said that they used herbs and dietary supple-ments yet 67 percent never discussed their use with a health care provider A 2011 Harvard Opinion Research Program study of more than 1500 US adults found that 36 percent did not tell their physi-cian about their use of supplements while 5 percent had been told to stop using the supplement by their health care provider One-fourth of these respondents said they would stop using the supplements if they were found to be ineffective The US Preventive Services Task Force doesnrsquot recommend regular use of any multivitamins or herbs citing lack of evidence from numerous long-term studies
Claims evidence and regulationIn spite of these findings supplement makers often make claims that cannot be backed up by research and industry oversight can be lacking While supplement makers must follow manufacturing prac-tices mandated by the US Food and Drug Administration (FDA) they do not have to prove that their product is safe and effective prior to marketingmdasha fact likely unknown by many consumers
Finished dietary supplement products and dietary ingredients are regulated under the Dietary Supplement Health and Education Act (DSHEA) of 1994 not by the FDA regulations that cover foods and drug products Manufacturers and distributors of dietary supplements and dietary ingredients are prohibited from marketing products that are adulterated or misbranded and are responsible for evaluating the safety and labeling of their products before marketing to ensure that they meet all the requirements of DSHEA and FDA regulations The FDA is responsible for taking action against adulterated or misbranded dietary supplement products only after they reach the market
For the most part the FDA relies on post-market surveillance efforts such as adverse event reporting consumer complaints and
A look at an unregulated industryBy Marsha K Millonig MBA BPharm
20 MINNESOTA HEAlTH CARE NEWS OctOber 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

facility inspections to identify potential safety concerns for dietary supplements One report notes the FDA only conducts spot-tests on 1 percent of the 65000 dietary supplements on the market If a concern is identified the FDA must demonstrate that the dietary sup-plement presents a significant or unreasonable risk or is otherwise adulterated before that product can be removed from the market
Because this approach has fallen short in the past the Food Drug and Cosmetic Act was amended by the Dietary Supplement and Nonprescription Drug Consumer Protection Act of 2006 to tighten oversight Manufacturers are now required to notify the FDA of supplement-related serious adverse events These are defined as any health-related events that result in for example a death a life-threatening experience an inpatient hospitalization or a birth defect or which require based on reasonable medical judgment a medical or surgical intervention to prevent those serious outcomes
The FDA received more than 6000 reports between 2008 and 2011 according to a March 2013 report from the Government Accountability Office (GAO) with most of those coming from industry The GAO said it believes these are probably under-reported because some consumers appear to report these events to poison control centers instead of the FDA
In spite of these efforts regulating dietary supplements remains problematic and many consumers are unaware of factors that can affect the safety and efficacy of these products The Council for Responsible Nutrition (CRN) a Washington DC-based trade association representing dietary supplement manufacturers says that 85 percent of American adults were confident in the safety quality and effectiveness of supplements Yet an analysis published by JAMA Internal Medicine in 2013 found that dietary supplements represented more than 50 percent of the FDArsquos Class I Pharmaceuti-cal recalls between 2004 and 2012 Most of these substances were for bodybuilding weight loss or sexual enhancement products that contained unapproved medicinal ingredients and almost 25 percent were manufactured outside of the US
And in February 2015 the New York State Attorney General had four major retailersmdashGNC Target Walgreens and Walmartmdashpull herbal products bearing each storersquos brand from their shelves following an investigation Authorities purchased 78 bottles of the leading brands of herbal supplements across New York State then conducted DNA analysis to determine whether they contained herbs listed on their labels Four out of five products did not contain any of these herbs and testing further revealed that pills often contained little more than cheap fillers One product marketed as ginseng contained only powdered garlic and rice while another one labeled as ginkgo biloba contained little more than powdered radish houseplants and wheat The investigation also stated that pills sold as St Johnrsquos wort and valerian root tested negative for the herbs on their labels Critics of the investigation said that herbal DNA could have been destroyed in the manufacturing process rendering the tests inaccurate although DNA was detected for other ingredients used as fillers
Read the labelsThe large number of recalls and lack of safety and efficacy requirements underscore the need for consumers to choose quality supplements and to use them appropriately The United States
Pharmacopeial Convention (USP) provides a Dietary Supplement Verification Program that allows manufacturers to affix product labeling with the USP mark if the tested product meets specific requirements The requirements include verification of product ingredients and amounts effective disintegration and dissolution for absorption absence of harmful contaminants and safe sanitary well-controlled manufacturing Consumers should look for the USP mark on vitamin and mineral supplement labels Consum-ers should also consult their pharmacist or other health care provider to share why they are seeking to use a supplement ask what studies show about the prod-uctrsquos effectiveness and seek advice on high quality supplement brands and how to use them correctly
The NIHrsquos Office of Dietary Supplements provides an overview on supplement use at httpsodsodnihgovfactsheets
MVMS-HealthProfessional This site has consumer updates on dietary supplements including new warnings and tips for spotting health fraud
Information about medicine and supplement interactions may be found at httpacshorg200011whats- the- story- drug- supplement- interaction
Marsha k Millonig MBa BPharm is interim executive director of the Minnesota Pharmacists Association An associate fellow at the University of Minnesota Center for Leading Healthcare Change she is also president and CEO of Catalyst Enterprises LLC
OctOber 2015 MINNESOTA HEAlTH CARE NEWS 21
Many consumers do not even discuss or disclose their supplement usage
with health care providers
USP mark
Psychiatric Care evolved888-9-prairie prairie-carecom
Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Womenrsquos HealtH
Technological advances have benefitted our lives in many ways As a long-time ob-gyn physician I can attest that this is true in gynecologic surgery particularly with regard to
minimally invasive laparoscopic hysterectomy While many individ-ual surgeons as well as the American College of ObGyn Committee (ACOG) prefer an alternative vaginal surgical approach I prefer the laparoscopic procedure for reasons stated below
BackgroundHysterectomies are among the most common gynecologic surgeries As many as 20 percent of women undergo a hysterectomy by the age of 55 for reasons including fibroids or benign lumps in the uterus uterine prolapse a sliding of the uterus from its normal position into
the vaginal canal cancer of the uterus cervix or ovaries endome-triosis in which uterine tissue attaches and grows elsewhere adeno-myosis a condition similar to endometriosis that affects the muscles of the womb abnormal vaginal bleeding and chronic pelvic pain These conditions may require a hysterectomy to remove the upper part of the uterus the entire uterus cervix and surrounding tissue and in some instances the ovaries
There are several ways to perform a hysterectomy and often the reason for the hysterectomy dictates what type of surgery is best In the past all hysterectomies required a large abdominal incision and lengthy recovery time Today women who have a normal-sized uterus have no history of abdominal surgeries and do not have cancer are good candidates for an alternative minimally invasive hysterectomy
ldquoMinimally invasive hysterectomyrdquo is performed in two ways The first type done through the vaginal canal without any other ab-dominal incisions has been performed for years and has historically been the alternative to large abdominal incisions The other method is the laparoscopic hysterectomy which is performed through small in-cisions in the abdomen using scopes (like telescopes) video monitors and long instruments Both of these procedures offer an easier recov-ery for the patient with fewer complications when compared with the abdominal hysterectomy although ACOG in its 2009 Committee Opinion advocated strongly in favor of vaginal hysterectomies
Weighing the choicesWhy do ACOG and some surgeons recommend the vaginal ap-proach over the minimally invasive laparoscopic approach One reason is that the data used for ACOGrsquos conclusion predates major advances in laparoscopic hysterectomy that have occurred since 2005 Since that time extensive data supporting use of laparoscopic hysterectomy demonstrates its success Another likely reason is the preference and training of the surgeon The laparoscopic hysterec-tomy is generally considered more technical and difficult than the other forms of hysterectomy and requires additional training
In practice since the early 80s I have personally taken part in the transition away from the abdominal approach to hysterectomy My initial approach was the vaginal hysterectomy but like many other surgeons I now prefer the laparoscopic hysterectomy My experience is that patient outcomes and satisfaction are improved with the laparoscopic approach and that patients have more rapid return to normal activities and to work (usually within two weeks) as well as less pain In fact Irsquove performed hundreds of laparoscopic hysterectomies and have not done a vaginal hysterectomy for more than five years
HysterectomyAlternative surgical approaches
By Jon Nielsen MD FACOG
22 MInneSOTA HeAlTH CAre neWS OctOber 2015
Read us onlineWherever you are
wwwmppubcom
The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

The case for laparoscopic hysterectomyHere I make my case for laparoscopic hysterectomy as the new ldquogold standardrdquo for hysterectomy
No recent data The main source of information used to cre-ate the ACOG Committee Opinion was the latest 2009 Cochrane review of 34 randomized trials of abdominal hysterectomy lapa-roscopic hysterectomy and vaginal hysterectomy including 4495 patients This report highlighted com-parisons with abdominal hysterectomy and confirmed the opinion that when a minimally invasive procedure could be performed rather than an abdominal ap-proach it should be done
Comparative data time cost The ACOG Committee Opinion focuses on cost effectiveness and efficiencies of the vaginal hysterectomy Unfortunately most of the comparisons are to abdominal hysterectomy rather than laparoscop-ic hysterectomy To date there is still a scarcity of data comparing vaginal and laparoscopic hysterectomy Older studies found that laparoscopic hysterectomies took longer than the vaginal hysterec-tomy but as surgeons and teams have mastered these newer more technical procedures laparoscopic hysterectomy operating time has shortened Technological surgical advances including the use of the barbed suture newer energy systems laparoscopic entry techniques and the focus on doing these procedures in efficient and consistent outpatient facilities have further reduced operating time
Those factors have also driven down the costs of laparoscopic hysterectomies one of the issues cited by the ACOG Committee Opinion in 2009 Use of disposable instruments was also cited as a reason for increased cost with laparoscopic hysterectomy Today these same devices are now often used with the vaginal approach which likewise increases cost
Moreover same-day discharge or surgery in ambulatory surgery centers is more common with laparoscopic than vaginal hysterecto-my subsequently decreasing cost At Oakdale ObGyn our practice performs more than 90 percent of laparoscopic hysterectomy as out-patient surgeries We are comfortable with that approach and would not be as comfortable with same-day discharge following vaginal hysterectomy
Training and safety A strong consistent trend has been away from vaginal hysterectomy in the last 20 years with less than 15 percent of hysterectomies now being done vaginally Most residency training programs are not focusing on training vaginal hysterec-tomy In fact surveys show that most residents are more com-fortable with the total laparoscopic hysterectomy or laparoscopic hysterectomy
Of note there were no differences in complication rates be-tween vaginal and laparoscopic hysterectomy However studies have shown that laparoscopic hysterectomy demonstrated less post-opera-tive pain and shorter hospital stays
Deciding whatrsquos best for patients A concluding recommenda-tion from the ACOG 2009 Committee Opinion was that in cases where a vaginal hysterectomy was not feasible then the laparoscop-ic hysterectomy was an appropriate alternative to the abdominal hysterectomy The problem is that there are many limitations that exist with the vaginal approach which in turn limit the type of cases that can be done vaginally Visualization and access to the
pelvis is limited especially the upper pelvis limiting comprehensive treatment of such conditions as endometriosis or other concomitant disease processes There are very few conditions that preclude the use of the laparoscopic hysterectomy
Call for more studies I recommend a reevaluation of all the current data regarding the relative value of these two techniques A likely outcome from such a study would be that both procedures
are safe cost effective and produce good outcomes While some surgeons have strong preferencesmdashand some insurance compa-nies favor one procedure over anothermdashthe final decision should be determined by the patient and the surgeon and informed by scientific evidence
ConclusionWomen for whom a hysterectomy is recommended should be clear why the hysterectomy is recommended and be educated on alterna-tives If a minimally invasive procedure is not being considered they should ask why not Questions about the surgeonrsquos experience with different types of hysterectomy are not inappropriate If the ratio-nale for recommendations does not seem to be clear then a second opinion may be appropriately sought
Jon nielsen mD FaCoG is a fellow of the American College of Obstetrics and Gynecology He practices with Oakdale Ob-Gyn a division of Premier Ob-Gyn of Minnesota
OctOber 2015 MInneSOTA HeAlTH CAre neWS 23
ldquoMinimally invasive hysterectomyrdquo is
performed in two ways
Visit a Farmers Market Visit a Farmers Market
Locally grown foods are fresh and tasty are a healthy choice offer a variety of food support your local economy
Visit Minnesota Grown at wwwminnesotagrowncomfor a list of over 950 farmers markets orchardsand berry farms
The Minnesota Diabetes and Heart Health CollaborativeWorking together to keep you informed wwwmn-dcorg
Minnesota Diabetes ampHeart Health Collaborative
EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

EnvironmEntal HEaltH
Mold is truly everywhere in our environment Oftentimes fungi are a great thingmdashwithout them we wouldnrsquot have natural decomposition of plants and we wouldnrsquot have
things such as penicillin bread and wine However when mold starts growing in our buildings it isnrsquot so beneficial Not only is indoor mold growth unsightly smelly and destructive but exposure to mold can cause negative health effects Building owners should not tolerate any indoor mold growth It doesnrsquot matter if the mold is green or black fuzzy or slimy all indoor molds can cause health effects and should be removed as soon as possible
Mold has three simple requirements for growth moderate tem-peratures nutrients and moisture The first two are present in every indoor environment ldquoRoom temperaturerdquo happens to be great for mold growth Common building materialsmdasheverything from wood and drywall to upholstery and carpetmdashare excellent food sources Since we canrsquot control temperature and building materials much the third requirement is key moisture Cozy dry homes resist mold growth so if building owners can quickly solve water and condensa-tion issues they can prevent mold problems
Health concernsFor most people the health problems associated with mold exposure can be summed up with one word allergies According to the Amer-ican Academy of Allergy Asthma amp Immunology (AAAAI) about 5 percent of the general population will suffer an allergic reaction to mold Typical allergy symptoms include irritated eyes runny nose sore throat and sneezing Mold and dampness are a well-known trigger for attacks in asthma patients The Institute of Medicine (IOM) stated in 2004 that there is sufficient evidence of an asso-ciation between damp indoor environments and upper respiratory tract symptoms cough wheeze and asthma symptoms Treatment of allergies and asthma should begin with a primary care provider and include discussion of environmental exposures and history of symptoms Referrals may be made to ear nose and throat (ENT) specialists pulmonologists or allergistsimmunologists
A very limited segment of the population is at risk for oppor-tunistic mold infections For the most part these infections will only occur in patients with weakened or impaired immune systems These immunocompromised patients include those with uncon-trolled diabetes or HIVAIDS or those undergoing treatment with chemotherapeutic drugs or organ transplant drugs The Centers for Disease Control and Prevention (CDC) recommends that indi-viduals with these conditions protect themselves by avoiding ar-eas with a lot of dust or with bird and bat droppings by wearing gloves when handling soil and by taking other steps Good com-munication with your health care provider is necessary if you are immunocompromised
Serious respiratory fungal infections can also occur in people with fully functional immune systems but are quite rare According to the CDC lung infections such as valley fever or histoplasmosis
indoor moldRisks and remediation
By Kelly Smeltzer MPH
24 MINNESOTA HEAlTH CARE NEwS OctOber 2015
Issues with
April 2014 bull Volume 12 Number 4
Medical researchJeffrey Miller MD and Timothy Schacker MD
Pediatric fracturesSteven W Meisterling MD
E-cigarettesBarbara A Schillo PHD
Donrsquot miss an issueHave you subscribed to Minnesotarsquos best source of health care information To receive your personal copy of Minnesota Health Care News each month
complete and return the form below
MPP Inc | 2812 East 26th Street | Minneapolis MN 55406 | mppubcom
NameTitle
Company
Address
CityStateZip
Phone Email
Annual Subscription $3600
Paid by Credit Card Visa MC Exp Date Bill Me
Card
Signature
Credit card orders may also be phoned in to 6127288600
can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

can occur in people who visit and live in certain areas and most are contracted from certain soils Birds and bats can carry these fungi as well so people exposed to their droppings should wear the appropri-ate personal protective equipment to minimize the risk of infection
Many mold species produce a chemical byproduct known as mycotoxins some of which are actually beneficial Penicillin for example is a derivative of a mold toxin but other toxins can cause severe illness in humans while evidence links ingestion of these toxins to severe illness there is little research available to show toxic effects from inhalation of these compounds in the home or the work-place It is important to remember that mold species do not always produce mycotoxins and that the amount of toxins found in our buildings is typically well below the amount that could cause a toxic effect
Addressing indoor moldBuilding occupants with symptoms of a mold allergy must find the mold source and solve the problem Searching indoor mold need not be complicatedmdashthe most practical investigative tools available are your eyes and nose Take a walk through the building and look for signs of extra moisture If you see evidence of water damage from leaking pipes or water intrusion look there first for mold Interview the building owner service providers and occupants if necessary and review previous records such as real estate disclosure state-ments Evaluate rooms such as bathrooms and kitchens that might have condensation problems It might be necessary to look behind
or underneath carpet furniture or cabinets If you smell an earthy or musty smell assume there is mold growing somewhere Visible mold growth can be a variety of colors or textures but often it will appear as discoloration or a fuzzy growth Tools such as moisture meters infrared cameras and boroscopes (thin snaking cameras) can be useful in these investigations
In most situations environmental mold testing is unnecessary If you can see or smell the mold then you know you have a mold issue The CDC US Environmental Protection Agency (EPA) and most state health departments discourage the routine use of mold
testing for several reasons Currently there are no health-based standards available to define unsafe amounts of mold Everyone reacts differently and insufficient research has been done to determine these standards As stated earlier the type of mold does not usually mattermdashall molds have the potential
to cause health effects so if you find mold it needs to be removed Finally mold testing is expensive and has some inherent problems No single mold test is going to detect all types of mold and levels of spores can vary greatly throughout a day In almost all cases the money spent on testing is better used to identify and solve the mois-ture problems in the building
Remediation of mold begins with one extremely important step solve the moisture problem No building owner wants to clean up
Issues with indoor mold to page 29
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 25
No indoor mold growth should be tolerated
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

OncOlOgy
The American Cancer Society estimates that 39500 people will be diagnosed with oral or oropharyngeal cancer (affect-ing the part of the throat just behind the mouth) this year
and that 7500 people will die of these cancers in 2015 Historically oral cancer has been associated with males over the age of 60 who regularly consume tobacco and alcohol products However statistics now show that in certain populationsmdashespecially younger individ-uals white males and people infected with the human papilloma virus (HPV)mdashthe incidence of oral cancer is increasing and that a
significant number of these cases are not diagnosed until they reach the advanced stages These trends are of particular concern since oral cancer can often be detected early during routine dental and medical exams
BackgroundTumors of the head and neck are among the top ten most common malignancies for both men and women An estimated 291108 peo-ple living in the US had oropharyngeal cancer in 2012 according to the National Cancer Institutersquos Surveillance Epidemiology and End Results Program (SEER) In Minnesota rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer Across the globe oropharyngeal cancer is the 11th most common cancer according to the World Health Organization (WHO)
Some 50 percent of all head and neck tumors originate within the oral cavity Approximately 90 percent of cancers in the oral mucosa originate in the thin flat (squamous) cells lining the mouth lips and oral cavity Other possible head and neck cancers include salivary gland tumors sarcomas (tumors of bone nerve cartilage fat muscle or blood vessels) and mucosal melanomas Cancers within the oral cavity most often occur on the tongue the tonsils and oropharynx (throat region) and along the gums or floor of the mouth
Although once associated with tobacco and alcohol consump-tion the patient demographic for head and neck cancer is changing There has been an alarming and steady increase in the incidence of oral cancers occurring in patients below the age of 40 and in particular females without identifiable risk factors Researchers have also focused on the role of viruses specifically those associated
Cancers of the neck and head
Detection and treatment
By Deepak Kademani DMD MD FACS
26 MINNESOTA HEAlTH CARE NEWS october 2015
Rates of oral cavity and pharynx cancer in 2015 were higher than rates of both cervical and ovarian cancer
In the next issue
bull Anemia
bull Advance care planning
bull Rotator cuff injuries
Your Guide to Consumer Information
with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

with HPVs which are now considered an independent risk factor for the development of oral cancer Fortunately the prognosis for treating cancers associated with HPV is favorable as these tumors show better responsiveness and survival rates when compared to HPV-negative tumors
Oral cancer is often preceded by precancerous lesions or abnormal tissue changes Patients may not be aware of these lesions and may not experience symptoms and many lesions are only identified during dental exams or oral screenings It is important to find monitor and manage such precancerous lesions because with time they may develop into oral cancer Oral lesions are typically categorized according to color and include white (leukoplakia) red (eryth-roplakia) and redwhite (erythroleuko-plakia) characteristics White lesions are associated with a malignant change in only 1 to 3 percent of cases while redwhite lesions are associated with a 50 percent incidence of malignant change Individuals with any lesion should alert their health care provider to ensure ongoing surveillance and to assess the need for a biopsy or surgical removal
Symptoms that could indicate oral cancer include jaw or dental pain changing or growing lesions loose teeth bleeding difficulty in speech articulation pain or difficulty in swallowing ear pain sensory and motor nerve compromise mass lesions at the primary site or cervical lymphadenopathy (affecting the lymph nodes in the neck)
Detection and treatmentUnfortunately despite advances in screening tools imaging technol-ogy and access to primary care physicians a significant number of these cancers are not diagnosed until they reach the advanced stages
As noted above 90 percent of oral cavity cancers originate in the squamous cells lining the lips and oral cavity It is widely believed that tobacco and alcohol create an irritated and thinned environment conducive to oral cancer Studies have shown that the death rate from oral cancer is about four times higher for cigarette smokers Additionally younger patients who use smokeless tobacco are also being diagnosed with oral cancer in significantly growing numbers Other possible contributing factors include poor oral hygiene irritation caused by ill-fitting dentures and rough surfaces on teeth poor nutrition some chronic infections and combinations of these factors
Patients with a history of smoking alcohol consumption or smokeless tobacco or snuff usage should perform monthly self-ex-aminations of their tongues and oral cavities For all individuals annual or biannual dental examinations are critical to early detection of oral cancer If a lesion looks suspicious a biopsy may be recommended to help establish a diagnosis and treatment plan If the lesion is dysplasia or precancerous ongoing monitoring may be recommended
If a cancer diagnosis is confirmed then further imaging may be indicated Com-puterized tomography (CT) scans andor magnetic resonance imaging (MRI) provides three-dimensional views of the tumor and the surrounding anatomy These images may show if lymph nodes are enlarged or if there are other areas of concern A more sensitive test the positron emission tomography (PET) scan may identify possible areas of cancer involvement including metastasis to the lymph nodes the lungs and other parts of the body Additional tests may include blood
work or a chest X-ray Since no single reliable test will determine if the cancer has spread clinical examina-tion and surveillance after surgery are very important
Patients diagnosed with oral cavity cancer should have their treatment planned by a team of doctors specializing in head and neck
cancer Early-stage cancer is typically managed with either surgery or radiation therapy While these two approaches have almost equal success in the control of recurrence the side effects of radiation
Cancers of the neck and head to page 28
october 2015 MINNESOTA HEAlTH CARE NEWS 27
Oral cancer can often be detected early during routine dental and medical exams
Do you have patients with trouble usingtheir telephone due to hearing loss speechor physical disability
If sohellipthe TED Programprovides assistive telephoneequipment at NO COSTto those who qualify
Please contact usor have your patientscall directly for moreinformation
1-800-657-3663wwwtedprogramorg
The Telephone Equipment Distribution Program is funded through theDepartment of Commerce Telecommunications Access Minnesota (TAM)and administered by the Minnesota Department of Human Services
Duluth bull Mankato bull MetroMoorhead bull St CloudTe
lepho
neEq
uipm
ent
Dis
trib
utio
n(T
ED)
Prog
ram
often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

often make this a less appealing option Advanced-stage tumors require additional modes of treatment often including surgery radiation and chemotherapy An individualized approach developed by a multi-disciplinary team will ensure the best treatment options
Ultimately the goal of treatment is to remove the primary site of the cancer along with a margin of noncancerous tissue one to two centimeters in all directions surround-ing the tumor This uninvolved region which varies by location may include bone tissue and teeth As with other cancers squamous cell carcinoma tends to spread through the lymphatic system The head and neck contain more lymph nodes than other body parts with some 700 located above the collarbone Therefore it may be necessary to remove the lymph nodes in the neck to prevent the spread of malignant cells
After the surgical removal of oral cancer lesions reconstructive surgery is often desirable to address both functional and cosmetic changes The goal of reconstruction is to reestablish normal functions such as speaking eating and appearance as quickly as possible One
of the major advances in the treatment of patients with oral and maxillofacial cancers has been the use of vascularized bone andor tissue transplantation
Following upAfter any diagnosis of cancer follow-up care and surveillance is essential to evaluate for recurrence The overall five-year prognosis for oral cancer is determined by the site of the cancer and the presence or degree to which the malignancy has spread A relatively small localized cancer has a 75 to 90 percent surviv-al rate over five years This is far lower if there has been any spread of the cancer beyond the neck Ultimately the best opportunity for
a cure in the oral cancer patient is at the time of initial diagnosis making detection and management critical The greatest improvement in survival from oral cancer will be due to increased public and provider awareness result-ing in diagnosis at an earlier stage
Deepak Kademani DMD MD FAcS is a board-certified oral and maxil-lofacial surgeon He is the fellowship director of the Oral Head and Neck Oncologic Surgery and Reconstructive Surgery Program at North Memorial Medical Center and The Humphrey Cancer Center
Cancers of the neck and head from page 27
28 MINNESOTA HEAlTH CARE NEWS october 2015
The death rate from oral cancer is about four times
higher for cigarette smokers
SunButterreg is for peanut and nut allergic children and great for everyone
SunButtercom SunButter
SUNFLOWER SPREAD
I am passionate about being an advocate for the elderly and disabled including in maltreatment injury and wrongful death claims
Other services includebull nursing home litigation
bull health care agent appointments
bull elder abuse and neglect
bull elder mediation
bull nursing home resident rights
bull estate planning
bull speaker
Please contact
Suzanne M Scheller Esq Scheller Legal Solutions LLC6312 113th Place NorthChamplin MN 55316
7636470042suzyschellerlegalsolutionscom
Elder and Advocacy Services
wwwschellerlegalsolutionscom
OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

OctOber 2015 MINNESOTA HEAlTH CARE NEwS 29
mold and have it return because the water is still present Once the moisture problem is repaired it is important to remove the mold growth Physical pieces of moldmdashspores and hyphaemdashare the elements that cause the allergic reaction Even dead mold can cause health reactions Removing the mold can be done in two ways clean-ing or removing the building material The approach used depends on the type of material For hard non-porous materials scrub the mold off with water and detergent In most cases bleach isnrsquot needed since detergent will work fine without the hazards of bleach More absorbent materials such as carpet drywall and upholstered furni-ture need to be bagged up and thrown away It is nearly impossible to remove mold growth from these porous materials After cleaning up mold dry the area completely before beginning to rebuild
A competent and prepared homeowner can tackle a mold clean-up project but it is important to think about safety first Individuals who are highly sensitive to mold might be better off leaving the job to someone else Anyone who cleans up mold should wear personal protective equipment (PPE) including gloves eye protection and re-spiratory protection Additional PPE might be necessary if the mold growth is extensive or covers a large area when contamination ex-ists in areas with many potentially sensitive individuals (eg hospi-tals clinics schools and senior housing) or if it exceeds 100 square feet it might be time to bring in professionals Mold remediation companies can contain the work area and use special air cleaners to prevent the movement of mold spores around the building
ConclusionIndoor mold issues can be frustrating but it is important to remem-ber one simple thing no indoor mold growth should be tolerated The color texture or species of mold doesnrsquot matter since all mold can cause health effects for the occupants If a person suspects a mold allergy or reaction it is best to consult a primary care physi-cian for advice on treating the symptoms then remove the indoor mold growth Find the mold with a thorough investigation for water damage and consider environmental testing as a last resort In nearly all cases it is better to save that money and use it to repair the source of moisture in the building The good news is that by controlling moisture and keeping our buildings dry it is possible to keep indoor mold growth to a minimum
Kelly Smeltzer mPH is an Indoor Air Quality Specialist with the Minnesota Department of Health Indoor Air Unit She holds a Master of Public Health (MPH) in Environmental Health from the University of Minnesota
Issues with indoor mold from page 25
Additional Reading
US Environmental Protection Agency httpwwwepagovmoldindexhtml
Centers for Disease Control and Prevention httpwwwcdcgovmolddefaulthtm
Minnesota Department of Health httpwwwhealthstatemnusdivsehindoorairmoldindexhtml
ldquoMultiple sclerosis upended the plans I had forcing me to face uncertainty Irsquove learned to adapt and focus on whatrsquos truly important to merdquo
mdash Susan diagnosed in 1995
What does MS equal to youJoin the Movementreg at MSsocietyorg
dreams lost dreams rebuilt
MS =
pubed11_MNHealthAdindd 1 52511 1058 AM
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
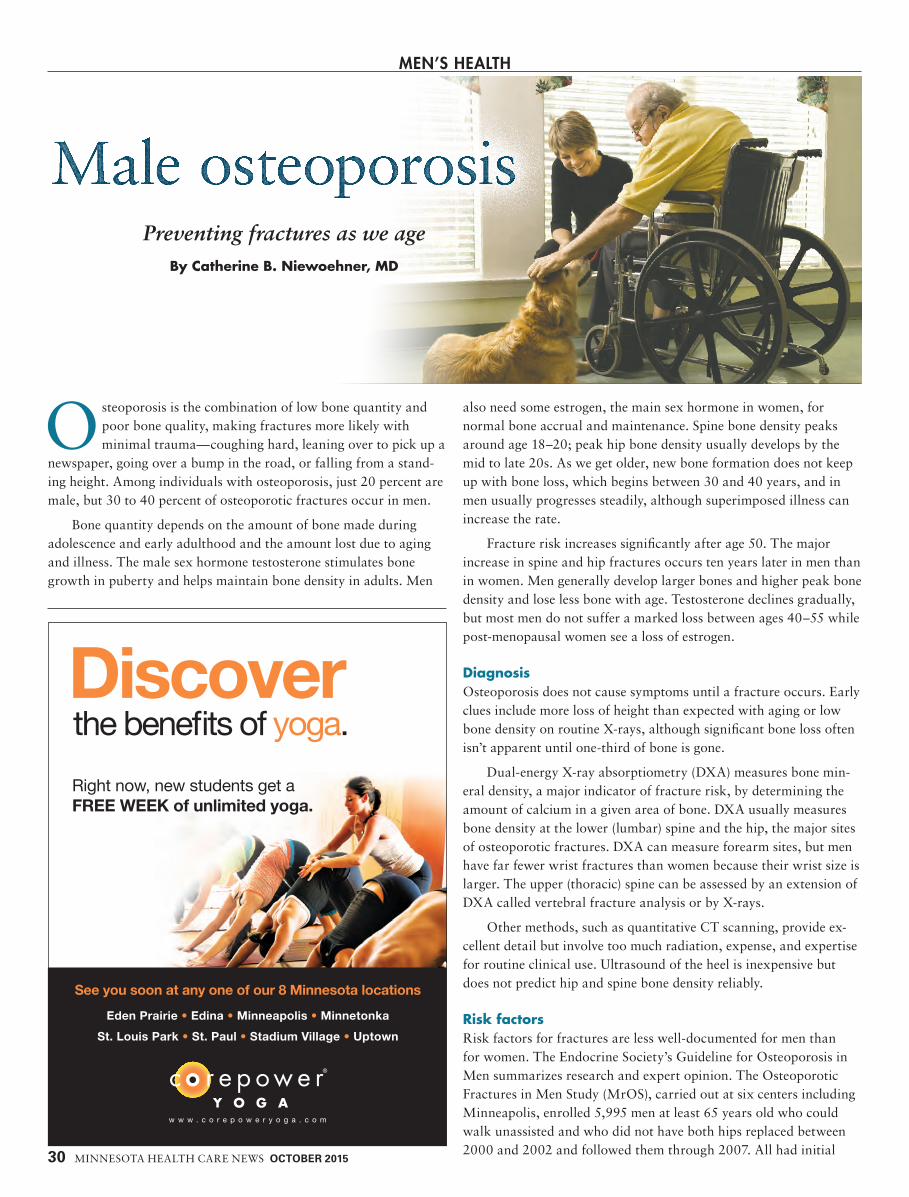
Menrsquos HealtH
Osteoporosis is the combination of low bone quantity and poor bone quality making fractures more likely with minimal traumamdashcoughing hard leaning over to pick up a
newspaper going over a bump in the road or falling from a stand-ing height Among individuals with osteoporosis just 20 percent are male but 30 to 40 percent of osteoporotic fractures occur in men
Bone quantity depends on the amount of bone made during adolescence and early adulthood and the amount lost due to aging and illness The male sex hormone testosterone stimulates bone growth in puberty and helps maintain bone density in adults Men
also need some estrogen the main sex hormone in women for normal bone accrual and maintenance Spine bone density peaks around age 18ndash20 peak hip bone density usually develops by the mid to late 20s As we get older new bone formation does not keep up with bone loss which begins between 30 and 40 years and in men usually progresses steadily although superimposed illness can increase the rate
Fracture risk increases significantly after age 50 The major increase in spine and hip fractures occurs ten years later in men than in women Men generally develop larger bones and higher peak bone density and lose less bone with age Testosterone declines gradually but most men do not suffer a marked loss between ages 40ndash55 while post-menopausal women see a loss of estrogen
DiagnosisOsteoporosis does not cause symptoms until a fracture occurs Early clues include more loss of height than expected with aging or low bone density on routine X-rays although significant bone loss often isnrsquot apparent until one-third of bone is gone
Dual-energy X-ray absorptiometry (DXA) measures bone min-eral density a major indicator of fracture risk by determining the amount of calcium in a given area of bone DXA usually measures bone density at the lower (lumbar) spine and the hip the major sites of osteoporotic fractures DXA can measure forearm sites but men have far fewer wrist fractures than women because their wrist size is larger The upper (thoracic) spine can be assessed by an extension of DXA called vertebral fracture analysis or by X-rays
Other methods such as quantitative CT scanning provide ex-cellent detail but involve too much radiation expense and expertise for routine clinical use Ultrasound of the heel is inexpensive but does not predict hip and spine bone density reliably
Risk factorsRisk factors for fractures are less well-documented for men than for women The Endocrine Societyrsquos Guideline for Osteoporosis in Men summarizes research and expert opinion The Osteoporotic Fractures in Men Study (MrOS) carried out at six centers including Minneapolis enrolled 5995 men at least 65 years old who could walk unassisted and who did not have both hips replaced between 2000 and 2002 and followed them through 2007 All had initial
Male osteoporosis
30 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Preventing fractures as we ageBy Catherine B Niewoehner MD
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

DXA scans and 4720 had subsequent scans They filled out questionnaires about race marital history education diet family history health problems including joint pain and back pain physical activity medications smoking and alcohol They filled out questionnaires about falls and fractures every four months and were tested for strength and cognition Many provided blood urine and DnA samples to measure sex hormone levels blood glucose thyroid hormone vitamin D levels and more
During the study 24 percent of new non-spine fractures were rib fractures nearly half involved falling from a standing height or lower Rib fractures were associated with old age especially over age 80 low hip bone density and previous rib fracture
Based on the above studies and many others major risk factors for fractures in men include
bullAge (over 70) bullCurrent smoking bullPrior fracture bullParental fractures bulllow testosterone bullFalls within the last year bullStroke history bullDiabetes mellitusbullDementia bullRheumatoid arthritis bullAlcohol (more than 10 drinks per week)
Risk factors related to specific systems include
bullStarvation poor calcium intake or vitamin D deficiencybull immobilization from stroke spinal cord injury or
prolonged bed restbull Poor gastrointestinal absorption especially celiac disease
inflammatory bowel disease or bariatric surgerybullRheumatoid arthritisbullChronic obstructive pulmonary disease (emphysema)bullCancer multiple myeloma or metastases to bonebull Endocrine Cushing syndrome (high cortisol) diabetes
hyperthyroidism and low testosterone
Men with low testosterone from a very young age who never develop a normal peak bone mass are particularly vulnerablemdashfor example men with delayed puberty Klinefelter syndrome or Kall-mann syndrome Men with prostate cancer being treated with drugs such as bicalutamide or lupron and others to suppress testosterone as completely as possible are at especially high risk
Drugs associated with osteoporosis include
bullGlucocorticoids (prednisone and others)bullAnti-seizure medicationsbullTreatment for HiVAiDSbull Drugs suppressing testosterone production or action
PreventionRecommendations include
Daily intake of 1000 to 1200 milligrams of calcium from diet or supplements Diet sources include dairy products canned salmon
or sardines with bones collard greens and calcium-supplemented foods such as soy milk almond milk orange juice tofu and supple-mented cereals Most supplements are absorbed better when taken in
divided doses with food
A blood vitamin D level of at least 20 to 30 ngL Vitamin D can be made from the action of sunlight on bare skin (no sunblock or clothing) by exposing bare arms and face or arms and legs to sunlight for 30-minute intervals from April to October Minneso-tans are too far away from the sun the rest of the year Elderly men have thinner skin and make less vitamin D from the same amount of exposure Many vitamin D supplements are available individual needs vary but common doses range from 400ndash2400 units daily
Weight-bearing exercise for 30 to 40 minutes three to four times weekly This is suggested for bone
strength muscle mass and fall preven-tion but there are no studies showing this amount of exercise actually prevents fractures
Limiting alcohol to two drinks per day or less and not smoking Excess alcohol inhibits formation of new bone
DXA scans of spine and hip These are recommended for all men over 70 and for men at ages 50 to 69 years if other risk factors
Male osteoporosis to page 32
OctOber 2015 MinnESOTA HEAlTH CARE nEwS 31
As we get older new bone formation does not keep up with bone loss
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

are present Bone density at the forearm can be helpful if other sites are impossible due to osteoarthritis surgery or weight over 300 pounds Medicare pays for the initial DXA only in men who already have vertebral fractures have low bone density on X-ray are treated with a glucocorticoid such as prednisone or men with hyperpara-thyroidism Medicare will pay for follow-up DXA scans usually at intervals of at least 24 months
TreatmentAdditional treatment is recommended for those who have had osteoporotic fractures and for men with bone density more than 25 standard deviations below the mean bone density scans for 30-year-old males
Other risk factors should be considered and tools have been developed that assess combinations of risk factors The world Health Organizationrsquos FRAX diagnostic tool assesses risk in 40- to 90-year-old patients who have not yet been treated Based on age sex raceethnicity height weight previous fracture family history smoking alcohol and bone density it calculates fracture risk for the next 10 years
Several drugs or classes of drugs are FDA-approved for preven-tion and treatment of osteoporosis in men These reduce fracture risk at both hip and spine
bull Bisphosphonates taken orally or intravenously inhibit osteoclasts the cells that break down bone Oral forms can cause gastrointestinal distress They accumulate in bone and can cause problems with healing of injury to the jaw This is rare with osteoporosis doses
bull Denosumab given subcutaneously also decreases the formation of osteoclasts it also is usually well-tolerated but has the same potential for rare non-healing of jaw injury as bisphosphonates
bull Teriparatide is a form of parathyroid hormone given by daily subcutaneous injec-tion it prolongs the life of osteoblasts the bone-forming cells it is the only treatment that builds new bone although nothing restores significant lost bone completely
what about testosterone replacement Testosterone increases bone density but we have no data showing that testosterone actually decreases the number of fractures Benefit for bone density in older men has not been shown unless the testosterone level measured in early morning is less than 200 ngdl Several promising new approaches are undergoing clinical trials
Catherine niewoehner MD is a staff physician in the EndocrinologyMetabolism Section at the VA Medical Center Minneapolis and a professor of Medicine at the University of Minnesota
Male osteoporosis from page 31
32 MinnESOTA HEAlTH CARE nEwS OctOber 2015
Men also need some estrogen
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I or a member of my family has become ill from household mold
3 I understand the causes of household mold
5 I am aware of how to remediate household mold problems
2 I am aware of the physical symptoms of household mold-related illness
4 I am aware of how to detect household mold
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
Strongly agree
Agree No opinion Disagree Strongly disagree
For more information please visit wwwmnhccaorg
We are pleased to present results of the most recent survey
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
0
10
20
30
40
50
60
70
80
September 2015 SurveyMINNESOTA HEALTH CARE CONSUMER ASSOCIATION
Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Be heard in debates and discussions that shape the future of health care policy There is no cost to join this informed and informative online community
Members receive a free monthly electronic newsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
JOIN US
OctOber 2015 Minnesota HealtH care news 33
When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

When starting a new program or returning to a previous one most people overestimate their fitness level and partake in a program thatrsquos too difficult Overtraining can quickly set in How do you know yoursquore doing too much too fast Here are some signs of overtraining difficulty elevating your heart rate feeling of simultaneous tightness and stiffness discom-fort in your tendons Delayed Onset Muscle Soreness (DOMS) even after low-intensity or low-volume training changes in appetite decreases in body weight mental fuzziness loss of focus during exercise loss of motivation to exercise sleep disturbances mood-related issues or general irritability persistent feelings of fatigue and loss of libido Ignoring these signs often leads to injury and a visit to the physician physical therapist or chiropractor
BenefitsThe benefits of exercise and staying in shape are numerous The Mayo Clinic cites seven ways exercise can improve your life
bull Exercise controls weight Routine exercise can help facilitate weight loss andor prevent weight gain
bull Exercise combats health conditions and diseases exercising boosts high-density lipoproteins (HDLrsquos) or good cholesterol
and decreases unhealthy triglycerides This helps keep the blood moving freely and prevents cardiovascular diseases
bull Exercise improves mood Physical activity stimulates brain chemicals that leave you feeling more happy and relaxed
bull Exercise boosts energy exercise and phys-ical activity deliver oxygen and nutrients to the tissues and help the cardiovascular system function more efficiently
bull Exercise promotes better sleep
bull Exercise puts the spark back into your sex life
bull Exercise can be fun Physical activity can get you outdoors connect you with friends and allow you to spend more quality time with your family
The key is to find a physical activity you enjoy Whether itrsquos working out at a gym hiking a Minnesota trail or playing in community sports as nike says ldquoJust Do Itrdquo If you get bored try something new Therersquos plenty to do year-round in Minnesota indoors and outdoorshellipno excuses
Mike Dixey Pt DPt cert MDt Pes cscs is a clinical specialist physical ther-apist at the Institute for Athletic Medicine in Savage He is also a credentialed McKenzie spine therapist and a certified strength amp conditioning specialist with the National Strength and Conditioning Association
A lifelong guide to exercise from page 13
34 MInneSOTA HeALTH CARe neWS october 2015
Most people overestimate their
fitness level
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks













![Wits univ business school gfc & hrm ir in mn cs oct 2011[1]](https://img.dokumen.tips/doc/110x75/553a1414550346e93a8b4a80/wits-univ-business-school-gfc-hrm-ir-in-mn-cs-oct-20111.jpg)















