Embed Size (px)
Citation preview
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 1/9
Measles, Mumps, Rubella (MMR) Vaccine discussion pack
an information guide for health professionals and parents
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 2/9
1
The MMR d iscussion pa cka n info rmation g uide fo r health prof essiona ls an d pa rents
Published by the H ealth Boards Executive, 2002.ISBN 0 9542449 1 5
Produced by the N ational D isease Surveillance Centre and the D epartm entof Public Health, Southern H ealth Board.
The publisher gratefully acknow ledges perm ission to use and adapt m aterialoriginally published in the follow ing:
• The M M R discussion pack produced by the H ealth Education Board forScotland, W oodburn H ouse, C anaan Lane, Edinburgh, EH 10 4SG incollaboration w ith the Scottish Executive and the Scottish C entre forInfection and Environm ental H ealth (SC IEH ) 2001.
• The M M R Story: M ythbuster w ritten by Dr Richard Roberts, M r D avidM organ, D r M arko Petrovic and M s C laire W illiam s and published byN orth W ales H ealth A uthority, 1999.
• M easles, M um ps and Rubella Vaccine published by Health Prom otionEngland, 2001.
These m aterials m ay be freely photocopied for the purposes of healtheducation. Perm ission should be sought from the H ealth Boards Executivebefore reproducing m aterial for any other purpose.
Further copies of the leaflet MMR your questions answered m ay beobtained from local health board health prom otion departm ents. Further
copies of the pack contents m ay be dow nloaded from the H ealth BoardsExecutive, H ealth Boards, or N D SC w ebsites. W ebsite addresses are given atthe back of the pack.
This inform ation pack has been endorsed by the follow ing organisations:Royal C ollege of Physicians of Ireland, Irish C ollege of G eneral Practitioners,D epartm ent of H ealth and C hildren.
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 3/9
Introduction
Som e parents m ay feel that the issues around im m unisation, in general, and
M M R in particular pose a real dilem m a for them about w hat is best for their
child. The sustained negative m edia coverage and high-profile public
debates over the last few years have also left m any health professionals
asking searching questions about M M R. These concerns have contributedto a decrease in the uptake of M M R vaccine and the re-em ergence of these
diseases in our population.
The MMR discussion pack w ill help professionals and parents review the
evidence around M M R and w ill help to provide the basis for inform ed
decision-m aking. It sets out the facts about the m ost com m on concerns
about M M R vaccine in a w ay that helps health professionals and parents to
explore these concerns together.
N ine m ain questions are covered and each question outlines the basic facts
plus Key Notes for parents, together w ith Additional Notes for health
professionals, w hich are fully referenced. W hilst the Addit ional Notes are
essentially for health professionals, the inform ation is presented in such a
w ay as to allow full discussion betw een health professionals and parents, on
each issue.
The form at allow s for exploration of all the issues in any order and as m uch,
or as little, of the inform ation can be photocopied to take aw ay, as desired.
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 4/9
Why aren’t the
vaccines given separately?
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 5/9
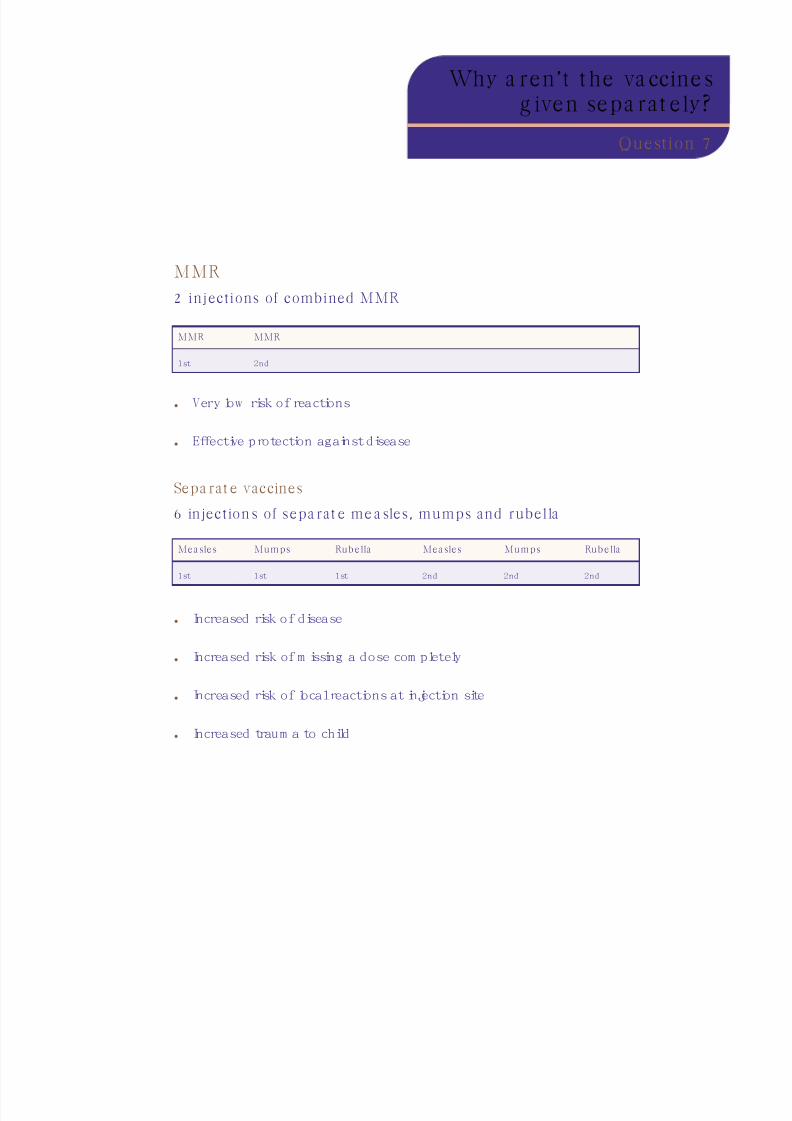
MMR
2 injections of combined MMR
• Very low risk of reactions
• Effective protection against disease
Sepa rat e vaccines
6 injection s of sepa rat e me a sles, mumps and rubella
• Increased risk of disease
• Increased risk of m issing a dose com pletely
• Increased risk of local reactions at injection site
• Increased traum a to child
Why a ren ’t t he va ccine sg iven sepa rat ely?
Question 7
Mea sles Mumps Rub ella Mea sles Mumps Rub ella
1st 1st 1st 2nd 2nd 2nd
MMR MMR
1st 2nd
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 6/9
Why a ren ’t t he vaccine sg iven sepa rat ely?
Key Notes
The issue of giving vaccines separately w as raised in the U K by D rA ndrew W akefield in a 1998 press interview . The suggestion cam e froma belief that if children catch m easles and m um ps w ithin one year ofeach other they are m ore likely to develop C rohn's disease later. It w asalso claim ed that M M R causes excess diarrhoea com pared to singlevaccines. There is no evidence to support these claim s - in fact theevidence strongly rejects any link betw een M M R and autism orinflam m atory bow el disease.
M M R vaccine is as effective in protecting against m easles, m um ps, andrubella as w hen each com ponent is given on its ow n. The com ponent
viruses do not interfere w ith each other and there is no advantage inreceiving the vaccines separately.
G iving the vaccines separately w ould m ean a child needing a total of sixinjections to com plete the course, instead of tw o. These children w ouldrem ain unprotected and at risk of disease for longer. Six injections couldalso m ean an increased risk of local reactions at the injection site.C ontrol program m es w ould be less effective and this w ould lead to m orecases of m easles, m um ps and rubella.
The use of three separate vaccines for m easles, m um ps and rubella hasnever been used in any country in the w orld. There have been no studiesdone to determ ine w hether or not this approach is safe or effective.
Likew ise there is no experience w ith using this approach. This raises anum ber of unansw ered questions: Is this approach safe? W ill it protectchildren against these diseases? W hat order should the vaccines begiven? H ow m uch tim e should be taken betw een vaccine doses?
In contrast the M M R vaccine has been in use for over 30 years andunderw ent rigorous studies to ensure that it w as safe and effectivebefore it w as released for general use. The com bined research evidenceand decades of experience w ith M M R has confirm ed that it is safe andeffective. Indeed, the W orld H ealth O rganisation recently concluded thatM M R is one of the safest vaccines ever produced.
A lthough licences for single m easles and m um ps vaccines do exist in
Ireland, no licensed single m easles or m um ps vaccine are m anufacturedfor, or available for the Irish m arket.
Som e of the unlicensed single antigen vaccines im ported into Irelandm ay be less effective and som e m ay have a higher risk of side-effectsthan the M M R vaccine.
Three separate injections to protect against m easles, m um ps and rubellahas never been recom m ended in Ireland and no country in the w orld hasrecom m ended single m easles, m um ps and rubella vaccines, w herecom bined M M R is available.
1
2
3
4
5
6
7
8

8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 7/9
Why a ren ’t t he va ccine sg iven sepa rat ely?
Additional Notes
The idea of giving single antigen vaccines, w ith an interval of at least 12
m onths betw een vaccines, instead of the com bined M M R vaccine w as
first publicised in the U K by D r A ndrew W akefield in press interview s
given after the publication of a paper in the Lancet in 1998, describing
children w ith developm ental and bow el problem s.26
The idea is based on a belief that children w ho catch m easles and
m um ps w ithin one year of each other are m ore likely to develop C rohn'sdisease later.69 W akefield and M ontgom ery have also claim ed that the
incidence of gastrointestinal adverse events is significantly higher after
M M R vaccination in the few w eeks follow ing its adm inistration in
com parison to single antigen vaccines.70 They claim that this leads to gut
dam age and subsequent autism . H ow ever, there is no evidence of
significantly excess gastrointestinal events follow ing M M R vaccination in
the original trial data.71 Indeed there is excellent evidence for a lack of
significant diarrhoea follow ing M M R. In a study from Finland, 581 tw in
pairs w ere random ised for one tw in to receive M M R and the other tw in
a placebo injection, then vice versa three w eeks later. D iarrhoea w as as
com m on in those receiving M M R as in those receiving a placebo.72 A trial
in the U K com pared M M R to a single antigen m easles vaccine. In a six-
w eek period of follow -up there w as no statistically significant difference
in diarrhoea betw een the tw o groups.73
The evidence strongly rejects any link betw een m easles or M M R and
C rohn's or autism (see Q uestion 4). The original rationale for suggesting
single antigen vaccines is therefore w ithout substance. H ow ever, som e
anti-vaccination groups have supported these view s, w hich have since
gained a high profile through national m edia and dedicated w ebsites,
resulting in increased perceived credibility.
The M M R vaccine is as effective in protecting against m easles, m um ps,
and rubella as w hen each com ponent is given on its ow n.16 There is no
evidence that the com ponent vaccine viruses interfere w ith each other.
Im m unity to the m easles com ponent and other antigens in M M R occurs
at different tim es; m easles after 6-11 days, rubella after 10-15 days and
m um ps after 15-21 days. It is norm al for children to be bom barded w ith
m icroorganism s via the gut and air, yet their im m une system s cope very
w ell.
1
2
3
8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 8/9
If single antigen vaccines w ere to be given one year apart, a child w ould
need a total of six injections at ages 1, 2, 3, 4, 5 and 6 years, to com plete
the course, instead of just tw o M M R vaccinations. These children w ould
be susceptible to those diseases for longer, and there is good evidence
that som e children w ould m iss doses altogether, resulting in m ore
unvaccinated children. The result w ould be to underm ine m easles,
m um ps and rubella im m unisation, reduce population im m unity and
increase the risk of children catching these diseases. The policy is notbased on financial considerations, but on the best w ay to protect
children. There is no scientific evidence to support the safety or efficacy
of giving M M R as three separate vaccines at defined intervals. In
contrast, M M R vaccine has been used for 30 years w ith an excellent
safety record.
A lthough licences for single m easles and m um ps vaccines do exist in
Ireland, no licensed single m easles or m um ps vaccine are m anufactured
for, or available for the Irish m arket.
The safety and efficacy of unlicensed m easles and m um ps vaccinesadm inistered in Ireland cannot be assum ed. Batch testing and cold chain
inform ation is m ost often lacking and som e strains are know n to have
unacceptable safety or efficacy profiles, in particular, the U rabe and
Rubini m um ps strains. The m anufacturers w ithdrew U rabe from Ireland
in 1993 and it has been show n to be associated w ith m um ps m eningitis
post-vaccination.74 Rubini has been show n to be of extrem ely low
efficacy and has been associated w ith subsequent outbreaks of m um ps
in Spain, Portugal, Italy and Sw itzerland because of the extrem ely low
level of protection it provides.75-77 The M M R vaccine contains the safe and
efficacious Jeryl Lynn m um ps strain.78
Single antigen m easles, m um ps and rubella vaccines as an alternative to
M M R has never been recom m ended in Ireland. Single antigen m easles
vaccine w as introduced for all children in Ireland in 1985, but w as
superseded by M M R in 1988. Single antigen rubella vaccine w as
introduced in 1971 as part of a schoolgirl im m unisation program m e to
protect w om en of childbearing age against rubella. Single antigen
m um ps vaccine has never been part of the Irish childhood im m unisation
program m e. Licensed single antigen rubella vaccine continues to be
available in Ireland, but this is prim arily for non-im m une w om en of
childbearing age.
4
5
6

8/10/2019 MMR Vaccine Discussion Pack
http://slidepdf.com/reader/full/mmr-vaccine-discussion-pack 9/9
The M M R vaccine is used in 93 countries around the w orld and no
country in the w orld recom m ends single antigen m easles, m um ps or
rubella vaccines, w here the com bined M M R vaccine is available. The use
of M M R vaccine, w hen available, is strongly supported by the W orld
H ealth O rganization.
France is often m entioned as a country w here single antigen vaccines are
given. H ow ever, the position in France is that children are given a singleantigen m easles vaccine from nine m onths of age only if they are in a
nursery, and there is a risk of a m easles outbreak. These children then
receive tw o further M M R vaccinations, as in Ireland. France does not
recom m end single antigen m um ps vaccine.79
In Japan, single antigen m easles and single antigen rubella vaccines
are recom m ended, as no M M R vaccine is available. H ow ever, Japan has
suffered from endem ic and epidem ic m easles. O ver the period 1992-
1997, there w ere 79 m easles deaths in Japan. In the U K w here the
uptake rate of M M R has been over 90% , there have been no acute
m easles deaths since 1992.79
H ow ever In Ireland w here the uptake ofvaccine has never reached the target of 95% there w ere 8 deaths
reported in the years 1990-1999 and 3 deaths in the year 2000.









![Vaccine hesitancy, vaccine refusal and the anti-vaccine ... · studies showing no link between measles–mumps–rubella (MMR) vaccination and autism [43–45] – and Wakefield being](https://img.dokumen.tips/doc/110x75/5d4f476888c993a3378b70e4/vaccine-hesitancy-vaccine-refusal-and-the-anti-vaccine-studies-showing.jpg)


















