Embed Size (px)
Citation preview

Migraine in Women
Rebecca Burch, MD
John R. Graham Headache Center Department of Neurology Brigham and Women’s Faulkner Hospitals

Disclosures • I have no disclosures

Objectives • Discuss epidemiology of migraine in women
• Review hormonal contributions to the presentation of
migraine in women
• Discuss headache management in situations specific to women

“The Femaleness of Migraine…is Inescapable.” ~ KMA Welch

Prevalence of Migraine
• Peak prevalence is in women of childbearing age • Subgroups of migraine also more common in women
Females Males
Age (in years) 20 30 40 50 60 70 80 100
0
5
10
15
20
25
30
Mig
rain
e Pr
eval
ence
(%)
Lipton R, et al. The American Migraine II Study.
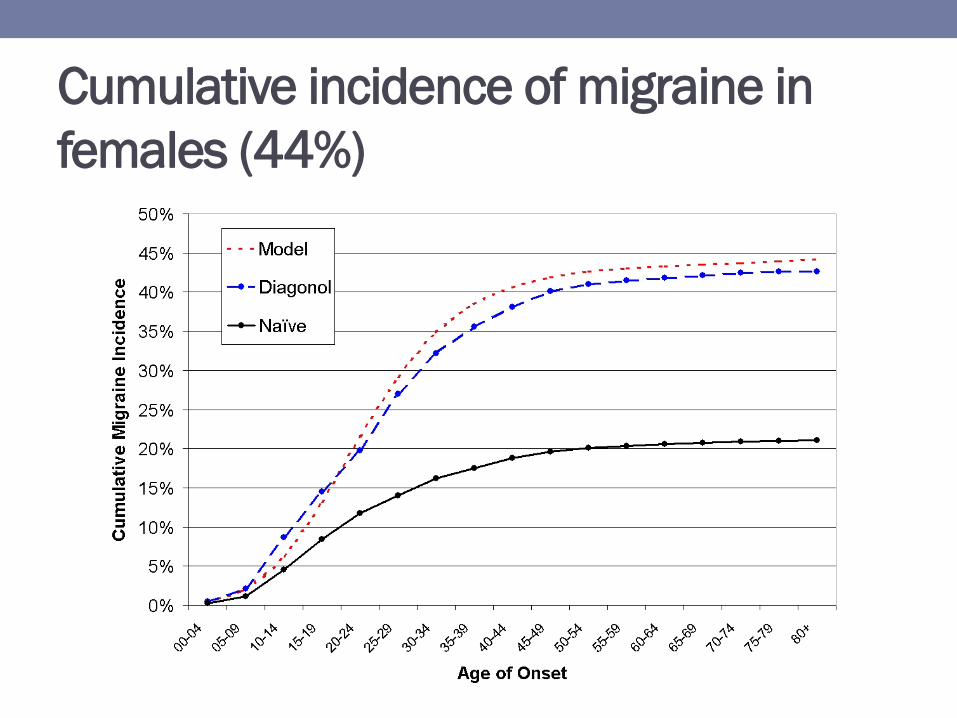
Cumulative incidence of migraine in females (44%)

Cumulative incidence of migraine in males (18%)

Clinical features of migraine in women
• Diagnostic criteria for men and women are identical • The clinical profiles of men with migraine differ from
those of women • Women more likely to experience migraine
accompanying symptoms • Population based telephone survey evaluating
migraine in the last week, ages 12-29: • Migraines more burdensome in females

In Men with Migraine, Headaches are Less Frequent, Less Painful and Less Disabling
0 5
10 15 20 25 30 35
Headache Frequency >/= 3
Per Month
Recent Headache Pain >/= 8
Missed Work or School
11
21 20 23
29 31
Male
Female Perc
ent

Why do women have more migraine?
• Hormonal factors may account for differences.
• 2 ways sex hormones might act: Developmental effects take place during a critical period and put a permanent stamp on the nervous system
Activational effects are the direct influences of circulating hormones that appear when hormonal levels rise, and wane when hormonal levels drop.

Theories behind hormonal effects on migraines 1. Neurotransmitter Imbalance Theory 2. Neuropeptide Theory 3. Cortical Spreading Depression Theory
• Declining estrogen increases CSD
Martin V. Headache 2006; 46: 3-23.
Welch K. Neurol Sci 2006; 27: S190-192
Eikermann-Haerter K. Headache 2007; 47: S79-85

Group Health Study • 3,000 boys and girls age 11 to 17 at baseline
participated in a telephone interview • 100% of headache sufferers and a 10% random
sample of non-headache sufferers sampled for in person assessment of pubertal stage
• Pubertal stage was predictive of rapid rise in prevalence in females • Not significantly associated with rise in males after adjusting
for age • May contribute to shifting sex profile in adolescence • Suggests that female and not male hormonal changes
matter
LeResche et al. (2009)

Menses is a powerful trigger factor for migraine in females not present in males
MacGregor E A et al. Neurology 2006;67:2154-2158
©2006 by Lippincott Williams & Wilkins

Hormonal epochs • Menarche/Puberty
• Menses
• Perimenopause
• Menopause/ andropause
• Incidence rises in girls
• Trigger for individual attacks
• Worsen, improve, no change
• Excess risk in women is reduced but persists

Epidemiology: take home message
•Migraine is more common and more burdensome in women
•Migraine has an epidemiologic profile consistent with •Enduring hormonal effects on disease risk
•Short-term effects of withdrawal on attacks

In the clinic • A 28 year old woman consults you with recurrent,
disabling, throbbing headaches occurring intermittently for 8 years.
• Headaches occur with menstrual periods, last 48 hours, are associated with vomiting and photo and phonophobia.
• Benign past medical history • Her neurologic examination is normal

ICHD Diagnostic Criteria For Migraine Without Aura • Lasting 4 to 72 hours • Two of the following
• Unilateral location • Pulsating quality • Moderate or severe intensity • Aggravation by or causes avoidance of routine physical activity
• At least one of the following: • Nausea and/or vomiting • Photophobia and phonophobia
• At least five attacks fulfilling the three bullet points above • No evidence of organic disease

Our patient • “I see zig-zag lines right before most of my headaches.
They get larger over the next 10 minutes and then fade away. Sometimes I have a blank spot in my vision.”
• “The whole thing lasts about 40 minutes and is followed by my typical bad headache.”

Aura
• Focal neurologic event(s)…visual, sensory, motor
• Usually precedes headache…but not always • Positive, negative, spreading and reversible
Aura

Is this aura? • “My vision gets blurry when I have a headache.
Sometimes I lose my appetite.” • “I can tell I am getting a headache because I feel tired.
I also notice changes in my mood and appetite.” • “I see zig-zag lines right before most of my headaches.
They get larger and then fade away. Sometimes I lose my vision.”

Visual Aura Rating Scale
Eriksen et al. The Visual Aura Rating Scale for Migraine Aura Diagnosis. Cephalalgia 2005;10:801-810.

Tip • Essentially all patients with any kind of aura ALSO
have visual aura • So to identify aura it is only necessary to ask about
visual aura • Visual aura is not visual blurring • Visual aura is not visual sensitivity
Eriksen et al. The Visual Aura Rating Scale for Migraine Aura Diagnosis. Cephalalgia 2005;10:801-810.

Testing • Primary headache is a clinical diagnosis • Testing is useful to rule out other disorders • Look for “red flags”
• Elderly • Unusual pattern • Worsening over time • Abnormal examination • No response to treatment
• No role for EEG • LP and neuroimaging most useful

Neuroimaging: What test to get?
• MRI generally superior to CT • Better look at posterior fossa • Superior imaging of vascular structures • Radiation risks of CT are not minor
• Plain CT indicated if acute bleed is suspected • Consult the radiologist!
• Other tests may be helpful (MRV, MRA)

Managing headaches: no major sex-specific differences • Abortive treatment
• Virtually all patients require
• Preventive treatment • Only a subset of patients with migraine and TTH; essential all
with CH • An underused intervention!
• One exception: Pregnancy

Reasonable lifestyle modifications
• Regular meals • Adequate sleep; Standardized sleep and wake times • Regular exercise and maintenance of normal weight • Limit or avoid caffeine, watch alcohol • No good evidence for other dietary restrictions

Options for acute therapy • Disorder • Tension-type HA
• Migraine
• Cluster HA
• Common treatments • NSAIDs, mild analgesics
• Ergot derivatives • Triptans • (barbiturates, narcotics)
• Injectable sumatriptan;
oxygen 10-12 liters with NRB mask for 15 minutes at headache onset
Cohen et al. High-flow oxygen for cluster headache: a randomized controlled trial. JAMA 2009;22:2451-7.

General principles of abortive therapy
• Use adequate dose • Use early/at mild stage of headache • Monitor response and adjust therapy accordingly (eg
combinations)

A few words on triptans • There are seven of them
• All available orally (2 as orally disintegrating tablets) • Results are similar when comparable doses are used • Nonetheless, patients usually have a favorite
• Two available as nasal sprays • One available as subcu injection
• Generic versions of sumatriptan are available in the US
• Sumatriptan already available without prescription in some countries
Loder E . Triptan therapy in migraine. N Engl J Med 2010;363:63-70

FDA Approved Triptans • Sumatriptan (generic) • Zolmitriptan • Naratriptan (generic) • Rizatriptan (generic) • Almotriptan • Eletriptan • Frovatriptan

Common Triptan Side Effects • Tingling • Warmth • Flushing • Chest discomfort • Dizziness

Triptans: Contraindications • Ischemic heart disease
• Angina pectoris • History of myocardial infarction • Documented silent ischemia
• Coronary vasospasm (including Prinzmetal’s angina) • Poorly controlled hypertension • Multiple risk factors for coronary artery disease,
unless workup is fully negative
Preventive Medications • Tension-type HA
• Migraine
• Tricyclics, NSAIDs
• Propranolol, timolol, divalproex sodium, topiramate and onabotulinum toxin are FDA-approved. TCAs, Biofeedback, ACEIs, ARBs, Vitamin B2, gabapentin and others used

Common Preventive Medications Evidence Level
Medication = FDA Indication
Usual Daily Dose
Comments
B Atenolol 50-100 mg A Propranolol 80-240 mg A Metoprolol 50-150 mg U Verapamil 180-480 mg Downgraded, favorable AE profile
A Divalproex sodium
250-1500 mg FDA pregnancy category X
U Gabapentin 300-1800 mg Downgraded, favorable AE profile
A Topiramate 25-150 mg FDA pregnancy category D B Amitriptyline 10-150 mg Downgraded but strong clinical
impression of benefit B Venlafaxine 37.5-150 mg Well tolerated, not sedating C Cyproheptadine 2-8 mg Pediatric population, sedating
Rizzoli, P. Acute and Preventive Treatment of Migraine, Continuum Neurol 2012;18(4):764-82

A case • A 19 year old woman presents for evaluation of
migraines without aura • Headaches occur with every monthly period,
• usually 1 day prior to start of menstruation and continuing for 2-3 days
• Migraines may occur at other times of the month, but rarely
• Takes sumatriptan every morning but headache always comes back
• Wants to know what treatment options are available

ICHD-3 beta • Pure menstrual migraine without aura: appendix • Menstrually-related migraine without aura: appendix • Estrogen withdrawal headache • Exogenous hormone-induced headache
The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24 Suppl 1:9-160.

Pure menstrual migraine without aura
• Diagnostic criteria • Attacks, in a menstruating woman fulfilling criteria for
migraine without aura • Attacks occur on days -2 to +3 of menstruation
• In at least 2 out of 3 menstrual cycles • At NO other times of the cycle
+3 +2 +1 -1 -2
ICHD-3b DEFINITION
0

Menstrually-related migraine without aura • Diagnostic criteria
• Attacks, in a menstruating woman fulfilling criteria for migraine without aura
• Attacks occur on days -2 to +3 of menstruation • In at least 2 out of 3 menstrual cycles • And additionally at other times of the cycle

Odds Ratio for Headache Attacks by Type and Time in Cycle
0
1
2
Days 7 to 3before
Days 2 to 1Before
Days 0 to 1 Days 3 to 5after
Ovulation
Time in Cycle
Odd
s R
atio
MWAMw/oATension
Stewart, Lipton et al, Neurology, 2003

Menstrual migraine prevalence • Population-based Norwegian survey: self report
• Prevalence of pure menstrual migraine 7.7% (6.9-8.7) = 2.7% of female population
• Prevalence of menstrually related migraine 13.2% (12.1-14.3) = 4.6% of female population
• BUT: • Cultural factors may play a role • Menstruation is a “magnet” explanation for symptoms that
may occur due to random chance • Prospective daily diaries for at least 2 months the only way to
properly diagnose Vetvik, et al. Headache 2010;11(2):87-92. Marcus et al. Headache 1010;50(4):539-550.

Estrogen withdrawal headache • Same patient as before, but gets headaches only
during the placebo week of combined oral contraceptives (COCs)
• Diagnostic criteria
A. Headache or migraine fulfilling criteria C and D B. Daily use of exogenous estrogen for > 3 weeks,
which is interrupted C. Headache or migraine develops within 5 days after last use
of estrogen D. Headache or migraine resolves within 3 days
Edlow AG, Bartz D. Rev Obstet Gynecol Spring 2010
Treatment options for menstrual headaches • Treatment as for non-menstrual migraine
• Triptans • Prevention • Focusing only on hormonal treatments is a pitfall!
• Short term prophylaxis • Continuous monophasic oral contraceptive pills • Additional estradiol
• Many of the hormonal strategies are of very modest
benefit compared to placebo or treatment as usual.

Triptans in MRM Mini-Prophylaxis
• New AAN/AHS guidelines • Frovatriptan class A
• Dosed 2.5 mg BID or daily for 2 days before menses, total of 6 days • Reduced frequency of headache and headache free menstrual periods
• Naratriptan and zolmitriptan class B • Naratriptan 1 mg BID 2 days before menses, total of 5 days • Zolmitriptan 2.5 mg BID/TID
• Consider need to treat breakthrough headache
Silberstein et al. Neurology 2012

Other preventative regimens • NSAIDs
• Naproxen TID– one small positive trial • Mefanamic acid 500mg TID at onset of MRM & continued for
duration of menses – one positive trial • Magnesium – insufficient evidence • Phytoestrogens – insufficient evidence • Transdermal estradiol 1.5mg, started 2 days before expected
onset of headache and continued for 7 days – two positive trials
Pringsheim T et al. Neurology 2008;70:1555-1563

Hormonal prophylaxis • Effect of hormonal contraceptives on migraine is
variable • First generation COCs tended to worsen migraine • Second and third generation effect unpredictable
• No RCTs with carefully collected HA data • Consider elimination of placebo week
• Three consecutive pill packs followed by one week of placebo
• Progesterone only pills?

Hormonal contraception, migraine, and stroke risk • Relative risks for stroke in women <45
• With aura: 2.3-3.6 • With migraine and smoking: 7.2-10.2 • With migraine and combined oral contraceptives (COCs): 6.6-
13.9 • With migraine and COCs and smoking: 34.4
• Absolute risk remains low
• 5 to 11.3 per 100,000 woman-years

Hormonal contraception, migraine, and stroke • Guidelines for migraine with aura
• ACOG and WHO: COCs present “unacceptable risk” • IHS: Individualized assessment of risk
• Guidelines for migraine without aura
• ACOG and WHO: • Under 35: No contraindication • Over 35: Risk usually outweighs benefits
• IHS: Individualized assessment of risk, depends on number of risk factors

Migraine and menopause • Improvement in migraine in 2/3 post-menopausal
women • Fluctuating estrogen levels during perimenopause
may exacerbate migraine • Effect of hormone replacement therapy on migraine is
unclear • Transdermal preferable • Increased risk for stroke similar to COCs
• Role for SSRIs/SNRIs?
Brandes JL Continuum 2012, Neri I, Maturitas 1993. Facchinetti F, Headache 2002

Migraine after menopause • Not all women see improvement • Treatment as for regular migraine • In the older patient:
• Evaluate cardiac risk factors if triptans used • Long term AED use is a risk factor for osteoporosis • Older patients may be more sensitive to TCA side effects • Cognitive effects from AEDs may be more bothersome
Brandes JL Continuum 2012, Neri I, Maturitas 1993. Facchinetti F, Headache 2002

Consultation rates and gender assumptions • Women more likely to consult than men for migraine • Assumption that females consult for a low level of symptom severity may affect diagnosis and treatment approach. • Video study: female ‘patients’
• Asked fewer questions by doctors • Fewer diagnostic tests recommended • Doctors were more likely to ‘tune into psychological cues and
search for psychological explanations for symptoms’
Hunt K et al J Health Serv Res Policy. 2011 Apr;16(2):108-17. AdamsA, et al. Sociol Health Illn 2008;30:1–18; ArberS, et al. Br J Gen Pract 2004;54:673–8
Environmental factors that may increase expression of migraine • Adverse childhood experiences • Intimate Partner Violence • Daily hassles and stress • Affective disorders
• All more common in females

Among women in a headache clinic
• 28.3% positive for PTSD • 9.8% and 36.9% endorsed recent and lifetime intimate
partner violence. • PTSD strongly associated with headache severity …
those with IPV had average of 9/90 additional days of disability.
Gerber MR, Fried LE, Pineles SL, Shipherd JC, Bernstein CA. Posttraumatic stress disorder and intimate partner violence in a women's headache center. Women Health. 2012 Jul;52(5):454-71.

Abuse • Women with migraine more likely to have a history of
abuse
• Risk increases with comorbid depression
• Risk factor for chronic headache
• All patients should be screened
Breslau N, Neurology 2003. Tietjen GE Neurology 2007

Kaplan–Meier curve for the cumulative percentage with adult-onset headache by age for persons with none, one, and two or more childhood family adversities.
Lee S et al. BJP 2009;194:111-116
©2009 by The Royal College of Psychiatrists
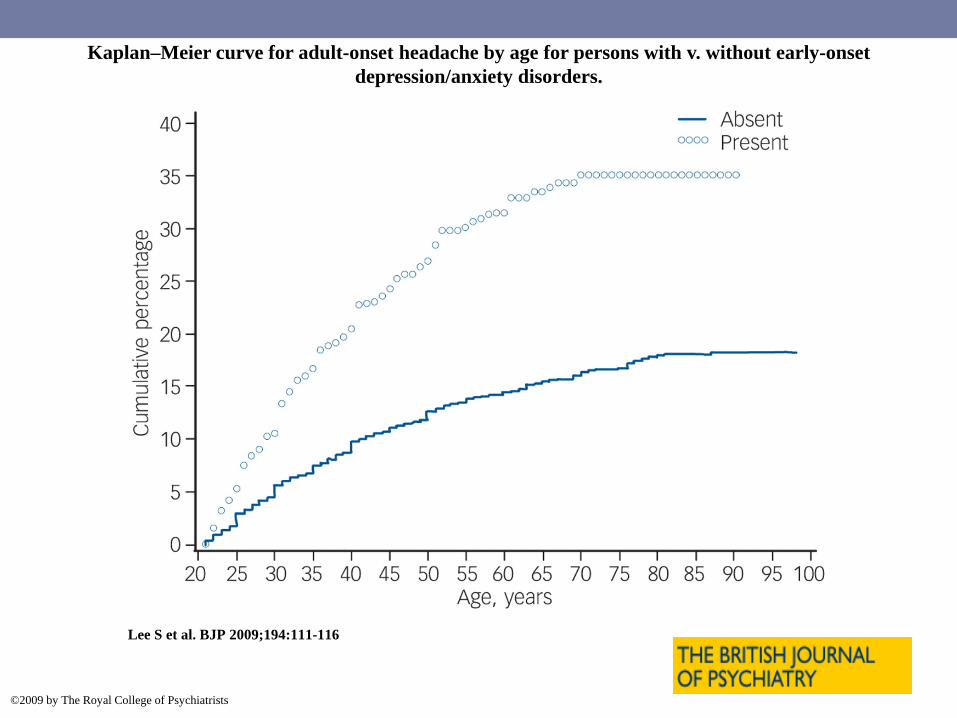
Kaplan–Meier curve for adult-onset headache by age for persons with v. without early-onset depression/anxiety disorders.
Lee S et al. BJP 2009;194:111-116
©2009 by The Royal College of Psychiatrists

What is so special about migraine in women? Three things
• The sex ratios of the 2 most disabling forms of headache are startlingly unequal: suggests special developmental and activational effects
• Comparing men and women with these headaches provides a special window into mechanisms of illness
• Overemphasis on the sex-specific aspects of these headaches is a special pitfall that can limit thinking

Thank you! [email protected]

What this suggests… • Gonadal hormones are important modulators of
migraine and cortical spreading depression (aura) • Probably also of factors underlying cluster headache
• A female preponderance has also been described for
familial (5:2) and sporadic (4.25:1) hemiplegic migraine.









![migraine - public.ppt [Read-Only] · 2012. 3. 20. · recurrent headache that lasts 4that lasts 4- -72 hours72 hours E18% of women E6% of men. Typical Features of Migraine EUsually](https://img.dokumen.tips/doc/110x75/612753e558f13c136d507d55/migraine-read-only-2012-3-20-recurrent-headache-that-lasts-4that-lasts.jpg)


















