Embed Size (px)
Citation preview

Mid-Term Clinical Outcomes Of
Endoscopic versus Open Radial Artery
Harvesting:
a Propensity-score Analysis
Bisleri G1, Giroletti L1, Hrapkowicz T2, Bertuletti M1, Zembala M2,
Arieti M3, Muneretto C1
1University of Brescia Medical School, Brescia, Italy2Silesian Center for Heart Diseases, Zabrze, Poland
3Ospedale di Desenzano, Desenzano, Italy

FINANCIAL DISCLOSURES
- GIANLUIGI BISLERI, MD:
- Karl Storz Gmbh: Inventor, Consultant
- Covidien AG: Consultant

ENDOSCOPIC RADIAL ARTERY HARVESTING
- Revival of radial artery as second conduit of choice for TAR

ENDOSCOPIC RADIAL ARTERY HARVESTING

- Revival of radial artery as second conduit of choice for TAR
- Encouraging outcomes following endoscopic radial harvesting
ENDOSCOPIC RADIAL ARTERY HARVESTING

ENDOSCOPIC RADIAL ARTERY HARVESTING

- Revival of radial artery as second conduit of choice for TAR
- Encouraging outcomes following endoscopic radial harvesting
- Improved technologies for minimally invasive harvesting techniques
ENDOSCOPIC RADIAL ARTERY HARVESTING

SEALED
SYSTEMS
NON-SEALED
SYSTEMS
CO2 insufflation
IS REQUIRED
CO2 insufflation
NOT REQUIRED
ENDOSCOPIC RADIAL ARTERY HARVESTING

- Revival of radial artery as second conduit of choice for TAR
- Encouraging outcomes following endoscopic radial harvesting
- Improved technologies for minimally invasive harvesting techniques
- Potential concerns about detrimental effect of endoscopic technique
ENDOSCOPIC RADIAL ARTERY HARVESTING
- Compare outcomes following OPEN vs ENDOSCOPIC – RA harvesting
- Endoscopic technique with a NON-SEALED approach
STUDY OBJECTIVE

SURGICAL TECHNIQUE

END-POINTS
- PRIMARY:
- Cardiac related mortality
- SECONDARY:
- Freedom from MACCEs (cardiac related mortality,
MI, PTCA re-intervention, REDO surgery, stroke)
- Freedom from sensory discomfort
(pain assessment - VAS score, dysesthesia)
- Forearm wound healing (Hollander scale)

STUDY POPULATION
420 patients
undergoing CABG
Open RA
Harvesting
(Group 1)
n° =313
Endoscopic RA
Harvesting
(Group 2)
n° = 107

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Group 1
Group 2
PRE- MATCH CHARACTERISTICS
*
*
*
P<0.05*

164 patients
Open RA
Harvesting
(Group 1)
n° = 82
Endoscopic RA
Harvesting
(Group 2)
n° = 82
PROPENSITY-MATCHED POPULATION

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Group 1
Group 2
POST- MATCH CHARACTERISTICS
P= NS

0
10
20
30
40
50
60
70
80
90
100
RA on RCA RA on IVP RA on OM RA on PL
Group 1
Group 2
P = NS%
RA TARGET SITE
RCA PDA OM PL

Group 1
Open RA
Harvesting
Group 2
Endoscopic RA
Harvesting
p-Value
Mean RA Harvesting time (min) 40,2 ± 3 37.5 ± 5 0.309
Mean n° graft / patient 2.39 ± 0.68 2.5± 0.71 0.960
Cross Clamp time (min) 53.2 ± 12.1 51.6 ± 9.4 0.923
CPB time (min) 85.2 ± 11.3 88.1 ± 7.2 0.553
INTRA-OPERATIVE CHARACTERISTICS
No conversion to open approach in endoscopic group

Group 1
Open RA
Harvesting
Group 2
Endoscopic RA
Harvesting
P Value
Hand Ischemia 0 0 1
Wound Infection 6 (7.3%) 0 0.007
Sensory alteration 18 (21.9%) 7 (8.5%) 0.0082
Pain (VAS score) 3.2 1.2 <0.05
Wound Healing
(Hollander scale)
3.95 5.1 <0.001
POST-OPERATIVE RA OUTCOMES
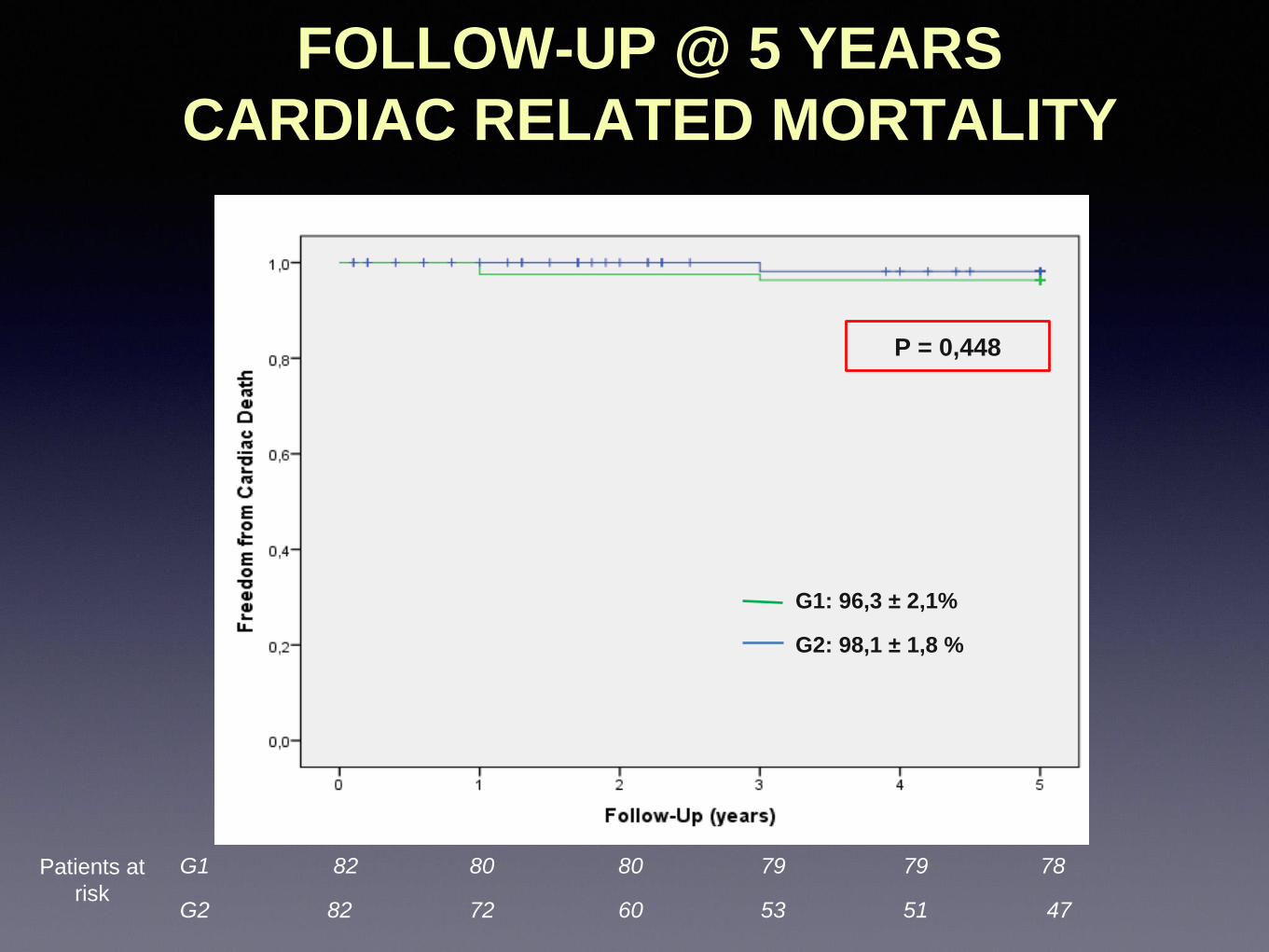
P = 0,448
G1: 96,3 ± 2,1%
G2: 98,1 ± 1,8 %
G1 82 80 80 79 79 78
G2 82 72 60 53 51 47
FOLLOW-UP @ 5 YEARS
CARDIAC RELATED MORTALITY
Patients at
risk
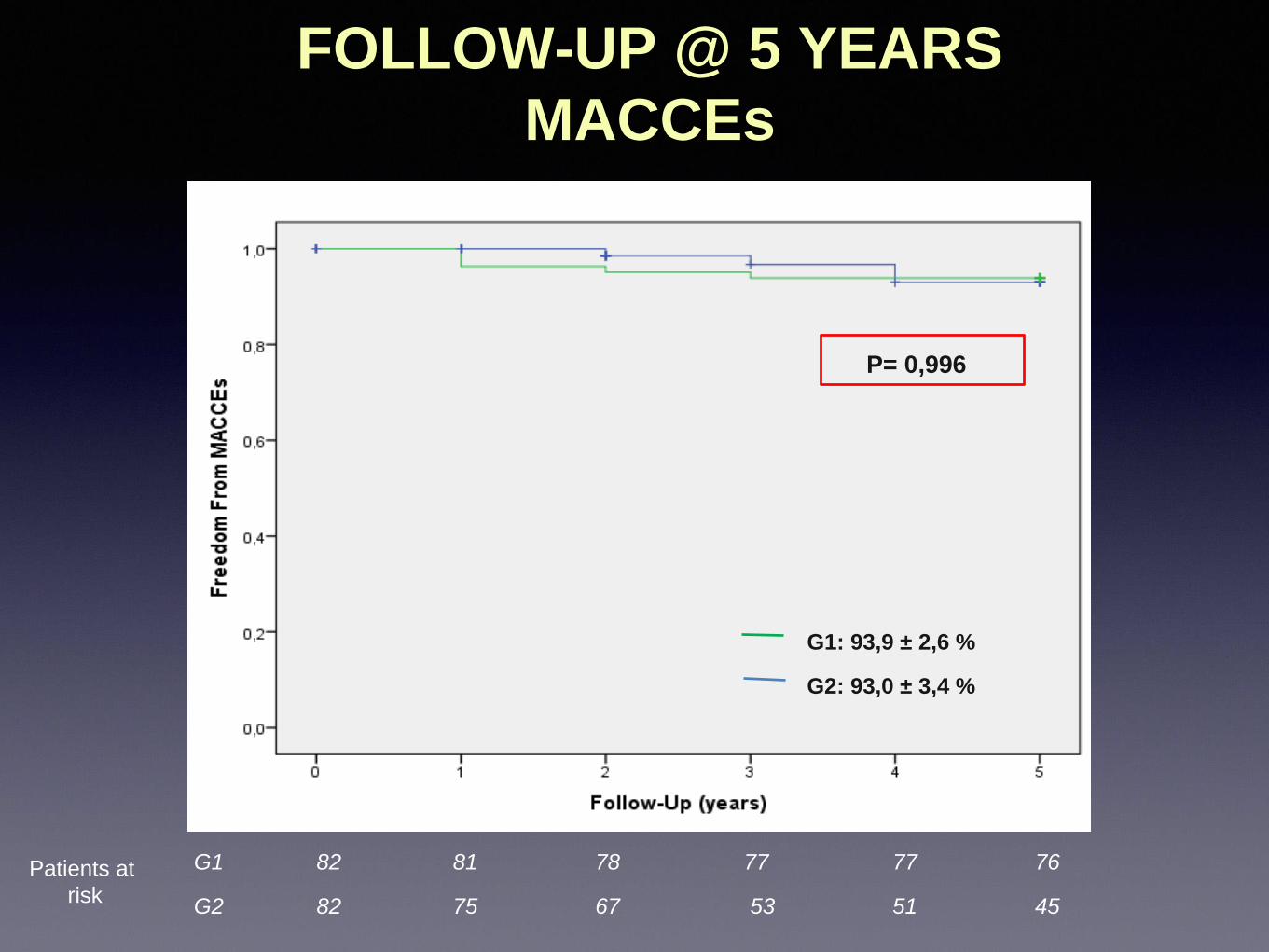
G1 82 81 78 77 77 76
G2 82 75 67 53 51 45
G1: 93,9 ± 2,6 %
G2: 93,0 ± 3,4 %
P= 0,996
FOLLOW-UP @ 5 YEARS
MACCEs
Patients at
risk

FOLLOW-UP @ 5 YEARS
NEUROLOGICAL DISCOMFORT
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Open Group Endoscopic Group
P=0,009

CONCLUSION
-ERAH can be safely performed combining a reusable
retractor and impedance-controlled RF vessel sealer.
-ERAH allows for improved cosmesis, reduced wound and
neurological complications at short term.
-The endoscopic approach IS NOT associated with
detrimental effects in terms of graft related events at 5
years follow-up.





























