Embed Size (px)
Citation preview

Clinical Investigative Study
Microvascular Imaging in Acute Ischemic Stroke
Gunter Seidel, MD, Florian Roessler, MD, Mohamed Al-Khaled, MDFrom the Department of Neurology, Asklepios Klinik Nord – Heidberg, Hamburg, Germany (GS); and Department of Neurology, University of Lubeck, Lubeck,Germany (FR, MA-K).
Keywords: Ischemic stroke, ultrasoundperfusion imaging, microvascular imag-ing, transcranial color-coded sonography.
Acceptance: Received July 18, 2011and in revised from November 8, 2011,Accepted for publication December 7,2011.
Correspondence: Address correspon-dence to Dr. Gunter Seidel, MD, Head ofthe Department of Neurology, AsklepiosKlinik Nord–Heidberg, Tangstedter Land-str. 400–D–22417 Hamburg, Germany.E-mail: [email protected].
Funding sources: none.
J Neuroimaging 2013;23:166-169.DOI: 10.1111/j.1552-6569.2012.00712.x
A B S T R A C T
BACKGROUNDMicrovascular imaging (MVI), a new ultrasound technology, is used to analyze brain per-fusion at the patient’s bedside. This study aims to evaluate the diagnostic and prognosticvalue of MVI in patients with acute ischemic stroke (AIS).METHODSNineteen patients suffering from AIS (mean age, 70.9 ± 12.2 years; 47% female; meanNIHSS-score, 12 ± 8) were investigated within the first 12 hours after symptom onset.We used the iU22 (Philips) system (S5–1 probe; low-mechanical index; depth, 13 cm),and 2 bolus injections of an ultrasound contrast agent (2.4 mL SonoVueTM per injection).The area of maximal perfusion deficit (AMPD) was compared with infarction on follow-upcranial computed tomography (CT) and NIHSS score 24 hours after stroke onset.RESULTSOf 19 patients, 15 patients (79%) had sufficient insonation conditions. Of these patients,12 had infarctions. The sensitivity and specificity of detecting infarctions with ultrasoundperfusion imaging were 91% and 67%, respectively. A significant correlation existedbetween the AMPD and NIHSS score at 24 hours after symptom onset (P = .023), andwith occlusion of the internal carotid artery (P = .005).CONCLUSIONPerforming bedside MVI in the early phase of AIS provides information on brainparenchyma perfusion and prognosis of AIS.
IntroductionSeveral studies1-5 have demonstrated the value of ultrasoundperfusion imaging (UPI) in visualizing the area of perfusiondeficit in patients with acute ischemic stroke. High-mechanicalindex (MI) imaging, which uses contrast microbubble destruc-tion to analyze bolus contrast kinetics in the brain parenchyma,was used in these studies. In the early phase of ischemic stroke,UPI is useful in detecting the area of perfusion deficit and indetermining an early prognosis of stroke. This bedside technol-ogy is available for use in the stroke unit when patients withacute ischemic stroke undergo a color-coded duplex work-upto evaluate their vascular status.
The aim of our explorative study is to evaluate the diag-nostic and prognostic value of microvascular imaging (MVI), anew UPI technology, which uses low MI that detects contrastagent in the cerebral microcirculation in real time. After onedestructive ultrasound pulse is performed, the replenishmentof contrast agent can be analyzed in real time, because low MIleads not to microbubble destruction. Investigation time is veryshort (up to only 7 seconds), therefore several imaging planescan be analyzed after a single contrast bolus injection. With thisnew method, we analyze brain perfusion in patients with acuteischemic stroke at a very early phase (<12 hours) and compare
with results of follow-up cranial computed tomography (CCT),and with clinical outcome 24 hours after stroke onset.
Methods and PatientsWe prospectively investigated patients suffering from acute is-chemic stroke with hemispheric symptoms after informed con-sent was given. We performed a clinical follow-up investigationat 24 ± 2 hours after symptom onset. The inclusion criterion wasthe onset of stroke symptoms less than 12 hours before the ultra-sound investigation. In all patients, CCT or magnetic resonancetomography (MRT) was performed as part of our routine pro-tocol. Exclusion criteria were intracranial hemorrhage detectedby CCT, pregnancy, and severe pulmonary or renal disease.A neurologic examination, which included the National Insti-tutes of Health Stroke Scale (NIHSS), was performed before theinvestigation. The baseline characteristic and the neurosonog-raphy findings of the brain-supplying arteries are displayed inTable 1.
Ultrasound Contrast Agent
SonoVueTM (Bracco) was used as an ultrasound contrast agent,which is routinely administered for the assessment of basal cere-bral arteries in patients with insufficient insonation conditions.
166 Copyright ◦C 2012 by the American Society of Neuroimaging

Table 1. Baseline characteristics∗
Baseline Characteristics All Patients, n = 19
Age, years, mean (SD) 70.9(12)Female sex 9(47)NIHSS score at admission, mean (SD) 12(8)Treatment with TPA 11(57)Time to assessment, hours mean (SD) 3.6(3)Dulexsonography finding of the symptomatic side –
ICA-occlusion 5(26)ICA-stenosis ≥50% 2(11)VA-occlusion/stenosis 0(0)MCA-occlusion 8(42)MCA-stenosis 1(5)ACA-occlusion/stenosis 0(0)PCA-occlusion/stenosis 1(5)
Detection of infarct on initial CCT 3(16)
NIHSS = National Institutes of Health Stroke Scale; TPA = tissue plasminogenactivator; ICA = internal carotid artery; VA = vertebral artery; MCA = middlecerebral artery; ACA = anterior cerebral artery; PCA = posterior cerebral artery;CCT = cranial computed tomography.∗Values are in number and (%) unless otherwise indicated.
We administered SonoVueTM (2.4-mL dose) as a bolus injec-tion. The injection line was flushed with 10 mL saline.
Ultrasound Perfusion Imaging
We used an iU22 ultrasound system (Philips Medical Systems)with a 1 to 5 MHz sector transducer (S5–1 probe) for the tran-scranial investigation and a 7.5-MHz sector transducer (L9–3probe) for the extracranial investigation. Before UPI was per-formed, extra- and transcranial color-coded duplex sonographywas conducted to assess the vascular status, and to determinethe transtemporal insonation conditions. MVI uses speciallydesigned post-processing software to map contrast agent pro-gression. The technique measures changes in the image fromframe to frame, suppressing background tissue signals and cap-turing additional contrast data. The additional data obtainedusing MVI dramatically enhances vessel conspicuity. An im-portant biophysical parameter is the mechanical index. Thisindex is an estimate of the maximum amplitude of the pressurepulse in tissue. It gives an indication as to the relative risk ofmechanical effects (streaming and cavitation). In the study weused a combination of a short destruction high-MI pulse (MI,.58) followed by low MI (MI, .15) in the real-time mode, whichtraces contrast reflow in the brain volume under investigation.Perfusion deficit was defined as no detectable ultrasound signalafter 7 seconds of sampling time. In each patient, UPI was per-formed with a maximum depth of 130 mm in the symptomatichemisphere. We used the axial imaging plane. Image loopswere stored in the ultrasound system for later offline analysisto measure the maximal area of perfusion deficit with QLabTM
software (Philips Medical Systems).
Statistics
We analyzed the data with a Statistical Product and ServiceSolutions (SPSS) software program (version, Predictive Analyt-ics Software [PASW] Statistics 18) and determined the mean,range, and standard deviation values to describe the data. Tocalculate the correlation between nonparametric variables, the
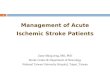
Fig 1. Panels A and B. Follow-up CCT at day 3 and MVI image (11.5hours after symptom onset) from a 41-years-old female suffering frominfarction in the MCA- and ACA territory. Notice the missing brightsignal in the ultrasound image in projection of the MCA and ACAterritory (arrows). The patient showed malignant course of the ACAand MCA infarction so hemicraniectomy was performed at day 2.∗indicates third ventricle. Panels C and D. Follow-up CCT at day 2and MVI image 2 hours after symptom onset (B) from a 85-years-old male suffering from MCA infarction due to M1-MCA occlusion.Notice the small MVI deficit in the insular cortex (arrows). In thefollow-up CCT a small cortical infarction in the insular region couldbe displayed.
Spearman rank correlation coefficient test was performed. Weused a t-test to determine the correlation between nonpara-metric variables. A significant correlation was assumed forP < .05.
ResultsNineteen patients (9 women, 10 men; mean age, 70.9 ± 12.2years; range, 41–84 years) suffering from acute ischemic stroke,with a mean initial NIHSS score of 12 points (range, 2–30),were included in our prospective study. At least 1 CCT scan,as part of our routine protocol, was performed for 17 strokepatients. For 2 patients, an MRI scan was performed as a pri-mary imaging tool. The mean time between the first symptomsof acute stroke and the ultrasound investigation was 3.6 hours(range, 1.1–11.5 hours). Systemic tissue plasminogen activator(tPA) therapy was performed in 11 of 19 patients (58%). Suf-ficient insonation conditions were present in 15 of 19 patients(79%). In these patients, only a transcranial ultrasound exami-nation could be performed. With UPI, we detected a perfusiondeficit in 12 of 15 patients (80%). Of these patients, 8 had mid-dle cerebral artery (MCA) infarctions, 2 had MCA and anteriorcerebral artery (ACA) infarctions, and 2 had posterior cerebralartery (PCA) infarctions. In Figure 1, UPI scans and follow-upCCT scans are shown of a patient suffering from ACA andMCA infarctions, and of another patient suffering from a smallMCA infarction. In both patients, the M1-segment of MCAwas occluded at the initial ultrasound investigation, indicating
Seidel et al: Microvascular Imaging 167

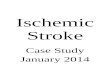
Fig 2. Diagram shows the correlation between the area of maximal perfusions deficit (AMPD) and the NIHSS at 24 hours after symptomonset, P = .023.
an excellent collateral flow in the patient with the small corticalMCA infarction. In 3 patients, UPI could not detect a perfusiondeficit. Follow-up CCT and MRT did not reveal an infarctionin 2 of these patients. One patient had a small cortical MCAinfarct was detected with MRI. The sensitivity and specificity,for detecting a perfusion deficit in the early course of the dis-ease in patients who had an infarction were 91% and 67%,respectively, in the follow-up investigation with the referencemethod (CCT, MRT). The mean area of maximal perfusiondeficit (AMPD) in the axial UPI scan was 1152 ± 709 mm2. TheAMPD in patients who had an internal carotid artery occlusionwas significantly greater than in those without an ICA-occlusion(1755 vs 862 mm2, respectively; P = .005). A greater area ofdisturbed perfusion was also found in patients with an MCAocclusion compared to patients with patent MCA (1371 vs779 mm2, respectively; P = .061), but the results failed to showsignificance. The AMPD value correlated significantly with theNIHSS score at 24 hours after symptom onset (Spearman rankcorrelation coefficient [rs], .602; P = .023; Fig 2). No significantcorrelation existed between the AMPD and the initial NIHSSscore before the investigation. No clinical or side effects oc-curred that could be related to the administration of the contrastagent.
DiscussionIn the past few years, evidence has mounted that blood flowin the microcirculation of the brain can be depicted with ul-trasound perfusion technologies. These technologies can beused to visualize brain perfusion deficits in patients with acuteMCA stroke.6-8 Performing low MI real-time UPI with theflush-replenishment technique for the evaluation of contrast ki-netics has several advantages over previous high MI triggeredultrasound techniques. Because low-MI techniques have verylow-scanning times, multiple imaging studies can be performedwithin the time it takes for one bolus injection of contrast agentto be administered.9,10
Kern et al demonstrated that real-time UPI with low MIidentifies correctly the ischemic brain tissue in patients withan acute MCA stroke, compared with the results of diffusion-weighted and perfusion MRI.11
Our study shows that MVI, a fast and simple qualitativemethod for detecting ultrasound contrast replenishment afterdestruction in the brain tissue, is useful in evaluating patientsin the early phase of acute ischemic stroke. The sensitivity ofpredicting infarction was high, but the specificity was only mod-erate. We found a significant correlation between the area ofmaximal perfusion deficit and the NIHSS score at 24 hours
168 Journal of Neuroimaging Vol 23 No 2 April 2013

after symptom onset, which is a predictor of clinical outcome.12
This together with the results of an earlier ultrasound perfusionstudy1 indicates that the maximal area of perfusion deficit isan additional early predictor for the clinical outcome after is-chemic stroke. One limitation of low-MI imaging is the pen-etration rate, particularly in moderate temporal acoustic bonewindows. The success rate of approximately 80% in our study isin accordance with another study that used UPI techniques.13
As described in previous studies using high-MI imaging, wealso found strip and edge artifacts in nearly every investigation.The safety of using SonoVueTM has been documented in nu-merous brain perfusion studies.13,14 Similar to previous studies,patients who were administered SonoVueTM in this study didnot exhibit side effects.
In conclusion, the low MI flush-replenishment technique to-gether with MVI post-processing is a promising tool for analyz-ing brain perfusion in the early phase of supratentorial ischemicstroke, and for predicting size of infarction and early prognosis.Future studies should focus on comparing UPI and perfusionMRI so as to investigate the threshold of perfusion detectionand low-perfusion state in the border zone of an absent contrastsignal.
References1. Seidel G, Meyer-Wiethe K, Berdien G, et al. Ultrasound perfu-
sion imaging in acute middle cerebral artery infarction predictsoutcome. Stroke 2004;35:1107-1111.
2. Kern R, Perren F, Schoeneberger K, et al. Ultrasound microbubbledestruction imgaging in acute middle cerebral artery stroke. Stroke2004;35:1665-1670.
3. Seidel G, Algermissen C, Christoph A, et al. Visualization of brainperfusion with ultrasound. Stroke 2000;31:151-154.
4. Seidel G, Albers T, Meyer K, et al. Perfusion harmonic imaging inacute middle artery infarction. Ultrasound Med Biol 2003;29:1245-1251.
5. Wiesmann M, Meyer, Albers T, et al. Parametric perfusion imag-ing with contrast-enhanced ultrasound in acute ischemic stroke.Stroke 2004;35:508-513.
6. Postert T, Federlein J, Weber S, et al. Second harmonic imaging inacute middle cerebral artery infarction: preliminary results. Stroke1999;30:1702-1706.
7. Eyding J, Krogias C, Wilkening W, et al. Detection of cerebralperfusion abnormalities in acute stroke using phase inversion har-monic imaging (PIHI): preliminary results. J Neurol Neurosurg Psy-chiatry 2004;75:926-929.
8. Stolz E, Allendorfer J, Jauss M, et al. Sonographic har-monic grey scale imaging of brain perfusion: scope of a newmethod demonstrated in selected cases. Ultraschall Med 2002;23:320-324.
9. Meairs S. Contrast-enhanced ultrasound perfusion imaging inacute stroke patients. Eur Neurol 2008;59:17-26.
10. Meyer K, Wiesmann M, Albers T, et al. Harmonic imaging in acutestroke: detection of a cerebral perfusion deficit with ultrasound andperfusion MRT. J Neuroimaging 2003;13:166-168.
11. Kern R, Diels A, Pettenpohl J, et al. Real-time ultrasound brainperfusion imaging with analysis of microbubble replenishment inacute MCA stroke. J Cereb Blood Flow Metab 2011;31:1716-24.
12. Kwakkel G, Veerbeek JM, van Wegen EE, et al. Predictivevalue of the NIHSS for ADL outcome after ischemic hemisphericstroke: does timing of early assessment matter? J Neurol Sci 201015;294:57-61.
13. Kaps M, Seidel G, Bokor D, et al. Safety and ultrasound-enhancingof an new sulfur hexaflouridecontaining agent in the cerebral cir-culation. J Neuroimaging 1999;9:150-154.
14. Hynynen K, McDannold N, Sheikov NA, et al. Local and re-versible blood brain barrier disruption by noninvasive focusedat frequencies suitable for trans-skull sonications. Neuroimage2005;24:12-20.
Seidel et al: Microvascular Imaging 169