Embed Size (px)
Citation preview

1
Methylglyoxal, a Diabetic Biomarker for Insulin Resistance, Vascular Dysfunction and Neuropathies
Yousif A Shamsaldeen, Louise S Mackenzie, Lisa A Lione and Christopher D Benham
Abstract: Diabetes mellitus is a pandemic metabolic disease characterized by chronically elevated blood glucose concentration due to insulin dysfunction. Diabetics are prone to limbs fungal infections and ulcers due to vascular injury and end-organ damage such as nephropathy, retinopathy and neuropathic pain all of which are associated with methylglyoxal elevation. Methylglyoxal is generated through carbohydrate, lipid and protein metabolism which are all found to be exacerbated in diabetes. Moreover, methylglyoxal is highly reactive with various cellular and interstitial molecules such as proteins and phospholipids to form stable adducts and advanced glycation end products. Methylglyoxal induces insulin resistance, pancreatic β-cells cytotoxicity, and induces endothelial dysfunction that accelerates retinopathy, another diabetes complication. Additionally, methylglyoxal induces hyperalgesia and neuronal inflammation associated with neuropathic pain. Therefore, methylglyoxal might represent a potential therapeutic target in diabetes and associated complications.

2
1. Introduction:
Diabetes mellitus (DM) is a pandemic metabolic disease characterized by chronically
elevated blood glucose concentration (hyperglycaemia) due to insulin dysfunction which is
attributed to insufficient -or blunted- insulin secretion and/or declined tissue sensitivity to
insulin1. The incidence of diabetes mellitus is increasing throughout the world and numbers
are expected to reach 592 million by the year 2035, mainly because of the increase in
obesity2. Approximately 50% of diabetics show diabetes complications by the time when
they are diagnosed3. Approximately 5 million people died from diabetes in 2014 globally
which accounts for a death every 7 seconds4. Despite the differences in aetiology, clinical
presentation, and disease prevalence, secondary complications, such as neuropathic pain,
occur in both type 1 and 2 diabetes mellitus5. Diabetes complications lead to a reduced
quality of life posing a huge economic burden to the health system and society5. In 2011 in
the UK, the NHS spent almost £24 billion on diabetes, 30% of which was spent on managing
complications, such as neuropathic pain. By 2035, it is estimated that diabetes will cost the
NHS approximately £40 billion, accounting for 17% of total health resource expenditure6.
Among diabetic patients approximately 10% are diagnosed with type-1-DM (T1DM) which is
mainly attributed to autoimmune activity where expressed plasma islet-cells antibodies
destroy pancreatic β-cells1, 7. Children, under 12 years comprise the majority of T1DM
patients who require life-long insulin treatment for survival. However, there are two types
of monogenic diabetes which are commonly misdiagnosed as T1DM due to early onset of
disease. These are neonatal diabetes (ND) which is diagnosed in the first 6 months of life,
whereas the second type; maturity-onset diabetes of the young (MODY) affects individuals
younger than 25 years, controlled largely through the use of sulphonylureas such as
glibenclamide7.
The large majority of diabetics, are of type-2-DM (T2DM), which is regarded as a complex
disease that embraces genetic factors, lifestyle, age, obesity, pregnancy and gender as risk
factors8. Unlike T1DM, patients of T2DM usually do not require insulin to survive since
insulin secretion is only partially deficient and/or the individual is insulin resistant. Insulin
resistance is mainly attributed to chronically elevated levels of insulin reducing sensitivity
and further increased by abdominal fat and hence obesity1. Reduced insulin secretion may
be due to insulin signalling cascade alteration and/or reduced pancreatic β-cells mass,

3
however, the extent of pancreatic β-cells mass reduction is controversial as some studies
stated that 65% loss of pancreatic β-cells is sufficient to induce diabetes9 while other studies
concluded that 10% reduction of pancreatic β-cells mass is also associated with numerous
altered insulin signalling components that initiate diabetes10.
2. Methylglyoxal and diabetes:
In addition to the previously mentioned diabetes complications, diabetics suffer from
frequent: thirst (polydipsia), urination (polyuria) and hunger (polyphagia)1 , these common
complications are recently found to be associated with plasma/tissue methylglyoxal (MGO)
elevation (Table 1).
Chronic hyperglycaemia is the main DM complication where blood glucose concentration
exceeds 7mmol/L (125mg/dl). This results in an increasing proportion of glucose metabolism
(approximately 0.5% of glycolysis), passing down alternate pathways to generate reactive
oxygen species (ROS) such as MGO that is highly reactive with various cellular and interstitial
molecules such as proteins and phospholipids to form stable adducts and advanced
glycation end products (AGE)11 12. Upon forming AGE, MGO is trapped intracellularly and
subsequently increases oxidative stress (OS) that disrupts the cellular membrane integrity
and thereby allows MGO leakage to the serum from where it can be measured for disease
progression and severity11 13 14. Physiological human plasma MGO concentration is
approximately 150nM and is doubled in T2DM patients’ plasma15. Moreover, glycolysis-
derived MGO interacts with cellular proteins and nucleic acids to accelerate AGE production
resulting in pancreatic β-cell cytotoxicity. This exacerbates hyperglycaemia and hence DM
complications11. However, clinical studies have failed to significantly correlate MGO to blood
glucose concentration due to 2 main technical reasons, (i) firstly it is essential to dissociate
MGO from protein without causing any DNA damage and/or oxidation to accurately
measure total MGO, and (ii) the heterogeneity of the samples due to diverse patient
backgrounds14.

4
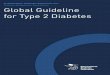
2.1. MGO sources:
Being an AGE precursor, MGO levels have been widely studied14. The 4 main MGO sources
are summarized in the following formula:
MGO total = MGO carbohydrates + MGO lipids + MGO proteins + MGO exogenous
As shown in figure 1, three main integrated metabolic pathways are involved in MGO
formation:
1. Carbohydrates:
Reducing sugars are able to react with proteins’ amino groups to yield Schiff’s base
which is structurally rearranged into Amadori product to be subjected to series of
reactions that generate AGE12. Accordingly, MGO is generated mainly through
phosphorylating glycolysis such as triose-phosphate enzymatic metabolism which
was found to be increased in hyperglycaemia, the pentose phosphate shunt, sorbitol
pathways such as xylitol metabolism and fourthly glucoxidation14 16. Moreover,
triose-phosphate accumulation is involved in diabetic nephropathy revealing the
involvement of carbohydrate generated MGO pathway in diabetes complication and
such a pathway was shown to be inhibited through thiamine17 18 (figure 1).
2. Lipid pathways:
Lipid peroxidation of polyunsaturated fatty acids yields short chain; 3-9 carbon long
fragment molecules of highly reactive aldehyde such as 2-Alkenol, 4-hydroxy-2-
alkenal as well as ketoaldehydes from which glyoxal compounds such as MGO is
generated from non-enzymatic and enzymatic metabolism of acetoacetate or
acetone intermediates, respectively12 14. Acetoacetate is a major ketone body (KB)
elevated in type 2 diabetics’ plasma19. Moreover, lipolysis shares a common
intermediate with carbohydrate metabolism; triose-phosphate through α-glycero-
phosphate dehydrogenase-metabolized glycerol14. Previous studies found that
lipolysis is increased in diabetes and suppression of lipolysis improves insulin
sensitivity and glucose utilization20 21. Moreover, isopropyl alcohol (IP) is significantly
increased (5mg/dl) in ketoacidosis diabetic plasma22. IP is a metabolite of acetone, as

5
the reaction is governed by alcohol dehydrogenase which favours the production of
IP when acetone is increased as in diabetes mellitus where glucose utilization is
compromised, and the body adapts the energy supply toward fatty acid oxidation
through NAD+ reduction into NADH. Therefore, when NADH/NAD+ ratio is increased,
NADH is utilized to produce IP from acetone22 23.
3. Protein metabolism:
Numerous in vitro studies demonstrate the vulnerability of tyrosine, serine,
threonine and glycine rich proteins toward oxidation as these residues are
enzymatically converted to acetone and aminoacetone intermediates which are
converted into MGO12 14. Moreover, semi-carbazide sensitive amine oxidase (SSAO)
which converts aminoacetone into MGO and hydrogen peroxide is the only enzyme
found elevated in diabetic plasma14. Protein catabolism is increased by
approximately 50% in streptozotocin treated rats, and this increased rate of protein
catabolism is attributed to insulin resistance and increased glucocorticoids
production in normal rats24.
4. Exogenous MGO:
AGE are ingested through heated and processed fats, proteins (Maillard reaction) as
well as sugars and tobacco25, whereas previous studies revealed that coffee and
whiskies are the main MGO-containing beverages26 27. The average daily
consumption of AGE is
16000kU AGE (kilo unit AGE per gram of serving size) which is even aggravated by
high temperature processing such as oven frying that increases the AGE content of
chicken breast to 900kU/g compared to boiled chicken breast
(100kU AGE/g)28. Chronic consumption of AGE-containing food/beverages causes
mild liver inflammation as well as fat disposition on parenchymal cells which alters
fasting insulin and thereby reduces glucose tolerance according to previous research
conducted on rat hepatocytes 27. In the Maillard reaction, reducing sugars such as
glucose interact with free amino groups found in proteins to form for instance
N-substituted glycosylamine which in the presence of water goes through Amadori
rearrangement to yield Amadori product, 1-amino-1-deoxy-2-ketose29. The

6
rearranged Amadori product (RAP) is then degraded through 2,3 enolisation to form
numerous fission products such as acetol, pyruvaldehyde and diacetyl compounds at
pH˃729. These carbonyl compounds are highly reactive with amino acids to form
aldehydes and α-aminoketones29. Previous studies found that Maillard reaction
products are significantly increased in diabetics’ skin collagen as Nε-carboxymethyl
lysine (CML), fructoselysine (FL) and pentosidine which are associated with
accelerated aging30. Additionally, CML is significantly elevated in diabetic plasma
when compared to healthy plasma, and such elevation is exacerbated when purely
prepared AGE beverages were ingested22. This elevation was associated with altered
vascular function through supressing the expression and function of eNOS as well as
stimulating the release of vascular cells adhesion molecules (VCAM-1)25.
2.2. MGO metabolism:
Two glutathione (GSH) dependent pathways contribute to MGO metabolism; glyoxalase
system (GLO), glyoxalase 1 and glyoxalase 2 (GLO1 & GLO2) and aldose reductase, of which
GLO-1 is the major pathway that converts MGO it to non-toxic D-lactate14 31. However, as
11% of glucose is metabolized through the sorbitol pathway, the bi-modal aldose reductase
acts as aldehyde reductase rather than ketone reductase and thereby preferentially
produces acetol which thereafter is converted retrospectively to MGO through CYP2E1 to
start a futile cycle that depletes the intracellular GSH and elevates acetol in diabetic
plasma14.

7
Figure 1 Endogenous sources of methylglyoxal (MGO) from glucose, lipid and protein metabolism. (A) Normal
non-diabetic condition shows low MGO production from un-affected glycolysis, lipolysis or proteolysis with
major sources represented in bold arrows. (B) Diabetes is associated with increased MGO production from
hyperglycaemia, accelerated lipolysis and proteolysis represented with thick borders and bold arrows which
are accompanied with compromised glyoxalase activity.
B
A

8
2.3. MGO and insulin:
Insulin secretion is a calcium-dependent cascade which starts when pancreatic β-cells
glucose-transporter-1 (GLUT-1) take up glucose due to elevated plasma-glucose. This results
in ATP synthesis and potassium ATP channel (KATP) closure. Once KATP are closed, Calcium
ions (Ca+2) enter through Voltage gated Ca+2 channels initiating insulin exocytosis32.
However, glucose is not the only insulin release stimulator as lipids and proteins are also
insulin secretagogues, in addition to other neurotransmitters and hormones such as
incretins which stimulate insulin secretion independently from Ca+2 as illustrated in figure
27.
Insulin resistance is a complex condition where a normal insulin concentration is not
sufficient to mediate glucose uptake and utilization due to insulin signalling disruption and
hence, more insulin is released to try to maintain glucose homeostasis33 34. MGO has been
shown to bind with insulin through targeting arginine residues located in chain B and at N-
terminus33. Subsequently, MGO-modified insulin chain B is heavier than free insulin by an
additional 126Da resulting in less glucose uptake and utilization. This has been
demonstrated in skeletal muscle L8 cells and 3T3-L1 adipocytes as well as a 50% reduction in
metabolism in H4-II-E hepatocytes33. This study is further supported by the fact that insulin
receptor substrate-1 (IRS-1) phosphorylation and PI3K activity are both suppressed dose
dependently following MGO and reversed with MGO scavenger; N-acetylcysteine34 (Table
1). Moreover, MGO (100μM) induces pancreatic β-cytotoxicity when applied to RINmf5
insulin secreting cells in culture11. Such an effect is comparable to a high glucose (16mM) apoptotic
effect on rat pancreatic β-cells11. These findings suggest that MGO might play a major role in
progressive stages of diabetes where chronic hyperglycaemia yields elevated MGO that reduces
insulin signalling and pancreatic β-cells numbers leading to a further reduction in insulin secretion11
(Figure 2). Moreover, when MGO 60mg/kg/day was infused in Sprague-Dawley rats for 28 days, it
resulted in a significant reduction in plasma insulin and a significant increase in fasting plasma
glucose. Additionally, plasma and pancreatic, muscle and, adipocyte tissues were all characterized by
significant MGO elevation associated with significant decrease in glutathione (GSH) and adipocyte
plasma membrane glucose transporter-4 (GLUT-4) as well as pancreatic GLUT-2 35.
Insulin binds to its corresponding tyrosine-kinase coupled endothelial receptor, insulin receptor (IR)
which is phosphorylated and provides a docking site for insulin receptor substrate-1 (IRS-1) to bind.
As it exerts tyrosine-kinase activity, IR phosphorylates IRS-1 to unveil an interactive sulfhydryl

9
(SH2) domain which is responsible for activating phosphatidylinositol 3-kinase /protein
kinase B (PI-3K/PKB) as well as Ras-mitogen activated protein kinase (MAPK) pathways.
These pathways phosphorylate approximately 40 cellular targets including Akt-dependent
endothelial nitric oxide synthase (eNOS) that generates nitric oxide (NO) to yield
endothelium-dependent vasodilation34 36 37 38. Therefore, MGO-induced insulin dysfunction
(reduced secretion and increased resistance) might directly cause vascular dysfunction, a
common complication in diabetes37 (Figure 3).

10
Figure 2 Insulin release from pancreatic β-cells through calcium dependent and independent pathways. GLUT-1 takes up glucose which is metabolised through glucokinase (GCK) to glucose-6-phophate which is metabolised in the mitochondria to generate ATP. A rise in [ATP] stimulates the closure of potassium ATP channels and depolarisation that triggers Ca+2 influx. Whereas glucagon like peptide-1 (GLP-1) stimulates insulin secretion via an exchange protein activated by cAMP (EPAC) and protein kinase A (PKA)-dependent mechanism which are activated through cyclic adenosine monophosphate (cAMP). Plus signs reveal stimulation. (A) normal insulin secretion. (B) Methylglyoxal (MGO) is toxic to pancreatic β-cells and forms insulin-adducts which endows insulin with higher molecular weight and less activity.
2.4. MGO and vasculature:
B
A

11
Numerous authors correlate highly accumulated MGO to vascular and other end organ
damage such as nephropathy and neuropathy39. Vascular dysfunction is a common
complication in DM which may culminate with renal failure, blindness and limb
amputation40 41.
As a highly reactive aldehyde MGO forms stable adducts when reacting with multiple
macromolecules through preferentially targeted aminoacids as for instance lysine;
Nε-carboxyethyl lysine (CEL), MGO-derived lysine-lysine dimer (MOLD), arginine; 5-
methylimidazolone, tetra-hydropyrimidine and argpyrimidine as well as sulfhydryl group-
containing cysteine which forms stabilized S-lactyl cysteine through keto-enol tautoumerism
from which CEL and MOLD are both elevated in DM12. Accordingly, MGO inhibits eNOS
through inhibiting the phosphorylation of serine 1177, thereby inhibiting NO production and
yielding vascular dysfunction40 (Figure 3). Moreover, rat thoracic aortic smooth muscle cells
(ASMC) treated with MGO (100μM) induces NO production and upon further investigations,
the researchers found that H2O2 generation was also enhanced39. Furthermore, induced NO
reacts with peroxides (O.2) forming the highly reactive oxidant peroxynitrite (ONOO-) so that
NO is bound and thereby physiologically non-functional. In addition, ONOO- itself is
considered as an essential atherosclerotic factor39. Furthermore, immunohistochemical-
based observations in kidneys from diabetic patients show increased argpyrimidine
formation in patient arteries suggesting MGO induces arterial injury as a further DM
complication42. Vascular function restoration in GLO-1-overexpressed STZ treated animals is
accompanied by MGO and AGE reduction and another study showed vascular function
restoration through MGO scavengers such as diacetyl cysteine40 41 (Table 1).
MGO is also a redox-based cell signalling regulator39, which oxidizes GSH to GSSH through
irreversible binding to arginine and thereby alters the cellular redox system which pushed
the cell toward oxidative stress-induced apoptosis33.
MGO blocks insulin-stimulated eNOS phosphorylation at serine-1177 and threonine-497 and
also inhibited tyrosine phosphorylation of IRS-1 and Akt37. GLO-1 inhibition results in
elevation of MGO and showed similar inhibitory effects on eNOS, IRS-1 and Akt
phosphorylation. Moreover, in vivo studies on mice administered i.p MGO 50-75mg/kg/day
for 5 consecutive days/week for 7 weeks showed significant insulin resistance accompanied
with compromised endothelial function that was attributed to IRS-1 inhibition through

12
serine-616 phosphorylation and eNOS signalling suppression37 (Figure 3). Additionally,
endothelial dysfunction is accompanied by an increase in oxidative stress markers such as
the vascular monocytes chemoattractant peptide-1 (MCP-1) and RAGE expression in Wistar
and Goto-Kakizaki rats43. Tetrahydropyrimidine (THP), an AGE product of MGO was elevated
in T1DM compared to non-diabetics (115.5U/μl vs 109.8U/μl) and such elevation was
strongly associated with an endothelial dysfunction marker, soluble vascular cell adhesion
molecule-1 (sVCAM-1) and phospholipase-A2 (sPLA2), a low grade inflammatory marker.
This data suggests MGO as a diabetic marker for vascular dysfunction44.
These diabetic vascular complications are commonly associated with retinopathy. MGO-
derived CML, CEL and hydroimidazalone-1 (MG-H1) are increased in diabetic wild type (WT)
rat retina but not in diabetic GLO-1 overexpressing transgenic rats or in non-diabetic rats.
GLO-1 overexpression prevented the generation of new capillaries in acellular tissues in
central and peripheral regions of retina as well as preventing cellular capillary
degeneration45.
In addition to all these vascular complications, the lifespan of erythrocytes (RBC) is reduced
in diabetes. The MGO concentration is doubled in diabetics’ RBC and elevated by fourfold in
diabetics’ plasma compared to non-diabetics’46. MGO accelerates RBC suicidal death,
eryptosis through enhancing phosphatidylserine exposure on the cell surface, a signal that
triggers cell death. Further, MGO was shown to reduce ATP and GSH levels in RBCs which
would accelerates eryptosis46 47. Moreover, ROS increment in haemodialysis patients (HD)
reveals that cell injury is a major factor that corresponds to ROS leakage and plasma ROS
increment, a fact that is supported by recent studies showing ROS such as methylglyoxal
induces RBC injury14 48.

13
Figure 3 Methylglyoxal (MGO) induces vascular dysfunction by interfering with insulin signalling. (A) Normal endothelial vasodilation stimulated through insulin binding to its insulin receptor (IR) which is phosphorylated to unveil intracellular binding site for insulin receptor substrate-1 (IRS-1) which is phosphorylated upon binding. Phosphorylated IRS-1 provides a sulfhydryl (SH2) residue which is then bound with phosphatidylinositol 3-kinase (PI3K) that phopsphorylates protein kinase B (PKB) which phosphorylates and activates Akt that activates endothelial nitric oxide synthase to generate nitric oxide (NO). NO diffuses into smooth muscle cells (SMCs) causing vasodilation (VD). (B) MGO reduces insulin secretion through pancreatic β-cells toxicity, binds to insulin forming the less active insulin-MGO adduct and inhibiting eNOS phosphorylation which results in less NO production and compromised endothelial vasodilation.
B
A

14
2.5. MGO and neuropathic pain:
Diabetes is one of the leading causes of chronic neuropathic pain 5. Neuropathic pain occurs
in both Type 1 and Type 2 diabetics and given the heterogeneity of mechanisms that drives
neuropathic pain in patients and over time, it is challenging to identify an optimum
treatment strategy5. Among the major diabetic complications is diabetic neuropathy where
nociception is exacerbated due to diabetes13. A recent study found diabetic plasma MGO
was approximately doubled and reached 1µM in diabetic individuals with hyperalgesia
which was associated with increased COX-2 expression and suppressed GLO-1 activity31.
In mice, MGO induced heat hyperalgesia in a dose dependent manner when administered in
WT mice31. Moreover, STZ diabetic mice showed GLO suppression which was associated
withand hyperalgesia, and such complication was reproduced in WT mice when GLO
expression was supressed31. MGO acutely depolarises the resting membrane potential in
sensory neurons increasing their excitability. Such neuropathic events were shown to be
NaV1.8 –dependent, as these events were absent in NaV1.8 –KO mice31Molecular studies
showed MGO triggers changes in NaV1.8 gating through DIII-DIV linker’s arginine residue
modification in mice dorsal root ganglion (DRG)31.
Furthermore, MGO increases the release of calcitonin gene related peptide (CGRP) in
peripheral nerves and nerve conduction in STZ-diabetic and control mice31. These neuronal
events are also accompanied by an increase in cerebral blood flow to areas associated with
nociception31.
A further mechanism for exacerbation of diabetic neuropathy is activation by MGO of
human ankyrin transient receptor potential TRPA1. An effect which was blocked by the
TRPA1 antagonist (HC030031)13. TRPA1 is expressed in sensory neurons and mediates
nociception through numerous noxious compounds such as the highly reactive electrophile,
MGO. Binding of MGO to the cysteine and lysine residues of the channel’s N-terminal
intracellular domain channel are necessary for channel activation by MGO13.
Sensory neurons from TRPA1 knockout mouse shows no calcium influx when treated with
MGO. MGO facilitates the release of CGRP from vagus and sciatic nerves as well as from the
skin that contributes to pain transmission and together with PKA and PLC leads to nerve
sensitization. MGO might contribute to neuropathic pain in diabetes13.

15
Table 1 Methylglyoxal effects on diabetes induction or diabetic complications
Model Diabetes related effect Significant findings
Sprague-Dawley rats
MGO 60mg/kg/day for 28 days induces insulin dysfunction and hyperglycaemia and therefore is concluded as diabetogenic
• Fasting plasma glucose elevation • Insulin release, GLUT-4, PI3-K and adipose
glucose uptake reduction35
Human insulin, cell culture studies on 3T3-L1 adipocytes, L8 skeletal muscle cells, H4-II-E cells and INS-1E cells.
MGO 10μM-1mM induces insulin resistance and thus is considered as diabetogenic
• Mass spectrophotometry: additional peaks of MGO-bound insulin
• L8-cells showed significant reduction in glucose uptake
• MGO binds INS-1E cells and reduces Insulin negative feedback33
RINmf5 insulin secreting cells
MGO 100μM-10mM induces cells toxicity and thus is considered as diabetogenic
• Fragmented nuclei cells elevation recorded microscopically and with multiparameter flow cytometry11
Human plasma and erythrocytes
MGO 30-300μM was shown to accelerate eryptosis
• HPLC analysis showed plasma and RBC MGO elevation
• MGO reduced GSH and ATP in RBC • MGO dose dependent annexin-V-positive
elevation46 Mouse aortic endothelial cells
MGO 500μM induces endothelial dysfunction through interfering endothelial insulin signalling
• Western blotting: Inhibiting IRS-1, Akt and eNOS phosphorylation37
Human plasma MGO derivatives were associated with endothelial dysfunction
• ELISA measurements showed sVCAM-1 and sPLA2 elevation associated with THP in T1DM patients44
STZ Wistar-Kyoto rats saphenous artery
MGO elevation was associated with vascular function which is a major complication in diabetes
• Mild impairment in cholinergic and sodium nitroprusside (SNP) induced vasodilation41
Wistar and Goto-Kakizaki rats
MGO induces endothelial dysfunction even when ingested (50-75mg/kg/day for 3 months)
• Cholinergic vasodilation significant impairment
• Aortic IHC showed significant reduction in free NO production accompanied with increase in superoxide generation
• Western blotting showed significant suppression of phosphorylated and total

16
Conclusion:
vasodilator stimulated phosphoprotein • Vascular inflammation through increased
monocyte chemoattractant peptide-1 # (MCP-1)43
Normal human LDL, human BJ fibroblast AND HepG2 cells and Charles River rats
MGO-bound LDL accelerates vascular complications such as atherosclerosis
• LDL particles significantly decreased through MGO binding
• Cell free microplate blocked wells showed significant aggregation tendency of MGO-bound LDL
• IHC: MGO increased LDL retention in rats aorta
• MGO-bound LDL binds significantly more to LDL receptors found on HepG2 and BJ cells49
Sprague Dawley rat aortic rings, rat aortic and human umbilical veins endothelial cells.
MGO 100μM induces endothelial dysfunction, a common diabetes complication
• Cholinergic endothelium dependent vasodilation significant impairment accompanied with significant decrease in endothelial NO production with suppressed eNOS phosphorylation estimated through western blotting40
Mice (TRPA1+/-) HEK 293t cells and DRG cultures
MGO 10mM induces neuropathic pain, a major diabetic complication
• MGO generates large inward current in HEK 293t cells and depolarizes the membrane from -100 to +100mV
• Calcium imaging reveals MGO binding to cysteine preferably to induce calcium entry
• TRPA1 or TRPV1 KO DRG showed significant lack of response to MGO13
Diabetic patients, WT and STZ mice mice (Glo-/+), mice (Scn-/-), human sciatic nerve, mice DRG, MGO treated Wistar rats
MGO 5μM administered systemically into rats induces hyperalgesia and neuronal inflammation for 3 hours
• MGO elevation was associated with diabetic neuropathy in T2DM patients31
• MGO depolarizes sensory neurons and modifies NaV1.8 to increase the neuronal excitation and facilitate nociception
• MGO slows NaV1.7 inactivation • In mice, MGO reduces nerve conduction and
increases calcitonin gene-related peptide (CGRP) and cyclooxygenase-2 (COX-2) expression to promote thermal and mechanical hyperalgesia in mice
• MGO increases blood flow to nociceptive cerebral regions31
Transgenic GLO-1 and normal Wistar rats
Restoring MGO metabolism prevents retinopathy, a common visual complication in diabetes
• Immunoblotting showed significant increase in CEL, CML, MG-H1 in diabetic Wistar rats’ retinas suppressed in GLO1 transgenic rats45

17
Diabetes mellitus is a metabolic disorder that is a major health burden in most of the
countries around the globe. Although numerous therapeutic options are available to control
diabetes, these medications are targeted mainly toward controlling the blood glucose level
through supplying insulin, enhancing insulin secretion, enhancing the tissues’ sensitivity
towards insulin, interfering with glucose absorption or re-absorption. However, diabetic
complications such as retinopathy, neuropathic pain, vascular and renal complications are
still the main diabetic complications that, in the long term, remain largely resistant to
treatments. Numerous studies reviewed in this paper show a correlation between MGO and
diabetes as well as diabetes complications which suggest that understanding the actions of
MGO might identify therapeutic targets for treating consequences of diabetes in the future.
3. References:

18
1. ADA, Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2012, 35 (1), S64-S71. 2. UK, D., Diabetes: Facts and Stats. Diabetes UK 2014, 3, 1-21. 3. Group, U. P. D. S., UK prospective diabetes study. Diabetologia 1991, 34 (12), 877-890. 4. IDF Diabetes atlas. http://www.idf.org/diabetesatlas. 5. Davies, M.; Brophy, S.; Williams, R.; Taylor, A., The Prevalence, Severity, and Impact of Painful Diabetic Peripheral Neuropathy in Type 2 Diabetes. Diabetes Care 2006, 29 (7), 1518-1522. 6. Hex, N.; Bartlett, C.; Wright, D.; Taylor, M.; Varley, D., Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabetic Medicine 2012, 29 (7), 855-862. 7. Ashcroft, F. M.; Rorsman, P., Diabetes mellitus and β-cells: the last ten years. Cell 2012, 148, 1160-1171. 8. Chao, E. C.; Henry, R. R., SGLT2 inhibition — a novel strategy for diabetes treatment. Nature Reviews Drug Discovery 2010, 9, 551-559. 9. Menge, B. A.; Schrader, H.; Breuer, T. G. K.; Dabrowski, Y.; Uhl, W.; Schmidt, W. E.; Meier, J. J., Metabolic consequences of a 50% partial pancreatectomy in humans. Diabetologia 2009, 52, 306-317. 10. Del Guerra, S.; Lupi, R.; Marselli, L.; Masini, M.; Bugliani, M.; Sbrana, S.; Torri, S.; Pollera, M.; Boggi, U.; Mosca, F.; Del Prato, S.; Marchetti, P., Functional and molecular defects of pancreatic islets in human type 2 diabetes. Diabetes 2005, 54, 727-735. 11. Sheader, E. A.; Benson, R. S. P.; Best, L., Cytotoxic action of methylglyoxal on insulin-secreting cells. Biochemical Pharmacology 2001, 61, 1381-1386. 12. Uchida, K., Role of reactive aldehyde in cardiovascular diseases. Free Radical Biology & Medicine 2000, 28 (12), 1685–1696. 13. Eberhardt, M. J.; Filipovic, M. R.; Leffler, A.; De la Roche, J.; Kistner, K.; Fischer, M. J.; Flemin, T.; Zimmermann, K.; Burmazovic, I. I.; Nawroth, P. P.; Bierhaus, A.; Reeh, P.; Sauer, S. K., Methylglyoxal activates nociceptors through transient receptor potential A1 (TRPA1): a possible mechanism of metabolic neuropathies. JBC 2012, 287 (34), 28291-28306. 14. Kalapos, M. P., Where does plasma methylglyoxal originate from? Diabetes Research and Clinical Practice 2012, 99 (3), 260-271. 15. Lu, J.; Randell, E.; Han, Y.; Adeli, K.; Krahn, J.; Meng, Q. H., Increased plasma methylglyoxal level, inflammation, and vascular endothelial dysfunction in diabetic nephropathy. Clinical Biochemistry 2011, 44 (4), 307-311. 16. Thornalley, P. J.; Jahan, I.; Ng, R., Suppression of the accumulation of triosephosphates and increased formation of methylglyoxal in human red blood cells during hyperglycaemia by thiamine in vitro. J. Biochem 2001, 129 (4), 543-549. 17. Jadidi, R. B.; Karachalias, N.; Ahmed, N.; Battah, S.; Thornalley, P. J., Prevention of incipient diabetic nephropathy by high dose thiamine and benfotiamine. Diabetes 2003, 52, 2110-2120. 18. Hammes, H. P.; Du, X.; Edelstein, D.; Taguchi, T.; Matsumura, T.; Ju, Q.; Lin, J.; Bierhaus, A.; Nawroth, P.; Hannak, D.; Neumaier, M.; Bergfeld, R.; Giardino, I.; Brownlee, M., Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nature Medicine 2003, 9 (3), 294-299. 19. Mahendran, Y.; Vangipurapu, J.; Cederberg, H.; Stančáková, A.; Pihlajamäki, J.; Soininen, P.; Kangas, A. J.; Paananen, J.; Civelek, M.; Saleem, N. K.; Pajukanta, P.; Lusis, A. J.; Bonnycastle, L. L.; Morken, M. A.; Collins, F. S.; Mohlke, K. L.; Boehnke, M.; Korpela, M. A.; Kuusisto, J.; Laakso, M., Association of ketone body levels with hyperglycemia and type 2 diabetes in 9,398 Finnish men. Diabetes 2013, 62, 3618-3626. 20. Lim, E. L.; Hollingsworth, K. G.; Smith, F. E.; Thelwall, P. E.; Taylor, R., Inhibition of lipolysis in type 2 diabetes normalizes glucose disposal without change in muscle glycogen synthesis rate. Clinical Science 2011, 121, 169-177. 21. Arner, P.; Langin, D., Lipolysis in lipid turnover, cancer, cachexia, and obesity-induced insulin resistance. Trends in endocrinology and metabolism 2014, 25 (5), 255-262.

19
22. Jones, A. E.; Summers, R. L., Detection of isopropyl alcohol in a patient with diabetic ketoacidosis. The Journal of Emergency Medicine 2000, 19 (2), 165-168. 23. Laffel, L., Ketone bodies: a review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab Res Rev 1999, 15, 412-426. 24. Mitch, W. E.; Bailey, J. L.; Wang, X.; Jurkovitz, C.; Newby, D.; Price, S. R., Evaluation of signals activating ubiquitin-proteasome proteolysis in a model of muscle wasting. American Journal of Physiology 1999, 25 (5), C1132-C1138. 25. Uribarri, J.; Negrean, M.; Stirban, A.; Buenting, C. E.; Sander, D.; Koschinsky, T.; Cai, W.; Vlassara, H., Single oral challenge by advanced glycation end products acutely impairs endothelial function in diabetic and nondiabetic subjects. Diabetes Care 2007, 30 (10), 2579-2582. 26. Banning, M., The carcinogenic and protective effects of food. British Journal of Nursing 2005, 14 (20), 1070-1074. 27. Patel, R.; Baker, S. S.; Liu, W.; Desai, S.; Alkhouri, R.; Kozielski, R.; Mastrandrea, L.; Sarfraz, A.; Cai, W.; Vlassara, H.; Patel, M. S.; Baker, R. D.; Zhu, L., Effect of dietary advanced glycation end products on mouse liver. PLoS ONE 2012, 7 (4), 1-7. 28. Goldberg, T.; Cai, W.; Peppa, M.; Dardaine, V.; Baliga, B. S.; Uribarri, J.; Vlassara, H., Advanced Glycoxidation End Products in Commonly Consumed Foods. Journal of the American Dietetic Association 2004, 104 (8), 1287–1291. 29. Martins, S. I. F. S.; Jongen, W. M. F.; van Boekel, M. A. J. S., A review of Maillard reaction in food and implications to kinetic modelling. Trends in Food Science & Technology 2001, 11 (9-10), 364-373. 30. Dyer, D. G.; Dunn, J. A.; Thorpe, S. R.; Bailie, K. E.; Lyons, T. J.; McCance, D. R.; Baynes, J. W., Accumulation of Maillard reaction products in skin collagen in diabetes and aging. J Clin Invest 1993, 91 (6), 2463-2469. 31. Bierhaus, A.; Flemin, T.; Stoyanov, S.; Leffler, A.; Babes, A.; Neacsu, C.; Sauer, S. K.; Eberhardt, M.; Schnölzer, M.; Lasischka, F.; Neuhuber, W. L.; Kichko, T. I.; Konrade, I.; Elvert, R.; Mier, W.; Pirags, V.; Lukic, I. K.; Morcos, M.; Dehmer, T.; Rabbani, N.; Thornalley, P. J.; Edelstein, D.; Nau, C.; Forbes, J.; Humpert, P. M.; Schwaninger, M.; Ziegler, D.; Stern, D. M.; Cooper, M. E.; Haberkorn, U.; Brownlee, M.; Reeh, P. W.; Nawroth, P. P., Methylglyoxal modification of Nav1.8 facilitates nociceptive neuron firing and causes hyperalgesia in diabetic neuropathy. Nature Medicine 2012, 1-9. 32. Miki, T.; Nagashima, K.; Tashiro, F.; Kotake, K.; Yoshitomi, H.; Tamamoto, A.; Gonoi, T.; Iwanaga, T.; Miyazaki, J.; Seino, S., Defective insulin secretion and enhanced insulin action in KATP channel-deficient mice. PNAS 1998, 95 (18), 10402–10406. 33. Jia, S.; Olson, D. J. H.; Ross, A. R. S.; Wu, L., Structural and functional changes in human insulin induced by methylglyoxal. FASEB 2006, 20, E871-E879. 34. Jia, X.; Wu, L., Accumulation of endogenous methylglyoxal impaired insulin signaling in adipose tissue of fructose-fed rats. Mol Cell Biochem 2007, 306, 133–139. 35. Dhar, A.; Dhar, I.; Jiang, B.; Desai, K. M.; Wu, L., Chronic methylglyoxal infusion by minipump causes pancreatic β-cell dysfunction and induces type 2 diabetes in Sprague-Dawley rats. Diabetes 2011, 60, 899-908. 36. Krüger, M.; Kratchmarova, I.; Blagoev, B.; Tseng, Y. H.; Kahn, C. R.; Mann, M., Dissection of the insulin signaling pathway via quantitative phosphoproteomics. PNAS 2007, 105 (7), 2451–2456. 37. Nigro, C.; Raciti, G. A.; Leone, A.; Flemin, T. H.; Longo, M.; Prevenzano, I.; Fiory, F.; Mirra, P.; D’Esposito, V.; Ulianich, L.; Nawroth, P. P.; Formisano, P.; Beguinot, F.; Miele, C., Methylglyoxal impairs endothelial insulin sensitivity in both in vitro and in vivo. Diabetologia 2014, 57, 1485–1494 38. Taniguchi, C. M.; Emanuelli, B.; Kahn, C. R., Critical nodes in signalling pathways: insights into insulin action. Nature Reviews Molecular Cell Biology 2006, 7, 85-96. 39. Chang, W.; Wang, R.; Wu, L., Methylglyoxal-induced nitric oxide and peroxynitrite production in vascular smooth muscle cells. Free Radical Biology & Medicine 2005, 38, 286-293.

20
40. Dhar, A.; Dhar, I.; Desai, K. M.; Wu, L., Methylglyoxal scavengers attenuate endothelial dysfunction induced by methylglyoxal and high concentrations of glucose. British Journal of Pharmacology 2010, 161, 1843–1856. 41. Ruiter, M. S.; Van Golde, J. M.; Schaper, N. C.; Stehouwer, C. D.; Huijberts, M. S., The role of methylglyoxal in hyperglycemia-induced impairments of vasoreactivity in rat saphenous artery. In Reactivity, recruitment and remodeling of collateral arteries in diabetes, Ruiter, M. S., Ed. Gildeprint Drukkerijen: Amsterdam, 2012; pp 83-98. 42. Oya, T.; Hattori, N.; Mizuno, Y.; Miyata, S.; Maeda, S.; Osawa, T.; Uchida, K., Methylglyoxal modification of Protein: chemical and immunochemical characterization ofmethylglyoxal-arginine adducts. JBC 1999, 274 (26), 18492-18502. 43. Sena, C. M.; Matafome, P.; Crisóstomo, J.; Rodrigues, L.; Fernandes, R.; Pereira, P.; Seic¸a, R. M., Methylglyoxal promotes oxidative stress and endothelial dysfunction. Pharmacological Research 2012, 65, 497-506. 44. van Eupen, M. G. A.; Scharm, M. T.; Colhoun, H. M.; Hansen, N. M. J.; Niessen, H. W. M.; Tarnow, L.; Parving, H. H.; Rossing, P.; Stehouwer, C. D. A.; Schalkwijk, C. G., The methylglyoxal-derived AGE tetrahydropyrimidineis increased in plasma of individuals with type 1 diabetes mellitus and in atherosclerotic lesions and is associated with sVCAM-1. Diabetologia 2013, 56, 1845-1855. 45. Berner, A. K.; Brouwers, O.; Pringle, R.; Klaassen, I.; Colhoun, L.; McVicar, C.; Brockbank, S.; Curry, J. W.; Miyata, T.; Brownlee, M.; Schlingemann, R. O.; Schalkwijk, C.; Stitt, A. W., Protection against methylglyoxal-derived AGEs by regulation of glyoxalase 1 prevents retinal neuroglial and vasodegenerative pathology. Diabetologia 2012, 55, 845-854. 46. Nicolay, J. P.; Schneider, J.; Niemoeller, O. M.; Artunc, F.; Otin, M. P.; Haik Jr., G.; Thornalley, P. J.; Schleicher, E.; Wieder, T.; Lang, F., Stimulation of suicidal erythrocyte death by methylglyoxal. Cell Physiol Biochem 2006, 18, 223-232. 47. Föller, M.; Huber, S. M.; Lang, F., Erythrocyte Programmed Cell Death. IUBMB Life 2008, 60 (10), 661-668. 48. Latscha, D. B.; Drüeke, T.; Sarsat, V. W., Dialysis-induced oxidative stress: biological aspects and, clinical consequences, and therapy. Seminars in Diabaetes 2001, 14 (3), 193-199. 49. Rabbani, N.; Godfrey, L.; Xue, M.; Shaheen, F.; Geoffrion, M.; Milne, R.; Thornalley, P. J., Glycation of LDL by methylglyoxal increases arterial atherogenicity. Diabetes 2011, 60, 1973-1980.