Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
Metformin Sensitizes EGFR-TKI–Resistant Human LungCancer Cells In Vitro and In Vivo through Inhibition of IL-6Signaling and EMT Reversal
Li Li1, Rui Han1,2, Hualiang Xiao3, Caiyu Lin1, Yubo Wang1, Hao Liu1, Kunlin Li1, Hengyi Chen1,Fenfen Sun1, Zhenzhou Yang4, Jianxin Jiang5, and Yong He1
AbstractPurpose: The EGF receptor tyrosine kinase inhibitors (EGFR-TKI) have become a standard therapy in
patients with EGFR-activating mutations. Unfortunately, acquired resistance eventually limits the clinical
effects and application of EGFR-TKIs. Studies have shown that suppression of epithelial–mesenchymal
transition (EMT) and the interleukin (IL)-6/STAT3 pathwaymay abrogate this acquiredmechanism of drug
resistance of TKIs. This study aims to investigate the effect of metformin on sensitizing EGFR-TKI–resistant
human lung cancer cells in vitro and in vivo through inhibition of IL-6 signaling and EMT reversal.
Experimental Design: The effect of metformin on reversing TKI resistance was examined in vitro and in
vivo using MTT, BrdUrd incorporation assay, invasion assay, flow cytometry analysis, immunostaining,
Western blot analysis, and xenograft implantation.
Results: In this study, metformin, a widely used antidiabetic agent, effectively increased the sensitivity of
TKI-resistant lung cancer cells to erlotinib or gefitinib.Metformin reversed EMT anddecreased IL-6 signaling
activation in TKI-resistant cells, while adding IL-6 to those cells bypassed the anti-TKI-resistance effect of
metformin. Furthermore, overexpression or addition of IL-6 to TKI-sensitive cells induced TKI resistance,
which could be overcome by metformin. Finally, metformin-based combinatorial therapy effectively
blocked tumor growth in xenografts with TKI-resistant cancer cells, which was associated with decreased
IL-6 secretion and expression, EMT reversal, and decreased IL-6–signaling activation in vivo.
Conclusion: Metformin, generally considered nontoxic and remarkably inexpensive, might be used in
combinationwith TKIs in patients with non–small cell lung cancer, harboring EGFRmutations to overcome
TKI resistance and prolong survival. Clin Cancer Res; 20(10); 2714–26. �2014 AACR.
IntroductionReversible small-molecule EGF receptor tyrosine kinase
inhibitors (EGFR-TKI), including gefitinib (Iressa) and erlo-tinib (Tarceva), have showndramatic therapeutic efficacy inpatients with non–small cell lung cancer (NSCLC) withEGFR-activating mutations, and have been recommendedas the standard first-line therapy in these patients (1, 2).However, despite excellent initial clinical responses, nearly
all responding patients eventually develop drug resistanceafter a median period of about 10 months (3). Thus,innovative treatment strategies are urgently needed to over-come therapeutic resistance to EGFR-TKIs to improve thesurvival of patients with NSCLC.
Molecular mechanisms underlying acquired TKI resis-tance are still not fully understood. Two principalmechanisms accounting for approximately 50% ofacquired resistance to TKIs in lung cancer are secondarymutations of a threonine-to-methionine substitution atamino acid position 790 (T790M) of EGFR and ampli-fication of the N-methyl-N0-nitro-N-nitroso-guanidine(MNNG) HOS transforming gene (MET) oncogene (3,4). Various other molecular mechanisms are alsoinvolved, including epithelial–mesenchymal transition(EMT). EMT is a process during which cells undergomorphologic changes from epithelial phenotype to mes-enchymal phenotype, resulting in enhanced motility andincreased invasion, proliferation, andmetastasis of cancercells (5). EMT has been associated with the sensitivity notonly to conventional chemotherapies in several types ofcancer (6, 7), but to EGFR-TKIs in lung cancer cells,xenografts, and patients (8). Targeting EMT may reverse
Authors' Affiliations: Departments of 1Respiratory Disease, 2ThoracicSurgery, 3Pathology, and 4Oncology; and 5StateKeyLaboratory of Trauma,Burns and Combined Injury, Daping Hospital, Third Military Medical Uni-versity, Chongqing, China
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
L. Li and R. Han contributed equally to this article.
Corresponding Author: Yong He, Department of Respiratory Disease,Daping Hospital, Third Military Medical University, Chongqing 400042,China. Phone: 86-23-68757791; Fax: 86-23-68757791; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-13-2613
�2014 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 20(10) May 15, 20142714
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

or prevent acquisition of therapeutic resistance to EGFRinhibitors (9). TGF-b is a major driving force of the EMTgenetic program (5). It was reported that TGF-b couldinduce interleukin (IL)-6 axis activation, further resultingin EMT and resistance to reversible TKI in lung cancer cells,while inhibiting IL-6/STAT3 signaling could restore TKIsensitivity (10). In NSCLC with T790M mutations, activa-tion of IL-6R/JAK1/STAT3 signaling could induce resistanceto irreversible EGFR inhibitors (11). IL-6/STAT3 signalingmay be a potential therapeutic target for enhancing theefficacy of EGFR-TKIs. Therefore, reversing EMT anddecreasing IL-6 signaling activation may be an effective wayto improve the response to EGFR-TKI treatment.Metformin is a widely used and well-tolerated drug for
diabetes and has arisen keen interest as a potentialanticancer agent ever since the report of the clinicalevidence that the cancer risk and mortality are reducedin diabetics receiving metformin (12). Metformin exertsremarkable antitumor properties in tumor cells andmouse models. It strongly inhibited the growth of lungcancer cells (13), and its combination with classicalchemotherapeutic agents, including paclitaxel, cisplatin,or doxorubicin, significantly suppressed breast tumorgrowth and prolonged remission in a xenograft model(14). Interestingly, metformin exposure significantly im-peded the TGF-b–promoted EMT process (15), decreasedIL-6 secretion, and suppressed STAT3 activity (16), sug-gesting that metformin may overcome TKI resistance byreversing EMT and inhibiting IL-6 signaling pathways.One recent study reported that metformin in combina-tion with gefitinib significantly enhanced the efficacy oftargeted therapy (17). However, the mechanism under-lying this effect remains unclear.
Here, we show that metformin in combination withgefitinib or erlotinib has a synergistic inhibitory effect onthe proliferation, migration, and invasion of cell linesresistant to TKIs. The effect of metformin against TKI resis-tance is attributed to its ability to reverse EMT and decreaseIL-6 signaling activation. In addition, this combinationaltherapy reduces tumor masses much more effectively thangefitinib or metformin alone in a xenograft mouse model,and this synergistic interaction is associated with the abilityof metformin to decrease the activation of STAT3 and AKTand reverse EMT. We thus provide rationale and experi-mental evidence for the combined use of metformin andTKIs to overcome TKI resistance in patients with NSCLCwith EGFR mutations.
Materials and MethodsCell lines and reagents
Gefitinib (Iressa) was purchased from Tocris Bioscienceand erlotinib (Tarceva) fromCaymanChemical. Both drugswere prepared in dimethyl sulfoxide (DMSO) to obtain astock solution of 10 mmol/L. Metformin (Sigma) wasdissolved in deionized water and stored at �20�C. Therecombinant human IL-6 (rhIL-6) was purchased fromPeproTech. Erlotinib-sensitive H1650 cells and erlotinib-resistant H1650-M3 cells were kindly provided by Dr. R.Sordella from Cold Spring Harbor Laboratory. Gefitinib-sensitive PC-9 cells andgefitinib-resistant PC-9GRcellsweregiftedbyProf. J. Xu andDr.M. Liu fromGuangzhouMedicalUniversity (China). H1975 cells were provided by theAmerican Type Culture Collection. All the cells were cul-tured in RPMI-1640 medium (HyClone) with Earle’s saltssupplemented with 10% FBS (Gibco), 2 mmol/L L-gluta-mine solution (Gibco), 100 U/mL penicillin (HyClone),and 100 mg/mL streptomycin (HyClone) at 37�C, with 5%CO2 and 90% humidity.
Cell growth, invasion, and migration assaysThe cytotoxic effects of gefitinib or erlotinib plus metfor-
min were determined by the MTT dye reduction methodand BrdUrd incorporation assay (10). Cell invasion wasmeasured using 24-well 6.5-mm-diameter inserts (8.0-mmpore size; Corning Incorporated). The relative cell invasionindex was calculated as reported (18). Cell migration wasevaluated using single-cell tracking assay as described earlier(19). Cell apoptosis was analyzed by flow cytometry. Formore details, please refer to the Supplementary Materialsand Methods.
Animal experimentsFor xenograft implantation, a total of 2� 106 PC-9GR or
PC-9 cells were injected subcutaneously into the back nextto the left forelimb of 6-week-old female BALB/cA-nu mice(Laboratory Animal Center of Third Military Medical Uni-versity, Chongqing, China), all of which developed tumorswith a size of �30 mm3 within 5 to 7 days. The mice werethen randomly assigned to 4 groups (8mice/group) with orwithout oral administration of 1mg/mLmetformin, or 250mg/L gefetinib, or both, in drinking water. Tumor volume
Translational RelevanceAlthough patients with non–small cell lung cancer
(NSCLC) with EGFRmutations show an excellent initialresponse to EGF receptor tyrosine kinase inhibitors(EGFR-TKI), their acquired resistance inevitably arisesand has no effective treatment yet. In this study, weinvestigated whether metformin could reverse TKI resis-tance in TKI-resistant cell lines and xenograft models.Our data suggest that metformin could effectively over-come TKI resistance both in vitro and in vivoby inhibitingthe interleukin-6 signaling pathway and reverting epi-thelial–mesenchymal transition. Thus, in patients withNSCLC with EGFR mutations, metformin might beused in combination with TKIs to delay or overcomeTKI resistance. We have already successfully started aclinical trial (http://www.clinicaltrials.gov/ct2/show/NCT01864681) to observe the benefits of metforminin combination with gefitinib to treat advanced patientswith NSCLC with EGFR mutations. This study providesthe preclinical evidence that metformin has promisingpotential to be developed as a novel anticancer agent.
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2715
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

was calculated as (length�width2)/2 andmeasured twice aweek (Fig. 5A). The animals were kept in individual venti-lated cages in compliance with institutional guidelines. Allanimal protocolswere approved by theEthicsCommittee ofthe ThirdMilitaryMedical University. After 4 weeks, tumor-bearing mice were sacrificed, and tumors were harvested,fixed with 4% paraformaldehyde, and embedded in paraf-fin. To assess survival, the animals were monitored for 90days until being euthanized. The distribution of survivalpercentages over time was estimated using the Kaplan–Meier method.
Statistical analysisAll data are presented asmean� SEM. Statistical analyses
were carried out using the unpaired, 2-tailed Student t testand statistical significance was assumed at a value of P <0.05. Kaplan–Meier curves were compared using the log-rank test.
For details of the Materials and Methods, please refer tothe Supplementary Materials and Methods.
ResultsMetformin resensitizes EGFR-TKI–resistant humanlung cancer cells in vitro
We first performed MTT assays to determine whethermetformin could enhance the inhibitory effects of TKIs onthe growth of TKI-resistant lung cancer cell lines, PC-9GRand H1650-M3. PC-9 cells were highly sensitive to gefitinib(Fig. 1A), whereas PC-9GR cells were highly resistant to it(Fig. 1B). Treatment with 5mmol/Lmetformin resensitizedPC-9GR to gefitinib (Fig. 1B and Supplementary Fig. S1).Similarly, H1650-M3 cells, whichwere resistant to erlotinibtreatment, displayed enhanced sensitivity to erlotinib aftermetformin treatment (Fig. 1C and Supplementary Fig. S1).Treatment with 5 mmol/L metformin alone for 48 hoursslightly decreased viability of PC-9GR cells and H1650-M3cells (Fig. 1D).
As metformin disrupts mitochondrial respiration, whichmay affect the results ofMTT assay, we then applied BrdUrdincorporation assay to measure cell proliferation to avoidany nonspecific effects ofmetformin. Our results confirmedthat metformin in combination with gefitinib resulted inrobust inhibitionof cell proliferation inPC-9GR and anoth-er well-established resistant cell line, H1975 cells (Fig. 1Eand Supplementary Fig. S2). To confirm thatmetformin canbe uptaken by the cell lines used in this study, we nextexamined the expression of organic cation transporter1 (OCT1), the transporter required for uptake of metfor-min, in PC-9, PC-9GR,H1650, andH1650-M3 cells. Resultsshowed that these cell lines expressed high levels of OCT1,suggesting thatmetformin canbeuptakenby those cell lines(Supplementary Fig. S3).
To further determinewhethermetformin in combinationwith TKIs has a better inhibitory effect on tumor cellinvasion and migration than metformin or TKIs alone, weperformed transwell assay and single-cell tracking assay.Both the invasion and motility of resistant PC-9GR cellswere increased as compared with those of parental PC-9
cells. Gefitinib treatment alone (IC2548h) had little effect on
invasion or motility. Interestingly, metformin alone wasable to decrease the invasion ability and migration rate ofPC-9GR cells, and could further enhance these effects whencombined with gefitinib (Fig. 1F and G). The same findingwas observed inH1650-M3 cells treatedwithmetformin, orerlotinib, or both (Supplementary Fig. S4). We next ana-lyzed the induction of apoptosis in PC-9GR cells treatedwith metformin alone or in combination with gefitinib.Flow cytometric analysis revealed that metformin aloneenhanced the apoptosis of PC-9GR cells, and the combi-nation therapy further augmented this effect (Fig. 1H).Taken together, these in vitro data suggest that the combineduse of metformin and gefitinib resensitizes resistant cells toTKIs and overcomes the acquired TKI resistance in thesecells.
Metformin reverses EMT in TKI-resistant lung cancercells
Knowing that EMT is extensively correlated with thera-peutic resistance to EGFR-TKIs (20), we next examinedwhether metformin could reverse EMT in TKI-resistant celllines. Typical epithelial morphology and expression of E-cadherin, an epithelial marker, was observed in PC-9 cellsand H1650 cells, whereas mesenchymal morphology andhigh expression of Vimentin (a marker of mesenchymalphenotype) and SNAIL (a key regulator of EMT) wereobserved in PC-9GR and H1650-M3 cells. Metformin treat-ment induced a transition from spindle-like to epithelial-like morphology, as evidenced by the upregulation of E-cadherin and downregulation of Vimentin and SNAIL inboth resistant cell lines (Fig. 2A–D and Supplementary Fig.S5). Western blot analysis results further demonstrated thatmetformin effectively increased E-cadherin expressionwhile suppressed Vimentin and SNAIL expression in theabsence or presence of TKIs as indicated (Fig. 2E andSupplementary Fig. S6). Based on these findings, we con-clude that metformin reverses EMT in TKI-resistant lungcancer cells.
Metformin decreases IL-6 signaling activation in TKI-resistant lung cancer cell lines
To identify the molecular mechanisms of overcomingacquired TKI resistance by metformin, we next examinedthe effect of metformin on IL-6 activation in TKI-resistantcell lines, which was reported to be the key mechanismunderlying TKI resistance and the promoter of the EMTprocess (10). We first performed ELISA analysis and real-time PCR analysis, finding higher levels of protein secretionand gene transcription of IL-6 in both resistant cell lines.Metformin treatment significantly decreased IL-6 proteinsecretion and gene expression in both resistant cell lines(Fig. 2F and Supplementary Fig. S7). STAT3 and AKT, thekey components of IL-6 signaling, were highly phosphor-ylated in both resistant cell lines. Metformin alone effec-tively downregulated STAT3 and AKT activation in PC-9GRcells and STAT3 activation in H1650-M3 cells, but it hadlittle effect on AKT activation in H1650-M3 cells. Exposure
Li et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2716
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

C
PC-9 PC-9GR
0 2.5 5 10 15 20
Erlotinib (µmol/L)
Gef
Met– +–
–– –+
–++
20
40
60
80
100
H1650
H1650-M3
H1650-M3+Met
0
20
40
60
80
100 PC-9GR
PC-9GR+Met
0
20
40
60
80
100 PC-9
Cel
l via
bili
ty
(% o
f co
ntr
ol)
Cel
l via
bili
ty
(% o
f co
ntr
ol)
Cel
l via
bili
ty
(% o
f co
ntr
ol)
Cel
l via
bili
ty
(% o
f co
ntr
ol)
0 0.005 0.01 0.05 0.1 1
Gefitinib (µmol/L)
0 1 2 4 8 16
Gefitinib (µmol/L)
A B
F
0
1
2
3
Rel
ativ
e ce
ll in
vasi
on
PC-9 PC-9GR
+––
++–+–
– –GefMet
G
*
†
‡
–10 0 10
–10
0
10
–10 0 10
–10
0
10
A
–10 0 10
–10
0
10
A
–10 0 10
–10
0
10
–10 0 10
–10
0
10
PC-9 PC-9GR PC-9GR+Met PC-9GR+Gef PC-9GR+Gef+Met
µm µm µm µm µm
PI
An
nex
in V
PI
An
nex
in V
PI
An
nex
in V
PI
An
nex
in V
Control Met Gef Gef+Met
H
0
50
100
PC-9GR H1650-M3
Met – –+ +
D*†
0
25
50
+ ++–+–
– –GefMet
Ap
op
tosi
s (%
)
*
†*
PC-9GR
Gef
Met
+–– –+
–++
E
DA
PI
/Brd
Urd
0
5
10
15
20
25
30
35
+ ++–+–
– –GefMet
*
†*
Inco
rpo
rati
on
of
Brd
Urd
(% o
f ce
lls)
PC-9GR
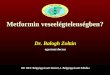
Figure 1. Metformin overcomes TKI resistance in TKI-resistant human lung cancer cells. A and B,metformin increased the sensitivity of gefitinib-resistant cells togefitinib. Cell viability of parental PC-9 and resistant PC-9GR cells treated with the indicated doses of gefitinib for 48 hours were assessed with the MTTmethod. C, parental H1650 and H1650-M3 cells were treated with the indicated doses of erlotinib for 48 hours. Cell viability, assessed by the MTT method, wasexpressedas%ofcontrol for each timepoint.D, treatmentwith5mmol/Lmetforminalone for48hoursslightlydecreased theviabilityofbothPC-9GRandH1650-M3 cells. The data shown represent the mean value of the percentage of viable cells � SEM (�, P < 0.05 and †, P < 0.01 compared with the control). E,metformin (5 mmol/L) and gefitinib (IC2548h) synergistically inhibited the proliferation of PC-9GR cells, as determined by BrdUrd incorporation assay. �, P < 0.01comparedwith control, †,P < 0.01 comparedwithmetformin alone. Scale bars, 50mm. F,metformin (5mmol/L) and gefitinib (IC2548h) synergistically inhibited theinvasiveness of PC-9GR cells. Scale bars: 100 mm. �, P < 0.01 compared with that of PC-9; †, P < 0.05 compared with PC-9GR; z, P < 0.05 compared withmetformin treatment alone.G,metformin treatment decreased single cellmotility. Each trace represents themovementof a single cell within an hour, with startingpoint set at (0, 0). H, metformin in combination with gefitinib enhanced apoptosis of PC-9GR cells. Images are representative of 3 independent experiments.�, P < 0.01 compared with control; †, P < 0.05 compared with metformin treatment. Met, metformin; Gef, gefitinib; DAPI, 40,6-diamidino-2-phenylindole.
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2717
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

to gefitinib or erlotinib slightly enhanced STAT3 and AKTphosphorylation, whereas metformin in combination witheither gefitinib or erlotinib decreased activation of STAT3andAKT in PC-9GR and STAT3 activation inH1650-M3 celllines, respectively (Fig. 2E and Supplementary Fig. S6). Wethen investigated the possible mechanism by which met-formin reduces STAT3 and AKT activation. Metformin dis-rupts mitochondrial respiration, leading to an increase inthe intracellular AMP: ATP ratio, and resulting in the acti-vation of AMPK by LKB1. Thus, we examined activation ofAMPK and acetyl coA carboxylase (ACC, a standard indi-cator of AMPK activity) under metformin treatment. Levelsof phosphorylated AMPK and ACC were significantlydecreased in resistant cell lines, whereas metformin alone
or in combination with either gefitinib or erlotinib signif-icantly increased the activation of AMPK and ACC (Fig. 2Eand Supplementary Fig. S6). In addition, all the cell linesused in this study expressed LKB1 (Supplementary Fig. S3).These results suggest that the inhibition of the IL-6 signalingpathway may represent the key mechanism by which met-formin overcomes TKI resistance.
Metformin overcomes IL-6–induced TKI resistance inTKI-sensitive lung cancer cells
Given that the stimulation of TKI-sensitive cells by IL-6could directly decrease erlotinib sensitivity (10), we theninvestigated whether metformin could overcome IL-6–induced TKI resistance. It was found that 48-hour culture
PC-9 PC-9GR PC-9GR+Met H1650 H1650-M3 H1650-M3+Met
Vim
enti
n
E-C
adh
erin
Mo
rph
olo
gy
A
C
P-AKT
P-STAT3
ββ-Actin
AKT
STAT3
H1650-M3
GefMet
H1650
E-Cad
Vim
SNAIL
– ++
PC-9GR
++––
–––
PC-9E
B
DPC-9 PC-9GR PC-9GR+Met H1650 H1650-M3 H1650-M3+Met
Vim
enti
n
E-C
adh
erin
Mo
rph
olo
gy
– +++
+––
––
P-AMPK
AMPK
P-ACC
ACC
0
50
100
150
200
250
PC-9 PC-9GR
+–– +––– – ++
H1650 H1650-M3
+–– +––– – ++
Pro
du
ctio
n le
vels
(p
g/m
L) *
*†
† †
†‡
F
Erl
Met –
GefMet
ErlMet
Figure 2. Metformin reverses EMTand decreases IL-6 signaling inTKI-resistant human lung cancercells. A and B, phase-contrastimages of parental and resistantcells in the presence or absence of5 mmol/L metformin for 48 hours.Scale bars: 100 mm. C and D,immunofluorescence stainingshowed that TKI-resistant cell linesexpressed high levels of Vimentinand low levels of E-cadherin,which was reversed by metformintreatment. The nucleus wasstained with 40,6-diamidino-2-phenylindole in the mergedimages. Scale bars: 30 mm. E,whole cell protein lysates fromdifferent cell lines wereimmunoblotted with indicatedantibodies. Similar results wereobtained in 3 independentexperiments. F,metformin alone orin combination with TKIssignificantly decreased IL-6secretion levels in TKI-resistantH1650-M3 and PC-9GR cells asdetermined by ELISA assays.�, P < 0.01 compared with parentalcell lines, respectively; †, P < 0.01,compared with untreated resistantcell lines, respectively; z, P < 0.05,compared with H1650-M3 cellstreated with metformin alone. Met,metformin; TKI, tyrosine kinaseinhibitor; E-cad, E-cadherin; Vim,Vimentin; Gef, gefitinib; Erl,erlotinib.
Li et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2718
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

in IL-6–containing medium was able to decrease the sen-sitivity of PC-9 cells to gefitinib. Interestingly, metforminaddition restored the sensitivity of PC-9 cells to gefitinib(Fig. 3A). Metformin alone increased sensitivity of PC-9cells to gefitinib, especially at low level of gefitinib (0.005mmol/L), although the difference of IC50 value was notsignificant when compared with the control. Similarly,overexpression of IL-6 in PC-9 cells (named PC-9psb cells)also resulted in decreased sensitivity to gefitinib, whereasmetformin treatment restored gefitinib sensitivity (Supple-mentary Fig. S8). When assessing the effects of IL-6 activa-tion on tumor cell invasion, we found that the addition ofIL-6 enhanced invasiveness of PC-9 cells. In contrast, met-formin inhibited invasionof PC-9 cells inducedby IL-6 (Fig.
3B). Taken together, these results suggest that IL-6 is suffi-cient to decrease gefitinib cytotoxicity, which can bereverted by metformin.
Next, we examined EMT and IL-6 activation in PC-9cells treated with IL-6 or IL-6 plus metformin. IL-6 treat-ment induced EMT in those sensitive cells, as character-ized by spindle-shaped morphology, the loss of E-cad-herin and the expression of EMT markers Vimentin andSNAIL (Fig. 3C–E). In addition, exposure to IL-6 resultedin significant phosphorylation of its downstream mole-cules STAT3 and AKT, but inhibited the activation ofAMPK and ACC (Fig. 3D and E). Metformin significantlyreverted EMT, diminished phosphorylation of STAT3 andAKT, and enhanced activation of AMPK and ACC (Fig.
P-STAT3
E-Cadherin
Vimentin
STAT3
P-AKT
AKT
β-Actin
SNAIL
IL-6
Met –
+
–
+–
+
IL-6
Met –
+
–
+–
+
Mer
ged
Vim
enti
n
E-C
adh
erin
Inva
sio
n
IL-6
Met –
+
–
+–
+
Cel
l via
bili
ty
(% o
f co
ntr
ol)
0 0.005 0.01 0.05 0.1 1
A B
C D
0
2
4
Mo
rph
olo
gy
Rel
ativ
e ce
ll in
vasi
on
+––
++–
IL-6Met
*
†
Gefitinib (µmol/L)
P-AMPK
AMPK
P-ACC
ACC
0
20
40
60
80
100
Control IL-6 IL-6+Met Met
0.0
0.5
1.0
1.5
2.0
2.5 PC-9
PC-9+IL-6
PC-9+IL-6+Met
Fo
ld c
han
ge
of
pro
tein
leve
ls
E-Cad Vim SNAIL pSTAT3 STAT3 pAKT AKT pAMPK AMPK pACC ACC
E
†
‡
†
§§
†
§
†
§
*
§
†
§†
§
Figure 3. Metformin reverses IL-6–induced TKI resistance, EMT, andIL-6 signaling activation. A,metformin reversed IL-6–inducedgefitinib-resistance in parentalPC-9 cells. Parental PC-9 cells(untreated, or treated with10ng/mL IL-6or IL-6plus5mmol/Lmetformin) were incubated withgefitinib at the indicatedconcentrations. Cell viability wasassessed with the MTT methodafter 48-hour treatment. B,metformin decreased IL-6–enhanced invasiveness of parentalPC-9 cells. Scale bars, 100 mm. �,P< 0.01 comparedwith no treatmentgroup; †, P < 0.01, compared withIL-6 treatment group. C, metforminreversed IL-6–induced EMT inparental PC-9 cells. Morphology ofPC-9 cellswith different treatmentswas shown by phase-contrastimages. Expression of E-cadherinand Vimentin was determined byimmunofluoresence staining. Cellswere counter-stained with 40,6-diamidino-2-phenylindole. Scalebars, 100 mm for phase-contrastimages and 30 mm forimmunofluorescence images.D, metformin decreased IL-6signaling activation in IL-6–stimulated parental PC-9 cells.Whole cell protein lysates fromPC-9 cellswith different treatmentswere immunoblotted withantibodies as indicated, andb-actin was used to confirm equalgel loading. Similar results wereobtained in 3 independentexperiments. E, quantification ofblots in D. �, P < 0.05 and†, P < 0.01, compared with PC-9cells, respectively; z, P < 0.05 andx, P < 0.01, compared with IL-6treatment, respectively. Met,metformin; E-cad, E-cadherin;Vim, Vimentin.
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2719
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

3C–E). In summary, our data indicate that the activationof STAT3 and AKT by IL-6 is sufficient to induce gefitinibresistance, acquisition of mesenchymal-like features andinvasion ability, whereas metformin could successfullyrestore gefitinib sensitivity, reverse EMT, and decreaseSTAT3 and AKT phosphorylation.
Metformin overcomes TKI resistance by inhibiting IL-6signaling activation
To establish a causal link between metformin treat-ment, IL-6 signaling inhibition, and enhanced TKIresponse, we increased IL-6 signaling in metformin-pre-treated TKI-resistant cells by adding IL-6 to the culturemedium. Further addition of IL-6 significantly dimin-
ished the response of metformin-pretreated PC-9GR cellsto gefitinib (Fig. 4A) and the response of metformin-pretreated H1650-M3 cells to erlotinib (SupplementaryFig. S9A). In addition, further exposure to IL-6 enhancedthe invasiveness of PC-9GR (Fig. 4B) and H1650-M3 cells(Supplementary Fig. S9B), decreased the expression of E-cadherin and increased the expression of Vimentin andSNAIL (Fig. 4C–E and Supplementary Fig. S9C–S9E). IL-6also restored and enhanced STAT3 and AKT phosphory-lation, while inhibited the activation of AMPK and ACCin both cell lines (Fig. 4D and E and Supplementary Fig.S9D and S9E). Taken together, these findings suggest thatmetformin overcomes TKI resistance by inhibiting IL-6signaling activation.
Gef
Met
IL-6
P-STAT3
E-Cadherin
Vimentin
STAT3
P-AKT
AKT
+
+
+
+
– +
SNAIL
Inva
sio
n
Gef
Met
IL-6
+
+
+
+
– +
0 1 2 4 8 16
Gefitinib (µmol/L)
Cel
l via
bili
ty (
% o
f co
ntr
ol)
A
Gef
Met
IL-6
+
+
+
+
– +
Mer
ged
V
imen
tin
E
-Cad
her
in
0
20
40
60
80
100 PC-9GR+Met
PC-9GR+Met+IL-6
0
1
2
3
Rel
ativ
e ce
ll in
vasi
on
PC-9GR cells
IL-6Met
C
B
D
+ ++
– ++
Gef
*
P-AMPK
AMPK
P-ACC
ACC
β-Actin
0
1
2
3 PC-9GR+Gef+Met
PC-9GR+Gef+Met+IL-6
Fo
ld c
han
ge
of
pro
tein
leve
ls
E-Cad Vim Snail pSTAT3 STAT3 pAKT AKT pAMPK AMPK pACC ACC
E
*
**
*
*
*
*
Figure 4. Inhibition of IL-6 signalingis essential for metformin toovercome gefitinib resistance inPC-9GR cells. A, addition of IL-6increased the viability ofmetformin-pretreated PC-9GRcells. PC-9GR cells werepretreated with 5 mmol/Lmetformin for 48 hours, and thentreated with gefitinib of differentdoses as indicated, still with 5mmol/L metformin, or 5 mmol/Lmetformin plus IL-6 (10 ng/mL).Cell viability was measured 48hours later. B, IL-6 enhanced theinvasion of metformin-pretreatedPC-9GR cells. Gefitinib (IC2548h)plus metformin (5 mmol/L)-pretreated PC-9GR cells weregrown in the presence or absenceof IL-6 (10 ng/mL) for 48hours, andthen cellular invasiveness wasassessed by the transwell assay.Scale bars, 100 mm. �, P < 0.01compared with that withoutaddition of IL-6. C,immunostaining showed thataddition of IL-6 increasedVimentin expression anddecreased E-cadherin expressionin metformin- plus gefitinib-pretreated PC-9GR cells. Cellswere counter-stained with 40,6-diamidino-2-phenylindole. Scalebars, 30 mm. D, addition of IL-6restored IL-6 signaling activationin metformin-pretreated PC-9GRcells. Whole cell protein lysatesfrom PC-9GR cells with differenttreatments were immunoblottedwith indicated antibodies andb-actin were used to confirm equalgel loading. Similar results wereobtained in 3 independentexperiments. E, quantification ofblots in D. �, P < 0.01, comparedwith that without addition of IL-6,respectively. Met, metformin; Gef,gefitinib; E-cad, E-cadherin; Vim,Vimentin.
Li et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2720
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

Metformin plus gefitinib potentiates gefitinib-inducedantitumor activity in PC-9GR/mouse xenograftsWe next tested the possibility that the metformin-based
combinatorial therapy is more effective in xenografts estab-lished with PC-9GR cells. Treatment withmetformin slight-ly slowed down the tumor growth in xenografts. Gefitinibalone resulted in xenograft shrinkage, similar to the resultobtained by metformin. Importantly, in accord with theabove results in cell lines, a synergic effect of metformin incombination with gefitinib was observed upon co-admin-istration of gefitinib andmetformin, which further reducedthe tumor size in this model (Fig. 5B). After 4 weeks of drugadministration when the animals were sacrificed, the com-bination therapy caused a 58%decrease in tumor volume ascompared with the control group (P < 0.01), whereasgefitinib alone and metformin alone both caused a 32%decrease (P < 0.05 for both as compared with thecontrol; Fig. 5C). During the experiments, no obviousweight loss was observed in mice treated with metformin,gefitinib, or both (Supplementary Fig. S10). Besides, nosignificant reduction in serum insulin levels or glucoselevelswasobservedwithmetformin treatment (Supplemen-tary Fig. S11). A similar combinatorial effect of metforminand gefitinib was observed in xenografts established withTKI-sensitive PC-9 cells. Gefitinib alone resulted in signif-
icant tumor shrinkage in PC-9 xenografts, whereas metfor-min in combination with gefitinib further reduced thetumor sizes (P < 0.05 as compared with gefitinib alone;Supplementary Fig. S12). We then evaluated the survival ofPC-9GR xenografts treated with gefitinib, or metformin, orboth. Log-rank test showed that metformin or gefitinibalone did not prolong the survival significantly as comparedwith the control (P ¼ 0.07 and 0.14). Treatment withmetformin þ gefitinib significantly prolonged the survivalof mice as compared with either metformin or gefitinibalone (P ¼ 0.044 and 0.043, respectively; Fig. 5D). Collec-tively, these results suggest that the combination of met-formin with gefitinib may overcome gefitinib resistance invivo.
The combinatorial effect ofmetformin with gefitinib inmouse xenografts is associated with EMT reversal andinhibition of IL-6 signaling
To clarify the underlying reason why combination ofmetformin and gefitinib is more effective than either drugalone, we next analyzed EMT and components of the IL-6signaling pathway in the context of metformin-based com-binatorial therapy in PC-9GR xenografts. Immunofluore-sence staining showed high expression of Vimentin and lowexpression of E-cadherin in the control and gefitinib alone-
Cells injection
1. Water
2. Met alone
3. Gef alone
4. Gef and Met
Drug application (0 wk)
Tumor ~30 mm3
5–7 days
Sacrifice (4 wk)
Tumor volume
measurement
Tu
mo
r vo
lum
e (m
m3 )
0 1 2 3 4
Weeks after drug application
0 1 2 3 4
BControl
Met
Gef
Gef+Met
0
500
1,000
1,500
2,000
2,500 Control
Met
Gef
Gef+Met
*
*
†‡
Su
rviv
al r
ate
D
Days after drug application
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
1.0
0.75
0.25
0.5
0
Control
Met
Gef
Gef+Met
C
A5
Figure 5. Oral administration ofmetformin together with gefitinibsuppresses tumor growth andprolongs survival. A, schematicfigure of the xenograft model usedin this study. B, tumor volume (mm3)of PC-9GR cells treated withgefitinib, metformin, and theircombination. �, P < 0.05 whencompared with the control;†, P < 0.05 as compared withmetformin alone; z, P < 0.05 ascompared with gefitinib alone. C,macroscopic appearance of thetumors at 4 weeks after drugadministration. D, Kaplan–Meiersurvival curves were calculated forthe 4 treatment groups mentionedabove. The log-rank testdemonstrated a statisticaldifference between the gefitinibplus metformin group andmetformin alone, or gefitinib alonegroups (P ¼ 0.044 and 0.043,respectively). Metformin or gefitinibalone did not prolong the survivalsignificantly as comparedwith the control group (P¼ 0.07 and0.14, respectively). Met, metformin;Gef, gefitinib.
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2721
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

treated groups, indicating that EMT occurred in bothgroups. Metformin treatment alone or in combination withgefitinib increased E-cadherin expression and decreasedVimentin expression (Fig. 6A). These resultswere confirmedby Western blot analysis (Fig. 6D). Similarly, in PC-9xenografts, metformin in combination with gefitinibincreased the expression of E-cadherin and decreased thatof Vimentin when compared with the control (Supplemen-
tary Fig. S13). Next, we examined IL-6 secretion and expres-sion in PC-9GR xenografts. Using ELISA analysis, wedetected higher levels of IL-6 in peripheral blood in thecontrol groups. Gefitinib treatment alone did not decreaseIL-6 secretion significantly as compared with the controlgroup. IL-6 levels were significantly decreased in bothmetformin alone-treated and the metformin þ gefitinibgroups (P < 0.05 for both, as compared with the control
β-Actin
p-STAT3
p-AKT
Control
STAT3
AKT
Met Gef Gef+Met
0
40
80
120
160
Control Met Gef Gef+Met
Pro
du
ctio
n
leve
ls (
pg
/mL
) IL-6
E-Cad/Vim/DAPI E-Cad/Vim/DAPI DIC MergedE-Cadherin Vimentin
Co
ntr
ol
Met
form
inG
efit
inib
Gef
+M
et
E-Cad
Vim
Control Met Gef Gef+MetB C
A
D
* †*
SNAIL
P-AMPK
AMPK
P-ACC
ACC
Figure 6. Metformin in combinationwith gefitinib reverses EMT anddecreases IL-6 signaling inxenograft tumors. A, metforminplus gefitinib reversed EMT inxenograft tumors. Each panelrepresents a representativeimmunostaining of a paraffin-embedded section (4 mm) for E-cadherin in green, Vimentin in red,and counter-staining with 40,6-diamidino-2-phenylindole (DAPI)in blue. The area indicated by thesquare is shown at highermagnification. Scale bars, 30 mm.B, metformin plus gefitinibdecreased IL-6 levels in the blood.The chart represents IL-6 levels inthe serum of mice from the 4groups determined by ELISA. Thedata are expressed as means �SEM (n ¼ 8 each). �, P < 0.01 ascompared with the control group;†, P < 0.01 as compared withgefitinib group. C, metformin plusgefitinib decreased IL-6expression in the tumor tissues.Paraffin-embedded sections(4 mm) from tumor tissues werestained for IL-6 usingimmunohistochemistry. Scalebars, 80 mm. D, Western blottinganalyzed the expression ofindicated markers on proteinextracts obtained from harvestedtumors, and b-actin was used as aloading control. Met, metformin;Gef, gefitinib.
Li et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2722
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

group; Fig. 6B). These results were confirmed by immuno-histochemisty of tumor sections using an anti-IL-6 antibody(Fig. 6C). Finally, Western blot analysis showed that STAT3and AKTwere strongly phosphorylated in the control groupand gefitinib treatment increased the phosphorylation ofSTAT3 and AKT. Metformin alone or in combination withgefitinib inhibited the activation of STAT3 and AKT, butsignificantly increased the activation of AMPK and ACC(Fig. 6D and Supplementary Figs. S14 and S15). The expres-sion of phosphorylated AKT and STAT3 was further con-firmed by immunohistochemistry (Supplementary Fig.S16). These results suggest that the therapeutic advantageof the combination of metformin with gefitinib is associ-atedwith its ability to reverse EMT and inhibit IL-6 signalingin vivo.
DiscussionHuman NSCLCs with activating EGFR mutations show
an excellent response to treatment with EGFR-TKIs, such asgefitinib and erlotinib. However, nearly all patients suc-cumb to relapse because of drug resistance, for which noeffective therapy is available at present. Thus, novel strate-gies are urgently needed to delay or overcome acquiredresistance to EGFR-TKIs. In this study, we have demonstrat-ed that metformin can effectively overcome drug resistanceto erlotinib and gefitinib. Furthermore, metformin plusgefitinib significantly decrease tumor growth in vivo andprolong animal survival.
Clinical implications of metformin plus TKIs toovercome drug resistanceSeveral epidemiological studies have indicated that
metformin uptake can lower the risk of several types ofcancer in patients with diabetes (21–23). The patientswith diabetes with breast cancer receiving metforminand neoadjuvant chemotherapy had a higher pathologiccomplete response rate than did those not receiving met-formin (24). In mouse xenografts, metformin exerted com-parable effects on tumor regression when it was combinedwith a 4-fold reduced dose of doxorubicin that is noteffective as a monotherapy (14). Metformin inhibited theproliferation of NSCLC (25) and breast cancer cell lines(26), and blocked transformation in an inducible modelsystem (27, 28). These reports, together with our findingsthatmetformin significantly enhances the effect of erlotiniband gefitinib on TKI-resistant cell lines in vitro and in vivo,suggest that metformin has the promising potential to beused as a novel anticancer agent.The dose of metformin we used in in vitro experiments is
higher than that used in diabetic patients. However, asmentioned by Iliopoulos and colleagues (14), metforminaccumulates in tissues at the concentration several-foldhigher than that in blood, so that a concentration of 1 to10 mmol/L might be attained in tumor tissues duringcancer treatment, as discussed elsewhere earlier (17). Inprevious in vivo experiments testing the antitumor effect ofmetformin on xenografts, the dose of metformin varies
from 200 mg/mL (14) to 200 mg/mL (17), and it is dilutedin drinking water, present throughout the experiment. Inthis study, we used 1 mg/mL metformin, corresponding to75 mg/kg as reported by Iliopoulos and colleagues (14).The well-established Reagan–Shawmethod (29) shows thehuman equivalent dose (mg/kg) ¼ animal dose (mg/kg) �animal Km/human Km, where Km values are based onbody surface area. For a 60 kg human adult, Km is 37,whereas for a 20-g mouse, it is 3. Thus, the humanequivalent of the murine dose of 75 mg/kg is 365 mg inan adult of 60 kg, which is much less than the maximummetformin dose of 2,550 mg/day recommended by theFood and Drug Administration. Thus, the in vivo dose ofmetformin in this study is within a therapeutic range inhumans.
Mechanistic implicationsUnderstanding the molecular mechanisms underlying
the ability of metformin to overcome TKI resistance ispivotal to develop it as a novel agent to treat patients withNSCLC. EGFR TKI treatment resulted in STAT3 activation,which was caused by IL-6 in an autocrine manner (11).Inhibiting IL-6/STAT3 suppressed cancer cell growth andenhanced the sensitivity to anticancer drugs (30). How-ever, AKT phosphorylation was upregulated in gefitinib-resistant NSCLC cells, and maintenance of PI3K/AKTpathway signaling was associated with therapeutic resis-tance to EGFR-TKIs. As IL-6 is a major activator of the JAK/STAT3 and PI3K/AKT pathways (31), inhibiting its sig-naling has emerged as a possible solution to the problemof EGFR-TKI resistance.
In this study, we observed robust activation of the IL-6signaling pathway in TKI-resistant cells when comparedwith their parental sensitive cells. In addition, IL-6 over-expression or addition in TKI sensitive PC-9 cells resulted ingefitinib resistance, accompanied by increased phosphory-lation of STAT3 and AKT. Metformin treatment effectivelyovercomes TKI resistance in established TKI-resistant celllines, IL-6 stimulated PC-9 cells, and IL-6 overexpressingPC-9psb cells. Furthermore, adding IL-6 into metformin-pretreated TKI resistant cell lines abolished metformin’seffect, restored TKI resistance, and reactivated the IL-6signaling pathway. Thus, our data provide compelling evi-dence that metformin overcomes acquired resistance tomolecular-targeted therapies by inhibiting IL-6 signalingpathways (Supplementary Fig. S17).
Besides the inhibitory effect on the IL-6 signalingpathway, metformin’s ability to reverse EMT may alsoplay an important role in overcoming TKI resistance. EMThas been associated with resistance to EGFR inhibitortreatment in NSCLCs (20). AXL, an EMT marker, wasfound to be upregulated in patients with NSCLC withacquired resistance to EGFR-TKI treatment, and AXL acti-vation is a major cause of EGFR-TKI resistance (32). Inthis study, we demonstrated that metformin reversed EMTin TKI-resistant lung cancer cell lines and IL-6–stimulatedPC-9 cells. We also found that metformin inhibited theIL-6/STAT3 pathway, whereas IL-6 is capable of inducing
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2723
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

EMT in cancer cells (33). Thus, we conclude that EMTreversal by metformin is associated with its ability toovercome TKI resistance.
Metforminmaydisrupt the evil axis of TGF-b/IL-6, EMT,cancer stem cells and drug resistance
Cancer stem cells (CSC), which constitute a smallportion of neoplastic cells, are hypothesized to be criticalinitiators of cancers and mediate resistance to conven-tional antitumor therapies (34). Lung CSCs have alsobeen successfully isolated from lung cancer cell linesbased on SP phenotypes (low Hoechst 33342 stainingpattern; ref. 35), and from primary patient tumors (36).These lung CSCs are resistant to most conventional drugscurrently used to treat patients with lung cancer. How-ever, lung cancer cells surviving conventional or targetedtherapies exhibited several CSC features, such as strongclonogenic capacity, self-renewal, and high tumorigenic-ity (37, 38). Interestingly, the 2 inflammation-associatedcytokines, IL-6, and TGF-b1 are capable of inducing EMTin human breast cancer cells, resulting in generating cellswith stem-cell properties (39, 40). Indeed, EMT–CSCs–drug resistance has been proposed to be an emerging axisof evil in the war against cancer (41). In addition, asshown in this study, TKI-resistant lung cancer cells dis-played EMT features and increased activation of IL-6signaling pathways. Besides, trastuzumab-refractory CSCpopulations were found to be significantly enriched in theexpression of mesenchymal markers, and an increasedsecretion of TGF-b (42). Thus, TGF-b/IL-6, EMT, CSCs,and drug resistance are strongly correlated with eachother to maintain the TKI resistance in lung cancer.
In this study, we found that metformin could inhibit IL-6secretion, decrease IL-6 signaling activation and reverseEMT. It was also reported that metformin could reverseTGF-b–induced EMT (15). In addition, metformin treat-ment inhibited the growth of breast CSCs (13), ovarianCSCs (43), pancreatic CSCs (44), and thyroid CSCs (45),possibly by transcriptionally repressing the stem cell prop-erty EMT (46). Taken together, metformin emerges as a newtherapeutic option to inhibit TGF-b/IL-6 activation, reverseEMT, kill CSCs, and then overcome TKI resistance, thusdisrupting this evil axis in the war against cancer (Supple-mentary Fig. S18). Given the important role of CSCs in TKIresistance, we are currently examining the effect of metfor-min on killing CSCs in TKI-resistant lung cancer cells.
Metformin may alleviate TKI-induced interstitialpneumonia
Acute interstitial pneumonia is one of the serious adverseeffects of TKI treatment (47). IL-6 is known to induceinterstitial pneumonia (48). TKI treatment activates AP-1in lung cancer cells and promotes IL-6 secretion, whichfurther increases the expression of collagen and a-actin,markers for fibrosis (49). In this study, we provide soundevidence that metformin can inhibit the IL-6/STAT3 axis.Also, it has been reported that TGF-b is an importantinducer of pulmonary fibrosis (50), whereas metformin
can significantly inhibit TGF-b signaling (15). Accordingly,the combination of metformin and EGFR-TKI may bemoreeffective and safer for patients, because this treatment maynot only overcome TKI resistance but prevent or alleviatethe development of acute interstitial pneumonia.
Therapeutic resistance to EGFR-TKIs is almost inevitablein patients with activating EGFR mutations who initiallyrespond well to therapy. Management of TKI resistance hasbecome the focus of research to lengthen overall survival ofthese patients. In this study,wehave proven for the first timethat metformin overcomes TKI resistance in vitro and in vivoby inhibiting the IL-6 signaling pathway and reverting EMT.In addition, we have successfully started a clinical trial(registered in Clinicaltrials.gov: http://www.clinicaltrials.gov/ct2/show/NCT01864681) to observe the clinical ben-efits of metformin in combination with gefitinib to treatpatients with advanced NSCLC with EGFR mutations. Ourfuture research aims at providing more solid evidence todevelop metformin in combination with TKIs as a newtherapeutic approach to prolonging the survival of patientswith NSCLC.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: L. Li, Y. HeDevelopment of methodology: R. HanAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): L. Li, R.Han,H. Xiao,C. Lin, Y.Wang,H. Liu, K. Li,H. Chen, F. SunAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): L. Li, R. Han, H. Xiao, C. Lin, Y. Wang, Z.YangWriting, review, and/or revision of the manuscript: L. Li, Y. HeAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): H. Xiao, K. Li, H. Chen, F. Sun,J. JiangStudy supervision: Z. Yang, Y. He
AcknowledgmentsThe authors thank J. Du (State Key Laboratory of Trauma, Burns and
Combined Injury, Third Military Medical University) for taking immuno-fluoresence images. The authors thank K. Zhang (Department of ClinicalLaboratory, Daping Hospital, ThirdMilitaryMedical University) for her helpwith flow cytometry analysis. The authors thankR. Sordella fromCold SpringHarbor Laboratory and Prof. J. Xu and Dr. M. Liu from Guangzhou MedicalUniversity, for kindly providing the valuable cell lines used in this study. Theauthors also thankProf.M. Zhao (Institute for RegenerativeCures,Universityof California at Davis), Prof. M. Chen (Medical English Department, ThirdMilitary Medical University), and Dr. W. Guo (Department of SystemsBiology, The University of Texas MD Anderson Cancer Center) for theircritical reading and useful suggestions on the writing.
Grant SupportThis work was supported by National Nature Science Foundation of
China (81172113, 81071912, and 81301840), China 863 program(2012AA02A201), Chongqing Science Technology Commission (CSTC2011BB5021), a foundation for PLA Young Scientists (13QNP117), and afoundation of Third Military Medical University (2012XLC08).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received September 22, 2013; revised February 25, 2014; accepted March13, 2014; published OnlineFirst March 18, 2014.
Li et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2724
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

References1. Soria JC, Mok TS, Cappuzzo F, Janne PA. EGFR-mutated oncogene-
addicted non-small cell lung cancer: current trends and future pro-spects. Cancer Treat Rev 2012;38:416–30.
2. Nguyen KS, Neal JW. First-line treatment of EGFR-mutant non-small-cell lung cancer: the role of erlotinib and other tyrosine kinase inhibi-tors. Biologics 2012;6:337–45.
3. Pao W, Miller VA, Politi KA, Riely GJ, Somwar R, Zakowski MF, et al.Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib isassociated with a second mutation in the EGFR kinase domain. PLoSMed 2005;2:e73.
4. Engelman JA, Janne PA. Mechanisms of acquired resistance toepidermal growth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer. Clin Cancer Res 2008;14:2895–9.
5. Thiery JP, Acloque H, Huang RY, Nieto MA. Epithelial-mesenchymaltransitions in development and disease. Cell 2009;139:871–90.
6. Voulgari A, Pintzas A. Epithelial-mesenchymal transition in cancermetastasis: mechanisms, markers and strategies to overcome drugresistance in the clinic. Biochim Biophys Acta 2009;1796:75–90.
7. Neel DS, Bivona TG. Secrets of drug resistance in NSCLC exposed bynew molecular definition of EMT. Clin Cancer Res 2013;19:3–5.
8. Uramoto H, Iwata T, Onitsuka T, Shimokawa H, Hanagiri T, Oyama T.Epithelial-mesenchymal transition inEGFR-TKI acquired resistant lungadenocarcinoma. Anticancer Res 2010;30:2513–7.
9. Bruzzese F, Leone A, Rocco M, Carbone C, Piro G, Caraglia M, et al.HDAC inhibitor vorinostat enhances the antitumor effect of gefitinib insquamous cell carcinoma of head and neck by modulating ErbBreceptor expression and reverting EMT. J Cell Physiol 2011;226:2378–90.
10. Yao Z, Fenoglio S, GaoDC,CamioloM, Stiles B, Lindsted T, et al. TGF-b IL-6 axis mediates selective and adaptive mechanisms of resistanceto molecular targeted therapy in lung cancer. Proc Natl Acad Sci U S A2010;107:15535–40.
11. KimSM,KwonOJ,HongYK,KimJH,Solca F,HaSJ, et al. Activation ofIL-6R/JAK1/STAT3 signaling induces De Novo resistance to irrevers-ible EGFR inhibitors in non-small cell lung cancer with T790M resis-tance mutation. Mol Cancer Ther 2012;11:2254–64.
12. Evans JM, Donnelly LA, Emslie-Smith AM, Alessi DR, Morris AD.Metformin and reduced risk of cancer in diabetic patients. BMJ2005;330:1304–5.
13. Hirsch HA, Iliopoulos D, Struhl K. Metformin inhibits the inflammatoryresponse associated with cellular transformation and cancer stem cellgrowth. Proc Natl Acad Sci U S A 2013;110:972–7.
14. Iliopoulos D, Hirsch HA, Struhl K. Metformin decreases the dose ofchemotherapy for prolonging tumor remission in mouse xenograftsinvolving multiple cancer cell types. Cancer Res 2011;71:3196–201.
15. Cufi S, Vazquez-Martin A, Oliveras-Ferraros C, Martin-Castillo B,Joven J, Menendez JA. Metformin against TGF-b-induced epitheli-al-to-mesenchymal transition (EMT): from cancer stem cells to aging-associated fibrosis. Cell Cycle 2010;9:4461–8.
16. Lin CC, Yeh HH, Huang WL, Yan JJ, Lai WW, Su WP, et al.Metformin enhances cisplatin cytotoxicity by suppressing stat3activity independently of the LKB1-AMPK pathway. Am J RespirCell Mol Biol 2013;49:241–50.
17. Morgillo F,SassoFC,DellaCorteCM,VitaglianoD,D'AiutoE, Troiani T,et al. Synergistic effects of metformin treatment in combination withgefitinib, a selective EGFR tyrosine kinase inhibitor, in LKB1 wild-typeNSCLC cell lines. Clin Cancer Res 2013;19:3508–19.
18. Xu X, Fan Z, Kang L, Han J, Jiang C, Zheng X, et al. Hepatitis B virus Xprotein represses miRNA-148a to enhance tumorigenesis. J ClinInvest 2013;123:630–45.
19. Li L, Hartley R, Reiss B, Sun Y, Pu J, Wu D, et al. E-cadherin plays anessential role in collective directional migration of large epithelialsheets. Cell Mol Life Sci 2012;69:2779–89.
20. Chung JH, Rho JK, Xu X, Lee JS, Yoon HI, Lee CT, et al. Clinical andmolecular evidences of epithelial to mesenchymal transition inacquired resistance to EGFR-TKIs. Lung Cancer 2011;73:176–82.
21. Ruiter R, Visser LE, van Herk-Sukel MP, Coebergh JW, Haak HR,Geelhoed-Duijvestijn PH, et al. Lower risk of cancer in patients onmetformin in comparison with those on sulfonylurea derivatives:
results from a large population-based follow-up study. Diabetes Care2012;35:119–24.
22. Chaiteerakij R, Yang JD, Harmsen WS, Slettedahl SW, Mettler TA,Fredericksen ZS, et al. Risk factors for intrahepatic cholangiocarci-noma: association between metformin use and reduced cancer risk.Hepatology 2013;57:648–55.
23. Zhang ZJ, Zheng ZJ, KanH, SongY, CuiW, ZhaoG, et al. Reduced riskof colorectal cancer with metformin therapy in patients with type 2diabetes: a meta-analysis. Diabetes Care 2011;34:2323–8.
24. Jiralerspong S, Palla SL, Giordano SH, Meric-Bernstam F, Liedtke C,Barnett CM, et al. Metformin and pathologic complete responses toneoadjuvant chemotherapy in diabetic patients with breast cancer. JClin Oncol 2009;27:3297–302.
25. Salani B, Maffioli S, Hamoudane M, Parodi A, Ravera S, PassalacquaM, et al. Caveolin-1 is essential for metformin inhibitory effect on IGF1action in non-small-cell lung cancer cells. FASEB J 2012;26:788–98.
26. Zakikhani M, Dowling R, Fantus IG, Sonenberg N, Pollak M.Metforminis an AMP kinase-dependent growth inhibitor for breast cancer cells.Cancer Res 2006;66:10269–73.
27. Hirsch HA, Iliopoulos D, Tsichlis PN, Struhl K. Metformin selectivelytargets cancer stem cells, and acts together with chemotherapy toblock tumor growth and prolong remission. Cancer Res 2009;69:7507–11.
28. Hirsch HA, Iliopoulos D, Joshi A, Zhang Y, Jaeger SA, Bulyk M, et al. Atranscriptional signature and common gene networks link cancer withlipid metabolism and diverse human diseases. Cancer Cell 2010;17:348–61.
29. Reagan-Shaw S, Nihal M, Ahmad N. Dose translation from animal tohuman studies revisited. FASEB J 2008;22:659–61.
30. Chiu HC, Chou DL, Huang CT, Lin WH, Lien TW, Yen KJ, et al.Suppression of Stat3 activity sensitizes gefitinib-resistant non smallcell lung cancer cells. Biochem Pharmacol 2011;81:1263–70.
31. Schafer ZT, Brugge JS. IL-6 involvement in epithelial cancers. J ClinInvest 2007;117:3660–3.
32. Zhang Z, Lee JC, Lin L, Olivas V, Au V, LaFramboise T, et al. Activationof the AXL kinase causes resistance to EGFR-targeted therapy in lungcancer. Nat Genet 2012;44:852–60.
33. Sullivan NJ, Sasser AK, Axel AE, Vesuna F, Raman V, Ramirez N, et al.Interleukin-6 induces an epithelial-mesenchymal transition phenotypein human breast cancer cells. Oncogene 2009;28:2940–7.
34. Al-Ejeh F, Smart CE, Morrison BJ, Chenevix-Trench G, Lopez JA,Lakhani SR, et al. Breast cancer stem cells: treatment resistance andtherapeutic opportunities. Carcinogenesis 2011;32:650–8.
35. HoMM,NgAV, LamS,Hung JY. Side population in human lung cancercell lines and tumors is enriched with stem-like cancer cells. CancerRes 2007;67:4827–33.
36. Eramo A, Lotti F, Sette G, Pilozzi E, Biffoni M, Di Virgilio A, et al.Identification and expansion of the tumorigenic lung cancer stem cellpopulation. Cell Death Differ 2008;15:504–14.
37. Levina V, Marrangoni AM, DeMarco R, Gorelik E, Lokshin AE. Drug-selected human lung cancer stem cells: cytokine network, tumorigenicand metastatic properties. PLoS ONE 2008;3:e3077.
38. Shien K, Toyooka S, Yamamoto H, Soh J, Jida M, Thu KL, et al.Acquired resistance to EGFR inhibitors is associated with a manifes-tation of stem cell-like properties in cancer cells. Cancer Res 2013;73:3051–61.
39. Yadav A, Kumar B, Datta J, Teknos TN, Kumar P. IL-6 promotes headand neck tumor metastasis by inducing epithelial-mesenchymal tran-sition via the JAK-STAT3-SNAIL signaling pathway. Mol Cancer Res2011;9:1658–67.
40. Xie G, Yao Q, Liu Y, Du S, Liu A, Guo Z, et al. IL-6-induced epithelial-mesenchymal transition promotes the generation of breast cancerstem-like cells analogous to mammosphere cultures. Int J Oncol2012;40:1171–9.
41. Singh A, Settleman J. EMT, cancer stem cells and drug resistance: anemerging axis of evil in the war on cancer. Oncogene 2010;29:4741–51.
42. Oliveras-Ferraros C, Vazquez-Martin A, Martin-Castillo B, Perez-Mar-tinez MC, Cufi S, Del Barco S, et al. Pathway-focused proteomic
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2725
Metformin Sensitizes EGFR-TKI–Resistant Human Lung Cancer Cells
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

signatures in HER2-overexpressing breast cancer with a basal-likephenotype: new insights into de novo resistance to trastuzumab(Herceptin). Int J Oncol 2010;37:669–78.
43. Shank JJ, Yang K, Ghannam J, Cabrera L, Johnston CJ, Reynolds RK,et al. Metformin targets ovarian cancer stem cells in vitro and in vivo.Gynecol Oncol 2012;127:390–7.
44. Bao B, Wang Z, Ali S, Ahmad A, Azmi AS, Sarkar SH, et al. Metformininhibits cell proliferation, migration and invasion by attenuating CSCfunction mediated by deregulating miRNAs in pancreatic cancer cells.Cancer Prev Res 2012;5:355–64.
45. Chen G, Xu S, Renko K, Derwahl M. Metformin inhibits growth ofthyroid carcinoma cells, suppresses self-renewal of derived cancerstem cells, and potentiates the effect of chemotherapeutic agents.J Clin Endocrinol Metab 2012;97:E510–20.
46. Vazquez-Martin A, Oliveras-Ferraros C, Cufi S, Del Barco S, Martin-Castillo B, Menendez JA. Metformin regulates breast cancer stem cell
ontogeny by transcriptional regulation of the epithelial-mesenchymaltransition (EMT) status. Cell Cycle 2010;9:3807–14.
47. InoueA,SaijoY,MaemondoM,GomiK,TokueY,KimuraY,et al. Severeacute interstitial pneumonia and gefitinib. Lancet 2003;361:137–9.
48. Moodley YP, Misso NL, Scaffidi AK, Fogel-Petrovic M, McAnulty RJ,Laurent GJ, et al. Inverse effects of interleukin-6 on apoptosis offibroblasts from pulmonary fibrosis and normal lungs. Am J RespirCell Mol Biol 2003;29:490–8.
49. Ishiguro Y, Ishiguro H, Miyamoto H. Epidermal growth factor receptortyrosine kinase inhibition up-regulates interleukin-6 in cancer cells andinduces subsequent development of interstitial pneumonia. Oncotar-get 2013;4:550–9.
50. Zhou Y, Lee JY, Lee CM, Cho WK, Kang MJ, Koff JL, et al. Amphir-egulin, an epidermal growth factor receptor ligand, plays an essentialrole in the pathogenesis of transforming growth factor-beta-inducedpulmonary fibrosis. J Biol Chem 2012;287:41991–2000.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2726
Li et al.
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613

2014;20:2714-2726. Published OnlineFirst March 18, 2014.Clin Cancer Res Li Li, Rui Han, Hualiang Xiao, et al. EMT Reversal
through Inhibition of IL-6 Signaling andIn Vivo and In VitroCells Resistant Human Lung Cancer−Metformin Sensitizes EGFR-TKI
Updated version
10.1158/1078-0432.CCR-13-2613doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/03/19/1078-0432.CCR-13-2613.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/10/2714.full#ref-list-1
This article cites 50 articles, 19 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/10/2714.full#related-urls
This article has been cited by 8 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/10/2714To request permission to re-use all or part of this article, use this link
on October 24, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2014; DOI: 10.1158/1078-0432.CCR-13-2613