PowerPoint Presentation
Metabolic Bone Diseases Constitution of boneIt is a specialized
dense connective tissueWhere the matrix is impregnated by calcium
salts making it hard and rigid Matrix is made up of organic and
inorganic intercellular substances and surround osteocytes
Bone has organized canalicular mechanism and is highly
vascularIt consists of cells and intercellular substances It is
covered by periosteumBone grows by surface deposition
Cells of bone Osteogenic cells they are precursors of other
cells They are found in the inner layer of periosteumOsteoblasts
they are found where active bone is being formed They lay down
fibers and matrix
Osteocytes they are resting cells in the bony matrix They lie in
spaces called lacunaeLacunae are surrounded by canaliculiCanaliculi
anastomose with neighboring lacunae canaliculiProcesses of
osteocytes occupy these canaliculi Osteoclasts they are large giant
cells They have 5-15 nucleiThey remove the bone or resorption of
bone All bone cells work in harmony
Intercellular substanceTwo typesInorganic matter is made up of
calcium It provides rigidity Strong acids dissolve salts Organic
matter is made of collagen fibers All the elements are secreted by
osteoblasts Organic matter is destroyed by burning
Histological classification Two typesCompact or dense Bone is
hardPresent in the shaft of long bones Cancellous or spongy Bone
has larger marrow spacesBone is less hard Present in the ends of
long bones
Microscopic structure of compact bone Bone is covered by
periosteumIt consists of two layers Outer fibrous layerInner
osteogenic and vascular layerPeriosteum is firmly bound to bone by
Sharpeys fibers Compact bone is characteristic by the presence of
Haversian system
Histology of boneCentrally situated Haversian canalContaining
vessels and nerves Canal is surrounded by 6-12 concentric lamellae
Lamellae are composed of collagen fibers with calcium deposits
Collagen fibers run spirally
Histology of boneBetween the lamellae or on the lamellae are
lacunae present They imprison osteocytes Canaliculi are occupied by
processes of osteocyte The processes are responsible for
nourishment of osteocytes
Histology of boneHaversian canals are connected with one another
and communicate with marrow cavity through Volkmanns canals
Interstitial lamellae lie in the angles between the adjoining the
haversian lamellae They belong to older bone Near periosteum outer
circumferential lamellae are present Near endosteum inner
circumferential lamellae are present
Centrally situated Haversian canalContaining vessels and nerves
Canal is surrounded by 6-12 concentric lamellae Lamellae are
composed of collagen fibers with calcium deposits Collagen fibers
run spirally
Between the lamellae or on the lamellae are lacunae present They
imprison osteocytes Canaliculi are occupied by processes of
osteocyte The processes are responsible for nourishment of
osteocytes
Haversian canals are connected with one another and communicate
with marrow cavity through Volkmanns canals Interstitial lamellae
lie in the angles between the adjoining the haversian lamellae They
belong to older bone Near periosteum outer circumferential lamellae
are present Near endosteum inner circumferential lamellae are
present
Definition & TypesMost of the diseases are associated with
depletion of bone tissue.Osteoporosis- Bone mass is abnoarmally
lowOsteomalacia- Osseous connective tissue(osteoid) is present but
insufficiently mineralizedOsteitis Fibrosa- PTH over-production
leads to bone resorption and replacement by fibrous tissue
OSTEOPOROSIS18OSTEOPOROSISporous boneskeletal disorder
characterised by compromised bone strength predisposing a person to
an increased risk of fracture. Bone strength Bone density (g/cm2 or
g/cm3) - peak bone mass and amount of bone loss. Bone quality -
architecture, turnover, damage accumulation, and mineralisation of
the bone18What is Osteoporosis?Osteoporosis, or porous bone, is a
disease characterized by low bone mass and structural deterioration
of bone tissue. This disease can weaken your bones so much that
even simple everyday activities can cause bones to break.
Osteoporosis strikes both men and women, although women are
afflicted in much greater numbers. While the effects of
Osteoporosis are devastating, there are things you can do now to
prevent and treat it. Osteoporosis is defined as a skeletal
disorder characterised by compromised bone strength predisposing a
person to an increased risk of fracture. Bone strength reflects the
integration of bone density and bone quality. Bone density (g/cm2
or g/cm3) is determined by peak bone mass and amount of bone loss.
Bone quality refers to the architecture, turnover, damage
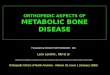
accumulation, and mineralisation of the bone19OSTEOPOROSISNormal
BoneOsteoporotic Bone
19On the left is an illustration of normal, healthy bone, and on
the right, osteoporotic bone. You can see the difference in bone
density clearly.Osteoporosis occurs when the holes between bone
become bigger, making it fragile and liable to break easily
OSTEOPOROSIS - DEFINITION
A progressive systematic skeletal disease characterized by low
bone mass and micro-architectural deterioration of bone tissue,
with a consequent increase in bone fragility and susceptibility to
fractureCLASSIFICATION OF OSTEOPOROSISPrimary osteoporosis in the
elderly can be classified as type I or II:Type I (menopausal)
osteoporosis occurs mainly in persons aged 51 to 75, is six times
more common in women, and is associated with vertebral and Colles'
(distal radius) fractures. Type II (senescent) osteoporosis occurs
in persons > 60, is two times more common in women, and is
associated with vertebral and hip fractures. Overlap between types
I and II is substantial, so this classification is of limited
clinical use. Primary osteoporosis is thought to result from the
hormonal changes that occur with age, particularly decreasing
levels of sex hormones (estrogen in women, testosterone in men).
Several other risk factors are usually contributory.
Secondary osteoporosis may be due to many causes. 22
23RISK FACTORSFemaleThin or small frameLow body weightSmoker
23In addition to warning signs, there are a significant number
of risk factors to consider for Osteoporosis. However, it is
important to be aware that you can have no risk factors and still
have Osteoporosis.The following risk factors have been
identified:Being female,Having a thin or small frame andHaving a
low body weight of 127 pounds or less.In addition, being a smoker
is a major risk factor as are
24RISK FACTORSAdvanced ageHistory of fragility fractureFamily
history- primary relative with Osteoporosis or fragility
fracture
24Reaching Advanced age, andHaving a history of fragility
fracture or a primary relative with a history of fragility fracture
or Osteoporosis.25RISK FACTORSPost MenopausalHormonal imbalances
can result in rapid bone lossWomen can lose up to 20% of their bone
mass in 5-7 years25In addition, post menopausal women are at great
risk because the hormonal imbalances of menopause can result in
rapid bone loss.Women can lose up to 20% of their bone mass in the
5-7 years after the onset of menopause.26Risk FactorsAmenorrhea,
Anorexia & BulimiaDiet low in calciumCertain medicationsLow
testosterone in men26Eating disorders such as Anorexia and
Bulimia,A diet low in calcium,Use of certain medications andLow
testosterone in men are all risk factors as well. 27ETHNICITY &
OSTEOPOROSISCaucasian & Asian-American Women High Risk
27Caucasian and Asian-American women are also at high risk. This
is due largely to differences in bone mass and density.The average
calcium intake among Asian-American women is about half that of
their Caucasian counterparts.While Asian-American women generally
have lower incidence of hip fractures than Caucasian women, the
prevalence of vertebral fractures is about equal between the two
populations.28MEN & OSTEOPOROSIS
Underdiagnosed Unrecognized Underreported Inadequately
researched 28While Osteoporosis does strike women at higher rates,
men are also at risk. Osteoporosis in men is underdiagnosed,
unrecognized, and inadequately reported and researched. As with
women, Caucasian men are at greater risk for Osteoporosis. Many of
the same risk factors apply to men:Lifestyle, age, heredity,
prolonged exposure to certain medications. chronic disease and
undiagnosed levels of testosterone all put men at increased risk
for Osteoporosis.29SYMPTOMS AND WARNING SIGNS29There are several
symptoms and warning signs indicative of Osteoporosis to be on the
lookout for:Persistent, unexplained back pain,Noticing that you are
shorter than you used to be,that you dont stand up as straight as
you used to, or that your posture is becoming hunched over or
stooped.PATHOPHYSIOLOGY Hallmark of osteoporosis is a reduction in
skeletal mass caused by an imbalance between bone resorption and
bone formation.Under physiologic condition, bone formation and
resorption are in fair balance.A change in either , that is,
increased bone resorption or decreased bone formation may result in
osteoporosisOsteoporosis can be caused both by a failure to build
bone and reach peak bone mass as a young adult and by bone loss
later in lifePATHOLOGYInadequate peak massExcessive bone
resorption: Deficiency of estrogenCalcium metabolism, Vitamin D
metabolism HyperparathyroidismInadequate bone formation during
remodelling
INVESTIGATIONSRadiological evidence of decreased bone mass is
more reliable.Following features may be noticed on X-rays: Loss of
vertical height of a vertebra due to collapseCod fish appearance.
The disc bulges into the adjacent vertebral bodies so that the disc
becomes biconvexGround glass appearance of the bones, conspicuous
in bones like the pelvisSinghs index: Singh et al. graded
osteoporosis into 6 grades based on the trabecular pattern of the
femoral neck trabeculae.Metacarpal index and vertebral index are
other methods of quantification
BIOCHEMISTRY: Serum calcium, phosphates and alkaline phosphatase
are within normal limitsTotal plasma proteins and plasma albumin
may be lowMarkers of bone resorption: deoxy-pyridinoline,
N-telopeptide
DENSITOMETRY:Method to quantify osteoporosisIn this method
absorption of photons (emitted from gamma emitting isotopes) by the
bone calcium is measured2 types of bone densitometry: ultrasound
based and X-ray basedDual energy X-ray absorptiometry (DEXA) scan
is an X-ray based bone densitometry, and is the gold standard in
the quantification of bone mass NEUTRON ACTIVATION ANALYSISCalcium
in the bone is activated by neutron bombing, and its activity
measured
BONE BIOPSYTREATMENTPrinciple objectives of treatment are
alleviation of pain and prevention of fracturesDivided into medical
and orthopeadicMEDICAL TREATMENTHigh protein diet: Increasing
protein intake may increase the formation of organic matrix of the
boneCalcium supplementation: Helpful in cases with deficiency of
calcium in their dietAndrogens: These hormones have an anabolic
effect on the protein matrix of bone, and in some instances
ameliorate symptomsEstrogens (HRT): Halt the progressive loss of
bone mass in postmenopausal osteoporosisVitamin D: This is given,
in addition to the above, to increase calcium absorption from the
gutAlandronate: Used in once a day dose, empty stomach.
Oesophagitis is a troubling complicationCalcitonin: Helps in
building up the bone mass and also acts as an analgesic
Biphosphanates:Sodium alendronate ( 10mg/day or
70mg/week)Risedronate (5mg/day or 35mg/week)Ibandronate: once a
monthSelective estrogen receptive modulator-SERM- Raloxifene
Teriparatide(recombinant PTH hormone): daily injectionUsed in
established osteoporosis, very low BMD, cannot tolerate
BiphosphonatesCI:Young, Pagets disease, radiation therapy
ORTHOPAEDIC TREATMENTExercises: Weight bearing is a major
stimulus to bone formation. Increased guarded activity would
therefore be of benefit to the patientBracing: Prophylactic bracing
of the spine by using an ASH brace or Taylor brace maybe useful in
prevention of pathological fractures in a severely osteoporotic
spinePREVENTIONAdequate intake of dietary calciumDecreased alcohol
consumption and caffeine useRegular exerciseSmoking
cessationOSTEOPETROSISDefinitionOsteopetrosis is a bone disease
that makes bones abnormally dense and prone to breakage
(fracture).Osteopetrosis, literally "stone bone", also known
asmarble bone diseaseandAlbers-Schnberg disease, is an extremely
rare inheriteddisorderwhereby thebonesharden, becomingdenser.A
clinical syndrome characterized by the failure of osteoclasts to
resorb bone. As a consequence, bone modeling and remodeling are
impaired.In contrast to more prevalent conditions likeosteoporosis,
in which the bones become less dense and more brittle,
orosteomalacia, in which the bones soften.Aetiology1. Failure of
Bone cells and bone modeling and remodeling
Osteoblasts synthesize bone matrix, which are composed
predominantly of type I collagen and are found at the bone-forming
surface.Extracellular matrix surrounds some osteoblasts, which
become osteocytes.Osteoclasts can tightly attach to the bone matrix
by integrin receptorsto form a sealing zone, within which is a
sequestered, acidified compartment.Acidification promotes
solubilization of the bone mineral in the sealing zone, and various
proteases, notably cathepsin K, catalyze degradation of the matrix
proteins.Bone modeling and remodeling differ in that modeling
implies a change in the shape of the overall bone and is prominent
during childhood and adolescence.Modeling is the process by which
the marrow cavity expands as the bone grows in diameter.Failure of
modeling is the basis of hematopoietic failure in
osteopetrosisRemodeling, in contrast, involves the degradation of
bone tissue from a preexisting bony structure and replacement of
the degraded bone by newly synthesized bone. Failure of remodeling
is the basis of the persistence of woven bone.2. Failure of
Osteoclast development and maturation
For precursor cells to mature, functional osteoclasts require
the action of 2 distinct signals. The first is
monocyte-macrophagecolony-stimulating factor (M-CSF), which is
mediated by a specific membrane receptor and its signaling cascade.
The second is the receptor activating NF-kappa B ligand (RANKL),
acting through its cognate receptor, RANK. A soluble decoy
receptor, osteoprotegerin, can bind RANKL, limiting its ability to
stimulate osteoclastogenesis.3. Genetic and molecular defects in
osteopetrosis
The primary underlying defect in all types of osteopetrosis is
failure of the osteoclasts to reabsorb bone.A number of
heterogeneous molecular or genetic defects can result in impaired
osteoclastic function:The specific genetic defect in humans is
known only in osteopetrosis caused by carbonic anhydrase II
deficiencyBased on its inheritance pattern, infantile osteopetrosis
seems to be transmitted in an autosomal recessive mannerViruslike
inclusions have been reported in osteoclasts of some patients with
benign osteopetrosis
Carbonic anhydrase isoenzyme II deficiency
This enzyme catalyzes the formation of carbonic acid from water
and carbon dioxide. Carbonic acid dissociates spontaneously to
release protons, which are essential for creating an acidic
environment required for dissolution of bone mineral in the
resorption lacunae. Lack of this enzyme results in impaired bone
resorption.Clinical FeaturesInfantile osteopetrosis
Infantile osteopetrosis (also called malignant osteopetrosis) is
diagnosed early in life. Failure to thrive and growth retardation
are symptoms.Nasal stuffiness due to mastoid and paranasal sinus
malformation is often the presenting feature of infantile
osteopetrosisNeuropathies related to cranial nerve entrapment occur
due to failure of the foramina in the skull to widen
completelyManifestations include deafness, proptosis, and
hydrocephalus.Dentition may be delayedOsteomyelitis of the mandible
is common due to an abnormal blood supplyBones are fragile and can
fracture easilyDefective osseous tissue tends to replace bone
marrow, which can cause bone marrow failure with resultant
pancytopeniaPatients suffer from anemia, easy bruising and bleeding
(due to thrombocytopenia), and recurrent infections (due to
inherent defects in the immune system)Extramedullary hematopoiesis
may occur, with resultant hepatosplenomegaly, hypersplenism, and
hemolysisOther manifestations include sleep apnea and blindness due
to retinal degeneration
They are often transverse fractures with multiple areas of
callus formation and normal healing.Additionally, there is crowding
of the marrow, so bone marrow function is affected resulting in
myelophthisic anaemia andextramedullary haematopoiesiswith
splenomegaly. This may terminate inacute leukaemia.
Adult osteopetrosis
Adult osteopetrosis (also called benign osteopetrosis) is
diagnosed in late adolescence or adulthood. Two distinct types have
been described, type I and type II, on the basis of radiographic,
biochemical, and clinical features.Approximately one half of
patients are asymptomatic, and the diagnosis is made
incidentally.Many patients have bone pains. Bony defects are common
and include neuropathies due to cranial nerve entrapment (eg, with
deafness, with facial palsy), carpal tunnel syndrome, and
osteoarthritis. Bones are fragile and may fracture easily.
Approximately 40% of patients have recurrent fractures.
Osteomyelitis of the mandible occurs in 10% of patients.Other
manifestations include visual impairment due to retinal
degeneration and psychomotor retardation.CharacteristicType IType
IISkull sclerosisMarked sclerosis mainly of the vaultSclerosis
mainly of the baseSpineDoes not show much sclerosisShows the
rugger-jersey appearancePelvisNo endobonesShows endobones in the
pelvisTransverse banding of metaphysisAbsentMay or may not be
presentRisk of fractureLowHighSerum acid phosphataseNormalVery
highInvestigationLaboratory findings in infantile
osteopetrosisSerum calcium - Generally reflects oral intake;
hypocalcemia can occur and cause rickets if it is severe
enoughParathyroid hormone (PTH) - Often is elevated (secondary
hyperparathyroidism)Acid phosphatase - Increased due to increased
release from defective osteoclastsCreatinine kinase isoform BB
(CK-BB) - levels are increased due to increased release from
defective osteoclasts
Laboratory findings in adult osteopetrosisAcid phosphatase and
CK-BB - Concentrations are often increased in type II diseaseSerum
bone-specific alkaline phosphatase - Values may also be increased
in various types of the disease
Genetic screening
Mutation screening of appropriate candidate genes should be
undertaken in patients whose presentation corresponds to any of the
known genetic lesions.Histologic findings
Failure of osteoclasts to resorb skeletal tissue is the
pathognomonic feature of true osteopetrosis. Remnants of
mineralized primary spongiosa are seen as islands of calcified
cartilage within mature bone. Woven bone is commonly seen.
Osteoclasts can be increased, normal, or decreased in
number.Radiography
Patients usually have generalized osteosclerosis.Bones may be
uniformly sclerotic, but alternating sclerotic and lucent bands may
be noted in iliac wings and near the ends of long bones. The bones
may be clublike or may have the appearance of a bone within bone
(endobone). Radiographs may also show evidence of fractures or
osteomyelitis.The entire skull is thickened and dense, especially
at the base. Sinuses are small and underpneumatized. Vertebrae are
extremely radiodense. They may show alternating bands, known as the
rugger-jersey sign
Differentiating type 1 from type 2 adult osteopetrosis
Type I disease - Sclerosis of the skull mainly affects the vault
with marked thickening; the spine does not show much sclerosis.Type
II disease - Sclerosis is found mainly in the base of the skull;
the spine always has the rugger-jersey appearance, and the pelvis
always shows subcristal sclerosis; transverse banding of metaphysis
is common in patients with type II disease but not in patients with
type I disease (this finding confirms type II disease, but its
absence does not necessarily indicate type I disease)
Treatment1. Vitamin D analogsThese supplements increase serum
calcium levels by increasing calcium absorption from the
gastrointestinal tract.Calcitriol(Rocaltrol, Calcijex,Vectical) in
large doses, with restricted calcium intake, sometimes improves
osteopetrosis dramatically. It can be used to treat infantile
osteopetrosis and appears to help by stimulating dormant
osteoclasts and, thus, bone resorption. Markers of bone turnover
(eg, serum osteocalcin, bone-specific alkaline phosphatase, urine
hydroxyproline levels) increase during therapy. However, calcitriol
usually produces only modest clinical improvement, which is not
sustained after discontinuation.2. CorticosteroidsThese agents have
anti-inflammatory properties and cause profound and varied
metabolic effects. Corticosteroids modify the body's immune
response to diverse stimuli.Prednisone is an immunosuppressant used
for the treatment of autoimmune disorders. It may decrease
inflammation by reversing increased capillary permeability and
suppressing polymorphonuclear leukocyte activity. The drug
stabilizes lysosomal membranes and suppresses lymphocytes and
antibody production.3. Hematopoietic Growth Factors
Epoetin alfa is a purified glycoprotein produced from mammalian
cells modified with gene coding for human erythropoietin (EPO).
Biological activity mimics human urinary EPO, which stimulates
division and differentiation of committed erythroid progenitor
cells and induces the release of reticulocytes from bone marrow
into the blood stream.Darbepoetin is an erythropoiesis-stimulating
protein closely related to erythropoietin, a primary growth factor
produced in kidney that stimulates development of erythroid
progenitor cells. Its mechanism of action is similar to that of
endogenous erythropoietin, which interacts with stem cells to
increase red cell production.Darbepoetin has longer a half-life
than epoetin alfa and may be administered weekly or biweekly.
4. ImmunomodulatorGamma-1b interferon is synthesized by
eukaryotic cells in response to viruses and a variety of natural
and synthetic stimuli. It possesses antiviral, immunomodulatory,
and antiproliferative activity. Gamma interferon has potent
phagocyte-activating effects not seen with other interferon
preparations. It works by stimulating osteoclast activity.Infantile
osteopetrosis
Vitamin D (calcitriol) appears to help by stimulating dormant
osteoclasts, thus stimulating bone resorption. Large doses of
calcitriol, along with restricted calcium intake, sometimes improve
osteopetrosis dramatically.However, calcitriol usually produces
only modest clinical improvement, which is not sustained after
therapy is discontinuedTreatment with gamma interferon improves
white blood cell function, greatly decreasing the incidence of new
infections. With treatment, trabecular bone volume substantially
decreases and bone-marrow volume increases. This results in
increases in hemoglobin, platelet counts, and survival rates.
Combination therapy with calcitriol is clearly superior to
calcitriol alone. Erythropoietin can be used to correct anemia.
Corticosteroids have also been used to treat anemia, as well as to
stimulate bone resorption.Adult osteopetrosis
Adult osteopetrosis requires no treatment by itself, although
complications of the disease may require intervention. No specific
medical treatment exists for the adult type.Surgical treatment
In pediatric osteopetrosis, surgical treatment is sometimes
necessary because of fractures.In adult osteopetrosis, surgical
treatment may be needed for aesthetic reasons (eg, in patients with
notable facial deformity) or for functional reasons (eg, in
patients with multiple fractures, deformity, and loss of function).
Severe, related degenerative joint disease may warrant surgical
intervention as well.Disease of mineralization : Osteomalacia /
RicketsDefinitiondiseases where organic matrix of the bone fails to
calcify properly, leaving large osteoid seams / inadequate
mineralization of bone* osteoid throughout the skeleton is
incompletely calcifiedin growing bones of children-> Ricketsin
bones of adult-> Osteomalacia
RicketsDefine : inadequate mineralization of growing bones in
children, affecting physeal growth and ossification, resulting in
deformities of endochondral skeleton
Etiology :Type 11. due to deficiency of vitamin D- diminished
intake eg malnutrition- diminished absorption eg gastric
abnormalities, biliary diseases- lack of exposure to sunlight
2. due to disturbance of vit D metabolism- hepatic factor eg
lack of 25 hydroxylation of vit D- renal factor eg lack of
1hydroxylation - unresponsive of target cells to 1-25 dihydroxy vit
D Type 21. defective absorption of phosphates through renal
tubules- hypophosphataemia rickets (X- linked dominant)- Fanconi
syndrome- renal tubular acidosis- oncogenic rickets
2. diminished intake or absorption of phosphatesClinical
features :- may present with tetany or convulsions- failure to
thrive, listlessness and muscular faccidity- craniotabes (pressure
over the soft membranous bones of the skull gives the feeling of a
ping pong ball being compressed and released)- bossing of the skull
(evident after age of 6 month)- broadening of ends of long bones,
commonly wrists and knees - delayed teeth eruption- Harrison's
sulcus (horizontal depression along lower part of chest)- Rachitic
rosary (costochomdral junctions on anterior chest wall become
prominent giving rise to appearance of a rosary)- muscular
hypotonia (child's abdomen becomes protuberant / pot belly because
of marked muscular hypotonia)- deformities- knock knees, bow
legs
Investigation :- X-ray -> delayed appearance of epiphysis
-> widening of epiphyseal plates (normal : 2-4mm) due to
excessive accumulation of uncalcified osteoid at growth plate ->
cupping of metaphysis -> splaying of the metaphysis -> bone
deformities eg knock knees, bow legs, coxa vara
Widening and cupping of the metaphyseal regions (see the image
below) Anteroposterior and lateral radiographs of the wrist
- serum calcium and phosphates decreases, alkaline phosphatase
increases- urine calcium decreases- calcium phosphate product
(calcium x phosphorus level mmol/L) normal : 3 diagnostic : <
2.4
Treatment :Medical treatment- Vit D 600 000 units single oral
dose induces rapid healing If line of sclerosis(healing) on
metaphyseal side of growth plate is not seen on X-ray within 3-4
weeks of therapy, same dose is repeated Unresponsive to Vit D
therapy, then maintenance dose of 400 IU of Vit D is given per
day
Surgical treatment (established long bone deformities)-
conservative methods eg. splints (mermaid splints), orthopaedic
shoes -> mild deformities correct spontanously- operative
methods eg. corrective osteomies -> moderate or severe
deformities often require surgery, after 6 months of starting
medical treatmentPrevention :- balanced diet that contains of
calcium (sources : daily products, soya beans, nuts) and Vit D
(sources : oily fish, eggs)- pregnant and breastfeeding women
should take daily supplement of 10ug of Vit D- Vit drops for all
babies and young children aged 6 months -5 yrs old
OsteomalaciaDefine : inadequate mineralization of bones in
adult, results of failure to replace turnover of calcium and
phosphorus in the organic matrix of boneHence, bone content is
demineralised and bone substance is replaced by soft osteoid
tissue
Etiology : - malabsorption- lack of exposure to sunlight-
under-nutrition during pregnancy- after partial gastrectomy
Clinical features :- bone pains (backache to diffuse bone pains
may occur)- muscular tenderness (difficulty in climbing stairs)-
spontaneous fractures occur usually in spine and may result in
kyphosis
Investigation :- X-ray-> diffuse rarefaction of bones ->
Looser's zone (pseudo-fractures) radiolucent zones occur at sites
of stress, commonly at pubic rami, axillary border of scapula,
ribs, medial cortex of the neck of femur -> triradiate pelvis
(female) -> acetabulum protruding into pelvis- low serum calcium
and phosphates, high alkaline phosphatase- bone biopsy->
excessive uncalcified osteoid
Treatment : - maintenance dose of 400 IU of Vit D daily- calcium
supplementation should be given- treat underlying causesMetabolic
Disease DisorderHigh bone turnoverPagets Disease and
HyperparathyroidismPagets disease(Osteitis deformans)Paget disease
is a localized disorder of bone remodeling that typically begins
with excessive bone resorption followed by an increase in bone
formation. This osteoclastic overactivity followed by compensatory
osteoblastic activity leads to a structurally disorganized mosaic
of bone (woven bone), which is mechanically -weaker, larger, less
compact, more vascular, and more susceptible to fracture than
normal adult lamellar bone. It is the second most common bone
disorder (after osteoporosis) in elderly persons. Paget disease may
involve a single bone but is more frequently multifocal. It has a
predilection for the axial skeleton (ie, spine, pelvis, femur,
sacrum, and skull, in descending order of frequency), but any bone
may be affected. After onset, Paget disease does not spread from
bone to bone, but it may become progressively worse at preexisting
sites.
EtiologyThe cause of Paget disease is unknown. Both genetic and
environmental factors have been implicated.Studies of potential
genetic markers for Paget disease have found an association between
human leukocyte antigenA (HLA-A), HLA-B, and HLA-C (class I) and
clinical evidence of disease. Alterations in cytokine expression
have been found in persons with Paget disease: elevated
interleukin-6 (IL-6) levels are found in bone marrow plasma and
peripheral blood in patients with Paget disease but not in healthy
controls.Macrophage-colony stimulating factor (M-CSF) may play a
role in Paget disease. M-CSF is a growth factor produced by many
cells, including osteoblasts and marrow fibroblasts. Significantly
high levels of M-CSF have been found in patients with untreated
Paget disease.Environmental factors - Viral infection(i.e
paramyxoviruses)
Symptoms
Most persons with Paget disease are asymptomatic. However, when
symptoms do occur, bone pain is the most common complaint. The bone
pain is dull, constant, boring, and deep below the soft tissues. It
may persist or exacerbate during the night.Hip pain is most common
when the acetabulum and proximal femur are involved, especially in
the sclerotic stage. Bowing of the femur and long bones or
protrusion of the acetabulum causes pain that becomes worse with
weightbearing and is relieved with rest. Knee and shoulder pain may
occur because of altered mechanical forces across the articular
joints from deformed bones.Nonspecific headaches, impaired hearing,
and tinnitus commonly result from skull involvement.The most common
cranial symptom is hearing loss, occurring in patients with skull
involvement. The most common neurologic complication is deafness as
a result of involvement of the petrous temporal bone.Back and neck
pain are common complaints, as Paget disease frequently affects the
spine, especially the lumbar and sacral regions. Softened bone at
the base of the skull may lead to platybasia, the descent of the
cranium onto the cervical spine. Progressive pain, paresthesias,
limb paresis, gait difficulties, or bowel and bladder incontinence
may be caused by compression of the spinal cord or spinal nerve
secondary to platybasia or vertebral
fractures.InvestigationsMeasurement of serum alkaline phosphatasein
some cases, bone-specific alkaline phosphatase (BSAP)can be useful
in the diagnosis of Paget disease. Elevated levels of urinary
markers, including hydroxyproline, deoxypyridinoline,
C-telopeptide,andN-telopeptide, may help identify patients with
Paget disease.Check for serum uric acid level- Elevated serum uric
acid levels have been found in men with severe Paget disease and
have been associated with gouty arthritis. Serum total acid
phosphatase is an osteoclastic enzyme that may be elevated in
active Paget disease. In males, however, the clinical value of this
finding is compromised, as acid phosphatase levels also may be
elevated in the presence of metastatic prostate carcinoma
Plain radiographs and bone scanning should be performed upon
initial diagnosis. Repeated radiography may be helpful in
monitoring an osteoarthritis program or in evaluating for malignant
degeneration.Computed tomography (CT) scanning and magnetic
resonance imaging (MRI) are not needed for the diagnosis of Paget
disease of bone. However, both are useful in the evaluation of
complications of Paget disease, such as neoplastic degeneration,
articular abnormalities, and spinal involvement with neurologic
compromise. Bone biopsies may be indicated to evaluate for
malignant transformation.
TreatmentThe short-term objective of Paget disease treatment is
to control disease activity. The long-term objectives of treatment
are to minimize or prevent disease progression and to decrease
complications from the disease, if possible.Indications for drug
treatment of Paget disease are as follows: Metabolic active disease
- Bone pain, fatigue fracture, skull/spine fracture, radiculopathy,
osteolytic lesions, bony deformities, weight-bearing bone
involvement, compression of spinal cord and nerve roots, bone
compression of the eighth cranial or optic nervePreparation for
orthopedic surgery (joint replacement anticipated at involved sites
within 6 months)Hypercalcemia or hypercalciuria - Recurrent renal
calculi due tohypercalciuria, or fractures; serum alkaline
phosphatase or urine hydroxyproline levels greater than twice the
upper limit of the reference range; immobilization
When Paget disease occurs around a joint, treatment is often
administered in an attempt to prevent development of
osteoarthritis. Drug therapy for Paget disease should include
bisphosphonate treatment with serial monitoring of bone markers.
Response to therapy is indicated by reduction of symptoms and
decreases in levels of BSAP (a bone formation marker) and
deoxypyridinoline,C-telopeptide,orN-telopeptide (bone resorption
markers).Secondary osteoarthritic pain may be reduced by
nonsteroidal anti-inflammatory drugs or other nonnarcotic
analgesics.Orthotic devices, including canes and walkers, may be
useful for patients with gait abnormalities resulting from Paget
disease that involves the lower limbs.Because of the increased risk
of malignancy, patients with Paget disease should be monitored
indefinitely. Chemotherapy, radiation, or both may be used to treat
neoplasms that arise from pagetic bone. Amputation may also be
necessary in the presence of a malignant transformation.
Hyperparathyroidism
Parathyroid gland anatomy and physiology
Normally 4 in numberLocated behind the thyroid gland one behind
each pole of the thyroidEach 6mm x 3mm x 2mm Dark brown
colorSecreted by the chief cells of the parathyroid glandControls
extracellular Calcium and phosphateRegulates intestinal
reabsorptionRegulates Renal excretionRegulates exchange of Ca and
PO4 ions in ECFExcess activity of Parathyroid - Rapid absorption of
calcium from bones HypercalcemiaRemoval of half - no major problem,
removal of - Hypoparathyroidism - Hypofunction of Parathyroid
Hypocalcemia - Tetany
HyperparathyroidismClassificationPrimary : excessive release of
PTH and manifests as hypercalcemia (no renal disease and no
malignancy) Looses sensitivity to circulating calcium : Parathyroid
adenoma Secondary: parathyroid glands become hyperplastic after
long-term hyperstimulation and release of PTH Elevated PTH levels
do not result in hypercalcemia Resistance to the action of PTH :
Chronic renal failure, intrinsic parathyroid gland abnormalities
Hyperparathyroidism + Renal pathology = Renal
osteodystrophyTertiary : excessive secretion of parathyroid hormone
(PTH) after a long period of secondary hyperparathyroidism and
resulting in hypercalcemia Long lasting disorders of the calcium
feedback control system Cannot be treated by
medicationSymptomsAsymptomatic hyperparathyroidism have no signs or
symptoms diagnosis being made on further investigation after a
coincidental finding of hypercalcemia Symptomatic
hyperparathyroidism associated with the effects of an increased
level of calcium - symptoms "neurological" in origin most common
symptom is fatigue and tiredness lack of energy, memory problems,
depression, problems with concentration, sleeping disorders Other
symptoms kidney - stones, bone pain - osteoporosisheadaches,
gastroesophageal reflux, decreased sex drive, thinning hair,
hypertension, and palpitations
Orthopaedic manifestations Bone pains due to Osteoporosis
Radiological Subperiosteal bone resorbtion and acroosteolysis
Radial side & tuft of phalanges Osteitis fibrosa cystica Brown
tumor of hyperparathyroidism Pepper Pot appearance - skull
Chondrocalcinosis & pseudogoutProximal muscle weakness
affecting lower more than upper limbs
Lateral radiograph skull: diffuse lytic lesions giving classical
pepper pot skull appearance.DiagnosisGold Standard : PTH
immunoassay
PTH Raised
RaisedCalcium levelsPrimary hyperparathyroidism PTH Raised
Normal Secondary hyperparathyroidismInvestigationsLaboratory
investigationsPTH level normal range for the PTH-intact assay -
10-65 pg/ml elevated PTH levels with hypercalcemia establishes
diagnosis of hyperparathyroidism in older individuals,
hypercalcemia of malignancy - associated with suppressed PTH levels
immunoradiometric assay for PTH detects fully intact molecule -
more accurate rapid PTH assay provides an accurate PTH level used
intraoperatively - determine quantitatively the excision of
hyperfunctioning parathyroid tissue decrease PTH concentration -
> 50% from the baseline level 5-10 mts after excision - absence
of residual hyperfunctioning tissue
Calcium levels: Hypercalcemia or normal calcium depending on the
type of hyperparathyroidism
Urinary calcium excretion : may be elevated
Phosphate levels: decreased serum phosphate level of < 2.5
mg/dL (0.81 mmol/L) may be seen
Increased bone turnover : elevated alkaline phosphatase and
urinary pyridinoline (bone resorption)
Imaging StudiesNoninvasive imaging modalities Technetium-99m
sestamibi imaging, Ultrasonography CT scanning & MRI
Ultrasonography and 99mTc sestamibi scanning widely available
and relatively inexpensive
Radiologytypical radiography findingsbone-density measurements
based on (DEXA) at the hip and spinebrown tumors are seen only in
patients who are severely affected soft tissue calcification in
joints, kidneys & lungs
CT scanning of spine provides estimates of spinal bone density
serial measurements provides an early indication progressive
osteopenia
Percutaneous needle biopsy - aspiration cytology & tissue
PTH malignancy suspected
TreatmentEmergency Department Care
Focused on the treatment of hypercalcemia Goal of treatment is
to reduce calcium level to below 11.5 mg/dL
Intravenous administration of isotonic saline First and vital
step in management of severe hypercalcemia Severe hypercalcemia -
nearly always accompanied by severe dehydration
Patients with hypercalcemia with alterations of mental status
loop diureticsfacilitate the urinary excretion of calcium prevents
volume overload - following administration of large volumes of
saline Initiation of loop diuretics should only after rehydration
has taken place
Postmenopausal with mild hyperparathyroidism - estrogen therapy
it may inhibit demineralization of the skeleton - reduce blood
calcium levels
directed at hypercalcemia symptomatic patients adviced surgery
removal of the parathyroid tumor (parathyroid adenoma) Present
belief : almost all patients with hyperparathyroidism should be
evaluated for surgery will almost always progress as the tumor
grows if surgery is not available - monitor Calcium level: via
urine tests - results inform kidney function Bone density: used to
assess the risk of osteoporosis Check for kidney stones: abdominal
X-rays
THANK YOU