Embed Size (px)
Citation preview

MERSEYSIDE FAMILY DOCTOR ASSOCIATION GP EVENT
Saturday 14 November 2015
WHERE IS PRIMARY CARE GOING?
Katherine Sheerin
Chief Officer
NHS Liverpool Clinical Commissioning Group

Overview
LOCAL TRANSFORMATION
HEALTHY LIVERPOOL GENERAL PRACTICE SPECIFICATION
NATIONAL PERSPECTIVE
REFLECTION AND QUESTIONS

The Ultimate Goal and ContextHealthy Liverpool ProgrammeVision ‘a healthcare system in Liverpool that is person-centred,
supports people to stay well and provides the very best in care’
Outcomes Improving health outcomes for people in Liverpool relative to
the rest of England and reducing health inequalities within the city
Quality of healthcare is consistent and high quality New model of care which is clinically and financially
sustainable
3

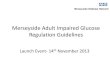
£643m£83m
£29m
£84m £13m
£128m
£147m
£58m
LIVERPOOL
HEALTH SPEND
CCG PROGRAMMES
PRESCRIBING
CHILDREN’S SOCIAL CARE
PUBLIC HEALTH
ADULT SOCIAL CARE
LEISURE/PARKS GENERAL PRACTICE
OTHER PRIMARY CARE
SPECIALISED SERVICES
£37m

LIVING WELL
DIGITAL HEALTH
COMMUNITY TRANSFORMATION
URGENT CARE
MENTAL HEALTH
HEALTHY AGEING
LEARNING DISABILITIES CHILDREN
System Wide Transformation Programmes
Continuous Improvement Programmes
HOSPITAL TRANSFORMATION
CANCERLONG TERM CONDITIONS
HEALTHY LIVERPOOL PROGRAMME

Liverpool Community Care Model

Healthy Liverpool Community Care Programme Plan on a Page
Vision and Outcome Ambition for Healthy Liverpool
Improved Health Outcomes Deliver First Class ServicesDelivering a Sustainable
System
Preventing people from dying
prematurely
Enhancing quality of life
Delaying and reducing the need
for care and support
Community Care Outcome Domains
Ensuring that people have a positive experience of
care and support
Specialist Clinical Integration‘care closer to home’
Community Care Teams‘no wrong door’
Managing Complex Needs‘supporting the vulnerable’
Enablers: Digital Care Estates Proactive Care High Quality Primary Care Community Engagement Workforce Access
Neighbourhood Collaborative
‘maximising community assets’
Prevention of ill health, health protection and maintaining healthy
lifestyles
‘a health care system in Liverpool that is person-centred, supports people to stay well and provides the very best in care’
Neighbourhood Delivery
Establish Community Care Team in each
Neighbourhood
Community Diagnostics
Seven Day Access
Scale up use of Assistive Technologies
Common Assessment Framework
Early Help Support
Clinical Model for Care Homes and Community
Beds
Pathways of Care for Long Term Conditions
Eliminating Unwarranted Variation in Care
Mental Health Integration
Dementia Clinical Network
Transformed Cancer Services
Children’s Pathways of Care
Planned Care Redesign
End of Life Services
Integration of non-medical programmes
Directory of Service Live Well Liverpool
Community Grants
Support for the Homeless
Collaboration with Housing and Fire and Rescue
Services
Maximise use of Community Estate
Complex Alcohol and Addictions
Healthy Lung Initiative
Tackling Social Exclusion
Health Trainer Services
Severe Mental Illness
Children with Complex Needs
Learning Disability
Embedding Self-Care Shared Decision Making Prevention at Scale Early Detection and Diagnosis
Establish Centres for Wellbeing
Targeted Support for ‘Hard to Reach’ Groups

EXCELLENT GENERAL PRACTICE IS
FUNDAMENTAL TO DELIVERING HEALTHY
LIVERPOOL!!!

Liverpool General Practice Specification
Standards for all practices
Investment equalised
Differential resources at risk
Clear performance targets
Prevention
Early Identification
Improved Clinical Management
Use of Resources
Access
What have we achieved?

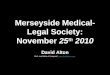
All A&E Attendances: Trust CatchmentYear
2009/10 109,505 86,178 693,835
2010/11 107,457 -2% 87,190 1% 713,560 2.80%
2011/12 107,985 0% 83,956 -4% 796,882 11.70%
2012/13 109,337 1% 86,380 3% 807,223 1.30%
2013/14 103,713 -5% 79,575 -8% 810,935 0.50%
2014/15 112,690 8.70% *113,239 Not comparable
847,080 4.50%
RLUBHT AHT Benchmark Trusts
Year
2009/10 57,944 99,013
2010/11 58,924 2% 97,335 -2%
2011/12 56,856 -4% 98,319 1%
2012/13 57,473 1% 102,226 4%
2013/14 56,120 -2% 101,163 -1%
2014/15 55,731 -0.7% 106,632 5%
Alder Hey Benchmark Trusts
Data Source: National AED Sitrep*Aintree A&E attendances increased during 2014/15 due to Walk in Centre activity being counted against AUH A&E
Acute Benchmarks Trusts: Bradford Teaching Hospital, St Helen’s and Knowsley Hospital, University Hospital of South Manchester, Salford Royal Foundation Trust, University Hospital of Birmingham Foundation Trust, Newcastle Upon Type Hospital Trust, Southport and Ormskirk Hospital Trust Childrens Benchmark Trusts: Sheffield Children's Hospital Trust, Birmingham Children's Foundation Trust
2014/15• Royal Liverpool Hospital reported a
8.7% increase in A&E activity during 2014/15 (112,690 attendances) compared to 2013/14 (103,713 attendances)
• Aintree Hospital’s increase in A&E activity during 2014/15 is not comparable to previous years due to walk in centre activity being counted against AUH.
• Peer providers of Royal Liverpool Hospital and Aintree Hospital reported a 4.5% increase in A&E attendances
• Alder Hey Children's hospital reported a 0.7% reduction in A&E attendance rates during 2014/15 compared to a 5% increase reported by peer providers

LCCG Data Source: General practice systems / immform returnEngland Data Source: http://www.phoutcomes.info/public-health-outcomes-framework
Year 2011/12 2012/13 2013/14 2014/15%
Variance on 11/12
Patients aged >65
LCCG 77.80% 77.69% 76.92% 77.12% -0.68
England 74.00% 73.40% 73.20% 72.70% -1.30
Patients aged <65 at
risk
LCCG 54.90% 57.47% 57.94% 58.24% 3.34%
England 51.60% 51.30% 52.30% 50.30% -1.30
Influenza Vaccinations

Vacs up to age 2: DTaPIPV at 1 year, HibMenC at 2 yrs, MMR1 at 2 years, PCV1 at 2 yearsVacs up to age 5: DTAPIPV at 5 years, MMR2 at 5 years*England benchmarks estimated using data from http://www.hscic.gov.uk/pubs/immstats .
2011/12 2012/13 2013/14 2014/15 % Variance on 11/12
Year
Vaccs up to age 2
LCCG 95.40% 95.77% 94.45% 93.82% -1.58%
England* 93.73% 94.13% 94.13% 93.44% -0.29%
Vaccs up to age 5
LCCG 87.90% 92.31% 91.40% 89.61% 1.71%
England* 86.70% 88.30% 88.37% 88.58% 1.88%
Childhood Vaccinations

Data source: general practice systems
YearPatients
drinking over recommended
levels
Of those, number
offered brief intervention
% Offered brief intervention
Year on year % variance
2011/12 14146 11317 80.00% 5.00%
2012/13 14578 12624 86.60% 6.59%
2013/14 12393 11159 90.04% 3.44%
2014/15 11244 10347 92.04% 2.00%
Alcohol: brief interventions

Data source: general practice systems
Prevalence in patients aged 40+
CHD HFStroke /
TIAAF
Hypertension
COPD DiabetesTotal on selected registers
Actual varience from baseline year
(2012)
% varience from baseline
year (2012)
End Mar 12 17406 3458 7906 6416 58649 12698 19225 125758
End Mar 13 20679 3836 8516 7443 65289 14214 21940 141917 16159 12.8%
End Mar 14 18540 3923 8833 7747 65889 14379 24304 143615 17857 14.2%
End Mar 15 18235 3924 8882 8045 66674 14661 24993 145414 19656 15.6%
• Since baseline year (2012) Liverpool has reported a 15.6% increase in QOF disease registers
• As at March 2015 Liverpool’s disease register size stands at 145,414• The number of extra entries on the register does not necessarily equal 16159 (as
reported end of March 2013) additional new patients as 1 patient can be on multiple registers

Data Source: Local SUS data flow
Based on ACS admissions to RLBUHT, AHT, AHCH, ST H&K
Definition: ACS admissions for Angina, Asthma, Cellulitis, Congestive Heart Failure, COPD, Convulsions and epilepsy, Diabetic complications, ENT, Flu and Pneumo
Year Non-elective admissions
% Variance (on previous year)
2011/12 6667 -11.47%
2012/13 6776 1.63%
2013/14 6590 -1.59%
2014/15 7328 11.19%
Variance 11/12 to 14/15 661 9.19%
Non-Elective ACS Admissions: LCCG

Data Source: Dr FosterNational ACS definition for 19 Ambulatory Care Sensitive ConditionsBenchmark: North of England Commissioning Region
Non-Elective ACS Admissions trends
LCCGRate per 1,000
LCCGTotal ACS
admissions
Ranking(Out of 68 CCGs, 1 =
Best)
North of England Commissioning
Region Rate2009/10 21.9 11,268 68 21.12010/11 24.7 11,912 64 19.72011/12 19.6 9,603 35 19.32012/13 19.5 9,669 23 202013/14 19.5 9,685 27 19.82014/15 21.4 10,620 31 21.1
2014/15• LCCG reported a slight
increase in ACS admission rates in 2014/15 with a rate of 21.4 per 1,000 population
• Based on historical data LCCG have moved from reporting the highest ACS admission rates in 2009/10, ranked 68 out of 68 CCGs within North of England Region to being ranked 31 out of 68 in 2014/15

Data Source: Local Sus data
Definition is GP referred (03) first outpatient attendances to Dermatology, T&O, Gynaecology, Rheumatology, ENT, Gastroenterology, Vascular Surgery and Urology (using TFC to define speciality)
Data source: Local SUS dataflow*Includes activity at ICATS, MCAS, RheuCAS but does not include those in primary care such as H Pylori testing, minor surgeryBased on activity at RLBUHT, AHT, AHCH, St H&K
Year GP Ref’d first OP atts*
% Variance (on previous
year)
GP Ref’d first OP atts plus assessment
services* atts
% Variance (on previous
year)
2011/12 43113 -8.73% 72403 -5.01%
2012/13 41338 -4.12% 69338 -4.23%
2013/14 42432 2.65% 66863 -3.57%
2014/15 38625 -8.97% 63997 -4.29%
Var 11/12 to 14/15 -4488 -10.41% -8406 -11.61%
GP Referred first outpatient attendances: LCCG

Prescribing Cost
• Prescribing cost increased by 2% (£1,829,924) during 2014/15 compared to 2013/14 for Liverpool CCG
• Cost variance reduced from 4% increase in costs reported in 2013/14 to 2% increase in cost reported in 2014/15
• Liverpool increase in prescribing cost during 2014/15 is reported to be lower than North West and National increase
Datasrouce: EPACT
YearPrescribing outturn
Variance on previous year
% VarianceNorth West %
VarianceNational %
Variance
2010/11 £87,958,7362011/12 £85,333,373 -£2,625,362 -3%2012/13 £79,422,452 -£5,910,921 -7% -4%2013/14 £82,437,116 £3,014,665 4% 3% 3%2014/15 £84,267,040 £1,829,924 2% 3% 3%

Datasrouce: EPACT
Prescribing trends
*ASTRO PU figures included above are different to those previously reported due to ASTRO PUweightings changing. North West changed to Merseyside Area Team in 2012/13 therefore coding changed and as such old North West data is not available 2012/13 and before for comparison

Diabetes 9 care processes
YearLCCG
% Receiving 9 care processes
Highest performingpractice
Lowest performingpractice
% Performance Varience
(highest performing practice - Lowest
performing practice
2012/13 42.4% 77.9% 20.0% 58.0%
2013/14 58.3% 91.6% 15.3% 76.3%
2014/15 65.1% 96.0% 10.8% 85.2%
Overall Var 12/13 to 14/15 22.7% 18.1% -9.2% 27.2%
Datasrouce: EMIS
• Overall performance has increased by 22.7% since 2012/13• Performance variance across the city has increased by 27.2%• The increase in performance variance is due to higher performing
practices increasing their rates and lower performing practices reducing their rates

EXCELLENT GENERAL PRACTICE IS
FUNDAMENTAL TO DELIVERING HEALTHY LIVERPOOL – BUT IS
THIS ENOUGH?

NATIONAL PERSPECTIVE
• FIVE YEAR FORWARD VIEW
• NEW CARE MODELS – ‘VANGUARDS’
• SEVEN DAY PRIMARY CARE SERVICE
• RCGP ‘BLUEPRINT’

THOUGHTS AND QUESTIONS