Embed Size (px)
Citation preview

MEDPHARM 03/22/2010
VIGNETTEA 58 YEAR OLD HEALTHY UNIVERSITY
PROFESSOR IS ENJOYING A PERIOD OF
ATTITUDE ADJUSTMENT WHEN HE
BECOMES AWARE OF A TINGLING
SENSATION IN THE LEFT GREAT TOE.
WITHIN HOURS THE TOE PAIN IS 10/10
THE Dx IS ACUTE GOUT


ANTIINFLAMMATORY-ANALGESIC-ANTIPYRETIC DRUGS
NONSTEROIDAL(NSAIDs) STEROIDAL 7 million Rx per year 3.8% of all Rx +
OTC Use increases with age Age >65 yr use 10-15% of NSAIDS RR of 3-5X for hospitalization/death due to
PUD ADRs cost ~$ 1 billion per year

NSAIDs NONSTEROIDAL ANTIINFLAMMATORY DRUGS
Aspirin Ibuprofen ( Advil, Motrin) And many others of differing
chemical classes Acetaminophen (Tylenol) Celecoxib (Celebrex)
NSAIDs Major Actions
ANALGESIA ANTIPYRETIC ANTIINFLAMMATORY Except acetaminophen
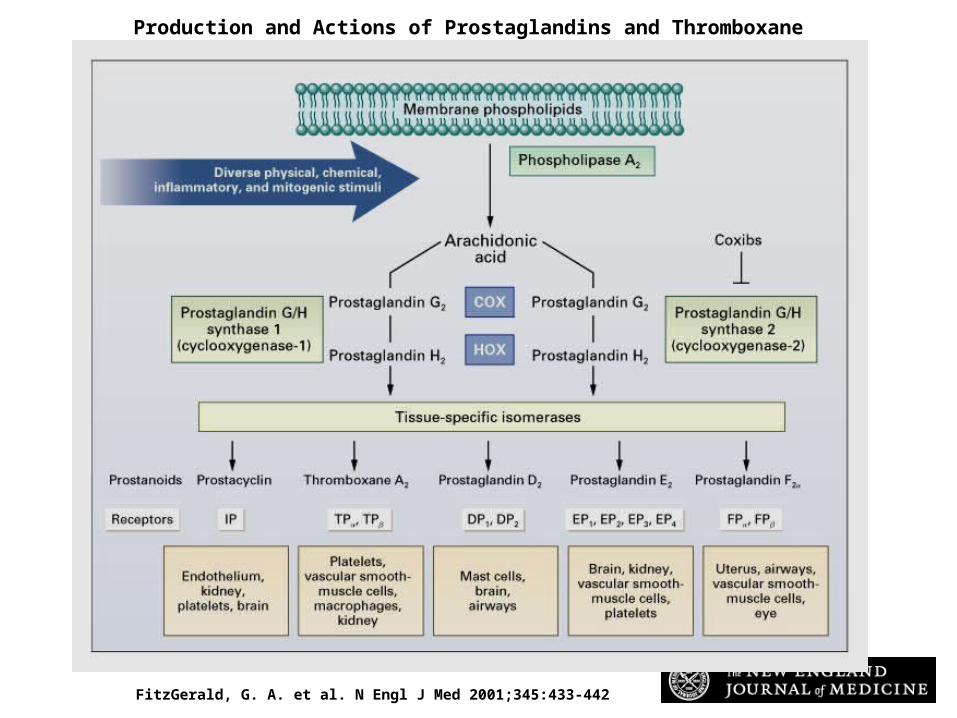
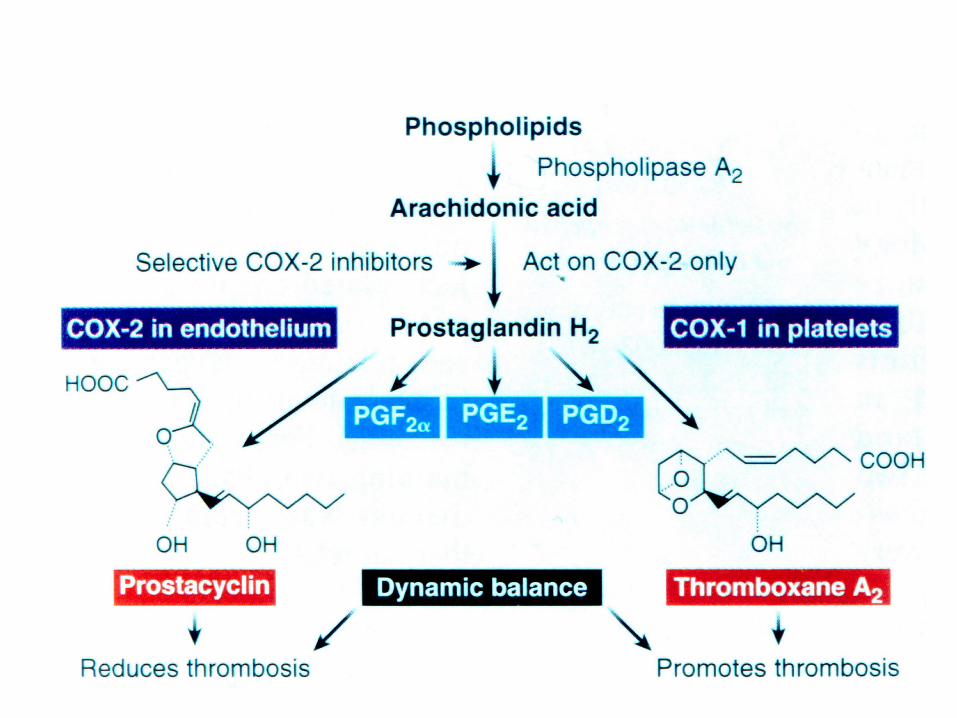
FitzGerald, G. A. et al. N Engl J Med 2001;345:433-442
Production and Actions of Prostaglandins and Thromboxane


Catella-Lawson F et al. N Engl J Med 2001;345:1809-1817
The Effect of Aspirin Alone and of Ibuprofen plus Aspirin on Platelet Cyclooxygenase-1

ASPIRIN Major Actions Antiinflammatory action Inhibits NFB activation to limit
production of proinflammatory mediators
Changes in vascular permeability, leukocyte infiltration and organ dysfunction are prevented


ASPIRIN Major Actions
ANALGESIA Blocks production of PGs that
sensitize nociceptors to inflammatory mediators
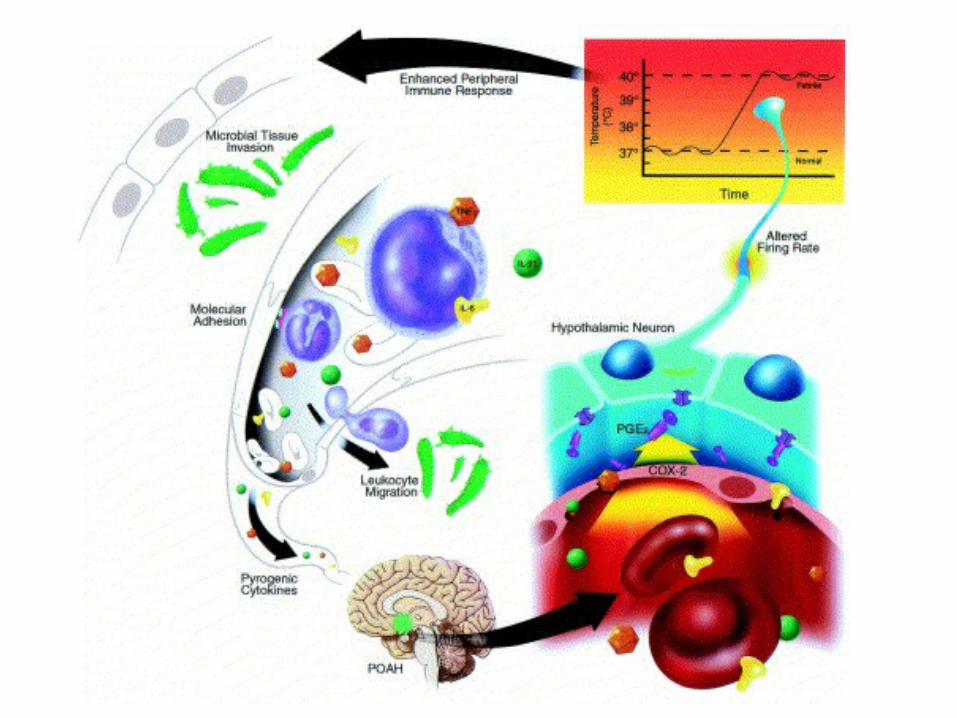
ASPIRIN Major Actions
Antipyretic action Block the production of PGE2 to
reset the hypothalamic temperature set point

ASPIRIN Major Actions
Antiplatelet/antithrombotic Decreases platelet production of
TXA2 by COX-1 to limit platelet aggregation and vasoconstrictiion

Normal physiologic interaction between PGI2 and TXA2 in platelet and endothelial cell biology
Blood Vessel WallEndothelial Cell (COX-2)
Ca2+/vessel smooth muscle constricts
Arachidonic acid
PGH2
Prostacyclin (PGI2)
cAMP/vessel smooth muscle relaxes
Arachidonic acid
PGH2
Thromboxane (TXA2)
cAMP aggregation
Ca2+ aggregation
Platelet (COX-1)

ASPIRIN / NSAID - ADRs (NOT ACETAMINOPHEN) GASTROINTESTINAL BLEEDING PREGNANCY RENAL ASPIRIN/other NSAID SENSITIVITY All due to alteration of normal prostaglandin physiology USE IS AVOIDED IN CHILDREN with viral
illness

ASPIRIN/OTHER NSAID SENSITIVITY REACTIONS Non-immunologicaly mediated Signs and symptoms Rhinitis Nasal polyps Asthma Urticaria Laryngeal edema BronchospasmAVOID ALL SALICYLATES/NSAIDs ACETAMINOPHEN IS OK TO USE

Copyright restrictions may apply.Gollapudi, R. R. et al. JAMA 2004;292:3017-3023.
Aspirin/Other NSAID Sensitivity Reactions via Inhibition of the Cyclooxygenase Pathway


ASPIRIN/ NSAIDs ADVERSE GI EFFECTS
BLEEDING
ULCERATION
OBSTRUCTION

Levy, D. J. N Engl J Med 2000;343:863
A 76-year-old woman had iron-deficiency anemia, a hematocrit of 24 percent, and a positive test for occult blood in stool

ASPIRIN/NSAIDs RISK FACTORS for GI EFFECTS Age > 65 years History of peptic ulcer or bleeding Multiple NSAID use High dose use Alcohol Anticoagulant use

NSAIDsMECHANISM of GI EFFECTS
LOSS of CYTOPROTECTIVE ACTIONS of GASTRIC PROSTAGLANDINS
Acid secretion is unabated Decrease in protective mucus Decrease in mucosal blood flow

NSAIDs BLEEDING
ANTI-PLATELET ACTIONS Loss of Thromboxane A2 Actions Platelet aggregation
inhibited Loss of vasoconstriction
NSAIDs on GESTATION and DELIVERY
BLEEDING Antepartum and postpartum
Transfusion requirement is increased
Gestation is prolonged Premature closure of the ductus

RENAL PROSTAGLANDINS
Modulate Na, K and water excretion NSAIDs (ibuprofen) block the above
to reduce Na & K excretion and may
cause inrease in blood pressure & weight

NSAIDs RENAL EFFECTS
Little effect on normal kidneys NSAIDs PROMOTE Na RETENTION When renal blood flow is impaired as
in: Heart failure Dehydration Kidney disease Normal aging
ANALGESIC USE & HEARING LOSS
REGULAR USE OF ASPIRIN+NSAIDS+ ACETAMINOPHEN INCREASES THE
RISK OF HEARING LOSS IN MEN
The impact is greater in younger persons

ASPIRIN & CHILDREN
AVOID IN FEBRILE ILLNESS The risk is that of Reyes’ syndrome
with liver injury and encephalopathy

Catella-Lawson F et al. N Engl J Med 2001;345:1809-1817
The Effect of Aspirin Alone and of Ibuprofen plus Aspirin on Platelet Cyclooxygenase-1
D-D-I

ASPIRIN DISPOSITION
ABSORPTION DISTRIBUTION METABOLISM EXCRETION

ASPIRIN PHARMACOKINETICS
DOSE-DEPENDENT HALF LIFE ASPIRIN 15 MINUTES SALICYLATE low dose 2-3 hours high dose 12-15 hours

ASPIRIN OVERDOSE
Combined metabolic acidosis & respiratory alkalosis

OTHER NSAIDs(IBUPROFEN) Several distinct chemical classes Kinetics and potency vary COX-1 and COX-2 inhibition COX inhibition is reversable Adverse event profile is like aspirin Great variability in individual response Change to another NSAID Not used as antiplatelet drugs
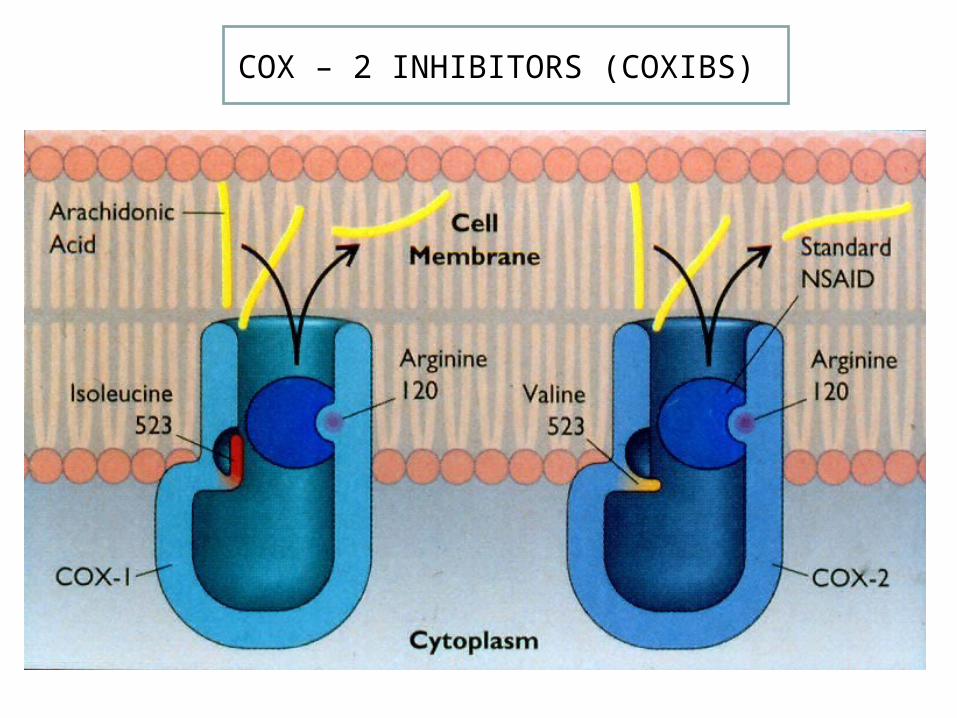
COX – 2 INHIBITORS (COXIBS))

SELECTIVE COX-2 INHIBITION

COX-1 COX-2

COXIBS SELECTIVE COX-2 INHIBITORS
THE PROBLEMATIC ASSUMPTIONS: COX-1 PRODUCTS ARE CONSTITUTIVE, i.e., HOMEOSTATIC/PROTECTIVE
COX-2 INDUCIBLE- PRODUCTS ARE ASSOCIATED WITH DISEASE STATES
COXIBS SELECTIVE COX-2 INHIBITORS
THE PROBLEM No clear distinction between the homeostatic and pathologic actions of the products of COX-1 and COX-2 The risk is that of MI & ischemic stroke

COXIBs APRIL 2008
Rofecoxib(Vioxx) Withdrawn
Valdecoxib(Bextra) Withdrawn
Celecoxib No direct-to customer marketing
FDA Panel: Keep COX-2 Drugs on
Market,Caution urged for all NSAIDs
STILL ON THE MARKET

COXIB ALTERNATIVES
FOR PATIENT AT RISK OF GI TOXICITY Salsalate,diclofenac,diflunisal & others May need to add: PPI(omeprazole) Misoprostol H-2 blocker(ranitidine)
MISOPROSTOL
A PROSTAGLANDIN ANALOG
Actions
Antisecretory
Prevention of NSAID ulcers
Adverse Effects
Diarrhea
Abortion

ACETAMINOPHEN
Analgesic and Antipyretic Inhibition of neuronal & vascular PGE2
generation
Poor antiinflammatory & antiplatelet activity: failure to inhibit platelet TXA2
inflammatory PGE2 synthesis Little GI toxicity Potentially hepatotoxic
ACETAMINOPHEN TOXICITY
Hepatotoxic when dose >4 gm/day Hepatotoxicity may occur @ doses
<4gm/d following binge drinking Hepatic centrilobular necrosis AST/ALT >1000 units Treat with n-acetylcysteine orally
ACETAMINOPHEN ACUTE LIVER FAILURE
55% of ALF in US Median dose 24 gm Unintentional OD 48% Intentional(suicide) 44% Survival 65% Death 27% Tx 8%

ACETAMINOPHEN /ALF RISK FACTORS
Depression Chronic pain Alcohol or narcotic use Simultaneous use of multiple
preparations of acetaminophen

ALCOHOL

Lee, W. M. N Engl J Med 2003;349:474-485
The Role of Ethanol in the Formation of N-acetyl-p-benzoquinone-imine (NAPQI), the Toxic Metabolite of Acetaminophen (APAP), and the Dynamics of Enzyme Induction
DISASTER AT THE FARM