Embed Size (px)
Citation preview

381DOS Times - Vol. 11, No. 6 December, 2005
The goal of perimetry is to establish an accurateestimate of visual field sensitivity. Perimetry is performedto detect early visual field defects, determine specificpatterns of visual field loss for differential diagnosis andmonitor for evidence of progression of field loss.Conventionally Standard Achromatic Perimetry (SAP) has
been used to achieve these purposes but there are certaininherent disadvantages. Newer techniques have developedin need for faster methods of screening, diagnosis andfollow-up as compared to conventional perimetry and toexamine motion attributes of vision that is involved earlyin glaucoma and not picked up by conventional perimetry.Frequency doubling technology (FDT) perimetry is such anewly developed technique for the screening and earlydetection of glaucoma.1-9
Frequency Doubling Theory
The human retina has approximately 1.2-to-1.5million neurons (also called retinal ganglion cell axons ornerve fibers) that bundle together to comprise the opticnerve. The irreversible loss of these retinal nerve fibersoccurs in glaucoma and other ocular conditions, associatedwith the classic gradual increase in optic nerve "cup" sizeover time. Some studies have suggested that up to 40percent of these retinal nerve fibers could die before any
notable visual field loss is found, so the patient may beunaware of any visual problem. It may take an average of3-5 years of gradual nerve fiber loss before varied amountsand patterns of glaucomatous visual field loss becomeapparent.
Retinal nerve fibers can be simply classified into two
main types that transmit signals from the retinal receptorcells by way of the optic nerve to the lateral geniculatebody and ultimately to the visual cortex. These are theMagno-cellular (or M) cells, and the Parvo-cellular (or P)cells.
The M-cell pathway is responsible for low-contrast;
high temporal frequency (or motion) stimulus detection.10
The P-cell pathway is responsible for high-contrast, lowtemporal frequency (or static) stimulus detection. The largerdiameter M cell neurons constitute approximately 10% ofthe total number of retinal nerve fibers. It has been foundthat a particular M-cell neuron sub-set comprising a thirdto a half of the M-cell neurons (called "non-linear" M-cells)
Frequency Doubling PerimetryTanuj Dada, Subrata Mandal
are usually the first to die in glaucoma, and this uniquepathological characteristic established the basis forfrequency doubling testing. When a low spatial frequencysinusoidal grating with alternating wide light and darkbars undergoes high temporal-frequency counterphaseflicker, (i.e., the black bands reverse to become white and
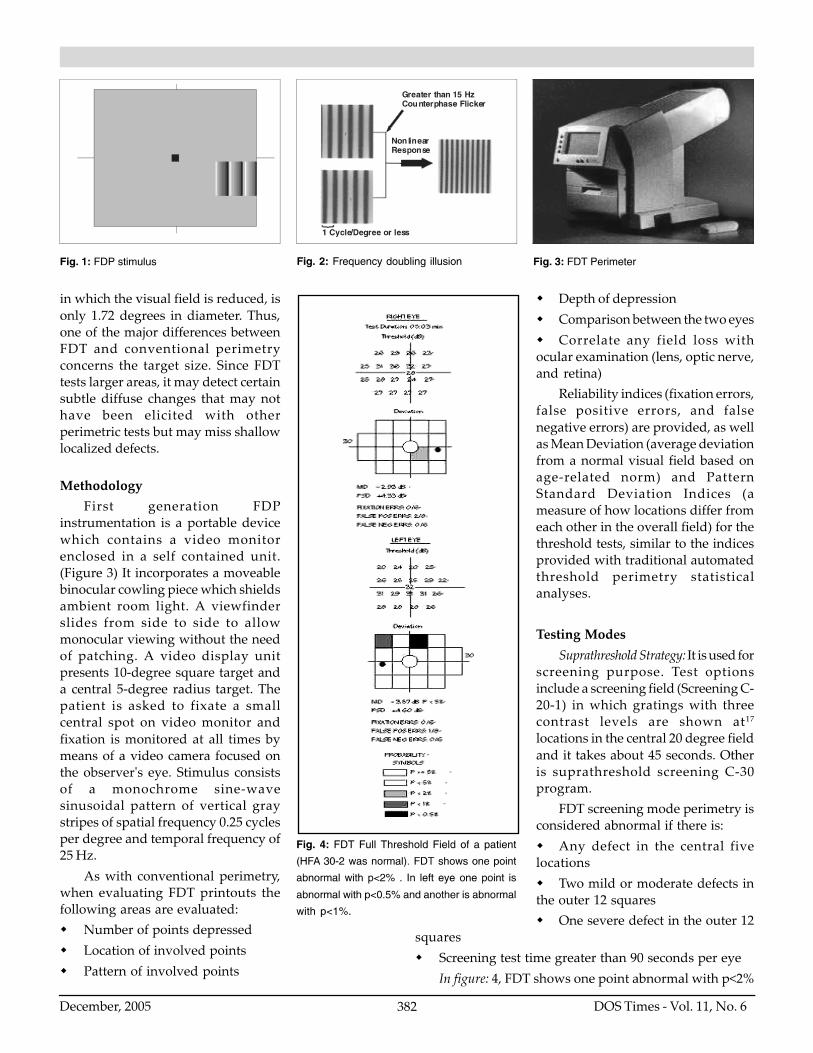
the white bands reverse to become black in rapid sequence)the grating appears to have twice as many light/dark bars(i.e., its spatial frequency appears doubled). Thisphenomenon is called the frequency doubling illusion.(Figure: 1, 2) It is the vulnerable "non-linear" M-cell neuronsthat are thought to transmit signals related to this illusion.Since these M-cell neurons tend to be among the first todie, selective testing by presenting alternate grating stimuliwas developed to attempt to identify earlier retinal neuronloss than by traditional automated perimetry.
Using the frequency doubling illusion as the basis fordevelopment, a perimeter was developed that has beencalled the Frequency Doubling Technology (FDT) perimeter(Welch Allyn & Humphrey Instruments, Inc). In FDT, ratherthan using a small spot of light as in conventionalperimetry, a large low spatial frequency sinusoidal grating(<1 cycle/degree) that consists of black and white barsundergoes a rapid counter phase flicker (>15 Hz) so thatthe black bars become white and the white bars become
black. The use of a low spatial frequency target undergoingrapid flicker leads to the frequency doubling illusion inwhich, at a certain level of contrast, the number of visiblelines appears to double. At this point the person viewingthe stimulus will see twice as many bars as are actuallypresent in the grating. Maddess10, 11 in his description ofthe frequency doubling illusion suggested that M cells, dueto their nonlinear properties, are the retinal cellsresponsible for eliciting the illusion.
There are two different theories as to how frequency-doubling perimetry is able to detect changes in the visualfield. In one theory, it is assumed that the large-diameteroptic nerve fibers (M) are preferentially damaged in theearly stages of glaucoma. In the other theory12, referred toas the Reduced Redundancy Theory, it is assumed that avisual field test will be more sensitive to early loss if onlya subset of the visual system is tested.
In comparison to conventional perimetry, FDT differsin its use of a target that stimulates a much larger retinalarea. The standard FDT target is a square ten degrees indiameter, which is much larger than the size III Goldmanntarget equivalent that shines a spot of light 0.43 degrees indiameter onto the retina. The size V Goldmann target, thelargest size available and usually reserved for conditions
Department of OphthalmologyR.P. Centre, AIIMS,New Delhi
MEDICAL OPHTHALMOLOGY
383DOS Times - Vol. 11, No. 6 December, 2005
and another point abnormal with p<5% in right eye. In lefteye one point is abnormal with p<0.5%, another point isabnormal with p<1% and four points abnormal with p<2%.Standard automated perimetry with HFA30-2 of the samepatient was normal.
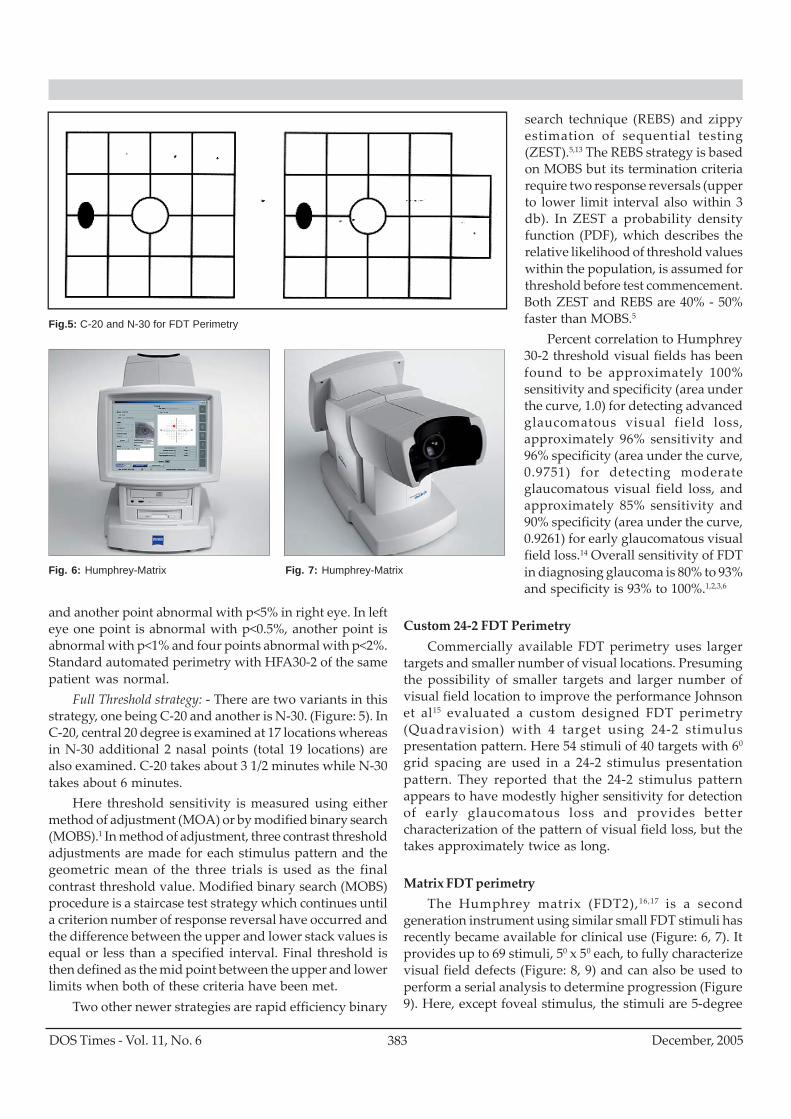
Full Threshold strategy: - There are two variants in thisstrategy, one being C-20 and another is N-30. (Figure: 5). InC-20, central 20 degree is examined at 17 locations whereasin N-30 additional 2 nasal points (total 19 locations) arealso examined. C-20 takes about 3 1/2 minutes while N-30takes about 6 minutes.
Here threshold sensitivity is measured using eithermethod of adjustment (MOA) or by modified binary search(MOBS).1 In method of adjustment, three contrast thresholdadjustments are made for each stimulus pattern and thegeometric mean of the three trials is used as the finalcontrast threshold value. Modified binary search (MOBS)procedure is a staircase test strategy which continues untila criterion number of response reversal have occurred andthe difference between the upper and lower stack values isequal or less than a specified interval. Final threshold isthen defined as the mid point between the upper and lowerlimits when both of these criteria have been met.
Two other newer strategies are rapid efficiency binary
search technique (REBS) and zippyestimation of sequential testing(ZEST).5,13 The REBS strategy is basedon MOBS but its termination criteriarequire two response reversals (upperto lower limit interval also within 3db). In ZEST a probability densityfunction (PDF), which describes therelative likelihood of threshold valueswithin the population, is assumed forthreshold before test commencement.Both ZEST and REBS are 40% - 50%faster than MOBS.5
Percent correlation to Humphrey30-2 threshold visual fields has beenfound to be approximately 100%sensitivity and specificity (area underthe curve, 1.0) for detecting advancedglaucomatous visual field loss,approximately 96% sensitivity and96% specificity (area under the curve,0.9751) for detecting moderateglaucomatous visual field loss, andapproximately 85% sensitivity and90% specificity (area under the curve,0.9261) for early glaucomatous visualfield loss.14 Overall sensitivity of FDTin diagnosing glaucoma is 80% to 93%and specificity is 93% to 100%.1,2,3,6
Custom 24-2 FDT PerimetryCommercially available FDT perimetry uses larger
targets and smaller number of visual locations. Presumingthe possibility of smaller targets and larger number ofvisual field location to improve the performance Johnsonet al15 evaluated a custom designed FDT perimetry(Quadravision) with 4 target using 24-2 stimuluspresentation pattern. Here 54 stimuli of 40 targets with 60
grid spacing are used in a 24-2 stimulus presentationpattern. They reported that the 24-2 stimulus patternappears to have modestly higher sensitivity for detectionof early glaucomatous loss and provides bettercharacterization of the pattern of visual field loss, but thetakes approximately twice as long.
Matrix FDT perimetryThe Humphrey matrix (FDT2),16,17 is a second
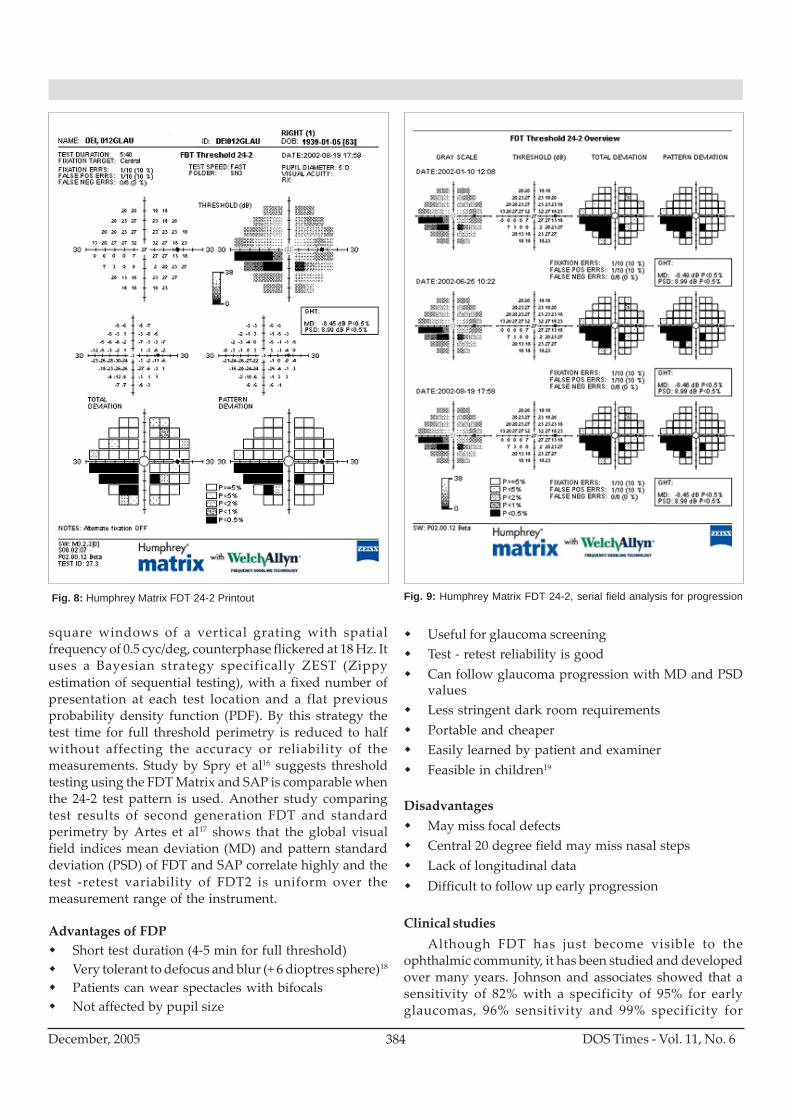
generation instrument using similar small FDT stimuli hasrecently became available for clinical use (Figure: 6, 7). Itprovides up to 69 stimuli, 50 x 50 each, to fully characterizevisual field defects (Figure: 8, 9) and can also be used toperform a serial analysis to determine progression (Figure9). Here, except foveal stimulus, the stimuli are 5-degree
Fig.5: C-20 and N-30 for FDT Perimetry
Fig. 6: Humphrey-Matrix Fig. 7: Humphrey-Matrix
DOS Times - Vol. 11, No. 6December, 2005 384
square windows of a vertical grating with spatialfrequency of 0.5 cyc/deg, counterphase flickered at 18 Hz. Ituses a Bayesian strategy specifically ZEST (Zippyestimation of sequential testing), with a fixed number ofpresentation at each test location and a flat previousprobability density function (PDF). By this strategy thetest time for full threshold perimetry is reduced to halfwithout affecting the accuracy or reliability of themeasurements. Study by Spry et al16 suggests thresholdtesting using the FDT Matrix and SAP is comparable whenthe 24-2 test pattern is used. Another study comparingtest results of second generation FDT and standardperimetry by Artes et al17 shows that the global visualfield indices mean deviation (MD) and pattern standarddeviation (PSD) of FDT and SAP correlate highly and thetest -retest variability of FDT2 is uniform over themeasurement range of the instrument.
Advantages of FDPShort test duration (4-5 min for full threshold)Very tolerant to defocus and blur (+ 6 dioptres sphere)18
Patients can wear spectacles with bifocalsNot affected by pupil size
Useful for glaucoma screeningTest - retest reliability is goodCan follow glaucoma progression with MD and PSDvaluesLess stringent dark room requirementsPortable and cheaperEasily learned by patient and examinerFeasible in children19
DisadvantagesMay miss focal defectsCentral 20 degree field may miss nasal stepsLack of longitudinal dataDifficult to follow up early progression
Clinical studiesAlthough FDT has just become visible to the
ophthalmic community, it has been studied and developedover many years. Johnson and associates showed that asensitivity of 82% with a specificity of 95% for earlyglaucomas, 96% sensitivity and 99% specificity for
Fig. 8: Humphrey Matrix FDT 24-2 Printout Fig. 9: Humphrey Matrix FDT 24-2, serial field analysis for progression

385DOS Times - Vol. 11, No. 6 December, 2005
moderate glaucomas and 100% sensitivity and 100%specificity for advanced glaucoma.
Quigley HA3 evaluated predictive power of FDP andfound close agreement between clinical examination ofoptic disc, nerve fibre layer and FDP. He suggested thatFDP can be potentially useful in screening glaucomatousoptic nerve damage.
In addition, Neahring20 and associates showed thatFDT was capable of detecting field loss associated withneurophthalmic conditions such as anterior ischemic opticneuropathy, compressive optic neuropathies and pseudo-tumor cerebri. The sensitivity of FDT was 81.3%, with aspecificity of 76.2%. When compared with sensitivity andspecificity of Humphrey perimetry 87.5% and 81.0%,respectively, the difference was not statistically significant.
Sponsel et al4 proposed a clinical scoring algorithmfor FDP modelled after the Hodapp-Paris-Anderson criteriafor scoring Humphrey visual field defect. Their new scoringalgorithm is as follows: severe visual field loss, more than1 FDP sector at probability 0.5%; moderate visual field loss,not severe, with either 1 FDP sector at probability 0.5% ormore than 13 sectors at 1% to 5%; early visual field loss,not moderate, with more than 4 sectors at 1% to 5%.
Studies by Chauhan et al and Spry et al show thatFDT exhibits lower intra and inter test variability thanSAP and test-retest variability in glaucoma patients withFDT does not increase as much with defect severity as itdoes with conventional perimetry.7, 8
Boden et al21 evaluated relationship of SITA and full-threshold standard perimetry to frequency-doublingtechnology perimetry in glaucoma. They found FDT detectsabnormal fields in more eyes than SAP-FT. Correlations ofFDT to standard perimetry global indices were similarregardless of the threshold strategy used for standardperimetry. They concluded that visual field defects may bedetected more often by FDT and SAP-SITA in eyes withearly visual field loss.
Medeiros FA et al22 evaluated whether frequencydoubling technology (FDT) perimetry results predictglaucomatous visual field defects, as assessed by standardautomated perimetry (SAP), in a glaucoma suspectpopulation. The analysis of FDT examinations duringfollow-up revealed that in 59% of converters, the FDTabnormalities preceded SAP visual field loss by as muchas 4 years and the initial development of glaucomatousvisual field loss as measured by SAP occurred in regionsthat had previously demonstrated abnormalities on FDTtesting.
Landers et al23 investigated whether frequency-doubling perimetry (FDP) predicts future visual field losswith achromatic automated perimetry (AAP), just as itmay be predicted with short-wavelength automated
perimetry (SWAP) and found that both SWAP and FDPdetect field loss earlier than AAP.
To know the agreement in results between frequencydoubling technology (FDT) and the conventionalautomated static perimeter in eyes with normal tensionglaucoma (NTG) and high tension glaucoma (HTG), Kogureet al24 in their study found that the best agreement of theresults of FDT and HFA was observed in eyes with NTGusing threshold of HFA. The eyes with HTG showed loweragreement with more abnormal points in FDT results,which suggest enough sensitivity of FDT in eyes with NTG,and higher sensitivity of FDT in eyes with HTG.
Regarding potential use of FDT as a screening device,Allen et al25 compared the Frequency Doubling Technology(FDT) C20-1 screening algorithm and the Humphrey FieldAnalyser II (HFA) 24-2 SITA-FAST in a large eye screening.They found low false positive rate and a good positivepredictive value comparing the FDT screening algorithmto the HFA 24-2 SITA-FAST in their study.
ConclusionsFDT is a promising method for the purpose of screening,
diagnosing and monitoring glaucoma which is comparableto SAP with some extra advantages. It is easily learnt bypatient as well as by the examiner. It takes shortest durationamongst all perimetric tests. As it is tolerant to blur (+ 6dioptres sphere), patients can wear spectacles with bifocalsand it is also not affected by pupil size. Only furtherevaluation and research will be able to illustrate if it is anymore sensitive in identifying loss associated with glaucomaand other conditions or is simply another method for theevaluation of the visual field. However due to its ease ofuse, simplicity, speed, affordability and portability it is animportant instrument that is quite useful in the evaluationof the visual field in early glaucoma and as a screening testfor a large population.
References1. Johnson CA, Samuels SJ. Screening for glaucomatous visual filed
loss with the frequency-doubling perimetry. Invest Ophthalmol VisSci 1997; 38: 413-425
2. Yamada N, Chen PP, Mills RP, et al. Screening for glaucoma withfrequency-doubling technology and Damato campimetry. ArchOphthalmol. 1999 Nov; 117(11):1479-84.
3. Quigley HA. Identification of glaucoma-related visual fieldabnormality with the screening protocol of frequency doublingtechnology. Am J Ophthalmol 1998: 819-829.
4. Sponsel WE, Arango S, Trigo Y, Mensah J. Clinical classification ofglaucomatous visual field loss by frequency doubling perimetry. AmJ Ophthal 1998: 830-836.
5. Turpin A, McKendrick AM, Jhonson et al.Performance of efficienttest procedure for frequency-doubling technology perimetry in normaland glaucomatous eyes. Invest Ophthalmol Vis Sci 2002; 43: 709-715.
6. Wadood AC, Azuara-Blanco A, Aspinall P et al. Sensitivity andspecificity of frequency doubling perimetry, Tendency-orientedperimetry, and Humphrey Swidish Interactive Thresold Algorithm-fast perimetry in a glaucoma practice. Am J Ophthal 2002; 133: 327-332.

DOS Times - Vol. 11, No. 6December, 2005 386
7. Chauhan BC, Jhonson CA. Test-retest variability of frequency doublingperimetry and conventional perimetry in glaucoma patients andnormal subjects. Invest Ophthalmol Vis Sci 1999; 40: 648-656.
8. Spry PGD, Jhonson CA, McKendrick AM et al. variability componentsof standard automated perimetry and frequency -doubling technologyperimetry. Invest Ophthalmol Vis Sci 2001; 42: 1404-1410.
9. Casson R, James B, Rubinstein A et al. Clinical comparison offrequency doubling technology perimetry and Humphrey perimetry.Br. J Ophthalmol 2001;85:360-362.
10. Maddess T, Henry GH,. Performance of nonlinear visual units inocular hypertension and glaucoma. Clin Vis Sci 1992;7:371-83
11. Maddess T, Goldberg I, Dobinson J et al. Clinical trials of thefrequency doubled illusion as a indicator of glaucoma. InvestOphthalmol Vis Sci 1995; 38: 413-25.
12. Johnson CA,selective versus nonselective losses in glaucoma. JGlaucoma (suppl 1994;3:S32-S44).
13. Turpin A, McKendrick AM, Jhonson et al. Development of efficientthreshold technology perimetry using computer simulation. InvestOphthalmol Vis Sci 2002; 43: 322-331.
14. Cello KE, Nelson-Quigg JM, Johnson CA. Frequency doublingtechnology perimetry for detection of glaucomatous visual field loss.Am J Ophthalmol. 2000 Mar;129(3):314-22.
15. Johnson CA, Cioffi GA, Van Buskirk EM. Frequency DoublingPerimetry Using a 24-2 Stimulus Presentation Pattern. Optom Vis Sci1999;76:571-81.
16. Spry PGD, Hussin HM, Sparrow JM. Clinical evaluation of frequencydoubling technology perimetry using the Humphrey Matrix 24-2threshold strategy. Br. J Ophthalmol 2005; 89:1031-1035.
17. Artes PH, Hutchison DM, Nicolela MT et al. Threshold and variabilityproperties of Matrix frequency -doubling technology and standardautomated perimetry in glaucoma. Invest Ophthalmol Vis Sci 2005;
46: 2451-2457.18. Anderson AJ, Johnson CA. Frequency-doubling technology perimetry
and optical defocus. Invest Ophthalmol Vis Sci. 2003 Sep;44(9):4147-52.
19. Blumenthal EZ, Haddad A, Horani A, Anteby I. The reliability offrequency-doubling perimetry in young children. Ophthalmology. 2004Mar;111(3):435-9.
20. Wall M, Neahering RK, Woodward KR. Sensitivity and specificity offrequency doubling perimetry in neuro-ophthalmic disorders: acomparison with conventional automated perimetry. InvestOphthalmol Vis Sci. 2002 Apr;43(4):1277-83.
21. Boden C, Pascual J, Medeiros FA, et al. Relationship of SITA and full-threshold standard perimetry to frequency-doubling technologyperimetry in glaucoma. Invest Ophthalmol Vis Sci. 2005 Jul;46(7):2433-9.
22. Medeiros FA, Sample PA, Weinreb RN. Frequency doublingtechnology perimetry abnormalities as predictors of glaucomatousvisual field loss. Am J Ophthalmol. 2004 May;137(5):863-71.
23. Landers JA, Goldberg I, Graham SL. Detection of early visual fieldloss in glaucoma using frequency-doubling perimetry and short-wavelength automated perimetry. Arch Ophthalmol. 2003Dec;121(12):1705-10.
24. Kogure S, Toda Y, Crabb D, et al. Agreement between frequencydoubling perimetry and static perimetry in eyes with high tensionglaucoma and normal tension glaucoma. Br J Ophthalmol. 2003May;87(5):604-8.
25. Allen CS, Sponsel WE, Trigo Y, et al. Comparison of the frequencydoubling technology screening algorithm and the Humphrey 24-2SITA-FAST in a large eye screening. Clin Experiment Ophthalmol.2002 Feb;30(1):8-14.
387DOS Times - Vol. 11, No. 6 December, 2005
Herpes Simplex Virus (HSV) is endemic in virtuallyevery human society throughout the world, from urbanto remote native tribes. Humans are the only naturalreservoirs for HSV and HSV disease is a significant healthproblem1,2,3,4.
HSV can be detected by polymerase chain reaction(PCR) in the trigeminal ganglia of 18.2% of cadavers ofpeople up to 20 years of age, which increases to reachalmost 100% in cadavers of people at least 60 years of age5.Latency with HSV is prevalent, with at least 33% of theworld manifesting recurrent HSV infections6. The majorportals of entry are the mucous membranes and externalskin. Crowding, poor hygiene and age influence HSV-1prevalence.
Recurrences are typically with the same strain andmay be triggered by fever, hormonal changes, ultraviolentexposure, psychological stress, ocular trauma andtrigeminal nerve manipulation7. The excimer laser has beenshown to trigger reactivation of latent HSV-18.
PathogenesisThe clinical sequelae of HSV infection are largely a result
of recurrent disease and the immunologic response witheach episode. After peripheral entry into the host andprimary infection with viral replication within the endorgan, HSV travels in a retrograde fashion to variousganglia, most commonly, the trigeminal ganglion, andpossibly the brain stem9,10,11. Immune defense mechanismsare both beneficial and harmful.
Clinical Manifestations1) Congenital and Neonatal Ocular Herpes
This is rare. It is usually acquired from genital herpesin the mother, during parturition12. Ocular manifestationsinclude skin lesions, conjunctivitis, epithelial and stromalkeratitis and cataracts.
Herpes Simplex KeratitisUmang Mathur
Cornea ServiceDr. Shroff's Charity Eye HospitalDaryaganj, New Delhi
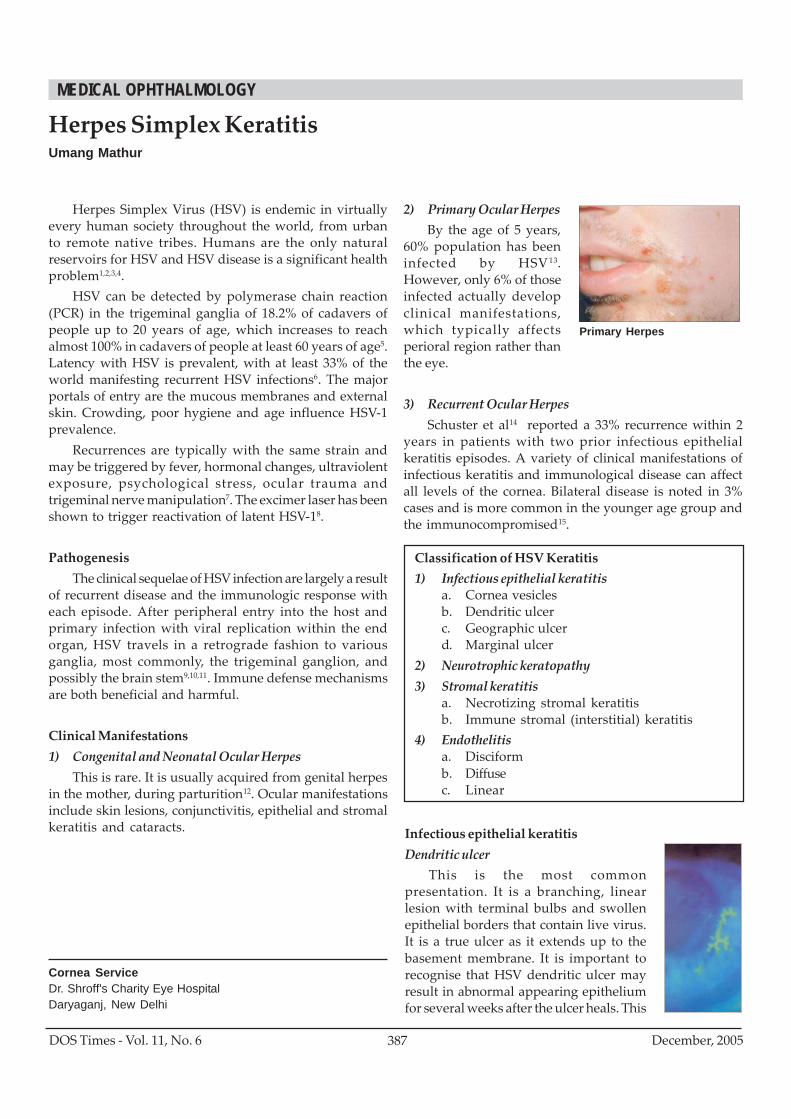
2) Primary Ocular HerpesBy the age of 5 years,
60% population has beeninfected by HSV13.However, only 6% of thoseinfected actually developclinical manifestations,which typically affectsperioral region rather thanthe eye.
3) Recurrent Ocular HerpesSchuster et al14 reported a 33% recurrence within 2
years in patients with two prior infectious epithelialkeratitis episodes. A variety of clinical manifestations ofinfectious keratitis and immunological disease can affectall levels of the cornea. Bilateral disease is noted in 3%cases and is more common in the younger age group andthe immunocompromised15.
Primary Herpes
Classification of HSV Keratitis1) Infectious epithelial keratitis
a. Cornea vesiclesb. Dendritic ulcerc. Geographic ulcerd. Marginal ulcer
2) Neurotrophic keratopathy3) Stromal keratitis
a. Necrotizing stromal keratitisb. Immune stromal (interstitial) keratitis
4) Endothelitisa. Disciformb. Diffusec. Linear
Infectious epithelial keratitisDendritic ulcer
This is the most commonpresentation. It is a branching, linearlesion with terminal bulbs and swollenepithelial borders that contain live virus.It is a true ulcer as it extends up to thebasement membrane. It is important torecognise that HSV dendritic ulcer mayresult in abnormal appearing epitheliumfor several weeks after the ulcer heals. This
MEDICAL OPHTHALMOLOGY
DOS Times - Vol. 11, No. 6December, 2005 388
epitheliopathy is dendritic in shape but is not ulceratedand does not require treatment.
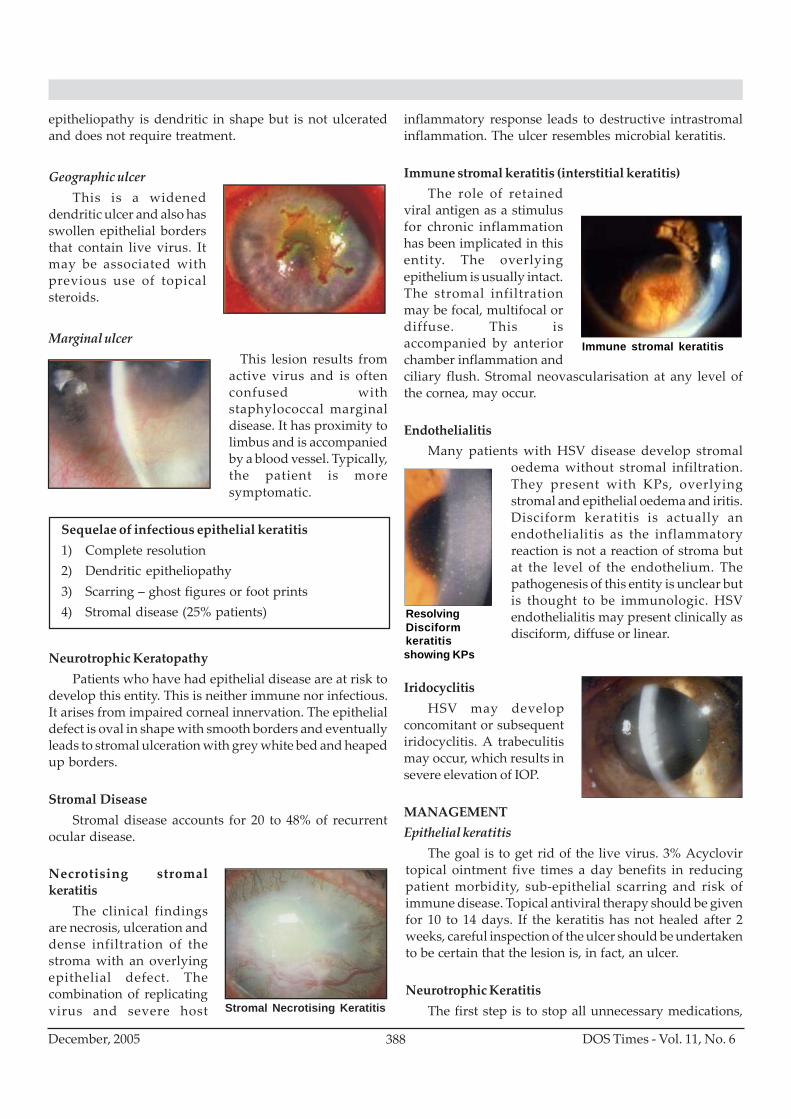
Geographic ulcerThis is a widened
dendritic ulcer and also hasswollen epithelial bordersthat contain live virus. Itmay be associated withprevious use of topicalsteroids.
Marginal ulcerThis lesion results from
active virus and is oftenconfused withstaphylococcal marginaldisease. It has proximity tolimbus and is accompaniedby a blood vessel. Typically,the patient is moresymptomatic.
Neurotrophic KeratopathyPatients who have had epithelial disease are at risk to
develop this entity. This is neither immune nor infectious.It arises from impaired corneal innervation. The epithelialdefect is oval in shape with smooth borders and eventuallyleads to stromal ulceration with grey white bed and heapedup borders.
Stromal DiseaseStromal disease accounts for 20 to 48% of recurrent
ocular disease.
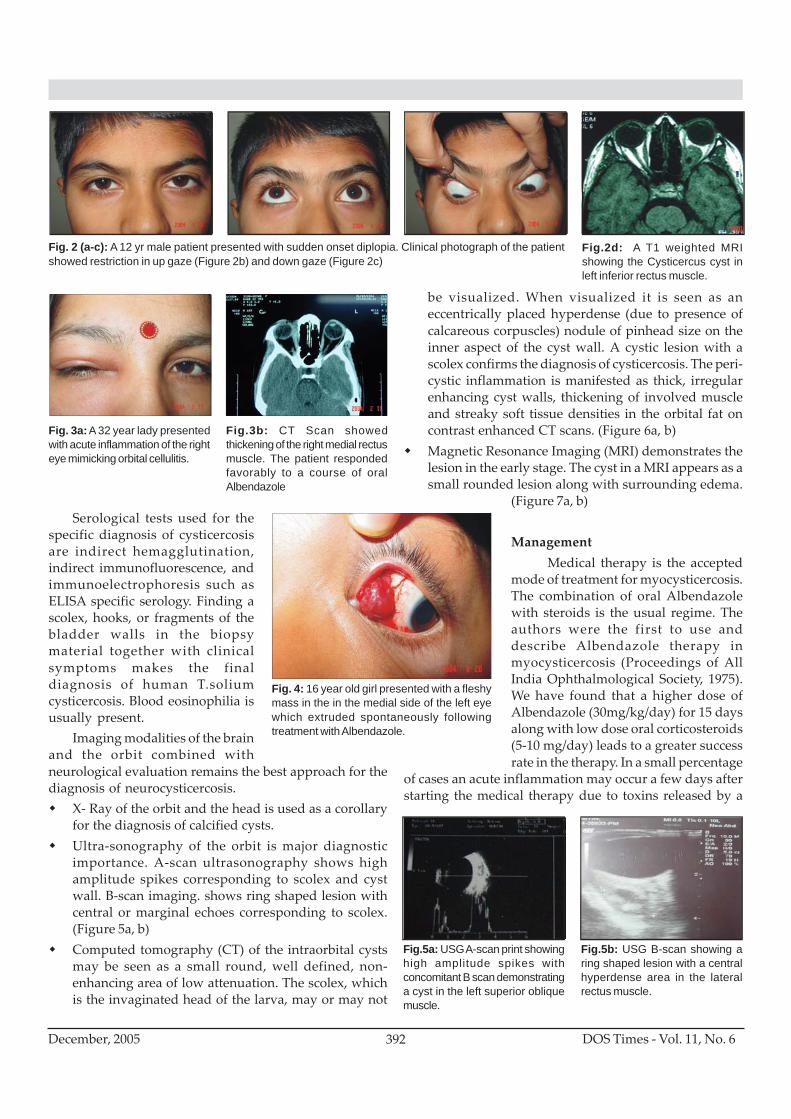
Necrotising stromalkeratitis
The clinical findingsare necrosis, ulceration anddense infiltration of thestroma with an overlyingepithelial defect. Thecombination of replicatingvirus and severe host
inflammatory response leads to destructive intrastromalinflammation. The ulcer resembles microbial keratitis.
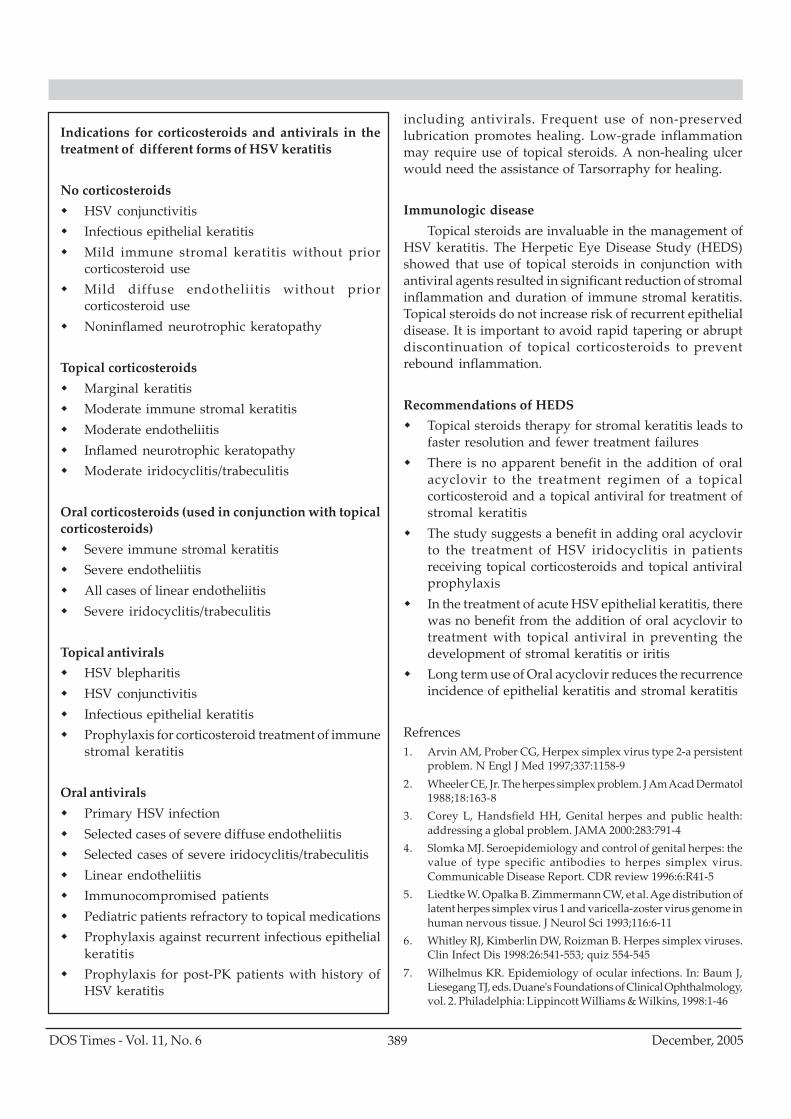
Immune stromal keratitis (interstitial keratitis)The role of retained
viral antigen as a stimulusfor chronic inflammationhas been implicated in thisentity. The overlyingepithelium is usually intact.The stromal infiltrationmay be focal, multifocal ordiffuse. This isaccompanied by anteriorchamber inflammation andciliary flush. Stromal neovascularisation at any level ofthe cornea, may occur.
EndothelialitisMany patients with HSV disease develop stromal
oedema without stromal infiltration.They present with KPs, overlyingstromal and epithelial oedema and iritis.Disciform keratitis is actually anendothelialitis as the inflammatoryreaction is not a reaction of stroma butat the level of the endothelium. Thepathogenesis of this entity is unclear butis thought to be immunologic. HSVendothelialitis may present clinically asdisciform, diffuse or linear.
IridocyclitisHSV may develop
concomitant or subsequentiridocyclitis. A trabeculitismay occur, which results insevere elevation of IOP.
MANAGEMENTEpithelial keratitis
The goal is to get rid of the live virus. 3% Acyclovirtopical ointment five times a day benefits in reducingpatient morbidity, sub-epithelial scarring and risk ofimmune disease. Topical antiviral therapy should be givenfor 10 to 14 days. If the keratitis has not healed after 2weeks, careful inspection of the ulcer should be undertakento be certain that the lesion is, in fact, an ulcer.
Neurotrophic KeratitisThe first step is to stop all unnecessary medications,
Sequelae of infectious epithelial keratitis1) Complete resolution2) Dendritic epitheliopathy3) Scarring – ghost figures or foot prints4) Stromal disease (25% patients)
Stromal Necrotising Keratitis
Immune stromal keratitis
ResolvingDisciformkeratitisshowing KPs
389DOS Times - Vol. 11, No. 6 December, 2005
Indications for corticosteroids and antivirals in thetreatment of different forms of HSV keratitis
No corticosteroidsHSV conjunctivitisInfectious epithelial keratitisMild immune stromal keratitis without priorcorticosteroid useMild diffuse endotheliitis without priorcorticosteroid useNoninflamed neurotrophic keratopathy
Topical corticosteroidsMarginal keratitisModerate immune stromal keratitisModerate endotheliitisInflamed neurotrophic keratopathyModerate iridocyclitis/trabeculitis
Oral corticosteroids (used in conjunction with topicalcorticosteroids)
Severe immune stromal keratitisSevere endotheliitisAll cases of linear endotheliitisSevere iridocyclitis/trabeculitis
Topical antiviralsHSV blepharitisHSV conjunctivitisInfectious epithelial keratitisProphylaxis for corticosteroid treatment of immunestromal keratitis
Oral antiviralsPrimary HSV infectionSelected cases of severe diffuse endotheliitisSelected cases of severe iridocyclitis/trabeculitisLinear endotheliitisImmunocompromised patientsPediatric patients refractory to topical medicationsProphylaxis against recurrent infectious epithelialkeratitisProphylaxis for post-PK patients with history ofHSV keratitis
including antivirals. Frequent use of non-preservedlubrication promotes healing. Low-grade inflammationmay require use of topical steroids. A non-healing ulcerwould need the assistance of Tarsorraphy for healing.
Immunologic diseaseTopical steroids are invaluable in the management of
HSV keratitis. The Herpetic Eye Disease Study (HEDS)showed that use of topical steroids in conjunction withantiviral agents resulted in significant reduction of stromalinflammation and duration of immune stromal keratitis.Topical steroids do not increase risk of recurrent epithelialdisease. It is important to avoid rapid tapering or abruptdiscontinuation of topical corticosteroids to preventrebound inflammation.
Recommendations of HEDSTopical steroids therapy for stromal keratitis leads tofaster resolution and fewer treatment failuresThere is no apparent benefit in the addition of oralacyclovir to the treatment regimen of a topicalcorticosteroid and a topical antiviral for treatment ofstromal keratitisThe study suggests a benefit in adding oral acyclovirto the treatment of HSV iridocyclitis in patientsreceiving topical corticosteroids and topical antiviralprophylaxisIn the treatment of acute HSV epithelial keratitis, therewas no benefit from the addition of oral acyclovir totreatment with topical antiviral in preventing thedevelopment of stromal keratitis or iritisLong term use of Oral acyclovir reduces the recurrenceincidence of epithelial keratitis and stromal keratitis
Refrences1. Arvin AM, Prober CG, Herpex simplex virus type 2-a persistent
problem. N Engl J Med 1997;337:1158-92. Wheeler CE, Jr. The herpes simplex problem. J Am Acad Dermatol
1988;18:163-83. Corey L, Handsfield HH, Genital herpes and public health:
addressing a global problem. JAMA 2000:283:791-44. Slomka MJ. Seroepidemiology and control of genital herpes: the
value of type specific antibodies to herpes simplex virus.Communicable Disease Report. CDR review 1996:6:R41-5
5. Liedtke W. Opalka B. Zimmermann CW, et al. Age distribution oflatent herpes simplex virus 1 and varicella-zoster virus genome inhuman nervous tissue. J Neurol Sci 1993;116:6-11
6. Whitley RJ, Kimberlin DW, Roizman B. Herpes simplex viruses.Clin Infect Dis 1998:26:541-553; quiz 554-545
7. Wilhelmus KR. Epidemiology of ocular infections. In: Baum J,Liesegang TJ, eds. Duane's Foundations of Clinical Ophthalmology,vol. 2. Philadelphia: Lippincott Williams & Wilkins, 1998:1-46

DOS Times - Vol. 11, No. 6December, 2005 390
8. Dhaliwal DK, Barnhorst DA Jr, Romanowski E, et al. Efficientreactivation of latent herpes simplex virus type I infection byexcimer laser keratectomy in the experimental rabbit ocular model.Am J ophthalmol 1998:125:488-92
9. Stevens JG, Nesburn AB, Cook ML: Latent herpes simplex virusfrom trigeminal ganglia or rabbits with recurrent eye infection,Nature 235:216, 1972
10. Stevens JG, Cook ML: Latent herpes simplex virus in spinal gangliaof mice, Science 173:843, 1971
11. Fraser N et al; Herpes simplex type 1 DNA in human brain tissue,Proc Natl Acad Sci USA 78:843, 1981
12. Nahmias A, Alford C Korones S: Infection of the newborn withherpesvirus hominis, Adv Pediatr 17:185, 1970
13. Goodman JL:Infections casused by herpes simplex viruses. InHoeprich PD, Jordan C, Ronald AR, editors: Infectious diseases,ed 5, Philadelphia, 1994, JB Lippincott
14. Shuster JJ, Kaufman HE, Nesburn AB: statistical analysis of the rateof recurrence of herpesvirus ocular epithelial disease, Am JOphthalmol 91:328-331, 1981
15. Wilhelmus KR, Falcon MG, Jones BR: Bilateral herpetic keratitis BrJ Ophthalmol 65:385-387, 1981

391DOS Times - Vol. 11, No. 6 December, 2005
Cysticercosis refers to human infection with the larvalform of the nematode, taenia solium due to the ingestion ofcontaminated food especially undercooked pork,contaminated water and vegetables. It is commonly seenin places with poor sanitation.
Life CycyleCysticercus cellulosae is the larval form of the pork
tapeworm, taenia solium. Human cysticercosis is acquiredby ingestion of tapeworm eggs shed in faeces. The infectionis usually acquired by consumption of poorly washedvegetables or fruits and may sometimes be due to auto-infection due to poor hygiene. The eggs mature and thelarvae penetrate the intestinal mucosa to enter the portalcirculation, from where they are carried to various targetorgans. The common systemic sites of involvement aresubcutaneous tissues, muscles, brain and eyes. The larvalform may enter the eye through the choroidal circulationand migrate into the subretinal space or enter the vitreousbody. Death of the larvae within the ocular tissues caninduce a severe inflammatory reaction, which may lead toblindness. Cysts embedded in the extraocular muscles maycause ocular movement disorders or proptosis.
Clinical FeaturesCysticercosis is most prevalent in India, Eastern
Europe, Central America, and Mexico. It commonly affectschildren and young adults. The cyst may lodge in any partof the body, central nervous system being the most commonsite. It may also lodge in the heart, skeletal muscles and inthe eye. In the eye it may be intraocular in location or maybe present in the orbit or the adnexa. Extraocular musclesare the commonest structure to be affected in the orbit.Depending on their size and location, orbital cysticercosismay be associated with chemosis, ocular pain, protrusionof the eye, periorbital swelling, drooping of eyelids, doublevision and restriction of ocular movements. Extraocularinvolvement may include involvement of the extraocularmuscles, lacrimal gland or optic nerve. The authors haveseen five different sets of presentations in over 150 cases
Orbital MyocysticercosisAshok K Grover, MD, MNAMS, FRCS,Shaloo Bageja, DNB, Zia Chaudhuri, MS, MNAMS. FRCS
Department of OphthalmologySir Ganga Ram Hospital,New Delhi
seen and treated by them.a) Proptosis (Fig 1a,b)b) Ocular motility restriction and diplopia (Figure
2a,b,c,d)c) Recurrent episodes of redness, swelling and pain that
may mimic orbital pseudotumor or even orbitalcellulites (Figure 3a,b)
d) Recurrent episodes of ptosis (Figure 8a,b)e) Subconjunctival cysts with or without abscess
formation (Figure 4)
DiagnosisThe diagnosis of myocysticercosis is based on clinical,
serologic, and radiological findings. The clinical findingsmay occasionally be non-specific and hence, non-diagnostic. The serology in myocysticercosis is rarelypositive in the experience of the authors. Thus, imagingstudies are the most helpful in establishing the diagnosisof cysticercosis.
Diagnosis of infection with adult T.solium is made bystool examination and finding the eggs of proglottids ofthe worm. One easy method for differentiating theinfection with Tania saginata from T.solium is the use ofhematoxylin-eosin (HE) staining of proglottids andobserving the number of uterine branches. The uterinebranches in T. solium infection is about 50 in number whilethat in T. saginata infection is about 150 in number. Thebranches are also more convoluted in a T.solium infectionthan in a T. saginata infection. Though stool examinationfor the adult worm may be performed in cases of suspectedmyocysticercosis infections, it is not essential that allpatients with myocysticercosis have the adult worm intheir intestines except in those cases, which are acquiredby auto-infection.
Fig.1b: A T1 weighted MRI showscyst in the right lateral rectusmuscle.
Fig. 1a: Clinical photograph of 8 yrold child who presented withproptosis of the right eye.
MEDICAL OPHTHALMOLOGY
DOS Times - Vol. 11, No. 6December, 2005 392
Serological tests used for thespecific diagnosis of cysticercosisare indirect hemagglutination,indirect immunofluorescence, andimmunoelectrophoresis such asELISA specific serology. Finding ascolex, hooks, or fragments of thebladder walls in the biopsymaterial together with clinicalsymptoms makes the finaldiagnosis of human T.soliumcysticercosis. Blood eosinophilia isusually present.
Imaging modalities of the brainand the orbit combined withneurological evaluation remains the best approach for thediagnosis of neurocysticercosis.
X- Ray of the orbit and the head is used as a corollaryfor the diagnosis of calcified cysts.Ultra-sonography of the orbit is major diagnosticimportance. A-scan ultrasonography shows highamplitude spikes corresponding to scolex and cystwall. B-scan imaging. shows ring shaped lesion withcentral or marginal echoes corresponding to scolex.(Figure 5a, b)Computed tomography (CT) of the intraorbital cystsmay be seen as a small round, well defined, non-enhancing area of low attenuation. The scolex, whichis the invaginated head of the larva, may or may not
Fig. 2 (a-c): A 12 yr male patient presented with sudden onset diplopia. Clinical photograph of the patientshowed restriction in up gaze (Figure 2b) and down gaze (Figure 2c)
Fig.2d: A T1 weighted MRIshowing the Cysticercus cyst inleft inferior rectus muscle.
Fig. 3a: A 32 year lady presentedwith acute inflammation of the righteye mimicking orbital cellulitis.
Fig.3b: CT Scan showedthickening of the right medial rectusmuscle. The patient respondedfavorably to a course of oralAlbendazole
be visualized. When visualized it is seen as aneccentrically placed hyperdense (due to presence ofcalcareous corpuscles) nodule of pinhead size on theinner aspect of the cyst wall. A cystic lesion with ascolex confirms the diagnosis of cysticercosis. The peri-cystic inflammation is manifested as thick, irregularenhancing cyst walls, thickening of involved muscleand streaky soft tissue densities in the orbital fat oncontrast enhanced CT scans. (Figure 6a, b)Magnetic Resonance Imaging (MRI) demonstrates thelesion in the early stage. The cyst in a MRI appears as asmall rounded lesion along with surrounding edema.
(Figure 7a, b)
ManagementMedical therapy is the accepted
mode of treatment for myocysticercosis.The combination of oral Albendazolewith steroids is the usual regime. Theauthors were the first to use anddescribe Albendazole therapy inmyocysticercosis (Proceedings of AllIndia Ophthalmological Society, 1975).We have found that a higher dose ofAlbendazole (30mg/kg/day) for 15 daysalong with low dose oral corticosteroids(5-10 mg/day) leads to a greater successrate in the therapy. In a small percentage
of cases an acute inflammation may occur a few days afterstarting the medical therapy due to toxins released by a
Fig. 4: 16 year old girl presented with a fleshymass in the in the medial side of the left eyewhich extruded spontaneously followingtreatment with Albendazole.
Fig.5a: USG A-scan print showinghigh amplitude spikes withconcomitant B scan demonstratinga cyst in the left superior obliquemuscle.
Fig.5b: USG B-scan showing aring shaped lesion with a centralhyperdense area in the lateralrectus muscle.
393DOS Times - Vol. 11, No. 6 December, 2005
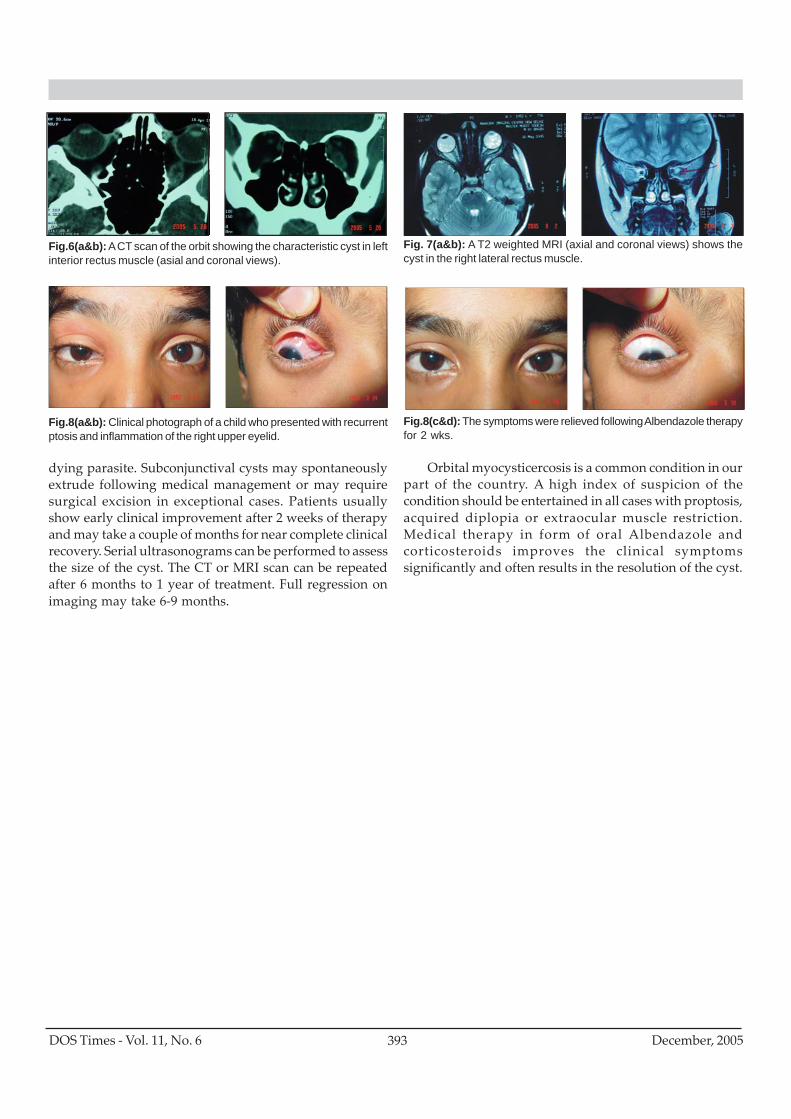
Fig.8(a&b): Clinical photograph of a child who presented with recurrentptosis and inflammation of the right upper eyelid.
Fig.8(c&d): The symptoms were relieved following Albendazole therapyfor 2 wks.
dying parasite. Subconjunctival cysts may spontaneouslyextrude following medical management or may requiresurgical excision in exceptional cases. Patients usuallyshow early clinical improvement after 2 weeks of therapyand may take a couple of months for near complete clinicalrecovery. Serial ultrasonograms can be performed to assessthe size of the cyst. The CT or MRI scan can be repeatedafter 6 months to 1 year of treatment. Full regression onimaging may take 6-9 months.
Orbital myocysticercosis is a common condition in ourpart of the country. A high index of suspicion of thecondition should be entertained in all cases with proptosis,acquired diplopia or extraocular muscle restriction.Medical therapy in form of oral Albendazole andcorticosteroids improves the clinical symptomssignificantly and often results in the resolution of the cyst.
Fig. 7(a&b): A T2 weighted MRI (axial and coronal views) shows thecyst in the right lateral rectus muscle.
Fig.6(a&b): A CT scan of the orbit showing the characteristic cyst in leftinterior rectus muscle (asial and coronal views).
DOS Times - Vol. 11, No. 6December, 2005 394
Transient visual loss refers to temporary visualimpairment of variable duration lasting from seconds tohours. Typically, episodes have an abrupt onset,progressing over a few seconds to involve whole or part ofone or both visual fields. Within the affected area visionmay be dimmed or completely lost. Sight usually returnswithin seconds or minutes but, exceptionally, attacks maylast several hours. We will be discussing the TransientVisual Loss here.
Causes of Transient Visual LossVascularThrombo embolic:
Atheromatous disease of internal carotid artery orophthalmic artery or vertebral artery.Carotid occlusions,Slow flow retinopathyVasculitis:Giant cell arteritis,Pararteritis nodosa,Systemic lupus erythematous,
NeurologicalPapilloedema,Migraine: ocular, classic.EpilepsyUhthoff's phenomenon
OcularAngle closure glaucomaHyphaemaOptic disc anomalies: drusen, coloboma,Retrobulbar tumours,
HaematologicalHyperviscosity-polycythemia, thrombocythaemia,multiple myelomaCoagulopathies, anaemia.
Transient Visual LossJaswant Arneja, M.S., Alka Pandey, M.S.
Initial DiagnosisThromboembolic disease is the most common cause of
transient visual loss and, if an alternative diagnosis cannotbe made, the patient should undergo detailedcardiovascular investigations. At presentation there arefour important causes:
Giant cell arteritis.Intermittent angle closure glaucoma.Slow flow retinopathy.PapilloedemaKey features of common or important causes of transient visual
loss:1. Giant cell arteritis: Age > 50, systemic symptoms, raised
ESR, disc swelling.2. Intermediate angle closure glaucoma: Shallow angles, aching
pain3. Slow flow retinopathy: Peripheral haemorrhages, narrow
arterioles, central retinal arteriole pulsation withminimal pressure on the globe.
4. Papilloedema: Swollen disc5. Thromboembolic disease: Normal fundus, peripheral
embolus.
1. HistoryA complete ocular and systemic history is essential in
the assessment of transient visual loss because ocularexamination is often normal. The following are of particularimportance.
Is the visual loss in one or both eyes?Observant patients will have noticed this but, more
often, patients may not be sufficiently aware to be certain.Beware of the error of confusing homonymous hemianopiawith uniocular loss. Retinal embolus from carotid arterydisease typically produces monocular transient visual loss(amaurosis fugax). The loss is often described as a shutterbeing lowered or raised.
Duration of each attackThis may vary but typical patterns are-Embolic disease- seconds or minutes.Migraine- minutes.Papilloedema- seconds and related to postureGlaucoma- minutes to hours.
Nayantara Eye HospitalSubhadra Colony,Delhi
MEDICAL OPHTHALMOLOGY
395DOS Times - Vol. 11, No. 6 December, 2005
Often the causes are variable but usually last over 30seconds.Precipitating factorsPosture -standing up for papilloedema and systemichypotension.Turning the head for carotid artery diseaseEye movements in some tumours of the orbitEating chocolate as trigger factor for migraineHaloes around lights in congestive glaucoma.Prolonged dim light as in cinema hall.Associated symptomsCurrent or previous symptoms include:Other neurological deficiets in thrombolic diseaseHeadache in papilloedema and giant cell arteritisVisual aura and other symptoms in migraine.Haloes around light in congestive glaucomaRisk factors for cardiovascular disease- smoking, raisedblood pressure, diabetes mellitus and hyperlipidaemia
2. ExaminationFull ocular and cardiovascular examinations are
required.Visual function assessment: This should include- visualacuity, visual field, pupil reactions. Most cases willhave negative findings but a number of cases oftransient visual loss may leave permanent visual lossof which the patient is unaware, e.g. papilloedemacauses enlarged blind spots.Anterior segment: Depth of anterior chamber for narrowangle glaucoma use a gonioscope, if in doubt.Measure intra ocular pressure (IOP)Look for causes of transient obstruction of the visual
axis, for example, soft lens matter occluding pupil aftercataract surgery.
Sources of spontaneous hypaema-e.g. Iris clip lens orAcintra ocular lens.
Posterior segmentRetinal vessels -for patterning and signs of old
embolismDisc- for swelling, atrophy or drusen.Retina- for peripheral haemorrhages: midperipheral
haemorrhages in slow flow retinopathy, or scatteredpunctate haemorrhage in pre retinal vein occlusion
Retinal tear with shifting fluid in posterior pole.
Causes of transient bilateral loss ofvision1. Migraine2. Cerebral hypoperfusion
a. Thromboembolismb. Systemic hypotensionc. Hyper viscosityd. Vascular compression
3. Epilepsy4. Papilloedema
Causes of transient monocular loss of vision1. Embolic cerebrovascular disease2. Migraine (vasospasm)3. Hypoperfusion (hypotension, Hyperviscosity, hypercoagulability)4. Ocular (intermittent angle closure glaucoma, hyphema, optic disc
oedema, partial retinal vein occlusion.5. Vasculities (e.g. giant cell arteritis)6. Uhthoff's phenomenon- Temporary decrease in acquity consquent to
exercise or other causes of increased body temperature in patients withdemyelinating optic neuropathy (multiple sclerosis).
7. Others - Psychogenic, Idiopathic
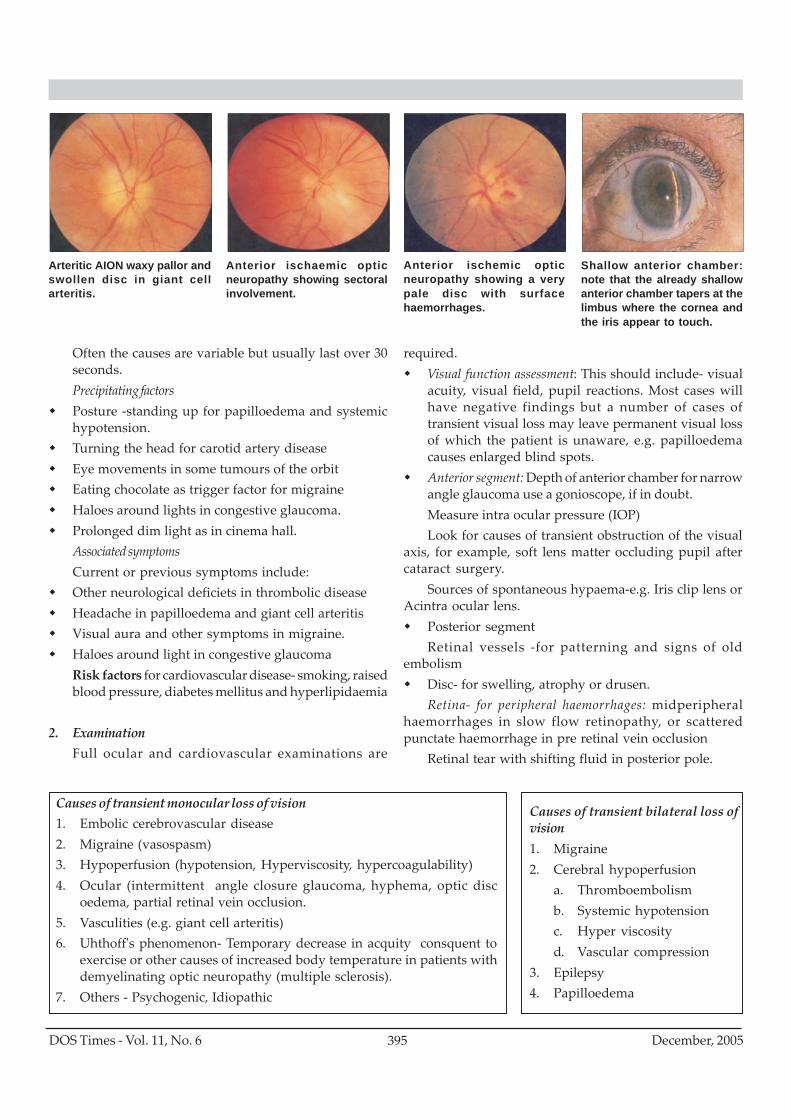
Arteritic AION waxy pallor andswollen disc in giant cellarteritis.
Anterior ischaemic opticneuropathy showing sectoralinvolvement.
Anterior ischemic opticneuropathy showing a verypale disc with surfacehaemorrhages.
Shallow anterior chamber:note that the already shallowanterior chamber tapers at thelimbus where the cornea andthe iris appear to touch.
DOS Times - Vol. 11, No. 6December, 2005 396
Cardiovascular system: Pulse and rhythm, BP, carotidauscultation, cardiac auscultation, peripheral pulse whenindicated.
3. InvestigationsThe ESR should be measured for all patients. A high ESR
in patients over the age of 50 strongly suggests giant cellarteritis, whereas in younger patients it may be associatedwith other vasculitic causes of transient visual loss.
Doppler studies are needed for carotid stenosis.Angiogrphy is carried out only if carotid surgery is beingconsidered.
4. Management of Specific ConditionsA) Giant Cell Arteritis
General features: malaise, weight loss, fever. Headacheand scalp tenderness- typically painful to put head onpillow. Pain on chewing in severe cases and jawclaudication. Aches and pains from polymyalgia.
Ocular features: non pulsatile temporal late stagearteritis- Ischemic optic neuropathy, central retinal arteryocclusion on moving eyes, diplopia from nerve palsy,
Diagnosis: ESR typically more than 80, Temporal arterybiopsy may show focal arteritis with giant cells.
Management: Immediate intravcenous injection ofhydro cortisone 200 mg, oral steroids to be started at thesame time, admission of patient for biopsy and control ofarteritis.
B) Anterior Ischaemic Optic Neuropathy.Anterior ischemic neuropathy (AION) is caused byocclusion of the posterior ciliary arteries supplyingthe preliminary optic nerve.Signs and symptoms- There is sudden loss of vision
and swelling of optic disc. Two forms of AION arerecognized: non arteritic and arteritic AION
Non arteritic AION: Peak incidence is in the 50-60 yearage range but can occur in much younger patients.Field loss is usually altitudinal or arcuate, but may betotal. Central vison is usually involved with resultantloss of acuity, but 40 % of affected eyes retain an acuityof 6/18 or better. Disc swelling may be subtle andlimited to the sector corresponding to the sectorinvolved to the visual field defect. Flame shaped dischaemorrhages are often seen.
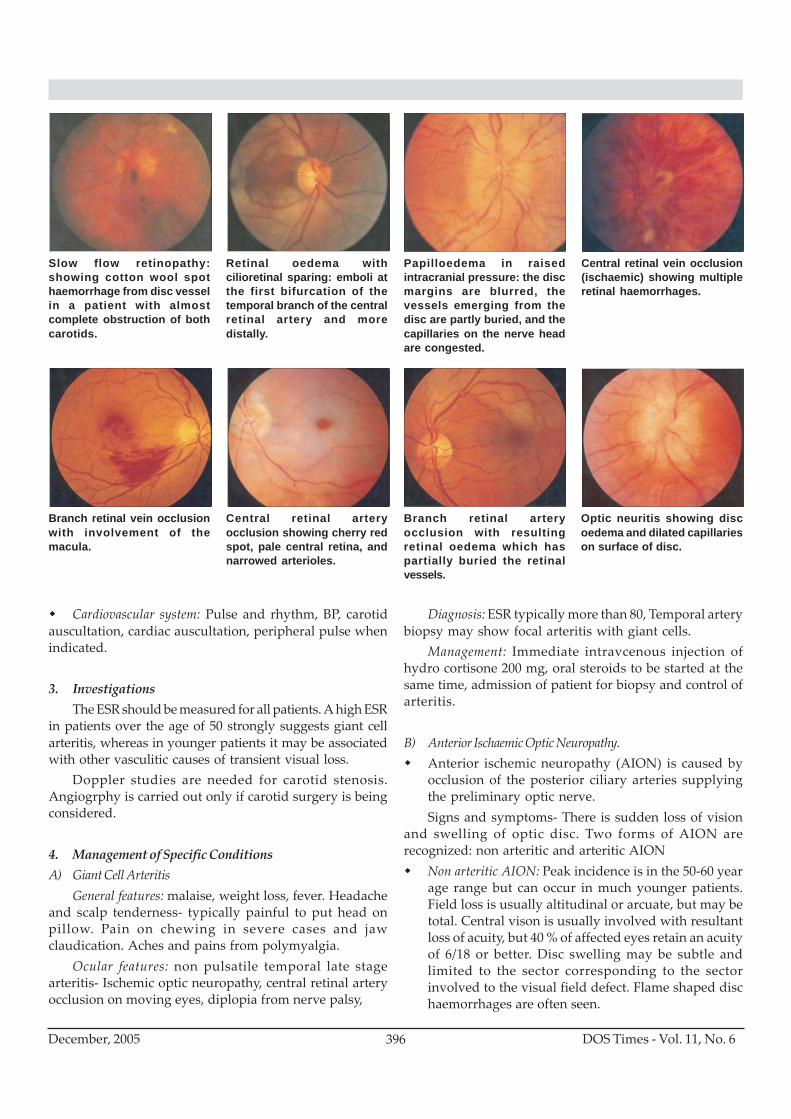
Slow flow retinopathy:showing cotton wool spothaemorrhage from disc vesselin a patient with almostcomplete obstruction of bothcarotids.
Retinal oedema withcilioretinal sparing: emboli atthe first bifurcation of thetemporal branch of the centralretinal artery and moredistally.
Papilloedema in raisedintracranial pressure: the discmargins are blurred, thevessels emerging from thedisc are partly buried, and thecapillaries on the nerve headare congested.
Central retinal vein occlusion(ischaemic) showing multipleretinal haemorrhages.
Branch retinal vein occlusionwith involvement of themacula.
Central retinal arteryocclusion showing cherry redspot, pale central retina, andnarrowed arterioles.
Branch retinal arteryocclusion with resultingretinal oedema which haspartially buried the retinalvessels.
Optic neuritis showing discoedema and dilated capillarieson surface of disc.

397DOS Times - Vol. 11, No. 6 December, 2005
Arteritic AION This is most common beyond the ageof 70 and very rare below 50. Patients usually presentwith profound loss of vision in one or both eyes, butpartial field loss may occur. They may haveexperienced visual loss in the preceding few days. Thedisc is swollen and milky white in colour.Non arteritic AION: local arteriosclerosis ( embolus is
an extremely rare cause).Arteritic AION: giant cell arteritis
Immediate screening:Screening for Giant Cell Arteritis (GCA): Systemic features
include headache, pain and tenderness of proximal musclegroups (polymyalgia rheumatica), jaw claudication, fever,weight loss, scalp tenderness, and pulseless temporalartery. On immediate ESR measurement, most patients willhave an elevated ESR, typically over 80 mm/hr. The agematched upper limit of normal is about half the patient'sage in millimeters per hour.
Treatment This should be as though it were giant cellarteritis, the systemic features of which may be absent.Two percent biopsy proven giant cell arteritis have anormal ESR. Giving immediate treatment to a patient withgiant cell arteritis may be sight saving, and a short courseof steroids (until giant cell arteritis is definitely excluded)is unlikely to harm a patient with non arteritis AION.Therefore, patients should be given hydrocortisone 200mg intravenously, pending further investigations.
C) Intermittent Angle Closure Glaucoma Symptoms oftransient visual loss caused by intermittent angle closureglaucoma are usually accompanied by eye ache andheadache, haloes around lights and intermittent blurringof vision. Signs include shallow anterior chamber, positivevan Herrick sign where the peripheral cornea is in contactwith the iris. Raised intraocular pressure is not alwayspresent except during an attack.Narrow or closed angleon gonioscopy will confirm the diagnosis. Management isby medical therapy to lower pressures by Diamox,pilocarpine or by beta blocker eye drops.
D) Slow Flow RetinopathySlow flow retinopathy is caused by severe stenosis of
the carotid circulation. It may be monocular or binocular.Symptoms and signs are:Intermittent blurring or loss of vison; residual blurredvision may occur because of retinal ischemiaPhotopsiaMid peripheral retinal haemorrhageCotton wool spotsMarked arterial attenuation and mild venous dilatation
Occasionally new vessels on disc and vitreoushaemorrhage.Low perfusion pressure in artery results in closure ofartery with minimally applied pressure.Management: This is similar to that for transient visual
loss by thromboembolic disease (see below)
E) Thrombo Embolic DiseaseTransient thrombosis or embolism associated with
atheromatous disease of the internal carotid or ophthalmicarteries accounts for most cases of monocular transientvisual loss. Such cases were previously said to have "amaurosis fugax" or " fleeting blindness". Less commonly,may be caused by emboli originating from the heart orproximal vessels. The risk of subsequent stroke, at 3-5%per annum, is five times greater than in an age matchedpopulation and 30% of patients will have a myocardialinfarction within five years.
Concurrent neurological symptoms are rare but theremay be a history of previous transient or permanentneurological deficits within the distribution of the carotidarteries. Retinal emboli, when present are diagniostic.
Symptoms and signs:There is transient loss of vision which usually lasts for
second to minutes-impairement lasts a little longer, upto20 min. Loss of vision begins as if a curtain was drawn upor down the field and recovery has the reverse effect. Anold emboli in peripheral arterial tree may be visble or theremay be no signs if the cause is platelet emboli which passthrough the circulation.
In central retinal artery occlusion (CRAO), Visualacuity is usually down to counting fingers or less, but somecases (11%) may retain some central vision because of apatent cilioretinal artery.Management:
The investigation and tratment of transient visual lossresulting from a thromboembolism are ideallycoordinated by someone (possibly a neurologist,cardiologist,ophthalmologist, and a vascular surgeon) whohas an interest in this field. The aims of treatment are toreduce the risks of subsequent stroke and myocardialinfarction.
Carotid duplex ultrasonography is the initial screeninginvestigation , which may be followed by angiography.
Management- Intravenous acetazolamide 500mg.Ocular massage for 15 mintus by pressing on the eye
for 10 second and then suddenly releasing.Anterior chamber paracentesis under topical
anaesthesia using 26 G needle.Aspirin 300 mg per day has been shown to reduce the

DOS Times - Vol. 11, No. 6December, 2005 398
risk of nonfatal stroke by 30 % after transient visual losscaused by thromboembolism. There is no definite evidencethat anticoagulation with either warfarin or heparin is ofbenefit. All patients require a cardiac assessment lookingfor ischemia and sources of emboli.
Risk factors- Cardivascular risk factors such assmoking, hypertension, diabetes, and hyperlipidemiashould be reviewed.
Investigations advised:- Full blood count, urgent ESR,plasma glucose and lipids, and ECG. Carotid duplexultrasonography and echocardiography can later beadvised. Patients should be advised to stop smoking andstart on aspirin (unless they have a history of allergy orpeptic ulceration).
F) PapilloedemaTransient visdual loss associated with papilloedema
characteristically lasts for a few seconds and usually affectsone eye at a time. Recurrences and repeated episodes arethe rule. Visual loss may be precipitated by alteration ofposture and can often be reproduced by gentle pressure onglobe. Other features of raised intracranial pressure maybe elicited, including headache, which is typically worsein the morning and exacerbated by coughing or changes inposture, nausea or vomiting, and horizontal diplopiacaused by VI cranial nerve palsy.
Signs: Swollen and hyperaemic disc, peripapillary flameshaped haemorrhages and engorged retinal veins
Management: Urgent investigation is needed to establishthe underlying cause.Blood pressure must be measured to
Causes of unilateral profound loss of vision - non-progressive1. BRAO or CRAO2. AION-arteritic or non arteritic3. BRVO or CRVO4. Traumatic optic neuropathy5. CSR6. Retinal detachment,7. Vitreous haemorrhage8. Functional (psychogenic) vision lossCauses of bilateral profound loss of vision non-progressive1. Occipital lobe infarction2. Pituitary apoplexy3. Functional4. Leber's hereditary optic neuropathy5. Head trauma
exclude malignant hypertension, CT scan is advised andthe patient referred for a neurological assessment.Treatment is that of the cause, although if cause ispseudotumour cerebri, then the treatment includes -acetazolamide and/ or frusemide, repeated lumberpunctures, fenestration of optic nerve or peritoneal shunts.
Other causes of disc swelling:Papilliitis or optic neuritis -visual acuity is usually
decreased.Malignant hypertension: BP raised.Central retinal vein occlusion (CRVO): rarely bilateral and
peripheral retinal haemorrhagesInfiltration of optic nerve head: granuloma, for example
sarcoid and neoplasia, for example leukaemia.Uveitis: signs of inflammation. It commonly affects only
one eye. There is no congestion of vessels.
G) Other Causes of Transient Visual LossTransient visual loss is an unusual presentation for aretrobulbar tumour but it should be considered ifepisodes are precipitated by eye movement.Patients with spontaneous hyphaema should bethoroughly screened.Optic disc drusen and coloboma may be coincidentalfindings.Vasculitis other than giant cell arteritis mayoccasionally cause transient visual loss. Arthritis, skinrashes, and Raynauds phenomenon, the antinuclearantibody titre and rheumatoid factor should bechecked..Coagulopathies are an uncommon cause of transientvisual loss, but should be considered in young patientsand those with unknown malignancy. Screening forlupus anticoagulant and coagulation factorabnormalities may be indicated.Hyperviscosity syndromes and anaemia will bedetected by a full blood count and ESR.Migraine: there are no distinguishing features ofmonocular transient visual loss resulting from ocularmigraine. In particular headache does not alwaysoccur with this type of migraine and occasionallyaccompanies transient visual loss caused bythromoembolic disease. The diagnosis of ocularmigraine must therefore be one of exclusion. When thetransient visual loss is binocular and is associated withheadache, migrating scintillations, and a familyhistory of migraine, the diagnosis of classic migraineis almost certain. If there are any atypical features,other causes of occipital ischaemia should beconsidered.Uhthoff's phenomenon-temporary decrease in acquity

399DOS Times - Vol. 11, No. 6 December, 2005
consequent to exercise or other causes of increased bodytempreture with demyelinating optic neuropathy(multiple sclerosis)EpilepsyFunctional or psychogenic
Profound Loss of VisionCauses of profound visual loss (which may not recover
fully) should also be screened if the patient presents in the
early stages. Sudden onset of profound visual loss indicatesa vascular aetiology (anterior ischemic optic neuropathy,retinal vein occlusion- BRVO, CRVO, or a Vitreoushaemorrhage- Diabetic or due to Eales dis.). Graduallyenlarging field defect over hours to a few days indicates aretinal detachment. Progressive dimming of vision overhours to a few days indicates optic neuritis and opticneuropathy. These causes are not discussed here, but shouldalways be kept in mind.

DOS Times - Vol. 11, No. 6December, 2005 400
IntroductionAllogeneic rejection is defined as a specific cell-
mediated immune reaction directed against the cornealallograft. It is directed against Major HistocompatibilityComplex (MHC) allo-antigens present on donor cells.
There are 3 main cell types transplanted at the time ofthe corneal graft: epithelial cells, stromal keratocytes andendothelial cells. An immune reaction directed againstepithelial cells is termed epithelial cell rejection and maymanifest as an epithelial rejection (Krachmer) line2.Epithelial cells are normally lost from the graft over amatter of months even in the absence of rejection, this doesnot affect graft clarity.
Stromal keratocyte rejection is uncommonly observedand may manifest as predominantly anterior stromalnummular inflammatory lesions (Krachmer dots)restricted to the graft. Transplanted keratocytes arenormally lost over time from the graft, being replaced byinvading host keratocytes. This usually does not affect graftclarity unless there is an underlying keratocyte metabolicdisorder such as occurs in some of the stromal dystrophieseg: granular, lattice and macular dystrophy. In these casesthis can lead to a recurrence of the disease within the graft.
Endothelial cells maintain a clear and compact corneain the face of the osmotic load of corneal stromalmucopolysaccharides through two-enzymatic pumps3.The most important is ATPase dependent, of lessimportance is a carbonic anhydrase pump. As such cornealendothelial cells are of prime importance in maintainingnormal corneal function.They are non-mitotic and thereforenon-replicatory in humans. As such the loss of sufficientendothelial cells as a result of an allogenic immune reactioncan lead to irreversible graft edema.
High-risk corneal graftsThe definition of high and low-risk largely relates to
outcomes as measured through corneal graft registries andchart reviews. According to the Corneal ColloborativeTransplantation Studies, high risk for graft rejectioninclude cases where there is more than two quadrants ofstromal vascularization and cases of re-grafts.
Corneal Graft Rejection: Management and PreventionNamrata Sharma MD, DNB, MNAMS, Jeewan S Titiyal MD, Rasik B Vajpayee MS, FRCSEd
Cornea & Refractive Surgery ServicesR.P. Centre, AIIMS,New Delhi
The Australian Corneal Graft Registry, one of the largestfound the following factors which were responsible forincreased chances of rejection5.
Indication for graft other than keratoconus or othercorneal dystrophyPrevious failed ipsilateral graftAphakiaInflammation at the time of the graft surgeryPresence of an anterior chamber or iris clip intraocularlensGraft size outside 7.0-7.9mm.Post-operative corneal neovascularization
Decreasing graft rejection in high-risk graftsThe mainstay of the success of reducing graft rejection
is the liberal use of topical corticosteroids.The matching of MHC and blood group antigens has
also been examined in several major studies including theCollaborative Corneal Transplantation Study (CCTS)6. Thisfailed to establish any benefit from matching for Class1 orClass 2 antigens for high-risk grafts. CCTS found asignificant reduction in the frequency of allograft rejectionin high-risk cases when the ABO blood group was matched.
Systemic (oral) cyclosporin A (CsA) has been evaluatedin several studies. As with solid organ transplantationdual or triple therapy immunosuppression is probablyrequired to significantly decrease the risk of rejection. Assuch the substantial risks and cost probably outweigh thesmall benefit of single therapy oral cyclosporin A7.
Prophylactic treatment of graft rejectionApart from avoiding and identifying high-risk grafts
one can reduce the incidence of rejection episodes byidentifying and treating high-risk episodes for the graft.
This includes any suture manipulation such asremoval or suture manipulation, as is the case in post-operative running suture adjustment to controlastigmatism.
Any intraocular surgery such as cataract extractionand intraocular lens implantation or corneal surgery suchas LASIK also represents an increased risk to the graft. Atsuch times it is appropriate to prophylactically treat witha short course of a potent topical corticosteroids, such as .prednisolone acetate 4 times a day for 1 week
SURGICAL OPHTHALMOLOGY

401DOS Times - Vol. 11, No. 6 December, 2005
Other risk factors for graft rejectionSeveral drugs are thought to affect graft survival either
through being proinflammatory or decreasing endothelialcell pump function.
Latanoprost, a topical synthetic prostaglandinanalogue, has been implicated in the reactivation andamplification of uveitis and cystoid macular oedema aspart of its’ general proinflammatory nature.
Dorzolamide, a topical synthetic carbonic anhydraseinhibitor, inhibits the endothelial cell enzymatic pumpmechanism. This action may jeopardize the graft.
Acute treatment of graft rejectionPrompt reversal of the rejection episode is the primary
aim of treatment. It is preferable to achieve reversal of agraft rejection episode quickly with minimal endothelialcell loss than slowly with more marked endothelial cellloss even if both result in a clear and compact corneal graft.For this reason prompt presentation and aggressivetreatment is of paramount importance.
Signs and SymptomsThe first step in the management of acute graft rejection
is adequate patient education with respect to thesymptoms of rejection and the need for promptpresentation. One of the first symptoms is photophobia,usually followed by ache, blur, redness and even tearing.
Graft rejection is uncommon in the first month or twofollowing surgery, presumably because it takes some timefor the host immune system to recognize and to becomeprimed to the donor alloantigens. This is not necessarilythe case if the donor alloantigens have already beenencountered by the host immune system as can occur withprior grafts or blood transfusions.
The signs of rejection can range from minimal anteriorchamber reaction with cell and flare up to a gross anteriorchamber reaction, even with a hypopyon with associatedkeratic precipitates and overlying stromal and evenmicrocystic epithelial edema. The area of affected corneamay be localized. This may be quite marked if there is aprogressive line of keratic precipitates, a Khodadoust line.
Usually no investigations are necessary althoughpachymetry over the effected area may be useful inmonitoring the effectiveness of treatment
Medica TherapyThe mainstay of treatment is the aggressive
administration of potent topical corticosteroids with goodintraocular penetration12,13. As such prednisolone ordexamethasone conjugated to acetate or sodium phosphateto increase penetration through an intact epithelium is
usually chosen. An added benefit is the enhancedabsorption provided by the epithelial barrier degradationseen with many preservatives such as benzylkoniumchloride.
The added benefit of oral or intravenouscorticosteroids is debated and only uncommonly used14,15.Concerns about compliance may also lead to the admissionof the patient to hospital for the first few days of treatment.After observing a clinical response to treatment the dosageof steroid is usually tapered over the next several weeks.As the presence of a recent rejection episode indicates anincrease in the risk of subsequent rejection it is advisableto keep the patient on some topical steroids for the nextyear or so.A commonly used treatment regime is:
Topical Prednisolone acetate hourly day and night for1 to 2 daysTopical prednisolone acetate 2 hourly for several daysfollowed by tapering over 1 month to 3 times a dayTopical prednisolone acetate three times a day for 1month then twice a day maintained for 6 months thendaily for six monthsIf the patient does not adequately respond to topical
treatment it is important to assess compliance and ifnecessary admit for inpatient administration of drops and/or add in systemic, usually oral steroids at a dosage of 1mg/Kg per day for 3 days. Topical 2% eye drops are alsogiven in qid doses for 6 months to 1 year.
Pulse Steroid TherapyMethylprednisolone 125–250mg intravenously at the
time of surgery followed by oral prednisolone 1 mg/kg/day slowly tapered in 3-6 months may be useful in high-risk cases.Severe or refractory rejection may also respondto systemic immunosuppression. The role of pulsedintravenous methylprednisolone for severe rejection is notproven and may only be of benefit if the patient presentsearly in the rejection episode4, some surgeons prefer to useshort term high dose oral prednisolone in these cases:
A single intravenous dose of Methylprednisolone500mgs 3 or
Oral prednisolone 80mgs daily 4 for 5-7 daysImmunosuppressants used in graft rejection
Cyclosporine ATopical
Cyclosporin A 2% in castor oil or 1% in artificial tears4 times daily
Commercial preparations offering better penetrationand efficacy should be shortly forthcoming.
DOS Times - Vol. 11, No. 6December, 2005 402
SystemicSome success has been achieved with the use of
systemic cyclosporin in high-risk keratoplasty10:4-5 mg/kg once or two divided doses dailyBlood Cyclosporin A level should be between 100 –
300ng/mlAll patient using Cyclosporin A need close monitoring
of blood pressure, renal function including serumcreatinine and liver enzymes.
Azathioprine50mgs daily increasing to a maintenance dose of 75 -
100mgs dailyUsed as a ‘steroid sparing’ agent in rejection for high-
risk keratoplasty.Renal, hepatic and bone marrow function must be
monitored.
Mycophenolate mofetil2000 - 3000mgs dailySuppresses lymphocyte proliferation in a similar
manner to azathioprine.Better tolerated than azathioprine.It may increasingly have a role in the management of
rejection in high-risk keratoplasty .
TacrolimusThis is a macrolide immunosuppressant that is a fungal
metabolite and suppresses both humoral and cellularimmune responses.
Renal function must be monitored and neurologicaladverse effects have been documented(more so withintravenous preparations).
It may surpass cyclosporin as the ‘steroid sparing’agent of choice in the future.
References1. Williams KA, Muehlberg SM, Lewis RF et al. Long-term outcome
in corneal transplantation. The Australian Corneal Graft Registry.Transplant Proc. 1997;29:983
2. Aldredge OC, Krachmer JH. Clinical types of corneal rejection.The manifestations, frequency, preoperative correlates andtreatment. Arch. Ophthalomol. 1981;99:599-604.
3. Bourne WM. Clinical estimation of corneal endothelial pumpfunction. Trans Am Ophthalmol Soc 98;96:229-239
4. Larkin DFP. Corneal transplantation for herpes simplex keratitis.Br. J. Ophthalmol. 1998;82:107-108.
5. Williams KA, Roder D, Esterman A, Meuhlberg SM, Coster DJ.Factors predictive of corneal graft survival. Report from theAustralian Corneal Graft Registry. Ophthalmol. 1992;99:403-414
6. The collaborative corneal transplantation studies (CCTS).Effectiveness of histocompatibility matching in high-risk cornealtransplantation. The collaborative corneal transplantation studiesresearch group. Arch. Ophthlmol. 1992;110:1392-1403.
7. Lam DS, Wong Ak, Tham CC, Leung AT. Theuse of combinedintravenous pulse and oral cyclosporin A in the treatment of cornealgraft rejection: a preliminary study. Eye 1998;12:615-618
8. Tambasco FP, Cohen EJ, Nguyen MD, Rapuano CJ, Laibson PR.Oral acyclovir after penetrating keratoplasty for herpes simplexkeratitis. Arch Ophthalmol. 1999;117:445-449.
9. Simon AL, Pavan-Langston D. Long-term oral acyclivir therapy.Effect on recrrent infectious herpes simplex keratitis in patientswith and without grafts. Opthalmol. 1996;103:1399-1404
10. The Herpetic Eye Disease Study Group. Acyclovir for theprevention of recurrent herpes simplex eye disease. N.Engl. J.Med. 1998;339:300-306
11. Konowal A, Morriaon JC, Brown SV, Cooke DL. Irreversiblecorneal decompensation in patients treated with topicaldorzolamide. Am J Ophthalomol. 1999;127:403-406
12. Barker NH, Henderson TRM, Ross CA, Coster DJ, Williams KA.Current Australian practice in the prevention and management ofcorneal allograft rejection. Clin. Exp. Ophthalmol. 2000;28:357-360.
13. Rinne JR, Stulting RD. Current practices in the prevention andtreatment of corneal graft rejection. Cornea 1992;11:326-328
14. Hill J, Maske R, Watson P. Corticosteroids in graft rejection.Ophthalmol. 1991;98:329-333.
15. Hudde T, Minassian DC, Larkin DFP. Randomised controlled trialof corticosteroid regimens in endothelial corneal allograftrejection. Br. J. Ophthalmol. 1999;83:1348-1352
16. Perry HD, Donnenfeld ED, Acheampong A et al. Topicalcyclosporin A in the management of postkeratoplasty glaucomaand corticosteroid-induced ocular hypertension and the penetrationof topical 0.5% cyclosporin A into the cornea and anterior chamber.CLAOJ 1998;24:159-165
403DOS Times - Vol. 11, No. 6 December, 2005
Subretinal fluid drainage during scleral buckling maynot be needed in all cases. It should however be done incase of retinal detachments which are associated withbullae, inferior breaks, PVR of grade B or greater, poorretinal pigment epithelial function ( in high myopes,ARMD), glaucoma and chronic detachments.
Site1. Drainage is safe on either side of the horizontal recti
muscles, as these areas have less choroidal vasculature.2. It is best to drain through sclera that will be buckled-
preferably in the posterior third of the bed of the buckle.In case the fluid is posterior to the buckle, the site ischosen posterior to the buckle and closed withpreplaced non –absorbable sutures.
3. Drain in an area where the retina appears less mobile,to avoid retinal incarceration
4. Avoid draining through the area of the cryoapplication, because cryopexy dilates choroidal vesselsand increases risk of bleeding.
5. Avoid drainage in the superotemporal quadrant toavoid gravitation of blood under the fovea in case of asubretinal bleed.
6. Do not drain near a large retinal break to preventvitreous draining out through the break.
Methods1. The classical method- 3-4 mm sclerotomy is made, its
margins diathermized and the choroidal knuckleexposed. The choroid is examined under themicroscope to look for large choroidal vessels, and thendiathermized. Entry through the choroids can be madewith a 26 g needle, 5-0 suture needle, sharp diathermyelectrode or even laser.
2. Needle drainage – Using a 26 g needle to pass directlythrough the sclera and enter the subretinal space. Maynot help in long standing detachments where the SRFis viscous.
3. Combined method-A partial thickness sclerotomy ismade (a thing layer of scleral fibres is retained) anddrainage done with 26 g needle.
Pearls for Subretinal Fluid DrainageS.N. Jha MD, H.K. Tewari MD, Amit Khosla MD, Neeraj Manchanda DO, DNB, Tinku Bali, MS, FRCS
Technique1. Complete all essential steps before drainage such as
break localization, retinopexy, buckle and sutureplacement. Also check that there is sufficient SRF todrain and that it has not shifted.
2. Make sure that the IOP is not elevated while perforatingthe choroids - ask the assistant to relax the tractionsutures and loosen all buckle sutures. Drainage of SRFwhen the IOP is high may cause retinal incarceration.Also make only a small opening in the choroid with a26g needle or the tip of a 5-0 suture needle to preventincarceration.
3. Do not allow sudden hypotony during SRF drainageas this could result in a suprachoroidal haemorrhage(especially in eyes with high myopia) or retinalincarceration. A controlled slow drainage has lessercomplications, and the assistant has an important roleto play at this step. As the SRF drains the assistantshould increase the IOP by pulling on the tractionsutures. IOP can also be maintained by indenting thesclera at constant pressure using cotton tippedapplicators in the quadrant opposite to the drainagesite tightening the buckle sutures, and tying theencircling band. Intraocular fluid or sterile air can alsobe injected to build up the volume in case of extremehypotony.
4. Pressure over the globe near the ora serrata in thequadrant of drainage helps in moving fluid out of thedrainage site. If drainage slows or stops prematurelythe sclerotomy can be manipulated with a fine toothforceps to reestablish flow.
5. Pigment particles in the SRF indicate that drainage isnearing completion. Small amounts of blood may beseen escaping with the SRF and may be innocuous.
6. In case of a larger subretinal haemorrhage, ensure thatblood does not pass into the macular area by rotatingthe globe and turning the patient’s head.
7. Total drainage of subretinal fluid is not necessary.Drainage should be enough to allow the scleral buckleto close the retinal breaks effectively. If after drainagethe retina follows the contour of the buckle. Thedrainage is usually adequate even if there is residualSRF. However if the buckling effect is not visible underthe retina, additional drainage is usually needed.
Department of OphthalmologySir Ganga Ram Hospital,New Delhi
SURGICAL PEARLS

DOS Times - Vol. 11, No. 6December, 2005 404
Intraocular pressure (IOP) plays a critical role in ocularhealth with derangements in IOP causing profoundstructural alterations in the eye. Measurement of IOP ishence of vital importance in ophthalmic examination. Thequantitative assessment of intraocular pressure is knownas tonometry; the instruments used for tonometry areknown as tonometers. Each technique has inherentadvantages and disadvantages, none is ideal.
HistorySchiotz in 1905 developed the prototype of indentation
tonometry. It was the first device that quantified IOP withrelative reproducibility along with the added advantageof economy of design and simplicity.
Maklakov in 1885 introduced the first applanationtonometer in which IOP was measured by flattening avariable area of corneal by a known weight.
Friedenwald (1948 & 1955) identified the role of‘coefficient of ocular rigidity’ which is a measure of theresistance of the eye to the distending forces of thetonometer. This was applied to improve the accuracy ofcalculation of IOP using the Schiotz tonometer.
Kalfa recognized the concept of ‘elastometric rise’, theequivalent of ocular rigidity in applanation tonometry andused it with the Maklakov tonometer.
Goldmann in 1954 introduced the applanationtonometer, the prototype of ‘constant corneal area’applanation methods. It was an improvement over Schiotzdevice both in terms of validity and reproducibility
Grolmann in 1972 introduced the prototype noncontact tonometer while Grant combined the concept ofSchiotz tonometry with continuous electronic monitoringto create the Electronic Indentation Tonometer. Hand-heldtonometers were designed by Halberg in 1967 asrefinements of the Maklakov and Posner (1964) tonometers.
Assessment of IOPDirect Method:
Manometry is used as a laboratory technique toperform continuous pressure measurements over time incadaveric eyes of humans or experimental animals. It is
TonometryDeepti Kautish MBBS, Charu Khurana MS, DNB, Usha Yadava MD, DNB
presently utilized to evaluate the effect of physiologicaland pharmacological manipulations on IOP and to studythe aqueous humor dynamics in post-mortem eyes.
Procedure – A hollow needle is introduced into theanterior chamber and connected to a reservoir of isotonicfluid which is raised just enough to prevent any loss ofaqueous from the eye. The height of the fluid column iscalibrated in centimeters of water or millimeters ofmercury to reflect the IOP.
Limitations -1. It is not practical for routine examination.2. If utilized in humans, it requires general anesthesia,
which itself alters IOP.3. The needle or cannula introduced into the eye causes
breakdown of the blood-aqueous barrier resulting inrelease of prostaglandins that modify IOP.
Indirect MethodsClassificationA. Indentation TonometersB. Appanation Tonometers
(i) Goldmann (Prototype)(ii) Goldmann – Type Tonometers
a) Perkins Tonometerb) Draeger Tonometer
(iii) Mackay Marg Applanator(iv) Mackay Marg – Type Tonometers
a) CAT 100b) Challenger Digitalc) Biotronicsd) Tono Pen (Hand-held)
(v) Maklakov Applanation Tonometer(vi) Maklakov Type Tonometers
a) Planometerb) Tonomatc) Halbergd) Barraquere) Ocular tension Indicatorf) Glaucotest
(vii) Pneumatic Tonometer (Pneumo-tonometer)
Guru Nanak Eye CentreMaharaja Ranjit Singh Marg,New Delhi
OPHTHALMIC PROCEDURES
405DOS Times - Vol. 11, No. 6 December, 2005
(viii) Non Contact Tonometera) X-Pert Tonometerb) Grolman Airblast Tonometerc) Keeler Pulsair Tonometer (Hand-held)
C. Miscellaneous Tonometers(i) Continuous-IOP Monitoring devices(ii) Self Tonometer(iii) Impact Tonometer(iv) Vibra Tonometer
D. Newer Tonometres(i) Trans-palpebral Tonometer (TG Dc- 01)(ii) Disposable Tonometers
a) Tonosafe – Acrylic Biprismb) Tonosheild – Silicone Shield
E. Other Methods(i) Tonography(ii) Ocular Blood Flow (OBF) Tonograph
Indentation/ Impression TonometryApparatus: Schiotz Tonometer
Principle: The cornea is indented in the shape of atruncated cone by standard weights (5.5g, 7.5g, 10g, 15g)which are applied via a plunger which moves freely withina shaft in the footplate. The resulting deformation of theglobe is measured with a scale reading. Value of thesestandard weights and the scale record of globe deformationis then used to determine IOP by correlations establishedin the Friedenwald tables.
Calculations: According to Freidenwald, the steady statepressure (Po) of an eye, is raised to a higher pressure (Pt)due to volume displacement caused by corneal indentation.This volume displacement causes some distension of theglobe – which itself is regulated by ‘ocular rigidity’ i.e.resistance of the eye to distending force of the tonometer.
Thus, calculations must include aconstant (k) i.e. “coefficient of ocularrigidity”. Friedenwald simplifiedthese tedious calculations & gave twotables in 1948 (k=0.0245) and 1955(k=0.0215). The former are supposedto be more accurate.
Technique: The patient is laidsupine with the cornea anesthetized.The fingers of the examiner spread theeyelids without putting pressure on
the globe while the patient is asked to fixate at a distantobject. The footplate is applied to the cornea and positionedto keep the tonometer vertical. The needle on the tonometerscale oscillates with the ocular pulse and the mid-point ofthe excursion is used as the scale reading. If the value of thescale reading is not greater than 4 units, additional weightsare added. Conversion tables are used to derive the IOP inmillimeters of mercury from the scale reading and plungerweight.
Errors1. Errors inherent to the instrument – due to difference
in weights of different parts of tonometers; differencein size, shape and curvature of footplate; friction arisingin movement of the plunger and the pointer on thescale.
2. Errors due to contraction of extraocular muscles.3. Errors due to accommodation – contraction of ciliary
muscle increases the aqueous outflow facility bypulling the trabecular meshwork and lowering IOP.
4. Error due to variation of corneal curvature – steep andthick corneas increase the fluid displacement by thetonometer, thus recording a false high IOP.
5. Errors due to high scleral/ocular Rigidity.6. Observer’s Error or Parallax Error in reading scale.7. Error due to blood volume alteration - variable
DOS Times - Vol. 11, No. 6December, 2005 406
displacement of intraocular blood during indentation.8. Moses Effect- false high IOP recorded if the cornea gets
sucked into the space between the plunger and hole inthe footplate.Error to the tune of + 2 mnHg in normal range of IOP,
and + 4mmHg in higher range of IOP has been reported.
Limitations of Indentation Tonometry1. Tables used to note IOP with reference to weight used
and scale reading obtained are based on average ‘k’values i.e. average “Coefficient of Ocular rigidity”.In cases with high ocular rigidity (high k) e.g. extreme
myopia, high hyperopia, chronic glaucoma,vasoconstrictor therapy, ARMD, the conversion tablesover-estimate IOP. In cases with low ocular rigidity (lowk) e.g. high myopia, miotic therapy, retinal detachmentsurgery using cryopexy, after intravitreal injection ofcompressible gas; vasodilator therapy, scleral buckling,vitrectomy; the conversion tables underestimate IOP.2. Corneal Variables: False high IOP is obtained with thick
corneas or very steep corneas. Keratoconus is notassociated with low ‘k’ – it is only an artifact whilemeasuring IOP due to thin cornea. The finding is notseen after keratoplasty. Measurements are unreliablein significant corneal pathologies.
3. Availability of other accurate applanation tonometersand their ease of application has significantly replacedSchiotz tonometers.
Applanation TonometryPrototype: Goldmann Tonometer - Introduced in 1954.
Principle: Imbert-Fick Principle also referred as theMaklakov-Fick Law which says that for an ideal sphere(perfectly spherical, dry, infinitely thin walled and perfectlyflexible), the pressure (P) inside sphere is equal to force (F)required to flatten/applanate the surface divided by thearea (A) of flattening i.e. P=F/A.
Calculations: Since cornea is not an ideal sphere, twoother significant forces should be considered:1. Force of capillary attraction (T) between tonometer
head and tear film –additive to (F).2. Additional force (C) independent of IOP which is
required to flatten the relatively inflexible cornea-opposite to (F).Hence, F+T = PA+Ci.e. IOP = (F+T-C)/A‘A’ is located on the interior surface of the cornea.
Goldmann applanation is designed such that A=7.35 mm2
and diameter of flattening of cornea is 3.06 mm. At thisvalue of ‘A’, the opposing forces of capillary attraction andcorneal inflexibility cancel out. In addition, at this ‘A’ theIOP (mmHg) = ten times the force applied to the cornea ingrams, a convenient conversion. Since only 0.5μl isdisplaced from the eye and the pressure induced by thetonometer tip is negligible, applanation tonometry is notsignificantly affected by ocular rigidity.
Instrument: The applanator tip contains a biprism whichit forms the contact point with the cornea. The tip isconnected via a rod to the body of the tonometer, whichcontains an adjustable spring that provides theappropriate applanating force. The force is adjusted byknob with a scale indicating the force applied in grams.
Clinical Measurement: The applanator is attached to slit

407DOS Times - Vol. 11, No. 6 December, 2005
lamp aligning the axis of the tip with the oculars andallowing visualization of the semicircles or mires.Maximum illumination with cobalt blue filter is adjustedin the slit lamp. The patient is positioned at the slit lamp,the cornea is anesthetized and tear film is stained with0.25% sodium flourescein.
The patient is instructed to fixate at distance, relaxand breathe normally. Breath holding or valsalva bypatient should be avoided. The tip is advanced toapproximate the cornea. The biprism splits the circle ofcontact into two semicircles/mires. When the inner marginsof these semicircles touch, a 3.06 mm diameter circle ofcornea is applanated. The mires appear green against ablue background. If mires are unequal in size, verticaladjustments are made. 1-gm position is used before eachmeasurement. It is more accurate to increase rather thandecrease the force of applanation. The tonometer knob isrotated until the end point is achieved. Ocular pulsationsare noted and the internal margin of each mire is aligned.
Sources of Error1. Wide, blurred mires and vertical misalignment result
in false high readings.2. Corneal Variables: Thin corneas and corneas thickened
by edema produce false low IOP readings while thickcorneas due to increased collagen result in false highreadings. For every 3 diopter increase in corneal powerthe average IOP is increased by 1mm Hg.
3. Corneal astigmatism results in a 1mm error for every4 diopters, underestimating for with-the-rule andoverestimating for against-the-rule astigmatism. Tominimize this error, the biprism is rotated until thedividing line between the prisms is 45º to the majoraxis of the ellipse.
4. Prolonged contact with cornea gives false low IOPreadings, apart from causing corneal injury.
5. Calibration should be done at least monthly.
Other Applanation Tonometers1. Perkins Applanation Tonometer – It uses the same
biprism as the Goldmann tonometer. The light sourceis powered by battery and a counter balance enablesits usage in both horizontal and vertical positions.Readings are consistent and comparable with theGoldmann applanator.It is especially useful for infants, children and invalidpatients who cannot sit at the slit lamp. It wasintroduced by Perkins in 1970.
2. Draeger Applanation Tonometer – It is similar to theGoldmann and Perkins applanator except that adifferent biprism is used. This instrument is alsoportable and useful in similar situations as the Perkins.It was introduced by J. Draeger (Germany) in 1966.
This hand held tonometer weighs only 700gms.
Mackay Marg TonometerPrinciple: The MacKay-Marg Tonometer applanates the
cornea via a plunger that moves within a sleeve, similar infashion to a Schiotz Tonomter. The excursion of this plungeris electronically coupled to a transducer and graphicallyrecords the movement of plunger on a moving paper strip.The plunger indents the cornea, recording on the graphpaper the sum of force required to flatten the cornea andthe intraocular pressure. As the tonometer advances, thesleeve abuts the cornea transferring the force required toflatten cornea to the sleeve. The pressure tracing thendecreases to a level that represents the IOP which occurswhen a corneal diameter of 3mm is applanated.
Sources of Error: Greater than 3mm corneal flatteningcauses false increase in IOP. Since IOP is recordedinstantaneously, multiple readings should be averaged tocompensate for fluctuation due to ocular pulsation.Specific Utility: In irregular and edematous corneas.
Mackay-Marg-Type Tonometers1. Cat 100 Applanation Tonometer2. Challenger Digital Electronic Applanation tonometer3. Biotronics
These tonometers have an internal logic program thatautomatically selects the acceptable measurements whiledeleting the inappropriate ones.4. Pneumatic tonometer: Works on a principle similar tothe MacKay Marg wherein a central sensing devicemeasures the IOP while the force required to bend thecornea is transferred to a surrounding structure. Theplunger is replaced by a column of air and the contactsurface is a polymeric silicone (Silastic) membrane. The aircolumn is continually vented via a port and changes inpressure in the column resulting from the applanation arerecorded via a transducer on a moving strip of paper. Itfinds special use in deformed corneas.5. Tono-Pen: It is a miniature hand-held MacKay-Margtype tonometer, weighing 16grams. A microprocessoranalyzes the waveform internally. Four to ten pressureestimations are obtained by briefly touching over thecornea, averaged and digitally displayed as mean ofaccepted estimations and their coefficient of variance (5%,10%, 20%, & >20%).
Manometric eye bank studies have indicated that theTonoPen is most accurate between 10-50 mmHg. Variousstudies have reported no statistical difference betweenGoldmann & Tono-Pen readings in the range of 10-35mmHg.-1 In another clinical study of 142 eyes, 63% ofTonopen readings were within +2mmHg of the Goldmannreadings and 77% were within +3mmHg of the Goldmannreadings with the best correspondence occurring between
DOS Times - Vol. 11, No. 6December, 2005 408
11-20mmHg. The Tonopen overestimated between 4-10mmHg and underestimated between 21-30mmHg.2
6. The ProTon tonometer works on the same principle asthe MacKay Marg but differs from the Tonopen in thatthe probe and display units are seperated.
Maklakov Applanation TonometryPrinciple: The IOP is estimated by measuring the area of
cornea that is flattened by a known weight. In this type oftonometry, the volume displacement is large enough toconsider the ocular rigidity in calculating IOP. Kalfa utilizeddifferent weights to calculate the ocular rigidity and termedit the ‘elastometric rise’.3
Instrument & Technique: It has a dumble shaped metalcylinder with flat endplates of polished glass on either endswith a diameter of 10mm. A set of 4 such instruments withweights of 5g, 7.5g, 10g & 15g are available. A layer of dye(suspension of argyrol, glycerin and water) is applied overeither end-plate which is placed vertically over theanesthetized cornea of supine patient. This produces acircular white imprint over end plate corresponding tothe area that was flattened. The diameter of this whitearea is measured with a transparent measuring scale to0.1mm and the IOP is read from conversion tablescorresponding to the weight used.
Maklakov Type TonometersThese are applanation tonometers in which variable
areas of the cornea are applanated.1. Maklakov-Kalfa – Prototype2. Applanometer – Ceramic end plates are used instead
of polished glass.3. Tonomat – It has disposable end plates.4. Halberg – Transparent end plates allowing direct
recording.5. Barraquer Tonometer – Plastic Tonometer for
Intraoperative measurements.6. Ocular Tension Indicator – Uses Goldmann biprism
and standard weights; used only for screening. Detectswhether readings are greater or less than 21mmHg
7. GlaucoTest – A screening tonometer with multiple endplates for selecting different ‘cut off’ pressures.4
Non-Contact TonometerIntroduced by Grolman in 1972, it has the unique
advantage of not touching the eye of the patient.Principle: A puff of room air directed over the patients’
anaesthetized cornea, momentarily deforms the cornea.The time from an internal reference point to the moment ofpresumed flattening is measured and converted to IOPbased on prior comparisons with readings from theGoldmann applanation tonometer.
The original NCT has 3 components and is mountedon a table(i) Alignment system – Allows the operator to align the
patient’s cornea in three dimensions i.e. Axial, vertical& lateral.
(ii) Optoelectronic applanation monitoring system whichconsists of a transmitter which directs a collimatedbeam of light at the corneal vertex and a receiver anddetector which accepts only parallel, coaxial raysreflected from cornea.
(iii) Pneumatic system which generates a puff of room air.
Pulsair TonometerIt is a newer, portable hand-held, non-contact
tonometer which has a precision within + 1mmHg of theGoldmann applanation tonometer.
X-Pert TonometerIn this instrument, an air puff is automatically
triggered when alignment criteria are met. The force of airrequired to achieve peak light detection is the measuredvariable.
Limitations of NCT1. The time interval for an average NCT measurement is1-3 millisecond which is 1/500th of one cardiac cycle. Themeasurements are random with respect to the phase ofthe cardiac cycle so that ocular pulse becomes a significantvariable i.e. it can’t be averaged with some tonometers.2. Glaucomatous eyes have greater momentaryfluctuations in IOP. Hence it is recommended that aminimum of three readings with in 3mmHg be taken andaveraged as IOP.
Miscellaneous Tonometers1. Continuous IOP monitoring devices(i) A strain gauge is placed in a contact lens to measure
changes in the meridional angle of the corneo-scleraljunction or
(ii) A strain gauge might be embedded in an encirclingscleral band to measure distension of globe or
(iii) A scleral applanting device maybe attached to apassive radio telemetric pressure transducer or
(iv) An instrument with applanating suction cups to allowbilateral recording of IOP for upto one hour in supinesubjects.
2. Self Tonometer: An applanation tonometer which canbe used by the patient himself without assistance.3. Home Tonometry can be practiced by teaching a familymember the technique of Schiotz tonometry.4. Impact Tonometry: Estimates IOP by measuring
409DOS Times - Vol. 11, No. 6 December, 2005
duration of contact of spring driven miniature hammerwith eye.5. Vibra Tonometer: Measures IOP by frequency ofvibrating probe in contact with cornea.
Comparison of TonometersFor Regular Corneas1. Schiotz Vs Goldmann: Schiotz reads lower than the
Goldmann applanation tonometer even when posturalinfluence is eliminated. Variation is maximum in the50-60 years age group.
2. Perkins Vs Goldmann: Difference of Perkins with theGoldmann when expressed as root mean squaredifference was 1.4 mm Hg. Perkins is accurate in bothhorizontal & vertical positions and has special utilityin infants & children in the operating theater.
3. Draeger Vs Perkins: Draeger has a more complexapparatus and is more difficult to use than Perkins.Also, patient acceptance is worse in Draeger’s.
4. MacKay Marg: When used without anesthesia meanIOP measured was approximately 2mmHg more thanthat obtained by same instrument with anesthesia.
7. Tonopen: It compares favourably against manometricreading in human autopsy eyes. It underestimatesGoldmann in higher ranges and over estimatesGoldmann readings in lower range.
8. Pneumatic Tonometer: Gives comparable andreproducible readings.
9. Non Contact Tonometer: Reliable within normal rangeof IOP but reliability decreases with high pressureranges, abnormal corneas and poor fixation.
Tonometry on Irregular CorneaIn cases of scarred or edematous corneas, the MacKay
Marg Tonometer is considered to be the most accurate.Pneumatic tonometers are also useful in patients withdiseased corneas. The Tonopen also compared favorablywith MacKay Marg on irregular corneas.
Tonometry Over Soft Contact LensesThe MacKay Marg tonometer, the Pneumatonograph
and Tonopen can measure IOP through bandage contactlenses with reasonable accuracy. Applanationmeasurements are said to be affected by the power ofcontact lenses with high water content. Correction tableshave been developed to compensate for this. Non Contacttonometer readings with and without soft contact lensesindicated that the power of the lens influenced thedifference in IOP between paired readings, with hyperopiclenses giving the greatest difference.
Tonometry with Gas-filled eyesIntraocular gas significantly alters scleral rigidity and
indentation tonometry is hence unreliable. The Pneumatictonometer and Tonopen compare favorably withGoldmann applanation readings.
Other Ocular Conditions1. In premature Infants with stage 5 Retinopathy of
prematurity, applanation Tonomentry was preferableto indentation.
2. In eye bank eyes with flat anterior chamber, none ofthe tonometric devices correlate well withmanometrically-determined pressures.
Disposable Tonometry DevicesThe risk of cross infection with use of devices that touch
the surface of eye has lead to the search for disposabletonometers. Commercially available devices include1. Tonosafe: It has an acrylic biprism and IOP
measurements show an accurate correlation withGoldmann applanation readings5.
2. Tonoshield: Utilizing a silicone shield, this tonometricdevice tends to overestimate IOP when compared withstandard Goldmann applanation.
Sterilization of tonometersContaminated tonometers are vectors of infections and
have the potential to transmit them from patient to patient.Various agents which have been isolated from tears includeAdenovirus 8, HSV I, HBV and HTLV III. Soaking theapplanation tip in diluted sodium hypochlorite, 70%isopropyl alcohol or 3% H2O2 can completely disinfect thetonometer. 10 minutes of rinsing in tap water can removeall detectable HBV surface antigens.
Bibliography1. Booth WA, Lee DA, Panek WC et al. The Tono-Pen. A manometric
and clinical study. Arch Ophthalmol 1988;106:12142. Frenkel REP, Hong YJ, Shin DH. Comparison of the Tono-Pen to
the Goldmann applanation tonometer Arch Ophthalmol1988;106:750
3. Friedenwald JS. Contribution to the theory and practice oftonometry II. An analysis of the work of Professor S Kalfa with theapplanation tonometer. Am J Ophthalmol 1939;22:375
4. Shields MB. Text book of Glaucoma (4th Ed.) William and Wilkins1998
5. Bhatnagar A, Gupta AK. Disposable devices for measuring IOP: aclinical study to assess accuracy. Eye 2005; 19:752-754
6. Albert DM, Jakobeic FA. Principles and Practice of Opthalmology(2nd Ed), WB Saunders 2000
7. Agarwal S, Agarwal A, Apple D. Text Book of Ophthalmology(2nd Ed.) Vol.3
8. Choplin NT, Lundy DC. Atlas of Glaucoma
DOS Times - Vol. 11, No. 6December, 2005 410
DescriptionDORZOLAMIDE (Dorzolamide hydrochloride
ophthalmic solution) is a carbonic anhydrase inhibitorformulated for topical ophthalmic use.
Dorzalamide hydrochloride is described chemicallyas:
(4S-trans)-4-(ethylamino)-5, 6-dihydro-6-methyl-4H-thieno [2, 3-b] thiopyran-2-sulfonamide 7, 7-dioxidemonohydrochloride. Dorzolamide hydrochloride isoptically active.
Its empirical formula is C10H16N2O4S3OHCl and itsstructural formula is shown in Figure 1:
It is a white to off-white, crystalline powder, which issoluble in water and slightly soluble in methanol andethanol.
The sterile ophthalmic solution is supplied as a sterile,isotonic, buffered, slightly viscous, aqueous solution ofDorzolamide hydrochloride. Each ml of Dorzolamide 2%contains 20 mg Dorzolamide (22.3 mg of dorzolamidehydrochloride). Inactive ingredients added to adjust thepH include hydroxyethyl cellulose, mannitol, sodiumcitrate dihydrate, sodium hydroxide and water forinjection. Benzalkonium chloride 0.0075% is added as apreservative.
DorzolamideSudipta Ghosh, MBBS, DOMS.
ICARE Eye Hospital and Post Graduate Institute,Glaucoma Research Center, E 3A,Sector 26, Noida (U.P.)
Table 1: Physical Properties of DorzolamideMolecular weight 360.9Melting point 264 Degree centigradepH 5.6Osmolarity 260 - 330mOsM
Fig. 1: Structural Formula of Dorzolamide
Mechanism of ActionDorzolamide ophthalmic solution contains
Dorzolamide hydrochloride, an inhibitor of humancarbonic anhydrase II. It catalyzes the reversible reactioninvolving the hydration of carbon dioxide and thedehydration of carbonic acid. In humans, carbonicanhydrase exists as a number of isoenzymes, the mostactive being carbonic anhydrase II (CA-II), found primarilyin red blood cells (RBCs), but also in other tissues. Inhibitionof carbonic anhydrase in the ciliary processes of the eye
decreases aqueous humor secretion, presumably byslowing the formation of bicarbonate ions with subsequentreduction in sodium and fluid transport. The result is areduction in intraocular pressure (IOP).
Pharmacokinetics/PharmacodynamicsWhen topically applied, dorzolamide reaches the
systemic circulation. Dorzolamide accumulates in RBCsduring chronic dosing as a result of binding to CA-II.Dorzolamide binds moderately to plasma proteins(approximately 33%). It is primarily excreted unchangedin the urine; the metabolite also is excreted in urine. Afterdosing is stopped, dorzolamide washes out of RBCsnonlinearly, resulting in a rapid decline of drugconcentration initially, followed by a slower eliminationphase with a half-life of about four months.
Indications and UsageOcular HypertensionOpen angle glaucomaPediatric glaucoma
Dosage and AdministrationThe dose is one drop three times daily.Dorzolamide may be used concomitantly with other
topical ophthalmic drug products to lower intraocularpressure.
StorageTemperature: 15-30° C or 59-86° F.The drug needs to be protected from light.
Side EffectsMore common: Itching, redness, swelling, or other sign
OCULAR PHARMOCOLOGY
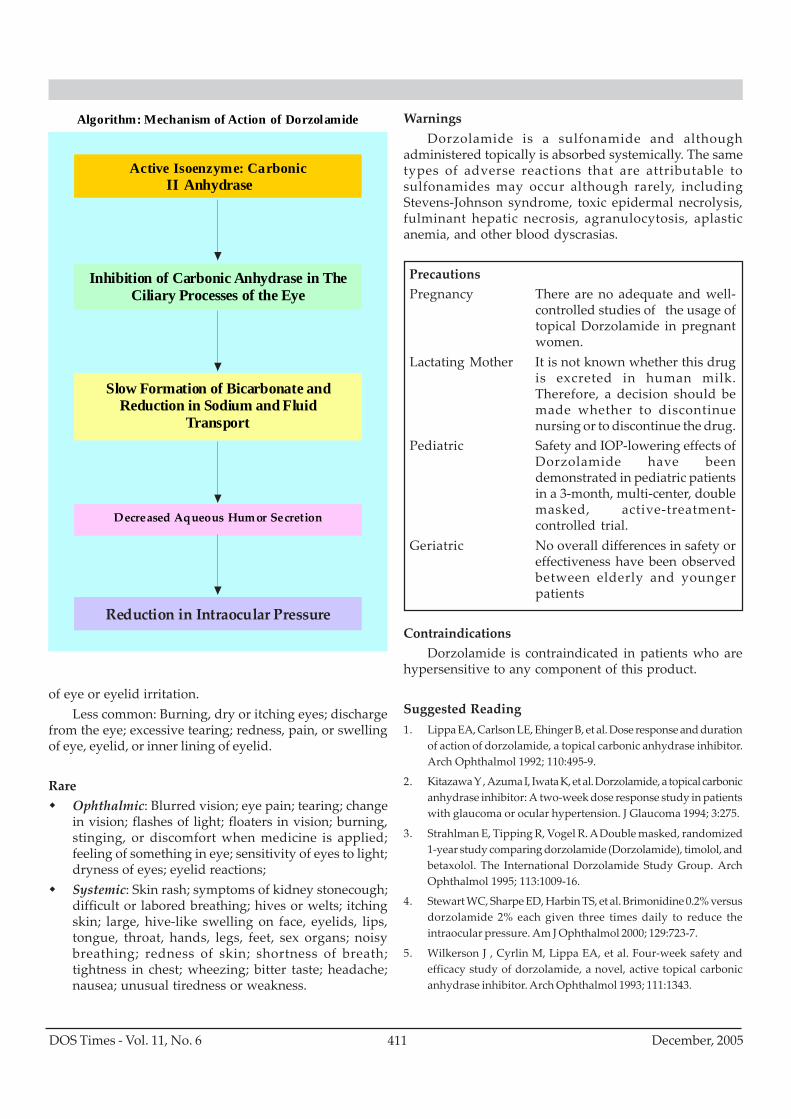
411DOS Times - Vol. 11, No. 6 December, 2005
of eye or eyelid irritation.Less common: Burning, dry or itching eyes; discharge
from the eye; excessive tearing; redness, pain, or swellingof eye, eyelid, or inner lining of eyelid.
RareOphthalmic: Blurred vision; eye pain; tearing; changein vision; flashes of light; floaters in vision; burning,stinging, or discomfort when medicine is applied;feeling of something in eye; sensitivity of eyes to light;dryness of eyes; eyelid reactions;Systemic: Skin rash; symptoms of kidney stonecough;difficult or labored breathing; hives or welts; itchingskin; large, hive-like swelling on face, eyelids, lips,tongue, throat, hands, legs, feet, sex organs; noisybreathing; redness of skin; shortness of breath;tightness in chest; wheezing; bitter taste; headache;nausea; unusual tiredness or weakness.
WarningsDorzolamide is a sulfonamide and although
administered topically is absorbed systemically. The sametypes of adverse reactions that are attributable tosulfonamides may occur although rarely, includingStevens-Johnson syndrome, toxic epidermal necrolysis,fulminant hepatic necrosis, agranulocytosis, aplasticanemia, and other blood dyscrasias.
PrecautionsPregnancy There are no adequate and well-
controlled studies of the usage oftopical Dorzolamide in pregnantwomen.
Lactating Mother It is not known whether this drugis excreted in human milk.Therefore, a decision should bemade whether to discontinuenursing or to discontinue the drug.
Pediatric Safety and IOP-lowering effects ofDorzolamide have beendemonstrated in pediatric patientsin a 3-month, multi-center, doublemasked, active-treatment-controlled trial.
Geriatric No overall differences in safety oreffectiveness have been observedbetween elderly and youngerpatients
ContraindicationsDorzolamide is contraindicated in patients who are
hypersensitive to any component of this product.
Suggested Reading1. Lippa EA, Carlson LE, Ehinger B, et al. Dose response and duration
of action of dorzolamide, a topical carbonic anhydrase inhibitor.Arch Ophthalmol 1992; 110:495-9.
2. Kitazawa Y , Azuma I, Iwata K, et al. Dorzolamide, a topical carbonicanhydrase inhibitor: A two-week dose response study in patientswith glaucoma or ocular hypertension. J Glaucoma 1994; 3:275.
3. Strahlman E, Tipping R, Vogel R. A Double masked, randomized1-year study comparing dorzolamide (Dorzolamide), timolol, andbetaxolol. The International Dorzolamide Study Group. ArchOphthalmol 1995; 113:1009-16.
4. Stewart WC, Sharpe ED, Harbin TS, et al. Brimonidine 0.2% versusdorzolamide 2% each given three times daily to reduce theintraocular pressure. Am J Ophthalmol 2000; 129:723-7.
5. Wilkerson J , Cyrlin M, Lippa EA, et al. Four-week safety andefficacy study of dorzolamide, a novel, active topical carbonicanhydrase inhibitor. Arch Ophthalmol 1993; 111:1343.
Algorithm: Mechanism of Action of Dorzolamide
Active Isoenzyme: Carbonic Anhydrase II
Inhibition of Carbonic Anhydrase in The Ciliary Processes of the Eye
Slow Formation of Bicarbonate and Reduction in Sodium and Fluid
Transport
Decreased Aqueous Humor Secretion
Reduction in Intraocular Pressure
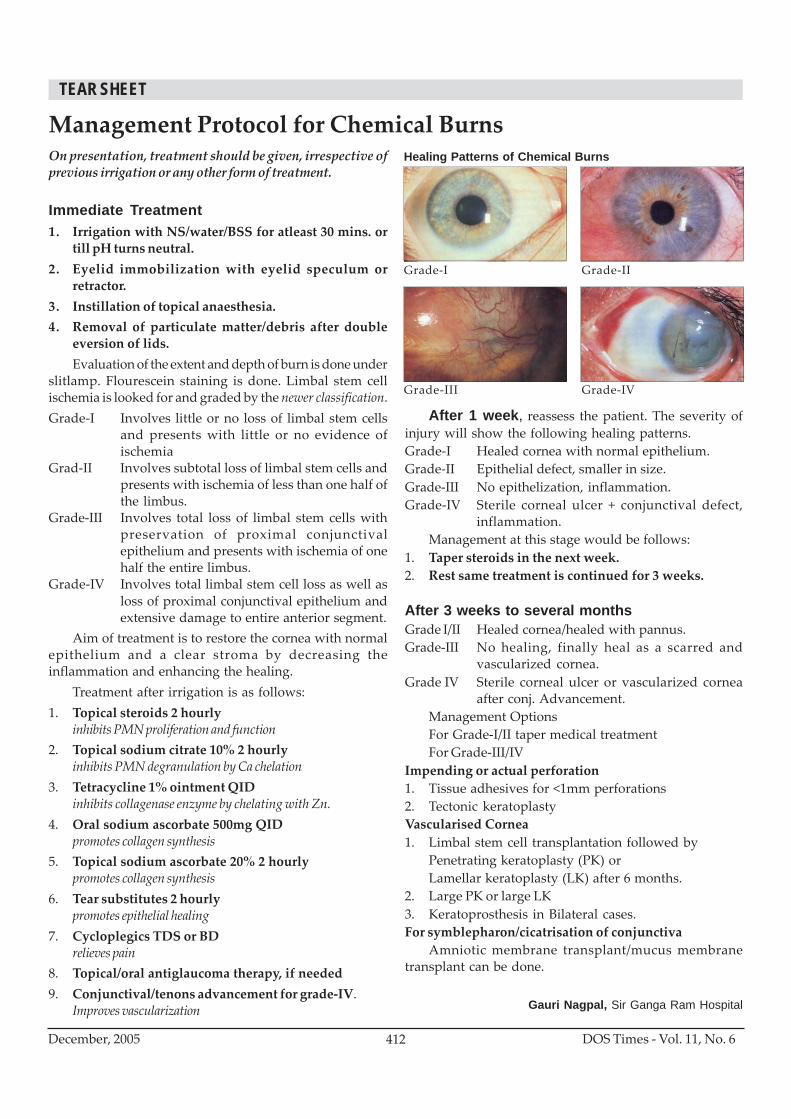
DOS Times - Vol. 11, No. 6December, 2005 412
On presentation, treatment should be given, irrespective ofprevious irrigation or any other form of treatment.
Immediate Treatment1. Irrigation with NS/water/BSS for atleast 30 mins. or
till pH turns neutral.2. Eyelid immobilization with eyelid speculum or
retractor.3. Instillation of topical anaesthesia.4. Removal of particulate matter/debris after double
eversion of lids.Evaluation of the extent and depth of burn is done under
slitlamp. Flourescein staining is done. Limbal stem cellischemia is looked for and graded by the newer classification.Grade-I Involves little or no loss of limbal stem cells
and presents with little or no evidence ofischemia
Grad-II Involves subtotal loss of limbal stem cells andpresents with ischemia of less than one half ofthe limbus.
Grade-III Involves total loss of limbal stem cells withpreservation of proximal conjunctivalepithelium and presents with ischemia of onehalf the entire limbus.
Grade-IV Involves total limbal stem cell loss as well asloss of proximal conjunctival epithelium andextensive damage to entire anterior segment.
Aim of treatment is to restore the cornea with normalepithelium and a clear stroma by decreasing theinflammation and enhancing the healing.
Treatment after irrigation is as follows:1. Topical steroids 2 hourly
inhibits PMN proliferation and function2. Topical sodium citrate 10% 2 hourly
inhibits PMN degranulation by Ca chelation3. Tetracycline 1% ointment QID
inhibits collagenase enzyme by chelating with Zn.4. Oral sodium ascorbate 500mg QID
promotes collagen synthesis5. Topical sodium ascorbate 20% 2 hourly
promotes collagen synthesis6. Tear substitutes 2 hourly
promotes epithelial healing7. Cycloplegics TDS or BD
relieves pain8. Topical/oral antiglaucoma therapy, if needed9. Conjunctival/tenons advancement for grade-IV.
Improves vascularization
Management Protocol for Chemical Burns
After 1 week, reassess the patient. The severity ofinjury will show the following healing patterns.Grade-I Healed cornea with normal epithelium.Grade-II Epithelial defect, smaller in size.Grade-III No epithelization, inflammation.Grade-IV Sterile corneal ulcer + conjunctival defect,
inflammation.Management at this stage would be follows:
1. Taper steroids in the next week.2. Rest same treatment is continued for 3 weeks.
After 3 weeks to several monthsGrade I/II Healed cornea/healed with pannus.Grade-III No healing, finally heal as a scarred and
vascularized cornea.Grade IV Sterile corneal ulcer or vascularized cornea
after conj. Advancement.Management OptionsFor Grade-I/II taper medical treatmentFor Grade-III/IV
Impending or actual perforation1. Tissue adhesives for <1mm perforations2. Tectonic keratoplastyVascularised Cornea1. Limbal stem cell transplantation followed by
Penetrating keratoplasty (PK) orLamellar keratoplasty (LK) after 6 months.
2. Large PK or large LK3. Keratoprosthesis in Bilateral cases.For symblepharon/cicatrisation of conjunctiva
Amniotic membrane transplant/mucus membranetransplant can be done.
Healing Patterns of Chemical Burns
Grade-I Grade-II
Grade-III Grade-IV
Gauri Nagpal, Sir Ganga Ram Hospital
TEAR SHEET





























