Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=imte20
Download by: [UNAM Ciudad Universitaria] Date: 25 September 2017, At: 10:48
Medical Teacher
ISSN: 0142-159X (Print) 1466-187X (Online) Journal homepage: http://www.tandfonline.com/loi/imte20
Toward a shared language for competency-basedmedical education
Robert Englander, Jason R. Frank, Carol Carraccio, Jonathan Sherbino,Shelley Ross, Linda Snell & on behalf of the ICBME Collaborators
To cite this article: Robert Englander, Jason R. Frank, Carol Carraccio, Jonathan Sherbino,Shelley Ross, Linda Snell & on behalf of the ICBME Collaborators (2017) Toward a sharedlanguage for competency-based medical education, Medical Teacher, 39:6, 582-587, DOI:10.1080/0142159X.2017.1315066
To link to this article: http://dx.doi.org/10.1080/0142159X.2017.1315066
Published online: 09 Jun 2017.
Submit your article to this journal
Article views: 698
View related articles
View Crossmark data
Citing articles: 3 View citing articles

Toward a shared language for competency-based medical education
Robert Englandera, Jason R. Frankb,c, Carol Carracciod, Jonathan Sherbinoe, Shelley Rossf ,and Linda Snellb,g; on behalf of the ICBME CollaboratorsaSchool of Medicine, University of Minnesota, Minneapolis, MN, USA; bRoyal College of Physicians and Surgeons of Canada, Ottawa,Canada; cDepartment of Emergency Medicine, University of Ottawa, Ottawa, Canada; dAmerican Board of Pediatrics, Chapel Hill, NC,USA; eDivision of Emergency Medicine, Department of Medicine, McMaster University, Hamilton, Canada; fDepartment of FamilyMedicine, University of Alberta, Edmonton, Canada; gCentre for Medical and Department of General Internal Medicine, McGill University,Montreal, Quebec, Canada
ABSTRACTThe paradigm shift brought about by the advent of competency-based medical education (CBME) can be characterized asan adaptive change. Currently, its development and implementation suffer from the lack of a lingua franca. A shared lan-guage is needed to support collaboration and dissemination across the world community of medical educators. TheInternational CBME Collaborators held a second summit in 2013 to explore this and other contemporary CBME issues. Wepresent the resulting International CBME Collaborator’s glossary of CBME terms. Particular attention is given to the termscompetency, entrustable professional activity (EPA), and milestone and their interrelationships. Medical education scholars andenthusiasts of the competency-based approach are encouraged to adopt these terms and definitions, although no doubtthe vocabulary of CBME will continue to evolve.
Introduction
Shared language is important in leading adaptive change.When people begin to use the same words with the samemeaning, they communicate more effectively, minimizemisunderstandings, and gain the sense of being on thesame page, even while grappling with significant differen-ces on the issues (Heifetz et al. 2009, p. 9).
The paradigm shift in medical education from anapproach focused on structure and process to one focusedon competencies is well under way (Carraccio & Englander2013). Getting from where we are currently – essentially,still in the world espoused by Flexner over 100 years ago(Flexner 1910) – to where we want to be in a competency-based model has all the hallmarks of an adaptive challenge.This type of challenge is distinct from a technical challengein the following ways: (1) the path is not clear; (2) the des-tination requires a change of identity for education andtraining programs; (3) the journey requires new competen-cies and experimentation for educators, clinical faculty, andtrainees alike; (4) the process generates disequilibrium andoften a sense of loss; and (5) the process takes longer toresolve than technical work (Heifetz et al. 2009). This kindof fundamental change is greatly facilitated by a sharedlanguage of related terms.
Ambiguity around the language of CBME has been high-lighted as an important barrier to the adoption of the newparadigm (Fernandez et al. 2012; Parent et al. 2013;Whitehead et al. 2013; Hautz et al. 2015). Frank et al. (2010)moved the field closer to a shared language with a seminalpaper that stemmed from the first summit of theInternational Competency-based Medical Education (CBME)Collaborators. However, since that paper’s publication, newterms have arisen in the field that not only suffer from a
lack of clear and common definitions but also create confu-sion between old and new terms. At the second summit ofthe International CBME Collaborators in 2013, participantssought to build on Frank et al.’s (2010) previous work, andon other papers that appeared in the literature since thatpublication, by working toward a shared understanding ofthe emerging concepts of milestones and entrustable pro-fessional activities (EPAs) (ten Cate 2013; Orgill & Simpson2014). This paper presents the work of the Collaborators indeveloping common definitions and attempts to identifythe relationships between EPAs, competencies, and mile-stones. It is hoped that this will be of help to medical edu-cators as they move toward the shared language sonecessary for this adaptive change in medical education.
Defining milestones
The concept of milestones has gained significant attentionin medical education, initially as a result of the Milestones
Practice points� A shared language to describe CBME will support
collaboration and help move the field forward.� CBME curricula are planned using a combination
of EPA, competencies and milestones.� A milestone is an observable marker of an individ-
ual’s ability that expresses the stepwise progres-sion of expertise.
� An EPA is a professional task that requires suffi-cient knowledge, skills, and attitudes and leads toa work outcome.
CONTACT Robert Englander [email protected] School of Medicine, University of Minnesota, 420 Delaware St SE, MMC 293, Minneapolis, MN 55455,USA� 2017 Informa UK Limited, trading as Taylor & Francis Group
MEDICAL TEACHER, 2017VOL. 39, NO. 6, 582–587http://dx.doi.org/10.1080/0142159X.2017.1315066
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017

Project of the Accreditation Council for Graduate MedicalEducation (ACGME). This project required each of the spe-cialties to define the “milestones” that during the course ofgraduate training marked advancement toward theachievement of the global competencies required forunsupervised practice (ACGME 2013). The CanMEDS 2015Framework of the Royal College of Physicians and Surgeonsof Canada is also focused on developmental milestones formedical training as part of its next iteration (Frank et al.2015). However, in European medical education the notionof a milestone is frequently described in different and“larger” terms than in current discourse in the UnitedStates or Canada. Therefore, the International CBMECollaborators debated a common definition that couldaccommodate multiple frameworks and contexts. The fol-lowing consensus definition emerged:
Milestone: A defined, observable marker of an individual’s abilityalong a developmental continuum.
This definition articulates the concept of an educationalmilestone as an explicit statement of the stepwise progres-sion of expertise that can be observed and assessed. Thisreflects the CBME construct of competencies – the abilitiesof a professional – as having a spectrum of developmentfrom novice to expert. This definition is both accurate andbroad enough to encompass the considerable variation inhow the concept of “milestones” has been operationalizedin medical education. The relationship of milestones toEPAs and competencies is discussed below.
Defining EPAs
In 2005, ten Cate (2005) first introduced the concept ofEPAs as a practical framework for implementing a compe-tency-based system of education. Subsequently, ten Cateand Scheele (2007) further described the concept using thespecialty of obstetrics and gynecology as an example. Sincethat time, a number of authors have described the imple-mentation of the concept, usually with one or two EPAs,and often with varying definitions or interpretations of thedefinition (Mulder et al. 2010; Hauer et al. 2013). Critical tothe definition of EPAs are the following features, as out-lined in the seminal papers of ten Cate and Scheele (tenCate 2005; ten Cate & Scheele 2007). An EPA:
� is part of essential professional work in a given context� requires adequate knowledge, skills, and attitudes� leads to recognized output of professional labor
In addition, ten Cate and Scheele delineated features ofEPAs that are ideal but not required. These include thatEPAs should:
� be confined to qualified personnel� be independently executable� be executable within a time frame� be observable and measurable in its process and out-
come (done well or not done well)� reflect one or more competencies (see “The relationship
between EPAs, competencies and milestones,” below)
On the basis of this work and the literature that hasdeveloped since, the International CBME Collaborators
developed the following consensus definition in the con-text of medical training:
Entrustable professional activity (EPA): An essential task of adiscipline (profession, specialty, or subspecialty) that anindividual can be trusted to perform without direct supervisionin a given health care context, once sufficient competence hasbeen demonstrated.
For an individual who has completed training and isentering practice, EPAs are tasks that he or she is trustedby society and the profession to perform withoutsupervision.
It follows, then, that a discipline, specialty, or health careprofession would have a set of EPAs that reflects the rele-vant scope of practice. To this end, comprehensive listshave been implemented to date for physician assistants inthe Netherlands (Mulder et al. 2010), obstetricians andgynecologists in the Netherlands (ten Cate & Scheele 2007),and psychiatrists in Australia and New Zealand (RANZCP2013).
Two additional terms are emerging in the literature as aresult of the EPA concept: “nested EPA” and “statement ofawarded responsibility (STAR).” The concept of a nestedEPA is relatively new and underdeveloped in the literature.The following working definition emerged from the post-summit work of the ICBME Collaborators:
Nested EPA: A task that requires proficiency in a subset of theknowledge, skills, and attitudes required for the broader EPA.The expectation for entrustment with the performance of anested task occurs at an earlier stage of the developmentaltrajectory than entrustment with the entire task. A nested EPApossesses the elements of its “parent” EPA; that is, it requiresthe integration of knowledge, skills, and attitudes; it isindependently executable within a given time frame byqualified personnel; and it leads to observable and measurableoutputs. An example of a nested EPA might be “understandingthe indications for and performing a caesarian section,” whichis a nested in the “parent” EPA “managing complicatedchildbirth”. (van Loon et al. 2014).
The related concept of a statement of awarded responsi-bility (STAR) was first introduced by ten Cate and Scheele(2007). Their original conceptualization has been modifiedin light of the work of Epstein and Hundert (2002) to givethe following definition:
Statement of awarded responsibility (STAR): A formal recognitionof the specific point at which entrustment for an EPA isgranted. STARs require supervisors to make deliberate decisionsover time about their trainees’ competence to perform allcritical activities for that EPA. The specific and formalimplications of a STAR differ from those of any evaluations thathave been the backbone of trainee performancedocumentation to date, in that a STAR allows the learner toperform the corresponding EPA without supervision. As a result,it bears a closer resemblance to a certification than anassessment or evaluation.
Other emerging terms in CBME
A number of other terms in the CBME literature haveemerged, especially in connection with the work of creat-ing technical standards for the electronic transfer of infor-mation that relates to EPAs, competencies, and milestones– as in an online portfolio (Willet 2012). These termsinclude competency benchmark, competency framework, and
MEDICAL TEACHER 583
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017

domain of competence. Working definitions for all of theterms related to CBME are given in Table 1.
The relationship between EPAs, competencies, andmilestones
The relationship between EPAs and competencies has beendelineated in the literature. EPAs are units of work, whereascompetencies are the abilities of individuals. One of thedefining markers of an EPA is that it requires the integra-tion of multiple competencies, usually across domains ofcompetence. For example, an EPA may incorporate specificcompetencies within the domains of patient care, medicalknowledge, and interpersonal and communication skills(using the ACGME framework), or specific competencies inthe roles of medical expert and health advocate (using theCanMEDS framework).
The authors recognize that the distinctions betweenEPAs and competencies are not always sharp. For example,“work in interprofessional teams to enhance patient safetyand improve patient care quality” is a competency withinthe ACGME framework, while one of the AAMC’s core EPAsfor entering residency is “collaborate as a member of aninterprofessional team” (AAMC 2013) The distinction is fur-ther muddied by the lack of consensus regarding the“sizing” of EPAs. The literature has included EPAs as “small”as performing a lumbar puncture and as “large” as manag-ing a common chronic disease in the outpatient setting(ten Cate 2013).
Nevertheless, EPAs and competencies complement eachother. Together, they provide a more holistic view of aphysician than either could provide independently. Appliedalone, constructs of competency can result in definitions ofthe physician’s role that are either so abstract or so
Table 1. International CBME Collaborators glossary of terms for competency-based medical education.
CompetencyCompetenceThe array of abilities (knowledge, skills, and attitudes) across multiple domains or aspects of performance in a certain context. Statements about competencerequire descriptive qualifiers to define the relevant abilities, context, and stage of training. Competence is multi-dimensional and dynamic. It changes withtime, experience, and setting. (Frank et al. 2010)
CompetencyAn observable ability of a health professional related to a specific activity that integrates knowledge, skills, values, and attitudes. Since competencies areobservable, they can be measured and assessed to ensure their acquisition. Competencies can be assembled like building blocks to facilitate progressivedevelopment. (Frank et al. 2010)
Competency-based medical educationAn outcomes-based approach to the design, implementation, assessment, and evaluation of medical education programs, using an organizing framework ofcompetencies. (Frank et al. 2010)
Competency benchmarkExpected performance level for a cohort of learners at a given point in education, training, or practice. (Willet 2012)
Competency frameworkAn organized and structured representation of a set of interrelated and purposeful competencies. (Willet 2012)
CompetentPossessing the minimum required abilities in all domains in a certain context at a defined stage of medical education, training, or practice. (Frank et al.2010)
Domains of competenceBroad, distinguishable areas of competence that in the aggregate constitute a general descriptive framework for a profession, such as the six domains ofcompetence described by the ACGME (Patient Care, Medical Knowledge, Professionalism, Interpersonal and Communication Skills, Systems-Based Practice,and Practice-Based Learning and Improvement) or the seven CanMEDS roles (Medical Expert, Professional, Communicator, Collaborator, Leader, HealthAdvocate, and Scholar). (Englander et al. 2013)
DyscompetencePossessing relatively less ability in one or more domains of health professional competence in a certain context and at a defined stage of education or prac-tice. (Frank et al. 2010)
IncompetentLacking the required abilities to carry out a context-specific task at the predetermined performance level for a defined stage of medical education, training,or practice.
Entrustable professional activitiesEntrustable professional activity: An essential task of a discipline (profession, specialty, or subspecialty) that a learner can be trusted to perform without directsupervision and an individual entering practice can perform unsupervised in a given health care context, once sufficient competence has been demon-strated.
Nested EPA: A nested EPA is a task unit that represents a foundational subset of the KSA required for the broader EPA. As a building block for the broaderEPA, the expectation for entrustment occurs at an earlier stage of the developmental trajectory. A nested EPA possesses the elements of its “parent” EPA(requires the integration of knowledge, skills and attitudes; is independently executable within a given timeframe by qualified personnel; and leads toobservable and measurable outputs).
Statement of Awarded Responsibility (STAR): A STAR is a formal recognition of the specific point at which entrustment for an EPA has been granted. STARsrequire supervisors to make deliberate decisions over time about their trainees’ competence to perform all critical activities for that EPA.
MilestonesMilestone: A defined, observable marker of an individual’s ability along a developmental continuum.
584 R. ENGLANDER ET AL.
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017

atomized as to become meaningless to supervisors andlearners in the real-world contexts of care delivery. Further,assessment systems based solely on competencieswithout explicit reference to the element of trust can pro-vide a somewhat artificial lens through which to viewgraded responsibilities. EPAs balance this limitation of thecompetency model by outlining, with high face validity, thespectrum of the health professional’s actual work. They pro-vide a useful structure for work-based assessment and forthe progression by which increasing responsibility is givento the learner. However, a competency framework remainsessential; without a mapping of the competencies requiredfor entrustment, assessors will lack a shared mental modelof what constitutes readiness for an EPA. Moreover, withouta competency framework to describe the complete spec-trum of necessary physician abilities, the result might be anuneven or overly technical view of the physician – that is, adefinition based solely on his or her work or output – andthus potentially ignore many of the specific abilitiesrequired of the twenty-first century physician, such as pro-fessionalism and advocacy.
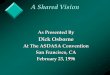
The relationship of EPAs and competencies to milestonesis a bit more confusing, since at least two models – one pri-marily in the US and one in Europe – are in use. Figure 1depicts the prevailing relationship between EPAs, domains ofcompetence, competencies, and milestones as applied in theUnited States. Each EPA can be linked or “mapped” to one ormore domains of competence and one or more competen-cies in each domain. Theoretically, EPAs can be mapped tomany competencies, but only a critical few of those compe-tencies are required to reach an entrustment decision.Through its Milestones Project, the ACGME charged each
specialty with developing milestones that marked thedevelopmental progression for a specific competency.Therefore, in the US framework, a milestone is a smallerconstruct than a competency and represents behaviorsassociated with a specific level of achievement for thatcompetency.
In Europe, milestones are conceptualized in some set-tings as considerably “bigger” than the EPAs or compe-tencies, such that a milestone is a marker of theachievement of a cluster of competencies or EPAs thatallows one to move, for example, from junior to seniorresidency. One can envision in this model a series ofEPAs or competencies required for each major transition(pre-clinical to clinical years, medical school to residency,junior to senior residency, and senior residency to prac-tice). The milestone, then, is the marker of achievementof all of the requirements for the transition from onestage of training to another. Figure 2 depicts the rela-tionship between milestones and EPAs in this model,and Figure 3 depicts the relationship between mile-stones and competencies in this model. These modelsare not mutually exclusive, as some institutions havecreated a hybrid model in which the attainment of cer-tain competencies and EPAs together make up the“milestone” that marks a transition point in education ortraining. Regardless of which approach is preferred, thedefinitions of EPAs and milestones discussed above arestill applicable.
The existence of such hybrid models reinforces theneed for clear definitions and a shared language for EPAs,milestones, and competencies. Accreditation requirementsare being revised to include all aspects of competency-based curriculum and assessment; some accreditationbodies have already included milestones terminology intheir documents (ACGME 2013); EPAs are likely comingsoon. As training programs work to ensure that theirassessment processes will meet accreditation standards,consensus on the definitions of milestones and EPAs willmake the process smoother.
Milestone 1
Milestone 2
Milestone 3
EPAEPAEPA
EPAEPA EPA EPA
EPAEPA EPA EPA
EPAEPA EPA EPA
EPA EPA EPA
Time in training
EPAEPAEPA
Figure 2. A model of the relationship between EPAs and milestones in whicha series of EPAs in the aggregate make up the milestone. Note that progresstoward EPAs for the next milestone may begin before the first milestone isattained. EPA: entrustable professional activity.
M1M2MxM1M2MxM1M2MxM1M2Mx
M1M2Mx
M1M2Mx
M1M2MxM1M2MxM1M2Mx
M1M2MxM1M2Mx
Figure 1. Predominant model of the relationship between EPAs, domains ofcompetence, competencies and milestones in the United States. Each EPAmaps to two or more domains of competence and one or more competencieswithin the domain. Each competency has associated milestones. As depictedin the figure, EPAs may overlap with other EPAs both in the domains of com-petence and in the specific competencies critical for entrustment. EPA:entrustable professional activity; DOC: domain of competence; C: competency;M: milestone.
MEDICAL TEACHER 585
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017

Conclusion and next steps
Having defined the outcomes expected of a physicianthrough frameworks such as the ACGME competencies andCanMEDS, the medical education community is movinginto the next phase of CBME. This phase involves definingthe developmental progression, or milestones, required toachieve those outcomes and developing frameworks suchas EPAs for implementing the teaching and assessment ofcompetencies in both undergraduate and graduate medicaleducation. The ICBME Collaborators saw the transition intothis phase as an opportunity to reexamine the language ofCBME to ensure that the community proceeds on the“same page” with a shared language. As with any adaptivechange, further terms will likely emerge, and existing termswill require refinement, especially as innovations in medicaleducation continue to enrich the literature. TheInternational CBME Collaborators are committed to follow-ing this progression and updating the medical educationcommunity at large through scholarly publications to opti-mize the implementation of CBME worldwide.
Disclosure statement
The supplement coeditors and authors declare that they have no com-peting interests. Resources and secretariat support for this project wasprovided by the Royal College of Physicians and Surgeons of Canada.
Notes on contributors
Robert Englander, MD, is an Associate Dean for UndergraduateMedical Education University of Minnesota School of Medicine, USA.
Jason R. Frank, MD, is the Director, Specialty Education, Strategy andStandards in the Office of Specialty Education at the Royal College ofPhysicians and Surgeons of Canada, and the Director of EducationalResearch & Development in the Department of Emergency Medicine,University of Ottawa, Canada.
Carol Carraccio, MD, is the Vice President, Competency-BasedAssessment, American Board of Pediatrics, USA.
Jonathan Sherbino, MD, is an Associate Professor in the Department ofMedicine, McMaster University, and an Assistant Dean with Program forEducation Research and Development, McMaster University, Canada.
Shelley Ross, PhD, is an Associate Professor and Director of Researchand Innovation, Competency-Based Achievement System Program, in
the Department of Family Medicine, Faculty of Medicine & Dentistry,University of Alberta, Canada.
Linda Snell, MD, is a Professor of Medicine and Core Faculty member,Centre for Medical and Department of General Internal Medicine,McGill University, and Senior Clinician Educator, Royal College ofPhysicians and Surgeons of Canada, Canada.
ORCID
Shelley Ross http://orcid.org/0000-0001-9581-3191
References
Association of American Medical Colleges [AAMC]. 2013. Core entrusta-ble professional activities for entering residency [Internet]. [cited2013 Dec 30]. Available from: www.mededportal.org/icollaborative/resource/887Accreditation Council for Graduate Medical Education[ACGME]. 2013. Milestones 2013 [Internet]. [cited 2013 Nov25]. Available from: www.acgme.org/acgmeweb/tabid/430/ProgramandInstitutional Accreditation/NextAccreditationSystem/Milestones.aspx
Carraccio CL, Englander R. 2013. From Flexner to competencies:reflections on a decade and the journey ahead. Acad Med.88:1067–1073.
Englander R, Cameron T, Ballard AJ, Dodge J, Bull J, Aschenbrener CA.2013. Toward a common taxonomy of competency domains for thehealth professions and competencies for physicians. Acad Med.88:1088–1094.
Epstein RM, Hundert EM. 2002. Defining and assessing professionalcompetence. JAMA. 287:226–235.
Fernandez N, Dory V, Ste-Marie LG, Chaput M, Charlin B, Boucher A.2012. Varying conceptions of competence: an analysis of howhealth sciences educators define competence. Med Educ.46:357–365.
Flexner A. 1910. Medical education in the United States and Canada: areport to the Carnegie Foundation for the Advancement ofTeaching. New York: Carnegie Foundation for the Advancement ofTeaching.
Frank JR, Snell L, Sherbino J, editors. 2015. CanMEDS 2015 physiciancompetency framework. Ottawa: Royal College of Physicians andSurgeons of Canada.
Frank JR, Snell LS, ten Cate O, Holmboe ES, Carraccio C, Swing SR,Harris P, Glasgow NJ, Campbell C, Dath D, et al. 2010. Competency-based medical education: theory to practice. Med Teach.32:638–645.
Hauer KE, Soni K, Cornett P, Kohlwes J, Hollander H, Ranji SR, tenCate O, Widera E, Calton B, O’Sullivan PS. 2013. Developing entrust-able professional activities as the basis for assessment of compe-tence in an internal medicine residency: a feasibility study. J GenIntern Med. 29:1110–1114.
Hautz SC, Hautz WE, Feufel MA, Spies CD. 2015. Comparability of out-come frameworks in medical education: implications for frameworkdevelopment. Med Teach. 37:1051–1059.
Heifetz R, Linsky M, Grashow A. 2009. The practice of adaptive leader-ship: tools and tactics for changing your organization and theworld. Boston: Cambridge Leadership Associates.
Mulder H, ten Cate O, KReineke D, Berkvens J. 2010. Building a compe-tency-based workplace curriculum around entrustable professionalactivities: the case of physician assistant training. Med Teach.32:e453–e459.
Orgill BD, Simpson D. 2014. Toward a glossary of competency-basedmedical education terms. J Grad Med Educ. 6:203–206.
Parent F, Jouquan J, De Ketele JM. 2013. CanMEDS and other“competency and outcome-based approaches” in medical educa-tion: clarifying the ongoing ambiguity. Adv Health Sci Educ TheoryPract. 18:115–122.
Royal Australian & New Zealand College of Psychiatrists [RANZCP].2013. Entrustable professional activity forms [psychiatry] [Internet].[cited 2013 Nov 26]. Available from: www.ranzcp.org/Pre-Fellowship/2012-Fellowship-Program/Training-program-forms/EPA-forms.aspx.
Milestone 1
Milestone 2
Milestone 3
C1 C7C5C3
C6C4C2
C1 C7C5C3
C6C4C2
C1 C7C5C3
C6C4C2
Figure 3. A model of the relationship between competencies and milestonesin which a series of competencies in the aggregate make up the milestone.Note that progress toward competencies for the next milestone may beginbefore the first milestone is attained. C: competency.
586 R. ENGLANDER ET AL.
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017

ten Cate O, Scheele F. 2007. Competency-based postgraduate training:can we bridge the gap between theory and clinical practice? AcadMed. 82:542–547.
ten Cate O. 2005. Entrustability of professional activities and compe-tency-based training. Med Educ. 39:1176–1177.
ten Cate O. 2013. Nuts and bolts of entrustable professional activities.J Grad Med Educ. 5:157–158.
van Loon KA, Driessen EW, Teunissen PW, Scheele F. 2014. Experienceswith EPAs, potential benefits and pitfalls. Med Teach. 36:698–702.
Whitehead CR, Austin X, Hodges BD. 2013. Continuing the competencydebate: reflections on definitions and discourses. Adv Health SciEduc Theory Pract. 18:123–127.
Willet T. 2012. Performance framework definitions [Internet]. [cited2012 Dec 5]. Available from: http://groups.medbiq.org/medbiq/dis-play/CWG/PerformanceþFrameworkþ-þDefinitions
MEDICAL TEACHER 587
Dow
nloa
ded
by [
UN
AM
Ciu
dad
Uni
vers
itari
a] a
t 10:
48 2
5 Se
ptem
ber
2017
















![[Global HR Forum 2011] Conscious Capitalism : Toward Shared & Sustainable Growth](https://img.dokumen.tips/doc/110x75/5590df0d1a28ab39578b46ed/global-hr-forum-2011-conscious-capitalism-toward-shared-sustainable-growth.jpg)










