Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Medical complications and outcomes at an onsite rehabilitationunit for older people
M. Mulroy • L. O’Keeffe • D. Byrne •
D. Coakley • M. Casey • B. Walsh • J. Harbison •
C. Cunningham
Received: 10 March 2012 / Accepted: 11 February 2013 / Published online: 1 March 2013
� Royal Academy of Medicine in Ireland 2013
Abstract
Background The rehabilitation of older patients in
Ireland after an acute medical event occurs at dedicated
onsite hospital units or at offsite centres. Information on
medical complications and outcomes is inadequate.
Aims Enumeration of medical complications of patients
admitted to a dedicated onsite rehabilitation unit for older
people, and the extent of co-morbidity in the population
with the effects that this had on the evolution of medical
complications.
Methods A retrospective analysis of patients admitted to
a 58-bed onsite unit over a 1-year period was performed.
Information collating co-morbidities, medical complica-
tions and functional outcomes was recorded.
Results Medical complications occurred in almost 95 %
of patients, where full data were available. Over one-third
required intravenous therapy.
Conclusion Twenty-four hour medical cover is required
for older patients managed at onsite rehabilitation units.
Further studies on offsite medical rehabilitation facilities
for older patients are required.
Keywords Onsite rehabilitation � Offsite rehabilitation �Complications � Outcomes
Methods
A retrospective chart review of all patients admitted to a
58-bed rehabilitation facility on the general hospital
campus of St James’s Hospital took place over a 12-month
period (July 2004–June 2005) following examination of the
admission and discharge dates from the Hospital In Patient
(HIPE) records. The catchment area for the hospital has
approximately 25,000 people aged 65 and over reflecting
approximately 2.3 rehabilitation beds per thousand, but up
to 25 % of beds can be occupied by patients awaiting
transfer to nursing homes so the actual rate available for
rehabilitation is closer to 1.75 beds per thousand [1]. A
proforma which detailed the patients age, date of admission
to the rehabilitation unit, time pending rehabilitation bed,
length of stay, source of referral, and discharge location
was recorded. Activities of Daily Living (ADL’s) were
noted pre- and post-admission to the unit. The Cumulative
Illness Rating Scale for Geriatrics (CIRSG) was used to
measure co-morbidities and severity of chronic medical
disease burden prior to transfer to rehabilitation. The
CIRSG has been validated as a measure of complexity in
frail older patients [2]. Thirteen organ systems were scored,
each between 0 and 4, which graded the severity of illness
from none (0) to critical (4) [3]. The classes of medications
that patients were admitted with were detailed, but limited
to eleven categories. Complications were defined as
requiring medical attention by a Non-Consultant Hospital
Doctor (NCHD) or a consultant and required an entry into
the medical notes. The time to first complication and the
number of complications were recorded in organ-based
categories which also included falls, new fractures, bio-
chemical abnormalities and psychiatry of old age inter-
vention. If patients required transfer to the main hospital
for further medical care or radiological investigations;
this was noted. The use of intravenous drug therapy fol-
lowing complications was recorded. The discharge desti-
nation of the patient, documented overnight stays for
graded discharge, documented family meetings, number of
M. Mulroy (&) � L. O’Keeffe � D. Byrne � D. Coakley �M. Casey � B. Walsh � J. Harbison � C. Cunningham
Medel Directorate, St James Hospital, Dublin 8, Ireland
e-mail: [email protected]
123
Ir J Med Sci (2013) 182:499–502
DOI 10.1007/s11845-013-0922-1

medications and selected ADL’s were noted. Six NCHD’s
were recruited to complete the proforma and each had to
score a minimum number of charts for the CIRSG to
minimise interrater variability. All reviewers had training
from the principal author in the use of scoring guidelines
and a pilot score of 10 charts (not included in the study)
from the acute geriatric ward was used per reviewer.
Spearman’s correlation coefficient between the principal
authors’ scores and the other reviewers was 0.72.
Data were stored using a Microsoft Excel spreadsheet
and statistics were performed using Datadesk statistical
software (version 6 Ithaca, NY).
Results
One hundred and fifty-five patients were admitted to the
rehabilitation unit over 12 months (July 2004–June 2005).
Hospital charts were available for 140/155 (90.3 %) of
patients and full clinical data were available for 112/155
(72.2 %) of patients. Computer records were available for
155/155 (100 %). 89/155 were females (59 %). The mean
age of patients on admission was 80.16 years (range
62–97 years). The mean waiting time for a rehabilitation
bed was 38.5 days (range 0–196 days). The median length
of stay on the rehabilitation unit for patients was 83 days
(range 2–460 days). 79/155 (51 %) of patients were refer-
red from the General Physicians, 46/155 (30 %) were
referred from the Geriatricians, 20/155 (13 %) were refer-
red from the Orthopaedic Surgeons, 8/155 (5 %) were
referred from the General Surgeons and 2/155 (1 %) were
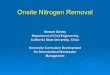
referred from the community. The indication for referral is
illustrated in Fig. 1. 125/155 (80.6 %) had one rehabilita-
tion admission, 24/155 (15.5 %) had two rehabilitation
admissions, 5/155 (3 %) had three rehabilitation admissions
and 1/155 (0.6 %) had four rehabilitation admissions over
12-month period.
The mean CIRSG was 8.1 (range 0–20). The mean Mini
Mental State Score was 22.9 prior to the patients’ transfer.
Of the patients with full data available, medical compli-
cations were found in 106/112 (94.6 %) of patients. The
median time to first medical complication was 7 days
(range 0–65 days). 13 % of all admissions required a
medical review within 48 h of admission. The total number
of discrete unscheduled medical reviews was 1,605 (mean
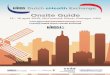
11.5 medical reviews per patient). A breakdown of organ-
specific complications is illustrated in Fig. 2.
Forty-two of 112 (38 %) required intravenous therapy
during their stay. 4/112 (3.6 %) patients had cardiorespi-
ratory arrests. 60/112 (53.5 %) required transfer for
radiological investigations. 20/112 (17.8 %) were trans-
ferred following an acute medical deterioration to the acute
geriatric ward. No patients required transfer to the emer-
gency department. In a multiple logistic regression looking
at age, gender, co-morbidity score, in-patient time waiting
for rehabilitation and in-patient mobility status prior to
transfer to rehabilitation only co-morbidity score was sig-
nificantly associated with subsequent use of intravenous
therapy (odds ratio 1.14 [95 % CI 1.03–1.27] for each point
increase in the CIRSG scale. Co-morbidity score was not
associated with inpatient mortality (odds ratio 1.07
[0.94–1.21] unadjusted and 1.08 [0.95–1.23] adjusted) or
rehabilitation length of stay (beta coefficient (s.e.) 1.48
(2.31) p = 0.52 unadjusted and 1.81 (2.28) p = 0.43
adjusted).
Fourteen of the 42 patients (33 %), who required
intravenous therapy died, 13(31 %) went to a nursing home
Stroke
Orthogeriatrics
Falls
Cardio/Chest
Others
Fig. 1 Indication for rehabilitation from source of referral: 17/112
(15 %) were stroke, 20/112 (17.8 %) were orthogeriatric/orthopaedic,
24/112 (21.4 %) were Falls, 9/112 (8 %) were cardio-respiratory,
42/112 (37.5 %) were combinations of the previous categories and
others
0
100
200
300
400
500
1
GIT/GUT
Skin
CVS
RS
Psych
RheumBiochem
Neuro
Fluid Imbalance
Injurious Fall
New Fracture
Fig. 2 Total cumulative complications recorded for 112/155 patients.
The most common complication involved gastrointestinal/genitour-
inary system 402/1,605, followed by skin 280/1,605, cardiovascular
188/1,605, respiratory 182/1,605, psychiatry 152/1,605, rheumato-
logical 101/1,605, biochemical 100/1,605, neurological 100/1,605,
fluid imbalance 49/1,605, injurious fall 44/1,605, and new fracture
7/1,605
500 Ir J Med Sci
123

and 15 (36 %) were discharged to the community. These
outcomes were significantly different (v2 = 32, 2df,
p \ 0.0001) for the 70 patients who did not require intra-
venous therapy during their stay: no deaths (0 %),
15(21 %) discharged to nursing homes and 55(79 %) dis-
charged to the community.
With regard to outcomes, computerised records of dis-
charge destination in all patients admitted were available.
96/155 (62.2 %) were discharged home, 33/155 (21 %)
were discharged to a long-term care facility, 6/155
(4 %) were transferred to another hospital, and 20/155
(12.6 %) died. Of the 96 patients discharged home, 37
(39 %) had documented overnight stays prior to discharge,
and 44 (45 %) had documented family meetings to facilitate
this with the multidisciplinary team. The median quantity of
medications following discharge increased from eight
medications (range 2–20) prior to admission to 11 medica-
tions (range 2–20) following discharge. Table 1 illustrates
selected groups of medications prescribed pre- and post-
rehabilitation.
Of those patients discharged from rehabilitation, 74/92
(80.4 %) were continent, 15/92 (16.3 %) were incontinent
with 3/92 (3.2 %) requiring long-term catheterisation.
Prior to admission to the acute hospital 89/112 (79 %)
were independent mobile (with or without an appliance),
but this had fallen to only 34/112 (30 %) preceding transfer
to the rehabilitation unit. At discharge, 79/112 (70 %) were
independently mobile (with or without an appliance).
Discussion
This represents the first data from an Irish onsite rehabili-
tation unit for older people which demonstrated that
patients had significant medical co-morbidity but most
returned home. Following listing for rehabilitation, patients
waited almost a month prior to transfer, reflecting a lack of
appropriate beds.
The management of older patients requiring rehabilita-
tion after an acute medical illness can be complex due to
the nature of the acute medical problem and the presence of
co-morbidities. There has been significant debate where
older patients requiring such rehabilitation should take
place. A recent review and meta-analysis of inpatient
rehabilitation has shown an increased level of function and
reduced mortality and admissions to nursing homes in such
patients [4]. In North America, the term ‘‘prehab’’ has been
used to describe intensive rehabilitation at the front door
when older patients are admitted to acute geriatric care
units. These units report similar findings to the inpatient
rehabilitation model with improved outcomes and reduced
placement into long-term care facilities [5]. The effect of
an acute geriatric unit, as well as standard management
units in Europe, has also reported similar outcomes [6, 7].
The models for providing rehabilitation for older people
in community or at off-campus sites are established in
Ireland. In the United Kingdom, nurse-led intermediate
care rehabilitation units have reported no significant
adverse outcomes to patients and comparable levels of
physical function [8]. In 2008, a Cochrane database review
found insufficient evidence of overall outcomes when
comparing rehabilitation of older patients in either their
own home, nursing home or in hospital [9]. The cost of
providing such diverse rehabilitation given the differing
casemix of pathologies treated is difficult to enumerate.
Where the sole provision of rehabilitation is for example
stroke, early discharge from the acute setting to provide
rehabilitation in the home setting can be cost-effective
without any adverse changes in mortality [10].
Almost all patients admitted to the inpatient rehabilita-
tion service at our hospital developed a medical compli-
cation requiring the minimum intervention of a medical
review, 13 % of which was required within 48 h of
admission. The nature of these complications was multi-
organ, and were treated by Geriatricians. Over the half of
the patients reviewed required radiological investigations
and 38 % required intravenous intervention for either fluids
or medications. Requiring intravenous treatment was
associated with significantly worse outcomes. The number
of medications prescribed increased by about three per
patient. Although the use of bone protection medications
and statins increased, the number being prescribed ben-
zodiazeopines failed to reduce and indeed increased (albeit
in 4 patients). Our unit’s failure to reduce the use of
sleeping tablets reflects the difficulty of implementing
guidelines into practice and may indicate a difficulty in
addressing this topic in older inpatients that proceed to
rehabilitation. Further research should address this area.
The average length of stay of almost 3 months, the sig-
nificant use of intravenous medications and radiological
investigations on the unit may reflect the experiences of
other onsite or offsite centres or may be profoundly dif-
ferent. It is important that other units publish their expe-
riences to inform a debate about the most efficient use of
scarce resources.
This study highlights the importance of patients having
access to medical care in a rehabilitation facility due to the
Table 1 Selected classes of prescribed medications pre and post
admission to rehabilitation
Medications Pre-admission (%) Post-rehabilitation (%)
Statin 36/112 (32) 52/92 (56.5)
Bone protection 30/112 (26) 63/92 (68.4)
Benzodiazepenes 22/112 (19.6) 26/92 (28.2)
Ir J Med Sci 501
123

incidence of medical complications. Patrick et al. [11]
previously described medical co-morbidities as a predictor
of rehabilitation efficiency whereby scores [5 were likely
to result in a poorer outcome from rehabilitation. It is likely
that our patients would have required medical care if it was
provided at an offsite location given that the mean CIRSG
was 8.1. It also highlights the amount of bed days lost by
not having timely access to rehabilitation beds (5,503 bed
days per annum in this sample). With a higher burden of
co-morbidities, rapid transfer to the acute care unit within
the hospital, with access to radiological investigations is
essential to avoid busy emergency departments. This model
works well for onsite campus rehabilitation where patient
complexity at a tertiary hospital level is high, however,
further Irish studies comparing this to an offsite rehabili-
tation unit will be required for the future. It is noteworthy
that while patients significantly increased their mobility
while on the rehabilitation ward that most failed to attain
their pre-hospital admission mobility. Further research into
rehabilitation in this frail inpatient group is warranted.
There were some limitations to the study. The study
refers to a period of 8 years ago although the unit remains
similar in terms of size, therapy staff numbers and
assessment practices. Several patients had more than one
medical chart and some charts were unavailable. Full
clinical data were found on 112/155 patients with limited
data on a further 28/155. Computerised data on all patients
located admission to different departments and their dis-
charge destination; however, discharge summaries would
give insufficient data to score CIRSG in these patients,
let alone individual complications given the median length
of stay of 83 days. Barthel scores were not collated as the
study examined medical complications only. The Func-
tional Independent Scale was not used as an outcome
measure and further studies should consider use of such
standardised scales. A full admission list of medications
was available, but only classes of medications on discharge
were recorded during this study.
Conclusion
Irish data on inpatient rehabilitation of older people’s
complications and outcomes are scarce. Onsite campus
rehabilitation of older patients requires 24 h medical cover
to diagnose and treat potential complications. Access to
diagnostics and the ability to treat with intravenous fluids
and medications are essential. Further studies are required
to compare the incidence of complications and outcomes at
rehabilitation facilities that are offsite. Economic evalua-
tive techniques need to explore which site offers the best
cost–benefit valuation although this would be limited given
the spectrum of indications for rehabilitation as well as the
co-morbidities of patients presenting. Better and timelier
access to rehabilitation would be associated with signifi-
cant bed-day savings for acute hospitals.
Conflict of interest None.
References
1. Walsh JB, Coakley D, Murphy C, Coakley JD, Boyle E, Johnson
H (2004) Demographic profile of the elderly population in Dublin
accident and emergency hospital catchment areas. Ir Med J
97(3):84–86
2. Parmelee PA, Thuras PD, Katz IR, Lawton MP (1995) Validation
of the cumulative illness rating scale in a geriatric residential
population. J Am Geriatr Soc 43:130–137
3. Linn BS, Linn MW, Gurel L (1968) The cumulative illness rating
scale. J Am Geriatr Soc 16:622–626
4. Bachmann S, Finger C, Huss A, Egger M, Stuck AE, Clough-
Gorr KM (2010) Inpatient rehabilitation specifically designed for
geriatric patients—a systematic review and meta-analysis of
randomised controlled trials. BMJ 340: c1718
5. Ahmed N, Pearce S (2010) Acute care of the elderly—a literature
review. Popul Health Manag 13(4):219–225
6. Baztan J, Suarez Garcia FM, Lopez Arriea J, Rodriguez-Manas L,
Rodriguez-Artalej F. Effectiveness of acute geriatric units on
functional decline, living at home, and case fatality amongst older
patients admitted to hospital for acute medical disorders : meta-
analysis. BMJ 338: 650
7. Van Craen K, Braes T, Wellens N, Denhaerynk K, Flamaing J,
Moons P, Boonens S, Gosset C, Petermans J, Milisen K (2009)
The effectiveness of inpatient geriatric evaluation and manage-
ment units: a systematic review and meta-analysis. J Am Geriatr
Soc 58 (1) 83–92
8. Griffiths P, Edwards M, Forbes A, Harris R (2005) Post acute
intermediate care in nursing led units: a systematic review of
effectiveness. Int J Nurs Stud 42(1):107–116
9. Ward D, Severs M, Dean T, Brook N (2008) Care home versus
hospital and own home environment for rehabilitation of older
people. Cochrane Database Syst Rev 4: CD 003164
10. Anderson C, NiMhurchu C, Brown PM, Carter K (2002) Stroke
rehabilitation services to accelerate discharge and provide
homebased care—an overview and cost analysis. Pharmacoeco-
nomics 20(8):537–552
11. Patrick L, Psych C, Knoefel F, Gaskowski P, Rexroth D (2001)
Medical comorbidity and rehabilitation efficiency in geriatric
inpatients. J Am Geriatr Soc 49:1471–1477
502 Ir J Med Sci
123