Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 171-177
Measurement of involuntary arm movement inathetotic patients
PETER D. NEILSON1
From the Division of Neurology, The Prince Henry Hospital, and the Schoolsof Medicine and Physics, University ofNew South Wales, Sydney, Australia
SYNOPSIS Visual tracking tests have been used to obtain a quantified statistical description of theinvoluntary movements of the arm about the elbow joint in a group of patients suffering fromathetoid cerebral palsy. Three separate components of involuntary activity can be recognized and itis possible that each may be a different physiological mechanism. First there are irregular movementswhich are represented by a continuous power spectrum which decreases with increasing frequency,reaching a negligible value between 2-3 Hz. The second component is a rhythmical low frequencymovement which is indicated by a predominant peak in the power spectrum at a frequency of 03-0-6 Hz. The presence of this peak was predicted in a previous paper because of underdampingdemonstrated in the closed loop voluntary control ofmovement in athetosis. The third component isthe athetoid action tremor in which both agonist and antagonist muscle groups contract vigorouslybut asynchronously at a frequency of 1 *54 Hz.
Athetosis has been described as a disorder of thecentral nervous system which is manifestedclinically by involuntary movements which lackfixed amplitude, rhythmicity, or direction(Koven and Lamm, 1954). Athetoid movementsare typically more severe in the upper limbs andinvolve the skeletal musculature of the distalparts more severely than the proximal (Bucy,1942). The disorder may involve the muscles ofarticulation, the face or neck, one extremity,both extremities of one side, both arms, or thetrunk (Putnam, 1939). These involuntary move-ments are known to be extremely variable (Herz,1931) and are very difficult to quantify. Theyhave been studied by a number of workers, par-ticularly Foerster (1921), Wilson (1925), andHerz (1931). Herz documented his analysis withmotion pictures. After studying the films heconcluded that athetoid movement contains nosynergistic coordinated activity nor is there aregular sequence of movement. Similarities withthe actions of grasping (Berger, 1903), pianoplaying, or relinquishing an object (Wilson,I Address for reprints: Clinical Sciences Building, The Prince HenryHospital, Little Bay, N.S.W., Australia.
171
1925) have been noted. The movements havebeen described as vermicular, cramplike, spas-modic, and writhing.
Description of the involuntary movement isconsidered important in both the diagnosis andclassification of athetosis. For example, theAmerican Academy for Cerebral Palsy accepts aclassification of cerebral palsy based on motorsymptomatology. Athetosis is classified into 12sub-groups based on a qualitative description ofthe involuntary movements (Minear, 1956;Phelps, 1956). The importance of classificationin athetosis was pointed out by Phelps (1956)with regard to selection of the treatment pro-gramme most appropriate for an individualpatient. Such a system of classification, how-ever, can be no better than the clinician's abilityto describe the involuntary movements. Descrip-tions based solely on inspection of the patient areprobably of doubtful reliability. For example,some authors describe the movements as mono-tonous (Jakob, 1925), while others emphasizethe variability (Herz, 1931); some authorsdescribe them as rhythmical (Lewandowsky,1910), while others say they are not rhythmical
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Peter D. Neilsont
(Bostroem, 1939; Koven and Lamm, 1954).Furthermore, precise information about speed,range, and power of involuntary movement islost in gross descriptive terms such as flailing,writhing, etc.
Before the introduction of the term athetosisby Hammond (1871) almost all abnormal in-voluntary activity was described as chorea (Herz,1944). The separation of chorea and athetosiswas initially criticized but it has proved to be ofclinical value and is retained by modern authors.
Analysis of motion pictures showed thatathetoid patients can display quick, jerky move-ments similar to those in chorea. This gives riseto the more inclusive term choreoathetosis.The electromyogram (EMG) from athetoid
muscles shows an asynchronous discharge ofmotor units resembling normal voluntary in-nervation but the opposing muscles do not relax(Putnam, 1939). The peculiar character ofathetoid movement is caused by lack of recipro-cal inhibition (Hoefer and Putnam, 1940).
Several types of involuntary activity have beenobserved in the EMG from athetoid muscle(Lindsley, 1936). In some patients there areslow squirming movements of the dystonic typeinvolving whole groups of muscles, in otherpatients there are oscillations of the limb causedby a series of clonic contractions which persistfor a few seconds at a time.
Lindsley (1936) and Hoefer and Putnam (1940)observed grouping of the impulses in the EMGfrom all cases. The frequency of the groupingsvaries from 2 to 11 volleys per second. They alsodescribed an oscillation of the limb resemblingthe tremor of Parkinson's disease. Hoefer andPutnam (1940) claimed that tremor coexists withthe choreoathetotic movement and that tremoris not a symptom of athetosis in its pure form.This view is supported by the observation thattremor has been seen to persist, while athetosishas been reduced by anterolateral spinal cordo-tomy (Putnam, 1933).A quantified description of athetoid movement
is required for both clinical and research pur-poses. For example, after a 12 year programmeof assessment of relaxant drugs in cerebral palsy,Denhoff and Holden (1961) concluded that thereis an urgent need to use more objective measuresto evaluate drug effectiveness.A recent study of voluntary control of move-
ment in athetosis (Neilson, 1974) suggests amethod by which involuntary movements may bequantified. The method is attractive because itprovides a statistical description of the athetoidmovements made during voluntary activity. Thisallows the possibility of investigating the inter-action between voluntary and involuntaryactivity. Involuntary movements usually subsidein sleep and some patients show practically noinvoluntary activity when they are in a restingstate (Koven and Lamm, 1954; Twitchell, 1961).During voluntary activity, however, athetoidmovement appears, causing an increase inenergy output, sweating and a marked rise inbasal metabolism (Putnam, 1939). In severecases purposive motion can be completely dis-rupted by athetoid activity.The purpose of the experiments explained
below is to provide a method of measurementand a quantified statistical description of in-voluntary arm movements about the elbow jointmade by athetotic patients while they are per-forming a sequence of voluntary arm move-ments.
METHOD
The method used for the tracking test was the sameas described previously (Neilson, 1973) and so willbe only briefly re-explained.The patient sat watching an oscilloscope screen on
which he could move a horizontal line up and downby flexion-extension movements of the right armabout the elbow. A 100 flexion movement caused a10 mm upward deflection of the oscilloscope line. Asecond not so bright and slightly defocused line onthe screen was moved up and down in an irregularfashion by the experimenter. The task for the patientwas to keep the two lines superimposed on thescreen. The positions of both the target and elbow-angle lines on the screen were recorded on a 4 channelGrass polygraph. A 10 mm upward deflection ofeither line corresponded to a 5 mm upward deflec-tion of the appropriate polygraph pen. The electro-myogram (EMG) and integrated EMG (IEMG) ofthe biceps brachii muscle were also recorded on thepolygraph. The time constant of the filter in theintegrator was adjusted to 0-16 sec. The EMG fromboth biceps and triceps muscles were amplified anddisplayed on a 17 in. oscilloscope so they could bemonitored and checked for artefact throughout theexperiment. The results from 10 athetotic cerebralpalsied patients were analysed.
172
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Measurement of involuntary arm movement in athetotic patients
TECHNIQUE OF ANALYSIS In the previous study themathematical relationship between the target signaland that portion of the elbow-angle signal coherentwith the target signal was computed. The relation-ship was described graphically by plotting the gainand phase frequency response curves. Statisticaldescriptions of the target, IEMG, and elbow-anglesignals were obtained by computing the auto powerspectrum of each signal. With this knowledge theauto power spectra describing both the voluntaryand involuntary arm movements can be calculated.To obtain the voluntary movement spectrum thepower spectrum of the target signal is multiplied bythe square of the gain at each frequency. In mathem-atical terms the output power spectrum equals theinput power spectrum multiplied by the square of thetransfer function (Blackman and Tukey, 1958;Jenkins and Watts, 1968). By subtracting the powerspectrum of the voluntary movements from that ofthe total elbow-angle signal, the power spectrumdescribing the involuntary arm movements is ob-tained. The power spectra of both the voluntary andinvoluntary components of the IEMG signal arecomputed in the same way.The statement that the spectra describe the
voluntary and involuntary activity is not completelyaccurate. More correctly, the division is between thatcomponent of either the elbow-angle or IEMG signalthat is coherent with the target signal and thatcomponent which is incoherent. This separation,however, parallels very closely the division betweenvoluntary and involuntary activity. Furthermore,athetoid power spectra of elbow-angle and IEMGsignals contained a secondary peak which was notpresent in the power spectra from either spastic
ELBOW-ANGLE N
az5,4,!,ItIS2l! a U46iLw114 It I4 Oo030a413 qq%117i. X,qaGqo.I.45'aVa&J.V LV aTARGET
EMG
IEMG
patients or normal subjects (Neilson, 1972a, b, 1974).This peak was almost certainly caused by the in-voluntary activity of athetosis. Thus it seems reason-able that the incoherent power spectra of the elbow-angle and IEMG signals provide an objectivedescription of the involuntary activity.As described above the IEMG signal was ob-
tained by integrating the EMG signal with a timeconstant of 0-16 sec. The EMG signal was full waverectified and filtered by a single pole low pass filterwith a corner frequency of 1 Hz. Consequently, theIEMG power spectrum includes the high frequencyattenuation introduced by the filter. The IEMGpower spectrum can be corrected for this attenuationby multiplying by the square of the inverse character-istics of the integrating filter. Both the corrected anduncorrected power spectra of the involuntary IEMGactivity have been computed in this study.
RESULTS
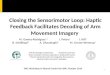
Polygraph recordings of target, elbow-angle,IEMG, and EMG signals were recorded duringthe visual tracking tests (Fig. 1). Inspection ofthe tracings shows fluctuations and oscillationsin the IEMG and elbow-angle signals which arenot correlated with the target signal. Thesefluctuations apparently represent the involuntaryactivity. The most striking feature in the poly-graph recordings is the pattern of bursts in theEMG and IEMG signals. It was present in bothflexor and extensor muscles whenever the patientwas voluntarily moving the arm but was absentwhen he was at rest. If the intervals between
FIG. 1. A typical page ofpolygraphtracings of elbow-angle, target, EMG,and IEMG signals recorded during avisual tracking test. Involuntary oscilla-tions and fluctuations can be seen in theelbow-angle signal and athetoid actiontremor can be seen clearly in both theEMG and IEMG tracings.
1 sWc
fI. lb -,q 3dtlV.l521:41 S1{l lb2a20 7 Qal543OV33iQZaa2 a2'7.l 1s ic,qx 1a71K1721 t5q J3l125.'1S,, it2 1t2I!lt
173
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Peter D. Neilson
bursts are measured during only a few seconds ofrecording one gets the impression that theactivity is rhythmical at a frequency of about2-5 Hz. Long-term recording, however, revealsthat both the amplitude and frequency of thebursts alter with time and that activity in oppos-ing muscle groups is poorly correlated. Theactivity is sometimes synchronous, sometimes
8A
ANGLE
2-
3-
1
4-
I:
asynchronous, and often the frequency of burst-ing is different in opposing muscle groups.
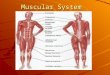
Using the technique of analysis explainedabove the power spectrum of the elbow anglesignal recorded during visual tracking wasdivided into voluntary and involuntary com-ponents (Fig. 2). Voluntary activity was greatestat low frequencies ( < 0-2 Hz) but decreased withincreasing frequency, becoming negligible by1-1 5 Hz. The power spectrum of the involuntarymovements started at intermediate levels ofpower at low frequencies, increased with fre-quency reaching a maximum between 0-3-0-6 Hz
IB
VOL
INVOL
FREQUENCY
FIG. 2. A. Auto power spectrum of the elbow-anglesignal recorded during a visual tracking test. B. Autopower spectrum of the component of the elbow-anglesignal that is coherent with the target signal. This isthe power spectrum of voluntary arm movement. Itdiminishes to a negligible value between 1-1J5 Hz.C. Auto power spectrum of the component of theelbow-angle signal that is incoherent with the targetsignal. This is approximately equivalent to the powerspectrum of the involuntary arm movement. Itdiminishes to a negligible value between 2-3 Hz andsometimes contains small secondary peaks at 1-5-3 Hzwhich are not present in this figure. In each spectrumpower is plotted in arbitrary units and frequency isplotted in Hz.
4
s 3
2
1
4
3a AIEMG
BVOL
1 2 3 4 5
C
. IVOL
2 3 4 5FREQUENCY
FIG. 3. A. Auto power spectrum of the IEMG signalrecorded during a visual tracking test. B. Power spec-trum of the component of the IEMG signal that iscoherent with the target signal. This is the powerspectrum of the voluntary component of the IEMGsignal. C. Power spectrum of the component of theIEMG signal that is incoherent with the target signal.In each spectrum power is plotted in arbitrary unitsandfrequency is plotted in Hz.
174
I
I
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Measurement of involuntary arm movement in athetotic patients
and then decreased again. Consequently therewas always a peak in the power spectra of theinvoluntary movements at a frequency 0-3-0-6Hz. Power diminished with increasing frequency,reaching a negligible value by 3Hz. Smallsecondary peaks could sometimes be seen at thehigher frequencies (I 5-3 Hz).A typical measure of power at 2 Hz was about
1-2 units (Fig. 2). This corresponds to anaverage amplitude of elbow-angle change ofabout 30 peak to peak. Individual oscillations at2 Hz were measured directly from the polygraphtracings with amplitudes as large as 100 peak topeak. This variation between the mean value andindividual measurements indicates that theamplitude of the elbow-angle oscillation at 2 Hzvaried with time. The amplitude of both theelbow-angle oscillation and the bursting in theEMG and IEMG signals could clearly be seen inthe polygraph recordings to change with time inan irregular fashion.The power spectrum of the IEMG signal was
also divided into voluntary and involuntarycomponents (Fig. 3). The voluntary IEMGspectrum had a large low frequency peak. Itdecreased with increasing frequency reaching anegligible value by 1-1-5 Hz. The involuntaryIEMG spectrum also had a large low frequencypeak but there was a secondarv peak as well(Fig. 3C). The secondary peak was caused by thebursting activity in the IEMG signal. The second-
8
6
4
2
11V G
1 2 3 4 5
FRECUEWCYFIG. 4. Auto power spectrum ofthe involuntary com-
ponent of the IEMG signal after it has been correctedfor the attenuation distortion introduced by the integra-ting filter. The large amplitude of the secondary peakemphasizes the magnitude of the athetoid actiontremor in the electromyogram. The broad base of thepeak indicates that the frequency of the tremor variesin the range 15-4 Hz.
ary peak was not sharply tuned as one mightexpect for rhythmiical bursting activity but wasbroad based and spread over a range of fre-quencies between 1 5-4 Hz. This is consistentwith the observation that the bursting frequencyvaried with time. The shape of the peak indicatesthat the frequency varied in the range 1 5-4 Hzwith a predominant frequency of about 2 5 Hz.A large amount of high frequency (>2 Hz)
IEMG activity was recorded and this is empha-sized by the large peak in the IEMG spectrumafter it has been corrected for the attenuationdistortion introduced by the integrating filter(Fig. 4). In spite of the magnitude of this activity,only very small elbow angle movements wererecorded at these frequencies and this is verifiedby the small power levels in the elbow-anglepower spectra (Fig. 2).
DISCUSSION
For the most part the fluctuations and oscilla-tions in the elbow-angle signal which cannot beseen in the target signal are caused by the in-voluntary movements of athetosis. The moststriking feature in the polygraph recording (Fig.1) is the occurrence of bursts ofEMG and IEMGactivity which may be seen in both agonist andantagonist muscle groups whenever the patientis active. Lindsley (1936) and Hoefer and Putnam(1940) described the grouping of impulses in theEMG as resembling the tremor of Parkinson'sdisease. The bursts of activity in athetosis, how-ever, are dissimilar to those of the tremor ofParkinson's disease in a number of respects(Andrews et al., 1973a). The broad base of thesecondary peak in the involuntary IEMG spec-trum (Fig. 4) indicates that the frequency of theEMG burst from biceps in an individual athetoticpatient varies over a wide range (1 5-4 Hz),whereas the tremor frequency in Parkinsonism isrelatively constant in any one patient in therange 3-7 Hz (Lance et al., 1963). In athetosistremor is not present at rest but appears duringvoluntary activity. In Parkinson's disease analternating tremor is present at rest and usuallydisappears during activity when it is replaced byan action tremor of higher frequency (10 Hz) inwhich the beats ofEMG activity are synchronousin antagonistic muscle pairs. In athetosis theEMG activity in opposing muscle groups is
175
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Peter D. Neilson
poorly correlated and the bursts may occur withdifferent frequencies in agonist and antagonist.These differences suggest that a neurologicalmechanism other than that causing the tremor ofParkinson's disease is operative and the termathetoid action tremor would seem appropriate.The results of this study oppose the view that
tremor is not a symptom of athetosis in its pureform (Hoefer and Putnam, 1940). In fact, it isargued that athetoid action tremor is one of themost outstanding features of athetosis. It is diffi-cult to observe athetoid action tremor by inspec-tion of the patient or by goniometric recordingbecause the movement is filtered out by the ab-normal mechanical load on muscle in athetosis(Neilson, 1974).
Putnam's finding that tremor and involuntarywrithing movement can be altered independentlyby anterolateral spinal cordotomy does notimply that tremor is an entity separate from theathetotic syndrome but could indicate that theyare generated by different neurological mechan-isms.Apart from athetoid action tremor two other
components of involuntary activity are revealedby the power spectrum of the involuntary elbow-angle movement. There is a continuous distribu-tion of power across the low frequency band(< 3 Hz) which indicates irregular low frequencyinvoluntary movement. As already discussed, thefalling off of the power spectrum towards 3 Hz iscaused by mechanical filtering. Mixed with theirregular movement is a very low frequency (0-3-06 Hz) rhythmical component which is indicatedby a predominant peak in the involuntary elbow-angle power spectrum (Fig. 3C). Again, thisrhythmical component is difficult to observe onclinical examination of the patient because it ismasked by irregular movement. The relativeflatness of the elbow-angle power spectrum (Fig.3A) illustrates this masking effect. The presenceof the low frequency rhythmical component waspredicted in a previous paper (Neilson, 1974)because of underdamping measured in thevoluntary control of movement in athetosis. Thisfinding suggests that the low frequency (0-3-0-6Hz) rhythmical movement is a transient responseof the closed loop voluntary control systemexcited by rapid voluntary movement. This find-ing indicates that at least two neurological
mechanisms probably contribute to the low fre-quency involuntary movement of athetosis.
In conclusion, a statistical description ofinvoluntary activity in the biceps muscle ofathetotic patients indicates at least three separatecomponents each of which may be caused by adifferent physiological mechanism. There are lowfrequency irregular movements which are obvi-ous on clinical examination and are commonlyrecognized as athetosis. This activity is probablygenerated in supraspinal centres (Bucy, 1942) andPutnam (1936) claims that it can be eliminated bysection of extrapyramidal tracts in the antero-lateral quadrant of the spinal cord. There is alsoan athetoid action tremor at about 2-5 Hz whichcan be seen most clearly in the electromyogram.It is quite unlike the tremor of Parkinson'sdisease and is only present when the patient isvoluntarily active. In addition, there is a lowfrequency rhythmical component caused by anabnormal underdamping measured previously inthe closed loop voluntary control of elbowposition.
I am most grateful to Associate Professor J. W.Lance and Professor E. P. George for their supportand encouragement and the Spastic Centre of NewSouth Wales for Centre Industries ResearchScholarship. The diagrams were photographed bythe Department of Medical Illustration, Universityof New South Wales.
REFERENCES
Andrews, C. J., Burke, D., and Lance, J. W. (1973a). Thecomparison of tremors in normal, parkinsonian andathetotic man. Journal of Neurological Science. (In press.)
Andrews, C. J., Neilson, P. D., and Knowles, L. (1973b).Electromyographic study ofthe rigidospasticity ofathetosis.Journal ofNeurology, Neurosurgery, and Psychiatry, 36, 94-103.
Berger, A. (1903). Zur Kenntnis der Athetose. Jahrbiichfur Psychiatrie und Neurologie, 23, 214-233.
Blackman, R. B., and Tukey, J. W. (1958). The MeasurementofPower Spectra. Dover Publications: New York.
Bostroem, A. (1939). Krankheiten des extrapyramidalenSystems. In Handbuch der Inneren Medizin, 3rd edn. Vol. 5,Part 1, pp. 668-710. Edited by G. V. Bergmann andR. Staehelin. Springer: Berlin.
Bucy, P. C. (1942). Neural mechanisms of athetosis andtremor. Journal of Neuropathology, 1, 224-239.
Denhoff, E., and Holden, R. H. (1961). Relaxant drugs incerebral palsy: 1949-1960. New England Journal ofMedicine, 264, 475-480.
Foerster, 0. (1921). Zur Analyse und Pathophysiologie derstriaren Bewegungsstorungen. Zeitschrift fiur die gesamteNeurologie und Psychiatrie, 73, 1-169.
Hammond, W. A. (1871). A Treatise on Diseases of theNervous System, pp. 654-662. Appleton: New York.
176
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from

Measurement of involuntary arm movement in athetotic patients
Herz, E. (1931). Die amyostatischen Unruheerscheinungen.Klinischkinematographische Analyse ihrer Kennzeichenund Begleiterscheinungen. Jahrbuch fur Psychologie undNeurologie, 43, 3-182.
Herz, E. (1944). Dystonia. I. Historical review; analysis ofdystonic symptoms and physiologic mechanisms involved.Archives of Neurology and Psychiatry, 51, 305-318.
Hoefer, P. F. A., and Putnam, T. J. (1940). Action potentialsof muscles in athetosis and Sydenham's chorea. Archivesof Neurology and Psychiatry, 44, 517-531.
Jakob, A. (1925). The anatomy, clinical syndromes andphysiology of the extrapyramidal system. Archives ofNeurology and Psychiatry, 13, 596-620.
Jenkins, G. M., and Watts, D. G. (1968). Spectral Analysisand its Applications. Holden-Day: San Francisco.
Koven, L. J. and Lamm, S. S. (1954). The athetoid syndromein cerebral palsy. Pediatrics, 14, 181-192.
Lance, J. W., Schwab, R. S., and Peterson, E. A. (1963).Action tremor and the cogwheel phenomenon in Parkin-son's disease. Brain, 86, 95-110.
Lewandowsky, M. (1910). Die zentralen Bewegungsst6run-gen. In Handbuch der Neurologie, Vol. I, part 2, pp. 685-772. Edited by M. Lewandowsky. Springer: Berlin.
Lindsley, D. B. (1936). Electromyographic studies of neuro-muscular disorders. Archives of Neurology and Psychiatry,36, 128-157.
Minear, W. L. (1956). A classification of cerebral palsy.Pediatrics, 18, 841-852.
Narabayashi, H., Nagahata, M., Nagao, T., and Shimazu, H.
(1965). A new classification of cerebral palsy based uponneurophysiologic considerations. Confinia Neurologica,25, 378-392.
Neilson, P. D. (1972a). Speed of response or bandwidth ofvoluntary system controlling elbow position in intact man.Medical and Biological Engineering, 10, 450-459.
Neilson, P. D. (1972b). Voluntary and reflex control of thebiceps brachii muscle in spastic-athetotic patients. Journalof Neurology, Neurosurgery, and Psychiatry, 35, 589-598.
Neilson, P. D. (1974). Voluntary control of arm movement inathetotic patients. Journal of Neurology, Neurosurgery, andPsychiatry, 37, 162-170.
Neilson, P. D., and Andrews, C. J. (1973). A comparison ofthe tonic stretch reflex in athetotic patients during rest andvoluntary activity. Journal of Neurology, Neurosurgery,and Psychiatry, 36, 547-554.
Phelps, W. M. (1956). Classification of athetosis with specialreference to the motor classification. American Journal ofPhysical Medicine, 35, 24-31.
Putnam, T. J. (1933). Treatment of athetosis and dystonia bysection of extrapyramidal motor tracts. Archives ofNeurology and Psychiatry, 29, 504-521.
Putnam, T. J. (1939). The diagnosis and treatment ofathetosis and dystonia. Journal of Bone and Joint Surgery,21, 948-957.
Twitchell, T. E. (1961). The nature of the motor deficit indouble athetosis. Archives ofPhysical Medicine, 42, 63-67.
Wilson, S. A. K. (1925). Some disorders of motility and ofmuscle tone, with special reference to the corpus striatum.Lancet, 2, 215-219.
177
Protected by copyright.
on May 30, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.2.171 on 1 February 1974. D
ownloaded from