Embed Size (px)
Citation preview

MDR-TB Diagnosis: How new and currenttools can be used to improve diagnosis
Claude Muvunyi MD, PhD
Meeting the Experts on MDR‐TB 8th December 2012, ITM, Antwerp

OUTLINE
• Part I: Sample Collection, Transport and Processing
• Part II: Overview of New lab techniques
Dr. Affolabi Dissou

Introducing New Technology• Infrastructure, biosafety measures and maintenance
• Equipment validation and maintenance
• Specimen transport and referral mechanisms
• Management of laboratory commodities and supplies
• Laboratory information data and management system
• Laboratory quality management
• Strategies for HR development and retention

Specimen• Appropriateness
• Collection
• Transport to laboratory
• Processing (Inoculation of media, Identification, DST, molecular test)
• Report

Appropriate Specimen• From relevant body site
• Lungs (Sputum)• Pleura
• Central nervous system• Lymphatic system• Genitourinary systems• Bones and joints• Disseminated (miliary
TB)• Pericardial disease
Type of sample
Sputum (resp. sample), CSF, gastric washings, lymph nodes (tissues), urine, faeces…
Source: CDC, 2001.

Collection (1)• Appropriate equipment (Proper containers for sputa)

Collection (2)• Good instructions to patient• Explain and demonstrate procedure

Wrong position
Collection (3)
- Sputum collection outside or in an empty room with very good ventilation
- The health worker should supervise,but should NOT stand in front of the patient

Collection (4)
How many? 2 or 3 for sputum? (spot/ morning)
Quality? salivary (white, watery, frothy)?
Quantity? at least 3 ml (3 – 5 ml)
Quality and amount of samples are crucial

Specimen Quality
Poor quality sputum
Better quality Source: CDC, 2007

Patient instruction for sputum sampling can improvetuberculosis diagnosis
A 16% increase in diagnostic yield Sputum samples from the intervention group were of greater volume
int j tuberc lung dis 9(7):814–817; 2005

TotalOdd Ratio P-value(95% Cl)
Gross appearance of sputum specimenssputum (versus saliva ) 1.69 (1.15-2.49) 0.007purulent, bloody (versus saliva, mucoid) 2.26 (1.58-3.23) <0.001
Volume of sputum specimens≥1ml (<1ml versus ≥1ml) 1.44 (1.02-2.03) 0.039≥2ml (<2ml versus ≥2ml) 1.30 (0.97-1.74) 0.080 ≥3ml (<3ml versus ≥3ml) 1.15 (0.84-1.58) 0.387 ≥4ml (<4ml versus ≥4ml) 1.44 (1.08-1.92) 0.014≥5ml (<5ml versus ≥5ml) 1.39 (0.76-2.53) 0.287
correlation of smear results with quality and quantity of sputum specimens
Yoon et al. BMC Infectious Diseases 2012, 12:172

Studies Method of collection
Number of specimens
% of positive smear
% of positive culture
Pande, et al. 1974 Spot 160 52 98Morning 160 85 92
Kim, et al. 1989 Spot 2,736 7Morning 2,968 12
Otto D. Schoch et al. 2007
Spot 83 54 39Morning 84 62 49
Case-yields of sputum specimens collected on the spot and morning

Case Yields of Multiple Sputum Specimenson Smear and Culture Examinations
(Review of 37 studies)
(Review of 4 studies)
Mase S, et al. I J TLD 2007;11(5):485-95.

Transport to Laboratory
• Safe packaging
• Temperature• Good labeling
Safe; Quick; Always in a cold box

Viability of M. tuberculosis in sputum stored at different temperatures
0
10
20
30
40
50
60
70
80
90
100
12
34
56
10090
81
63
29
10
100 100
100
9081
73
Room Refrigerator
Day 0Day 3 Day 7
Day 14Day 21
Day 28
Paramasivan CN et al. Tubercle. 1983 Jun;64(2):119-24.
No. of sputa tested: 41

0102030405060708090
100
12
34
5
99
87
5040
37
99 97
8067 67
Room Refrigerator
Day 0Day 3
Day 7Day 14 Day 28
Viability of M. tuberculosis in sputum stored at different temperatures
H. T. Banda et al. Int j tuberc lung dis 4(3):272–274 2000
No. of sputa tested: 30
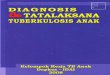
Transport ≤ 4 days for ≥ 90% of specimens
Yes No
Ship to reference laboratory
Decontaminate with 4% NaOH
Centrifuge at 300g and decent
Inoculate on LJ medium
Inoculate on Ogawa Medium
Add cetylpyridinium and ship to reference laboratory
Centrifuge at 3000g with cooling turned off and decant repeat
centrifugation after suspending the pellet in sterile 2% NaCl solution
Inoculate on LJ medium
Processing: Decision for transport medium, decontamination, centrifugation, and choice of medium.

Reporting
• Recod result in TB laboratory register
• Verify lab serial number on specimen report form and register are the same before reporting
• Submit timely reports to the treatment facilities
• Maintain an accurate TB laboratory register and worksheet register
• Signature

20
Specimen Transportation in the Lab Network
DH Laboratories
HC Laboratories
NRL , CHUK, (CHUB in near future)
Samples sent for CD4 count, Hematology, clinical chemistry and QC
Daily basis with motorbike
Feedback
Samples sent for specialized analysis ( DBS, VL Tb culture, DST and epidemic disease)
Samples sent for specialized analysis ( DBS, VL Tb culture, DST and epidemics diseases)
Tests performed and feedback sent twice per week to different levels by TRAC NET, phone call and courier
21
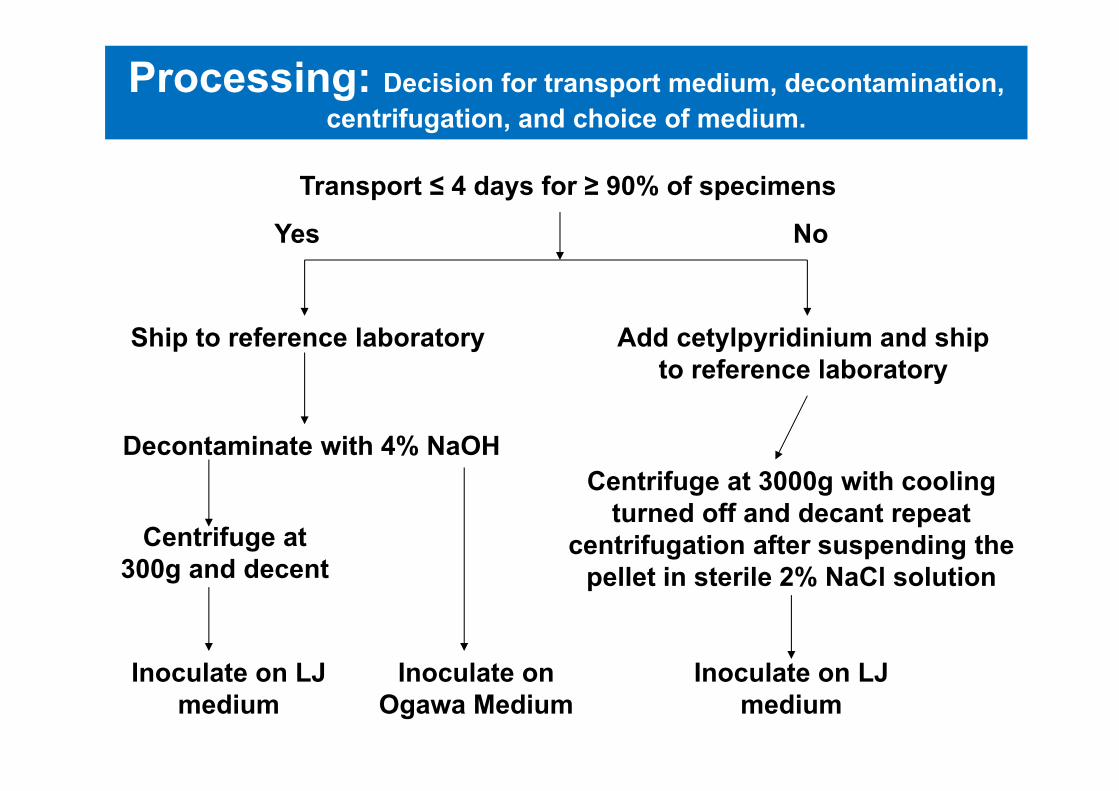
Map Of Rwanda Showing the District Hospital Selected for Sample transportation (Pilot)
DistrictHospital
ByumbaRutongoKibogoraBushenge
Shyira
Ruhengeri
Kaduha
Gitwe
Gakoma
Nyanza
Kagbayi
Nyagatare
Ngarama
KiziguroGahini

Summary• Good quality specimens are the cornerstone for high quality
tuberculosis diagnosis and treatment monitoring.
• Proper collection procedures and containers, adequate volumes and appropriate specimen transport conditions can all affect TB lab results.
• AFB in specimens do not lose their acid-fastness over time, but they rapidly lose their viability
• Recovery of viable bacilli decreases because of the ability to recover from other contaminating organisms
MDR-TB Diagnosis: How new and currenttools can be used to improve diagnosis
Dissou Affolabi MD, PhD
Meeting the Experts on MDR‐TB 8th December 2012, ITM, Antwerp