-
8/6/2019 McLeod Heme Tovee Class
1/131
MCCQE Hematology Review
Anne McLeod e-mail [email protected]
Office 416-340-3395
-
8/6/2019 McLeod Heme Tovee Class
2/131
GOALS and OUTLINE
Review MCCQE objectives and samplequestions
Few blood films
Few things not in the objectives
Practice questions
-
8/6/2019 McLeod Heme Tovee Class
3/131
MCCQE OBJECTIVES
www.mcc.ca/ObjectivesObjectives listed alphabetically
Practice Questions
-Exams-Mccqe1-Getting started-Practice exams
Two types of sample questions: MCQand CRS
-
8/6/2019 McLeod Heme Tovee Class
4/131
MCCQE OBJECTIVES
Bleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)Anemia (#42-1)
Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities (#120)
Lymphadenopathy (#54)
Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
5/131
Bruising & Bleeding-History
Pattern - lifelong or recent, deepseated bleeds or superficial
bruisingand petechiae
Bleeding challenges- circumcision,tonsils, wisdom teeth,
menstruation,pregnancy, appendix
Other PMHx - cancer, renal or liverdisease
-
8/6/2019 McLeod Heme Tovee Class
6/131
Bruising & Bleeding-Hx and Px
Family history - bleeding or transfusion
Drugs - ASA, NSAIDS, alcohol and herbals
Check for the spleen, petechiae/purpura,
telangiectasia and evidence other systemicdisease
-
8/6/2019 McLeod Heme Tovee Class
7/131
HEMOSTASIS
Three steps:
1. Primary Hemostasis
Vascular response, platelets and *vWF
2. Secondary Hemostasis
Fibrin clot formation (coag cascade) *vWF*carrier for FVIII
3. Fibrinolysis
-
8/6/2019 McLeod Heme Tovee Class
8/131
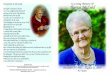
VWF
VWF
VWF
VWF
VWF
VWF
VWF
VWF =von Willebrand Factor
Subendothelium
VWF
VWF
VWF
VWFVWFVWF
VWFVWF
PRIMARY HEMOSTASIS
-
8/6/2019 McLeod Heme Tovee Class
9/131
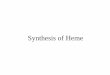
Subendothelium
HEMOSTASIS
2. Secondaryhemostasis - fibrin clot
1. Primary hemostasis-platelet plug
-
8/6/2019 McLeod Heme Tovee Class
10/131
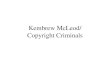
Subendothelium
HEMOSTASIS
3. Fibrinolysis andwound healing
-
8/6/2019 McLeod Heme Tovee Class
11/131
PRIMARY HEMOSTASIS-Vessel
HEREDITARY: HHT (Osler-Rendu-Weber)
Connective tissue (Ehler-Danlos)
ACQUIRED: Drugs -Steroids
Senile purpura
Infections
Vasculitis
-
8/6/2019 McLeod Heme Tovee Class
12/131
-
8/6/2019 McLeod Heme Tovee Class
13/131
PRIMARY HEMOSTASIS-Platelets
Too few platelets-thrombocytopenia
Dont work- platelet dysfunction
-
8/6/2019 McLeod Heme Tovee Class
14/131
PRIMARY HEMOSTASIS-Thrombocytopenia
DECREASED
PLATELETPRODUCTION
INCREASED
PLATELETDESTRUCTION
SEQUESTRATION
ie. plateletsstuck in thespleen/liver
-
8/6/2019 McLeod Heme Tovee Class
15/131
Accelerated Platelet Destruction
Non-immune-DIC, sepsis
Immune- TTP, ITP, SLE, drugs(heparin,
quinidine,cephalosporins)
Look at the blood film/smear!!
-
8/6/2019 McLeod Heme Tovee Class
16/131
-
8/6/2019 McLeod Heme Tovee Class
17/131
-
8/6/2019 McLeod Heme Tovee Class
18/131
-
8/6/2019 McLeod Heme Tovee Class
19/131
-
8/6/2019 McLeod Heme Tovee Class
20/131
-
8/6/2019 McLeod Heme Tovee Class
21/131
HIT
Platelet
Activated
Heparin-PF4
Complex
HIT Antibody
-
8/6/2019 McLeod Heme Tovee Class
22/131
Treatment of HIT Any heparin or LMWH contraindicated
in HIT
Need to use an alternative like a directthrombin inhibitor eg.
Hirudin orargatroban
Warfarin may worsen the thrombosis ifnot overlapped with an
alternativeanticoagulant until therapeutic
-
8/6/2019 McLeod Heme Tovee Class
23/131
Venous Limb Gangrene
-
8/6/2019 McLeod Heme Tovee Class
24/131
Confusing PLATELET
Problems
ITP HIT
PlateletPlatelet Platelet
UnControlled
vWF Release+
TTP
ActivatedActivatedNo activation
-
8/6/2019 McLeod Heme Tovee Class
25/131
Platelet Dysfunction1. Congenital-rare
2. Acquired COMMON!
Drugs - ASA, NSAIDs, Anti-Platelet agentsAlcohol, Uremia
Liver disease
Bone marrow disorders eg. MPD, MDS,MM
-
8/6/2019 McLeod Heme Tovee Class
26/131
Von Willebrands Disease Disorder of Primary ( Increased BT)
and
Secondary hemostasis (Increased PTT)
Treatment DDAVP if mild disease, HemateP ( blood product with
lots of VWF) ifsevere
Test family members usually autosomaldominant
-
8/6/2019 McLeod Heme Tovee Class
27/131
HEMOSTASIS SCREEN
Primary Hemostasis
CBC
Blood film/smear
Bleeding time
Platelet function tests
Tests for vWD
-
8/6/2019 McLeod Heme Tovee Class
28/131
HISTORY tells you :
PRIMARY SECONDARY
HEMOSTASIS HEMOSTASIS
Surface cuts Prolonged Normal
Onset after injury Immediate Delayed
Typical type / site Superficial Deep
Petechiae, purpura Subcutaneous
Mucosal bleed: Bleed into:
Nose, mouth, gums Joints, muscles,GI tract, Uterus GI /GU
tracts
Post op/trauma
-
8/6/2019 McLeod Heme Tovee Class
29/131
CLOT
GENERATION
OF
THROMBIN
EXTRINSIC(TISSUE FACTOR)
PATHWAY
INTRINSIC
PATHWAY
Secondary Hemostasis
-
8/6/2019 McLeod Heme Tovee Class
30/131
Disorders of Secondary Hemostasi
Hereditary
Hemophilia A (factor VIII deficiency) andHemophilia B (factor IX
deficiency) are X-linked and produce hemarthroses andhematomas and
are treated withrecombinant factor concentrates or if mild
deficiency DDAVP
von Willebrands disease
-
8/6/2019 McLeod Heme Tovee Class
31/131
Disorders of Secondary Hemostasis
Acquired
vitamin K deficiency (factors II, VII, IX and
X)
liver disease (all factors other than VIII)
DIC
Inhibitors Drugs- warfarin, heparin
-
8/6/2019 McLeod Heme Tovee Class
32/131
Standard Heparin
Usually administered in hospital becausecareful monitoring
required if given IV
Aim is to achieve an aPTT of 2.5-3X normalie. 60-90s
IV bolus followed by continuous infusion
Short half-life once IV infusion stoppedaPTT normalizes in ~4
hrs
-
8/6/2019 McLeod Heme Tovee Class
33/131
Standard Heparin
Easy to over anticoagulate patientswhich carries a very high
risk ofbleeding
Standard heparin can be reversed by
protamine
-
8/6/2019 McLeod Heme Tovee Class
34/131
Warfarin
-
8/6/2019 McLeod Heme Tovee Class
35/131
Warfarin
Vitamin K antagonist
Rapidly absorbed from GI tract buttakes few days to be
therapeutic
Dosing varies
Very close monitoring of INR required
in first few weeks
Dont start without heparin also!
-
8/6/2019 McLeod Heme Tovee Class
36/131
Treatment of Warfarin Overdose
Vitamin K -works in 6-12 hrs
Fresh frozen plasma- worksimmediately but BLOOD PRODUCTuse if
life threatening bleeding only!!!
Careful monitoring of INR best way to
prevent bleeding
-
8/6/2019 McLeod Heme Tovee Class
37/131
Extrinsic Pathway
PROTHROMBIN TIME - PT /INR
Increased if deficiency of factor VII and also of
common pathway factors- X, V, II and fibrinogen.
Results also reported as INR - to allow for
standardization between laboratories.
Used for monitoring oral anticoagulant (Warfarin)
therapy.
-
8/6/2019 McLeod Heme Tovee Class
38/131
Intrinsic Pathway
ACTIVATED PARTIAL THROMBOPLASTIN TIME
- aPTT
Detects deficiencies of the intrinsic
pathway factors XII, XI, IX, VIII and also
common pathway X, V, II and fibrinogen.
Used to monitor anticoagulation therapy
with standard heparin.
-
8/6/2019 McLeod Heme Tovee Class
39/131
50/50 MIX
PT/INR or PTT prolonged
Rule out presence of warfarin or heparin
If corrects=factor deficiency
If doesnt correct=inhibitor
-
8/6/2019 McLeod Heme Tovee Class
40/131
HEMOSTASIS SCREEN
THROMBIN CLOTTING TIME - TT
A test for conversion of fibrinogen to fibrin
Detects fibrinogen deficiency
Detects abnormal fibrinogens - dysfibrinogenemia
Detects inhibitors of fibrin polymerization - FDPs
(Fibrin degradation products) or D-dimers.
Detects thrombin inhibition eg. Heparin
-
8/6/2019 McLeod Heme Tovee Class
41/131
Quiz-Treatment of Bleeding Platelet transfusions
Vitamin K
Antifibrinolytics
DDAVP
FFP and cryoprecipitate
Protamine sulphate
-
8/6/2019 McLeod Heme Tovee Class
42/131
Sample Questions-MCQ
Which of the following is true about
hemorrhagic disease of the newborn:
Results from Vit K deficiency
More common in females
More common in bottle fed infants
Requires treatment with FFP
Evident in the first 24 hrs of life
-
8/6/2019 McLeod Heme Tovee Class
43/131
Sample Questions-MCQ Mr H has hemophilia which is shown to be
due to anti-
hemophilic globulin deficiency. There is no hemophilia
in his wifes family. He has 4 sons and 4 daughters.
Which is true?:
0 sons have H, 2 daughters carriers
4 sons H, 2 daughters carriers
0sons
H,0
daughters carriers 0 sons H, 4 daughters carriers
2 sons H, 4 daughters carriers
-
8/6/2019 McLeod Heme Tovee Class
44/131
Made up question- CRS A 65 year old man is admitted with loss
of
consciousness a few hours after a fall. He had been
experiencing a flu-like illness for several days
according to his daughter. CT head shows a subdural
hematoma and he requires urgent surgery.
According to his daughter he takes several heart pillsand she
tells you he had surgery to replace his heart
valve 6 yrs ago.
-
8/6/2019 McLeod Heme Tovee Class
45/131
Made up question- CRS
You are called by the lab : Hb 100
MCV 95 WBC 12 Plts 350 INR 8.0
aPTT 55 Fibrinogen N Creat LFT N.
What do you think is the most likely
cause of the elevated INR?
-
8/6/2019 McLeod Heme Tovee Class
46/131
Made up question- CRS
What are you going to do prior to his
surgery? Choose 3 Transfuse pRBC
Transfuse platelets
Give FFP
Give cryoprecipitate
Give Vit K
Give protamine
Cross and type forpRBC
Give DDAVP
-
8/6/2019 McLeod Heme Tovee Class
47/131
Made up question- CRS
After treatment the
surgeons want to
know if he can go to
the OR now what
blood tests will you
do? Choose 2 or
choose NONE:
INR and PTT
Thrombin time
CBC
INR
Heparin level
Warfarin level
Bleeding time
NONE
-
8/6/2019 McLeod Heme Tovee Class
48/131
MCCQE OBJECTIVESBleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)
Anemia (#42-1)
Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities (#120)
Lymphadenopathy (#54)Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
49/131
Hereditary Causes of Thrombophilia
Antithrombin III
deficiency
Protein C deficiency
Protein S deficiency
Factor V Leiden
Prothrombin 20210
-
8/6/2019 McLeod Heme Tovee Class
50/131
Acquired Risk Factors for VTE Age
Previous thrombosis
Immobilization
Surgery
Malignancy
Nephrotic syndrome
APLA syndrome
Myeloproliferative
disorders
BCP / HRT
Pregnancy/postpartum
Obesity Heavy smoker
-
8/6/2019 McLeod Heme Tovee Class
51/131
Who should be screened?Hereditary
Age
-
8/6/2019 McLeod Heme Tovee Class
52/131
ThrombophiliaWorkup after H+PINITIAL
CBC
Screen forantiphospholipid antibody
Fasting homocysteine
APCR-functional screenfor Factor V Leiden
DNA testing for Factor VLeiden and Prothrombinmutations
POST HEPARIN
Antithrombin
POST WARFARIN
Protein C,S
-
8/6/2019 McLeod Heme Tovee Class
53/131
Diagnosis Physical exam not useful
D-dimers
Doppler ultrasound
Ventilation/Perfusion scan
CT chest with PE protocol
We dont use Impedanceplethysmography
-
8/6/2019 McLeod Heme Tovee Class
54/131
Treatment of VTE
Antiplatelet agents-Phlebitis only
Anticoagulants
- standard heparin
low molecular weight heparins
warfarin
new agents
Thrombolytic agents
-
8/6/2019 McLeod Heme Tovee Class
55/131
Sample Question-CRS 28 yr old G2P2 woman presents 5 days
post SVD with 2 day history of aching and
tenderness L inguinal region. L leg isdiscoloured and swollen.
No othersymptoms she is breastfeeding.
What tests if any would you order choose
up to 3:
-
8/6/2019 McLeod Heme Tovee Class
56/131
Sample Question-CRS ABG
Blood culture
CBC Doppler US of leg
Ear oximetry
ECG
Endometrial culture
ESR
Fibrinogen leg scan
IPG
Pelvic US
PT, PTT Radionucleotide
phlebography of leg
Thermography of legs
Venogram L leg Vent/Perf scan
No tests
-
8/6/2019 McLeod Heme Tovee Class
57/131
Sample Question-CRS Pt admitted with
baby to start
treatment in 4-6hrs what orderswould you write?Choose up to
5.
Acetominophen
Aspirin daily
Antibiotics IV Bedrest
CXR
CBC
Daily IPG IVC filter
-
8/6/2019 McLeod Heme Tovee Class
58/131
Sample Question-CRS Heparin IM
Heparin IV bolus
Heparin by IV constantinfusion
Heparin SC
Initial PTT
PTT at 4 hrs post bolus Plt count q 3 days
Stop breastfeeding
Streptokinase
Support hose Surgery consult
Traction L leg
Tubal ligation
Vitamin K Warfarin
-
8/6/2019 McLeod Heme Tovee Class
59/131
Sample Question-CRS Patient treated to
prepare for
discharge whatwould you do?Choose as many aswant.
Avoid ASA Contraception
Support hose
Heparin 3-4 mons
Heparin 5-6 mons Reg PT and PTT
Reg PT
Stop breastfeeding
Vitamin K
Warfarin 3-4 mons Warfarin 5-6 weeks
-
8/6/2019 McLeod Heme Tovee Class
60/131
MCCQE OBJECTIVESBleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)
Anemia (#42-1)
Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities (#120)
Lymphadenopathy (#54)Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
61/131
Approach to Anemia Focus on bleeding, drugs, family
history, diet and bowel habits
Look at MCV, WBC, diff, plts and film
New or old
MCV very helpful !!
-
8/6/2019 McLeod Heme Tovee Class
62/131
Approach to Anemia
Look at the blood film!!!
Micro Macro vs Normo
-
8/6/2019 McLeod Heme Tovee Class
63/131
Microcytic Anemia T
A
I
L
S
Look at the blood film!!!
-
8/6/2019 McLeod Heme Tovee Class
64/131
Iron Ferritin is the best blood test for assessing
iron stores but is increased by
inflammation, cancer and liver disease
Nail changes
Pica, blue sclerae, glossitis, angularstomatitis, sore burning
mouth,esophageal web
-
8/6/2019 McLeod Heme Tovee Class
65/131
Iron - Clinical Points Blood film is usually diagnostic
Bone marrow examination is rarely needed
Iron deficiency is nevera final diagnosis The 10-10-1 rule
10 mg in diet
10% absorbed
1 mg absorbed and lost daily Consider Celiac disease
-
8/6/2019 McLeod Heme Tovee Class
66/131
-
8/6/2019 McLeod Heme Tovee Class
67/131
-
8/6/2019 McLeod Heme Tovee Class
68/131
Iron - Therapy Iron replacement requires normalization of
the hemoglobin and the body stores (3mons after hemoglobin
normal)
Iron therapy is a balance between the doseof elemental iron and
GI tolerance
Iron supplements are good forpremenopausal women and
potentiallyharmful to men
-
8/6/2019 McLeod Heme Tovee Class
69/131
-
8/6/2019 McLeod Heme Tovee Class
70/131
Anemia of Chronic Disease Common in patients with infection,
cancer,
inflammatory and rheumatologic diseases
Iron can not be remobilized from storage Blunted production of
erythropoietin and
response to erythropoietin
Usually normocytic and normochromic but
may be microcytic if severe
-
8/6/2019 McLeod Heme Tovee Class
71/131
Thalassemia Poikilocytosis and basophilic stippling may
be seen in the blood film
Hemoglobin electrophoresis is onlydiagnostic for
beta-thalassemia and maynot be diagnostic if iron deficiency is
alsopresent
Hb H prep and/or DNA analysis needed todiagnose
alpha-thalassemia
-
8/6/2019 McLeod Heme Tovee Class
72/131
-
8/6/2019 McLeod Heme Tovee Class
73/131
-
8/6/2019 McLeod Heme Tovee Class
74/131
Sample Question Lead exposure can cause all of the
following except:
a) Abdo painb) porphyrinuria
c) Cirrhosis of the liver
d) Paresise) anemia
-
8/6/2019 McLeod Heme Tovee Class
75/131
-
8/6/2019 McLeod Heme Tovee Class
76/131
Made up Question A woman with HB SC disease presents in
pregnancy. She asks if the baby will have
HB SC disease. Choose the correctanswer:
a) Baby can not have SC disease
b) Baby will have sickle cell trait
c) Baby will be normal
d) More information is needed
-
8/6/2019 McLeod Heme Tovee Class
77/131
Sideroblastic Anemia Produces a dimorphic blood film
with microcytes and macrocytes
Marrow shows ring sideroblasts
Usually acquired and associated witha myelodysplastic syndrome,
drugs
or toxins Rarely due to pyridoxine deficiency
-
8/6/2019 McLeod Heme Tovee Class
78/131
-
8/6/2019 McLeod Heme Tovee Class
79/131
Macrocytic AnemiaOval macrocytes (megaloblastic)
B12, folate, drugs
Round Macrocytes
Reticulocytosis
Alcohol/ Liver Disease
Myelodysplasia
-
8/6/2019 McLeod Heme Tovee Class
80/131
B12 Deficiency Be aware of the neurological
complications
Never treat possible B12 deficiencywith folate - the CNS lesions
mayprogress
Schilling test distinguishes perniciousanemia from other
causes
-
8/6/2019 McLeod Heme Tovee Class
81/131
Folic Acid Deficiency The peripheral blood film and bone
marrow
are identical to B12 deficiency
Women of childbearing age should takesupplemental folate to
prevent neural tubedefects in their children
Folate supplementation lowershomocysteine levels leading to less
heartdisease and stroke
-
8/6/2019 McLeod Heme Tovee Class
82/131
-
8/6/2019 McLeod Heme Tovee Class
83/131
-
8/6/2019 McLeod Heme Tovee Class
84/131
Normocytic Anemia
Are the retics high or low?
-
8/6/2019 McLeod Heme Tovee Class
85/131
Normocytic AnemiaHigh Retics= making RBC butbeing lost
Bleeding
Hemolysis
MyelofibrosisTreated nutritional deficiency
-
8/6/2019 McLeod Heme Tovee Class
86/131
-
8/6/2019 McLeod Heme Tovee Class
87/131
Hemolytic Anemia
Destruction of RBC leads to increasedretics, increased indirect
bilirubin andincreased LDH
Hereditary or acquired
-
8/6/2019 McLeod Heme Tovee Class
88/131
Hemolytic AnemiaIntravascular RBCs being destroyed
in the blood vessel and hemoglobin
lostTests:
RBC fragments, decreased
haptoglobin, hemoglobinuria Become iron deficient over time
-
8/6/2019 McLeod Heme Tovee Class
89/131
Hemolytic AnemiaExtravascular hemolysis-RBCs being
destroyed by RE system and hemoglobinrecycled:
Autoimmune hemolytic anemia -like ITPantibody on surface of RBC
destroyed tooearly by RE system
Test: Direct antiglobulin test (Coombstest),dont become iron
deficient
-
8/6/2019 McLeod Heme Tovee Class
90/131
-
8/6/2019 McLeod Heme Tovee Class
91/131
Hemolytic Anemia-Intra and Extra
Inherent RBC Defects
Membrane defects - hereditaryspherocytosis and
hereditaryelliptocytosis
Enzyme defects - G6PD
Hemoglobinopathy - Sickle CellDisease
-
8/6/2019 McLeod Heme Tovee Class
92/131
-
8/6/2019 McLeod Heme Tovee Class
93/131
Sample Question What would be the best test to confirm
the diagnosis of hereditary spherocytosis:
a) RBC enzyme studiesb) HLA studies
c) Bone marrow
d) Osmotic fragility
e) Coombs test
-
8/6/2019 McLeod Heme Tovee Class
94/131
-
8/6/2019 McLeod Heme Tovee Class
95/131
-
8/6/2019 McLeod Heme Tovee Class
96/131
Normocytic AnemiaLow Retics= not making RBC
Bone marrow problem-MDS,leukemia, cancer, aplasticanemia
EPO problem- uremia, ACDThyroid
-
8/6/2019 McLeod Heme Tovee Class
97/131
Anemia by ageMore common in elderly:
bone marrow problemsMDS,MM leukemias (CLL,CML, AML) Low
Kids get acute leukemias notchronic or MDS or MPD
-
8/6/2019 McLeod Heme Tovee Class
98/131
Made up question A 32 yr old woman presents with
few day history of easy bruising
and headache. CBC: Hb 135 MCV 95 WBC 12 Plt
3
What are you going to order? What is your diagnosis?
-
8/6/2019 McLeod Heme Tovee Class
99/131
Made up question A 32 yr old woman presents with
a 1 day history of petechiae andheadache.
CBC: Hb 85 MCV 99 WBC 12 Plt 3
What are you going to order?
What is your diagnosis?
-
8/6/2019 McLeod Heme Tovee Class
100/131
MCCQE OBJECTIVESBleeding tendency/bruising
(#15-1)Hypercoagulable state (#15-2)
Anemia (#42-1)Polycythemia/Elevated Hemoglobin
(#42-2)White blood cell abnormalities (#120)
Lymphadenopathy (#54)Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
101/131
Polycythemia/ Increased Hemoglobin
Increased Hgb may be due toincreased RBC mass or decreasedplasma
volume
Need to measure red cell mass(blood volume studies)
-
8/6/2019 McLeod Heme Tovee Class
102/131
Increased Red cell mass Independent of EPO= Polycythemia
Rubra Vera (low EPO level)
Secondary to Increased EPOAppropriate EPO elevation ie.
Hypoxemia,
Hb defects, carbon monoxide
Inappropriate EPO elevation ie. EPO
secreting tumours, polycystic kidneys, postrenal transplant,
androgens
-
8/6/2019 McLeod Heme Tovee Class
103/131
Polycythemia Rubra Vera Must be differentiated from
secondary
erythrocytosis and other MPD
Arterial and venous thromboses/ Bleeding Splenomegaly often
massive
Increased neutrophil count and/or plateletcount is seen
frequently
Treatment is phlebotomy or hydroxyurea
-
8/6/2019 McLeod Heme Tovee Class
104/131
MCCQE OBJECTIVESBleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)
Anemia (#42-1)Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities(#120)
Lymphadenopathy (#54)Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
105/131
WBC DifferentialNeutrophils (ANC)
Lymphocytes
MonocytesEosinophils
Basophils
Left shifted- bands, myelocytes,metamyelocytes
-
8/6/2019 McLeod Heme Tovee Class
106/131
-
8/6/2019 McLeod Heme Tovee Class
107/131
-
8/6/2019 McLeod Heme Tovee Class
108/131
-
8/6/2019 McLeod Heme Tovee Class
109/131
-
8/6/2019 McLeod Heme Tovee Class
110/131
Leukemoid Reactions CML mimicked by acute bacterial
infection
inflammatory reactions, severe marrow
stress such as bleeding, underlying tumorsand treatment with
G-CSF and GM-CSF
CLL mimicked by pertussis, TB and mono
CMML and acute monoblastic leukemia
mimicked by TB
-
8/6/2019 McLeod Heme Tovee Class
111/131
Chronic Myeloproliferative Disorders Polycythemia rubra vera
Chronic granulocytic (myelogenous)leukemia
Idiopathic Myelofibrosis
Essential thrombocythemia
-
8/6/2019 McLeod Heme Tovee Class
112/131
-
8/6/2019 McLeod Heme Tovee Class
113/131
-
8/6/2019 McLeod Heme Tovee Class
114/131
Approach to Neutropenia History - drugs, toxins, recurring
mouth
sores, family history, ethnic background
Physical - splenomegaly, bone pain If the patient is
asymptomatic recheck the
WBC after exercise
Blood film - are granulocytic precursors or
blasts present Bone marrow
Severity significant (ANC< 500)
-
8/6/2019 McLeod Heme Tovee Class
115/131
Approach to Neutropenia (ANC
-
8/6/2019 McLeod Heme Tovee Class
116/131
Approach to Lymphocytosis
Young people think MONO
Old people CLL
-
8/6/2019 McLeod Heme Tovee Class
117/131
Infectious Mononucleosis Fever, pharyngitis, generalized
adenopathy
splenomegaly and hepatomegaly
Monospot and EBV antibodies are positive immune thrombocytopenia
and anemia
seen
the blood film shows atypical lymphs
with granules, coarse chromatin andspreading cytoplasm with
pseudopods
-
8/6/2019 McLeod Heme Tovee Class
118/131
-
8/6/2019 McLeod Heme Tovee Class
119/131
Chronic Lymphocytic Leukemia Common in the elderly
the blood film shows a lymphocytosis that
may be extreme and smudge cells lymphadenopathy and
splenomegaly
Often complicated by autoimmune anemiaand thrombocytopenia
treatment is observation, alkylatingagents, fludarabine,
steroids or radiation
-
8/6/2019 McLeod Heme Tovee Class
120/131
Multiple Myeloma The blood film shows rouleaux
a monoclonal immunoglobulin can be in
serum or urine Hypercalcemia, renal failure, lytic bone are
frequent
Treat hydration, steroids,
bisphosphonates, chemotherapy or BMT Need to distinguish from
MGUS
-
8/6/2019 McLeod Heme Tovee Class
121/131
-
8/6/2019 McLeod Heme Tovee Class
122/131
MCCQE OBJECTIVESBleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)
Anemia (#42-1)Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities (#120)
Lymphadenopathy (#5
4)Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
123/131
Is it LYMPHOMA?Ask about B symptoms- fever, night
sweats, weight loss
Is there evidence of infection?LNs-tender, size,
consistency,
fixed/matted
Examine spleen
Always consider LN biopsy
-
8/6/2019 McLeod Heme Tovee Class
124/131
Made up Question-CRSA 70 yr old man presents with 6 month
history of
fatigue, night sweats and weight loss. Examreveals diffuse
adenopathy.
What investigations would you do first?Choose 2
a) CBC with differential
b) INR and PTT
c) Blood film/smear
d) CT thorax and abdo
e) Lymph node biopsy
-
8/6/2019 McLeod Heme Tovee Class
125/131
MCCQE OBJECTIVESBleeding tendency/bruising (#15-1)
Hypercoagulable state (#15-2)
Anemia (#42-1)Polycythemia/Elevated Hemoglobin (#42-2)
White blood cell abnormalities (#120)
Lymphadenopathy (#54)
Splenomegaly (#2-3)
-
8/6/2019 McLeod Heme Tovee Class
126/131
SplenomegalySpleen should not be palpable in adults
Ask about B symptoms and look for LNs
Spleen exam- percussion most sensitive(JAMA paper)
Causes:
Infiltrative vs. Congestive vs. Increaseddemand for splenic
function
-
8/6/2019 McLeod Heme Tovee Class
127/131
Sample Question-MCQ22 yr old man who had splenectomy 2 yrs
ago
post trauma presents with confusion, coughand fever which
developed over 12 hrs.
On arrival VS T 41 RR 28 BP 90/70HR 130
Which of the following would best confirm the diagnosis?
a) Blood culture
b) CXR
c) Sputum sampled) ECG
e) Urine culture
-
8/6/2019 McLeod Heme Tovee Class
128/131
Sample Question-MCQA 22 yr old woman presents with iron
deficiency
anemia and easy bruising. Her INR/PT isnormal and PTT is
slightly prolonged.
Which of the following is the most likely diagnosis?
a) DIC
b) Liver failure
c) Von Willebrand disease
d) Hemophilia A (factor VIII def)
e) Factor XII deficiency
-
8/6/2019 McLeod Heme Tovee Class
129/131
Sample Question-MCQA 30 yr old woman presents with a swollen
left calf. She
has no family history of blood clots.Her INR/PT isnormal and her
PTT is prolonged. Investigationsdemonstrate a DVT.
Which of the following is the most likely etiology of
herDVT?
a) Von Willebrand disease
b) Antithrombin deficiency
c) APLA
d) Pregnancy
e) Age
-
8/6/2019 McLeod Heme Tovee Class
130/131
Sample Question-MCQA 60 yr old man with prostate cancer
presents
with a painful swollen right leg.
Which of the following is the most appropriateinvestigation?
a) CXR
b) venogram
c) Doppler US of leg
d) D dimer
e) PSA
-
8/6/2019 McLeod Heme Tovee Class
131/131
MCCQE Hematology Review
Anne McLeod
e-mail [email protected]
Office 416-340-3395