Embed Size (px)
Citation preview

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 1/40
F i r s t a i d
Introduction
Priorities
Gen era l principles of firsta id
Gene ral assessment ofthe situa tion
Dressing s, band ag es,slings a nd splints
First a id sat chels andboxes
Severe bleeding
Unconscious casualt y
Burns an d scalds
Suffocation (asphyxia)
Strangula t ion
Choking
Epileptic fits
Shock
Bleeding
Wounds
FracturesDislocations
Head injuries
Chest injuries
Blast injuries
Tran sporta tion
CHAPTER 1
5
Introduction
When a ship is in port , or nea r to port w here hospita l a nd
other expert medical a t tent ion are a vai lab le , the f i rst a id
treatment necessary aboard ship is similar to that practised
ashore. At sea, in th e a bsence of t hese fa cilities, trained ships’
of f icers are required to give types of treatment beyond tha t
accepted a s norma l f irst aid.
The conten t of t his chapt er covers the know ledge o f f irst
a id necessary for the safe and ef f icient immediate treatment
of casual t ies before they are transported to the ship’s
hospital or to a cabin for any necessary definitive treatment
of th e type described in Chapter 4.
However, anyone aboard ship may f ind a casual ty andevery seam an should know three b asic life-saving a ctions to
be given immediately while wai t ing for tra ined help to
arrive. These a re:
to g ive artif icial respiration by t he mou th t o nose/mout h
m eth od ;
to pla ce an unconscious casua lty in the unconscious
position;
to stop severe bleeding.
PrioritiesOn f ind ing a casualty :
ensure your ow n safety ;
i f necessary , remove the casual ty f rom danger or danger
f rom the casual ty (but see the note below on enclosedspaces);
give immediate treatment to t he casualty who is not
brea thing a nd/or w hose heart h as stopped, is bleeding
severely or unconscious – others can be trea ted la ter;
send for help.
If there is more t han o ne unconscious or bleeding ca sualty:
send for help;
trea t the most serious injury f irst in the order of :
• not breat h ing and/or heart s topped ;
• unconsciousness.
• serious b leeding;
If th e ca sua lty is in a n ENCLOSED SPACE:
DO NOTenter the en closed space unless you a re a tra ined
membe r of a rescue tea m acting unde r instructions;
send for help and inform the ma ster.
It must be assumed tha t t he a t mosphere in the space is
hostile. The rescue team MUSTNOT ente r unless w earing
breath ing appa ratus which must a lso be f i t ted to the casual ty
as soon a s possible. The casua lty must be remo ved q uickly to
the nearest safe ad jacent area outside the enclosed space
unless his injuries and the likely time of evacuation makes
some treatment essentia l before movement.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 2/40
6 THE SHIP CAPTAIN’S MED ICAL GUID E
General principles of first aid on board shipThe g ene ral principles are:
make a rapid examinat ion of t he pat ient to assess responsiveness and t he extent of the
injury;
check breat hing, heart a nd look for serious bleeding;
• i f breath ing has stopped , g ive a rt i f icia l respirat ion ;
• if the heart ha s stopped , give hea rt compression and a rtif icial respirat ion;
• arrest serious bleeding;
hand le the pat ient as little a nd as gent ly as possible so as to:
• prevent furth er injuries; and
• prevent further shock ;
see that the pa t ient is put in the most comfortab le posit ion possib le a nd loosen t ight
cloth ing so t hat he can breat he easi ly ;
do no t remove more cloth ing tha n is necessary and , w hen you d o, remove i t gently . With an
injured l imb, get the sound l imb out o f the cloth ing f i rst a nd then peel the clothes of f the
injured limb, which should be supported by ano ther person during t he process. If cutt ing
cloth es is indicated t o expose the injured part, do so. In removing a b oo t or shoe remove the
lace and , i f necessary, cut the upper do wn tow ards the to ecap; keep onlookers aw ay.
alwa ys remember that shock can be a g reat da nger to l i fe and one of the main objects of
first a id is to prevent t his;
you ma y have to improvise splints, ba nda ges et c. (Figure 1.23);
do not g ive a lcohol in any form;
do no t mo ve the pa t ient unti l he is f i t to be moved . Bleeding should be a rrested , f ractures
immobil ised and shock treated . See that the necessary personnel and eq uipment for
smooth and ef f icient transport are a vai lab le ;
never consider anyone to be dead unti l you and o thers agree that :
• b rea th in g h a s stopped ;
• no pulse is fe lt a nd no sounds are heard w hen the examiner’s ear is put to the chest ;
• the eyes are glazed and pupils are d i la ted ;
• there is a progressive cool ing of t he body.
(For a f urther description o f the d iagn osis of d eat h Chapte r 12).
General assessment of the situationOnce i t has been estab l ished tha t there is no immediate threat to l i fe there wil l be t ime to ta ke
stock of the situation. Reassurance and quick and effective attention to injuries and
compa ssionat e trea tment of t he injured person w ill alleviate his condition . Remembe r:
a calm and systematic approach should be ado pted ;
give nothing by mouth ;
protect the casualty f rom heat or cold , remembering that in the t ropics open steel decks can
be very hot ; never underest imate and do not treat as minor in juries:
• unconsciousness
• suspected in ternal b leeding
• s t ab or pun cture w oun d s
• w ound s near joints (see fractures);
• possible fractures
• eye injuries

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 3/40
Cha pt er 1 FIRSTAID 7
Dressings, bandages, slings and splints
Standard dressing
A standa rd dressing consists of a t h ick pad o f ga uze w hich is a t tached to a b anda ge, leaving
abo ut 30cm of t ail. The dressing is packed in a pap er cover and is sterile. Therefo re, w hen t he
package is opened , i t is important that the ga uze pad should not be a l low ed to t ouch anything
(including you r f ingers) befo re it is applied to the w ound .
Stand ard dressings are available in three sizes:
Small Ga uze pa d mea sures 7.5 cm by 10 cm.
Medium Gau ze pa d mea sures 10 cm by 15 cm.
Large Ga uze pa d mea sures 15 cm by 20 cm.
Alw ays select a dressing w ith a pa d w hich is larger tha n the
wo und w hich you have to cover up.In use the pa d is placed upon the w ound, the ta i l is taken
round the l imb and held , the ba ndag e is held ta ut a s it is
taken round the af fected part so as to ` lock ’ the ta i l in
posit ion . The ba ndag ing can then b e continued to hold the
dressing firmly in place by making turns above and below
the pa d so th at they o verlap it (Figure 1.1).
Bandages
Bandages are required to a pply and maintain pressure on a wo und to stop b leeding, to keep a
dressing in place, to provide support, and t o prevent mo vement. Wherever a stan dard d ressing is
not used i t is customary to cover a w ound in the fo l low ing wa ys:
dry dressing – sterile gauz e or lint covered by a layer of cot ton w oo l and held in place by a
rol ler or tr iangular banda ge;
non-stick dressing – sterile paraff in ga uze covered by sterile ga uze or lint and cott on w ool
and held in place as above.
NOTE: Never use cott on w oo l as the f irst layer o f a dressing. When using lint alw ays put t he
smooth surfa ce next to the skin.
Tube gauze finger bandage
Cut o f f a p iece o f tub e gauze b an d a ge
60 cm long. Lay th is on a f lat surfa ce and
make a longi tudinal cut a t one end
10 cm long th roug h bot h thicknesses of
the ba nda ge (Figu re 1.2). The t ails so
formed, ‘B’, will be used to secure the
b an d age .
Insert the applicator into the
bandage at end ‘B ’ , then push al l the
ban da ge o n to it. Then pull 2.5 cm of
th e b an d age o f f th e en d o f th e
ap plicato r (Figure 1.3). Tuck th is inside.
Hold the finger dressing in place.Insert the f inger in to the a pplicator a nd
push it gent ly tow ards the base of the
f inger. Hold the band ag e in place with
your th um b an d w i th d raw th e
applicator w i th a slight turning mot ion .
The ba nda ge w ill slip off th e applicato r
and wil l mould f i rmly to the f inger
(Figu re 1.4).
Figure 1.1
A
60 cm
10 cm
B1B2
Figure 1.3 B1 B2
Figure 1.4
Figure 1.2

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 4/40
When the a pplicator comes of f the f inger, hold the banda ge a nd the a pplicator f i rmly and
turn throu gh 360 deg rees (Figure 1.5).
Re-insert the t ip of the f inger in to the a pplicator and push it once ag ain to t he base of the
fing er (Figure 1.6).
Repea t the complet e mano euvre until the ba nda ge is all used up. Then tie loosely at t he ba se
of the finger (Figure 1.7). Tape the ba se of t he dressing avo iding encircling the finger.
Triangular bandage
This is the most useful bandag e in f i rst a id . It can be used as a broa d or na rrow fo ld banda ge t o
hold dressings in place. It can a lso b e used fo r immobilising limbs or a s a sling. It is made from
calico or similar mat erial by cutting diag ona lly across a squ are o f mat erial having 1 metre sides.
The ends should alwa ys be tied with a reef kno t.
Broad and narrow fold bandages
Figure 1.8 shows how to make a broad a nd a narrow fold banda ge.
The main w ays in which a tr iangular banda ge can b e used , e ither as a temporary dressing or
to secure or cover a prope r dressing, are a s follow s:
Hand bandage
See Figu re 1.9
Wrist and palm bandage
Place palm on the middle of a narrow fold banda ge. Take the ends and cross the ba ndag e at the
back of the ha nd , leaving out the thumb. Take turns of the ba ndag e round a nd round the w rist
and tie off at the b ack (Figure 1.10).
8 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.6Figure 1.5 Figure 1.7
Figure 1.8 Broad and narrow fold bandages.
(a ) Tria ng ula r b a nd a g e la id f la t . (b ) Fo lded once.
(d) Folded three t imes – narrow f old ba ndag e.(c) Folded tw ice – broad f old ba ndag e.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 5/40
Cha pt er 1 FIRSTAID 9
Elbow bandage
Fold over the base of the bandage and place the back of the
elbow in the middle of the banda ge so that the point l ies a t the
back of the upper arm. Take the ends of the b anda ge round t he
forearm, cross them in the bend o f the elbow, a nd then t ake
them round the upper a rm – to ma ke a ‘ f igure of e ight ’ . Tie of f
a t t he back of the arm a bout 10 cm abo ve the elbow. Fold dow n
the po int an d fix it with a safet y pin (Figure 1.11).
Shoulder bandage
Stand facing the casualty’s injured side. Place the centre of an
open ba ndag e on his shoulder with the point running up the
side o f th e neck (Figure 1.12a). Fold a hem inw ards a long t he
base, carry the ends round th e middle of the a rm, cross and tie
them on the out er side (Figure 1.12b). This will secure the low er
border of the ba ndag e. Apply an arm sl ing. Turn the po int of the
shoulder banda ge already applied down o ver the knot of the
arm sling. Pull it tig ht a nd pin it in pla ce (Figure 1.12c).
Figure 1.10
Figure 1.11
(a) Place the hand on the
banda ge. Bring dow n point ‘C’
over the back of the hand t o the
wrist
(b) Turn ‘A’ over the b ack of th e
hand, under ‘B ’ and half around
the w rist .
(c) Turn ‘B’ ove r the b ack of t he
hand , over ‘A’ and ha lf around
the w rist .
(d) Take t urns w ith ‘A’ and ‘B’
round the wris t and tie of f .
(a )
(b) (c) (d)
Figure 1.12
A
C
B
A B A B
(a)
(b) (c)
Figure 1.9 Hand bandage

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 6/40
10 THE SHIP CAPTAIN’S MED ICAL GUID E
Crutch bandage
Tie a narrow fold banda ge round the w aist ; a t
the middle of the back pass another one
un d er it an d a l low en d s to h an g d ow n a t th e
same level. Grasp both these ends and bring
them fo rward under the crutch . Pass one end
under the waist bandag e in f ront and t ie of f
(Figu re 1.13).
Hip bandage
Tie a narrow fold banda ge round the wa ist
with the knot on injured side. Pass the point
of ano ther banda ge up under the knot , turn af o ld a t th e b ase o f th e b a n d age a n d b r in g th e
ends round the th igh t o t ie of f on the o uter
side. Pull the point up to rem ove creases and
then fold i t down o ver the knot and f ix wi th
safe ty p in (Figure 1.14).
Knee bandage
Place the point of the ba ndag e in the f ront of
the middle of the th igh , turn a fold a t the ba se
of the ba ndag e so that i t is abo ut 10 cm below
the kneecap . Take th e ends round t he ba ck of
the joint in a f igure-of-eight and tie off in
f ront w el l above the kneecap. Fold the point
down over the knot and f ix wi th safety pin
(Figu re 1.15).
Foot bandageLay the foo t f la t on the ba ndag e. Bring point
‘A’ up over the foo t in front of t he a nkle. Take
‘B’ over the foot and behind the a nkle . Do the
same with ‘C’ . Knot in f ront of the ankle
(Figu re 1.16).
Figure 1.13
Figure 1.14
Figure 1.16
Figure 1.15
A
CB
B
AB
C

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 7/40
Cha pt er 1 FIRSTAID 11
Eye bandage
Place the middle of a na rrow fold ba ndag e d iagona l ly across
the a ffected eye so as to cover the d ressing. Take bo th end s
round the head , cross them at the back and bring them
forwa rd aga in . Tie of f over the forehead but not over the
eye (Figure 1.17).
Head and scalp bandage
Figure 1.18 is self-explanatory. It is important that the
ban da ge is placed just abo ve the eyebro w s. The ta ils ‘B’ and
‘C’ should be ta ken well under the o cciput (the bump o n theback of the head where t he neck joins the head) , and pulled
fair ly t ight before tak ing them round to the f ront t o be t ied
off . Failure to d o th is w ill result in the ba nda ge f alling off , if
the pat ient should b end o ver (Figure 1.18).
Ring pad
Spread al l the f ingers of o ne hand to form a rough circle of
the required size . Make two turns of a narrow fold banda ge
round th e ends of the f ing ers. Tw ist the rema inder of the
bandage round the circle so formed to make a grommet
(Figu re 1.19).
To pa ss a na rrow-fold band ag e under the legs or body
when t he casual ty cannot be moved –
Obtain a long piece of wo od o r a spl in t . Lay the narrow
fold banda ge on a f la t surface. P lace the splin t on top o fi t . Then fold a bout 22 cm of the b anda ge ba ck over the
splint. Holding the splint a nd the ba nda ge firmly, gently
push the w hole under the pa t ient w here i t is required
and carry on pushing unti l the end comes out on the
opposi te side. Free the bandage and draw i t through.
Withdra w t he splint. Ma ke the necessary tie.
Figure 1.19
Figure 1.18
Figure 1.17
A
C
B
A
C
B
AC
B

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 8/40
Slings
Slings are usually made fro m triang ular ban da ges, or they can b e improvised. The ma in wa ys in
which to ma ke a sl ing a re as fol lows:
Large arm sling
Place the tr iangular ba ndag e on t he chest , carrying the point behind the elbow of the injured
arm. One end is then placed over the shoulder of the uninjured side a nd the other hang s down.
Gently set t le the a rm across the banda ge, turn up i ts low er end over the forearm a nd t ie i t over
the shoulder of t he uninjured side so that it fu lly takes the w eight o f the fo rearm. Finally fold
the p oint o ver the elbo w and pin it in place (Figure 1.20).
Collar and cuff sling
This is used t o suppo rt the w rist. To a pply a collar and cuff sling, bend the ca sualty’s elbow to a
right a ngle. Pass a clove hitch round h is w rist. Move his forea rm across his chest w ith his f ingers
tou ching his oppo site shoulder. Tie the ends of the ba nda ge in the ho llow just ab ove the
collarb one (Figure 1.21).
Triangular sling
This keeps the ha nd w el l ra ised and , wi th a pad und er the arm, is used to treat a f racture of the
collar b one (Figure 1.22). Place t he ca sualty’s forearm across his chest so t hat his f ingers point
tow ards the shoulder and the centre of the palm rests on the breast bone. Lay an o pen banda ge
on the f orearm w ith one end (C) over the hand and t he point w el l beyond the elbow (A). Steady
the l imb and tuck the base of the banda ge w el l under the hand and f orearm so that the low er
end (B) may be brought under the bent e lbow and then upwards across the back to the
uninjured shoulder, where it is tied to end (C) in the hollow ab ove the co llar bo ne. The point o fthe ba ndag e (A) is then tucked wel l in , betw een the fo rearm and ba ndag e in f ront , and the f old
thus formed is turned backwa rds over the lower pa rt of t he upper arm and pinned .
12 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.20 Figure 1.21

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 9/40
Cha pt er 1 FIRSTAID 13
Improvised slings and supports
The aff ected ha nd or a rm can be supporte d, w hen no sling is readily ava ilab le, by simple
metho ds, some o f w hich are illustrate d in Figure 1.23.
Splints
Sets of splints of various lengt hs are included in ships’ stores. When pro perly applied to a limb,
they rel ieve pain by immobil ising the f ra cture and prevent further da mag e to the surrounding
muscles, blood vessels and nerves. The sharp end s of the bon e are prevent ed fro m piercing t he
skin and turning a closed f racture in to a n open f ra cture with i ts a t tendant dang ers.
When choosing a splin t i t should be long eno ugh a lmost to reach the join t below and t he
joint abo ve the site of t he fra cture. The only exception to this rule is the splint used in fracturesof t he th igh b one. This should be long enoug h to stretch f rom t he ankle to t he armpit .
All splints must be fixed to t he limb in at lea st four places – ab ove an d below the site of t he
f racture and at both ends. Although w ooden splin ts are general ly used in f i rst a id , subst itutes
can be used in emerg ency situat ions. These can be in the form o f suitably sized pieces of w oo d
or meta l , folded cardboard , new spapers or maga zines, or pieces of st ick or broom hand les
fastened tog ether to g ive the necessary wid th .
Whatever is used , the spl in t must be padded so that there is a layer of sof t ma teria l about
11/2 cm thick betw een t he splint a nd t he skin. Unpa dded splints w ill cause pa in and p ossible
dama ge to the skin .
Figure 1.23
Figure 1.22
A
C
B
CB

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 10/40
14 THE SHIP CAPTAIN’S MED ICAL GUID E
Inf latable splint s are a useful method for temporarily immobilising limb fractures but are
unsuitab le for f ra ctures which are more tha n a short d istance above the knee or e lbow as they
canno t pro vide sufficient immobilisat ion in these places. The splint is applied to the limb a nd
inf la ted by mouth . Other method s of in f la t ion can ma ke the splin t too t ight a nd thus slow
dow n or stop the circulation. Inflata ble splints can be a pplied over wou nd dressings.
The splints are ma de of clear plastic and a ny bleeding from a w ound ca n easily be seen.
Needless to say, all sharp objects and sha rp edg es must be kept w ell clear of the plastic to avoid
a puncture.
In f la tab le splin ts may be used to transport a pat ient a bout the ship or during moving to
hospital. They should not be left in place for more tha n a few hours. Other means of
immobilising the fra cture should be used af ter tha t period.
Remember that the sound leg is a very good splint to which an injured leg can be secured
pending more elaborate measures, and, similarly, the arms can be immobilised against the
trunk. If the pat ient is to be mo ved by Neil Robertson stretcher, no add itional splints may benecessary du ring first aid.
First aid satchels or boxes
These should conta in at least the items required by MSN 1726 for th e ‘f irst a id kit’ . One should
be kept close to the ship’s medical store for swift t ransfer to t he site of an a ccident . If you ha ve
more tha n one, t he other(s) should be placed aw ay f rom the medical store so tha t i f the store is
destroyed by fire you h ave a n ea sily reached first aid kit. These kits should be checked
freq uently and re-stocked as required.
Severe bleeding
lay the casual ty dow n;
press w here the b lood come s from, using a clean h and kerchief , dressing or cloth;
press w ith your hand o r f ist on t he w ound if not hing else is available. If possible we ar
disposable gloves.
if the arms or legs are wo unded , lif t th em up to a near vertical position a s this w ill help to
stop t he blee ding (Figu re 1.24);
tie a dressing firmly round the w ound t o maint ain the pressure;
i f b lood continues to come through the dressing, apply another banda ge on the top o f the
first one . Banda ge mo re firmly.
keep the injured part a s still as possible and t he casualty a t rest becau se movement d isturbs
(and destroys) the b lood clot;
aft er bleeding ha s been contro lled, rest the limb as show n in Figure 1.24;
this trea tmen t applies eq ually to bleeding from a n amput at ion site. Here pressure should
be applied over and a round the end of the stump.
Figure 1.24

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 11/40
Cha pt er 1 FIRSTAID 15
Unconscious casualty
The immediate t hreat to life may be:
breath ing obstructed by the tong ue fa l l ing ba ck and
blocking the throa t ;
stopped heart .
Check f or b reat hing at o nce – Look/Listen/Feel
look for movements of the chest and a bdomen;
feel for a ir on your cheek
l is ten for breath ing w ith your ear over the mouth and
no se (Figure 1.25);
not e the colour o f fa ce and lips – norma l or blue/grey
t inge?
I f breath ing:
place the casualty in the un conscious or recovery
po sition (Figure 1.26);
NOTE: no pillow s should b e used un der th e hea d;
pull up the leg a nd the a rm on the side to w hich
the he ad is facing, pull up the chin;
stretch ot her arm out as pictured
For subsequent t reatment of an unconscious
patient see Chapter 3 .
Not breath ing:
With the ca sualty lying fla t on his back, open t he airw ay
by making sure that the hea d is tilted ba ck w hilst lif ting
the chin upw ards a nd fo rwa rds (Figure 1.27), which will
move the tong ue forwa rd and clear the a irwa y.
Open the mouth a nd mop out any obvious obstruct ions
such as blood , vomit or secretions. If dent ures are wo rn
only remove them if they a re broken or displaced. Use
your f ingers, a hand kerchief or a clean piece of clot h.
These actions may relieve the obstruction t o brea thing .
The casualty may g asp and sta rt to brea the na tura lly. If so,
place in the unconscious position.
Sti l l not breath ing:
Begin a rtif icial respirat ion at once – seconds count .
Open the a irwa y by making sure tha t the head is t i lted
back whilst l i f t ing the chin upwa rds and forw ards.
w ork from the side in a convenient po sition;
pinch the casualty’s nose with your index finger a nd
thumb. Af ter tak ing a ful l breath , seal you l ips about t he
patient ’s mouth and b low in to h is mouth unti l you see
the chest rise. This should t ake a bout 2 seconds fo r full
infla tion . (Figure 1.28)
give tw o effe ctive inflat ions quickly, then not e if the
colour of t he fa ce and lips is improving.
Figure 1.25
Figure 1.26
Figure 1.27
Figure 1.28
The un conscious positio n

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 12/40
16 THE SHIP CAPTAIN’S MED ICAL GUID E
If there is improvement :
continue the a rt i f icia l respirat ion , mainta in ing a ra te of
about a do zen in f la t ions each minute . It ma y help your
t iming to count to f ive , s low ly, betw een in f la t ions;
see section abo ve on ‘If breat hing’.
If there is no improvement :
liste n fo r hea rt soun ds (Figure 1.29);
fee l the pu lse at t he ne ck (Figure 1.29);
I f no heart beat is fe l t , the heart has stopped . A tra ined
first-aider must begin chest compression at once. Unless
circulat ion is restored, the bra in will be w ithout o xygen andthe pe rson will be de ad in fo ur to six minutes:
the casualty must be lying on his back on a h ard surface,
e.g. deck, otherw ise the comp ression w ill be lost;
place your han ds tog ether a s show n in Figure 1.30;
press (1/2 second dura tion, 100 times a minut e) f irmly and
rapid ly on the middle of t he lower ha l f of the b reast
bone suf f icient to produce a dow nwa rd movement of
ab ou t 4 cm (Figure 1.31);
artif icial respirat ion (Figure 1.30) must a lso be carried ou t
w hen giving heart compression since breat hing stops when
the hea rt s tops. It can be g iven by o ne person, a l ternately
compressing 15 times and t hen filling t he lungs with a ir
tw ice or, ideally, by two people – one giving heart
compression and t he ot her giving artif icial respiration, a t a
ratio o f 5 chest compressions to 1 lung inflat ion;
i f the heart s tarts to beat the colour of the face and l ips
w ill improve a nd t he eye pup ils will get smaller;
listen ag ain fo r heart sound s and fee l for a neck pulse. If
they are hea rd , stop heart compression but continue w ith
artif icial respirat ion until natura l breathing is resto red.
When you are sat isf ied that the heart is beat ing and
unassisted breathing is restored, transfer the casualty by
stretcher, in th e unconscious position, to the ship’s hospital
or a cab in for further treatment . See Chapter 3 for continued
nursing ca re.
Unfortunately these measures are not always successful.
Failure to restart the heart after cardiac arrest is common
even in the best environment, such as a fully equipped
hospital. It may be necessary to decide to stop artif icial
respiration and chest compression. If in doub t SEEK RADIO
MEDICAL ADVICE.
Figure 1.29
Figure 1.31
Hard surface
Figure 1.30

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 13/40
Cha pt er 1 FIRSTAID 17
Burns and scalds
Clothing on fire
by far the b est wa y to put o ut a f ire on a person is to use a dry powd er f ire extinguisher at once;
i f a dry pow der ext inguisher is not a vai lab le , then lay the person dow n and smother the
f lames by wrapping h im in any avai lab le materia l (not ma de of man-made f ibre), or throw
buckets of wa ter over him, or use a ho se;
make sure a ll smouldering clothing is extinguished.
NOTE: The po w der from a f ire extinguisher will not cause much, if any, eye da mag e. Most
people shut their eyes tight ly if sprayed w ith pow der. Any pow der wh ich get s in the eye should
be w ashed out immediately a f ter the f i re ha s been extinguished and while cool ing is being
undertaken.
Heat burns and scalds
all heat burns should be cooled a s quickly as possible with running cold w at er (sea or fresh)
for a t least ten minut es, or by immersing in cold wa ter and keeping the injured part in
mot ion; cooling o f extensive burns (>15%) should be avoided as hypo thermia w ill result.
i f i t is not po ssib le to cool the burn on the spot , the casualty should be ta ken to w here
cool ing can be carried out ;
t ry to remove cloth ing g ently but do no t tea r of f any w hich adheres to t he skin ;
then cover the bu rned area s with a dry, non-fluffy, dressing w hich is larger tha n the burns
and ba ndag e in place;
further treatment as in Chapter 4 .
Electrical burns and electrocution
make sure you do not become t he next casualty w hen approa ching a ny person w ho is inconta ct with electricity:
if possible, switch off the current;
otherw ise , insulate yourself . Remove your w atch a nd rings, wear rubber boo ts or stand o n
an insulat ing mat , th ick DRY newspaper or w ood ;
alterna tively, pull the ca sualty from th e source of supply with a n insulat ed flex or push him
aw ay w ith a strong non-conductor, such as a piece of DRY woo d ;
check immediately for breath ing and heartbea t :
• i f not breath ing, g ive a rt i f icia l respirat ion ;
• if heart is sto pped, g ive chest compression a nd a rtif icial respiration;
send for help;
w hen the casualty is breat hing, cool any burned area s and a pply a clean, dry, non-fluffy
covering to the b urned area .
Chemical splashes
remove conta minated cloth ing. Drench w ith wa ter to w ash the chemical awa y;
carry on wa shing fo r a t least ten minutes. If you a re in any doubt t hat the chemical has been
completely cleared f rom the sk in , repeat t he w ashing for a further ten minutes;
give priority to w ashing the eye s if aff ected, as they a re particularly vulnerable to chemical
splashes. If only one eye is aff ected, incline the hea d to t hat side to p revent the chemical
f rom running across in to the other eye.
8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 14/40
18 THE SHIP CAPTAIN’S MED ICAL GUID E
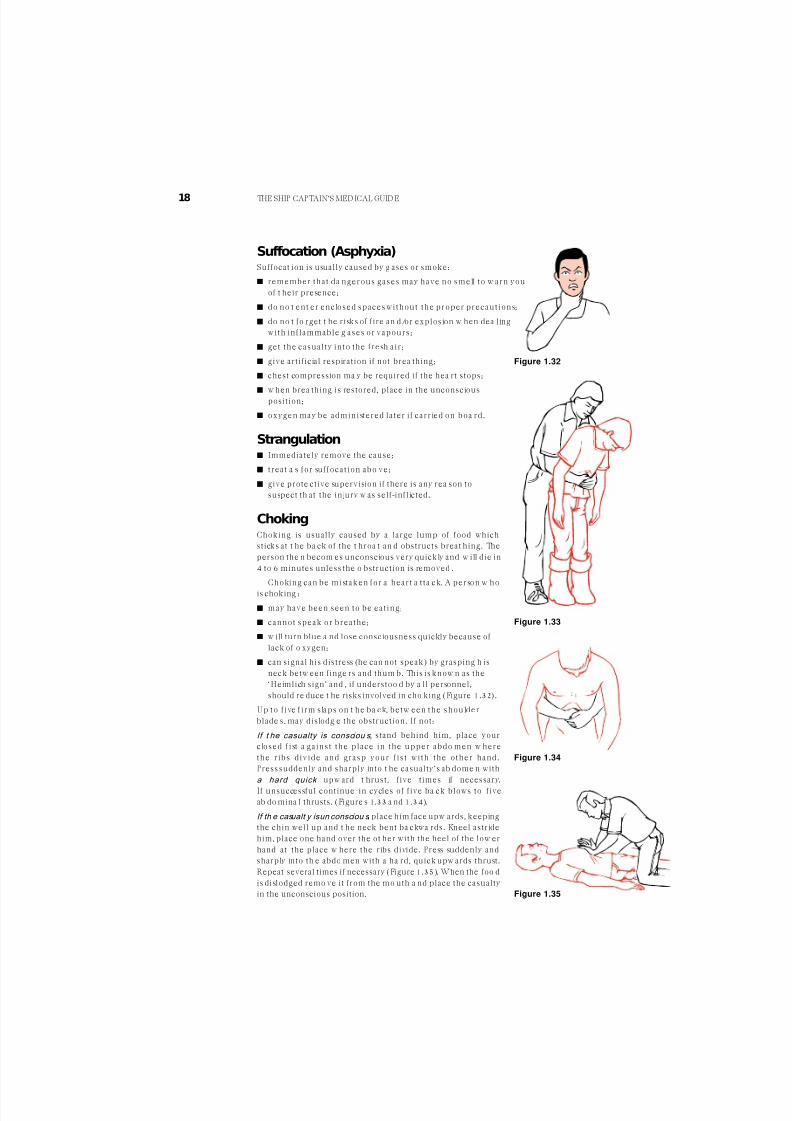
Suffocation (Asphyxia)Suffocat ion is usually caused by g ases or smoke:
remember that da ngerous gases may have no smell to w arn you
of t heir presence;
do no t ent er enclosed spaces without the proper precautions;
do no t fo rget t he risks of f ire an d/or explosion w hen dea ling
with in f lammable g ases or vapours;
get the casual ty in to the f resh a ir ;
give artif icial respiration if not brea thing;
chest compression ma y be required if the hea rt stops;
w hen brea thing is restored, place in the unconsciousposition;
oxygen may be administered la ter i f carried on boa rd .
Strangulation Immediately remove the cause;
t reat a s for suf focat ion abo ve;
give prote ctive supervision if there is any rea son to
suspect th at the injury w as self-inflicted.
ChokingChoking is usually caused by a large lump of food which
sticks at t he ba ck of the t hroa t an d obstructs breat hing. The
person the n becom es unconscious very quickly and w ill die in
4 to 6 minutes unless the o bstruction is removed .
Choking can be mistaken for a heart a t ta ck. A person w ho
is choking :
may have been seen to be eat ing;
cannot speak or breathe;
w ill turn blue a nd lose consciousness quickly because of
lack of o xygen;
can signal his distress (he can not speak) by grasping h is
neck betw een finge rs and thum b. This is know n as the
‘Heimlich sign’ and , if understoo d by a ll personnel,
should re duce t he risks involved in cho king (Figure 1.32).
Up to f ive f i rm slaps on t he ba ck, betw een the shoulder
blade s, may dislodg e the obstruction. If not:
If t he casualty is consciou s, stand behind him, place your
closed f ist a gainst the place in the upper abdo men w here
the ribs d ivide and grasp your f is t wi th the other hand .
Press suddenly and sharply into t he casualty’s ab dome n with
a hard quick upw ard t hrust, f ive times if necessary.
If unsuccessful continue in cycles of f ive ba ck blows to f ive
ab do mina l thrusts. (Figure s 1.33 a nd 1.34).
If th e casualt y is un consciou s , place him face upw ards, keeping
the chin well up and t he neck bent ba ckwa rds. Kneel astride
him, place one hand over the ot her with the heel of the low er
hand at the place w here the ribs divide. Press suddenly and
sharply into th e abdo men with a ha rd, quick upw ards thrust.
Repeat several times if necessary (Figure 1.35). When the foo d
is dislodged remo ve it from the mo uth a nd place the casualty
in the unconscious position.
Figure 1.32
Figure 1.33
Figure 1.34
Figure 1.35

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 15/40
Cha pt er 1 FIRSTAID 19
Epileptic fits – convulsions
The fit ma y vary from a mome nta ry loss of con sciousness (petit ma l) in which the pa tient ma y
sway but does not actual ly f a l l, to a ma jor a t ta ck (grand mal) as follows: the pat ient suddenly
loses consciousness and fa lls to the grou nd, possibly with a cry; he remains rigid for some
seconds, during which he stops breathing and the face becomes flushed; the convulsion then
starts with irregular, jerky movemen ts of the limbs, rolling of t he eyes, gnashing of t he teet h,
with perhaps some f roth ing a t t he mouth . He ma y lose control and pa ss urine or f a eces. Af ter a
variable time, but usually in a few minutes, the convulsion ceases and h e falls into w hat app ears
to be a deep sleep.
Treatment
prevent the p at ient from hurting h imself in the convulsive stag e;
never restrain him forcibly, as this may cause injury, but remo ve hard objects and surround
him by pillow s, cloth ing or ot her soft mat erial;
af ter t he fit is over, check for injuries. Assuming the pat ient is uninjured, let h im sleep it o ff .
He may be rather confused and dazed when he comes round . Reassure h im and do not
leave h im until you are sure he is awa re of h is surroundings and knows w hat he is doing.
In the event of the pa t ient having several f i ts , one af t er the o ther, i t may b e necessary to g ive
him an a nti-epileptic drug such as Diazepa m. SEEK URGENT RADIO MEDICAL ADVICE.
Shock and circulatory collapse
Shock occurs when the b ody’s circulato ry system is unable to distribute oxygen e nriched b lood
to a ll part s of the bod y. If untrea ted , the bod y’s vital orga ns (brain, heart , lungs, kidneys) can
fail, lead ing to collapse, unconsciousness and e ventua lly deat h.
Causes
The commo nest cause is loss of bo dy fluid from t he circulation. It can result, either fro m externa lor internal bleeding , (e.g. a s occurs in fractures of t he thigh ), the f orma tion of large blisters and
the w eeping o f f luid from large b urns and from d ama ged blood vessels in crush injuries. Shock
can also be found in severe heart attacks, and in certain diseases characterised by excessive
vomiting and d iarrhoea.
The first-aider should a lwa ys be on t he look-out fo r this condition as it can de velop even
w hile the ca sualty is under close observation a nd it ma y be missed. Fear, pain an d exposure to
cold make shock worse.
Symptoms and signs
The pa tient:
w ill usually lie still, ta king little not ice o f his surroundings
w ill complain of fe eling fa int, cold and thirsty. He may shiver;
his l ips and t he edg es of the ears may be b lue;
his skin w ill be pa le, cold and clamm y;
his pulse will be rap id and w eak;
his respirat ion w ill be rapid and shallow a nd, as shock deepens, he will give freq uent sighs;
he may start to vomit ;
if untreat ed, he may lapse into unconsciousness and la ter die.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 16/40
20 THE SHIP CAPTAIN’S MED ICAL GUID E
Treatment
The primary aim is to t reat w hat ever condition is causing the shock;
lay the pat ient f la t and , i f in juries permit , e levate the feet a nd legs so tha t b lood f lows to
the hea rt and b rain (see note below on exceptions to this rule);
do no t mo ve him unless in a posi t ion of da nger;
stop a ny bloo d loss. Cover burns a nd scalds. Immob ilise fra ctures.
loosen any tight clothing w hich restricts breathing mo vement;
keep wa rm but do not overheat .
deal w i th any pa in . Morphine may be g iven a s necessary
give small sips of w at er if t here is no suspicion of ab domina l injury but NEVER give fluids to
an unco nscious casua lty. A ba dly burned or scalded person ma y require much more fluid; move to a place of safet y as gently as possible. Roug h hand ling w ill increase the pa in and
the sho ck.
Exceptions to the lay flat rule:
if there is an injury to t he fa ce, mouth or jaw w ith a lot o f bleeding, place in the unconscious
posit ion with the head t urned with the d amag ed side underneath a nd , i f possib le , wi th a
head -dow n tilt. This w ill prevent bloo d running dow n into the t hroat and lung s;
if there is a pene tra ting w ound o f the chest, or if breathing is diff icult, prop up to a ssist
breath ing;
if unconsciousness occurs, put into t he unconscious position w ith as little disturbance a s
possible to t he injured part.
Bleeding
External bleeding
Bleeding from small blood vessels occurs when there is a minor cut o r abra sion o f the skin. Bloo d
ooz es from the w ound ; it usually stops by itself or w hen a d ressing is applied. It is gene rally of
no consequence.
In large a nd deep w ound s, the bloo d w ells up in a stea dy stream. The volume of bloo d loss
depends on the number of b lood vessels dama ged a nd , a l though i t may appea r a larming, i t is
not usually dange rous, unless allow ed to continue.
When large arteries are damag ed , bright red b lood w ill spurt f rom the w ound in t ime with
the heart bea ts. This bleeding is usually profuse a nd t he pa tient’s life w ill be end ang ered. This is
a ra re situat ion .
In all cases of external bleeding, fo llow the t hree cardinal rules:
lay the pat ient dow n;
lif t up th e aff ected pa rt if possible;
press f irmly w here the b lood come s from. Use a d ressing or a clean cloth o r hand kerchief
but, if non e should be a vailable, use the ba re hand or f ingers. When po ssible disposab le
gloves should be wo rn to protect yourself .
This procedure w ill stop the flow of b lood.
When b leeding ha s been controlled , apply a standa rd dressing to the w ound a nd ba ndag e
firmly and w idely in position. There may be a slight sta ining of bloo d throu gh t he dressing,
which is of little consequence, but if blood soaks quickly through the pad it is a sign that the
bleeding ha s not been prop erly controlled. If this hap pens, do not d isturb the d ressing, but put
ano ther stand ard dressing o n top a nd ba nda ge mo re firmly. This w ill usually stop t he bleeding.
Very occasionally, a third dressing may be req uired.
Do not d isturb the d ressings until you are prepa red to und erta ke definitive treat ment . The
bleeding stops because of the fo rmation of a clot . I f you remove t he dressing, the clot w i ll break
and b leeding w ill start a ga in .

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 17/40
Cha pt er 1 FIRSTAID 21
Special types of external bleeding
From an op en fracture
The bleeding comes mainly f rom a round the break and not f rom
the bone.
do no t a t tempt to elevate t he part , th is wi ll cause further pain
a n d d a m a g e ;
app ly a dressing, sterile if possible, padd ing aro und th e
w ound . Firm banda ging w ill apply the necessary pressure to
the t issue around the exposed bo ne ends.
From a t oot h socket:
The socket may bleed a fte r the extraction o f a t oo th. Thiskind o f bleeding is seldom serious. At least tw o-thirds of t he
‘blood ’ which is spat o ut w ill be saliva, so the b lood loss is
unlikely to be great ;
i f the gum ma rgins are splayed out , squeeze them g ently
tog ether to close up the to oth socket ;
fold a piece of ga uze tightly and place it in the socket so tha t it
is standing proud o f the level of the remaining t eeth;
the casua lty should close his mouth, biting firmly on th e ga uze
in the to oth socket. The pressure should be ma intained f or
20 minutes. If the socket is still bleeding o n remo ving the
ga uze pad , the procedure should be repeated a s of ten as is
necessary (Figure 1.36).
From th e ear passage:
This is usually caused b y a he ad injury or by bla st:
place a large pad over the ea r and ba ndag e i t in posi t ion ;
keep the af fected ear downw ards;
if the casualty is unconscious, place in the unconscious
posit ion with the af fected ear downw ards;
never plug the ea r passag e with cotto n wo ol or other mat erial.
From the n ose:
the casual ty should si t wi th h is head o ver a ba sin or bo wl
w hile pinching the soft part o f his nose firmly for 10 minutes;
(Figu re 1.37);
he should then release the pressure slowly;
i f b leeding ha s not stopped , he should repeat the ma noeuvre
for a furthe r 10 minutes;
it might be necessary to do t his for a t hird time;
if bleeding has not stoppe d af ter half-an-hour, it might t hen be
necessary to pa ck the no se with ribbon g auz e. (See Chap ter 4)
From the l ips, cheek and to ngue:
press on bo th sides of th e lip, cheek or to ngue t o stop
bleeding;
use a piece of ga uze or a swa b on each side to help mainta in
pressure a nd stop the fingers slipping (Figure 1.38);
pressing is usua lly most ea sily done b y the casua lty with
direction from ano ther person, or helped by looking in a mirror.
Figure 1 .36
Figure 1.37
Figure 1 .38
A
C
B

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 18/40
22 THE SHIP CAPTAIN’S MED ICAL GUID E
Internal bleeding
Internal bleeding may be caused by injury, disease, or by the action of certain poisons. Any
severe injury to t he bod y will cause bleeding of va rying degree . Bleeding ma y be limited to the
soft tissues, such as muscles, but w hen a bone b reaks there is alw ays bleeding a t the fracture
site. Minor injury will aff ect only the superficial tissues and th e bleeding may b e limited to sma ll
amo unts w hich will app ear a s bruising. Grea ter force w ill result, in addition t o bruising, in the
forma tion of a collection of bloo d w ithin the deepe r tissues (a haema tom a). This causes painful
swelling of the a f fected part and may be d i f f icult t o d ist inguish f rom a f racture . Whatever the
nat ure of such injuries, the bloo d loss very rarely enda ngers life.
In cont rast, bleeding from injury to interna l orga ns is alw ays very serious and ma y quickly
enda nger life. Such bleeding is alw ays concealed and its presence has to be ded uced from th e
histo ry of th e injury, a rising p ulse rat e an d th e signs and sympto ms of shock which occur rapidly.
The abd ominal organs are poo rly protected by the abdo minal wal l and t hey are part icularlyliab le to injury by d irect o r crushing f orces. These interna l injuries require expert t reat ment
urgently and every ef fort must be made to del iver the casual ty to medical care . Alwa ys get
RADIO MEDICAL ADVICE. There is l it t le tha t can be do ne ab oard because a b lood transfusion
may be needed .
If internal bleeding is suspected:
put in bed with a head-down t i l t ;
if conscious an d in pa in or restless, give morph ine 10 mg;
cover with only one b lanket ;
record the pulse rate at 10 minute intervals. A fa lling rate ma y indicat e tha t the b leeding
ha s sto ppe d (Figure A);
give fluid per rectum (Chapter 3);
if the injury is abd omina l, allow the pa tient t o suck flakes of ice. With bleeding fro m oth er
parts of the b ody, sips of w ater ma y be given;
trea t for shock.
Coughing up or vomiting blood
NOTE: remember tha t bleeding ca n occur from the ba ck of t he nose, a t oot h socket, bleeding
gums, e tc . It is important that th is should not b e confused with b leeding f rom the stomach or
lungs.
Coughing up of blood
In some lung diseases and cases of injury to t he chest, blood ma y be coug hed up. Except in cases
of injury this is seldom fa ta l.
Treatment is the same a s for in ternal b leeding w ith the exception tha t t he pat ient should be
placed at rest with the head and shoulders raised. It is not usually necessary to give fluid per
rectum. For furth er care see Chapt er 4.
See Examinat ion of sputum (Chapter 3).
Vomiting blood
Blood may be vomited i f the stoma ch is in jured by a wo und of the a bdomen o r i f b lood collects
in the stoma ch as a result of a bleeding pep tic ulcer. In the lat ter case the pa tient ma y sudde nly
vomit a quantity of dark brown fluid like coffee grounds. He feels faint and looks pale. If the
bleeding a nd vomiting cont inue he w ill suffer increasingly from shock.
Treat ment is the same a s for internal bleeding. For further trea tment of t his condition, see
Chapter 7 . If there is a wo und of t he abd omen, th is should be treat ed .

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 19/40
Cha pt er 1 FIRSTAID 23
WoundsA wound at any si te in the body poses three problems:
control of b leeding;
prevention of shock
prevention of in fect ion
There a re some simple rules:
never wash the w ound – except in cases of a n animal b i te
never try to remove pieces of meta l or glass from a w ound un less they a re superficial and
can be ea sily lif ted o ut. If pieces can be removed , do it by g rasping the ma terial with sterile
ga uze or use sterile forceps, if available;
do not po ur ant iseptic in to a w ound;
as soon as possible, cover the w ound w ith a suitable dressing.
Bullet or metal fragment wounds
In this type o f injury, loo k for and trea t a ny exit wo und. This is usually larg er tha n the e ntry
wo und. Remember that there may be underlying bo ne f ractures and t hat the bul let or metal
f ragment may ha ve been def lected f rom t he bone t o cause serious in ternal damage, t he only
signs of w hich may be increasing shock.
Figure A Haemorrhage – the falling temperature and the rising pulse rate

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 20/40
24 THE SHIP CAPTAIN’S MED ICAL GUID E
Chest wounds
A superf icia l chest w ound should be treat ed a s for any w ound elsewhere but a penetrat ing
wo und (a sucking wo und) of the chest must be sealed immediately , otherw ise air is draw n into
the chest cavity and the lungs cannot inflate as the vacuum inside the chest is destroyed.
A useful dressing fo r a sucking w ound ca n be mad e from a pa raff in ga uze dressing. Place the
paraf f in gauze o ver the wound, smooth the foi l on to the chest wal l and seal three edges only
w ith zinc oxide adh esive plaster. In emerg ency, a suita ble dressing may b e improvised fro m
petroleum jelly, gauze and kitchen foil or polythene or, alternatively, a wet dressing may be
used to provide a n airtight sea l. If not hing else is available, use the casua lty’s ow n blood stained
clot hing to p lug the w ound t empo rarily. The aim is to prevent air entering t he chest but to
allow it to escape if necessary.
The usual rules ab out sto pping bleeding b y pressing w here the bloo d comes from also apply.
Start a p ulse chart soon t o check on p ossible interna l bleeding in a ll chest injuries. The
respirato ry rate shou ld also be recorded . See also sections on chest injuries.
Conscious casualties should be placed in the half-sitting-up position because breathing is
easier in this position.
NOTE: DO NOT GIVE MORPHINE to a pat ient w i th th is type of w ound, even i f he is suf fering
from a lot of pa in, as the morphine will increase the b reat hing diff iculties.
G e t RADIO MEDICAL ADVICE.
Abdominal wounds
A superficial abdominal wound will require the
same treatment a s any wound, but for more serious
wo unds, if the a bdominal contents do not pro t rude ,
cover the w ound w ith a large standard dressing and
place the casualty in the half-sitting-up position
(Figure 1.39). In t his position t he w ound w ill not
ga pe ope n. As the ab dom inal muscles are slack, the
abdo minal contents w i ll not bulge t hrough. I f the
w ound runs more or less vertically, it may b e best to
lay the man f la t .
If the abdo minal contents do pro t rude th rough
th e w oun d , DO NOT ATTEMPT TO PUT THEM BACK.
Cover with a loo sely applied large sta nda rd dressing
or dressings until further treatment can be given.
Shock w ill develop quickly and shou ld be trea ted a s
described previously, with the following important
exceptions:
prop up if ne cessary;
DO NOT give anything by mouth.If thirsty, the lips should be mo istened ; not hing mo re.
(See a lso Crush w ounds and Stab w ounds below) .
G et RADIO MEDICAL ADVICE.
Head wounds
The w ound i tself should be treated in the same w ay a s any other w ound. Scalp wo unds of ten
bleed briskly. A firm bandage will usually arrest the bleeding, but some ingenuity may be
required in applying the ba ndag e so as to keep it f i rmly on the head and t ransmit the necessary
pressure to the pad. Firm pressure by the fingers over the pad for a few minutes before it is
f inally f ixed in position will help to stop th e bleeding.
The possibility of bra in dama ge is of grea ter importa nce and t w o rules should be observed:
morphine should be given only if conscious an d in much pain fro m more serious injuries
elsewhere;
if unconscious, put in the unconscious position and give the t reat ment d escribed in
Chapte r 4.
G et RADIO MEDICAL ADVICE.
Figure 1.39
8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 21/40
Cha pt er 1 FIRSTAID 25
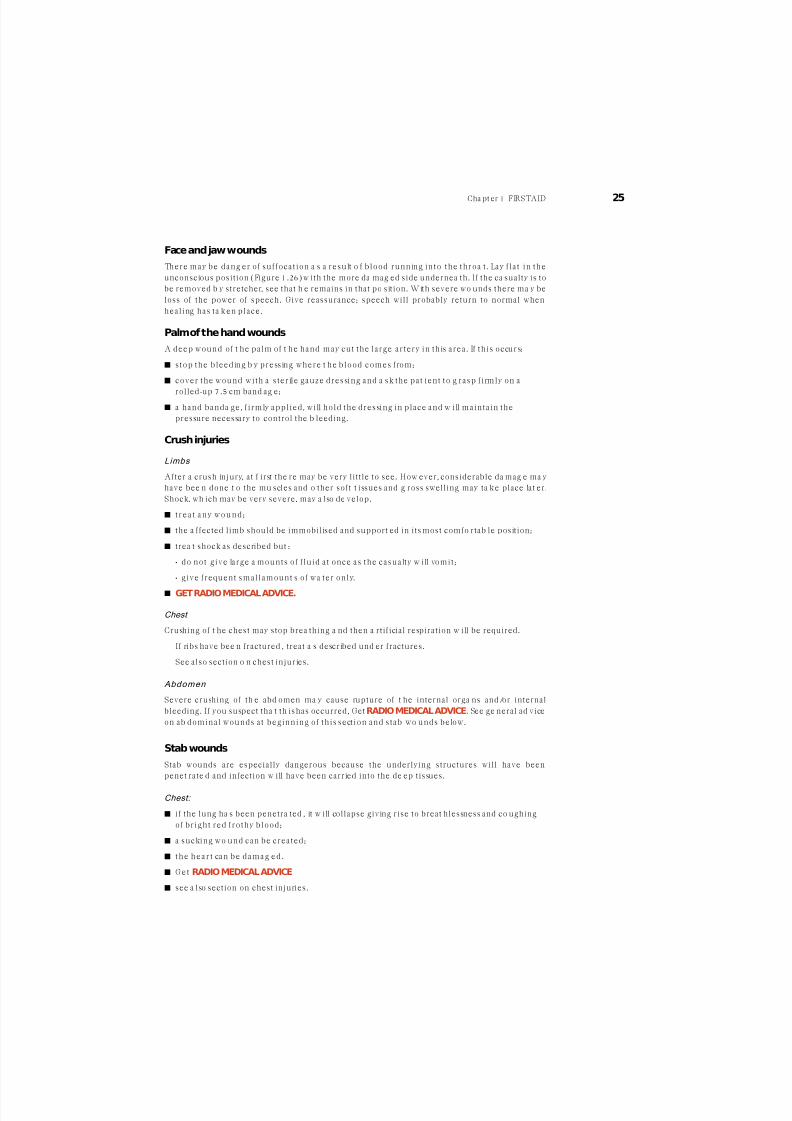
Face and jaw wounds
There may be dang er of suf focat ion a s a result o f b lood running in to the throa t . Lay f la t in the
unconscious position (Figure 1.26) w ith the more da mag ed side undernea th. If the ca sualty is to
be removed b y stretcher, see that h e remains in that po sition. With severe wo unds there ma y be
loss of the power of speech. Give reassurance; speech will probably return to normal when
heal ing has ta ken place.
Palm of the hand wounds
A deep wound of t he palm of t he hand may cut the large artery in th is area . If th is occurs:
stop the b leeding b y pressing where t he b lood comes f rom;
cover the wound with a sterile gauze dressing and a sk the pat ient to g rasp f i rmly on a
rolled-up 7.5 cm band ag e;
a hand banda ge, f i rmly applied , wi ll hold the dressing in place and w ill maintain the
pressure necessary to control the b leeding.
Crush injuries
Limbs
After a crush injury, at f irst the re may be very little to see. How ever, considerable da mag e ma y
have bee n done t o the mu scles and o ther soft t issues and g ross swelling may ta ke place lat er.
Shock, wh ich may be very severe, may a lso de velop.
t rea t an y w oun d ;
the a ffected limb should be immobilised and support ed in its most comfo rtab le position;
trea t shock as described but :
• do not g ive large a mounts of f luid a t once as the casualty w i ll vomit ;
• g ive f requent small amount s of wa ter only.
GET RADIO MEDICAL ADVICE.
Chest
Crushing of t he chest may stop brea thing a nd then a rtif icial respiration w ill be required.
If ribs have bee n fractured , treat a s described und er fractures.
See also section o n chest injuries.
Abdomen
Severe crushing of th e abd omen ma y cause rupture of t he internal orga ns and/or internal
bleeding. If you suspect tha t th is has occurred, Get RADIO MEDICAL ADVICE. See ge neral ad vice
on ab dominal wounds at beginning of th is sect ion and stab wo unds below.
Stab wounds
Stab wounds are especially dangerous because the underlying structures will have been
penet rate d and infection w ill have been carried into the de ep tissues.
Chest:
if the lung ha s been penetra ted , it w ill collapse giving rise to breat hlessness and co ughing
of bright red f rothy b lood ;
a sucking wo und can be created ;
th e h ea r t can b e d am ag ed .
G et RADIO MEDICAL ADVICE
see a lso section on chest injuries.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 22/40
26 THE SHIP CAPTAIN’S MED ICAL GUID E
Abdomen
Depending o n the position of the w ound (see Anat omy Diagra ms, Annex II), an org an ma y be
pierced, giving rise to pe ritonitis and internal bleeding. See genera l advice at b eginning o f this
section. Get RADIO MEDICAL ADVICE.
Limbs
Muscles, nerves and b lood vessels may b e cut. Bleeding, bo th interna l and e xternal, w ill occur.
Whatever the si te of the stab w ound, the immediate trea tment is the same:
stop externa l bleeding by pressure
prevent furth er infection by applying suita ble dressings
trea t shock if necessary.
Fractures
A fracture is a broken bo ne. The bone ma y be broken into tw o or more pieces w ith separat ion
of the f ragments or i t may ha ve one or more f issured cracks without any separat ion .
Most f ractures are caused by d irect fo rce, but fo rce may be transmit ted through t he body t o
cause injury indirectly elsew here. Tw o classical examples are: a fa ll on the o utstretched hand ,
causing a f racture of the col lar bone; a nd a f a l l f rom a height on to the heels, causing a f racture
of th e ba se of the skull.
A much less commo n type is a stress fracture. The bo ne become s wea kened in a w ay
comparable to met al f a t igue. Sudden, strong muscular ef fort may snap the bone.
In simple terms, a fracture ma y be ope n to infection or closed to infection.
A closed fracture
There is no communicat ion bet ween the f racture a nd the surface of the bo dy.
An open fracture
There is communicat ion b etw een a skin wound and the f racture . Open f ractures are a lwa ysserious because germs may enter through the w ound t o cause in fect ion of t he broken bone a nd
the surround ing tissues.
NOTE: A skin w ound may b e present bu t, unless it is deep eno ugh t o rea ch the b roken bon e,
the fracture is still closed. Open or closed fra ctures are somet imes complicated b y d am age to
importa nt structures such a s the bra in, lung , blood vessels or nerves.
Principles of treatment
It is not possible to set fractu res on bo ard ship. Indeed , many fractu res may not req uire sett ing
and unskilled attempts might prejudice healing. First aid measures should ensure adequate
immobil isat ion . Wherever a f racture case has to be kept on b oard f or more tha n tw o or t hree
days, the join ts above a nd below the f racture site should be gent ly put through a ful l range o f
movements, morning a nd night .
Lasting d ama ge ma y result if a joint surface is involved in the fra cture and in a ll cases w here
this is suspected , RADIO MEDICAL ADVICEmust be sought .
Antib iot ic treatment must a lwa ys be given as soon as an open f racture is d iag nosed or
suspected.
Examination
The follow ing signs and sympto ms will indicat e tha t the b one is proba bly broken:
a hea vy b low o r other force has been applied to the body o r l imbs. The casual ty or others
may have heard the bone break ;
intense pain, especially on pressure or moveme nt a t the site;
swelling. The site ma y be sw ollen and /or bruised. This may be d ue t o inte rnal bleeding ;
loss of use. The casualty ma y be una ble or unw illing t o use the injured part because of the

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 23/40
Cha pt er 1 FIRSTAID 27
pain. He may a lso experience severe pain if an a tte mpt, even very gent ly, is mad e to h elp
him make the m ovement . Wat ch his fa ce for signs of pa in. Occasionally, if the broken end s
of a bone a re impacted tog ether, the person may be a b le to use the part but usual ly only
with a f a ir amount o f pain ;
distort ion . Compare goo d a nd ba d l imbs or sides of the body to see if the part is swo llen ,
bent , tw isted o r shortened ;
irregularity. The irregular edg es of a b roken bone ca n sometimes be seen in an ope n
fracture. They ma y be seen o r felt unde r the skin in a closed fra cture;
unnatural movement and grat ing of bo ne ends. Neither of these symptoms should be
sought del iberately. A limb may feel l imp and wo bbly and g rat ing ma y be fe l t w hen trying
to a pply support t o the limb. In either of the se situat ions, the bone is certa inly broken.
General treatment
bleeding should be treated as described ;
rest the a ffected p art b y immobilisation. This prevents further da mag e, relieves pain and
stops further bleeding;
all fractures or suspected fra ctures must be immobilised before ma king a ny att empt t o
move th e casualty. This can be d one using w oo den, improvised or inflat ab le splints, or by
fixing a limb to the bo dy, or – in the case of t he legs – by lashing o ne to the o ther.
Immobilise a limb in t he po sition in w hich it is
found, if it is comfortable. If it does become
necessary to move an injured limb, because of
poor circulation or for any other reason, f irst
apply traction by pulling the limb gently and
f irmly aw ay f rom the body before a t tempting to
move it (Figure 1.40).
Keep pulling until it has been securely
immobilised and then release the traction veryslow ly. Sudden release can ca use pain.
Circulat ion of the blood in a f ractured l imb.
Check that the circulation t o t he limb is intact. To
do t h is, press on the na i l of t he thumb o r of the
big toe. When circulation is normal the nail
becomes white when pressed and pink when
released. Continue checking until you are
satisfied that all is w ell. Dang er signs are:
blueness or w hiteness of f ingers and to es;
coldness of the parts below the f racture ;
loss of f eeling below the injury. Test for t his by touching lightly on f ingers and toe s and
asking the casual ty i f he can feel anything;
ab sence of pulse.
If there is any do ubt a t a ll ab out the circulation, loo sen all tight an d limb-encircling d ressings
at once and stra ighten out the l imb, remembering to use tract ion when doing so. Check circulat ion again. If the l imb does not become pink and w arm and you cannot detect a pulse ,
then medical help is urgently necessary if amputation is to be avoided. Get RADIO MEDICAL
ADVICE.
remember tha t fractures can cause severe internal
b leeding ;
alwa ys look for and treat for shock;
morphine may be necessary to control pain.
Figure 1.40

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 24/40
28 THE SHIP CAPTAIN’S MED ICAL GUID E
Collar bone, shoulder blade and shoulder
Fractures in these areas are of ten t he result either of a fall on
the o utstretched ha nd o r a f a l l on to the shoulder. Direct
violence to the parts is a less common cause of these
fractures.
P lace loose padding about the size of a f is t in to the
armpit. Support the arm u sing a triang ular sling (Figure 1.41).
Then t ie the arm to t he body, using a narrow fold banda ge.
Keep the casualty sitting up as he will probably be most
comfort ab le in this position.
Upper arm
Upper arm f ractures are usua lly caused by direct violence.Bind the upper arm to the body, using a broad fold
banda ge. Bend the elbow gently and a pply a col lar and cuf f
sling (Figure 1.42). Keep t he casua lty sitting up so t hat the
weight o f the a rm can supply tract ion to the lower f rag ment .
Alterna tively, upper a rm fractures ma y be splinted . Bend
the elbow gently. Use three well padded splints. Place one
behind the upper arm, one in f ront and t he th ird f rom the t ip
of th e shoulder to the elbow . Banda ge th e splints securely in
place. Support the a rm with a collar and cuff sling (see also
Fig ure 1.21).
Elbow
Fractures in this area can be e specially dang erous because of
damage to b lood vessels and nerves around the elbow.
Check circulation a nd fe eling in the fing ers. If th e f inger t ips
are w hite or b lue and feel ing is absent or a l tered , the elbow
must be straight ened a t once. Tell the casua lty to lie dow n.Be gentle . Apply tract ion o n the ha nd and forearm. Bring t he
arm and forearm slowly and carefully to the casualty’s side.
Now place plenty of loose padding betw een the arm and t he
body and also around the a rm. Then b ind the forearm to the
bod y by encircling ties. Check the circulat ion ag ain w hen you
have m ade the encircling t ies. If the circulation is poor, the
ties should be loosely secured until the casualty has to be
move d (Figu re 1.43).
Figure 1.42
Figure 1.43
Figure 1.41

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 25/40
Cha pt er 1 FIRSTAID 29
Forearm and wrist
Fractures in this area commonly result from a fall on the o utstretched hand. Bend the elbow until
the f orea rm is across the bod y. Then a pply an a rm sling (Figure 1.20). Remove an y finge r rings.
Later , apply two wel l padded splin ts to the back and f ront of the fo rearm and secure f i rmly,
using na rrow fo ld banda ges. Support the arm w ith a broa d a rm sling. For f ractures of the w rist
bones, put a broad , w el l padded spl in t on the f ront o f the forearm and t he palm of the hand .
Put plenty of padd ing on the b ack of the fo rearm and ha nd and secure. Use a broad arm sling
for support .
Hand and fingers
Fractures of the hand bones (metacarpals) and the f inger bones are a common resul t of
shipboa rd accidents and expert t reatment may be many da ys awa y. As f ixat ion in a stra ight
splint is only permissible for a short time, the t reat ment de scribed in the following pa rag raphsshould be undertaken i f the casual ty has to be kept on board . Always remove rings
immediately.
The hand bon es (met acarpals):
apply a crepe bandag e around the ha nd and w rist f irmly enough to support the injured
part but not so t ight a s to prevent movement of the w rist and f inger join ts ;
check tha t circulation t o th e fingers is present;
elevate the ha nd by placing the a rm in a t r iang ular sl ing to reduce the swel ling;
encourage t he casual ty to mo ve the w rist and al l the f inger join ts f requently.
The fingers:
strap the f inger to t he ad jacent f inger, using zinc oxide
ad hesive pla ster (as show n in Figure 1.44);
be careful that you do not prevent movement of the
finger joints. Do not put t he plaster directly over thefracture ;
to a void swel l ing, e levate the ha nd by putt ing the a rm in
a triang ular sling;
encourage t he casual ty to mo ve al l the f inger join ts .
Open fracture of t he f ingers:
stop the b leeding and apply a dressing to the w ound;
if the dressing prevents strap ping to th e adjacent f ing er,
use as a splint, a strip of aluminium or other soft met al
2 cm w ide and long enoug h to stretch f rom the t ip of the
f inger to just below the w rist join t ;
immob ilise the finge r in the position show n in Figure 1.45.
This is don e by bend ing the splint to conf orm w ith the
joints , using the same f inger of the unda maged hand a s a
pat t ern , and ta k ing care to ensure tha t the splin t wi l l notd ig in to the ba ck of the ha nd or in to the w rist ;
pad the spl in t w i th tw o layers of e last ic adhesive
banda ge a long i ts length . Turn the ba ndag e over the
ends to prot ect the skin;
f ix the splint to t he finge r with zinc oxide plaster cut to
suitable widths;
give stand ard a ntib iot ic treatment .
Figure 1.44
Figure 1.45

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 26/40
30 THE SHIP CAPTAIN’S MED ICAL GUID E
Crush injuries to t he hand
Severe crushing injuries to the hands may cause multiple open or closed fractures of the
metacarpal or f inger bones. Other wo unds are l ikely to be present .
stop the bleeding a nd apply dressings;
pain w ill be severe. Give ana lgesics (Morphine if necessary);
if hospita l treatme nt is not a vailable quickly, read th e section on def initive treat ment of
wo unds and t reat a ccord ingly.
Hip to knee
A broken thigh b one is a po tent ially serious injury. It cau ses significant internal bleeding into
the mu scles of the t high a nd, w ith the a ssociated pain, shock very quickly develops. If it iscombined with other serious injuries, the blood loss may be so great as to require blood
replacement. Get RADIO MEDICAL ADVICE.
a brea k of the neck of the t h igh bone causes shortening of t he injured leg and t he casual ty
w ill lie with the w hole low er limb a nd foo t f lopped o utw ards. There w ill be severe pain in
the region of the h ip;
f ractures of t he shaf t of the th igh bo ne exhib i t the usual s igns and symptoms of a f racture .
Severe pain is a no rmal fea ture.
If you th ink tha t the t high is broken:
f irst, pad betw een the t highs, knees, calves and an kles, using folded b lankets or any oth er
suitable soft material;
bring t he go od leg to the broken leg . Do t h is slow ly and careful ly ;
bring t he feet tog ether. I f a t tempting to d o t h is causes pain , apply tract ion to t he injured
leg gently and slowly, and t hen try ag ain ;
t ie encircl ing b anda ges: around bo th feet ; hal fwa y betw een the knees and the a nkles; justabove t he knees; and at the upper th ighs. Avoid making a ny t ies over the site o f the
fra cture (Figure 1.46);
the shoe on the a f fected side can no w be removed so tha t you can check the circulat ion in
the t oes – i f necessary, loosen any b anda ges – and then replace the f igure-of-eight ba ndag e
around the a nkles and feet ;
t reat for shock and pain – morphine w ill be needed .
Kneecap
This fracture ma y be caused by direct violence or as a result of a sudden stress on the b one.
It is commo nly a closed fractu re. When a n open fra cture occurs, the w ound shou ld be treat ed
before spl in t ing is undertaken and antib iot ic treatment should be given .
place the casua lty in a half-sitting-up position and put supports behind his back to ma intain
this. Raise the leg a nd hold it in a comfort ab le position.
Figure 1.46

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 27/40
Cha pt er 1 FIRSTAID 31
choose a splin t long eno ugh to reach f rom the buttock to beyond t he heel , pad i t w el l and
apply it a long the back of the leg . Put addi t ional padding behind the hol low a t the heel so
as to l if t i t o f f the splin t , and a lso behind the knee;
secure the spl in t in place with ba ndag es round the t h igh , round the low er leg just below
the knee and w ith a f igure-of-eight banda ge a t the a nkle , and elevate the leg on a suitab le
suppo rt (Figure 1.47).
When th e casualty is moved t o th e cabin or to the ship’s hospital, he should be kept in a sitting
posit ion w ith the leg elevated .
When medical at tent ion will not be ava ilab le for some time and it is obvious tha t the re is a
wide ga p betw een the f rag ments of the knee cap, carry out the procedure described a bove, but
put a f igure-of-eight ba ndag e round t he knee, beginning a bove the knee cap and f in ishing
over pa dding app lied just below it (Figure 1.48).
This method w ill draw the f rag ments toget her and ho ld them in place. Check that the
circulat ion is inta ct.
Knee to foot
Low er l imb
These should be t reated in the same w ay a s f ractures of t he th igh . See a lso below for f ractures
of bot h legs.Ankle
An ankle fracture which is stable and
without any deformity can be given
adequate but temporary f i rst a id by
placing the injured ankle on a
number of pi l low s to keep i t a t rest
(Figu re 1.49).
In more serious fractures of the
ankle it is usual to f ind a g ood deal of
defo rmity and swelling, and splinting
may b e necessary.
remove th e casualty’s shoe an d sock;
obta in two spl in ts , long eno ugh to stretch f rom just below the knee to the sole of the foo t .
Pad these wel l to a l low fo r the deformity and swelling, and apply them to bo th sides of the
leg;
f ix them in place with a f igure-of-eight b anda ge t o the foot and place other ba ndag es just
below the knee and a bove the ankle ;
check tha t t he circulation is intact.
Heel bone
These fractures usually occur w hen the casualty ha s fallen from a h eight a nd land s on his heels.
As force has been t ransmitted upw ards, there ma y be mo re serious fractures elsew here, e.g. spine
and b ase of t he skull, and the pa tient should be ca refully examined t o exclude these.Treat a s
above, for f ractures of t he ankle .
Figure 1.47 Figure 1.48
Figure 1.49

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 28/40
32 THE SHIP CAPTAIN’S MED ICAL GUID E
Bones of the f oot
Severe injuries are usually the result of he avy w eights being
dropped on to unprotected feet or of crushing. Fractures of the
toes may occur when they a re stubbed aga inst some hard o bject .
remove the bo ot o r shoe a nd the socks carefully;
t rea t an y w oun d .
keep the foot e levated and use pi llows to keep i t in a
comfortab le posit ion .
Both legs
As there is no g ood leg to act a s a splin t for the o ther, external
splinting w ill have to be used. There ma y be considerable bloo dloss if bot h legs are broken.
have w ell padded splints ava ilable. These should reach fro m
the th igh to the ankles on the o utside of bo th the legs for
below t he knee f ractures, and f rom the a rmpit to the a nkles
for ab ove the knee f ractures;
pad betw een the th ighs, knees, calves and ankles;
bring bo th feet tog ether as gently as you can , using tra ct ion
if necessary.
t ie a f igure-of-eight ba ndag e round the feet a nd a nkles to
keep the feet tog ether;
apply the padded splin ts to t he outside of bot h legs;
t ie enough encircl ing b anda ges to keep the splin ts and the
legs secured firmly tog ethe r. Avoid making a ny ties over the
site of a ny brea k (Figu re 1.50);
check the circulation in bo th fe et a s described for th igh
fractures;
move th e casualty in a Neil Robe rtson stretcher.
Jaw
Normally, fractures of the low er jaw give little tro uble.
the casual ty sits w i th the teeth clenched , of ten refusing to
speak much on a ccount o f the pa in ;
the spasm of th e jaw mu scles caused by pain keeps the teet h
clenched a nd jaw immobilised;
a ba nda ge, tied a s in Figure 1.51, will support the low er jaw.
A major haza rd arises when bo th sides of t he lower jaw are
f ractured . In th is case , the jaw w ith the tongue a t ta ched on the
inside of i t , can move backwards and may obstruct the a ir
passage.
hoo k a f inger, yours or the casualty’s, over and beh ind the
lower f ront teeth a nd pull the jaw, and w ith it the tong ue,
forwards;
if possible, arrange f or the casualty to sit up w ith his hea d
forwards;
if he cannot sit up, on account o f ot her injuries, place him in
the unconscious position a nd someon e must stay with him,
keeping the jaw pulled fo rwa rd , i f necessary, and wa tching
carefully for any sign of obstructed breath ing.
Figure 1.50
Figure 1.51

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 29/40
Cha pt er 1 FIRSTAID 33
Spine
Alw ays suspect a f racture of th e spine i f a person has fa l len a d ista nce of over tw o met res.
Check careful ly how the injury happened . Ask i f there is pain in the back . Most people w ith
f ractures of t he spine have pa in but a very few DO NOT. I f in doubt , t reat the injury as a
f ractured spine.
A FRACTURED SPINE IS POTENTIALLY A VERY SERIOUS INJURY. IF YOU SUSPECT A
FRACTURED SPINE, TELL THE CASUALTY TO LIE STILL AND DO NOT ALLOW ANYONE TO
MOVE HIM UNTIL FIRST AID TREATMENT HAS BEEN COMPLETED.
Any careless movement of a casualty w i th a f ractured spine could dama ge o r sever the spinal
cord, resulting in perma nent p ara lysis and loss of f eeling in the legs, and d oub le incontinence
for life. He can, how ever, be safely rolled over onto o ne side or the oth er because, if this is don e
very gently a nd caref ully, there is very little movemen t o f the spine.
First, estab lish whet her the spinal cord has been d ama ged . To do this: ask the casualty if he can fe el any ting ling o f the f eet o r legs. Tingling usually means that
there is some pressure on t he spinal cord;
ask him to mo ve his toes. If he is unab le to d o t his, then para lysis is present a nd indicates
severe dama ge t o t he spinal cord ;
run your f ingers light ly over the skin of the lowe r legs and fee t. Absence of sensat ion
indicat es severe dama ge to t he spinal cord.
If any of t hese are found , get RADIO MEDICAL ADVICE.
next , place padding bet ween t he legs;
t ie the feet a nd ankles tog ether with a f igure-of-eight banda ge a nd get the casual ty ly ing
st il l and stra ight . Use gentle tract ion on the hea d and on the feet to stra ighten him out . Do
not bend him. Take you r time;
t ie a narrow fold banda ge a round the casual ty a t the level of h is e lbow s and mid th ighs.
This meth od keeps th e casua lty rigid (Figure 1.53);
place pads to f i l l and support the ho l low s of the spine at the small of the ba ck and a t the
ne ck (Fig ure 1.52);
he can no w lie safely in this position for a s long as is necessary. So do not be in a hurry to
move him;
prepare a st i f f support ing stretcher ready fo r the pat ient . There may be a need to st i f fen
the Neil Robertson stretcher with broom hand les. A canvas stretcher wi l l not d o u nless i t
has st i f f woo den bo ards la id transversely over the canvas to provide a r ig id support for
the b ack . Tw o pa ds must be provided to support and f i ll the hol low s of the spine in the
small of the ba ck and behind th e neck . The ba ck pad should be larger tha n the neck pad
(Figure 1.52);
Figure 1.52

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 30/40
when the stretcher has been prepared
and is alongside the casua lty, the next
job is to lif t him onto t he prepared
stret cher as de scribed in Figure s 1.53 to
1.58;
NOTE: In Figu res 1.54 t o 1.58 t he
encircling b and ag es show n in Figure
1.53 round the t h ighs and at the
elbows have been o mitted for clari ty.
See also Note s at end o f this Section;
to l i f t the casual ty, have at least two
people g rasping ea ch side of the
blanket and one person at the head
and one at t he feet to provide in line
support. Those lif ting t he bla nket
should be spaced so that more lif ting
pow er is avai lab le a t t he body end ,
w hich is heavy compared to t he legs.
A further person is required to push the
prepared stretcher under the casualty
w hen h e is lift ed (Figu re 1.57);
lif t t he casualty very slow ly and
carefully to a height of about hal f a
metre. The heig ht shou ld be just
enoug h to slip the stretcher under the
casualty. Be careful, take time, keep
the casualty straight (Figure 1.58);
slide the stretcher between the legs
of t he person w ho is support ing the
ankles. Then mo ve the stretcher
tow ards the hea d end unti l it is exact ly
undernea th the casua lty. Adjust the
posit ion of the pa ds to f i t exact ly
under the curves in the small of the
back and neck;
lowe r the ca sualty very, very slow ly on
to t he stretcher. Mainta in suppo rt
until he is resting firmly on the
stret cher (Figu re 1.58);
the casual ty is now ready for removal .
34 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.56 Prepare the b lanket for l i ft ing
the casualty – roll the ed ges t ightly.
Figure 1.55 Roll the casualty g ently over
Figure 1.53 Place a half rolled blanket
alongside the casualty.
Figure 1.54 Roll the casualty gently ont o
his side – the att endant closest to his
head , or a third at t endant , must support
the casualty’s head.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 31/40
Cha pt er 1 FIRSTAID 35
When the casualty has been very carefully transported to a
matt ress on the d eck, or other very f irm bed, w here he may
remain undisturbed flat on his back, the most
important single po int is to keep him a s still as
possible. He must continue to be
supported with pillows, etc., as described
later in the text. Every care and a ttent ion,
and encouragement must be given to help
him to rema in still, w hether or no t a ny para lysis is
present. Bags f illed with sand should be placed as
necessary to prevent the body or limbs rolling. A urine
bott le should be constant ly available, and a cat heter should
be used to relieve him if necessary. He should pa ss any fae ces
on to cot t on w ool or other materia l : he must not b e l if ted onto a bed pa n. His back should be t reat ed, so far a s possible, to
prevent sores. He must be put ashore at the very earliest
possible moment . Get RADIO MEDICAL ADVICE.
NOTES:
(1) As there are a number of people
helping a nd since i t is important to t ake
great care in handling the casualty, i t
may be helpful to have a person read
out the particular instruction before
each opera tion is carried out.
(2) At lea st seven peo ple are req uired to
carry out t his ma noe uvre. In ships w ith
small crew s, there ma y be insufficient
numbers of men available. In this case,
do not a t tempt t o move the casualty but
carry out the instructions given abo ve on
immobil ising him and padding the na turalcurves of the spine. The casua lty should
then be kept w arm, his pain should be treated
(see section on a na lgesics and, if he is on the d eck, he should b e
protected from the elements with suita ble wa terproof coverings.
Neck
Injuries to the neck are often compression fractures of the
vertebrae due, for example, to a person standing up
suddenly and bumping his head violently, or by something
falling on his head. Falls from a height can a lso prod uce neck
injuries. Treat ment is similar t o t hat described ab ove fo r
fractures of t he spine, because the neck is the upper pa rt of
the spine.
the casual ty should be la id f la t , i f not a lready in th is
position, and should be kept still and stra ight;
a semi-rigid neck collar should then be a pplied gent ly to
stop movement o f the neck while an assistant stead ies
the hea d. An improvised neck collar can be mad e quite
easi ly f rom a newspaper. Fold the new spaper so t hat the
wid th is about 10 cm at t he f ront . Fold the bott om edg e
over to p roduce a slightly narrow er back. Then fo ld this
around the neck with the t op edge under the chin and
the bott om edge o ver the top o f the col lar bones;
t ie a ba ndag e, scarf or a necktie over the newspaper to
ho ld it in place. This w ill keep th e ne ck still (Figu re 1.59).
Figure 1.58
Figure 1.59
Figure 1.57

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 32/40
36 THE SHIP CAPTAIN’S MED ICAL GUID E
Chest
See Fract ured ribs.
Pelvis
A fracture of t he pelvis w ill result from d irect violence in the pelvic area o r from a fall from a
height w hen the casualty has landed o n bot h feet wi th t he legs held st i f f ly. The main da nger of
this injury is of da mag e to t he pelvic orga ns, especially the blad der and the uret hra (the pipe
which leads f rom the b ladder t o t he t ip of the penis).
the casualty w ill complain of pa in in the
hip, groin and pelvic area s and,
perhaps, a lso o f pa in in the lower ba ck
and butt ock areas, made wo rse bymoving o r coughing;
he w ill be unable to stand , despite
there being n o injury to the leg s;
he may wa nt to pa ss urine a l though he
may be unable to do so. I f urine is
passed, it may be blood -stained.
there ma y be signs of interna l bleeding ;
the compression test is useful. Press
gently on the f ront o f both h ip bones in
a do wnw ard and inward d irect ion so as
to comp ress the p elvis. This will give rise
to sha rp pain if it is broken. Some
movement of t he pelvic bones may also
be fe lt if the re is a f ractu re (Figure 1.60),
but do not continue pressing in a n
at tempt to elicit this sign, as furtherdama ge may be caused .
If you th ink tha t the pe lvis may be fractured , tell the casualty:
n ot to m ove ;
not t o pa ss any urine if he can a void it. If urine is passed, look for staining w ith blood .
Remember that :
if the bladd er or urethra is dama ged , urine can leak into the t issues;
bleeding into t he surrounding tissues and into t he pelvic and low er abd ominal cavities may
be severe. A pulse chart must be sta rted immediat ely to check for interna l haemorrha ge.
lay the p at ient in his most comforta ble position. This will usually be on his back. If he w ant s
to bend the knees, support them with pi l low s. Place padding betw een the legs;
apply a broad fold banda ge round bot h knees and a f igure-of-eight ba ndag e around the
ankles;
move the casual ty wi th great care . Use the same t echnique a s for f racture of the spine. keep checking for interna l bleeding.
when moved to a cab in or to the ship’s hospi ta l , a l low the casual ty to l ie in w hatever
position he finds most comfo rtab le;
morphine may be required to control the pain ;
RADIO MEDICAL ADVICEshould be o bta ined .
Figure 1.60

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 33/40
Dislocations
A dislocat ion is present w hen a b one ha s been displaced fro m
its normal p osition a t a joint (Figure 1.61).
It ma y be d iagno sed :
when an injury occurs a t or nea r a join t and the join t
cannot b e used normally;
movemen t is limited or impossible;
there is pain, ofte n qu ite severe. The pa in is mad e w orse
by at t empts to move the join t ;
the a rea is misshapen bo th by t he d islocat ion a nd by
swelling (bleeding) w hich occurs around the d islocation;
with the exception of no gra t ing of bo ne ends, the
evidence for a d islocation is very similar to tha t of a
f racture ;
alwa ys remember that f ractures and d islocat ions can
occur together.
Treatment
dislocat ions can b e closed or o pen. If a w ound is present,
a t or near the d islocat ion , the w ound should be covered ,
both t o stop b leeding and to help to prevent in fect ion ;
give antib iot ic treatment ;
do not a t t empt to reduce a d islocat ion . A f racture may
also be present and at t empted manipulat ion to reduce
the dislocation in these circumsta nces can make ma tte rs
worse;
prevent movem ent in the a ffected a rea by suitable immobilisat ion. The techniqu es for
immobilisat ion are exactly the same a s for fractures of the same a rea(s).
look out fo r impaired circulation a nd loss of fee ling. If these are present, and if you cann ot
feel a pulse a t the w rist or ankle , try to move t he l imb g ently in to a posit ion in which
circulation can return a nd keep the limb in this position. Loo k then for a chan ge o f the
fingers or toes, from w hite or blue to pink;
tra nsport the ca sualty in the most comfo rtab le position. This is usually sitting up f or upper
limb injuries and lying dow n fo r low er limb injuries;
for further treat ment o f d islocat ions of the shoulder and of t he f ingers, see Chapter 4 .
Head injuriesHead injuries commonly resul t f rom blow s to the head and f rom fa l ls , of ten f rom a height .
Most preventable serious head injury deaths result from obstructed breathing and from
breathing d i f f icult ies, not f rom brain d ama ge. Apart f rom covering serious head wo unds, your
at t ention should be concentrated on the l i fe-saving measures which support no rmal breath ing
and w hich prevent ob structed brea thing. This w ill ensure tha t the b rain get s sufficient o xygen
easily. In this way you have a good chance of keeping the casualty alive in order to get him
skilled medical aid in a hospital; ge t RADIO MEDICAL ADVICE.
NOTE: in the case of some hea d injuries or w here a foreign bod y or a fracture is directly below
an o pen w ound, you should NOTcontrol b leeding by d irect pressure on top of t he w ound. In
these circumstances a sterile gauze dressing is applied o ver the w ound a nd a banda ge is padded
around the w ound a nd over the edge o f the dressing, held f i rmly in place by a banda ge.
See Chapter 4 for further in formation .
Cha pt er 1 FIRSTAID 37
Figure 1.61
(b) Dislocated
(a) Normal

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 34/40
Chest injuriesSee also Wound s, Crush woun ds, Sta b w ound s.
Fracture of the ribs
This is a common fracture w hich is usually caused by fa lling a ga inst a ha rd surface or by
a crushing injury. Signs a nd sympto ms are:
sharp, continuous pain w hich is increased w hen brea thing in or by coughing ;
shallow breath ing t o prevent chest movements;
marked localised te nderness when t he injured a rea is felt gent ly.
Uncomplicated rib fracture:
make the casualty sit dow n in the norma l sitting po sition bu t, if pain is severe, place
him in the half-sitting-up position, leaning over to w ards the injured side;
tran sport him in this position t o t he ship’s hospital or his cab in;
t reat pain ;
do no t put strapping around his chest ;
keep him at rest in the po sition he f inds most comforta ble, either in bed or sitting in
a cha ir or o n t he f loor (Figure s 1.62, 1.63, 1.64).
Severe chest injur ies
The ribs form a rigid cag e w hich prote cts the heart a nd lungs.
Severe force may cause any one or a combinat ion of the
follow ing injuries:
a superficial wou nd a nd/or bruising of t he chest
a penet rat ing (sucking) wound o f the chest w al l
multiple rib fractu res on one o r both sides of the chest,
tog ether with in jury to t he underlying lung and i ts
covering (the pleura ); a ‘stove-in’ segment o f the chest w all.
The frag ments of a f ractured rib are u sually held in place by
the muscles betw een t he ribs. After severe injury, a rib
f ragment may be driven inwards, causing a tear in the
covering of t he lung w ith consequent leaking of b lood or a ir
into t he chest cavity. The lung on t hat side w ill then collapse
and /or b e comp ressed, resulting in diff iculty in b reath ing.
There may b e a blue/grey ting e to the skin of the f ace a nd lips,
and th e casualty may coug h up frothy blood-sta ined sputum.
Treatment
G et RADIO MEDICAL ADVICE and g et the casual ty to expert
treatment , or expert treatment to the casual ty , as soon as
possible.
place in the half-sitt ing-up position leaning to w ards the
injured side (Figure 1.62). If bo th sides a re injured, kee p
in the upright half-sitting up position (Figure 1.63); keep the air passage clear. Remove den tures, if w orn, and
encourage h im to spit o ut a ny b lood , vomit or secret ions;
deal w i th any sucking w ound.
tran sport to ship’s hospital, or cabin, as soon a s possible,
but keeping him in the sitting p osition advised abo ve;
w hen in bed, in the correct position, relieve pain but DO
NOTGIVE MO RPHINE;
wa tch for signs of in ternal b leeding and obstructed
breath ing.
38 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.64
Figure 1.63
Figure 1.62

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 35/40
Cha pt er 1 FIRSTAID 39
Unconscious casualt y
Transport and later nu rse in bed in the un conscious position, lying on t he injured side (not the
uninjured side) and w ith a head -dow n tilt.
Stov e-in chest in jury
In a very severe injury, multiple fractures of the ribs may lead to a portion o f the chest w all
being ‘stove-in’. That portion cont ains adjacent ribs which have been fra ctured at bot h ends,
thus a l low ing the port ion to ha ve f ree movement independent f rom a nd in the opposite
direction to the mo vement of t he rest of the rib cage . This is called parad oxical movemen t and
it is an impo rtan t sign in diagno sis.
Treatment
give treat ment a s for multiple fractures of ribs;
using t he f la t hand , e i ther the casualty or t he a t tenda nt should maintain f i rm pressure over
the stove-in portion o f the chest w all;
a pa d of fo lded cloth should be placed over the dama ged a rea and banda ged f irmly in
place, using w ide crepe ba nda ges to encircle the chest. If brea thing mo vements are
hindered by the chest banda ge, strips of elastic adhesive ban da ge, w hich do not encircle
the chest , may be used .
NOTE: Infections of t he lung may a ppea r as a serious complication o f a ny severe chest injury.
Whenever a casualty has to be kept on bo ard , a lwa ys start a course of ant ib iot ic treatment .
Blast injuries
Explosions cause a sudde n and violent disturba nce of the a ir; f ires can be sta rted a nd to xic ga ses
produced .
men may be throw n dow n and so injured . Further in jury may occur f rom fa l ling w reckage;
the bla st of air itself may strike the bo dy with such violence as to cause severe or fata linternal injuries;
cases of bu rns or asphyxia ma y occur.
Apart from fractures, wo unds, severe bleeding, burns and a sphyxia, any combinat ion of the
follow ing injuries may be fo und.
Head
The effe ct of blast injury to the hea d is rather like concussion. In some ca ses there may b e
para lysis due t o spinal cord dama ge. The pa tient ma y be unconscious or he ma y be extremely
dazed . Dazed casualt ies can be found si t t ing about , incapable of moving and no t caring wha t
is going on . Althoug h appa rently to o utw ard appea rances uninjured , they do not ha ve the
energy, or indeed the w ill, to mo ve. They w ill appea r confused and disorienta ted.
if unconscious, put in th e unconscious position immedia tely. Check for breat hing, hea rt
stopped and b leeding;
i f dazed , ta ke them by the ha nd and lead them t o safety . Tell them f irmly wha t they must
do. Detai l someone to look af ter them.
Lungs
The blast of air may da mag e the a ir sacs and t he small blood vessels of t he lungs.
bleeding ma y take place inside the lungs;
the pa t ient may be shocked ;
he may ha ve diff iculty in breathing. There may be a feeling of t ightne ss in the chest and
there may be pa in ;

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 36/40
lips, ears and the skin of the f ace ma y be blue;
he may cough up a b lood-sta ined f roth ;
ta ke the pat ient into the f resh air if possible;
support him in t he ha lf-sitting -up po sition
loosen t ight cloth ing t o a l low him to brea the more ea sily;
keep him w arm and treat f or shock ;
encourage h im to cough and spi t out a ny secret ions
produced ;
artif icial respiration o r assisted respiration ma y be
required if brea thing f ails or becomes diff icult.
PATIENTS WITH CHEST INJURIES MUSTNEVERBE GIVENMORPHINE
Abdomen
Abdominal injury to casualties in the sea can happen as a
result o f unde rwa ter explosions but similar injury can be d ue
to explosions on b oa rd ship. The fo rce of th e explosion
dama ges the in ternal orga ns and causes in ternal b leeding.
The ma in feat ures of this type o f injury are:
shock;
abdo minal pain ;
both of which may become evident some t ime af ter the
explosion. If these conditions are fo und, start a pulse chart .
Treat ment is that f or shock and for interna l bleeding .
Transportation
Unless there is danger from fire, explosion or toxic
substances, do not mo ve a casualty until suspected fractures
have been immobil ised and b ad b leeding ha s been stopped .
Then check out t he best rout e for tra nsport an d lif t th e
casualty gently and carry him smoothly. Every jolt means
unnecessary pain.
The method of t ransport wi l l depend on the situat ion of
the casual ty and the na ture of the injury. Whatever metho d
is used , try to gain the conf idence of the person you are
carrying by explain ing w hat you a re about t o do a nd then
carrying out the ma noeuvre in an ef f icient manner.
Ordinary man-handling ma y be po ssible, in w hich case
two helpers carry a casual ty wi thout forming their hands
into a seat , by ea ch using an a rm to support the casual ty ’s
ba ck and sho ulders and e ach using his spare hand to support
the casua lty under his thighs.
If conscious, the casua lty may help to support himself with
his hands o n th e shoulders of the helpers (Figure 1.65).
The four-handed sea t can be used w hen a hea vy person
has to be carried . The d isadvantag e of th is type of seat is that
the casual ty must be ab le to co-operate a nd to ho ld on with
both arms around the shoulders of the two men carrying
him. It canno t be saf ely used to neg ot iate la dders (Figure 1.65).
The ha nds should b e pla ced a s in Figure 1.66.
One advantage of the three-handed seat (Figure 1.67) is
that one arm and ha nd of a helper is le f t f ree and can be used
40 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.66
Figure 1.65 Position taken upwhen man-handled, or a four-
arm seat is being used; in the
former instance two arms are at
the back of the patient and only
two are under his thighs.
Figure 1.67

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 37/40
either to suppo rt an injured limb or a s a backsupport for th e casualty. According to t he nat ure
of the injury, it is decided w hich of t he t w o he lpers has the f ree a rm (Figures 1.68 and 1.69).
The firema n’s lif t w hich should no t b e used unless the helper is as well built as the casualty isespecial ly useful when you have to move a ma n by yourself a nd need t he use of your r ight hand
for hold ing on to a ladder. Rol l the pat ient so t hat he is ly ing face dow nwa rds, l if t h im up so
tha t, w hen you sto op do w n, you can put your hea d unde r his left arm (Figure 1.70). Then put
your left arm between his legs and grasp his left hand, letting his body fall over your left
shoulde r (Figure 1.71).
Steady yoursel f and t hen stand upright , a t the same t ime shi f t ing h is weight so that he l ies
w ell balanced a cross the b ack of yo ur shoulders (Figure 1.72). Hold the ca sualty’s arm a bove t he
w rist. In this position it is easy to carry the pa tient up a ladder a s one hand is free to gra sp the rail
(Figu re 1.73).
Cha pt er 1 FIRSTAID 41
Figure 1.69
Figure 1.73Figure 1.71 Figure 1.72
Figure 1.70Figure 1.68

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 38/40
As a last resort, the drag-carry method may have to be used in narrow spaces, particularly
where t here is wreckage fol lowing a n explosion a nd w here i t may be po ssib le for o nly one man
to reach a t rapped casual ty and to rescue him. Af ter in i t ia l rescue, tw o men may be ab le toundertake further movement t hrough a narrow space. The metho d is demonstrated in Figures
1.74 and 1.75. Ensure that the casua lty’s w rists, which are tied t og ether, do not interfere w ith
any breath ing a pparatus the rescuer may be wea ring, and safeg uard the casual ty ’s head with a
bump ha t if possible.
Neil Robertson stretcher
This particula r type o f stret cher is show n in Figure 1.76. It is a simple de vice for moving a
casualty safely from a diff icult place where the ordinary stretcher with stif f poles would be
useless. Other pa tte rns of rescue stretcher are a vailable but a ll aim to a chieve the same purpo se.
The casualty is enveloped in a prot ecting but somew hat f lexible case, so th at he ta kes up as little
room a s possible. The stretcher can b e bent slightly in turning sharp corne rs in na rrow passag es,
as when b eing hoisted up t he ladder wa ys f rom eng ine-rooms, or through the ha tches of cargo
tanks.
The stretcher is made of stout canvas, stif fened by w ood en slats (Figure 1.76). The p ortion ‘A’
ta kes the hea d and n eck, w hich are stea died by a canva s stra p passing o ver the forehea d. Thus,
the hea d of an unconscious pat ient can be stead ied .
42 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.76
Figure 1.74 Figure 1.75
A
B
C
D

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 39/40
Cha pt er 1 FIRSTAID 43
The po rtion ‘B’ is w rappe d round the chest, not ches being cut on w hich the armpits rest. This
part ha s three canva s strap s w hich are used for fa stening the stretcher round t he chest. The
portion ‘D’ folds round the hips and legs dow n to t he ankles. It is secured by tw o canva s strap s.
A central ba ckbone of stou t rope pa sses along t he under surface. This has tw o beckets
passing out f rom i t on ei ther side which can be used as handles, for carrying t he pat ient or for
securing t ackles w hen he is slung ho rizonta lly.
At the head end , the rope ends in a g rommet w hich takes extra purchase f rom tw o brass
eyelets let into the ca nvas. At th e foo t end o f the ro pe is a ga lvanised iron ring w hich is secured
to the stretcher by a span going to brass eyelets in the canvas. When more rigidity in the
stretcher is required, a s in moving th ose w ith injuries to t he ba ck, a couple of b room ha ndles,
slipped thro ugh t he ropes undernea th, w ill fulf il this purpose ad mirably.
Some stretchers have a rope ab out 9 f t long f ixed to t he ga lvanised ring a t the fo ot end . This
is a stead ying rope for use in craf t below, o r on q uay, when the pat ient is low ered over the side
of th e ship. When the pa tient is carried abo ut the ship, this rope can be pa ssed unde r the variousstraps to keep i t f rom tra i l ing o n the deck or otherw ise get t ing in the w ay.
The pa tient should b e lif ted o n to and secured in the stretcher as shown in Figures 1.77 to 1.80.
Cases of fracture of t he spine or other ba ck and pelvic injuries should be t ransferred to the
stretcher as d irected under spinal injury.
Figure 1.77 Getting ready to lift
the casualty sufficiently for the
Neil Robertson stretcher to be
slid under him. With only three
attendants, the wrists of an
unconscious patient have to be
tied together – but not tightly.
Figure 1.80 Strapped up – the arms can be strapped inside or outside the chest section
of the stretcher, depending upon the injuries.
Figure 1.78 Lower the patient slowly –
if he is unconscious, support his head.
Figure 1.79 Ensure patient’s armpits are in the
correct place before you finish lowering him.

8/20/2019 Mcga-shs Capt Guide Chap1
http://slidepdf.com/reader/full/mcga-shs-capt-guide-chap1 40/40
44 THE SHIP CAPTAIN’S MED ICAL GUID E
Figure 1.82
Hoisting a
casualty through
a hatch (see also
Figure 1.83).
Figure 1.81 Carrying the
patient – but keep the head
section level with the chest
section if the neck may be
hurt.
The pa tient shou ld be carried by f our men , if possible
(Figure 1.81). At difficult corners, the stretcher should be
lowered at t he foot end , and the casual ty passed by tw o of
the men t o the o thers. The carry can t hen be resumed by the
four b earers.
When passing the casual ty through a narrow hatch , or
lif ting him up over a height, or lowering him to a boat
alongside, put the lif ting hook or a rope through thegrommet a t the head end and a further steadying rope
throug h the g alvanised ring at the fo ot end (Figures 1.82 and
1.83).
Moving an unconscious casualty
If possible, carry an unconscious casualty in the unconscious
position and a lwa ys with a he ad -dow n tilt. The tilt is also
necessary w hen carrying a ca sualty suffering from shock or
loss of bloo d.
Figure 1.83 Moving a
casualty vertically. Note: to
steady the stretcher, a ropegoes from the foot of the
stretcher to a seafarer
below.