Embed Size (px)
Citation preview

28 PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 PHILIPPINE ACADEMY OF OPHTHALMOLOGY
Correspondence to
Patricia Q. Grulla, MD
Department of Ophthalmology and Visual Sciences
University of the Philippines–Philippine General Hospital
Taft Avenue, Ermita
1000 Manila, Philippines
Telefax : +63-2-3022491
E-mail : [email protected]
The authors have no proprietary or financial interest in
any product used or cited in this study.
Presented at the annual meeting of the Philippine
Academy of Ophthalmology, November 2007, and the
World Ophthalmology Congress in Hong Kong, June
2008.
CASE REPORT
PHILIPPINE JOURNAL OF
Ophthalmology JANUARY – JUNE 2009VOL. 34 • NO. 1
ABSTRACTObjective
To present 3 cases of Möbius sequence exposed in utero to misoprostol anddiscuss their clinical presentations, etiopathogenesis, and management.
MethodsMedical records of 3 patients with Möbius sequence and prenatal exposure
to misoprostol were reviewed. Clinical findings were compared with thosereported in the literature.
ResultsLack of facial-muscle movement, lagophthalmos with secondary exposure
keratitis, decreased ability to crease forehead, and shallow nasolabial fold implyfacial-nerve dysfunction. Small- and large-angle esotropia and apparentorthotropia with abduction limitation showed varying degrees of abducensnerve involvement. Two patients had early prenatal exposure to misoprostolduring the first 3 months of gestation.
ConclusionA history of misoprostol exposure should be routinely elicited from parents
of children with Möbius sequence. Associated deficiencies in Möbius sequenceand its variants require a multidisciplinary approach.
Keywords: Cranial-nerve-VI and -VII palsy, Möbius sequence, Möbius syndrome,Misoprostol, Abortion
PHILIPP J OPHTHALMOL 2009; 34(1): 28-33 © PHILIPPINE ACADEMY OF OPHTHALMOLOGY
Patricia Q. Grulla, MD1
Alvina Pauline D. Santiago, MD1
Marissa N. Valbuena MD, MHPed1,2
1Department of Ophthalmology and VisualSciencesUniversity of the Philippines–PhilippineGeneral HospitalManila, Philippines
2College of MedicineUniversity of the Philippines Manila
Möbius sequence with prenatalexposure to misoprostol

PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 29PHILIPPINE ACADEMY OF OPHTHALMOLOGY
WITH steadily increasing rates ofunwanted pregnancies, many unpre-pared mothers attempt abortion.Misoprostol (Cytotec), a prostaglandinanalog used to treat gastric ulcers, iscommonly exploited for its abortifa-cient properties. Recent studies havedescribed Möbius sequence, acongenital nonprogressive sixth- andseventh-cranial-nerve palsy, amonginfants exposed in utero to the drugduring unsuccessful abortion.1-3
CASE REPORTSIn this study, we present 3 such
cases of Möbius sequence followingprenatal exposure to misoprostol.
Case 1A two-year-old girl was referred to
the ophthalmology department of theUniversity of the Philippines–Philippine General Hospital (UP-PGH) for evaluation for Möbiussequence. She was born full term toa 20-year-old primigravid. She wassmall for gestational age, weighing2,050 grams. Apgar score was 9. At 1month age of gestation(AOG), themother attempted abortion withmisoprostol 200 mg/tab, taking 1tablet orally and inserting 1 tabletintravaginally. At birth, inversion ofboth feet, small head circumference,and mild dilatation of lateral ventri-cles with absent corpus callosum oncranial computed tomography werenoted. Developmental milestoneswere markedly delayed. Intermittentesotropia (ET) was observed at 1month of age.
On ophthalmologic examination,dazzle testing for both eyes was unre-liable due to weak and inconsistentlid closure to bright halogen light.There was central steady fixation onvertical gaze with slight left-eye prefer-ence. Horizontal gaze could not beassessed. Full cycloplegic refraction(FCR) with atropine was +1.00 dioptersphere for both eyes. Epican-thal foldsand lagophthalmos were observed.The patient had 10- to15-degree ET
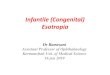
Figure 1. Two-year-old girl with misoprostol exposure
at 1 month AOG. She has 10-15o ET, epicanthal folds,
and lagophthalmos (A). There is minimal eye movement
on up- and downgaze, not apparent on lateral gaze (B)
A
B
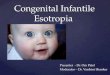
Figure 2. An eight-year-old boy whose mother allegedly
attempted abortion with intake of misoprostol at 5 months
AOG. There is a 55 PD ET by Krimsky testing (A), and
limited abduction on duction and version in both eyes (B).
A
B
A B
Figure 3. An 18-month-old boy whose mother attempted abortion with intake of 2 tablets of misoprostol for 3 consecutive
days. He is orthotropic on primary gaze with no lateral eye movements in both eyes (A), and has talipes equinovarus of
the right lower extremity (B).
by Krimsky with slight left-eyepreference (Figure 1A). Minimal eyemovement on up- and downgaze wasnoted (Figure 1B). This was confirmedby the presence of doll’s eye reflex forvertical gaze which was not apparenton lateral gaze. On biomicroscopy,there was punctate dye uptake in thecentral inferior 1/3 of the cornea.The rest of the eye examination wasunremarkable.
Patient was started on eye lubri-cants 2 times/day. The preferred eyewas patched. After evaluation by theother subspecialty clinics, follow-upwas advised.
Case 2The patient was an eight-year-old
boy whose mother allegedlyattempted abortion with intake ofmisoprostol (dose and route unre-called) at 5 months AOG. Otherabortifacients were also taken. Shehad a difficult pregnancy and diedfrom childbirth complications.
He was born full term via sponta-neous vaginal delivery to a 35-year-oldG5P4 (4-0-0-4) mother at a localhospital with a birth weight of 1,540grams. At birth, he had poor cry andfair activity, with minimal movementof extremities. He was diagnosed with

30 PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 PHILIPPINE ACADEMY OF OPHTHALMOLOGY
autism and global developmentaldelay. At 5 months of age, there wasalternating intermittent ET, whichbecame permanent at around 5 yearsof age. Systemic evaluation showedmultiple congenital anomalies(esotropia, micrognathia, epicanthalfold, microcephaly, undescendedtestes).
On initial ophthalmologic consult-ation, visual acuity (by LEA chart) wasat least 20/80 in each eye. Fullcycloplegic refraction was +1.00diopter sphere in the right eye and–1.00 diopter sphere in the left. Hehad prominent epicanthal folds. Nolagophthalmos was observed. Therewas alternating esotropia, with 55prism diopter by Krimsky testing(Figure 2) and left-eye preference.Limited abduction was observed inboth eyes on duction and version.Anterior-segment and fundus exami-nations were normal. Shallow naso-labial folds were present with limitedability to raise the forehead.
A medial rectus recession in botheyes was recommended. Patching ofthe left eye 4 hours a day was advised.Remeasurement of the deviationprior to the contemplated musclesurgery was also recommended.
Case 3The patient was an 18-month-old
boy referred for visual prognosti-cation. The patient was born full termvia spontaneous vaginal delivery to a35-year-old G4P3 (3-0-0-3) motherwho took 2 tablets of misoprostol (200mg/tab) orally per day for 3 conse-cutive days 1 month into the preg-nancy. Minimal vaginal bleeding wasnoted but pregnancy continued andprogressed to term. At birth, rightclub foot was observed (Figure3B).Consultation at UP-PGH showedtalipes equinovarus, shallow leftnasolabial fold, left-lid lag, mask-likefacies, and limited extraocular move-ments. Möbius sequence was consi-dered. He was referred to pediatrics,orthopedics, neurology, ENT, and
ophthalmology for further evalua-tion. He underwent serial casting andpercutaneous tenotomy of the rightfoot at 3 months of age.
On ocular examination, dazzlereflex could not be clearly elicited.There appeared to be good centralfixation in both eyes. Horizontal eyemovements could not be assessed dueto lack of lateral gaze. Although thepatient seemed to have right-eyepreference, this was not consistentand reliable. Red-orange reflex wassymmetrical on Bruckner’s test witha short acting cycloplegic refractionof –2.50 diopter sph –1.00 diopter cylx 180 and –2.50 sph. The eyes wereorthotropic on primary gaze. Therewas mild limitation on abduction with
a 10 prism diopter esotropia byKrimsky and exotropia on downgaze.Anterior- and posterior-segmentexaminations were unremarkable. Nosurgical intervention was considered.Spectacle correction and monitoringfor amblyopia were recommended.
Patient also had recurrent bouts ofpneumonia and died of respiratoryfailure at age 2 years and 2 months.
DISCUSSIONIn the clinical setting, the constel-
lation of findings of large-angleesotropia with various gaze palsies,associated with mask-like facies,incomplete eyelid closure, prominentupper lip, inability to close the mouth,drooling, poor suck, and speech
Table 1. Salient features of 3 cases of Möbius sequence.
Case 1
2/F
1 month AOG
1 tablet oral
1 tablet intravaginal
(-)
CSM,1 left eye
preference?
+1.00 D sph both eyes
10-15 PD ET
Absent
Intact
OU
OU
Epicanthus,
lagophthalmos
Normal
Bilateral, complete
Normal BAER2
Intact gag reflex
No tongue deviation
Yes
Normal
Clinodactyly, 5th digit,
both hands; club feet
Case 2
8/M
5 months AOG (?)
unknown
Alcohol, cigarette
smoke, illicit drugs
20/80 OU (LEA
chart), left eye
preference
+1.00 D OD
–1.00 D OS
55 PD ET
Partial
Intact
OU
None
Epicanthus
Normal
Bilateral, incomplete
(upper > lower)
Intact gross hearing
Intact gag reflex
No tongue deviation
Yes
Hypoplastic left nipple
Normal
Case 3
2/M
1 month AOG
2 tablets oral for 3
days
(-)
CSM1 no obvious
preference
–2.50 D x –1.00 D x
180 OD, –2.50 D OS
10 PD ET
Partial
Intact
OU
None
None
Normal
Bilateral, incomplete
(+) hearing loss
Intact gag reflex
No tongue deviation
Developmentally at
risk
Normal
Club feet
Features
Age (years)/sex
Misoprostol exposure
Timing
Dosage and route
Exposure to other agents
during pregnancy
Best-corrected visual acuity
Cycloplegic refraction
Strabismus deviation in
primary gaze
Lateral gaze
Vertical gaze
Abduction limitation
Adduction limitation
Eyelids
Fundus
CN-VII palsy
CN-VIII palsy
CN IX, X
CN XII
Mental retardation
Chest findings
Extremities
1Central, steady, maintained2Brainstem-auditory-evoked response

PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 31PHILIPPINE ACADEMY OF OPHTHALMOLOGY
impairment raises a high index ofsuspicion for Möbius sequence, adisorder primarily involving the facialand abducens motor nerves.
Ocular conditions that may presentwith large-angle esotropia with limi-ted lateral rectus function includecongenital sixth-cranial-nerve palsy,congenital infantile esotropia, andDuane syndrome. These conditions,however, do not have signs andsymptoms characteristic of facial-nerve involvement as seen in Möbiussequence.
Möbius sequence is a rare disorder,occurring in 1 of every 50,000 livebirths with no sex predilection.3 VonGraefe initially described a patientwith congenital facial diplegia in 1880but Paul Julius Möbius, a Germanneurologist, reviewed more cases andreported an association with conge-nital, nonprogressive bilateral facialand abducens nerve palsy along withother systemic abnormalities.2 Severaldiagnostic criteria since then havebeen proposed. The latest was byVerzijl4 who suggested facial palsy withimpairment of ocular abduction asthe primary criterion for Möbiussyndrome. The distribution of thefacial-nerve dysfunction with moresevere involvement of the upper facialmuscles and a relative sparing of thelower facial muscles, plus the inabilityto abduct the eye beyond the midline(usually bilateral and complete), arehighly characteristic of the syndrome.Features commonly associated withMöbius syndrome, but are notessential for diagnosis, are listed inTable 2. Frequently mentioned in theliterature was Möbius-Polandsyndrome or Hanhart syndrome,which is descriptive of patients withdysfunction of cranial nerves VI andVII associated with extensive limbanomalies (in contrast to Möbiussyndrome which consists primarily ofcranial-nerve deficits).5 The thirdpatient showed traits of this syndromevariant, being diagnosed with talipesequinovarus at birth and subse-
Table 4. Ocular features of Möbius sequence in different studies.
Feature
Esotropia
Abduction limitation
Adduction limitation
Exotropia
Orthotropia
Facial Diplegia
Lagophthalmos
Epicanthus
Visual impairment
Others
Misoprostol exposure
Cronemberger
et al 20011
(n=16)
75%
93.8%
65.6%
6.3%
68%
75%
Compound
hyperopic
astigmatism 55%
V pattern 50%
18.8%
Stromland
et al 20022
(n=25)
100%
100%
Mostly bilateral
+/- head turn
16%
Moderate
Myopia/
Hyperopia
Abnormal
tearing 50%
None
Verzijl
et al 20034
(n=37)
65%
95%
13.5%
Bilateral 92%
Unilateral 8%
Complete 34%
Incomplete 62%
Conjugated horizontal
gaze palsy 48%
Duane’s syndrome
34%
CFEOM1 8%
None
Santiago and
Uy 20046
(n=7)
85.7%
100%
42.8%
14.2%
14.2%
100% Bilateral
complete
71.4%
100%
DVD2,
cocontraction,
ptosis, lid fissure
narrowing 14.2%
None
Table 2. Commonly associated systemic features of Möbius sequence.3
1. Other cranial nerve involvement (CN II, V, IX, X, XI, XII; relative sparing of the accessory nerve)
2. Orofacial malformations (small palpebral fissure, epicanthal fold, ocular hypertelorism, bifid uvula,
cleft palate, micrognathia, microstomia, external ear deformity with occasional hearing loss,
airway problems with aspiration)
3. Limb malformations (clubfoot, agenesis or rudimentary fingers or toes, mostly syndactyly or
brachydactyly)
4. Musculoskeletal system defects (scoliosis, pectoral hypoplasia [Poland-Moebius syndrome], or
other chest wall deformity)
Table 3. Ocular features of Möbius sequence.5
Sixth-cranial-nerve palsy with decreased abduction ability
Small palpebral fissure
Epicanthal folds
Hypertelorism
Esotropia [E+] up to 100 prism diopters (PD)
Lagophthalmia with or without associated exposure keratitis
Situs inversus of retinal vessels and tortuous retinal vasculature
Mild to moderate refractive errors
Entropion
Ptosis
Anomalous head posture
Head tilt if vertical strabismus is present
Amblyopia and decreased binocular vision
Third- and fourth-cranial-nerve palsies
Generally preserved vertical eye movements and convergence
Normal pupillary function, occasionally poorly reactive and miotic
1Congenital fibrosis of the extraocular muscles2Dissociated vertical deviation

32 PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 PHILIPPINE ACADEMY OF OPHTHALMOLOGY
quently undergoing corrective orthopedic surgery.Involvement of the other cranial nerves led to
significant speech and feeding problems. Bulbar weakness,especially cranial nerves IX and X, may cause dysphagia.The hypoglossal nerve was the third most commonlyaffected, often leading to tongue atrophy with inability toprotrude the tongue beyond the lips.
Associated neuropsychiatric disorders included autismand mental retardation, seen in 24.7 to 28.5%2 and 10 to75%3 of patients, respectively.
Ocular features associated with Möbius sequence havebeen studied extensively (Table 3), with few cases involvedin most series (Table 4).
Common ocular findings included esotropia andabduction limitation, characteristics essential to theinclusion criteria in most studies. These were usuallyobserved within the first 6 months of life, and inapproximately 50% of cases, abducens-nerve palsy was theonly ocular palsy. A face turn was sometimes present onprimary gaze and attempted lateral gaze.2 Large-angleesotropias have been reported, some measuring up to 100prism diopters. Vertical and convergence ability wereusually intact. When the third or fourth cranial nerveswere involved, incomplete or complete ophthalmoplegiawas sometimes present.5 Exotropia and orthotropia havebeen seen in a minority of patients. In this study, 2 patientshad esotropia while the other was orthotropic on primarygaze. All presented with abduction limitation; 1 patientalso had adduction limitation and the third had exotropiaon downgaze only.
Seventh-cranial-nerve palsy usually causes facialweakness. This may manifest soon after birth as difficultyin sucking, drooling, and incomplete closure of the eyelidsduring sleep. Sometimes, facial paralysis may not benoticed until a few weeks or months later when the infant’sinability to smile or lack of facial movement with cryingarouses the parents’ concern. Inability to close the mouthwith prominence of the upper lip, lack of tissue saggingand wrinkling cause the distinctive “mask-like” facies.7
Verzijl and colleagues4 observed that 62% of patients hadincomplete unilateral facial-nerve palsy, primarily affectingthe upper face with relative sparing of the lower-facial-nerve muscles. In contrast, Santiago and Uy6 reported thatall their patients had bilateral complete facial diplegia.Associated lagophthalmos, postulated to be from aberrantinnervation of the orbicularis oculi muscle in 68 to 71.4%of patients, have been observed in 2 studies. Althoughexposure keratitis was commonly seen with lagoph-thalmos, this was not reported in any of the 4 case seriesprobably due to bilateral Bell’s phenomenon.1 Epicanthuswas also a common finding. Various refractive errors werepresent and in the Cronemberger study, there was apositive correlation between reduced visual acuity and
mental retardation.1 In this study, only 1 patient presentedwith complete facial diplegia and lagophthalmos. Two ofthe 3 patients had epicanthus. Cycloplegic refraction wasacceptable for age.
A history of prenatal misoprostol exposure in Möbiussequence has been reported in 18.8% of patients.1 Otherstudies reported various adverse antenatal events. In thisseries, all 3 patients had prenatal exposure to misoprostol.Since June 2005, 14 cases of Möbius syndrome have beenseen at the UP–PGH pediatric ophthalmology clinic, 5(35.7%) of whom had a history of prenatal exposure tothe drug.
The etiopathogenesis of Möbius sequence is stillunclear. Studies have proposed genetic and ischemiccauses, teratogens being implicated in both.2 The termMöbius syndrome has been replaced with Möbius“sequence” to represent a pattern of multiple anomaliesderived from a single structural defect or mechanicalfactor, usually due to multiple etiologies. This is in contrastto “syndrome,” which implies a single cause.
Genetic research has localized point mutations forMöbius sequence which affect cranial-nerve-nuclei deve-lopment and axonal transport.8-9 Verjizl proposed lower-brainstem maldevelopment to explain facial andabducens-nerve palsy, as well as motor-function deficitsseen in many patients with Möbius sequence confirmedby imaging and EMG studies.4 The ischemic theorysupposes an ischemic event in the lower brainstem causingdisruption of its blood supply during the early embryonicperiod.10 Studies have implied in utero exposure to variousteratogens, including misoprostol, in Möbius sequencepresumably caused by constriction of uterine vessels.
Misoprostol is a prostaglandin E1 agonist used in theprevention and treatment of gastric NSAID-inducedulcers. Its uterotonic and cervical ripening actions makeit an important drug in obstetrics for medical abortionand induction of labor. But this is also why it is exploitedand misused for pretermination of unwanted pregnan-cies.
Congenital anomalies, including Möbius sequence,associated with misoprostol use in failed abortion attemptshave been documented.12-14 Case series by Gonzalesreported Möbius sequence in 4 of 7 (53.1%) and 17 of 47(36.7%) of newborns exposed to misoprostol around 2months AOG.13-14 A cohort study done by Pastuszak15
showed that attempted abortion with misoprostol wasassociated with a significantly increased risk for Möbiussequence. Among the mothers of patients with Möbiussequence, 47 (49%) had used misoprostol compared with3 (3%) mothers from the other study group.
Studies have hypothesized that misoprostol’s uterotoniceffects cause contraction of the uterine vessels, inter-rupting blood supply to the primitive subclavian artery

PHILIPP J OPHTHALMOL VOL 34 NO. 1 JANUARY - JUNE 2009 33PHILIPPINE ACADEMY OF OPHTHALMOLOGY
References
1. Cronemberger MF, Moreira JB, Brunoni D, et al. Ocular and clinical manifestations
of Möbius syndrome. J Pediatr Ophthalmol Strab 2001; 41: 156-162.
2. Stromland K, Sjogreen L, Miller M, et al. Möbius sequence: a Swedish multidiscipline
study. Eur J Paediatr Neurol 2002; 6: 35-45.
3. Marques-Dias MJ, Gonzales CH, Rosemberg S. Möbius sequence in children
exposed in utero to misoprostol: neuropathological study of three cases. Birth Defects
Res A Clin Mol Teratol 2003; 67: 1002-1007.
4. Verzijl HF, van der Zwaag B, Cruysberg JRM, Padberg GW. Möbius syndrome
redefined: a syndrome of rhombencephalic maldevelopment. Neurology 2003; 61:
327-333.
5. Laby DM. Möbius syndrome. In: Rosembaum A and Santiago AP, eds. Clinical
Strabismus Management: Principles and Surgical Techniques. Philadelphia: W.B.
Saunders, 1999; Chap 26: 358-370.
6. Santiago AP, Uy CB. Möbius sequence with varied strabismus presentations in
Filipino patients. Philipp J Ophthalmol 2004: 29: 178-185.
7. Palmer CA. Emedicine. Möbius syndrome. 30 April 2007. http:// www.emedicine.com/
neuro/topic612.htm. Accesed July 2007.
8. Kniffin CL, McKusick VA, Smith M. Online Mendelian Inheritance in Man. Johns
Hopkins University. Möbius syndrome. http://www.ncbi.nih.gov/entrez/
dispomim.cgi?id=157900. Accesed July 2007.
9. Traboulski E. Congenital abnormalities of cranial-nerve development: overview,
molecular mechanisms, and further evidence of heterogeneity and complexity of
syndromes with congenital limitation of eye movements. Trans Am Ophthalmol 2004;
102: 373-389.
10. Bouwes Bavinck J, Weaver DD. Subclavian artery supply disruption sequence:
hypothesis of a vascular etiology for Poland, Klippel-Feil, and Möbius anomalies.
Am J Med Genet 1986; 23: 903-919.
11. Goldberg AB, Greenberg MB, Darney PD. Misoprostol and pregnancy. N Engl J
Med 2001; 344: 38-47.
12. Orioli IM, Castilla EE. Epidemiological assessment of misoprostol teratogenicity.
Br J Obstetr Gynaecol 2000; 107: 519-523.
13. Gonzales CH, Vargas FR, Perez ABA. Limb deficiency with or without Möbius
sequence in seven Brazilian children associated with misoprostol use in the first
trimester of pregnancy. Am J Med Genet 1993; 47: 59-64.
14. Gonzales CH, Marques-Dias JM, Kim CA, et al. Congenital abnormalities in Brazilian
children associated with misoprostol misuse in first trimester of pregnancy. The
Lancet 1998; 351: 1624-1627.
15. Pastuszak AL, Schuler L, Speck-Martins CE, et al. Use of misoprostol during
pregnancy and Möbius syndrome in infants. New Engl J Med 1998; 338: 1881-
1885.
16. Shepard TH. Möbius syndrome after misoprostol: a possible teratogenic mechanism.
The Lancet 1995; 346: 780.
with ischemic damage to the prenatal brainstem and otherinvolved embryonic end organs.10 The sixth and seventhcranial nerves are commonly affected possibly due to theirrhombencephalic position, a flexure point of the embryowhen misoprostol effects a uterine contraction.16 Neuropa-thological studies support this theory, where ischemic-anoxic foci of gliosis, necrosis, and calcification were notedfrom the dorsal pons to the medulla, involving somecranial-nerve nuclei.3
A study by Stromland and colleagues2 of 25 patientswith Möbius sequence noted abnormal patterns of tearing;6 patients, also diagnosed with autism, did not exhibitemotional tearing. This was a similar finding in a studyon thalidomide embryopathy, where subjects who hadsixth- and seventh-cranial-nerve palsy also had a highfrequency of aberrant tearing. Abnormal lacrimation isan unusual finding but may exist more frequently thanpreviously reported, as there is often no specific inquirymade regarding lacrimation. It is postulated to result fromaberrant innervation of the lacrimal gland. The nucleusfor lacrimation is situated in the brainstem close to thenuclei for cranial nerves VI and VII, a location that couldpossibly explain its association with palsy of the sixth andseventh cranial nerves.
There is no difference in the ophthalmologic manage-ment of patients with Möbius sequence with known in uteroexposure to misoprostol versus those with or without otherknown prenatal risk factors.
Nonsurgical ophthalmologic management includesdetection and treatment of amblyopia, giving bestcorrection, and prevention and treatment of primary andsecondary dry-eye conditions. Full cycloplegic refractionand patching are usually initially employed to correcterrors of refraction and deviation. Eye lubricants are givento prevent corneal decompensation.5
There is no single surgical approach to correct strabis-mus of patients with Möbius sequence. The most import-ant factor in surgical planning is the degree of residualabducting power present. These patients often haveseverely impaired or lack any abduction ability withsecondary medial rectus muscle contracture. Surgicaloptions include LR recessions/augmentations, transpo-sitions, and MR injection of Botulinum toxin.
In summary, attempted abortion with misoprostol isassociated with an increased risk of Möbius sequence ininfants. It is not uncommon that such patients are initiallybrought in for consultation for their ophthalmologiccondition. A history of misoprostol use for failed abortion
should be routinely elicited. Aside from strabismusevaluation, work-up should include testing for primarytear dysfunction (from aberrant cranial-ner ve-Vinnervation) as well as secondary causes of dry eye andassociated complications.
Besides treating specific eye problems, recognizing keysigns and symptoms and associated risk factors is importantin identifying patients suspected to have Möbiussequence. Associated deficiencies in Möbius sequence andits variants require a multidisciplinary approach fromdifferent subspecialties. Parent counseling and educationare invaluable. The public should be educated on thepotential teratogenic effects of misoprostol in order toreduce its use as an abortifacient.